Embed Size (px)
Citation preview
BRIEF COMMUNICATION
Improved protocol for processing stented porcine coronaryarteries for immunostaining
Arun H. S. Kumar • Scott D. McCauley •
Brian G. Hynes • John O’Dea • Noel M. Caplice
Received: 15 December 2010 / Accepted: 20 January 2011 / Published online: 9 February 2011
� Springer Science+Business Media B.V. 2011
Abstract Percutaneous coronary intervention has resul-
ted in a paradigm shift in the treatment of coronary artery
disease and myocardial infarction. However, neither bare-
metal stents nor polymer-coated drug-eluting stents repre-
sent ideal therapies at this time due to the undesired
in-stent stenosis or delayed thrombosis. Hence there is
pressing clinical need for greater understanding of the
cellular mechanisms involved. It is hoped that this in turn
will provide insight into designing and developing the next
generation of stents. Although immunohistochemistry and
immunofluorescence are appropriate tools in understanding
the molecular histology, performing these techniques on
stented blood vessels is technically challenging because of
poor permeability of antibodies into the stented blood
vessels which are embedded in methacrylate-based resins
and inadequate image resolution due to autofluorescence.
Hence there is a need to develop techniques which can
facilitate immunohistochemistry/immunofluorescence pro-
cedures on stented blood vessel cross-sections. In this study
we describe an improved protocol for processing stented
porcine coronary arteries for immunostaining with smooth
muscle cell, endothelial cell, monocyte and macrophage
markers. We first identified the optimal conditions for resin
embedding of stented artery and cross sectioned the vessels
using high speed precision wafering diamond blade. The
sections were then ground using two levels of water
sandpaper on a Metaserve 2000 grinder to achieve the
desired thickness. For immunostaining, we developed a
novel deplasticization protocol which favors optimal anti-
body permeabilization. Our protocol not only provides
feasibility of improved immunostaining of stented artery
sections but also results in high quality images.
Keywords Stent � Immunofluorescence � Porcine
coronary artery � In-stent restenosis
Introduction
Percutaneous coronary intervention treatment of myocar-
dial ischemia and acute coronary syndromes is extensively
used in the interventional cardiology clinical practice.
Although, stenting of arterial lesions has improved the
outcomes when compared to traditional balloon angio-
plasty (Hudson et al. 2010) in-stent restenosis (ISR)
remains a significant problem, particularly with bare metal
stents (BMS) (Mitra and Agrawal 2006). This has led to the
development of drug-eluting stents (DES) as an alternative;
however, the increased rate of late-stent thrombosis (LST)
with the use of DES is also a concern (Stahli et al. 2009).
Hence it has become necessary to understand the molecular
mechanisms responsible for these limitations so as to
develop better approaches for cardiac interventions in
future.
Stenting of porcine coronary arteries provides important
preclinical model not only to evaluate novel stents for
efficacy and safety but also facilitates understanding of the
mechanisms involved in ISR and LST. Unfortunately, the
precise cellular mechanisms underlying both ISR and LST
are still incompletely understood. This has been in part due
to technical limitations in histological evaluation of stented
Electronic supplementary material The online version of thisarticle (doi:10.1007/s10735-011-9316-8) contains supplementarymaterial, which is available to authorized users.
A. H. S. Kumar � S. D. McCauley � B. G. Hynes � J. O’Dea �N. M. Caplice (&)
Centre for Research in Vascular Biology (CRVB), Biosciences
Institute, University College Cork, College Road, Cork, Ireland
e-mail: [email protected]
123
J Mol Hist (2011) 42:187–193
DOI 10.1007/s10735-011-9316-8

artery sections (Rippstein et al. 2006). To accurately
characterize the profile of the cells contributing to the neo-
intima formation leading to ISR, use of specific antibodies
to smooth muscle cell, endothelium, macrophages, mono-
cytes and other cell specific markers is required (Jonas
et al. 2005). However, a prerequisite for a good staining
process is a good tissue section of the stented artery. This
challenge has been over come in the recent years by the
development of methyacrylate resins which provides con-
siderable advantage over traditional paraffin or OCT
embedding techniques when sectioning stented arteries
using saw and grinding (SG) techniques (Brasen et al.
