Embed Size (px)
Citation preview
Rapid Communication
Degenerative Aortic Valve Stenosis, but not CoronaryDisease, Is Associated With Shorter Telomere Length
in the ElderlyDavid J. Kurz, Barbara Kloeckener-Gruissem, Alexander Akhmedov, Franz R. Eberli, Ines Buhler,
Wolfgang Berger, Osmund Bertel, Thomas F. Luscher
Objective—The mechanisms responsible for the age-related increase in the incidence of calcific aortic valve stenosis (CAS)are unclear but may include telomere-driven cellular senescence. Because telomere length varies widely amongindividuals of the same age, we hypothesized that patients with shorter telomeres would be prone to develop CAS latein life.
Methods and Results—Mean telomere length was measured in leukocytes from a cohort of 193 patients �70 years of agewith and without CAS. Pilot experiments performed in 30 patients with CAS and controls pair-matched for age, sex,and presence or absence of coronary disease demonstrated significantly shorter telomeres in the CAS group both bySouthern blot hybridization (5.75�0.55 kbp versus 6.27�0.7 kbp, P�0.0023) and by a quantitative polymerase chainreaction-based technique (relative telomere length 0.88�0.19 versus 1.0�0.19, P�0.01). This finding was thenconfirmed in the whole cohort (CAS n�64, controls n�129, relative telomere length�0.86�0.16 versus 0.94�0.12,P�0.0003). Both groups were comparable for potential confounding characteristics. Subgroup analysis according to thepresence or absence of coronary disease demonstrated no association of this disorder with telomere length.
Conclusions—In the elderly, calcific aortic stenosis, but not coronary disease, is associated with shorter leukocyte telomerelength. (Arterioscler Thromb Vasc Biol. 2006;26:e114-e117.)
Key Words: aging � aortic stenosis � coronary disease � risk factors � telomere
Degenerative calcific aortic valve stenosis (CAS) is astrictly age-related disorder which can be distinguished
from other forms of aortic stenosis such as post-rheumaticvalve disease or congenital abnormalities (eg, bicuspidvalve). CAS has a prevalence of �4% among those older than85 years1 and is currently the most frequent reason forperforming valve replacement surgery. However, the mech-anisms leading to CAS and its tight association with advanc-ing age remain largely unknown.
At the cellular level, aging leads to a permanent nondividingstate known as replicative senescence, which ensues in somaticcells after a predetermined number of cell divisions and inducescharacteristic changes in gene expression, morphology, andcellular function.2 Entry into the senescent state can be triggeredby the loss of telomere integrity.3 Telomeres build the physicalcaps of chromosomes and, in humans, consist of several thou-
sand repeats of the sequence TTAGGG associated with telomerebinding proteins. Telomeres shorten during replication of so-matic cells, ultimately leading to senescence with progressingbiological age.4 In the human vasculature, telomere length (TL)was found to be shorter at sites with increased hemodynamicstress.5,6 Because the cusps of the aortic valve are exposedlife-long to high levels of mechanical and shear stress, theymight also be prone to the accumulation of senescent cells,which in turn could contribute to the development of age-relatedCAS. Because TL varies widely among individuals of the sameage,7–10 mainly because of hereditary factors,7,9,10 patients withheritably shorter telomeres might have a predisposition towardCAS. We therefore investigated whether the presence of age-related CAS was associated with shorter telomeres in peripheralblood leukocytes. These have been shown to represent a legiti-mate surrogate of tissue TL.8,11
Original received January 5, 2006; final version accepted April 5, 2006.From CardioVascular Center (D.J.K., F.R.E., I.B., T.F.L.), Cardiology, University Hospital; Cardiovascular Research (D.J.K., A.A., T.F.L.), Institute
of Physiology, University of Zurich; Department of Molecular Genetics (B.K.-G., W.B.), Institute of Medical Genetics, University of Zurich; Cardiology(D.J.K., O.B.), Triemli Hospital, Zurich, Switzerland.
Correspondence to David J. Kurz, MD, Cardiovascular Research, Institute of Physiology, University of Zurich-Irchel, Winterthurerstrasse 190,CH-8057 Zurich, Switzerland. E-mail [email protected]
© 2006 American Heart Association, Inc.
