Embed Size (px)
Citation preview

Terms and Conditions for Use of PDF
The provision of PDFs for authors’ personal use is subject to the following Terms & Conditions:
The PDF provided is protected by copyright. All rights not specifically granted in these Terms & Conditions are expressly
reserved. Printing and storage is for scholarly research and educational and personal use. Any copyright or other notices or
disclaimers must not be removed, obscured or modified. The PDF may not be posted on an open-access website (including
personal and university sites).
The PDF may be used as follows:
� to make copies of the article for your own personal use, including for your own classroom teaching use (this includes posting
on a closed website for exclusive use by course students);
� to make copies and distribute copies (including through e-mail) of the article to research colleagues, for the personal use by
such colleagues (but not commercially or systematically, e.g. via an e-mail list or list serve);
� to present the article at a meeting or conference and to distribute copies of such paper or article to the delegates attending
the meeting;
� to include the article in full or in part in a thesis or dissertation (provided that this is not to be published commercially).
This material is the copyright of the original publisher.Unauthorised copying and distribution is prohibited.

This material is
the copyright of the
original publisher.
Unauthorised copying
and distribution
is prohibited.
Disease-Modifying Approach to theTreatment of Alzheimer’s DiseaseFrom a-Secretase Activators to c-Secretase Inhibitorsand Modulators
Francesco Panza,1 Vincenzo Solfrizzi,1 Vincenza Frisardi,1 Cristiano Capurso,2
Alessia D’Introno,1 Anna M. Colacicco,1 Gianluigi Vendemiale,2,3 Antonio Capurso1
and Bruno P. Imbimbo4
1 Department of Geriatrics, Center for Aging Brain, Memory Unit, University of Bari, Bari, Italy
2 Department of Geriatrics, University of Foggia, Foggia, Italy
3 Internal Medicine Unit, IRCSS Casa Sollievo dalla Sofferenza, San Giovanni Rotondo, Foggia, Italy
4 Research & Development Department, Chiesi Farmaceutici, Parma, Italy
Contents
Abstract. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5371. The ‘Amyloid Cascade Hypothesis’ . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5382. a-Secretase Activators. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 540
2.1 The a-Secretase Pathway . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5402.2 Different Classes of a-Secretase Activators . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 540
3. b-Secretase Inhibitors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5433.1 Peptidic b-Secretase Inhibitors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 544
4. g-Secretase Inhibitors and Modulators . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5454.1 g-Secretase Inhibitors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5454.2 g-Secretase Modulators . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 548
5. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 549
Abstract In the last decade, advances in understanding the neurobiology of Alz-heimer’s disease (AD) have translated into an increase in clinical trials assess-ing various potential AD treatments. At present, drugs used for the treatmentof AD only slightly delay the inevitable symptomatic progression of the dis-ease and do not affect the main neuropathological hallmarks of the disease,i.e. senile plaques and neurofibrillary tangles. Brain accumulation of oligo-meric species of b-amyloid (Ab) peptides, the principal components of senileplaques, is believed to play a crucial role in the development of AD. Based onthis hypothesis, huge efforts are being made to identify drugs able to interferewith proteases regulating Ab formation from amyloid precursor pro-tein (APP). Compounds that stimulate a-secretase, the enzyme responsiblefor non-amyloidogenic metabolism of APP, are being developed and one ofthese, EHT-0202, has recently commenced evaluation in a phase II study. Thediscovery of inhibitors of b-secretase (memapsin-2, b-amyloid cleaving en-zyme-1 [BACE-1]), the enzyme that regulates the first step of amyloidogenic
REVIEW ARTICLEDrugs Aging 2009; 26 (7): 537-5551170-229X/09/0007-0537/$49.95/0
ª 2009 Adis Data Information BV. All rights reserved.

This material is
the copyright of the
original publisher.
Unauthorised copying
and distribution
is prohibited.
