Embed Size (px)
Citation preview

CT angiography in highly calcified arteries: 2D manual vs. modified automated3D approach to identify coronary stenoses
Marco A. S. Cordeiro1,2, Albert C. Lardo2,3,4,5, Marcelo S. V. Brito1, Miguel A. RosarioNeto1, Maria H. A. Siqueira1, Jose R. Parga1, Luiz F. Avila1, Jose A. F. Ramires1, JoaoA. C. Lima2,3, Carlos E. Rochitte1
1Heart Institute (InCor), University of Sao Paulo Medical School, Sao Paulo, Brazil; 2Division ofCardiology, Department of Medicine, The Johns Hopkins University School of Medicine, Baltimore, MD,USA; 3Department of Radiology, The Johns Hopkins University School of Medicine, Baltimore, MD, USA;4Department of Biomedical Engineering, The Johns Hopkins University School of Medicine, Baltimore, MD,USA; 5Department of Surgery, The Johns Hopkins University School of Medicine, Baltimore, MD, USA
Received 4 August 2005; accepted in revised form 22 September 2005
Key words: computed tomography, coronary angiography, coronary disease, imaging, stenosis
Abstract
Background: Two-dimensional axial and manually-oriented reformatted images are traditionally used toanalyze coronary data provided by multidetector-row computed tomography angiography (MDCTA).While apparently more accurate in evaluating calcified vessels, 2D methods are time-consuming comparedwith automated 3D approaches. The purpose of this study was to evaluate the performance of a modifiedautomated 3D approach (using manual vessel isolation and different window and level settings) in apopulation with high calcium scores who underwent coronary half-millimeter 16-detector-row CT angi-ography (16�0.5-MDCTA). Methods: ECG-gated 16�0.5-MDCTA (16�0.5 mm cross-sections,0.35�0.35�0.35 mm3 isotropic voxels, 400 ms rotation) was performed after injection of iopamidol (120-ml, 300 mg/ml) in 19 consecutive patients (11 male, 62±10 years-old). Native arteries were independentlyevaluated for ‡50%-stenoses using both manual 2D and modified automated 3D approaches. Stents andbypass grafts were excluded. Conventional coronary angiography was visually analyzed by 2 observ-ers. Results: Median Agatston calcium score was 434. Sensitivities, specificities, positive and negativepredictive values for detection of ‡50% coronary stenoses using the 2D and modified 3D approaches were,respectively: 74%/63%, 76%/80%, 45%/34%, and 91%/93% (p=NS for all comparisons). Overall diag-nostic accuracies were 75 and 78%, respectively (p=NS). Uninterpretable vessels were, respectively: 37%(77/209) and 35% (73/209) – p=NS. Time to analyze a single study was 160±23 and 53±11 min,respectively (p<0.01). Conclusions: This modified automated 3D approach is equivalent to and signifi-cantly less time consuming than the traditional manual 2D method for evaluation of ‡50%-stenoses by16�0.5-MDCTA in native coronary arteries of patients with high calcium scores.
Abbreviations: 16�0.5-MDCTA – half-millimeter 16-detector-row CT angiography; 2D – two-dimensional;3D – three-dimensional; CAD – coronary artery disease; CCA – conventional coronary angiography;CPR – curved multiplanar reformation; CT – computed tomography; ECG – electrocardiogram;HU – Hounsfield units; JHH – The Johns Hopkins Hospital; kV – kilovolt; LAD – left anterior descending;
The International Journal of Cardiovascular Imaging (2006) 22: 507–516 � Springer 2006DOI 10.1007/s10554-005-9044-9

LCx – left circumflex; LM – left main; mA – milliampere; MDCTA – multidetector-row computedtomography angiography; MIP – thin-slab maximum intensity projection; mm – millimeter; MPR –multiplanar reformation; ms – millisecond; RCA – right coronary artery; s – second
Introduction
Multidetector-row computed tomography angi-ography (MDCTA) has recently been introducedas a potential noninvasive substitute to conven-tional coronary angiography (CCA) for the in vivoevaluation of vessel lumen in patients with coro-nary artery disease (CAD) [1].Two-dimensional images acquired by MDCTA
have traditionally been the primary focus ofanalysis, with utilization of both axial and man-ually-oriented reformatted images obtained viamultiplanar reformation (MPR), curved multi-planar reformation (CPR), and thin-slab maxi-mum intensity projection (MIP) [2, 3]. Thismanual 2D approach has been demonstrated tobe more time-consuming than standard auto-mated 3D analyses, with the trade-off of lessaccurate assessment of highly calcified arterialsegments [4].The main purpose of this study was to evaluate
the performance of a modified automated 3D ap-proach, as compared to the traditional manual 2Dmethod, in a population with a high likelihood ofelevated coronary calcium scores who underwentCCA for clinical indications and subsequentlyperformed noninvasive coronary angiographywith a half-millimeter 16-detector-row system(16�0.5-MDCTA). Such modified approach con-sists of manual isolation of the coronary arterialtree assisted by adjustment of different windowand level settings prior to appliance of the auto-mated vessel probe on the 3D cardiac volumerenderings deemed as the most appropriate forevaluation of the left and right coronary systems.Secondarily, we also evaluated the diagnosticaccuracy of 16�0.5-MDCTA for assessment ofcoronary artery stenoses ‡50%, in comparisonwith CCA, in this challenging subgroup of patientswith a high pretest probability of CAD and cal-cified vessel walls.
