Embed Size (px)
Citation preview
Discriminative Validityof the Global Physiotherapy Examination-52
in Patients with Long-Lasting Musculoskeletal Painversus Healthy Persons
Kvåle, Skouen, and Ljunggren Alice KvåleJan Sture Skouen
Anne Elisabeth Ljunggren
ABSTRACT. Objectives: The aims of thisstudy were to evaluate the discriminative abil-ity of a body examination in healthy subjectsversus patients with long-lasting musculo-skeletal pain, and further to compare physi-cal findings in patients with localized versuswidespread pain, and between women andmen.
Methods: The Global Physiotherapy Ex-amination [GPE-52] was used to evaluatebodily aberrations in 247 patients [159 women,88 men] with long-lasting musculoskeletalpain. The GPE consists of 52 standardizedtests within five main domains: Posture, Res-piration, Movement, Muscle, and Skin. Pa-tients were categorized into three subgroupsaccording to pain distribution: pain localizedeither to the upper or lower body, or wide-spread pain. For comparison, 104 healthypersons without pain [64 women, 40 men]were also examined.
Results: Significant differences were foundbetween healthy persons and patients within
all five main domains, most within the Move-ment and Muscle domains, least within theRespiration and Skin domains. Patients withwidespread pain had significantly higherscores, indicating aberrations, within the Move-ment and Muscle domains compared to pa-tients with localized pain. Men had higherscores within Posture and Movement, whereasfemale patients had significantly higher scoreswithin Skin.
Conclusions: Indications were providedthat the GPE-52, especially the Movementand Muscle domains, discriminate betweenpatients groups and healthy subjects, and giveinformation about degree of bodily aberra-tions. Different characteristics were founddepending on gender and pain distribution.[Article copies available for a fee from The HaworthDocument Delivery Service: 1-800-HAWORTH.E-mail address: <[email protected]>Website: <http://www.HaworthPress.com> 2003by The Haworth Press, Inc. All rights reserved.]
Alice Kvåle, PT, MSc, is Research Fellow, Section of Physiotherapy Science, Faculty of Medicine, University ofBergen, Bergen, Norway.
Jan Sture Skouen, MD, PhD, is Associate Professor, Section of Physiotherapy Science, Faculty of Medicine, Uni-versity of Bergen and The Outpatient Spine Clinic, Haukeland University Hospital, Bergen, Norway.
Anne Elisabeth Ljunggren, PT, PhD, is Professor, Section of Physiotherapy Science, Faculty of Medicine, Uni-versity of Bergen, Bergen, Norway.
Address correspondence to: Alice Kvåle, Section of Physiotherapy Science, University of Bergen, Ulriksdal 8c,N-5009 Bergen, Norway [E-mail: [email protected]].
The authors want to thank the physiotherapists Tove Dragesund and Hildegunn Lygren who took part in the ex-amination of the patients. Special thanks to Assistant Professor Liv Inger Strand for her interest and support in writ-ing this paper. The authors greatly appreciate the support from psychometrician Tom Backer Johnsen, Faculty ofPsychology, University of Bergen, when performing the Structural Equation Modeling.
This work was financed by the Royal Norwegian Department of Health and Social Affairs, and by a researchgrant from the Faculty of Medicine, University of Bergen, Bergen, Norway.
Submitted: January 6, 2003.Revision accepted: April 16, 2003.
Journal of Musculoskeletal Pain, Vol. 11(3) 2003http://www.haworthpress.com/store/product.asp?sku=J094
2003 by The Haworth Press, Inc. All rights reserved.Digital Object Identifier: 10.1300/J094v11n03_04 23

KEYWORDS. Movement, muscle, norma-tive data, pain drawing, posture, respiration,skin
INTRODUCTION
The diagnostic process for patients withlong-lasting pain problems is complex andtime consuming. Signs and symptoms that maybe related to a patient’s report of musculo-skeletal problems are difficult to assess andquantify. Evaluation of patients with persistentmusculoskeletal pain should include physical,psychosocial, and behavioral information forplanning appropriate treatment and for moni-toring change in health status (1,2). No univer-sally accepted criteria for assessment of pa-tients with long-lasting pain, however, seemto exist (3).
Patients with long-lasting musculoskeletalproblems often have no obvious explanationfor their pain symptom, and may report pain inseveral areas (4,5). A too narrow focus in theassessment process may overlook possiblepredisposing and maintaining factors. Morefunction-based measures (6), and assessmentof impairments should be performed to pro-vide an objective basis to aid decisions in thediagnostic process and to evaluate treatmentprogression. However, single physical testsof, for example, range of motion and musclestrength, may not be useful alone, becausethey tend to lack sensitivity, specificity, andresponsiveness (7).
For the last few years a standardized and ex-tensive physiotherapy evaluation method hasbeen used in several pain and rehabilitationclinics in Scandinavia, as a basis for better un-derstanding the changes that might take placewithin bodily domains, such as in Posture,Respiration, Movement, Muscle, and Skin. Themethod, formerly called the Global Physio-therapeutic Muscle Examination, has 78 tests[GPM-78], and was originally developed forevaluation of patients with psychosomatic andpsychiatric problems (8). The GPM is basedupon a construct that the whole body may re-act to long-lasting physical and/or psychologi-cal problems, causing changes in posture, res-piration, flexibility, and muscle tension. All ofthese aspects should therefore be included in
the evaluation process of patients with long-lasting pain [> 8-12 weeks] problems (9,10).In a recent study of patients with long-lastingmusculoskeletal pain problems, the concur-rent validity was demonstrated between thismethod and psychological findings, but mainlyin patients with widespread pain (11). Whetherall 78 items would be equally useful when ex-amining patients with long-lasting pain, hasbeen questioned. A recent examination of theconstruct of the GPM-78 by means of struc-tural equation modeling (12) has been per-formed and resulted in a modified, shorter andsounder version, called the Global Physiother-apy Examination [GPE-52] (13-15).
Attempts to determine what is normal, ex-cessive, or diminished regarding physical char-acteristics, must take into account variationsfound in a normative sample. As patients withlong-lasting musculoskeletal pain are presumedto differ from healthy subjects, the aim of thisstudy was to examine the ability of the GPE-52to discriminate between patients with long-lasting musculoskeletal pain and healthy con-trols. Furthermore, as patients with long-last-ing musculoskeletal pain constitute a hetero-geneous group, it would also be of interest toexamine whether the GPM-52 could discrimi-nate between patients with localized and wide-spread pain. And finally, as there seem to befew studies regarding comparison of physicalfindings between women and men, this wasalso examined.
