Embed Size (px)
Citation preview

JOURNAL CLUB
CONTEMPORARY REVIEW
Contemporary Review of RhinoplastyPatrick C. Angelos, MD; Mark J. Been, MD; Dean M. Toriumi, MD
W e conducted a contemporary review covering advances and trends in primaryand functional rhinoplasty as published during the past decade. Specifically, wereviewed studies supporting the evidence for functional rhinoplasty, nasal valvesurgery, and septal reconstruction. In addition, key articles discussing cephalic
malpositioning of the lower lateral cartilages and tip contouring are reviewed. We also report stud-ies involving lateral osteotomy techniques, computer imaging, and the use of homologous, allo-plastic, and absorbable implants. When appropriate, we review outcomes data from key studiesbecause these data are becoming increasingly important for evidence-based medicine, physiciangrading, and procedure reimbursement. Using evidence-based approaches whenever possible willhelp to ensure predictable patient outcomes. Arch Facial Plast Surg. 2012;14(4):238-247
Rhinoplasty may be the most challengingprocedure in all of facial plastic surgery. Thisis evident in the fact that entire textbooksare devoted solely to the topic. While basicprinciples remain largely unchanged, newconcepts and techniques are continuouslyevolving (Table). This contemporary re-view seeks to cover some of the more re-cent advances in rhinoplasty surgery.
OUTCOMES IN FUNCTIONALRHINOPLASTY AND NASAL
VALVE REPAIR
One of the continuing challenges in rhino-plasty has been the lack of randomized con-trolled trials. This lack is in part due to theinherent ethical concern in blindly random-izing surgical procedures. Therefore, muchof the current evidence is based on obser-vation and retrospective studies. Rhee andcolleagues5 performed a 25-year system-atic literature review to search for evi-dence supporting the role of functional rhi-noplasty and nasal valve repair. After amultistep search, the authors filtered infor-mation, including various interventions and
outcomes measures. In data extraction andquality assessment, 44 articles ultimatelymet inclusion criteria based on quality re-view and were assigned a level of evidence.These studies collectively enrolled morethan 2295 patients, and the procedures in-cluded batten grafts, spreader grafts, but-terfly onlay grafts, structural bone grafts, andsuture suspension. Rhee et al5 graded 42 ofthe 44 studies as level IV (case series/case
report) evidence and only 2 studies as levelIIb (cohort studies). Owing to the lack ofstudies with higher levels of evidence andthe heterogeneity of study designs and out-comesmeasuresreported,poolingofthedatawas not possible and a true meta-analysiscould not be conducted. However, in thatreview, all 44 studies reported improve-ments as a whole for treated cohorts withnasal valve collapse in a consistent effect.
CME available online atwww.jamaarchivescme.comand questions on page 233
Journal Club slides availableat www.archfacial.com
Author Affiliations: Department of Otolaryngology–Head and Neck Surgery,University of Illinois at Chicago.
ARCH FACIAL PLAST SURG/ VOL 14 (NO. 4), JULY/AUG 2012 WWW.ARCHFACIAL.COM238
©2012 American Medical Association. All rights reserved.
Downloaded From: http://archfaci.jamanetwork.com/ by a Emory University User on 11/25/2012
Another limitation in studying outcomes in functionalrhinoplasty is the lack of objective tools for the preopera-
tive and postoperative assessments of nasal valve insuffi-ciency. Rhinomanometry, which measures nasal cavity
Table. Overview of Studies Evaluated
Source Aim/Objective Study Size Study Design Outcomes Conclusions
GryskiewiczandGryskiewicz,12004
Comparison ofperforating vscontinuous lateralosteotomytechniques onpostoperativeecchymosis andedema
75 Total patientsdivided into 3arms of 25patients each,testing variousosteotomytechniques
Prospective,randomized,partiallyblindedstudy
After testing both methods, theperforating internal method wassuperior (group A; P � .01 in bothtests)
Perforating lateral osteotomies with a2-mm straight osteotome reducepostoperative ecchymosis and edemain rhinoplasty patients compared withthe continuous osteotomy (4-mmcurved, guarded osteotome)
Constantian,22005
Review and evaluatethesis that the boxyor ball nasal tip arenot unique entitiesbut rather variants ofalar cartilagemalposition
100 Consecutivepatientsundergoingprimary and 100consecutivepatientsundergoingsecondaryrhinoplasties
Retrospectiveanalysis
68% Of primary rhinoplasty patientsand 87% of secondary patients hadalar cartilage malposition (P � .001);orthotopic lateral crura weresignificantly more common thanmalpositioned lateral crura inprimary rhinoplasty (P � .001);frequency of malpositioned crurawas significantly higher in secondaryrhinoplasty (P � .001)
Although patients undergoing openrhinoplasty have more complaints andmore postoperative deformities, theseoutcomes may be inherent with theirinitial problems, necessitating an openapproach initially
Most,3 2006 Review outcomes infunctional rhinoplastydescribing a modifiedextracorporealseptoplastytechnique
12 Consecutivepatients
Prospectiveobservationaloutcomesstudy
Significant improvement in meanpostoperative NOSE score for entirecohort (P � .01)
Anterior septal reconstruction techniqueimproves nasal airway function andaesthetics in severe septonasaldeviation and avoids the most commoncomplication of standardextracorporeal septoplasty bypreserving the dorsal strut of septalcartilage and its attachment to thenasal bones at the keystone area
Toriumi,4 2006 Identify ideal tipcharacteristics anddescribe newconcepts in nasal tipcontouring
No patients Computermodel andclinicalreview
Numerous aesthetically pleasing nasaltips were evaluated and a series ofimages was created to demonstratehow specific contours createhighlights and shadows
These concepts will help surgeons focusmore on creating favorable shadowsand highlights and less on narrowing;contouring will look more natural andbetter withstand the forces of scarcontracture and its negative effect onrhinoplasty outcomes
Rhee et al,52008
Systematic review ofevidence supportingfunctional rhinoplastyor nasal valve repair
82 Articles reviewed,of which 44 metinclusion criteria
Systematicreview
Most studies were level IV evidence;2 were level IIb; all generallysupported effectiveness of functionalrhinoplasty
Substantial level IV evidence supports theefficacy of modern-day rhinoplastytechniques for treatment of nasal valvecollapse; use of comparison cohortsand standardized objective outcomemeasures will improve future studies
James andKelly,6 2008
Review cartilagerecycling inrhinoplasty usingPDS foil as anabsorbablebiomechanicalscaffold, indications,complications, andlong-term stability
58 Primary andsecondaryrhinoplasties inwhich PDS foilwas used withautologouscartilage foraesthetic andvalvularreconstruction
Retrospectiveoutcomeanalysis
The PDS foil was used most often toconstruct columellar struts, septalextension grafts, and alar battens;other uses included revisionseptoplasty and upper lateralreplacement grafts; minorcomplications (1 infection, 1 partialextrusion); long-term postoperativestability of the nose was satisfactory(mean FU, 18 mo) for structural andaesthetic purposes
Technique is simple and effective; makingmaximal use of otherwise discardedcartilage fragments protects other graftharvest sites and decreases incidenceof graft depletion
Peled et al,72008
Perform meta-analysisof commonly usedmaterials anddescribe removalrates
14 Studies Meta-analysis The most commonly used materials aresilicone, expanded PTFE, and porousHDPE; the removal rate for PTFE andHDPE implants was 3.1%; forsilicone implants, significantly higherat 6.5%
Alloplastic implants have acceptablecomplication rates and can be usedwhen autogenous materials areunavailable or insufficient; outcomeswith HDPE or PTFE implants may beslightly better than those with silicone;improved reporting of implant failuresand FU times are needed to betterdefine specific guidelines for use ofthese materials
Kridel et al,82009
Evaluate the use ofIHCC grafts
357 Patientsundergoingprimary orsecondaryrhinoplasty withIHCC grafts
Retrospectiveanalysis
Total complication rate of 3.25%,including graft warping, infection,resorption, and mobility; patientsatisfaction was �94% after a meanFU of 7.87 y
As a grafting material in rhinoplasty, IHCCis well tolerated and yields superbfunctional, structural, and cosmeticresults
Boahene andHilger,92009
Review indications,technique, andoutcomes of alarrim grafting inrhinoplasty
31 Patients Retrospectiveanalysis
Indications were cephalic position ofthe LLCs, correction of alar flare, andalar collapse; no complications at amean FU of 6 mo
Alar rim grafting is a simple and versatileapproach to providing additionalsupport to external nasal valve and forimproving nasal base contour
(continued)
ARCH FACIAL PLAST SURG/ VOL 14 (NO. 4), JULY/AUG 2012 WWW.ARCHFACIAL.COM239
©2012 American Medical Association. All rights reserved.