Methods
Study population
Both male and female patients likely to havehigher coronary calcium scores based on their agesranging between 40–79 years and a high pretestprobability of CAD [5, 6] originally referred toCCA for clinically-driven reasons were consideredeligible to participate in this study. Exclusion cri-teria included inability to perform coronary16�0.5-MDCTA within 60 days of the corre-sponding CCA, acute coronary syndromes, dysp-nea precluding a 30-s breath-hold, a constantirregular rhythm, a serum creatinine greater than1.5 mg/dl, any allergy to iodine compounds, morethan one cardiac catheterization during the pre-ceding year, a recent exposure to fluoroscopylonger than 35 min, and a history of intracoronarybrachytherapy.Nineteen consecutive patients were initially
enrolled, with the anticipation, based on our pre-liminary experience studying a similar populationby 16�0.5-MDCTA (pilot study at JHH, 2004),that approximately 200 vessels (including majorcoronary arteries and their first order branches)would ultimately be available for analysis. Amongthese individuals, 11 were male and 8 were female,aged 62±10 years old. The institutional reviewboard of the Heart Institute (InCor), University ofSao Paulo Medical School approved thisstudy and all participants gave a written informedconsent.
MDCTA scan protocol
MDCTA was performed with a half-millimeter16-detector-row scanner (AquilionTM16 – ToshibaMedical Systems Corporation, Otawara, Japan).Heart rate during the exam was 65±14 bpm, and
508

no participants received beta-blockers specificallyfor the performance of the MDCTA exam.Prospectively ECG-triggered 3.0-mm-thick
cross-sections for calcium score measurementswere acquired prior to contrast infusion accordingto the protocol originally validated by electron-beam computed tomography [5]. Subsequently, a120-ml bolus of iopamidol at a concentration of300 mg/ml (IopamironTM 300 – Schering AG,Berlin, Germany) followed by a saline chaser(30 ml) was injected intravenously at a rate of5 ml/s (during the first two thirds), and then at3 ml/s for the remaining of the infusion. For bolustracking, successive axial slices were acquired overthe ascending aorta immediately after the begin-ning of radiocontrast infusion. A region of interest(Sure StartTM, Toshiba Medical Systems Corpo-ration, Otawara, Japan) was positioned in theaortic root cranially to the emergence of the leftcoronary artery. As the signal in the ascendingaorta reached a predefined threshold of 150Hounsfield units (HU) detected by bolus-trackingand graphically represented by a curve of aver-aged HU enhancement plotted against time dis-played on the scanner’s console, the patient wasinstructed to sustain an inspiratory breath-hold of29 s on average. Helical scanning was alwaystriggered manually.We used a scanning protocol with a gantry
rotation time of 400 ms and slice collimation of16�0.5 mm which were applied at a pitch of 3.2,using a tube voltage of 135 kV and a current of350 mAs. A scanning field of view of 320 mm wascombined with a detector collimation of 16�0.5 mm, a slice reconstruction overlap of 40% (ateach 0.3 mm), and a 512�512 pixel matrix, ulti-mately generating truly isotropic voxels of0.35�0.35�0.35 mm3. No current modulation wasused. Scanning direction was always craniocaudal.After acquisition of the helical CT raw data,
retrospective ECG synchronized slices werereconstructed by a multisegment reconstructionalgorithm [7]. Erosion and dilation filtering algo-rithms were not implemented. Because data wereacquired continuously, the reconstruction windowcould be positioned at any point within the cardiaccycle. In this particular study, it was done at 10time points, with the center of the reconstruction
window between 0 and 90% of the cardiac cycle, at10% intervals. At the observers’ discretion, addi-tional window positions were also obtained.