2001; Rippstein et al. 2006). Although this improved
methodology has considerably advanced the quality of
stented artery sections which are suitable for classical
histological staining, the possibility of high quality
immunostaining (immunofluorescence) remains a chal-
lenge. While several investigators have described immu-
nostaining, the images acquired had poor resolution and
were associated with a high degree of autofluorescence
(Malik et al. 1998; Brasen et al. 2001; Jonas et al. 2005;
Rippstein et al. 2006). Achieving good immunostaining of
stented arterial sections will facilitate understanding the
molecular histology and cellular dynamics of ISR. A major
barrier to achieving good immunostaining is the use of high
dense methyacrylate resin which is difficult to completely
deplasticize. Consequently the permeabilization of the
antibody becomes problematic and limits the quality of
immunostaining. To address this limitation we optimized
an ideal combination of commercially available methac-
rylate-based resin and developed an improved deplastici-
zation protocol, which provides significantly improved
quality of immunostaining. In this study we outline a
detailed protocol for the successful processing of stented
porcine coronary arteries to obtain improved immunoflu-
orescence labeling.
Materials and methods
Protocol for stenting porcine coronary artery
Female Landrace pigs (25–30 kg; n = 4) were anaesthe-
tized using single intramuscular injection of a combination
of Xylazine (2 mg/kg), and Ketamine (15 mg/kg). The
anaesthesia was maintained using Isoflurane (1.5–2% iso-
flurane delivered via oxygen as a carrier gas). A 5 cm
incision was made 2 cm lateral and parallel to the trachea
and by blunt dissection the carotid artery was exposed and
secured. An arterial cut down was performed in order to
provide access for interventional sheath placement to
facilitate the insertion of balloon catheter and stent
placement. A Philips fluoroscopy C-arm was used to
visualize the location and guide balloon and stent to its
appropriate position in the left anterior descending coro-
nary artery. The bare metal stent (2.5 9 15 mm) was
deployed in the appropriate position with the stent to artery
ratio of 1.1:1. After the stent placement check angiography
confirmed TIMI-3 flow in the stented artery, following
which the guide and stent delivery equipment were with-
drawn under fluoroscopy. The arteriotomy site was then
closed using 8/0 sutures and the surgical wound was closed
using the 4/0 sutures and smeared with betadine. Eight
weeks post procedure the pigs were euthanized by overdose
of pentobarbital and the coronary artery with stent was
dissected out and fixed in chilled 4% paraformaldehyde for
24 h at 4�C.
Embedding of stented coronary artery in resin
Paraformaldehyde fixed stented coronary artery was
washed for 4 h in chilled PBS containing 6.8% sucrose at
4�C and then dehydrated in 100% acetone for 60 min at
4�C. The stented artery was transferred to a 5 ml poly-
styrene tube consisting of infiltration solution (100 ml base
liquid Technovit 8100 mixed with 0.4 g hardener I;
Heraeus Kulzer GmbH, Wehrheim/Ts, Germany) for
overnight at 4�C and then the stent was embedded in the
resin by mixing 0.15 ml of hardener II (Heraeus Kulzer
GmbH, Wehrheim/Ts, Germany) with 5 ml of infiltration
solution. The polystyrene tube with the stent and resin was
sealed with an air tight cap and left at 4�C overnight for
hardening.
Sectioning grinding of the resin embedded stent
After embedding the stented arteries in the resin, a Buehler
IsoMet 5000 high-speed precision saw (Buehler; Dussel-
dorf, Germany) was used to cut cross sections of the
stented artery. The resin block was removed from the
polystyrene tube by cutting it with a hand saw. The resin
block was cleaned and dried using a filter paper and then
mounted perpendicular on to glass slides using super glue
(Bostik, UK). A tiny drop was used, and the block was held
in place by hand under consistent pressure for a minimum
of 30 s to ensure even contact with the slide, and to avoid
the formation of bubbles underneath. The block was then
secured on to a holder in the saw, and the blade was
adjusted to a cutting width of 1 mm. A wayfaring diamond
blade (12.7 9 0.4 mm; Buehler; Dusseldorf, Germany)
was used at a cutting speed of 1,200 rpm with a blade-feed
rate of 10.1 mm/min. During the sectioning, water was
continually jetted on to the cutting surface as a coolant to
minimize friction heat. This resulted in a 100 lm thick
section on the glass slide. The protocol was repeated to cut
the entire length of the stent.