Downloaded From: http://archfaci.jamanetwork.com/ by a Emory University User on 11/25/2012
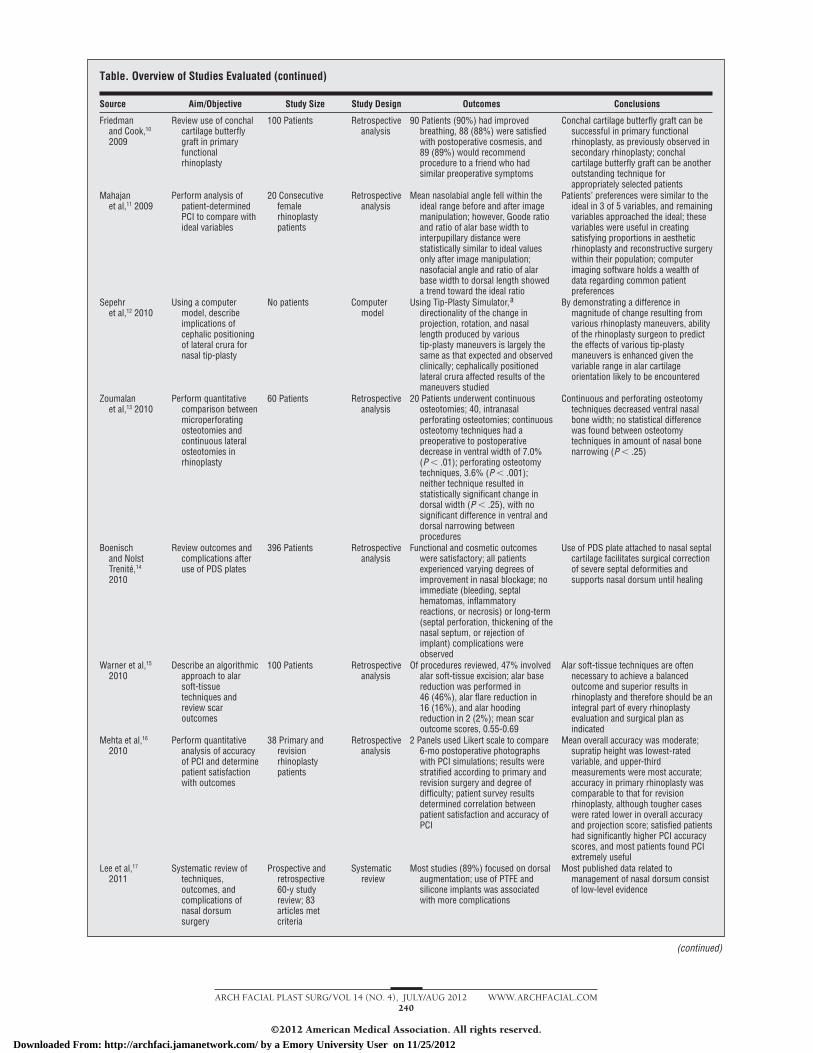
Table. Overview of Studies Evaluated (continued)
Source Aim/Objective Study Size Study Design Outcomes Conclusions
Friedmanand Cook,10
2009
Review use of conchalcartilage butterflygraft in primaryfunctionalrhinoplasty
100 Patients Retrospectiveanalysis
90 Patients (90%) had improvedbreathing, 88 (88%) were satisfiedwith postoperative cosmesis, and89 (89%) would recommendprocedure to a friend who hadsimilar preoperative symptoms
Conchal cartilage butterfly graft can besuccessful in primary functionalrhinoplasty, as previously observed insecondary rhinoplasty; conchalcartilage butterfly graft can be anotheroutstanding technique forappropriately selected patients
Mahajanet al,11 2009
Perform analysis ofpatient-determinedPCI to compare withideal variables
20 Consecutivefemalerhinoplastypatients
Retrospectiveanalysis
Mean nasolabial angle fell within theideal range before and after imagemanipulation; however, Goode ratioand ratio of alar base width tointerpupillary distance werestatistically similar to ideal valuesonly after image manipulation;nasofacial angle and ratio of alarbase width to dorsal length showeda trend toward the ideal ratio
Patients’ preferences were similar to theideal in 3 of 5 variables, and remainingvariables approached the ideal; thesevariables were useful in creatingsatisfying proportions in aestheticrhinoplasty and reconstructive surgerywithin their population; computerimaging software holds a wealth ofdata regarding common patientpreferences
Sepehret al,12 2010
Using a computermodel, describeimplications ofcephalic positioningof lateral crura fornasal tip-plasty
No patients Computermodel
Using Tip-Plasty Simulator,a
directionality of the change inprojection, rotation, and nasallength produced by varioustip-plasty maneuvers is largely thesame as that expected and observedclinically; cephalically positionedlateral crura affected results of themaneuvers studied
By demonstrating a difference inmagnitude of change resulting fromvarious rhinoplasty maneuvers, abilityof the rhinoplasty surgeon to predictthe effects of various tip-plastymaneuvers is enhanced given thevariable range in alar cartilageorientation likely to be encountered
Zoumalanet al,13 2010
Perform quantitativecomparison betweenmicroperforatingosteotomies andcontinuous lateralosteotomies inrhinoplasty
60 Patients Retrospectiveanalysis
20 Patients underwent continuousosteotomies; 40, intranasalperforating osteotomies; continuousosteotomy techniques had apreoperative to postoperativedecrease in ventral width of 7.0%(P � .01); perforating osteotomytechniques, 3.6% (P � .001);neither technique resulted instatistically significant change indorsal width (P � .25), with nosignificant difference in ventral anddorsal narrowing betweenprocedures
Continuous and perforating osteotomytechniques decreased ventral nasalbone width; no statistical differencewas found between osteotomytechniques in amount of nasal bonenarrowing (P � .25)
Boenischand NolstTrenite,14
2010
Review outcomes andcomplications afteruse of PDS plates
396 Patients Retrospectiveanalysis
Functional and cosmetic outcomeswere satisfactory; all patientsexperienced varying degrees ofimprovement in nasal blockage; noimmediate (bleeding, septalhematomas, inflammatoryreactions, or necrosis) or long-term(septal perforation, thickening of thenasal septum, or rejection ofimplant) complications wereobserved
Use of PDS plate attached to nasal septalcartilage facilitates surgical correctionof severe septal deformities andsupports nasal dorsum until healing
Warner et al,15
2010Describe an algorithmic
approach to alarsoft-tissuetechniques andreview scaroutcomes
100 Patients Retrospectiveanalysis
Of procedures reviewed, 47% involvedalar soft-tissue excision; alar basereduction was performed in46 (46%), alar flare reduction in16 (16%), and alar hoodingreduction in 2 (2%); mean scaroutcome scores, 0.55-0.69
Alar soft-tissue techniques are oftennecessary to achieve a balancedoutcome and superior results inrhinoplasty and therefore should be anintegral part of every rhinoplastyevaluation and surgical plan asindicated
Mehta et al,16
2010Perform quantitative
analysis of accuracyof PCI and determinepatient satisfactionwith outcomes
38 Primary andrevisionrhinoplastypatients
Retrospectiveanalysis
2 Panels used Likert scale to compare6-mo postoperative photographswith PCI simulations; results werestratified according to primary andrevision surgery and degree ofdifficulty; patient survey resultsdetermined correlation betweenpatient satisfaction and accuracy ofPCI