MATERIALS AND METHODS
Subjects
The material comprised 247 consecutivepatients [159 women, 22 to 66 years, mean age44.2, SD 10.0; 88 men, 24 to 64 years, meanage 42.5, SD 11.1], sick-listed for an averageof 3.3 months [SD 2, range 1-20] because ofmusculoskeletal disorders. An experienced medi-cal doctor decided the medical diagnoses. Thepatients’ primary diagnosis could be groupedinto four broad categories: 9.3 percent had aneck diagnosis, 49.4 percent low back pain,22.7 percent had general muscular pain, and18.6 percent had other diagnosis. Patients were
24 JOURNAL OF MUSCULOSKELETAL PAIN
excluded from the study if they were pregnant,were registered substance abusers, or had otherdiseases, such as progressive neurological dis-ease, active rheumatological disease, or otherserious medical conditions from other organs.The patients participated in a large random-ized controlled rehabilitation project (16), anddata are from the standard battery of examina-tions before treatment. In addition to physicalexaminations, the patients filled in differentforms of questionnaires concerning psycho-social factors, pain intensity [measured on a100 mm visual analog scale], pain distribution[measured by counting number of squaresmarked on pain drawing (17)], and disability[measured by mean score of the DisabilityRating Index [DRI] (18)].
A total of 104 healthy employed personswere later examined [64 women, 21 to 63years, mean age 41.8, SD 10.8; 40 men, 22 to65 years, mean age 40.0, SD 12.7]. They hadnot been sick-listed due to musculoskeletalpain the last year, or had any episodes withstrong pain the last 14 days before examina-tion. The healthy persons constituted a conve-nience sample, and were not familiar with thetest instrument prior to examination. Age groupsfrom 20 to 65 years, with 60 percent womenand 40 percent men were made in advance,and participants recruited until the healthy sam-ple had a similar age and gender span as thepatient sample.
All subjects were thoroughly informed bypersonal instruction, and written consent ob-tained at inclusion. The study was accepted bythe Regional Ethics Committee and performedaccording to the World Medical AssociationDeclaration of Helsinki, which is an interna-tional accepted code of ethics, stating ethicalguidance in medical research involving hu-man subjects.
Categorization Based on Pain Drawing
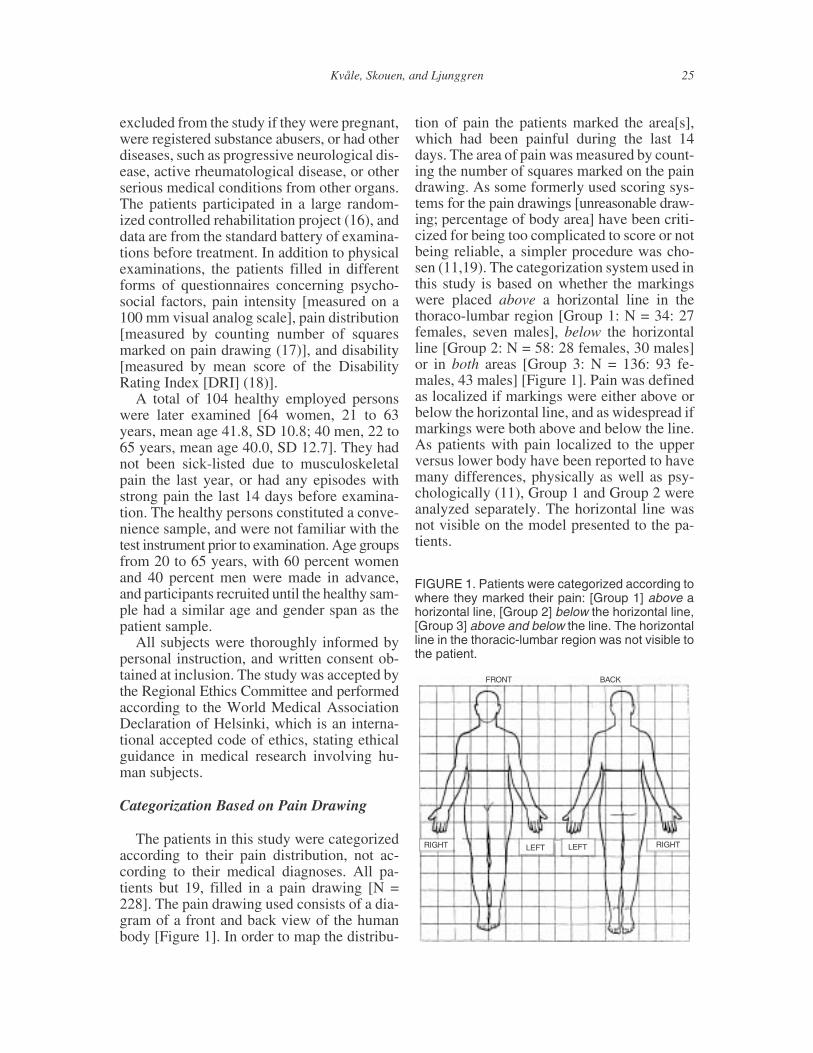
The patients in this study were categorizedaccording to their pain distribution, not ac-cording to their medical diagnoses. All pa-tients but 19, filled in a pain drawing [N =228]. The pain drawing used consists of a dia-gram of a front and back view of the humanbody [Figure 1]. In order to map the distribu-
tion of pain the patients marked the area[s],which had been painful during the last 14days. The area of pain was measured by count-ing the number of squares marked on the paindrawing. As some formerly used scoring sys-tems for the pain drawings [unreasonable draw-ing; percentage of body area] have been criti-cized for being too complicated to score or notbeing reliable, a simpler procedure was cho-sen (11,19). The categorization system used inthis study is based on whether the markingswere placed above a horizontal line in thethoraco-lumbar region [Group 1: N = 34: 27females, seven males], below the horizontalline [Group 2: N = 58: 28 females, 30 males]or in both areas [Group 3: N = 136: 93 fe-males, 43 males] [Figure 1]. Pain was definedas localized if markings were either above orbelow the horizontal line, and as widespread ifmarkings were both above and below the line.As patients with pain localized to the upperversus lower body have been reported to havemany differences, physically as well as psy-chologically (11), Group 1 and Group 2 wereanalyzed separately. The horizontal line wasnot visible on the model presented to the pa-tients.
Kvåle, Skouen, and Ljunggren 25
FRONT BACK
RIGHT RIGHTLEFT LEFT
FIGURE 1. Patients were categorized according towhere they marked their pain: [Group 1] above ahorizontal line, [Group 2] below the horizontal line,[Group 3] above and below the line. The horizontalline in the thoracic-lumbar region was not visible tothe patient.

The Global Physiotherapy Examination[GPE-52]
The GPE-52 yields information of fivebodily domains: Posture, Respiration, Move-ment, Muscle, and Skin. These domains aredivided into 13 subdomains, each with fourtests [Table 1]. Each of the 52 tests includedare standardized and scored as defined in amanual (8,20). A book, a video, and a manualcontaining detailed description of the tests,with pictures of each examination, are at thispoint published only in Norwegian. However,description of the tests and the scoring scale isalso available in English. The examiner’s main“instruments” while using the GPE-52 are ob-servation, palpation, and handling. In addi-tion, a ruler and a goniometer are used. Thevariables represent items from the whole body.One fourth of the tests are nonside specific.When assessing limbs, only the left side of thebody is examined, based on claims that pa-tients with long-lasting problems tend to havesimilar degrees of aberrations in both bodyhalves (8,20). If a major impairment is presentin the right body half, this area will also be ex-amined, but not scored.