188 J Mol Hist (2011) 42:187–193
123

The 100 lm thick cross section of the stented artery was
ground using two levels of water sandpaper on a Metaserve
2000 grinder (Buehler, Germany). The sections were ini-
tially ground using P800 grit to achieve the desired thick-
ness, 7–10 lm, which took approximately 20 s at a speed of
60 rpm, placing the sample on the sandpaper intermittently
at 1 s intervals. The slides were then smoothed and polished
using P2500 grit paper at 200 rpm for 10 s, at 1 s intervals.
Deplasticization of the stented cross section
Prior to both histological and immunofluorescence stain-
ing, slides were deplasticized to remove excess embedding
resin. Deplasticization was achieved by placing the slides
in Xylene for 20 min twice, 2-methoxyacetate (2-MEA) for
10 min twice, 70% ethanol for 10 min, distilled water
for 10 min, and finally phosphate buffered saline (PBS) for
10 min. It was vital to continually check on the slides
throughout the steps, especially during the 2-MEA
immersion, to ensure the sample did not lift off the slide. If
the sample appeared to be coming off, it was removed from
the solvent and placed in 70% ethanol, continuing with the
steps as described above. All steps were carried out at room
temperature. Once the slides were in PBS, they were either
stained directly for morphometric analysis using histolog-
ical stains or further prepared for immunofluorescence by
an antigen-retrieval protocol.
Immunofluorescence labeling
Prior to immunofluorescence staining, superior results were
achieved by performing antigen retrieval and permeabi-
lizing the tissues to maximize antibody binding. This was
achieved by placing the samples in 4% paraformaldehyde
(PFA) for 10 min at 4�C. Slides were then washed twice in
PBS for 5 min, then placed in a Coplin jar containing
1 mM EDTA (pH 8), and submerged in a boiling water
bath for 15 min. This was followed by 10 min in chilled
methanol at -20�C.
Deplasticized and permeabilized tissue section bound-
aries were marked with a wax pen. They were then incu-
bated in blocking buffer (10% normal goat serum in 0.2%
Triton-X 100 PBS) for 20 min at room temperature with
shaking. This was followed by incubation with primary
antibodies diluted in blocking buffer overnight at 4�C.
Primary antibodies used were: rabbit anti-SMA (Abcam,
1:100), rabbit anti-Calponin (Abcam, 1:100), rabbit anti-
eNOS (Abcam, 1:50), rabbit anti-CX3CR1 (Prosci, 1:50),
and rat anti-F4/80 (Prosci, 1:50), along with appropriate
IgG controls at 1:50 dilution. Sections were then washed in
PBS for 5 min three times, and exposed to fluorescent-
labeled secondary antibodies (goat anti-rabbit/rat 546/488)
diluted in blocking buffer to 1:250/500 for 40 min at room
temperature in humidified chambers with shaking. After
three 5 min PBS washes, slides were incubated with DAPI
at 1:1,000 in distilled water for 10 min, washed in PBS in a
Coplin jar for 5 min, then dried, and covered with anti-
fade, coverslip and sealed with nail polish. The immuno-
stained sections were imaged using Nikon confocal
microscope (Nikon eC1 plus, TE2000E).
Hematoxylin and Eosin (H&E) staining
For H&E staining, deplasticized slides were placed on a
surface shaker in Mayer’s hematoxylin contained in a
Coplin jar for 10 min, followed by rinsing in running tap
water for 15 min. They were then placed in Eosin stain for
10 s, then washed in 70% ethanol for 5 s and cleared in
Xylene for 5 min. Slides were then allowed to air dry
before mounting of a coverslip with DPX prior to imaging
using Nikon upright microscope (Nikon Eclipse 80i).