Mean overall accuracy was moderate;supratip height was lowest-ratedvariable, and upper-thirdmeasurements were most accurate;accuracy in primary rhinoplasty wascomparable to that for revisionrhinoplasty, although tougher caseswere rated lower in overall accuracyand projection score; satisfied patientshad significantly higher PCI accuracyscores, and most patients found PCIextremely useful
Lee et al,17
2011Systematic review of
techniques,outcomes, andcomplications ofnasal dorsumsurgery
Prospective andretrospective60-y studyreview; 83articles metcriteria
Systematicreview
Most studies (89%) focused on dorsalaugmentation; use of PTFE andsilicone implants was associatedwith more complications
Most published data related tomanagement of nasal dorsum consistof low-level evidence
(continued)
ARCH FACIAL PLAST SURG/ VOL 14 (NO. 4), JULY/AUG 2012 WWW.ARCHFACIAL.COM240
©2012 American Medical Association. All rights reserved.
Downloaded From: http://archfaci.jamanetwork.com/ by a Emory University User on 11/25/2012

pressure and flow, and acoustic rhinometry, which ana-lyzes the nasal cross-sectional area as a function of dis-tance from the nostrils, are objective measures of nasal ob-struction,but thesemeasuresareusedprimarily for researchpurposes and are not commonly used in the clinic. Studieshave shown little or no correlation between these tech-niques and the patient’s subjective symptoms or the sever-ityofnasal airwayobstruction.20 Peaknasal inspiratory flowis another tool used to measure the highest airflow a pa-tient can achieve during maximum forced nasal inspira-tion throughbothnostrils. Inherentweaknessesof this tech-nique include being effort dependent and its incorporationof lung function. Studies have found a poor correlation be-tween peak nasal inspiratory flow vs rhinomanometry andacoustic rhinometry.21 All objective tests currently avail-able share the common weakness of poor correlation withpatient symptomscores.22 Therefore,other tools areneededto objectively measure nasal airway obstruction.
Historically, no disease-specific quality-of-life instru-ment has been available to assess rhinoplasty tech-niques, and reports have used general rhinologic quality-of-life measures and other non–disease-specific measures.In response to the lack of a disease-specific quality-of-life instrument, the Nasal Obstruction Symptom Evalu-ation (NOSE) scale was developed.23 In the NOSE trial,Stewart and colleagues23 used this instrument to mea-sure subjective sensation of nasal obstruction. The NOSEscale serves as one of the primary accepted tools to as-sess postoperative nasal obstruction subjectively.
Using the NOSE instrument, Most24 conducted a pro-spective study of 41 patients to assess the efficacy of func-tional rhinoplasty techniques in improving disease-specificqualityof life.Selectedpatientshadnasalobstructionfor at least 1 year as the result of an identifiable anatomiccause, including septal deviation, turbinate hypertrophy,and internal or external valve collapse. Mean NOSE scoresdecreased in all patients who underwent functional rhino-plasty (58.4 v. 15.7; P� .01), with lower scores indicatingimprovements in nasal obstruction. Most24 also based theexamination of NOSE scores on the procedure performed,
including spreader grafting (all inclusive), spreader graft-ing with septoplasty and turbinate modification, spreadergrafting without turbinate modification, external valve sus-pension, and septoplasty with turbinate reduction. Eachsubgroup of patients demonstrated significant improve-ments in postoperative NOSE scores.
Recent advances and techniques in nasal valve sur-gery and middle vault reconstruction beyond tradi-tional spreader grafts include conchal cartilage butterflygrafts and autospreader flaps. Butterfly grafts, which wereinitially described for secondary rhinoplasty, have alsobeen shown to be effective in primary functional rhino-plasty in properly selected patients.10 A relatively new tech-nique in primary rhinoplasty is the autospreader flap. Thistechnique involves using the transverse portion of the up-per lateral cartilage rotated medially to function as aspreader graft (Figure 1).
To validate the use of conchal cartilage butterfly graftsin primary rhinoplasty, Friedman and Cook10 collectedoutcomes data regarding patient satisfaction, nasal ob-struction, and cosmesis in 100 patients who were iden-tified as having nasal valve collapse on examination usinga modified Cottle maneuver. After septorhinoplasty withconchal cartilage butterfly grafting (without concurrentturbinate procedures), approximately 90% of the pa-tients reported improved breathing, were satisfied withtheir cosmesis, and would recommend the procedure.Friedman and Cook10 concluded that this graft is effec-tive in primary functional rhinoplasty; however, theirstudy was limited by its retrospective nature and lack ofa validated instrument such as the NOSE scale.