The 52 items are defined according to anempirically defined standard or ideal, giventhe score zero, and deviations from the stan-dard can go in two directions [decreased or in-creased] [Table 2]. The two directions giveclinical information, but the main focus is ontotal degree of problems. An early version ofthe GPM, consisting of only five scoring cate-gories on an ordinal scale, was not sensitiveenough to reveal change, therefore it was di-vided into a finer scoring scale (9,21,22). Thescale used during the last 10 years consists of15-steps ranging from �2.3 to +2.3 (11,20).An impression of degree of problems in thepatient’s somatic status is obtained throughsummation of the absolute score values to a to-tal GPE-52 sum score, five main domain sumscores, and 13 subdomain sum scores. An ex-amination takes about 30 minutes. The methodis taught briefly as part of the basic physio-therapy education in Norway. However, in or-der to use the method reliably, further special-ization including a two to three day course,followed by practice is considered to be neces-sary.
26 JOURNAL OF MUSCULOSKELETAL PAIN
TABLE 1. Schematic Overview of the Main Do-mains, the Subdomains, and the Items Included inthe Global Physiotherapy Examination-52
5 main domains 13 subdomains 52 separate items
Posture Posture standing Knee position
Lumbar lordosis L1-5
Epigastrium lateral
Head protrusion
Posture supine Foot rotation
Low-costal medial angle
Shoulder protraction
Head position
Respiration Respiration standing/ Hypogastrium medial2
Respiration supine Epigastrium lateral2
Low-costal lateral2
High-costal medial2
Movement Passive range of motion Knee flexion in long-sitting
Hip abduction
Shoulder flexion
Lateral cervical flexion
Flexibility Retraction shoulder
Lumbo-sacral flexibility
Head-nod flexibility
Head rotation
Passive movement Elbow drop
Hip circumduction
Compression thorax
Arm elevation
Active movement Rolling sit-up [+]
Toe-forefoot-ankle flexion [+]
Distance teeth mouth open
Chin protrusion pout [+]
Muscle Stretch palpation of Abdominals/ diaphragm 2
muscle/Reaction to Gastrocnemius medial2
stretch Rectus femoris2
Sternocleidomastoid2
Pressure palpation Erector spinae Th 8-10
of muscle Triceps brachii
Gastrocnemius medial
Upper trazius
Skin Pressure palpation of skin Erector spinae Th 8-10
Rectus femoris
Trapezius
Sternocleidomastoid
Stretch palpation of skin Triceps brachii
Gastrocnemius medial
Rectus femoris
Sternocleidomastoid
2 Examined in 2 subdomainsA few items have only one direction, these are marked with [+], indicatingthat the scale ranges from 0 to +2.3, i.e., a 7-point scale, with zero indicat-ing the ideal state, and 2.3 the gravest deviation. The other items can be bi-polar, ranging from �2.3 to +2.3, i.e., a 15-point scale.

Presently ongoing research on the dimen-sional structure of the GPE-52, using principalcomponent factor analysis, revealed that the13 subdomains were unidimensional and clas-sified into five meaningful factors. These fac-tors are consistent with the original empiri-cally defined main domains (9), except for thesubdomain Passive range of motion, whichformerly was placed within the domain ofPosture (11). This subdomain loaded togetherwith the three subdomains included under thedomain Movement. Variables adding little in-formation and with poor measurement fit (12),have been omitted in the recent GPE-52 ver-sion, but the included items still represent thewhole body (13-15).
Intertester reliability of the GPE-52 has pre-viously been examined by three physiothera-pists [PTs] who were to perform the physicalexaminations of the patients included in thisstudy. Both patients and healthy persons wereexamined. Acceptable relative and absolutereliability was achieved, and with mean differ-ences between the testers less than one pointapart for the total sum score (13-15). Overallintraclass correlation coefficients [ICC model2.1] was 0.91 for the GPE-52 sum score, andranged from 0.60 to 0.89 for the main do-mains. Measurement error [sw] for the main
domains ranged from 1.1 to 1.6. For Posture andRespiration the somewhat low ICCs [0.65 and0.60] seemed due to limited range in scores, asthe size of the sw was similar as for the Skindomain [1.1], which had an ICC of 0.76. Oneof the three PTs examined later all the healthypersons. As the healthy subjects were exam-ined after the patients, a new inter-tester ex-amination was performed to ensure that thisPT still used the scoring scale in a reliableway. Similar acceptable inter-tester results wereachieved.
Statistics
Statistics were performed using the Statisti-cal Package of Social Sciences [release 11.0].Parametric statistics was applied in this studyas the data was normally distributed. The meanvalues and standard deviations [SD] of theGPE-52 are presented for healthy persons andfor the patient group[s]. Independent t-testswere calculated for differences between thetwo samples. One-way analysis of variancewith Scheffé’s post hoc test was used to ana-lyze differences between the three patient groupsfor the GPE-52. All P-values are two-sided,and values < 0.05 were considered significant.
Kvåle, Skouen, and Ljunggren 27
TABLE 2. A Schematic View of the Application of the Scoring Scale in the Global Physiotherapy Examina-tion-52
� SCALE +
�2 [much] �1 [somewhat] 0 +1 [somewhat] +2 [much]
DOMAIN �2.3 �2.0 �1.7 �1.3 �1.0 �0.7 �0.3 0 +0.3 +0.7 +1.0 +1.3 +1.7 +2.0 +2.3
1. Posture8 tests
Extended Flexed
2. Respiration8 tests
IncreasedToo much movement
Decreased movementParadoxical movement
3. Movement16 tests
Too large rangeToo flexible
Good Reduced rangeToo restrained
4. Muscle12 tests
Too stretchableNo/indifferent reactionToo compressive
Too shortPainfulToo distended
5. Skin8 tests
Too stretchableToo compressive
Too shortToo distended
1 Maximum possible score: 8 tests � 2.3 = 18.412 tests � 2.3 = 27.618 tests � 2.3 = 41.4
Positive and negative scores give clinical information, whereas absolute values indicate degree of aberrations away from the standard. The scoring scalehas two main groups on both sides of the main group 0. The standard, also called “ideal” or “good,” lies in the middle of main group 0. Each main group issubdivided in three. To avoid use of several decimals [.333 and .667], the scores have been rounded [.3 and .7]. Thus, maximum possible score for eachtest is 2.3, and total possible sum score with 4 tests is 9.2.1 The manual contains standardized definitions for each item of how to transfer the quality andquantity [cm or degree] into a score.

To evaluate the discriminative validity ofthe different domains, the scores from thehealthy subjects were compared to those of thepatients also by means of a receiver operatingcharacteristic curve [ROC]. Area under thecurve was calculated. The greater the area un-der the curve, the greater the ability of the in-strument to distinguish between the two groups.The ROC area must be > .50 in order to showdiscriminative ability above chance (23).