APP metabolism, has proved to be particularly difficult because of inherentmedicinal chemistry issues and only one compound (CTS-21166) has pro-ceeded to clinical testing. Conversely, several compounds that inhibitg-secretase, the pivotal enzyme that generates Ab, have been identified, themost advanced being LY-450139 (semagacestat), presently in phase III clinicaldevelopment. There has been considerable disappointment over the failure ofa phase III study of tarenflurbil, a compound believed to modulate the ac-tivity of g-secretase, after encouraging phase II findings. Nevertheless, otherpromising g-secretase modulators are being developed and are approachingclinical testing. All these therapeutic approaches increase the hope of slowingthe rate of decline in patients with AD and modifying the natural history ofthis devastating disease within the next 5 years.
Alzheimer’s disease (AD) is an age-related pro-gressive neurodegenerative disorder with an en-ormous unmet medical need, characterized byrelatively slow chronic but progressive impairmentin cognition, behaviour and functionality. Thenumber of people with AD, which currently af-fects more than 26million people worldwide withan expected increase to more than 106million by2050,[1] is rising quickly because of the aging ofthe population and the fact that there are noeffective treatments for the disorder available. Atpresent, only cholinesterase inhibitors (ChEIs)and the NMDA-receptor antagonist memantinehave received US FDA approval for the symp-tomatic treatment of AD. In recent years, in aneffort to identify clinical targets of potential thera-peutic agents for AD, people with mild cognitiveimpairment (MCI) have been enrolled in trials ofdrugs that were effective in patients with AD.[2,3]
However, previous studies have shown that notallMCI subjects have predementiaAD.[4] Such pre-dementia syndromes have been defined for AD,but have not yet been operationalized for otherspecific forms of dementia.[4,5] Therefore, giventhat, at present, the predementia syndromes forvascular dementia, Lewy body dementia andfronto-temporal dementia are not well clinicallydefined, the clinical target for treatment of late-life cognitive disorders may be restricted to AD atvarious stages, particularly mild to moderate,and amnestic MCI, which is recognized as thepredementia syndrome of Alzheimer’s pathology.
Evidence from controlled clinical trials suggeststhat ChEIs in particular can stabilize patients’
symptoms for periods of time ranging between 1and 3 years but without modifying progression ofthe disease.[6] Indeed, despite many theoretical con-siderations suggesting that ChEIs or memantinemay have a disease-modifying effect, only symp-tomatic effects of these compounds have beenproven.[7] Individual ChEIs have additionalpharmacological effects besides inhibition ofacetylcholinesterase.[8,9] However, a clinical benefitfrom these additional effects has not been convinc-ingly shown.[10] A very recent large meta-analysisbased on 59 studies showed that both ChEIs andmemantine had consistent effects in the domainsof cognition and global assessment, but summaryestimates showed small effect sizes.[11] Finally,another meta-analysis of studies of ChEIs todetermine the impact of these drugs on MCI[12]
showed that use of ChEIs in MCI was not associ-ated with any delay in the onset of ADor dementia.Epidemiological studies yielding mainly cross-sectional data have suggested that NSAIDs,[13]
estrogens,[14] HMG-CoA reductase inhibitors(statins)[15] and tocopherol (vitamin E)[16] mayhelp reduce the incidence of AD. However, biasesin case selection and several other sources oferror are inherent in epidemiological studiesand subsequent clinical trials have often beendisappointing.
1. The ‘Amyloid Cascade Hypothesis’
In the last decade, advances in understandingthe neurobiology of AD have translated into anincrease in clinical trials assessing various potential
538 Panza et al.
ª 2009 Adis Data Information BV. All rights reserved. Drugs Aging 2009; 26 (7)

This material is
the copyright of the
original publisher.
Unauthorised copying
and distribution
is prohibited.