Arterioscler Thromb Vasc Biol. is available at http://www.atvbaha.org DOI: 10.1161/01.ATV.0000222961.24912.69
e114
Atherosclerosis and Lipoproteins
by guest on September 6, 2015http://atvb.ahajournals.org/Downloaded from by guest on September 6, 2015http://atvb.ahajournals.org/Downloaded from by guest on September 6, 2015http://atvb.ahajournals.org/Downloaded from by guest on September 6, 2015http://atvb.ahajournals.org/Downloaded from by guest on September 6, 2015http://atvb.ahajournals.org/Downloaded from by guest on September 6, 2015http://atvb.ahajournals.org/Downloaded from by guest on September 6, 2015http://atvb.ahajournals.org/Downloaded from

MethodsPatientsThe study population (n�193) was recruited prospectively frompatients �70 years of age undergoing diagnostic coronary angiog-raphy. Case patients (n�64) all had critical CAS scheduled for valvereplacement surgery and underwent elective angiography to assessfor concomitant coronary artery disease (CAD). Absence of CADwas defined as lack of or minimal coronary atheromatosis asvisualized by angiography. Patients with type I diabetes mellitus,total cholesterol �8 mmol/L, serum creatinine �200 �mol/L, orrecent immunosuppressant/antineoplastic chemotherapy were ex-cluded. Echocardiography was performed in case patients to assessthe mean systolic pressure gradient over the aortic valve, aortic valvemorphology, and left ventricular ejection fraction. In controls(n�129), aortic stenosis was excluded by direct measurement of theaortic valve pressure gradient during left ventricular catheterization.These 2 methods of quantifying transvalvular pressure gradientshave been repeatedly cross-validated and are accepted to be ofequivalent sensitivity and specificity.12 Written informed consentwas obtained from all patients, and the protocol was approved by theinstitutional ethics committee.
TL AnalysisTL analysis was performed by a team blinded to patient character-istics. Blood samples were taken after an overnight fast. WholeEDTA blood was frozen immediately and stored at �80°C untilfurther processing.
DNA IsolationGenomic DNA was extracted using the PureGene DNA extractionkit (Gentra Systems, Minneapolis, Minn) or magnetic bead technol-ogy (Chemagen, Baesweiler, Germany). Control experiments con-firmed that TL analysis of the same sample extracted by bothtechniques delivered virtually identical results.
Terminal Restriction Fragment Determination bySouthern BlotTerminal restriction fragment (TRF) length analysis was performedusing standard techniques.4 For details, see the online data supple-ment available at http://atvb.ahajournals.org. Each case sample wasrun with its pair-matched control on adjacent lanes. Results are themean of 2 independent assessments for each sample. The interassayvariability was 7.8%� 7%.
TL Determination by Quantitative PolymeraseChain ReactionIn a parallel approach, relative TL was determined using a previouslydescribed13 and validated14–16 polymerase chain reaction-basedmethod. For details, see the online data supplement available athttp://atvb.ahajournals.org.
Statistical AnalysisStudent t tests were used to compare continuous variables. Thedistribution of categorical variables was compared with the �2 test.Values of P�0.05 were considered significant.
ResultsPilot experiments were performed on a set of 30 cases and 30controls, selected from the cohort to be pair-matched for age,sex, and the presence or absence of CAD, factors that havepreviously been associated with differences in leukocyteTL.7–9,17 Clinical, risk factor and hemodynamic characteris-tics of these patients were comparable and are summarized inTable I (see online data supplement available at http://atvb.ahajournals.org). The 2 groups were comparable withregard to cardiovascular risk factor profiles, plasma levels oflipoproteins and C-reactive protein, body mass index, andstatin use.
TRF length determined by Southern blot analysis demon-strated that the CAS patients had on average significantlyshorter telomeres than the controls, with the differencebetween the means of the 2 groups equaling 0.52 kbp(5.75�0.55 versus 6.27�0.7 kbp, P�0.002) (Figure 1). Theaverage annual decline in TRF length as calculated by linearregression was 35.2�21.8 base pairs/year and was not sig-nificantly different between groups (ANCOVA, data notshown). These results were confirmed using a quantitativepolymerase chain reaction-based method of TL analysis.Although less sensitive, this approach has recently becomemore widely used because of its suitability for high-throughput analysis.13–16 The mean relative TL of the CASpatients and controls included in the pilot experiments was0.88�0.19 and 1.0�0.19, respectively (P�0.01). Linearregression analysis for the correlation between these 2 verydifferent methods of measuring TL delivered a correlationcoefficient of 0.262 for the relationship between relative TLand TRF length (P�0.0001, data not shown).