RESULTS
Background Data
No significant difference was found in agebetween the women or the men when compar-ing healthy and patients [Women: F[1, 222] =2.46, P = 0.118; Men: F[1,127] = 1.25, P =0.267]. Patients with widespread pain [Group3] had significantly higher pain intensity, largerarea of pain, and a worse situation in terms ofdisability measured with DRI, compared toGroup 2 [Table 3]. Significant differences werealso found between Group 3 and Group 1 re-garding DRI and number of squares marked asbeing painful. No significant differences werefound between patients in Groups 1 and 2 re-garding pain and disability.
Comparison of Global PhysiotherapyExamination-52 Scores Between HealthySubjects and Patients
Global Physiotherapy Examination-52 sumscore: A significant difference [F[1, 349] =
14.68, P < 0.001] was found in sum score be-tween healthy individuals and patients, healthypersons had a mean score of 33.9 [SD 6.4,range 21.2-47.1], and patients a mean sumscore of 46.9 [SD 8.0, range 25.2-68.8]. TheROC-area regarding difference between healthyand patients was 0.894, indicating very highsensitivity. Comparison of scores between gen-der within group showed that healthy maleshad significantly higher total GPE-52 sum score[mean score 37, SD 5.2], compared to healthywomen [mean score 32, SD 6.4], but withinthe patient sample no significant differencewas found in total sum score.
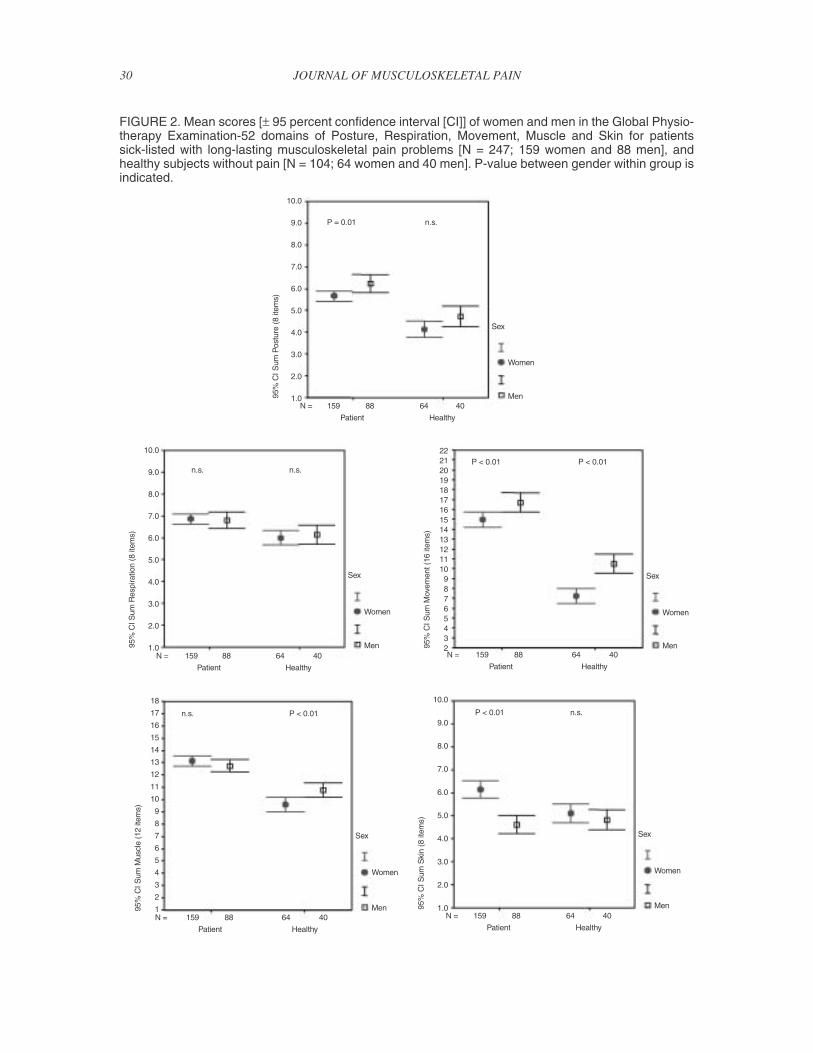
Main domains: Mean and standard devia-tion for healthy persons and patients are pre-sented in Table 4. Significant differences [P <0.05] were found between the two samples inall five domains. Differences in mean scoreswere largest in the Movement domain [F[1,349] = 13.43, P < 0.001], than in Muscle [F =10.14, P < 0.001] and Posture [F = 7.77, P <0.001], and least in the domains Respiration[F = 4.35, P < 0.001] and Skin [F[1, 349] =2.43, P = 0.016]. Area under the curve is listedin Table 4. Healthy females had on averagesignificantly less aberrations in Movement andMuscle compared to healthy men [Figure 2].Female patients had significantly higher scoresin the Skin domain compared to male patients,whereas male patients had more aberrations inthe domains Posture and Movement.
Subdomains: Significant differences betweenhealthy and patients were found in 12 out of 13subdomains [Table 4]. The highest scores, in-dicating most aberrations, were found withinFlexibility, and Reaction to stretch palpationof muscle, in patients with long-lasting mus-culoskeletal pain. Within Pressure palpationof skin, the comparison resulted in a nonsig-nificant difference between healthy personsand patients.
Comparison of Global PhysiotherapyExamination-52 Scores in Healthy Subjectsand Three Patient Groups Categorized byPain Drawing
Significant differences [P < 0.05] were foundin GPE-52 total sum score and all main do-mains, except Skin, between the healthy sub-jects and each of the three patient groups [Ta-
28 JOURNAL OF MUSCULOSKELETAL PAIN
TABLE 3. Background Data for Healthy Subjectsand Patients Subcategorized into Three GroupsAccording to Their Pain Drawing1
Healthymean [SD]
N = 34
Group 1mean [SD]
N = 34
Group 2mean [SD]
N = 58
Group 3mean [SD]
N = 136
Age 41.1 [11.5] 41.5 [10.0] 41.2 [10.5] 45.1 [10.3]
Pain [VAS] No pain 47.1 [19.3] 40.9 [22.0] 53.1 [18.9]
Pain area2 No pain 14.5 [8.2] 13.0 [8.5] 30.3 [18.1]
DRI3 No disability 37.0 [12.6] 44.4 [18.4] 52.6 [17.1]
1 Group 1: Pain marked above a horizontal line in the thoracic-lumbar re-gion
Group 2: Pain marked only below the lineGroup 3: Pain marked both above and below the horizontal line
2 Pain area: Number of squares marked as painful on pain drawing3 DRI: Disability Rating Index

ble 5]. Significant differences were also foundbetween healthy subjects and each of the pa-tient groups in most of the subdomains. Pa-tients in Group 1 had more aberrations regard-ing Posture supine, Respiration standing, Passiverange of motion, Flexibility, Active move-ment, Reaction to stretch of muscle, and Pres-sure palpation of muscle, when compared tohealthy subjects. Patients in Group 2 differedsignificantly from healthy subjects regardingPosture supine, all subdomains of movement,as well as in Reaction to stretch of muscle, andPressure palpation of muscle. Patients withwidespread pain [Group 3] differed signifi-cantly in all subdomains, except Respirationsupine, Stretch palpation of muscle, and Pres-sure palpation of skin.