In a recent study to measure the efficacy of a mid-vault reconstruction technique (the autospreader flap)in dorsal reductive rhinoplasty, Yoo and Most18 per-formed a prospective observational study using this tech-nique and analyzed outcomes using the NOSE scale. Theauthors hypothesized that patients undergoing cos-metic rhinoplasty without preexisting nasal obstruction
Table. Overview of Studies Evaluated (continued)
Source Aim/Objective Study Size Study Design Outcomes Conclusions
Yoo and Most,18
2011Outcomes of
autospreadertechnique basedon NOSE scale
38 Patients,including anaesthetic groupwithoutobstructivecomplaints and acombinedfunctional andaesthetic groupwith obstruction
Prospectiveobservationaloutcomesstudy
Aesthetic group had low preoperativeNOSE scores without significantpostoperative change; the obstructedgroup had significant reduction inNOSE scores (P � .001)
Midvault reconstruction usingautospreader graft may help preventpostoperative nasal obstruction dueto midvault collapse
Rohrich et al,19
2012Review indications
and outcomes ofcolumellar strutsin primaryrhinoplasty
1491 Primaryrhinoplastypatients withcolumellar strutplacement
Retrospectiveanalysis
Struts were most commonly placed tomaintain adequate tip projection(34%), to address tip asymmetry(26%), for a combination of these(22%), and to address intraoperativeloss of tip projection (12%); 6% whohad a strut required revision surgeryfor excessive columellar show
Authors describe short struts, longfloating struts, and long fixed strutsand indications for each based onstrength and symmetry of LLCs andadequacy of tip projection
Abbreviations: FU, follow-up; HDPE, high-density polyethylene (Medpor; Porex Surgical, Inc); IHCC, irradiated homologous costal cartilage; LLC, lower lateralcartilage; NOSE, Nasal Obstruction Symptoms Evaluation; PCI, preoperative computer imaging; PDS, polydioxanone; PTFE, polytef (Gore-Tex; WL Gore & Associates,Inc).
a Indicates Matlab Tip-Plasty Simulator software (MathWorks).
ARCH FACIAL PLAST SURG/ VOL 14 (NO. 4), JULY/AUG 2012 WWW.ARCHFACIAL.COM241
©2012 American Medical Association. All rights reserved.
Downloaded From: http://archfaci.jamanetwork.com/ by a Emory University User on 11/25/2012

and those undergoing combined aesthetic and func-tional rhinoplasty would not exhibit worsening nasal ob-struction. In their study, patients were divided into thosewithout nasal obstruction who underwent aesthetic rhi-noplasty and those with concomitant severe nasal ob-struction due to septal deviation, turbinate hypertro-phy, or valvular insufficiency who required aesthetic andfunctional rhinoplasty. The NOSE scale was used to as-sess preoperative and postoperative degrees of nasal ob-struction. Thirty-eight patients completed all question-naires. In the 21 patients undergoing aesthetic rhinoplastyalone, the preoperative mean NOSE scores were low and,although postoperative scores improved, the change didnot reach statistical significance. In the group undergo-ing combined functional rhinoplasty and aesthetic rhi-noplasty, significant improvement in mean postopera-tive NOSE scores occurred. The preoperative NOSE scoresfor the combined rhinoplasty group were significantlyhigher than the scores for the cosmetic rhinoplasty group.
These results, as noted by the senior author, compare fa-vorably with the previously published studies on func-tional rhinoplasty.
OUTCOMES IN SEPTAL RECONSTRUCTION
Nasal septal deformity is a significant contributor to na-sal obstruction and is an extremely common problem en-countered in rhinoplasty. With adequate preservation ofthe dorsal-caudal L-strut, mild septal deviation may betreated with traditional septoplasty procedures involvingsubmucous resection techniques. More severe and com-plex deformities may require advanced techniques, in-cluding caudal-septal extension and replacement grafts.In an effort to measure the efficacy of a modified extra-corporeal technique for anterior septal reconstruction,Most3 reported the outcomes in a series of 12 patients. Inthat prospective observational study, preoperative and post-operative evaluations were performed using photographsand the NOSE scale. The reported technique for anteriorseptal reconstruction was a modified extracorporeal tech-nique designed to preserve a dorsal remnant at the key-stone area. This technique used an external rhinoplastyapproach with a hemitransfixion incision of the left side.In analysis of the outcomes, no notching or saddling oc-curred during the average follow-up of 5.4 months. Na-sal obstruction was improved, with average NOSE scoresdecreased for patients who underwent anterior septal re-placement, with or without turbinectomy (P� .01).
CEPHALIC MALPOSITIONINGOF LOWER LATERAL CARTILAGES
AND NASAL TIP CONTOURING
Currently one of the popular topics in rhinoplasty is ce-phalic orientation or malposition of the alar cartilages,specifically, the lateral crura of the lower lateral carti-lages (LLCs) (Figure 2). Although this concept is notnew, increasing attention and studies have led to betterdescription of this anatomic variant and techniques foraltering position and ultimately tip shape.
A
B
Figure 1. Diagram of the autospreader technique. A, The upper lateralcartilage is scored after hump takedown, parallel to the nasal bone. B, Theupper lateral cartilage is turned in and sutured in mattress fashion to theseptum. Reprinted from Yoo and Most.18
A B
Figure 2. Malposition of the alar cartilages. A, Anteroposterior (frontal) viewwith the lateral crura in orthotopic position. B, Anteroposterior (frontal) viewwith the lateral crura in cephalic position. The green lines indicate the vectorof the right lateral crus; blue lines, the vector of the left lateral crus; blacklines, the vertical midsagittal line; and angle, the angle between the lateralcrural vector and the midsagittal line. Reprinted from Sepehr et al.12
ARCH FACIAL PLAST SURG/ VOL 14 (NO. 4), JULY/AUG 2012 WWW.ARCHFACIAL.COM242
©2012 American Medical Association. All rights reserved.
Downloaded From: http://archfaci.jamanetwork.com/ by a Emory University User on 11/25/2012

The thesis of a recent study by Constantian2 of 200consecutive patients undergoing primary and second-ary rhinoplasty is that most boxy and ball tips are notunique entities but rather constitute anatomic variantsof alar cartilage malposition. In that review, lateral cru-ral orientation was defined by the axis of the crus lateralto the lateral genu. Orthotopic lateral crura were de-scribed as running toward the lateral canthus of the ip-silateral eye; cephalically malpositioned lateral crura rantoward the ipsilateral medial canthus. Constantian2 foundthat most patients (68% of primary and 87% of second-ary rhinoplasty patients) had alar cartilage malposition.Orthotopic lateral crura were more common in primaryrhinoplasty patients; malpositioned lateral crura weremore common in secondary rhinoplasty patients. In allpatients with alar cartilage malposition, including pri-mary and secondary rhinoplasty patients regardless oflobular configuration, valvular reconstruction as mea-sured by rhinomanometry at least doubled the geomet-ric mean nasal airflow in most patients. For surgical cor-rection, all primary rhinoplasty patients underwentdissection of the lateral crura and replacement along thealar rim, whereas some secondary rhinoplasty patientsalso required composite grafts. From these results, theauthor concluded that patients with a boxy or a ball tipare much more likely to have malpositioned lateral cruraand the associated functional deficits.