We next tested whether the association between shorter TLand CAS found in the pilot study could be reproduced in theentire cohort of 193 patients, made up of 64 CAS patients and129 controls. Baseline characteristics were comparable andhardly differed from the pilot study pair-matched groups(Table). The mean relative TL in the CAS group was
Figure 1. A, Representative autoradiogramof Southern blot hybridization signals froma telomere-specific probe to DNA extractsfrom patients �70 years of age withsevere calcific aortic stenosis (AS) or pair-matched controls (C). B, Distribution ofmean leukocyte terminal restriction frag-ment (TRF) lengths from the 60 patients inthe pilot study. Mean TRFs from patientswith calcific aortic stenosis (CAS) were onaverage 0.52 kilobase pairs (kbp) shorterthan their pair-matched controls. Circlesand horizontal bars represent individualpatients and the mean value, respectively.
Kurz et al Telomere Length in Aortic Stenosis e115
by guest on September 6, 2015http://atvb.ahajournals.org/Downloaded from
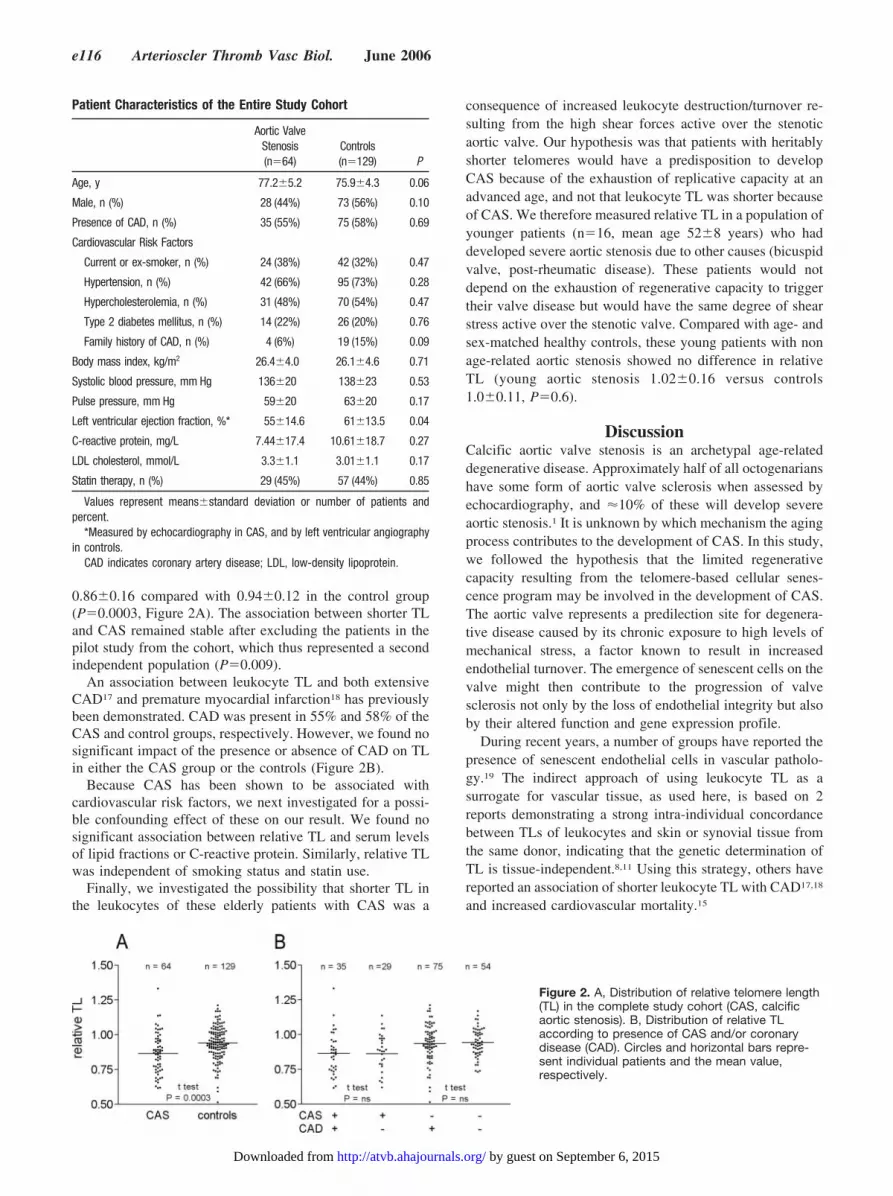
0.86�0.16 compared with 0.94�0.12 in the control group(P�0.0003, Figure 2A). The association between shorter TLand CAS remained stable after excluding the patients in thepilot study from the cohort, which thus represented a secondindependent population (P�0.009).