Results
Optimization of the resin embedding of stented artery
One of the major limitations in the processing of stented
artery for immunofluorescence staining is the hardness of
the resin. The quality of immunostaining is inversely pro-
portional to the hardness of the resin. However, the hard-
ness can only be compromised to an extent which allows
for its cutting without distorting the embedded stented
artery. Hence we opted for a moderate resin strength which
would provide us just enough hardness to hold the stented
artery intact during the process of cutting. This was
achieved by using a milder infiltration solution (i.e., 100 ml
base liquid Technovit 8100 mixed with 0.4 g hardener I in
comparison to the suggested 0.6 g hardener I by Heraeus
Kulzer GmbH, Wehrheim/Ts, Germany) followed by a
milder resin hardener (i.e., 0.15 ml instead of 0.17 ml of
hardener II mixed with 5 ml of infiltration solution). This
protocol allowed us to consistently achieve adequate
hardness for comfortable sectioning of 100 lm thick resin
embedded stented artery without distorting its structure
(Supplement Fig. 1A). Our approach allowed us to look
into the finer microvascular structures within the plaque
(Supplement Fig. 1A) and as well as mononuclear cell
aggregates and smooth muscle coverage near the stent stud
(Supplement Fig. 1B).
Immunofluorescence labeling of stented artery
cross-sections
The sections ground to 7–10 lm thickness and deplasti-
cized were used for immunostaining. The main cell types
J Mol Hist (2011) 42:187–193 189
123
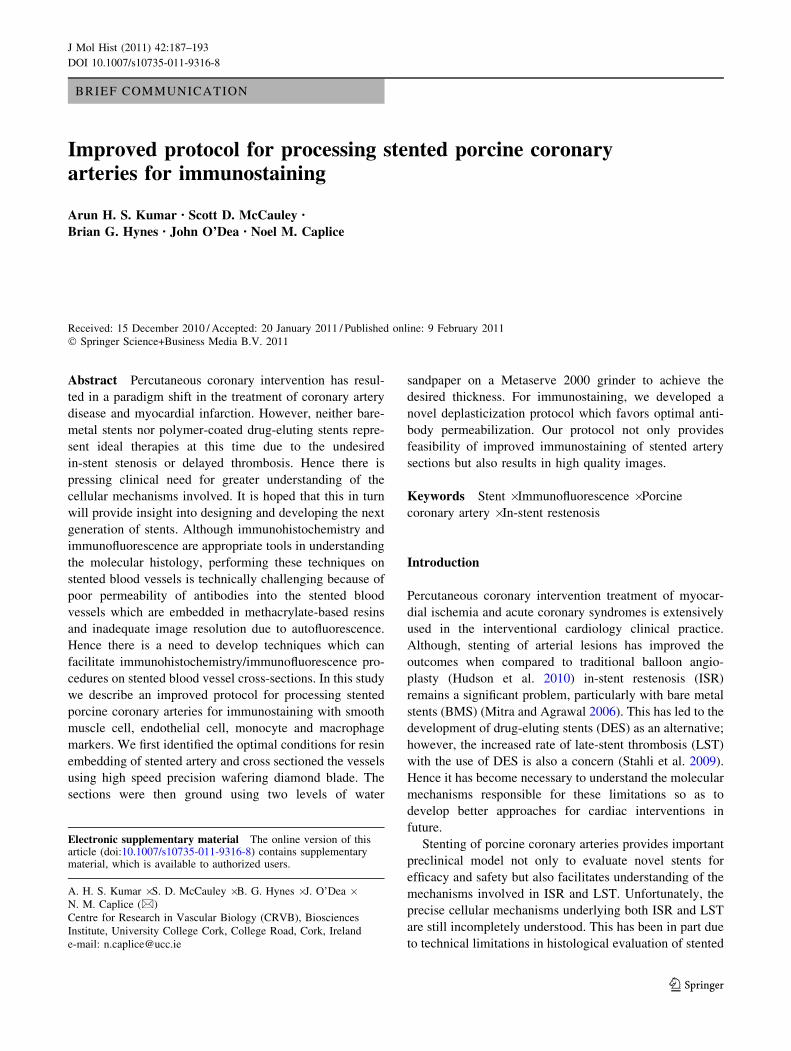
visualized were endothelial cells, vascular smooth muscle
cells, monocytes and macrophages as these cells are
directly relevant to the pathophysiology of instent reste-
nosis. Our protocol resulted in good immunofluorescence
staining for smooth muscle cell markers i.e., a-smooth
muscle actin (Fig. 1) and Calponin (Supplement Fig. 1C)
without any interference from autofluorescence or non-
specific staining (IgG control panel of Fig. 1). The neoin-
tima as expected was predominantly composed of smooth
muscle cells with patches of non smooth muscle regions.