MDCTA image interpretation
Two experienced observers (M.A.S.C. andM.S.V.B.) independently reviewed in a blindedfashion all coronary 16�0.5-MDCTA images.M.A.S.C. utilized the so-called modified auto-
mated 3D approach, a method recently developedin the cardiovascular CT imaging laboratory ofThe Johns Hopkins Hospital (Baltimore, MD).This stepwise method makes use of the observer’svisually-guided application of an automated vesseltracking algorithm (VitreaTM2, version 3.5 – VitalImages Inc, Plymouth, MN) on the 3D cardiacvolume rendered images subjectively chosen as themost appropriate for evaluation of the left andright coronary systems, and is described in detailas follows (Figure 1):
• Step 1: Adjustment of different window andlevel settings on the 3D cardiac volume render-ings generated from each of the 10 originallyreconstructed phases;
• Step 2: Visual selection of the best cardiac phase(more arterial contrast enhancement and lessartifacts) to analyze the left and right coronarysystems (not necessarily the same phase forboth);
• Step 3: Manual isolation, with exclusion ofother cardiac structures also assisted by frequentadjustment of different window and level set-tings, of the entire left (left main – LM, leftanterior descending – LAD, left circumflex –LCx, with their corresponding side branches)and right (right coronary artery – RCA and itsside branches) coronary systems;
• Step 4: Visually-guided application of the auto-mated vessel probe on every artery, beginningwith the more distal segments of the sidebranches. This semi-automated centerline detec-tion of the coronary vessel lumen on slabs of 3Dcardiac volume renderings ultimately generatestwo orthogonal 2D CPR images as well as aseries of cross-sectional views derived fromthem;
509
• Step 5: Careful evaluation by visual assessmentof every orthogonal 2D CPR and cross-sec-tional image automatically reformatted by thesoftware, with final diagnosis of significantcoronary stenoses always based on these 2Dimages.
M.S.V.B. used the traditional manual 2Dapproach described elsewhere [1–3]. Differentwindow and level settings were also used on thestandard 2D axial and manually-oriented refor-matted images obtained via MPR, CPR, and MIP.The 4 main coronary arteries – LM, LAD, LCx,
and RCA, including their first order branches(excluding septal and right marginal branches)
were visually screened for the presence of ‡50%luminal stenoses. Bypass grafts were excludedfrom the analysis. Stented lumens were alsoexcluded, but not the segments proximal and distalto them. Total and regional (each major nativeartery territory) Agatston calcium scores [5] werealso obtained. Bypass grafts, stents, and metalclips were carefully avoided during coronarycalcium measurements.
Conventional coronary angiography
Coronary angiograms were performed accordingto standard techniques [8]. A joint panel of twoexperienced observers blindly reviewed all CCAs.
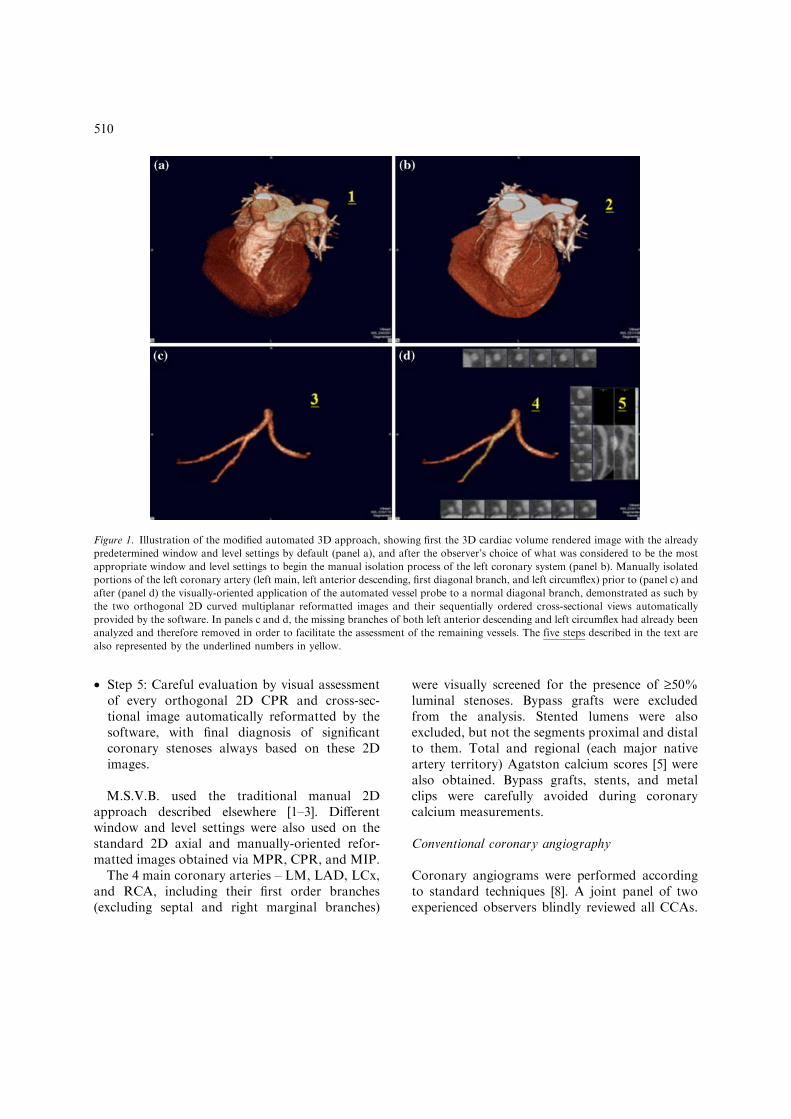
Figure 1. Illustration of the modified automated 3D approach, showing first the 3D cardiac volume rendered image with the already
predetermined window and level settings by default (panel a), and after the observer’s choice of what was considered to be the most
appropriate window and level settings to begin the manual isolation process of the left coronary system (panel b). Manually isolated
portions of the left coronary artery (left main, left anterior descending, first diagonal branch, and left circumflex) prior to (panel c) and
after (panel d) the visually-oriented application of the automated vessel probe to a normal diagonal branch, demonstrated as such by
the two orthogonal 2D curved multiplanar reformatted images and their sequentially ordered cross-sectional views automatically
provided by the software. In panels c and d, the missing branches of both left anterior descending and left circumflex had already been
analyzed and therefore removed in order to facilitate the assessment of the remaining vessels. The five steps described in the text are
also represented by the underlined numbers in yellow.