An association between leukocyte TL and both extensiveCAD17 and premature myocardial infarction18 has previouslybeen demonstrated. CAD was present in 55% and 58% of theCAS and control groups, respectively. However, we found nosignificant impact of the presence or absence of CAD on TLin either the CAS group or the controls (Figure 2B).
Because CAS has been shown to be associated withcardiovascular risk factors, we next investigated for a possi-ble confounding effect of these on our result. We found nosignificant association between relative TL and serum levelsof lipid fractions or C-reactive protein. Similarly, relative TLwas independent of smoking status and statin use.
Finally, we investigated the possibility that shorter TL inthe leukocytes of these elderly patients with CAS was a
consequence of increased leukocyte destruction/turnover re-sulting from the high shear forces active over the stenoticaortic valve. Our hypothesis was that patients with heritablyshorter telomeres would have a predisposition to developCAS because of the exhaustion of replicative capacity at anadvanced age, and not that leukocyte TL was shorter becauseof CAS. We therefore measured relative TL in a population ofyounger patients (n�16, mean age 52�8 years) who haddeveloped severe aortic stenosis due to other causes (bicuspidvalve, post-rheumatic disease). These patients would notdepend on the exhaustion of regenerative capacity to triggertheir valve disease but would have the same degree of shearstress active over the stenotic valve. Compared with age- andsex-matched healthy controls, these young patients with nonage-related aortic stenosis showed no difference in relativeTL (young aortic stenosis 1.02�0.16 versus controls1.0�0.11, P�0.6).
DiscussionCalcific aortic valve stenosis is an archetypal age-relateddegenerative disease. Approximately half of all octogenarianshave some form of aortic valve sclerosis when assessed byechocardiography, and �10% of these will develop severeaortic stenosis.1 It is unknown by which mechanism the agingprocess contributes to the development of CAS. In this study,we followed the hypothesis that the limited regenerativecapacity resulting from the telomere-based cellular senes-cence program may be involved in the development of CAS.The aortic valve represents a predilection site for degenera-tive disease caused by its chronic exposure to high levels ofmechanical stress, a factor known to result in increasedendothelial turnover. The emergence of senescent cells on thevalve might then contribute to the progression of valvesclerosis not only by the loss of endothelial integrity but alsoby their altered function and gene expression profile.
During recent years, a number of groups have reported thepresence of senescent endothelial cells in vascular patholo-gy.19 The indirect approach of using leukocyte TL as asurrogate for vascular tissue, as used here, is based on 2reports demonstrating a strong intra-individual concordancebetween TLs of leukocytes and skin or synovial tissue fromthe same donor, indicating that the genetic determination ofTL is tissue-independent.8,11 Using this strategy, others havereported an association of shorter leukocyte TL with CAD17,18
and increased cardiovascular mortality.15
Patient Characteristics of the Entire Study Cohort
Aortic ValveStenosis(n�64)
Controls(n�129) P
Age, y 77.2�5.2 75.9�4.3 0.06
Male, n (%) 28 (44%) 73 (56%) 0.10
Presence of CAD, n (%) 35 (55%) 75 (58%) 0.69
Cardiovascular Risk Factors
Current or ex-smoker, n (%) 24 (38%) 42 (32%) 0.47
Hypertension, n (%) 42 (66%) 95 (73%) 0.28
Hypercholesterolemia, n (%) 31 (48%) 70 (54%) 0.47
Type 2 diabetes mellitus, n (%) 14 (22%) 26 (20%) 0.76
Family history of CAD, n (%) 4 (6%) 19 (15%) 0.09
Body mass index, kg/m2 26.4�4.0 26.1�4.6 0.71
Systolic blood pressure, mm Hg 136�20 138�23 0.53
Pulse pressure, mm Hg 59�20 63�20 0.17
Left ventricular ejection fraction, %* 55�14.6 61�13.5 0.04
C-reactive protein, mg/L 7.44�17.4 10.61�18.7 0.27
LDL cholesterol, mmol/L 3.3�1.1 3.01�1.1 0.17
Statin therapy, n (%) 29 (45%) 57 (44%) 0.85
Values represent means�standard deviation or number of patients andpercent.