AD treatments. AD involves aberrant proteinprocessing and is characterized by the presence ofboth intraneuronal protein clusters composed ofpaired helical filaments of hyperphosphorylatedtau protein (neurofibrillary tangles) and extra-cellular protein aggregates (senile plaques [SPs]).Therefore, Alzheimer’s classic pathological descrip-tion of AD as a ‘two hallmarks disorder’[17] wasconfirmed by subsequent observations.[18] Theseneuropathological hallmarks of AD have stronglyinfluenced recent therapeutic approaches.[19]
The SPs are the result of misprocessing of theamyloid precursor protein (APP), a type-1 trans-membrane protein, by b- and g-secretases to forma toxic b-amyloid (Ab) peptide of 40- to 42-amino-acids that aggregates and initiates a pathogenicself-perpetuating cascade ultimately leading toneuronal loss and dementia (figure 1).[20] Extra-cellular, and perhaps also intracellular, Ab exertsneurotoxic effects.[21] Extracellular Ab peptidescluster in a b-sheet structure to form SPs. According
to the ‘amyloid cascade hypothesis’,[22] develop-ment of SPs is thought to precede and precipitatethe formation of neurofibrillary tangles as a resultof the cellular changes invoked, and the oligo-meric forms of Ab peptide are the main cause ofneuronal death in AD.
APP may be metabolically processed accord-ing to two pathways (figure 1). In the so-callednon-amyloidogenic pathway, the a-secretase en-zyme cleaves APP within the Ab sequence andreleases its transmembrane fragment soluble APPa-cleaved (sAPPa), which appears to exert neuro-protective activity. In the amyloidogenic path-way, the b-secretase enzyme releases APP plus a12-kDa protein fragment (C99), which in turn iscleaved by the g-secretase enzyme giving way toAb (figure 1). Accumulation of toxic, aggregatedforms of Ab seems to be crucial in the patho-genesis of familial forms of AD.[23] At the sametime, many studies have found a weak correlationbetween Ab deposits and cognitive status,[24] and
APP N
...NL−1
Plaque
sAPPα
p3
α-Secretase
γ-Secretase
C99β-Secretase
γ-SecretaseAβ
(1−40 and 1−42)
sAPPβ
C83
712−714
770C
γ -Sites
β-Site
α-Site
α
β
γ
672
687
671
α-Secretase pathway(non-amyloidogenic)
β-Secretase pathway
γ
β-Secretase α-Secretase γ-Secretase
↓ (Swedish mutation)
...KM−1↓D1 ↓ ↓ ↓AEFRHDSGY10↓EVHHQK16 LVFFAEDVGSNKGAIIGLMVGGVV40 IA42 TVIVITLVMLK...
a
b
Fig. 1. Schematic overview of amyloid precursor protein (APP) processing. The top panel shows the APP region comprising the trans-membrane sequence (underlined) and the sequences of b-amyloid (Ab)1–40 (D1–V40) and (Ab)1–42 (D1–A42) peptides. Numbers indicateamino acid positions. The b-secretase cleaves at D1 and Y10. The a-secretase cleaves at K16, and the g-secretase cleaves at V40 and/or A42.Below the sequence is a representation of APP showing the residue numbers of interest in b- and g-secretase cleavage. (a) represents thenon-amyloidogenic a-secretase pathway in which soluble APPa-cleaved (sAPPa) and C83 are generated. Subsequent hydrolysis by theg-secretase produces a p3 peptide that does not form amyloid deposits; and (b) represents the amyloidogenic pathway in which cleavage ofAPP by the b-secretase to liberate sAPPb and C99 is followed by g-secretase processing to release Ab peptides (Ab1–40 and Ab1–42) found inplaque deposits.
Secretase-Based Drugs in Alzheimer’s Disease 539
ª 2009 Adis Data Information BV. All rights reserved. Drugs Aging 2009; 26 (7)

This material is
the copyright of the
original publisher.
Unauthorised copying
and distribution
is prohibited.
some have shown that cognitively healthy elderlypeople can have substantial amyloid burden.[25,26]
In the present article, we briefly review theprofile of drugs that target the proteases involvedin both the non-amyloidogenic and amyloido-genic pathways of APP metabolism. In particular,we focus on a-secretase activators, b-secretaseinhibitors and g-secretase inhibitors and mod-ulators that have reached clinical testing. There-fore, we chose not to include active and passiveimmunization,[27] or other promising drugs forAD such as dimebon (dimebolin).[28] We reviewedstudies from the English-language literature pub-lished before December 2008. To this end, wesearched the PubMed database of the NationalCentre for Biotechnology Information (availableat http://www.ncbi.nlm.nih.gov) by author and thefollowing keywords: ‘drugs targeting b-amyloid’,‘a-activators’, ‘b-secretase inhibitors’, ‘g-secretaseinhibitors’, ‘g-secretase modulators’, ‘mild cogni-tive impairment’, ‘dementia syndromes’, ‘Alzhei-mer’s disease’ and ‘MCI’.