Comparison of Global PhysiotherapyExamination-52 Scores Between the ThreePatients Groups
Global Physiotherapy Examination-52 sumscore: Mean and standard deviation for thethree patient groups are listed in Table 5. Sig-nificant differences were found in sum scorebetween the three groups, and patients withwidespread pain had the highest sum score.There was no significant difference betweengender, within group, in GPE-52 sum score.
Main domains: Significant differences be-tween the patient groups were found in themain domains of Movement and Muscle [P �0.001]. Within Movement, Scheffé’s post-hoctest revealed significantly higher scores forpatients in Group 3, compared to patients inGroup 1 and 2. Within Muscle, Scheffé’s post-hoc test revealed that the difference was sig-nificant only between Group 2 and 3 [Table 5].No significant difference was found betweengroups in the domains Posture, Respiration, orSkin.
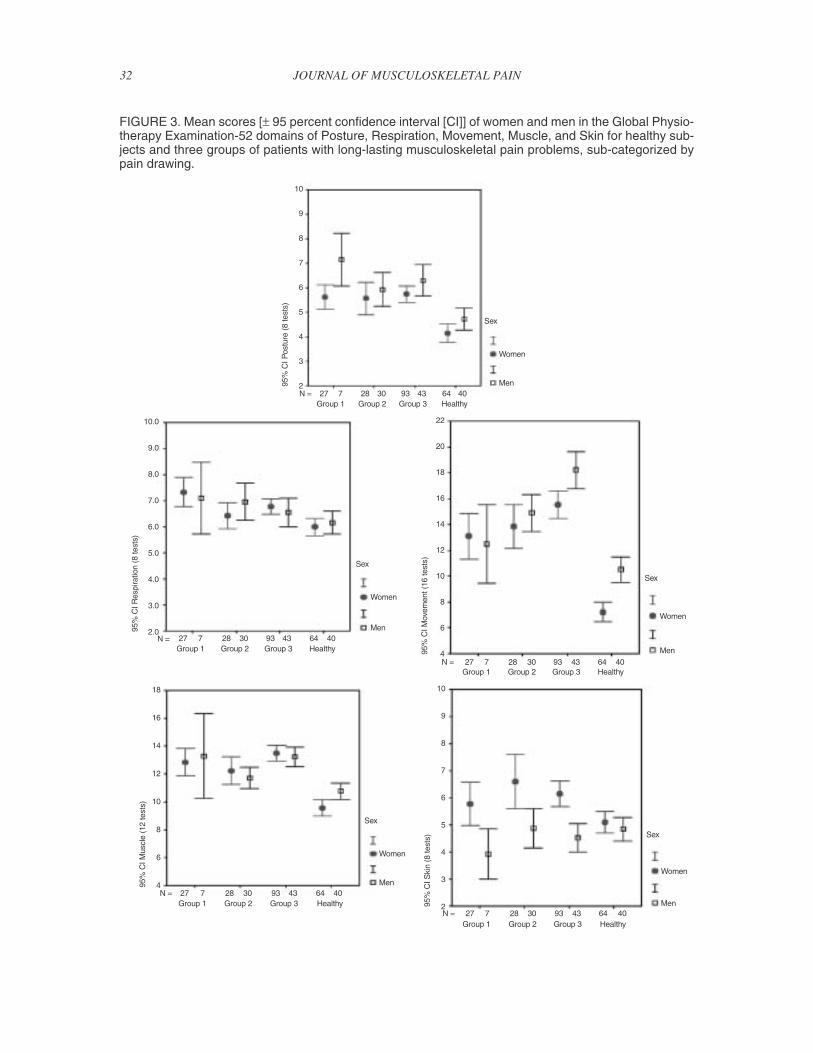
In Figure 3 the mean scores, with 95 percentconfidence interval, are illustrated separatelyfor women and men in the three patient groups.As there were only seven men in Group 1, theconfidence interval is large for this group. InPosture, male patients in Group 1 had signifi-cantly higher scores compared to women inthe same group. In Movement, scores differedsignificantly between gender within group forpatients in Group 3, men having very highscores. Within the Skin domain, the femalepatients had significantly higher scores com-pared to men, in all patient groups.
Subdomains: One-way analysis of variancerevealed significant differences in bodily ab-errations between the different patient groupsin seven out of 13 subdomains. Scheffé’s post-hoc tests revealed pairwise significant differ-ences in the subdomains: Passive range of mo-
Kvåle, Skouen, and Ljunggren 29
TABLE 4. Mean [and Standard Deviation] of the Global Physiotherapy Examination-52 Within Five MainDomains and 13 Subdomains in Healthy Persons and Patients with Long-Lasting Musculoskeletal Pain
Main domains[sum score]
Healthymean [SD]
N = 104
Patientmean [SD]
N = 247Subdomains
[sum of 4 tests]
Healthymean [SD]
N = 104
Patientmean [SD]
N = 247ROC-area
95% CI forarea under the
curve
Posture 4.4 [1.5] 5.9 [1.7] Posture standing 2.5 [1.1] 2.9 [1.0] .627** .562; 6918 tests [ROC = 0.755]** Posture supine 1.9 [1.0] 3.0 [1.3] .755** .701; 810
Respiration 6.1 [1.3] 6.8 [1.6] Respiration standing 3.7 [0.8] 4.2 [0.9] .696** .638; 7548 tests [ROC = 0.655]** Respiration supine 2.4 [0.7] 2.6 [0.9] .589** .524; 654
Movement Passive range of motion 2.1 [1.2] 3.7 [1.7] .768** .712; 82016 tests 8.5 [3.4] 15.6 [4.9] Flexibility 3.0 [1.5] 5.4 [1.6] .860** .820; 900
[ROC = 0.880]** Passive movement 1.8 [1.2] 3.2 [1.7] .740** .685; 795Active movement 1.6 [0.9] 3.3 [1.5] .848** .807; 889
Muscle 10.0 [2.3] 13.0 [2.6] Stretch palpation of muscle 3.9 [1.1] 4.2 [1.1] .579* .513; 64512 tests [ROC = 0.802]** Reaction to stretch of muscle 3.0 [1.3] 4.7 [1.5] .802** .755; 849
Pressure palpation of muscle 3.2 [0.7] 4.1 [1.0] .783** .733; 832
Skin 5.0 [1.5] 5.6 [2.3] Pressure palpation of skin 2.9 [0.9] 3.0 [1.3] .496 .434; 5578 tests [ROC = 0.569]* Stretch palpation of skin 2.1 [0.9] 2.6 [1.3] .612** .551; 674
* P < 0.05** P < 0.01
Differences between the two samples are listed with ROC area, with 95 percent confidence interval. Significant difference between the two groups, exam-ined with independent t-tests, is indicated with asterisk.