*Measured by echocardiography in CAS, and by left ventricular angiographyin controls.
CAD indicates coronary artery disease; LDL, low-density lipoprotein.
Figure 2. A, Distribution of relative telomere length(TL) in the complete study cohort (CAS, calcificaortic stenosis). B, Distribution of relative TLaccording to presence of CAS and/or coronarydisease (CAD). Circles and horizontal bars repre-sent individual patients and the mean value,respectively.
e116 Arterioscler Thromb Vasc Biol. June 2006
by guest on September 6, 2015http://atvb.ahajournals.org/Downloaded from

The main finding of this study is that patients with severeCAS have on average shorter telomeres than appropriatelymatched controls. A second important finding was the lack ofassociation between shorter TL and the presence of angio-graphically verified CAD in this elderly population. Thisfinding was consistently present in both the CAS and controlgroups (Figure 2B). This result contrasts with other publica-tions reporting shorter leukocyte TL in patients withCAD.17,18 However, of these 1 study investigated only pa-tients who had sustained an acute myocardial infarctionbefore the age of 50,18 whereas in the other study reported bythe same group only 1 patient and 2 controls were older thanage 70 years.17 One might speculate that shorter TL inpatients with premature CAD might be related to a moreinflammatory nature of the disease compared with CAD inthe elderly.
Although our findings show a clear association betweenshorter TL and CAS, they do not demonstrate a causalrelationship. Additional factors, such as chronic inflamma-tion, hypercholesterolemia, or increased levels of oxidativestress, might contribute to the development of CAS andindependently thereof accelerate leukocyte telomere erosion.Nonetheless, in our population no such confounding associ-ations were identified. Alternatively, one could speculate thatthe hemodynamic shear forces active over the stenotic aorticvalve might increase leukocyte turnover and would thus leadto shorter telomeres. Our findings from a smaller group ofyoung patients with severe aortic stenosis attributable to othercauses (postrheumatic disease, bicuspid valve) and age- andsex-matched controls showed that this was not the case,supporting a role for shorter telomere length selectively in thedevelopment of age-related degenerative CAS.
Evolutionary aging theories suggest that genes or processesthat were selected to benefit young organisms can haveunselected deleterious effects that become manifest in olderorganisms and thereby contribute to the aging phenotype.20
The process of telomere-based replicative senescence fits thisconcept in humans by protecting against the development ofcancer during the years of reproductive activity, but resultingin degenerative disorders at advanced ages. The associationwe report here between age-related CAS and shorter TL iscompatible with the concept that the telomere-dependentexhaustion of regenerative capacity may participate in thedevelopment of this disorder.
AcknowledgmentsWe acknowledge technical assistance of S. Pancera and Y. Gruissemin extracting DNA.
Source(s) of FundingThis work was supported by the Swiss National Science Foundation(grants 3100-066976 [D.J.K.], 3100-067786 [W.B.], and 3100-068118.02 [T.F.L.]) and the Swiss Heart Foundation (D.J.K.).
Disclosure(s)None.
References1. Stewart BF, Siscovick D, Lind BK, Gardin JM, Gottdiener JS, Smith VE,
Kitzman DW, Otto CM. Clinical factors associated with calcific aorticvalve disease. Cardiovascular Health Study. J Am Coll Cardiol. 1997;29:630–634.
2. Campisi J. Senescent cells, tumor suppression, and organismal aging:good citizens, bad neighbors. Cell. 2005;120:513–522.
3. Blackburn EH. Switching and signaling at the telomere. Cell. 2001;106:661–673.
4. Harley CB, Futcher AB, Greider CW. Telomeres shorten during ageing ofhuman fibroblasts. Nature. 1990;345:458–460.
5. Chang E, Harley CB. Telomere length and replicative aging in humanvascular tissues. Proc Natl Acad Sci U S A. 1995;92:11190–11194.