In a mathematical model to determine the relative ef-fectiveness of various tip rhinoplasty (tip-plasty) maneu-vers on cephalic positioning of the lateral crura, Sepehret al12 estimated the results of changes in projection, ro-tation, and nasal length for overall changes in the lengthof the lateral crura. Various commonly used rhinoplastytechniques, including alar strut grafts and lateral cruralrepositioning, were modeled in a software program (theMatlab Tip-Plasty Simulator; MathWorks). The authorsfound that the modeled changes in projection, rotation,and nasal length of various surgical maneuvers are largelythe same as those observed clinically. Specifically, ce-phalically positioned lateral crura (as compared with or-thotopic lateral crura) affect the results of the various tip-plasty maneuvers, including changes in projection,rotation, and nasal length. Sepehr et al12 concluded thatthe cephalically positioned lateral crura can affect the re-
sults of various tip-plasty surgical maneuvers, at least asmeasured geometrically in a computer model.
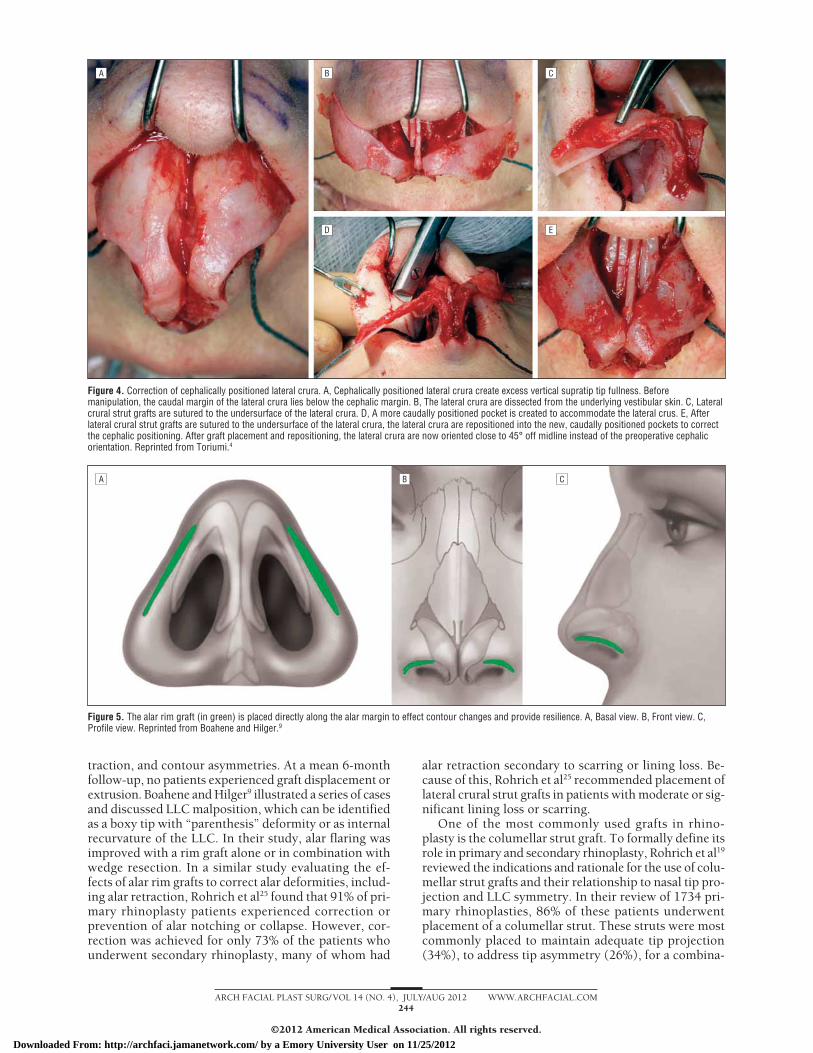
Nasal tip refinement is one of the more common andchallenging goals in rhinoplasty, especially in creating anatural-appearing tip, because this procedure is com-plex and 3-dimensional. In an effort to identify the char-acteristics that make an ideal nasal tip, Toriumi4 evalu-ated numerous aesthetically pleasing nasal tips and createda series of images to demonstrate how specific contourscreate shadows and highlights that can help guide thesurgeon in creating a natural-appearing tip. A more natu-ral-appearing tip, as the composite images demon-strated, possessed a horizontally oriented tip highlightwith a smooth transition from the tip lobule to the alarlobule. A key indicator of a favorable tip shape was astraight undisturbed line from tip lobule to alar lobuleon the base view (Figure 3). This treatise in tip rhino-plasty also covered various concepts in the analysis ofnasal contours, tip aesthetics, stabilization of the base ofthe nose, and techniques to control nasal tip contour. Thearticle included a discussion on cephalic positioning ofthe lateral crura and provided surgical techniques, in-cluding lateral crural strut grafts with caudal reposition-ing of the lateral crura (Figure 4).
Alar rim grafts are useful in repositioning of the alarmargin, providing support, correcting asymmetries, andhelping to prevent external valve collapse along the nos-tril margin.25 These long narrow grafts are placed in a pre-cise pocket just caudal to the area of the marginal inci-sion at the caudal border of the lateral crus (Figure 5).These grafts provide moderate support against caudal lat-eral wall collapse but are often not needed in cases of lat-eral crural strut grafting with caudal repositioning.4 In aretrospective review to determine the potential indica-tions for placement of alar rim grafts in primary and re-vision rhinoplasty, Boahene and Hilger9 reported theirindications and technique and reviewed the functionaland aesthetic outcomes in a series of 150 patients. Theyidentified 31 cases (26 primary and 5 revision rhinoplas-ties) in which alar rim grafting was used. The most fre-quently identified indications for placement of alar rimgrafts were cephalic malposition of the LLCs (29%) andcorrection of alar flare (29%). Other reported indica-tions included dynamic external valve collapse, alar re-
BA
Figure 3. A favorable nasal tip contour has ahorizontal orientation with a shadow in thesupratip area that continues into thesupra-alar regions. A, There is a smoothtransition from the tip lobule to the alarlobule without a line of demarcation. Thetip-defining points are seen as a horizontallyoriented highlight with shadows above andbelow. B, The base view shows a triangularshape with no notching between the tiplobule and the alar lobule. The horizontalcomponent of the nasal tip with a definedwidth is set by the position of the domes.Reprinted from Toriumi.4
ARCH FACIAL PLAST SURG/ VOL 14 (NO. 4), JULY/AUG 2012 WWW.ARCHFACIAL.COM243
©2012 American Medical Association. All rights reserved.