2. a-Secretase Activators
2.1 The a-Secretase Pathway
The a-secretase cleavage of APP occurs mainlyat the plasmamembrane, although part of it couldalso take place in intracellular compartmentsalong the secretory pathway in the trans-Golginetwork/late trans-Golgi or the endoplasmic re-ticulum.[29-31] a-Secretase cleaves APP at the ly-sine (Lys)16-leucine (Leu)17 bond within the Absequence, thus precluding the formation and de-position of Ab.[32] a-Secretase cleavage generatesan extracellular N-terminal fragment, termedsAPPa, and a C-terminal transmembrane frag-ment, called C83. sAPPa possesses potent neuro-protective[33] and memory-enhancing effects.[34]
An alternative to inhibition of the amyloidogenicenzymes to decrease brain Ab burden in AD pa-tients would be to activate the a-secretase process-ing of APP, although potentiating the a-cleavageis perceived to be more difficult than inhibitingb- and/or g-secretases. Although neurons containa certain level of basal a-secretase activity, pro-
teolysis by this enzyme can be increased phar-macologically using a variety of approaches.[29]
The identity of a-secretase has not been com-pletely elucidated. Several plasma membrane-associated or intracellular proteases have beenproposed as a-secretase candidates, e.g. cathepsinB, gelatinase A, plasmin, calpains or yapsin.[29]
Nonetheless, none of the above-cited candidatesentirely fulfill the main characteristics assignedto a-secretase. At present, it is known that theenzyme is a member of the a disintegrin andmetalloprotease (ADAM) family of proteases andmay be ADAM10, ADAM17/tumour necrosisfactor-a-converting enzyme (TACE)[35] or evenADAM9.[36] Structurally, ADAMs are type 1 inte-gral membrane proteins with both a disintegrindomain and a metalloprotease catalytic site.[37]
Recently, studies in transgenic animals havepointed toADAM10 as the putative a-secretase.[38]
Activation of a-secretase has regained interest asa therapeutic drug target in AD.[39] Overexpres-sion of ADAM10 in transgenic animals led to adecrease in amyloid pathology, while transgenicexpression of a catalytic inactive form of theenzyme resulted in an increase in amyloid patho-logy.[38] Activation of a-secretase may have thedouble advantage of not only precluding neuro-toxic Ab peptide formation but also generatingthe putatively neuroprotective sAPPa.[40]
2.2 Different Classes of a-Secretase Activators
The a-secretase pathway can be either con-stitutive or upregulated by protein kinase C(PKC) and multiple other agents able to bothreduce Ab production and trigger the release ofthe neuroprotective and memory enhancingsAPPa product.[29] One possible strategy may beto upregulate ADAM10 or ADAM17/TACEa-secretase gene expression. Another approachmay be to use statins, retinoids or neuropeptidessuch as pituitary adenylate cyclase-activatingpolypeptide to stimulate a-secretase or PKC ac-tivities.[19] The mechanisms underlying the ap-parent reduction in risk of AD in people takingstatins[15] are poorly understood, but one hypo-thesis is related to the ability of statins to increasesAPPa levels via a-secretase activation. Indeed,
540 Panza et al.
ª 2009 Adis Data Information BV. All rights reserved. Drugs Aging 2009; 26 (7)

This material is
the copyright of the
original publisher.