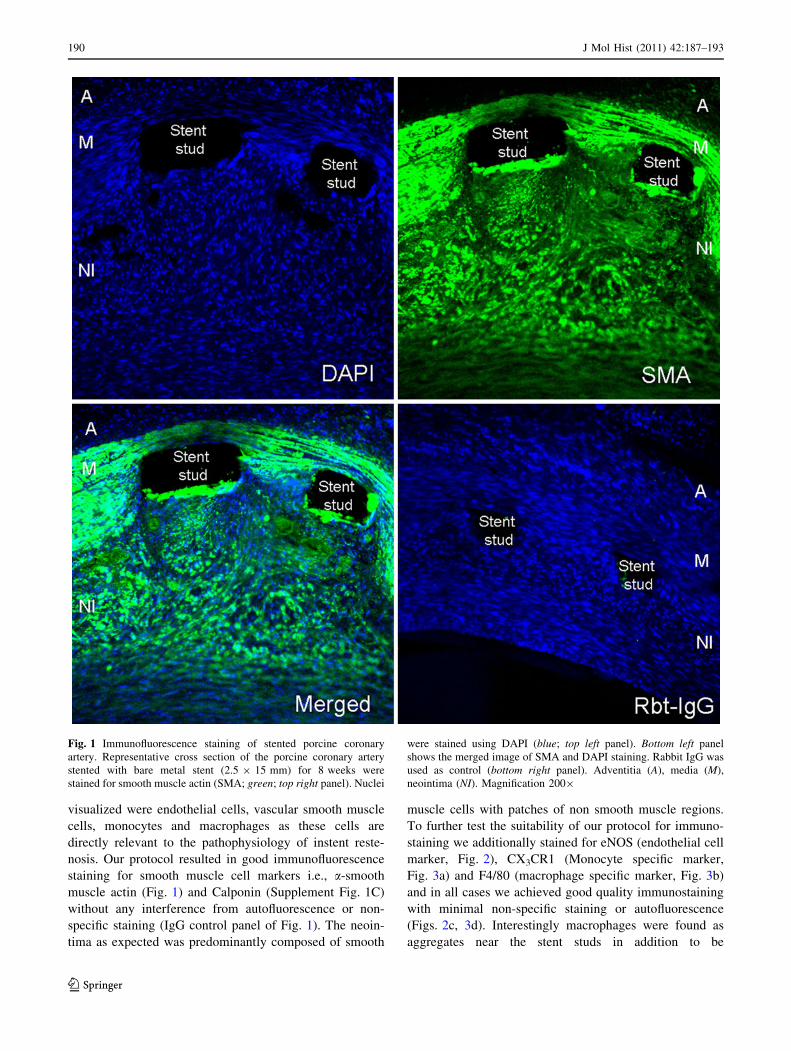
To further test the suitability of our protocol for immuno-
staining we additionally stained for eNOS (endothelial cell
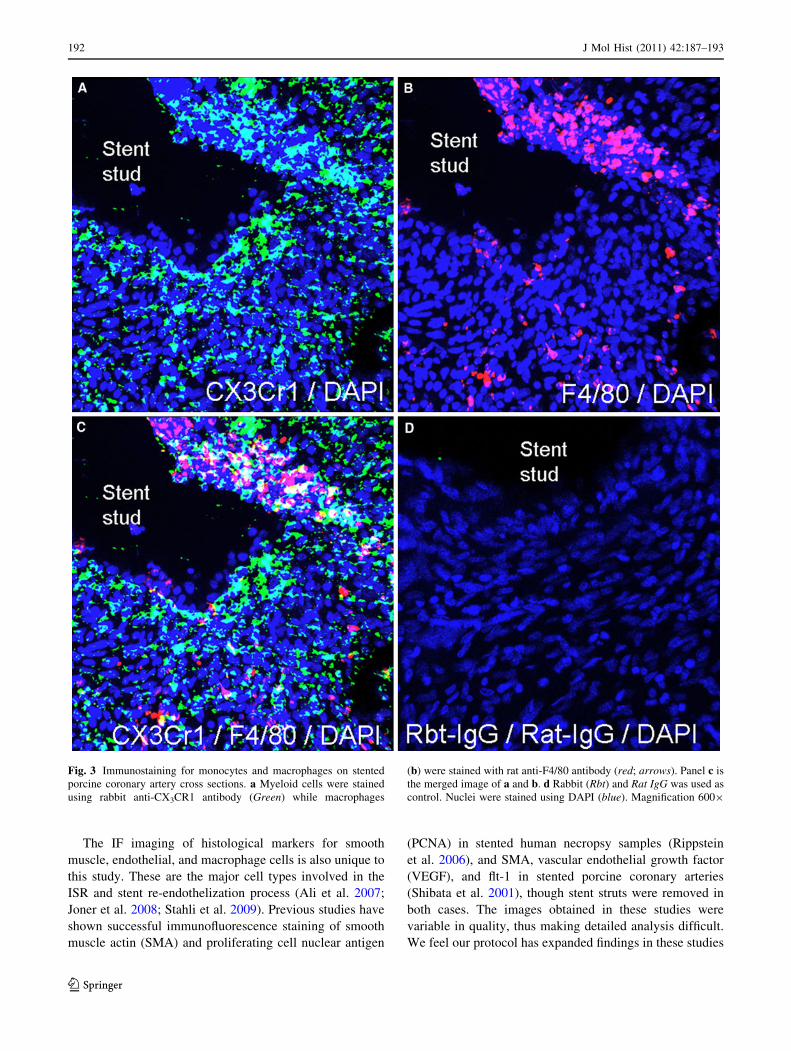
marker, Fig. 2), CX3CR1 (Monocyte specific marker,
Fig. 3a) and F4/80 (macrophage specific marker, Fig. 3b)
and in all cases we achieved good quality immunostaining
with minimal non-specific staining or autofluorescence
(Figs. 2c, 3d). Interestingly macrophages were found as
aggregates near the stent studs in addition to be
Fig. 1 Immunofluorescence staining of stented porcine coronary
artery. Representative cross section of the porcine coronary artery
stented with bare metal stent (2.5 9 15 mm) for 8 weeks were
stained for smooth muscle actin (SMA; green; top right panel). Nuclei
were stained using DAPI (blue; top left panel). Bottom left panel
shows the merged image of SMA and DAPI staining. Rabbit IgG was
used as control (bottom right panel). Adventitia (A), media (M),
neointima (NI). Magnification 2009
190 J Mol Hist (2011) 42:187–193
123
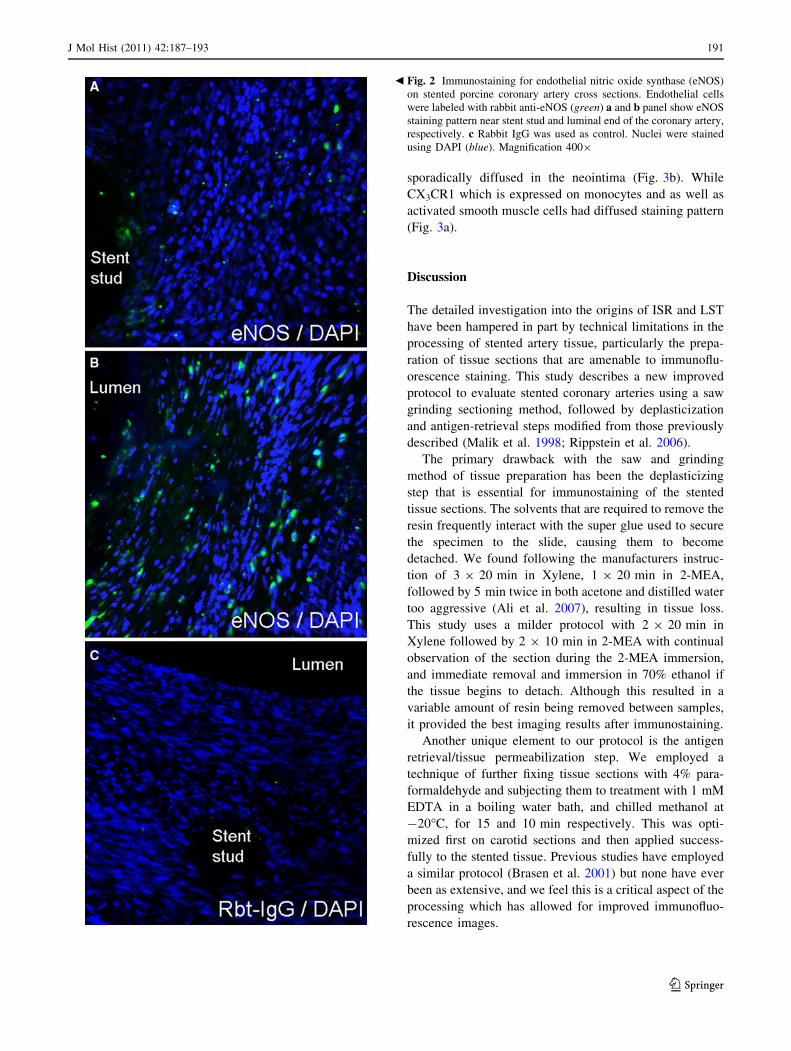
sporadically diffused in the neointima (Fig. 3b). While
CX3CR1 which is expressed on monocytes and as well as
activated smooth muscle cells had diffused staining pattern
(Fig. 3a).
Discussion
The detailed investigation into the origins of ISR and LST
have been hampered in part by technical limitations in the
processing of stented artery tissue, particularly the prepa-
ration of tissue sections that are amenable to immunoflu-