6. Okuda K, Khan MY, Skurnick J, Kimura M, Aviv H, Aviv A. Telomereattrition of the human abdominal aorta: relationships with age and ath-erosclerosis. Atherosclerosis. 2000;152:391–398.
7. Slagboom PE, Droog S, Boomsma DI. Genetic determination of telomeresize in humans: a twin study of three age groups. Am J Hum Genet.1994;55:876–882.
8. von Zglinicki T, Serra V, Lorenz M, Saretzki G, Lenzen-GrossimlighausR, Gessner R, Risch A, Steinhagen-Thiessen E. Short telomeres inpatients with vascular dementia: an indicator of low antioxidativecapacity and a possible risk factor? Lab Invest. 2000;80:1739–1747.
9. Nawrot TS, Staessen JA, Gardner JP, Aviv A. Telomere length andpossible link to X chromosome. Lancet. 2004;363:507–510.
10. Vasa-Nicotera M, Brouilette S, Mangino M, Thompson JR, Braund P,Clemitson JR, Mason A, Bodycote CL, Raleigh SM, Louis E, Samani NJ.Mapping of a major locus that determines telomere length in humans.Am J Hum Genet. 2005;76:147–151.
11. Friedrich U, Griese E, Schwab M, Fritz P, Thon K, Klotz U. Telomerelength in different tissues of elderly patients. Mech Ageing Dev. 2000;119:89–99.
12. Currie PJ, Hagler DJ, Seward JB, Reeder GS, Fyfe DA, Bove AA, TajikAJ. Instantaneous pressure gradient: a simultaneous Doppler and dualcatheter correlative study. J Am Coll Cardiol. 1986;7:800–806.
13. Cawthon RM. Telomere measurement by quantitative PCR. NucleicAcids Res. 2002;30:e47.
14. Broberg K, Bjork J, Paulsson K, Hoglund M, Albin M. Constitutionalshort telomeres are strong genetic susceptibility markers for bladdercancer. Carcinogenesis. 2005;26:1263–1271.
15. Cawthon RM, Smith KR, O’Brien E, Sivatchenko A, Kerber RA. Asso-ciation between telomere length in blood and mortality in people aged 60years or older. Lancet. 2003;361:393–395.
16. Grabowski P, Hultdin M, Karlsson K, Tobin G, Aleskog A, Thunberg U,Laurell A, Sundstrom C, Rosenquist R, Roos G. Telomere length as aprognostic parameter in chronic lymphocytic leukemia with special ref-erence to VH gene mutation status. Blood. 2005;105:4807–4812.
17. Samani NJ, Boultby R, Butler R, Thompson JR, Goodall AH. Telomereshortening in atherosclerosis. Lancet. 2001;358:472–473.
18. Brouilette S, Singh RK, Thompson JR, Goodall AH, Samani NJ. Whitecell telomere length and risk of premature myocardial infarction. Arte-rioscler Thromb Vasc Biol. 2003;23:842–846.
19. Erusalimsky JD, Kurz DJ Cellular senescence in vivo: Its relevance inageing and cardiovascular disease. Exp Gerontol. 2005.
20. Campisi J. Cancer and ageing: rival demons? Nat Rev Cancer. 2003;3:339–349.
Kurz et al Telomere Length in Aortic Stenosis e117
by guest on September 6, 2015http://atvb.ahajournals.org/Downloaded from

Online data supplement Kurz DJ et al. Degenerative aortic valve stenosis, but not coronary disease, is associated with shorter telomere length in the elderly.
1
Online data supplement
Kurz DJ et al. Degenerative aortic valve stenosis, but not coronary
disease, is associated with shorter telomere length in the elderly.
Methods
Terminal restriction fragment determination by Southern blot
Terminal restriction fragment (TRF) length analysis was performed using standard
techniques 1. Aliquots (1.5 µg) of genomic DNA were digested with 20 units each of the
restriction enzymes HinfI and RsaI during 3 hours at 37°C (final concentration 1 U/µl).