Unauthorised copying
and distribution
is prohibited.
in vitro studies have shown that lovastatin,[41]
atorvastatin,[42] simvastatin[43] and rosuvastatin[44]
stimulated sAPPa shedding from human celllines. The stimulating effects of simvastatin onsAPPa have been observed in the cerebrospinalfluid (CSF) ofADpatients after 1 year of treatmentwith 20mg/day but, unfortunately, this study wasuncontrolled.[45] Whether statins act by alteringthe distribution of APP and the various secretasesbetween raft and nonraft regions of the cell mem-branes or by altering the fluidity of the membraneis not clear. Alternatively, the expression of APPand secretases may be modified by statins.[32] Re-cently, it has also been proposed that the stimu-lating effects of statins on sAPPa are mediated, atleast in part, by modulation of the isoprenoidpathway and Rho-associated protein kinase 1.[43]
Furthermore, enhancement of a-secretase ac-tivity can be obtained by direct stimulation ofPKC or activation of receptors that work throughPKC. Indeed, activation of a-secretase is con-trolled by the protein phosphorylation signaltransduction pathway of PKC. Thus, phorbolesters are direct PKC activators and have beenshown to significantly enhance the secretion ofsAPPa in vitro,[46] to reduce Ab in vitro[47] andin vivo,[48] and to prevent Ab toxicity in rat hip-pocampal neurons.[49] Unfortunately, phorbolesters are tumour promoters and therefore arenot viable options for drug development. Thisissue was partially resolved with the design ofbenzolactam-based synthetic drugs, which havebeen shown to bind to PKC[50] and, when appliedat micromolar concentrations, are associatedwith increased sAPPa secretion in cells derivedfrom AD patients.[50,51]
A step forward in the search for potent andharmless PKC activators was made with the de-monstration that bryostatin 1, a macrolide lac-tone with promising anticancer activity isolatedfrom Bugula neritina, was able, at sub-nanomolarconcentrations, to promote sAPPa secretion infibroblasts from AD patients.[52] In addition,bryostatin 1 exhibited sub-nanomolar affinity forPKC[53] and intraperitoneal treatment of APPtransgenic mice with 1mg/kg of this compoundfor 17 weeks produced a significant increase inbrain sAPPa concentrations and a decrease in
brain Ab40 levels.[52] Prolonged intraperitonealtreatment with bryostatin 1 (40 g/kg three timesper week) in APP+ presenilin 1 (PS1) double trans-genic mice significantly reduced brain Ab42levels.[52] The Blanchette Rockefeller Neuro-sciences Institute in the US is sponsoring aphase II clinical trial of a single dose of bryo-statin 1 in patients with mild to moderate AD(single 1-hour intravenous infusion of 10 or 15mg/m2
of bryostatin 1); recruitment for this trial has notcommenced as yet (table I).[54] A number of neu-rotransmitters (glutamate, serotonin) and growthfactors (epidermal growth factor) also appearedto stimulate a-secretase via PKC activation.[32]
A physiological alternative for activation ofa-secretase could be to stimulate a-secretaseactivity via muscarinic receptors with selectivemuscarinic M1 receptor agonists or ChEIs, whichhave clearly demonstrated this capacity bothin vitro and in vivo.[55] Talsaclidine, a selective M1
receptor agonist, has been shown to reduce bothAb42 and Ab40 concentrations in the CSF of ADpatients in two 4-week, double-blind, placebo-controlled studies involving 24 and 40 subjects,respectively.[56,57] Lowering of total Ab levels inthe CSF of AD patients has also been describedfor the selective M1 receptor agonist AF102B.[58]
Furthermore, intra-peritoneal injection of M1
receptor-specific AF267B reduced Ab pathologyas well as cognitive deficits via selective activationof ADAM17/TACE.[59] Unfortunately, selectiveM1 receptor agonists have important cholinergic-mediated adverse effects, the most serious beingsyncope, which limit their clinical use.
Direct stimulation of ADAM9/10/17 activityand/or expression is a promising strategy for po-tentiating a-secretase processing of APP.[29]
Overexpression of the a-secretase ADAM10or activation of its promoter with retinoic acid(tretinoin) may achieve this objective.[55] Further-more, the green tea constituent epigallocatechin-3-gallate stimulates a-secretase cleavage of APPvia the maturation of pro-ADAM10 into its60 kDa active form.[60] In addition, the synapse-associated protein SAP97 drives ADAM10 to thepost-synaptic membrane by a direct interactionand, thereby, positively modulates sAPPa pro-duction.[61] None of these alternatives has
Secretase-Based Drugs in Alzheimer’s Disease 541
ª 2009 Adis Data Information BV. All rights reserved. Drugs Aging 2009; 26 (7)

This material is
the copyright of the
original publisher.