Downloaded From: http://archfaci.jamanetwork.com/ by a Emory University User on 11/25/2012
traction, and contour asymmetries. At a mean 6-monthfollow-up, no patients experienced graft displacement orextrusion. Boahene and Hilger9 illustrated a series of casesand discussed LLC malposition, which can be identifiedas a boxy tip with “parenthesis” deformity or as internalrecurvature of the LLC. In their study, alar flaring wasimproved with a rim graft alone or in combination withwedge resection. In a similar study evaluating the ef-fects of alar rim grafts to correct alar deformities, includ-ing alar retraction, Rohrich et al25 found that 91% of pri-mary rhinoplasty patients experienced correction orprevention of alar notching or collapse. However, cor-rection was achieved for only 73% of the patients whounderwent secondary rhinoplasty, many of whom had
alar retraction secondary to scarring or lining loss. Be-cause of this, Rohrich et al25 recommended placement oflateral crural strut grafts in patients with moderate or sig-nificant lining loss or scarring.
One of the most commonly used grafts in rhino-plasty is the columellar strut graft. To formally define itsrole in primary and secondary rhinoplasty, Rohrich et al19
reviewed the indications and rationale for the use of colu-mellar strut grafts and their relationship to nasal tip pro-jection and LLC symmetry. In their review of 1734 pri-mary rhinoplasties, 86% of these patients underwentplacement of a columellar strut. These struts were mostcommonly placed to maintain adequate tip projection(34%), to address tip asymmetry (26%), for a combina-
A B C
D E
Figure 4. Correction of cephalically positioned lateral crura. A, Cephalically positioned lateral crura create excess vertical supratip tip fullness. Beforemanipulation, the caudal margin of the lateral crura lies below the cephalic margin. B, The lateral crura are dissected from the underlying vestibular skin. C, Lateralcrural strut grafts are sutured to the undersurface of the lateral crura. D, A more caudally positioned pocket is created to accommodate the lateral crus. E, Afterlateral crural strut grafts are sutured to the undersurface of the lateral crura, the lateral crura are repositioned into the new, caudally positioned pockets to correctthe cephalic positioning. After graft placement and repositioning, the lateral crura are now oriented close to 45° off midline instead of the preoperative cephalicorientation. Reprinted from Toriumi.4
A B C
Figure 5. The alar rim graft (in green) is placed directly along the alar margin to effect contour changes and provide resilience. A, Basal view. B, Front view. C,Profile view. Reprinted from Boahene and Hilger.9
ARCH FACIAL PLAST SURG/ VOL 14 (NO. 4), JULY/AUG 2012 WWW.ARCHFACIAL.COM244
©2012 American Medical Association. All rights reserved.
Downloaded From: http://archfaci.jamanetwork.com/ by a Emory University User on 11/25/2012

tion of the previous two (22%), and to address the in-traoperative loss of tip projection (12%). Rohrich et al19
described short struts, long floating struts, and long fixedstruts and the indications for each based on strength andsymmetry of the LLCs and adequacy of tip projection.In this series, 6% of patients who had a strut requiredrevision surgery for excessive columellar show second-ary to improper carving, placement, or fixation of the strut.
Alar soft-tissue techniques, especially alar base and/orflare reduction, are commonly used in rhinoplasty. Un-til recently, little in the literature summarized these tech-niques and reported outcomes with scar analysis. In a de-scription of alar soft-tissue techniques in rhinoplasty,Warner et al15 presented an algorithmic approach andidentified quantifiable guidelines and scar outcomes ina series of 100 patients undergoing rhinoplasty. In theirseries, 47% of patients underwent alar soft-tissue exci-sion, highlighting how common these procedures are inrhinoplasty. Alar base resection was by far the most com-mon alar soft-tissue technique performed, followed byalar flare reductions; alar hooding resections were per-formed very infrequently. By quantitatively examiningscar outcomes, findings from their study suggest that scarsafter the use of these techniques heal exceptionally well,even without dermabrasion, which was performed in somepatients in a similar study by Kridel and Castellano.26
OSTEOTOMIES
Nasal osteotomies are commonly used to narrow a widebony vault, to close an open-roof deformity, or tostraighten deviated nasal bones. Two basic techniques areused for performing lateral osteotomies. The first, a con-tinuous technique, creates a single continuous fractureline. The second, a perforating technique, creates a post-age-stamp fracture pattern that can be made into a con-tinuous fracture by digital manipulation.
In a clinical comparison between osteotomy tech-niques in rhinoplasty,1 a prospective, randomized, par-tially blinded study was designed to test the hypothesisthat the perforating method causes less postoperative ec-chymosis and edema compared with the continuous lat-eral osteotomy technique. Gryskiewicz and Gryskie-wicz1 demonstrated, by means of a subjective clinicalimpression, that perforating lateral osteotomies with a2-mm straight osteotome reduced postoperative ecchy-mosis and edema in rhinoplasty patients compared withthe continuous osteotomy (with a 4-mm curved, guardedosteotome).
In another study to compare microperforating and con-tinuous lateral osteotomies quantitatively in rhino-plasty, Zoumalan et al13 determined the difference in na-sal bone narrowing between the 2 techniques. Their studywas a retrospective analysis of 2 groups of patients eachundergoing 1 technique. The first group consisted of 20consecutive patients from 2000 through 2003 who hadisolated lateral continuous osteotomies. The second groupconsisted of 40 consecutive patients from 2003 through2005 who received isolated lateral perforating osteoto-mies. Preoperative and postoperative photographs wereused for a blinded analysis of ventral (junction of the flat-tened surface of the maxilla and the ascending process
of the maxilla) and dorsal (width of the plateau or dor-sal nasal highlight) widths as measured on the frontal viewwith a fixed interpupillary distance to create a multi-plier. Zoumalan et al13 found that both techniques re-sulted in a decrease in ventral nasal width, neither tech-nique resulted in a significant change in dorsal width,and there was no difference in ventral and dorsal nar-rowing when comparing the 2 techniques.
HOMOLOGOUS, ALLOPLASTIC, ANDABSORBABLE GRAFTING MATERIALS
Homologous grafts that are commonly used in rhino-plasty include irradiated rib for structural grafting andacellular dermal matrix for soft-tissue augmentation.These grafting sources historically have been believed tobe less predictable than autologous tissue in their abilityto resist resorption and warping. This view, however, isassociated with studies with low levels of evidence, in-consistent design, small patient numbers, and short follow-up. Similarly, previous studies evaluating the use ofalloplastic materials have not provided definitive recom-mendations on implant selection, location, and long-term follow-up expectations.