orescence staining. This study describes a new improved
protocol to evaluate stented coronary arteries using a saw
grinding sectioning method, followed by deplasticization
and antigen-retrieval steps modified from those previously
described (Malik et al. 1998; Rippstein et al. 2006).
The primary drawback with the saw and grinding
method of tissue preparation has been the deplasticizing
step that is essential for immunostaining of the stented
tissue sections. The solvents that are required to remove the
resin frequently interact with the super glue used to secure
the specimen to the slide, causing them to become
detached. We found following the manufacturers instruc-
tion of 3 9 20 min in Xylene, 1 9 20 min in 2-MEA,
followed by 5 min twice in both acetone and distilled water
too aggressive (Ali et al. 2007), resulting in tissue loss.
This study uses a milder protocol with 2 9 20 min in
Xylene followed by 2 9 10 min in 2-MEA with continual
observation of the section during the 2-MEA immersion,
and immediate removal and immersion in 70% ethanol if
the tissue begins to detach. Although this resulted in a
variable amount of resin being removed between samples,
it provided the best imaging results after immunostaining.
Another unique element to our protocol is the antigen
retrieval/tissue permeabilization step. We employed a
technique of further fixing tissue sections with 4% para-
formaldehyde and subjecting them to treatment with 1 mM
EDTA in a boiling water bath, and chilled methanol at