Unauthorised copying
and distribution
is prohibited.reached the clinic with the exception of muscari-nic receptor agonists, which have already beenextensively tested in AD patients. Other agentscan also increase non-amyloidogenic cleavage ofAPP, including 17-estradiol, bradykinin, copper,testosterone, insulin, calmodulin and Ginkgobiloba extracts.[32]
At present, most of the available a-secretaseactivators are drugs intended for other pharma-cological actions, and this lack of specificityrepresents their major limitation. However, pro-
mising preclinical results have been recentlydisclosed for EHT-0202. This a-secretase stimu-lator specifically regulates GABA-A receptorsand is also a phosphodiesterase type 4 inhibitor.In vitro studies have shown that EHT-0202 isneuroprotective against Ab toxicity in a GABA-A-dependent manner and its neuroprotectiveeffect is associated with sAPPa induction.[62]
Neuroprotective and procognitive effects ofEHT-0202 have been shown in several in vivoADand aging-related pharmacological models that
Table I. Potentially disease-modifying drugs in clinical testing for the treatment of Alzheimer’s disease (AD). Compounds are aimed at
interfering with the generation, deposition or clearance of b-amyloid (Ab)
Classes of
drugs
Compound
(company/institution)
Mechanisms of action Adverse effects Status
a-Secretase
activators
Bryostatin 1
(Blanchette
Rockefeller
Neurosciences
Institute)
Increase in brain sAPPaconcentrations and decrease
in brain Ab40 levels
Commonly reported adverse effects
include myalgia, fatigue, nausea,
headache, vomiting, anorexia,
anaemia and lymphopenia
Phase II clinical trial in progress
(ClinicalTrials.gov identifier:
NCT00606164)
EHT-0202 (ExonHit) Regulates GABA-A receptors
inducing amyloid precursor
protein production and
reducing Ab plaque formation;
also a PDE4 inhibitor
Well tolerated Phase II clinical trial in progress
(ClinicalTrials.gov identifier:
NCT00880412)
b-Secretase
inhibitors
CTS-21166,
ASP-1702
(CoMentis/Astellas)
Reduction in Ab concentrations No severe adverse effects reported Completed phase I clinical trial in
2008; phase II clinical trials are
planned (ClinicalTrials.gov
identifier: NCT00621010)
g-Secretase
inhibitors
LY-450139/semagacestat
(Eli-Lilly)
Reduction in Ab concentrations GI problems; goblet cell hyperplasia in
intestinal epithelium; changes in the
immune system with a decrease in
lymphocytes in the spleen and thymus;
hair colour changes; skin rashes;
transient period of Ab reduction may be
followed by elevated Ab
Completed phase II clinical trial
in 2007; phase III clinical trial in
progress (ClinicalTrials.gov
identifier: NCT00594568)
MK-0752 (Merck) Reduction in Ab1-40
concentrations in CSF of
healthy volunteers
Inhibits Notch cleavage. Significant
GI toxicity in humans
Completed phase I clinical trials
(ClinicalTrials.gov identifier:
NCT00803894)
E2012 (Eisai) Notch sparing Lenticular opacity in rats Completed phase I clinical trials
(conducted in Japan,
ClinicalTrials.gov identifier: not
available)
BMS-708163 (Bristol
Myers Squibb)
Notch sparing.
Reduction in Ab concentrations
in CSF of healthy volunteers
Well tolerated Started phase II clinical trials
(ClinicalTrials.gov identifier:
NCT00810147)
GSI-953/begacestat
(Wyeth)
No reduction of Ab1-40
concentrations in CSF of
healthy volunteers
Improves memory in a
transgenic mouse model of AD
Well tolerated Started phase II clinical trials
(ClinicalTrials.gov identifier:
NCT00479219)
CSF = cerebrospinal fluid; GI = gastrointestinal; PDE4 = phosphodiesterase type 4; sAPPa = soluble amyloid precursor protein a-cleaved.
542 Panza et al.
ª 2009 Adis Data Information BV. All rights reserved. Drugs Aging 2009; 26 (7)

This material is
the copyright of the
original publisher.