510

Significant stenoses were visually graded as caus-ing ‡50% luminal narrowing. If the same majorartery or first order branch was found to havemore than one significant stenosis, only the mostproximal was compared to the correspondingcoronary 16�0.5-MDCTA lesion [2, 7].
Statistical analysis
As previously mentioned, an estimated sample sizeof approximately 200 interpretable vessels wasbased on our preliminary experience studying asimilar population by 16�0.5-MDCTA (pilotstudy at JHH, 2004). Since 19 patients representeda small number for a per-patient analysis and aper-segment analysis could decrease diseaseprevalence and potentially generate an artificialincrease in specificities and negative predictivevalues, we opted to perform solely a per-vesselevaluation in these individuals.Standard descriptive statistics were expressed as
mean±SD. Because of an asymmetric distribu-tion, coronary calcification levels were expressedas medians and ranges. Fisher’s exact test was usedto calculate the diagnostic accuracy of coronary16�0.5-MDCTA via both the manual 2D and themodified automated 3D approaches for detectionof stenoses ‡50% in the native coronary arteries ascompared to CCA. A p value <0.05 was consid-ered as of statistical significance, and 95% confi-
dence intervals were calculated for each diagnosticmeasurement.
Results
All CCAs and 16�0.5-MDCTAs were performedwithout complications and data from the 19patients were included in the final comparativeanalysis. Average interval between each CCAand its corresponding coronary 16�0.5-MDCTAwas 16±10 days. Total Agatston calcium scoreranged from 0 to 3459 (median 434). Regionalcalcium scores for LM-LAD combined, LCx,and RCA territories are described in Tables 1and 2.
Diagnostic accuracy measurements
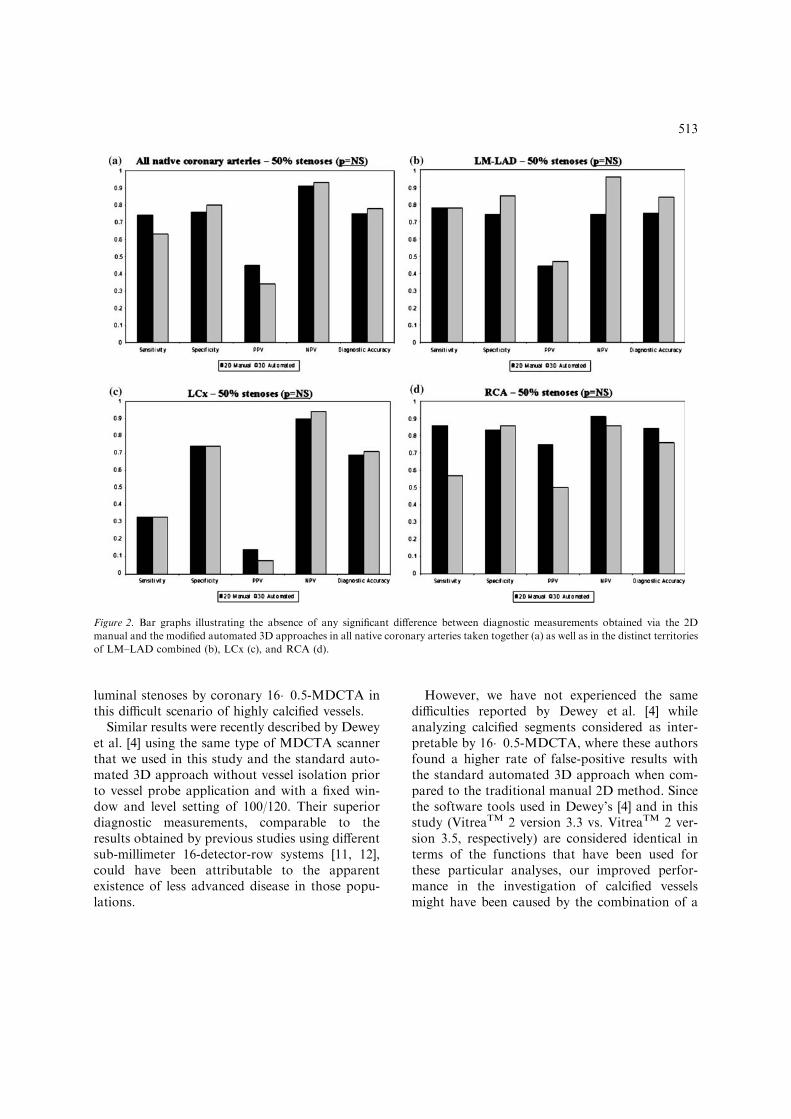
Sensitivities, specificities, positive and negativepredictive values, in addition to diagnostic accura-cies of bothmanual 2D andmodified automated 3Dapproaches for detection of ‡50% coronary ste-noses by 16�0.5-MDCTA in all native vesselscombined as well as in LM-LAD, LCx, and RCAterritories independently are detailed in Tables 1and 2, respectively. As can be seen in Figure 2, nosignificant difference was noted between the twoapproaches in relation to the diagnostic measure-ments evaluated for all 4 major coronary territories.