Set-up experiments verified complete DNA digestion under these conditions. Digests
were separated on a 0.7% agarose gel and transferred to a positively labeled nylon
membrane (Hybond N+, Amersham Biosciences) under high-salt conditions. The blots
were hybridized with a 32P-labeled oligonucleotide telomere probe
(CCCTAACCCTAACCCTAA) and exposed to a phospho-imager after standard high-
stringency washes. Hybridization signals were quantified by computer-assisted scanning
densitometry using the public domain NIH Image software. The mean TRF lengths were
calculated by integrating the signal intensity over the entire TRF distribution as a
function of TRF length using the formula TRF length = Σ(ODi) / Σ(ODi/Li), where ODi
and Li are the signal intensity and TRF length respectively at position i on the
autoradiogram 1. Identical molecular weight standards run on either side and in the
middle of the gel confirmed homogeneous migration conditions. In order to minimize

Online data supplement Kurz DJ et al. Degenerative aortic valve stenosis, but not coronary disease, is associated with shorter telomere length in the elderly.
2
problems resulting from inter-gel variability, each case sample was run with its pair-
matched control on adjacent lanes of the same gel.
Telomere length determination by quantitative PCR
In a parallel approach relative TL was determined using a previously described 2 and
validated 3-5 PCR-based method. In a reaction volume of 10 µl, genomic DNA (6ng) was
combined with a mastermix in 384-well plates as dispensed by robotic pipetting. Each
plate contained sample DNA as well as five serial dilutions of reference DNA, which
served as standards in calculating the relative TL. Each DNA sample was analyzed at
least 4 times. A first mastermix contained telomere-specific primers (100nM of tel1b:
CGGTTTGTTTGGGTTTGGGTTTGGGTTTGGGTTTGGGTT, and 900 nM of tel2b:
GGTTGCCTTACCCTTACCCTTACCCTTACCCTTACCCT) in the presence of 1.7
mM MgCl2 while a second mastermix, analyzed on a separate plate, contained primers
specific for the single copy gene beta globin (hbg) (300 nM of hbg1:
GCTTCTGACACAACTGTGTTCACTAGC and 700 nM of hbg2:
CACCAACTTCATCCACGTTCACC) in the presence of 2.5 mM MgCl2. Amplification
was performed with 0.8 U Hotstar polymerase and its corresponding 10x buffer and
MgCl2 stock (Quiagen) in the presence of 0.15x SYBR Green (Applied Biosystems,
Rotkreuz, Switzerland) and 2.5 mM dithiothreitol. Amplification was performed with a
Prism 7900 Sequence Detection System (Applied Biosystems, Rotkreuz, Switzerland).
The temperature cycling regime was adapted from the preprogrammed cycling conditions
as follows: after 15 minutes at 95°C, 25 cycles followed for the telomere probe at 56°C
(30 seconds) and 72°C (30 seconds) while 35 cycles were applied for the hbg probes with
the annealing temperature of 58°C. ABI Prism 7900 SDS software version 2.2 was used

Online data supplement Kurz DJ et al. Degenerative aortic valve stenosis, but not coronary disease, is associated with shorter telomere length in the elderly.
3
for analysis. Relative TL (2-ddCt) was calculated as described in the User Bulletin #2 (ABI
PRISM 7700 Sequence detection System) from mean Ct values of 4 to 8 replicates for
each sample. Patient and control TLs were calculated relative to those obtained for a
standard DNA sample, present on all plates. The functionality and reproducibility of the
assay was confirmed on a series of DNA extracts from serially passaged human
endothelial cells with a known linear decrease in TL (data not shown).

Online data supplement Kurz DJ et al. Degenerative aortic valve stenosis, but not coronary disease, is associated with shorter telomere length in the elderly.