-20�C, for 15 and 10 min respectively. This was opti-
mized first on carotid sections and then applied success-
fully to the stented tissue. Previous studies have employed
a similar protocol (Brasen et al. 2001) but none have ever
been as extensive, and we feel this is a critical aspect of the
processing which has allowed for improved immunofluo-
rescence images.
Fig. 2 Immunostaining for endothelial nitric oxide synthase (eNOS)
on stented porcine coronary artery cross sections. Endothelial cells
were labeled with rabbit anti-eNOS (green) a and b panel show eNOS
staining pattern near stent stud and luminal end of the coronary artery,
respectively. c Rabbit IgG was used as control. Nuclei were stained
using DAPI (blue). Magnification 4009
b
J Mol Hist (2011) 42:187–193 191
123
The IF imaging of histological markers for smooth
muscle, endothelial, and macrophage cells is also unique to
this study. These are the major cell types involved in the
ISR and stent re-endothelization process (Ali et al. 2007;
Joner et al. 2008; Stahli et al. 2009). Previous studies have
shown successful immunofluorescence staining of smooth
muscle actin (SMA) and proliferating cell nuclear antigen
(PCNA) in stented human necropsy samples (Rippstein
et al. 2006), and SMA, vascular endothelial growth factor
(VEGF), and flt-1 in stented porcine coronary arteries
(Shibata et al. 2001), though stent struts were removed in
both cases. The images obtained in these studies were
variable in quality, thus making detailed analysis difficult.