Table 1. Diagnostic accuracy of 16�0.5-MDCTAa compared to CCA for detection of ‡50% coronary stenoses using the manual 2D
approach.
All native arteries LM/LADb LCx RCA
‡50%c 19 9 3 7
Calcium score (Agatston) 434 (0, 3459)d 260 (0, 1110) 13(0, 802) 71 (0, 1547)
Sensitivity (%) 74 (51–88)e 78 (44–93) 33 (7–81) 86 (47–97)
Specificity(%) 76 (65–84) 74 (58–86) 74 (53–87) 83 (55–95)
Positive predictive valuef (%) 45 (29–62) 44 (23–67) 14 (3–53) 75 (40–93)
Negative predictive valuef (%) 91 (81–96) 74 (58–86) 90 (68–97) 91 (62–98)
Diagnostic accuracy (%) 75 (65–83) 75 (61–85) 69 (50–84) 84 (62–94)
CCA: conventional coronary angiography; 2D: two-dimensional.
LM, LAD, LCx, and RCA indicate left main, left anterior descending, left circumflex, and right coronary artery, respectively.a16�0.5-MDCTA: half-millimeter 16-detector-row spiral computed tomography angiography.bLM/LAD: the two territories combined.cNumber of ‡50% coronary stenoses visually detected by CCA.dMedian, (range).e95% confidence interval.fPrevalence of ‡50% coronary stenoses = 14%, 15%, 7%, and 24%, respectively.
511

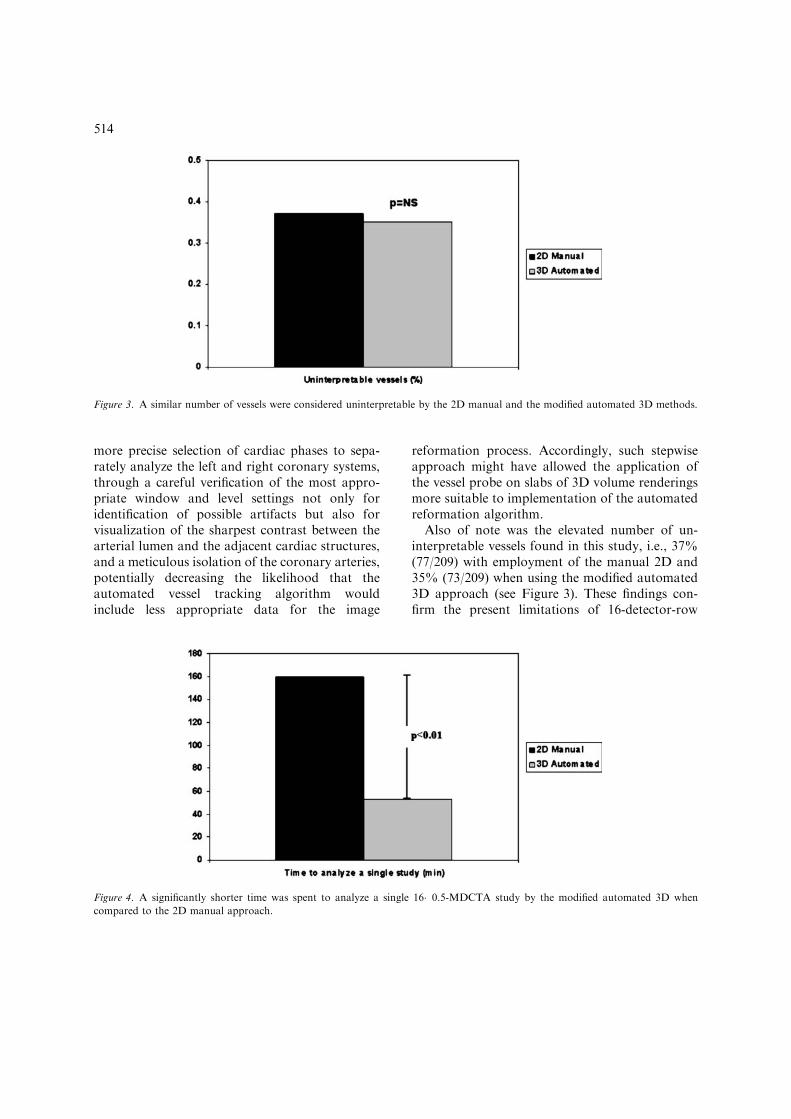
Interpretability
Of 209 major coronary arteries and first orderbranches initially evaluated, 37% (77/209) and35% (73/209) were considered uninterpretable bythe manual 2D and the modified automated 3Dapproaches, respectively (p=NS), as illustrated inFigure 3. In both cases, uninterpretability wasmainly attributed to calcium-unrelated artifactsrepresented by motion, noise, and low contrastenhancement isolated or most commonly in com-bination (58/77 or 75% in the 2D, and 53/73 or73% in the 3D approach – p=NS), followed bycalcium-related artifacts represented by excessiveblooming secondary to severe vessel calcification(17/77 or 22%, and 17/73 or 23%, respectively– p=NS).
Time to analyze a single coronary 16�0.5-MDCTAstudy
The average time spent to complete the analysis ofthe coronary lumen of a single case acquired by16�0.5-MDCTA was significantly longer using themanual 2D (160±23 min) compared to the mod-ified automated 3D approach (53±11 min,p<0.01), as shown in Figure 4.
Discussion