In a follow-up study to their preliminary report, Kridelet al8 helped change this concept with a long-term (24-year) study of irradiated homologous costal cartilage(IHCC) grafts in 357 patients. Their retrospective re-view included 1025 irradiated rib grafts that were evalu-ated for warping, infection, resorption, mobility, and ex-trusion. A total of 1025 IHCC grafts (including 201 dorsalgrafts) and 373 other grafts (including 218 autogenouscartilage grafts) were used. The total complication raterelated to IHCC grafts was 3.25%, which included warpedgrafts, infections, resorption, and graft mobility. Of the218 autologous cartilage grafts used at the same opera-tive intervention along with IHCC grafts, 3 (1.38%) un-derwent minimal resorption. The overall comparative re-sorption rates were 1.01% for IHCC vs 1.37% forautologous cartilage. Kridel et al8 concluded that theseresults justify the use of IHCC grafts in rhinoplasty basedon safety, reliability, time, and cost-effectiveness.
In a recent meta analysis on the use of alloplastic ma-terials in rhinoplasty surgery, Peled et al7 reported theirfindings with the 3 most commonly used implants. Aftera systematic review, additional search, and independentextraction, they selected 20 articles for meta-analysis witha mean follow-up ranging from 1 month to 11 years. Thealloplastic materials most commonly used included sili-cone, expanded polytef (Gore-Tex; WL Gore & Associ-ates, Inc), and porous high-density polyethylene (Med-por; Porex Surgical, Inc). The overall implant removal ratewas highest for silicone at 6.5%. The polytef and high-density polyethylene implants had similar removal ratesat 3.1%. Although these data may not capture the overallor true removal rates for alloplastic materials, they pro-vide evidence of the safety of these implants. Peled et al7
conclude that improved reporting of implant failures andlonger follow-up are needed to better define the specificguidelines for the use of these materials.
In a systematic review of techniques addressing thenasal dorsum, Lee et al17 isolated articles providing data
ARCH FACIAL PLAST SURG/ VOL 14 (NO. 4), JULY/AUG 2012 WWW.ARCHFACIAL.COM245
©2012 American Medical Association. All rights reserved.
Downloaded From: http://archfaci.jamanetwork.com/ by a Emory University User on 11/25/2012

on outcomes and complications of various techniques.Of the 83 articles meeting inclusion criteria, 89% fo-cused on augmentation, showing acceptable results withgenerally low levels of complications with the use of vari-ous types of cartilage, bone, and soft tissue. The use ofsynthetic implants, such as polytef and silicone, showedhigher complication rates, including displacement andextrusion, but overall acceptable results. Lee et al17 notedthat most of the published data related to managementof the nasal dorsum is low-level evidence, and further levelI, II, and III studies are warranted.
A new and increasingly popular method of graftingand scaffolding in rhinoplasty involves the use of polydi-oxanone (PDS) resorbable plates (Mentor Worldwide)in combination with cartilage grafts. These plates, ini-
tially developed for use in orbital reconstruction, are beingused for septal reconstruction and in combination withautologous cartilage for various grafts in rhinoplasty.14
In an outcomes analysis of 58 primary and secondaryrhinoplasties in which PDS plates were used in combi-nation with autologous cartilage for aesthetic and val-vular reconstruction of the nose, James and Kelly6 re-ported graft performance, complications, and technicalaspects of PDS plate use. These authors evaluated com-parative photographic documentation at postoperativeintervals for a mean of 18 months. In primary and sec-ondary rhinoplasty, the PDS plate/cartilage graft con-struct was most commonly used to fashion a floating colu-mellar strut. This combination method was alsocommonly used for septal extension grafts and alar bat-ten grafts. Other uses included revision septoplasty andupper lateral cartilage replacement grafts. During 6 to 40months of follow-up, they observed no loss of tip pro-jection. No operative revisions were required, and the PDSplates were well tolerated by all patients with only 2 mi-nor complications, including 1 infection and 1 partial in-tranasal extrusion.
Boenisch and Nolst Trenite14 evaluated the useful-ness of a resorbable PDS plate to support septal cartilagein external septoplasty, assessed its mechanical stabil-ity, and described the surgical technique and clinical ex-perience in 396 patients since 1996. The indication wastypically posttraumatic severe septal deformity. This tech-nique involves removal of the quadrangular cartilage anddivision into straight fragments, which are sutured to theplate and replaced as a free graft (Figure 6). All pa-tients experienced varying degrees of functional improve-ment in nasal blockage. During a mean follow-up of 12months, straightening of the nasal septum was achievedin almost 90% of the patients, correlating with subjec-tive improvements. To confirm this objectively, the au-thors performed postoperative rhinomanometry. The re-sults showed remarkably improved nasal flow in 324patients (81.8%). They reported no immediate postop-erative complications, and only 3 patients were re-ported to have long-term dorsal irregularities.
COMPUTER IMAGING IN RHINOPLASTY
Digital imaging is now routinely used in plastic surgery,where it serves as a component of the medical record andaids in preoperative planning and evaluation of postopera-tive results. Computer imaging in rhinoplasty has the ad-vantages of aiding in communication and setting realisticpatientexpectations.Tworecentstudieshaveevaluatedout-comes related to computer imaging in rhinoplasty.11,16
In an effort to compare patients’ goals in aesthetic rhi-noplasty with aesthetic ideals, Mahajan et al11 have lookedat changes requested by patients through computerimaging during the initial consultation. They then com-pared these computer simulations with set ideals andfound that the mean nasolabial angle fell within the idealrange before and after image manipulation; however, theGoode ratio and the ratio of alar base width to interpu-pillary distance were statistically similar to ideal valuesonly after image manipulation. Overall, they found thatthe patients’ preferences were similar to the ideal in 3 of
A
B
C
Figure 6. Polydioxanone (PDS) plate surgical technique. A, Cartilagefragments are sutured to the PDS plate. B, The finished graft. C, The graft isreimplanted into the nose. Reprinted from Boenisch and Nolst Trenite.14
ARCH FACIAL PLAST SURG/ VOL 14 (NO. 4), JULY/AUG 2012 WWW.ARCHFACIAL.COM246
©2012 American Medical Association. All rights reserved.
Downloaded From: http://archfaci.jamanetwork.com/ by a Emory University User on 11/25/2012

5 variables, and the remaining variables approached theideal. Mahajan et al11 stressed that computer imaging soft-ware holds a wealth of data regarding common patientpreferences.
To determine the accuracy of preoperative computerimaging (PCI) compared with postoperative results, Mehtaet al16 quantitatively evaluated results in 38 patients whounderwent primary and revision rhinoplasty. Six-month postoperative photographs and “morphed” PCIimages were graded on a 5-point Likert scale by 2 pan-els of judges who assessed a total of 12 variables. Thejudges found that the supratip height was the lowest-rated variable, whereas measurements of the upper thirdwere the most accurate. As one might expect, satisfiedpatients had significantly higher PCI accuracy scores, andmost patients found the PCI extremely useful. That studysupports the use and accuracy of PCI but is limited byan average follow-up of approximately 8 months. Morestudies evaluating the long-term outcomes of PCI areclearly warranted.