30 JOURNAL OF MUSCULOSKELETAL PAIN
10.0
9.0
8.0
7.0
6.0
5.0
4.0
3.0
2.0
1.0
10.0
9.0
8.0
7.0
6.0
5.0
4.0
3.0
2.0
1.0
10.0
9.0
8.0
7.0
6.0
5.0
4.0
3.0
2.0
1.0
2221201918171615141312111098765432
18
17
16
15
14
13
12
11
10
9
8
7
6
5
4
3
2
1
P = 0.01
P < 0.01
P < 0.01 P < 0.01
P < 0.01
n.s.
n.s.
n.s.
n.s.
n.s.
Sex
Sex
SexSex
Sex
Women
Women
WomenWomen
Women
Men
Men
MenMen
Men
Patient
PatientPatient
Patient Patient
Healthy
HealthyHealthy
Healthy Healthy
159
159159
159 159
88
8888
88 88
64
6464
64 64
40
4040
40 40
95%
CIS
umP
ostu
re(8
item
s)
95%
CI S
umR
espi
ratio
n(8
item
s)
95%
CIS
umS
kin
(8ite
ms)
95%
CI S
umM
ovem
ent (
16ite
ms)
95%
CI S
umM
uscl
e(1
2ite
ms)
N =
N =N =
N = N =
FIGURE 2. Mean scores [± 95 percent confidence interval [CI]] of women and men in the Global Physio-therapy Examination-52 domains of Posture, Respiration, Movement, Muscle and Skin for patientssick-listed with long-lasting musculoskeletal pain problems [N = 247; 159 women and 88 men], andhealthy subjects without pain [N = 104; 64 women and 40 men]. P-value between gender within group isindicated.

tion, Flexibility, Passive movement, Activemovement, Reaction to stretch palpation ofmuscle, and Pressure palpation of muscle–Group 3 having the highest scores. WithinRespiration standing, patients in Group 1 hadthe highest scores.
DISCUSSION
In this study, the GPE-52 seemed to be avalid method to find physical characteristicsboth in healthy persons and in patients withlong-lasting musculoskeletal problems. Sig-nificant differences were found between healthypersons and patients in all the five main bodilydomains assessed, and all but one of the sub-domains. The main domains Movement andMuscle differentiated most, information fromthe domains Respiration and Skin least. Fur-thermore, use of the GPE-52 showed that therealso were different physical findings in pa-tients with localized versus widespread pain,patients with widespread pain having morephysical aberrations. Different characteristicswere also found between patients who hadpain localized to the upper versus lower body.In clinical practice it is important to identifythe physical problems or aberrations of an in-dividual patient. Understanding of normal vari-ation might help to distinguish between a prob-lem that should be the focus of treatment, andwhich should not.
The therapists in this study were not blindedfor which subjects were patients and healthy,but extensive work on intertester examina-tions in both healthy persons and patients priorto the collection of data was done to ensure thesame use of the GPE-52 for both samples. TheGPE-52 may appear to be complex, but aseach item is well defined and standardized it isfairly easy to learn and use. The testers’ scoresreflected high inter-tester reliability, and alltesters were experienced in use of the GPE-52.Global Physiotherapy Examination-52 measuresseem representative for patients on long-termsick-leave due to musculoskeletal problems,and accordingly the findings are considered tohave external validity (16).
Distinct subgroups of patients as measuredby the GPE-52 were exposed. Patients withwidespread pain [Group 3] had high scores in-dicating aberrations in the main domains Move-ment and Muscle. Distinct psychological char-acteristics have also been found for the threesubgroups, patients with widespread pain hav-ing significantly more health concerns, soma-tization, and depression compared to patientswith localized pain (11). The present cross-sectional study has not the ability to tell whyaberrations develop or which came first re-garding the physical and/or psychological ab-errations. Flexibility measures may be influ-enced by a number of factors such as pain,psychological problems, in addition to ana-tomical and physiological limitations (24-26).
Kvåle, Skouen, and Ljunggren 31
TABLE 5. Scores of Main Domains of the Global Physiotherapy Examination-52 in Three Patient GroupsCategorized by Pain Drawing1
Main domainsof GPE-52
Group 1mean [SD]
N = 34
Group 2mean [SD]
N = 58
Group 3mean [SD]
N = 136
P-value betweenpatient groups
Post-hoc testP-value
Posture8 tests
5.9 [1.4] * 5.8 [1.8] * 5.9 [1.8] * P = 0.819
Respiration8 tests
7.3 [1.4] * 6.7 [1.7] 6.7 [1.6] * P = 0.129
Movement16 tests
13.0 [4.2] * 14.4 [4.1] * 16.4 [5.1] * P < 0.001 Gr. 1 vs. 3 = 0.001Gr. 2 vs. 3 = 0.032
Muscle12 tests
12.9 [2.6] * 12.0 [2.3] * 13.4 [2.6] * P = 0.001 Gr. 2 vs. 3 = 0.001
Skin8 tests
5.4 [2.0] 5.7 [2.4] 5.6 [2.3] P = 0.807
GPE-52 sum 44.5 [6.7] * 44.5 [7.4] * 48.1 [8.1] * P = 0.004 Gr. 1 vs. 3 = 0.060Gr. 2 vs. 3 = 0.015
1 Group 1: Pain marked above a horizontal line in the thoracic-lumbar regionGroup 2: Pain marked only below the lineGroup 3: Pain marked both above and below the horizontal line
P-values for differences between the patient groups [ANOVA] are listed. Significant differences between healthy persons and each patient group are indi-cated * [P < 0.05]. Scheffé’s post-hoc test shows pair wise differences between the patient groups.
32 JOURNAL OF MUSCULOSKELETAL PAIN
10
9
8
7
6
5
4
3
2N = 27 7 28 30 93 43 64 40
Sex
Women
Men
Group 1 Group 2 Group 3 Healthy
95%
CIP
ostu
re(8
test
s)
10.0
9.0
8.0
7.0
6.0
5.0
4.0
3.0
2.0N = 27 7 28 30 93 43 64 40
Sex
Women
Men
Group 1 Group 2 Group 3 Healthy
95%
CIR
espi
ratio
n(8
test
s)
22
20
18
16
14
12
10
8
6
4N = 27 7 28 30 93 43 64 40
Sex
Women
Men
Group 1 Group 2 Group 3 Healthy
95%
CIM
ovem
ent(
16te
sts)
18
16
14
12
10
8
6
4N = 27 7 28 30 93 43 64 40
Sex
Women
Men
Group 1 Group 2 Group 3 Healthy
95%
CIM
uscl
e(1
2te
sts)
10
9
8
7
6
5
4
3
2N = 27 7 28 30 93 43 64 40
Sex
Women
Men
Group 1 Group 2 Group 3 Healthy
95%
CIS
kin
(8te
sts)
FIGURE 3. Mean scores [± 95 percent confidence interval [CI]] of women and men in the Global Physio-therapy Examination-52 domains of Posture, Respiration, Movement, Muscle, and Skin for healthy sub-jects and three groups of patients with long-lasting musculoskeletal pain problems, sub-categorized bypain drawing.