This is one of the first studies specifically designedto address patients with a high likelihood of ele-vated coronary calcium scores by 16-detector-rowMDCTA. In fact, among the 19 patients selectedto take part in this study, 13 (13/19 or 68%) had atotal Agatston calcium score ‡400, representing apopulation with high calcium scores [6] and atgreatest risk for absolute progression of coronarycalcification [9]. Even in such a challenging sub-group of patients for coronary MDCTA [7, 10,11], we were able to show that the modifiedautomated 3D approach is equivalent to the tra-ditional manual 2D method for detection of ‡50%luminal stenoses in the human native coronaryarterial tree, as can be demonstrated by the over-lap between all comparable 95% confidenceintervals shown in Tables 1 and 2 (correspondingto a p=NS for all possible comparisons), and alsothat it is significantly less time-consuming(p<0.01) (see Figure 4). We were able to show aswell relatively good specificities (76% with themanual 2D, and 80% with the modified automated3D method) and negative predictive values (91%with the manual 2D, and 93% with the modifiedautomated 3D approach) for detection of ‡50%
Table 2. Diagnostic accuracy of 16�0.5-MDCTAa compared to CCA for detection of ‡50% coronary stenoses using the modified
automated 3D approach.
All native arteries LM/LADb LCx RCA
‡50%c 19 9 3 7
Calcium score (Agatston) 434 (0, 3459)d 260 (0, 1110) 13(0, 802) 71 (0, 1547)
Sensitivity (%) 63 (41–81)e 78 (44–93) 33 (7–81) 57 (25–84)
Specificity (%) 80 (72–87) 85 (73–92) 74 (59–85) 86 (65–95)
Positive predictive valuef (%) 34 (21–51) 47 (25–70) 8 (2–36) 50 (21–79)
Negative predictive valuef (%) 93 (86–97) 96 (86–99) 94 (80–98) 86 (65–95)
Diagnosticaccuracy (%) 78 (70–84) 84 (73–91) 71 (57–82) 76 (58–88)
CCA: conventional coronary angiography; 3D: three-dimensional.
LM, LAD, LCx, and RCA indicate left main, left anterior descending, left circumflex, and right coronary artery, respectively.a16�0.5-MDCTA: half-millimeter 16-detector-row spiral computed tomography angiography.bLM/LAD: the two territories combined.cNumber of ‡50% coronary stenoses visually detected by CCA.dMedian, (range).e95% confidence interval.fPrevalence of ‡50% coronary stenoses = 14%, 15%, 7%, and 24%, respectively.