Unauthorised copying
and distribution
is prohibited.
included Ab intoxication, scopolamine-inducedamnesia and Barnes tests. In phase I clinicaltrials, the compound was shown to be orallybioavailable, well tolerated, not sedative or eme-tic, and devoid of adverse effects. A phase IIstudy in 35 AD patients is currently ongoing toevaluate the safety and tolerability of EHT-0202when administered orally for a 3-month periodin conjunction with a ChEI.[62] The trial is alsocollecting preliminary data on clinical efficacy,particularly in regard to effects on cognition andbehaviour (table I). Therefore, despite the dif-ficulties associated with the development ofa-secretase activators, the emergence of agentsable to promote this pathway opens up new areasof investigation and might hold promise in ADtherapy.
3. b-Secretase Inhibitors
b-Secretase or b-amyloid cleaving enzyme-1(BACE-1, memapsin-2, Asp-2) is an attractivetarget for the development of inhibitor drugs toprevent and treat AD. Indeed, the first step in theprocess of cleavage of membrane-bound APP isthe formation of sAPPb and C99 peptide byBACE-1 (figure 1).[63] In 1999, the cloning andidentification of b-secretase as a protease[64] in-vigorated research into both the protease and itsinhibitor drugs.[65] BACE-1 is a 501-amino-acidtype-1 integral membrane protein with aspar-tic residues at positions 93 and 289 that arethought to be responsible for proteolytic activity(figure 2).[63] There are strong reasons whyb-secretase is considered an interesting ther-apeutic target. Indeed, inhibition of this step mayeliminate the subsequent harmful steps in the
cascade of AD pathogenesis. Furthermore, inknockout animals, lack of BACE-1 abolishes Abgeneration in the absence of further abnormal-ities, suggesting that blockade of BACE-1 mayreduce progression of amyloid pathology withoutmajor adverse effects.[66] Importantly, however,some BACE-1 knockout mice exhibited hypo-myelination of peripheral nerves and aberrantaxonal segregation of small-diameter afferentfibres,[67] and these findings raise some concernabout the safety of inhibiting BACE-1 as a treat-ment for AD. Nevertheless, the fact that BACE-1knockout mice remain generally healthy makesBACE-1 a viable therapeutic target for inhibitionof Ab production in AD. b-Secretase cleaves theAPP substrate bearing the Swedish mutationmuch more efficiently than the wild-type APPsequence,[68] explaining the increased Ab releasein AD patients carrying this mutation (figure 1).Finally, b-secretase is an aspartic protease, forwhich the inhibition mechanism and design of‘transition-state mimetics’ is well known.[69] Forthese reasons, BACE-1 and its closely relatedhomologue, BACE-2 (memapsin-1, Asp-1), whichshares 79% sequence identity with BACE-1 andalso cleaves APP at the b-secretase site, havebecome important drug targets suggesting thelikelihood of patient safety with a b-secretase in-hibitor drug aimed at partial inhibition of theprotease activity.[65,70] The biological functionsof BACE-2 have yet to be clarified, although itis known that it also cleaves APP within the Abdomain.[70]
However, progression of b-secretase inhibitorsto clinical trials has been slow and the protease isgenerally thought to be a difficult target for drugdevelopment. Indeed, b-secretase inhibitors arenot easy to find because BACE-1 has a large
Signalpeptide
93 96 289 292
DSTGDTGSConserved active
site residues
Preprotein Catalytic domain TM C-tail COOH
1
H2N
22 46 460 477 501
Fig. 2. Schematic representation of the protein structure of human b-secretase, indicating the conserved active site residues. Numbersindicate amino acid positions. C-tail = cytoplasmic tail; DTGS and DSGT = aspartyl protease active sites; TM = transmembrane domain.
Secretase-Based Drugs in Alzheimer’s Disease 543
ª 2009 Adis Data Information BV. All rights reserved. Drugs Aging 2009; 26 (7)

This material is
the copyright of the
original publisher.