Within the domain Muscle, a difference wasfound regarding muscular findings betweenpatients with widespread and localized pain, acontinuum being found from patients withwidespread having the highest scores, patientswith neck pain intermediate, and patients withpain in the lower body, least aberrations. Emo-tional distress and anxiety, muscle overloadfrom poor posture, inappropriate patterns ofmuscle use, including failure to relax, are amongrecognized sources related to muscular aberra-tions (9,27,28).
Patients with pain localized only to the lum-bar region and/or lower extremities [Group 2]had less muscular problems than the other twogroups, but still a high degree of Movementaberrations. This group of patients had mainlylow back pain diagnosis [LBP], and a close as-sociation between movement aberrations andLBP have been reported in several studies(26,29). A former study suggested that pain-related fear plays an important role in the de-velopment of guarded movement in patientswith LBP, more so than pain severity or dis-ability levels (29). If the physical changes inpatients with long-lasting musculoskeletal painmainly are related to Movement aberrations,this could for many patients be addressed in afear-reduction approach in treatment. High scorewithin Movement, without other possible in-fluencing factors, may indicate a potential forchange with the right treatment approach, butfurther studies must examine this.
Patients with neck and shoulder problems[Group 1] had fewer problems regarding Move-ment than the other groups, but high scoreswithin Muscle and much higher scores in Res-piration compared to the other groups. Scoringof inspection of the respiration movement inupright position (13), tended to differentiatebetween patients with pain localized above thethoraco-lumbar line, compared to patients witheither more widespread pain or pain in thelower part of the body [F[2, 227] = 3.52, P =0.012]. In a study of patients with cranio-man-dibular dysfunction, inhibited respiration ap-peared to be a characteristic (30). Restrainedbasic respiration may cause recruitment of so-called auxiliary musculature. To make theseact as muscles of respiration their origin mustbe kept fixed, which again leads to activationof neck, throat, and jaw muscles. Respiration
aberration and long-lasting contractions of aux-iliary musculature may maintain problems inpatients with pain in the upper body, if not ad-dressed in treatment. Furthermore, this couldincrease the risk for developing widespreadpain (31,32).
Interesting differences in physical findingsbetween gender were found in our study. Inaccordance with a former study which includedmuch the same items within Movement (22),our study showed that men had the highest de-gree of aberrations when compared to females.Furthermore, our study showed that this dif-ference was related to men with widespreadpain. In a former study, lack of flexibility andreduced ability to relax correlated with healthconcerns in men (11). This could indicate thatmen with widespread pain react with fear andmovement aberrations (29), to a much largerdegree than females do, but further studies areneeded. Interestingly, no difference was foundbetween gender within the patient groups re-garding muscular findings, and little seems tohave been reported in literature. Within thedomain Skin, female patients had significantlyhigher scores compared to male patients andhealthy subjects [Figure 2 and 3], indicatingthat they had reduced elasticity of skin. Littlehas been reported regarding possible aberra-tions regarding skin quality as measured bypressure or stretch palpation in patients withmusculoskeletal pain problems. Findings inthis study seem to be in accordance with find-ings of a study where patients with fibromyalgia[FMS] were compared to normal controls andto very fit controls (33). In Granges and Little-john’s study (33), a continuum was demon-strated from patients with FMS to fit controls,with unfit controls having intermediate val-ues. Patients with FMS had many musculartender points and significantly more objectivephysical signs from the skin: diffuse skinfoldtenderness, increased reactive hyperemia, andwidespread decreased tissue compliance.
Although a significant difference was foundin Posture between healthy subjects and pa-tients, an ideal posture is uncommon also inhealthy subjects, and some degree of posturalabnormalities is often found (34,35). In an-other study with similar examination items,postural items having to do with spinal devia-tions in the sagittal plane did not differentiate
Kvåle, Skouen, and Ljunggren 33

between healthy persons and patients, whereaspostural items related to extremities did (36).Assessment of posture may be an importantcomponent in physical evaluation, especiallywhen composite scores from several items areused. Correlation between aberrations in pos-ture and psychological problems have alsobeen reported in patients with long-lasting wide-spread musculoskeletal pain (11).
One could ask whether the choice of eachcomponent in the GPE is relevant (3). The lackof discriminative information might be usedas an argument for omitting some of the sub-domains in future examinations of patientswith long-lasting musculoskeletal pain. Res-piration supine, Stretch palpation of muscle,and Pressure palpation of skin did not revealsignificant differences, neither between healthyand patients nor between groups of patients.Accordingly, these three subdomains could beomitted when the GPE is used to assess pa-tients with musculoskeletal pain. On the otherside, further studies regarding physical find-ings between or within groups, could providevaluable information, also within these sub-domains. Significant associations have beenreported between aberrations in Respirationsupine and psychological problems (11), whichmight be a valuable aspect to consider whenplanning treatment.
Classification of patients into more homo-geneous subgroups might permit better under-standing of the patients’ problems and moredifferentiated treatment (37). The pain draw-ing classification system used in this study canbe recommended in future studies, as distinctphysical findings were revealed for the threepatient groups. In accordance with former stud-ies, it seems that the more extensive the painis, the more aberrations there seems to be, bothphysically and psychologically (11,38). Itshould have consequence for choice of treat-ment that patients with widespread pain seemto have more physical and psychological prob-lems, and patients with localized pain less pro-nounced findings, and furthermore that pa-tients with pain localized to the upper versuslower body also show distinct physical char-acteristics. A thorough examination of physi-cal aberrations may result in better understand-ing and treatment. The GPE-52 seems to be auseful assessment instrument in patients with
long-lasting musculoskeletal pain problems,although further studies should be done in or-der to evaluate the responsiveness of the test-battery. The subjects included in this studywere considered representative for persons inNorway. It would, however, be of interest toexamine both patients and healthy subjectswith the GPE-52 in other settings, as little seemsto have been reported regarding how culturaldiversity may influence musculoskeletal find-ings, such as movement and palpable quali-ties.
REFERENCES
1. Rudy TE, Turk DC, Brena SF: Differential utilityof medical procedures in the assessment of chronic painpatients. Pain 34: 53-60, 1988.
2. Turk DC, Rudy TE: Towards a comprehensiveassessment of chronic pain patients. Behav Res Ther 25:237-49, 1987.
3. Refshauge KM, Gass EM: Musculoskeletal phys-iotherapy: clinical science and practice. Butterworth-Heinemann Ltd, Oxford, 1995.
4. Andersson HI, Ejlertsson G, Leden I, RosenbergC: Characteristics of subjects with chronic pain, in rela-tion to local and widespread pain report. A prospectivestudy of symptoms, clinical findings and blood tests insubgroups of a geographically defined population. ScandJ Rheumatol 25: 146-54, 1996.