512
luminal stenoses by coronary 16�0.5-MDCTA inthis difficult scenario of highly calcified vessels.Similar results were recently described by Dewey
et al. [4] using the same type of MDCTA scannerthat we used in this study and the standard auto-mated 3D approach without vessel isolation priorto vessel probe application and with a fixed win-dow and level setting of 100/120. Their superiordiagnostic measurements, comparable to theresults obtained by previous studies using differentsub-millimeter 16-detector-row systems [11, 12],could have been attributable to the apparentexistence of less advanced disease in those popu-lations.
However, we have not experienced the samedifficulties reported by Dewey et al. [4] whileanalyzing calcified segments considered as inter-pretable by 16�0.5-MDCTA, where these authorsfound a higher rate of false-positive results withthe standard automated 3D approach when com-pared to the traditional manual 2D method. Sincethe software tools used in Dewey’s [4] and in thisstudy (VitreaTM 2 version 3.3 vs. VitreaTM 2 ver-sion 3.5, respectively) are considered identical interms of the functions that have been used forthese particular analyses, our improved perfor-mance in the investigation of calcified vesselsmight have been caused by the combination of a
Figure 2. Bar graphs illustrating the absence of any significant difference between diagnostic measurements obtained via the 2D
manual and the modified automated 3D approaches in all native coronary arteries taken together (a) as well as in the distinct territories
of LM–LAD combined (b), LCx (c), and RCA (d).
513
more precise selection of cardiac phases to sepa-rately analyze the left and right coronary systems,through a careful verification of the most appro-priate window and level settings not only foridentification of possible artifacts but also forvisualization of the sharpest contrast between thearterial lumen and the adjacent cardiac structures,and a meticulous isolation of the coronary arteries,potentially decreasing the likelihood that theautomated vessel tracking algorithm wouldinclude less appropriate data for the image
reformation process. Accordingly, such stepwiseapproach might have allowed the application ofthe vessel probe on slabs of 3D volume renderingsmore suitable to implementation of the automatedreformation algorithm.Also of note was the elevated number of un-
interpretable vessels found in this study, i.e., 37%(77/209) with employment of the manual 2D and35% (73/209) when using the modified automated3D approach (see Figure 3). These findings con-firm the present limitations of 16-detector-row
Figure 4. A significantly shorter time was spent to analyze a single 16�0.5-MDCTA study by the modified automated 3D when
compared to the 2D manual approach.
Figure 3. A similar number of vessels were considered uninterpretable by the 2D manual and the modified automated 3D methods.
514

MDCTA for evaluation of highly calcified vessels[7, 11, 13]. However, the number of uninterpret-able vessels found in this particular group ofpatients was higher than initially expected. Aspreviously mentioned, based on our preliminaryexperience with a similar group of patients stud-ied by 16�0.5-MDCTA (pilot study at JHH,2004), we had anticipated that around 200 vesselswould be considered interpretable in this popu-lation. The differences observed (132 and 136interpretable vessels by using the traditionalmanual 2D and the modified automated 3Dmethod, respectively) could have been caused bydifferent iodine concentrations in the radiocon-trasts utilized (320 mg/ml in the pilot study vs.300 mg/ml in the present study) as well as bydiverse radiation doses implemented (higher inthe former). Moreover, the ethnicities were alsodifferent (North Americans in the first vs. SouthAmericans in the second).In conclusion, this study demonstrates that the
modified automated 3D approach (using manualvessel isolation assisted by diverse window andlevel settings prior to visually-guided vessel probeapplication) is equivalent to the traditional manual2D method (using different window and level set-tings to analyze the axial and manually-orientedMPR, MIP, and CPR images) for detection of‡50% luminal stenoses in the native coronaryarterial tree of patients with high calcium scores bythe currently most available generation ofMDCTA systems worldwide, i.e., 16-detector-rowscanners, and is also significantly less time-con-suming. These results suggest as well the suitabilityof this particular type of approach for the evalu-ation of coronary lumens in patients with lesscalcified vessel walls, highlighting even further itsclinical feasibility. In addition, 16�0.5-MDCTAexcludes ‡50% stenoses with relatively high accu-racy in patients with elevated coronary calciumscores.
Acknowledgements
Grant support: this work was funded by theNational Institutes on Aging (Bethesda, MD)
RO1- AG021570-01 grant, by the Johns HopkinsReynolds Cardiovascular Center (D. W. ReynoldsFoundation, Las Vegas, NV), by the ZerbiniFoundation (Fundacao E. J. Zerbini, Sao Paulo,SP, Brazil), and partly supported by ToshibaMedical Systems Corporation (Otawara, Japan).Dr Cordeiro is funded by the Brazilian NationalResearch Council (CNPq, Brasılia, DF, Brazil) asa postdoctoral fellow (fellowship grant 202706/02-8) in the Division of Cardiology of The JohnsHopkins University School of Medicine (Balti-more, MD).