We feel our protocol has expanded findings in these studies
Fig. 3 Immunostaining for monocytes and macrophages on stented
porcine coronary artery cross sections. a Myeloid cells were stained
using rabbit anti-CX3CR1 antibody (Green) while macrophages
(b) were stained with rat anti-F4/80 antibody (red; arrows). Panel c is
the merged image of a and b. d Rabbit (Rbt) and Rat IgG was used as
control. Nuclei were stained using DAPI (blue). Magnification 6009
192 J Mol Hist (2011) 42:187–193
123

to provide an improved method of processing stented artery
for immunofluorescence imaging.
Considering the clinical burden of both ISR and LST, it
is critical that strategies be developed to tackle both events,
something which requires a detailed knowledge of the
vascular biology which immunofluorescence imaging can
help provide. Our modified stented artery processing pro-
tocol provides an enhanced method of performing immu-
nofluorescence staining on stented vascular tissue with the
stent strut and tissue structure unaltered. Future studies
focused on specific cellular processes of ISR and LST may
exploit this methodology.
Acknowledgments This work was supported by grants from Sci-
ence Foundation Ireland, Dublin, Ireland (R11482 and RFP06-NMC),
Irish Heart Foundation, Dublin, Ireland (R12348-BH and AHSK), and
HRB summer research fellowship (SM). There are no conflicts of
interests to report.
References
Ali ZA, Alp NJ, Lupton H, Arnold N, Bannister T, Hu Y, Mussa S,
Wheatcroft M, Greaves DR, Gunn J, Channon KM (2007)
Increased in-stent stenosis in ApoE knockout mice: insights from
a novel mouse model of balloon angioplasty and stenting.
Arterioscler Thromb Vasc Biol 27:833–840
Brasen JH, Kivela A, Roser K, Rissanen TT, Niemi M, Luft FC,
Donath K, Yla-Herttuala S (2001) Angiogenesis, vascular
endothelial growth factor and platelet-derived growth factor-
BB expression, iron deposition, and oxidation-specific epitopes
in stented human coronary arteries. Arterioscler Thromb Vasc
Biol 21:1720–1726
Hudson PA, Kim MS, Carroll JD (2010) Coronary ischemia and
percutaneous intervention. Cardiovasc Pathol 19:12–21
Jonas M, Edelman ER, Groothuis A, Baker AB, Seifert P, Rogers C
(2005) Vascular neointimal formation and signaling pathway
activation in response to stent injury in insulin-resistant and
diabetic animals. Circ Res 97:25–33
Joner M, Nakazawa G, Finn AV, Quee SC, Coleman L, Acampado E,
Wilson PS, Skorija K, Cheng Q, Xu X, Gold HK, Kolodgie FD,
Virmani R (2008) Endothelial cell recovery between comparator
polymer-based drug-eluting stents. J Am Coll Cardiol
52:333–342
Malik N, Gunn J, Holt CM, Shepherd L, Francis SE, Newman CM,
Crossman DC, Cumberland DC (1998) Intravascular stents: a
new technique for tissue processing for histology, immunohis-
tochemistry, and transmission electron microscopy. Heart
80:509–516
Mitra AK, Agrawal DK (2006) In stent restenosis: bane of the stent
era. J Clin Pathol 59:232–239
Rippstein P, Black MK, Boivin M, Veinot JP, Ma X, Chen YX,
Human P, Zilla P, O’Brien ER (2006) Comparison of processing
and sectioning methodologies for arteries containing metallic
stents. J Histochem Cytochem 54:673–681
Shibata M, Suzuki H, Nakatani M, Koba S, Geshi E, Katagiri T,
Takeyama Y (2001) The involvement of vascular endothelial
growth factor and flt-1 in the process of neointimal proliferation
in pig coronary arteries following stent implantation. Histochem
Cell Biol 116:471–481
Stahli BE, Camici GG, Tanner FC (2009) Drug-eluting stent
thrombosis. Ther Adv Cardiovasc Dis 3:45–52
J Mol Hist (2011) 42:187–193 193
123




