CONCLUSIONS
Rhinoplasty and the associated aspects of evaluation andtreatment will continue to evolve and challenge sur-geons with their complexity and nuances. For this rea-son, many facial plastic surgeons prefer rhinoplasty toother procedures.27 Nevertheless, as rhinoplasty contin-ues to evolve, surgeons and patients clearly would ben-efit from more evidence-based approaches and out-comes studies to further validate specific techniques.
Accepted for Publication: April 8, 2012.Correspondence: Dean M. Toriumi, MD, Department ofOtolaryngology–Head and Neck Surgery, University ofIllinois at Chicago, 1855 W Taylor St, Third Floor, Chi-cago, IL 60612.Author Contributions: Study concept and design: Ange-los, Been, and Toriumi. Acquisition of data: Angelos andBeen. Analysis and interpretation of data: Angelos and Been.Drafting of the manuscript: Angelos, Been, and Toriumi.Critical revision of the manuscript for important intellec-tual content: Angelos. Administrative, technical, and ma-terial support: Angelos and Been. Study supervision:Toriumi.Financial Disclosure: None reported.Online-Only Material: This article is featured in theArchives Journal Club. Go to http://archfacial.com todownload teaching PowerPoint slides.
REFERENCES
1. Gryskiewicz JM, Gryskiewicz KM. Nasal osteotomies: a clinical comparison ofthe perforating methods versus the continuous technique. Plast Reconstr Surg.2004;113(5):1445-1458.
2. Constantian MB. The boxy nasal tip, the ball tip, and alar cartilage malposition:variations on a theme—a study in 200 consecutive primary and secondary rhi-noplasty patients. Plast Reconstr Surg. 2005;116(1):268-281.
3. Most SP. Anterior septal reconstruction: outcomes after a modified extracorpo-real septoplasty technique. Arch Facial Plast Surg. 2006;8(3):202-207.
4. Toriumi DM. New concepts in nasal tip contouring. Arch Facial Plast Surg. 2006;8(3):156-185.
5. Rhee JS, Arganbright JM, McMullin BT, Hannley M. Evidence supporting func-tional rhinoplasty or nasal valve repair: a 25-year systematic review. Otolaryn-gol Head Neck Surg. 2008;139(1):10-20.
6. James SE, Kelly MH. Cartilage recycling in rhinoplasty: polydioxanone foil as anabsorbable biomechanical scaffold. Plast Reconstr Surg. 2008;122(1):254-260.
7. Peled ZM, Warren AG, Johnston P, Yaremchuk MJ. The use of alloplastic ma-terials in rhinoplasty surgery: a meta-analysis. Plast Reconstr Surg. 2008;121(3):85e-92e.
8. Kridel RW, Ashoori F, Liu ES, Hart CG. Long-term use and follow-up of irradi-ated homologous costal cartilage grafts in the nose. Arch Facial Plast Surg. 2009;11(6):378-394.
9. Boahene KD, Hilger PA. Alar rim grafting in rhinoplasty: indications, technique,and outcomes. Arch Facial Plast Surg. 2009;11(5):285-289.
10. Friedman O, Cook TA. Conchal cartilage butterfly graft in primary functionalrhinoplasty. Laryngoscope. 2009;119(2):255-262.
11. Mahajan AY, Shafiei M, Marcus BC. Analysis of patient-determined preoperativecomputer imaging. Arch Facial Plast Surg. 2009;11(5):290-295.
12. Sepehr A, Alexander AJ, Chauhan N, Chan H, Adamson PA. Cephalic positioningof the lateral crura: implications for nasal tip-plasty. Arch Facial Plast Surg. 2010;12(6):379-384.
13. Zoumalan RA, Shah AR, Constantinides M. Quantitative comparison between mi-croperforating osteotomies and continuous lateral osteotomies in rhinoplasty.Arch Facial Plast Surg. 2010;12(2):92-96.
14. Boenisch M, Nolst Trenite GJ. Reconstruction of the nasal septum using polydi-oxanone plate. Arch Facial Plast Surg. 2010;12(1):4-10.
15. Warner JP, Chauhan N, Adamson PA. Alar soft-tissue techniques in rhinoplasty:algorithmic approach, quantifiable guidelines, and scar outcomes from a singlesurgeon experience. Arch Facial Plast Surg. 2010;12(3):149-158.
16. Mehta U, Mazhar K, Frankel AS. Accuracy of preoperative computer imaging inrhinoplasty. Arch Facial Plast Surg. 2010;12(6):394-398.
17. Lee MR, Unger JG, Rohrich RJ. Management of the nasal dorsum in rhino-plasty: a systematic review of the literature regarding technique, outcomes, andcomplications. Plast Reconstr Surg. 2011;128(5):538e-550e.
18. Yoo S, Most SP. Nasal airway preservation using the autospreader technique:analysis of outcomes using a disease-specific quality-of-life instrument. Arch Fa-cial Plast Surg. 2011;13(4):231-233.
19. Rohrich RJ, Hoxworth RE, Kurkjian TJ. The role of the columellar strut in rhino-plasty: indications and rationale. Plast Reconstr Surg. 2012;129(1):118e-125e.
20. Kim DW, Rodriguez-Bruno K. Functional rhinoplasty. Facial Plast Surg Clin NorthAm. 2009;17(1):115-131, vii.
21. Bermuller C, Kirsche H, Rettinger G, Riechelmann H. Diagnostic accuracy of peaknasal inspiratory flow and rhinomanometry in functional rhinosurgery. Laryngo-scope. 2008;118(4):605-610.
22. Pawar SS, Garcia GJ, Kimbell JS, Rhee JS. Objective measures in aesthetic andfunctional nasal surgery: perspectives on nasal form and function. Facial PlastSurg. 2010;26(4):320-327.
23. Stewart MG, Smith TL, Weaver EM, et al. Outcomes after nasal septoplasty: re-sults from the Nasal Obstruction Septoplasty Effectiveness (NOSE) study. Oto-laryngol Head Neck Surg. 2004;130(3):283-290.
24. Most SP. Analysis of outcomes after functional rhinoplasty using a disease-specific quality-of-life instrument. Arch Facial Plast Surg. 2006;8(5):306-309.
25. Rohrich RJ, Raniere JJ Jr, Ha RY. The alar contour graft: correction and pre-vention of alar rim deformities in rhinoplasty. Plast Reconstr Surg. 2002;109(7):2495-2508.
26. Kridel RW, Castellano RD. A simplified approach to alar base reduction: a reviewof 124 patients over 20 years. Arch Facial Plast Surg. 2005;7(2):81-93.
27. Larrabee WFJ Jr. In praise of rhinoplasty. Arch Facial Plast Surg. 2010;12(6):371-372.
ARCH FACIAL PLAST SURG/ VOL 14 (NO. 4), JULY/AUG 2012 WWW.ARCHFACIAL.COM247
©2012 American Medical Association. All rights reserved.
Downloaded From: http://archfaci.jamanetwork.com/ by a Emory University User on 11/25/2012





