References
1. Nieman K, Oudkerk M, Rensing BJ, van Ooijen P, Munne
A, van Geuns RJ, et al. Coronary angiography with multi-
slice computed tomography. Lancet 2001; 357(9256): 599–
603.
2. Nieman K, Cademartiri F, Lemos PA, Raaijmakers R,
Pattynama PM, de Feyter PJ. Reliable noninvasive coro-
nary angiography with fast submillimeter multislice spiral
computed tomography. Circulation 2002; 106(16): 2051–
2054.
3. Ropers D, Baum U, Pohle K, Anders K, Ulzheimer S,
Ohnesorge B, et al. Detection of coronary artery stenoses
with thin-slice multi-detector row spiral computed tomog-
raphy and multiplanar reconstruction. Circulation 2003;
107(5): 664–666.
4. Dewey M, Schnapauff D, Laule M, Lembcke A, Borges
AC, Rutsch W, et al. Multislice CT coronary angiography:
evaluation of an automatic vessel detection tool. Rofo
2004; 176(4): 478–483.
5. Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR,
Viamonte M Jr., Detrano R. Quantification of coronary
artery calcium using ultrafast computed tomography. J Am
Coll Cardiol 1990; 15(4): 827–832.
6. Rumberger JA, Brundage BH, Rader DJ, Kondos G.
Electron beam computed tomographic coronary calcium
scanning: a review and guidelines for use in asymptomatic
persons. Mayo Clin Proc 1999; 74(3): 243–252.
7. Dewey M, Laule M, Krug L, Schnapauff D, Rogalla P,
Rutsch W, et al. Multisegment and halfscan reconstruc-
tion of 16-slice computed tomography for detection of
coronary artery stenoses. Invest Radiol 2004; 39(4): 223–
229.
8. Bashore TM, Bates ER, Berger PB, Clark DA, Cusma JT,
Dehmer GJ, et al. American College of Cardiology/Society
for Cardiac Angiography and Interventions Clinical Expert
Consensus Document on cardiac catheterization laboratory
standards. A report of the American College of Cardiology
Task Force on Clinical Expert Consensus Documents. J
Am Coll Cardiol 2001; 37(8): 2170–2214.
515

9. Schmermund A, Baumgart D, Mohlenkamp S, Kriener P,
Pump H, Gronemeyer D, et al. Natural history and
topographic pattern of progression of coronary calcifica-
tion in symptomatic patients: An electron-beam CT study.
Arterioscler Thromb Vasc Biol 2001; 21(3): 421–426.
10. Kuettner A, Kopp AF, Schroeder S, Rieger T, Brunn J,
Meisner C, et al. Diagnostic accuracy of multidetector
computed tomography coronary angiography in patients
with angiographically proven coronary artery disease. J Am
Coll Cardiol 2004; 43(5): 831–839.
11. Hoffmann U, Moselewski F, Cury RC, Ferencik M, Jang
IK, Diaz LJ, et al. Predictive value of 16-slice multidetector
spiral computed tomography to detect significant obstruc-
tive coronary artery disease in patients at high risk for
coronary artery disease: patient-versus segment-based
analysis. Circulation 2004; 110(17): 2638–2643.
12. Kuettner A, Beck T, Drosch T, Kettering K, Heuschmid
M, Burgstahler C, et al. Diagnostic accuracy of noninvasive
coronary imaging using 16-detector slice spiral computed
tomography with 188 ms temporal resolution. J Am Coll
Cardiol 2005; 45(1): 123–127.
13. Kaiser C, Bremerich J, Haller S, Brunner-La Rocca HP,
Bongartz G, Pfisterer M. et al. Limited diagnostic yield of
non-invasive coronary angiography by 16-slice multidetec-
tor spiral computed tomography in routine patients
referred for evaluation of coronary artery disease. Eur
Heart J 2005.
Address for correspondence: Carlos E. Rochitte, Heart Institute
(InCor), University of Sao Paulo Medical School, Instituto
do Coracao do Hospital das Clınicas da Faculdade de Medicina
da Universidade de Sao Paulo (InCor-HCFMUSP), Setor de
Ressonancia Magnetica e Tomografia Computadorizada Car-
diovascular, Av. Dr. Eneas de Carvalho Aguiar, 44, Sao Paulo,
SP, Brasil, CEP 05403-000
Tel.: +55-11-3069-5586; Fax: +55-11-3069-5587
E-mail: [email protected]
516




