5. Waddell G: The back pain revolution. ChurchillLivingstone, Edinburgh, 1998.
6. Simmonds MJ, Harding V, Watson PJ, ClaveauY: Physical therapy assessment: Expanding the model.In: Devor M, Rowbotham MC, Wiesenfeld-Hallin Z,eds. Proceedings of the 9th World Congress on Pain:Progress in pain research and management. IASP Press,Seattle, 2000, pp.1013-30.
7. Waddell G, Somerville D, Henderson I, NewtonM: Objective clinical evaluation of physical impairmentin chronic low back pain. Spine 17: 617-28, 1992.
8. Sundsvold MØ, Vaglum P, Denstad K: Globalfysioterapeutisk muskelundersøkelse. Private publish-ing company, Oslo, 1982.
9. Sundsvold MØ, Vaglum P: Muscular pains andpsychopathology: Evaluation by the GPM method. In:Michel TH, ed. International Perspectives in PhysicalTherapy. 1: Pain. Churchill Livingstone, London, 1985,pp. 18-47.
10. Bunkan BH, Thornquist E: Psychomotor ther-apy: An approach to the evaluation and treatment ofpsychosomatic disorders. In: Hegna T, Sveram M, eds.International perspectives in physical therapy. 5: Psy-chological and psychosomatic problems. ChurchillLivingstone, London, 1990, pp. 45-74.
34 JOURNAL OF MUSCULOSKELETAL PAIN

11. Kvåle A, Ellertsen B, Skouen JS: Relationshipsbetween physical findings (GPE-78) and psychologicalprofiles (MMPI-2) in patients with long-lasting muscu-loskeletal pain. Nord J Psychiatry 55: 177-84, 2001.
12. Kline RB: Principles and practice of structuralequation modeling. The Guilford Press, London, 1998.
13. Kvåle A, Johnsen TB, Ljunggren AE: Examina-tion of respiration in patients with long-lasting muscu-loskeletal pain: Reliability and validity. Adv Physiother4: 169-81, 2002.
14. Kvåle A, Johnsen TB, Ljunggren AE: Examina-tion of movement in patients with long-lasting muscu-loskeletal pain: Reliability and validity. PhysiotherapyResearch International 8: 36-52, 2003.
15. Kvåle A, Ljunggren AE, Johnsen TB: Palpationof muscle and skin. Is this a reliable and valid procedurein assessment of patients with long-lasting muscu-loskeletal pain? Adv Physiother 5: 2003.
16. Haldorsen EM, Kronholm K, Skouen JS, UrsinH: Multimodal cognitive behavioral treatment of pa-tients sicklisted for musculoskeletal pain: A randomizedcontrolled study. Scand J Rheumatol 27: 16-25, 1998.
17. Öhlund C, Eek C, Palmbald S, Areskoug B,Nachemson A: Quantified pain drawing in subacute lowback pain. Validation in a nonselected outpatient indus-trial sample. Spine 21: 1021-30, 1996.
18. Salén BA, Spangfort EV, Nygren AL, NordemarR: The Disability Rating Index: An instrument for theassessment of disability in clinical settings. J ClinEpidemiol 47: 1423-35, 1994.
19. Skouen JS, Vilsvik D, Ellertsen B: A new andsimple classification system of chronic low back painpatients. The International Society for the Study of theLumbar Spine, 24th Annual Meeting, 1997, pp. 108-9.
20. Sundsvold MØ: Global Fysioterapeutisk Mus-kelundersøkelse. Til bruk i klinisk arbeid og forskning.[Manual]. Sundsvold MØ, 1997.
21. Sundsvold MØ: Muscular tension and psycho-pathology. Psychother Psychosom 26: 219-28, 1975.
22. Sundsvold MØ, Vaglum P, Østberg B: Move-ments, lumbar and tempomandibular pain and psycho-pathology. Psychother Psychosom 35: 1-8, 1981.
23. Deyo RA, Diehr P, Patrick DL: Reproducibilityand responsiveness of health status measures–statisticsand strategies for evaluation. Controlled Clin Trials 12:142S-58S, 1991.
24. Battié MC: The reliability of physical factors aspredictors of the occurrence of back pain reports. Doc-toral Dissertation, Gothenburg University. 1989.
25. Sihvonen T, Partanen J, Hanninen O, SoimakallioS: Electric behavior of low back muscles during lumbar
pelvic rhythm in low back pain patients and healthy con-trols. Arch Phys Med Rehabil 72: 1080-7, 1991.
26. Sihvonen T, Lindgren KA, Airaksinen O, ManninenH: Movement disturbances of the lumbar spine and ab-normal back muscle electromyographic findings in re-current low back pain. Spine 22: 289-95, 1997.
27. Lowen A: Joy: The surrender to the body and tolife. Penguin/Arkana, New York, 1995.
28. Simons DG, Mense S: Understanding and mea-surement of muscle tone as related to clinical musclepain. Pain 75: 1-17, 1998.
29. Watson PJ, Booker CK, Main CJ: Evidence forthe role of psychological factors in abnormal paraspinalactivity in patients with chronic low back pain. J Mus-culoske Pain 5(4): 41-56, 1997.
30. Krogstad BS: Myofunctional and emotional as-pects of temporomandibular disorders. Doctoral Disser-tation, University of Oslo, 1998.
31. Ursin H: Sensitization, somatization, and subjec-tive health complaints. A review. International Journalof Behavioral Medicine 4: 105-16, 1997.
32. Wigers SH: Clinical studies of fibromyalgia withfocus on etiology, treatment and outcome. Doctoral Dis-sertation, Norwegian University of Science and Tech-nology, Trondheim, Norway, 1996.
33. Granges G, Littlejohn GO: A comparative studyof clinical signs in fibromyalgia/fibrositis syndrome,healthy and exercising subjects. J Rheumatol 20: 344-51,1993.
34. Griegel-Morris P, Larson K, Mueller-Klaus K,Oatis CA: Incidence of common postural abnormalitiesin the cervical, shoulder, and thoracic regions and theirassociation with pain in two age groups of healthy sub-jects. Phys Ther 72: 425-31, 1992.
35. Grimmer K: An investigation of poor cervicalresting posture. Australian Journal of Physiotherapy 43:7-16, 1997.
36. Friis S, Bunkan BH, Ljunggren AE, Moen O,Opjordsmoen S: What are the basic dimensions of bodyposture? An empirical evaluation of the ComprehensiveBody Examination. I. Nord J Psychiatry 52: 319-26,1998.
37. Kreitler S, Gohar H, Ezer T, Niv D: Pain charac-teristics and their psychosocial and clinical correlates.The Pain Clinic 11: 313-27, 1999.
38. Dworkin SF, Von Korff M, LeResche L: Multi-ple pains and psychiatric disturbance. An epidemiologicinvestigation. Arch Gen Psychiatry 47: 239-44, 1990.
Kvåle, Skouen, and Ljunggren 35





