4
Table I:
Characteristics of pair-matched patients in the pilot study with and without calcific aortic
valve stenosis
Aortic valve stenosis
(n = 30)
Controls
(n = 30)
P value
Age* (y) 76.9 ± 4.0 76.9 ± 4.0 1.0
Male* (n, %) 14 (47%) 15 (50%) 0.8
Presence of CAD* (n, %) 13 (43%) 14 (47%) 0.8
Cardiovascular Risk Factors
Current or ex-smoker (n, %) 14 (47%) 8 (27%) 0.11
Hypertension (n, %) 22 (73%) 24 (80%) 0.54
Hypercholesterolemia (n, %) 17 (57%) 14 (47%) 0.44
Type 2 diabetes mellitus (n, %) 8 (27%) 7 (23%) 0.77
Family history of CAD (n, %) 2 (7%) 6 (20%) 0.13
Body Mass Index (kg/m2) 26.1 ± 4.2 25.7 ± 3.0 0.72
Systolic blood pressure (mm Hg) 137 ± 19 147 ± 27 0.11
Pulse pressure (mm Hg) 56 ± 22 69 ± 23 0.03
Left ventricular ejection fraction (%)† 56 ± 16 64 ± 15 0.07
C-reactive protein (mg/l) 4.64 ± 4.25 7.83 ± 11.92 0.19
LDL-Cholesterol (mmol/l) 3.37 ± 1.12 3.09 ± 0.81 0.32
Statin therapy (n, %) 12 (40%) 11 (37%) 0.79
Calcific aortic valve stenosis (n, %) 30 (100%) 0 (0%) N/A
Mean pressure gradient (mm Hg) 50 ± 15 N/A N/A
Calculated aortic valve area (cm2) 0.75 ± 0.17 N/A N/A
Values represent means ± standard deviation or number of patients and percent. *
features used to pair-match subjects. †measured by echocardiography in CAS, and by left
ventricular angiography in controls. CAD, coronary artery disease; LDL, low density
lipoprotein; ns, not significant; N/A, not applicable.

Online data supplement Kurz DJ et al. Degenerative aortic valve stenosis, but not coronary disease, is associated with shorter telomere length in the elderly.
5
References
1. Harley CB, Futcher AB, Greider CW. Telomeres shorten during ageing of human fibroblasts. Nature. 1990;345:458-460.
2. Cawthon RM. Telomere measurement by quantitative PCR. Nucleic Acids Res. 2002;30:e47.
3. Broberg K, Bjork J, Paulsson K, Hoglund M, Albin M. Constitutional short telomeres are strong genetic susceptibility markers for bladder cancer. Carcinogenesis. 2005;26:1263-1271.
4. Cawthon RM, Smith KR, O'Brien E, Sivatchenko A, Kerber RA. Association between telomere length in blood and mortality in people aged 60 years or older. Lancet. 2003;361:393-395.
5. Grabowski P, Hultdin M, Karlsson K, Tobin G, Aleskog A, Thunberg U, Laurell A, Sundstrom C, Rosenquist R, Roos G. Telomere length as a prognostic parameter in chronic lymphocytic leukemia with special reference to VH gene mutation status. Blood. 2005;105:4807-4812.
6. Slagboom PE, Droog S, Boomsma DI. Genetic determination of telomere size in humans: a twin study of three age groups. Am J Hum Genet. 1994;55:876-882.

Bühler, Wolfgang Berger, Osmund Bertel and Thomas F. LüscherDavid J. Kurz, Barbara Kloeckener-Gruissem, Alexander Akhmedov, Franz R. Eberli, Ines
Telomere Length in the ElderlyDegenerative Aortic Valve Stenosis, but not Coronary Disease, Is Associated With Shorter
Print ISSN: 1079-5642. Online ISSN: 1524-4636 Copyright © 2006 American Heart Association, Inc. All rights reserved.
Greenville Avenue, Dallas, TX 75231is published by the American Heart Association, 7272Arteriosclerosis, Thrombosis, and Vascular Biology
doi: 10.1161/01.ATV.0000222961.24912.692006;26:e114-e117; originally published online April 20, 2006;Arterioscler Thromb Vasc Biol.
http://atvb.ahajournals.org/content/26/6/e114World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://atvb.ahajournals.org/content/suppl/2006/04/24/01.ATV.0000222961.24912.69.DC1.htmlData Supplement (unedited) at:
http://atvb.ahajournals.org//subscriptions/
at: is onlineArteriosclerosis, Thrombosis, and Vascular Biology Information about subscribing to Subscriptions:
http://www.lww.com/reprints
Information about reprints can be found online at: Reprints:
document. Question and AnswerPermissions and Rightspage under Services. Further information about this process is available in the
which permission is being requested is located, click Request Permissions in the middle column of the WebCopyright Clearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of theArteriosclerosis, Thrombosis, and Vascular Biologyin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on September 6, 2015http://atvb.ahajournals.org/Downloaded from





