Unauthorised copying
and distribution
is prohibited.
catalytic side domain that may not avidly bindsmall molecules.[71] Successful precedents in thedrug development of other aspartic protease tar-gets, particularly renin andHIV protease, and theability to use structure-based design, in somewaysfacilitated the search for b-secretase inhibitors.[32]
However, despite similarities with other asparticproteases, there are also some key differences inthe BACE-1 active site. It is more open and lesshydrophobic than other aspartic proteases, sug-gesting that enzyme selectivity is indeed possiblewith a small-molecule inhibitor. Moreover, ab-secretase inhibitor drug needs to penetratethe brain-blood barrier (BBB), which is easierwith a small-molecule inhibitor. Unfortunately,tight binding of a transition-state mimetic ofb-secretase requires about six residues and itis, therefore, difficult to reduce the size of theinhibitors.[71]
3.1 Peptidic b-Secretase Inhibitors
Over the last 7 years, several peptide-basedb-secretase inhibitors have been described.[72] Theseinhibitors have been based on peptide-derivedstructures, which act as transition state mimeticsbased on the amino acid sequences at the cleavagesite of APP by BACE-1.[73-75] Descriptions ofnonpeptidic b-secretase inhibitors that have notutilized the transition state mimetic approach arescarce and these are disclosed primarily in patentapplications.[32] There have also been sporadicreports of naturally occurring noncompetitiveinhibitors, such as hispidin[76] and catechins,[77]
but their micromolar potency and poor specifi-city compared with other proteases limit theirpharmacological development as such.
The first-generation b-secretase inhibitorsOM99-1 and OM99-2, designed as transitionstate mimetics using b-secretase residue pre-ferences in eight subsites and a hydroxyethyleneisostere, were very potent, but they were essen-tially peptidic in nature and lacked drug-likecharacteristics.[73] Modification of OM99-2 re-sulted in the identification of smaller inhibitors(molecular weight in the range of low 700 Da)with maintained nanomolar potency.[74] Othermodifications of OM99-2 recently led to func-
tionalized 15- or 16-residue cycloamide-urethanederivatives.[78] Recently, the crystal structureof a potent 13-residue inhibitor called OM03-4,bound to b-secretase, revealed the existence ofthree other subsites (S5–S7) and the interactionof a tryptophan with the S6 subsite of theenzyme.[79] A b-secretase inhibitor designed topenetrate the BBB has been shown in proof-of-concept experiments to reduce both Ab40 andAb42 in the brain of transgenic AD miceTg2576.[80] Very recently, alternative therapeuticapproaches targeting b-secretase have been re-ported.[65] For example, a reduction in brainAb in AD mice as a result of BACE-1 im-munization, where antibodies of BACE-1 are theinhibitors, has been shown to improve cogni-tive performance in the animals,[81] therebysubstantiating the therapeutic target. Finally,regulation of the endocytosis of APP andb-secretase has been shown to be affected byapolipoprotein E (APOE) and is mediated byAPOE receptor 2 and adaptor protein X11.[82]
Compounds that weaken APOE interactionwith APOE receptor 2 in vivo may lead to a re-duction in Ab; however, at present, the meansto effectively modulate the activities of thesecomponents to achieve Ab reduction remain tobe discovered.[65]
In the last few years, the current generation ofb-secretase inhibitors has demonstrated that mostof the required drug properties can be designedinto a single inhibitor molecule.[71] By usingcrystal structure-based design cycles, significantadvances have been made in the development ofdrug-like b-secretase inhibitors sufficiently smallto penetrate cell membranes and the BBB, withhigh potency and selectivity for inhibition of Abproduction in vitro and in vivo.[71] The recentlydeveloped agent GRL-8234 has shown excellentenzyme inhibitory activity as well as cellular inhi-bitory potency in Chinese hamster ovary cells.[83]
GRL-8234 has also exhibited very impressive in vivoproperties. Intraperitoneal administration ofGRL-8234 to Tg2576 mice resulted in a 65%reduction of Ab40 production at 3 hours after asingle dose of 8mg/kg.[83] Therefore, b-secretaseinhibition appears to be another viable target forthe treatment of AD.[84]
544 Panza et al.
ª 2009 Adis Data Information BV. All rights reserved. Drugs Aging 2009; 26 (7)
This material is
the copyright of the
original publisher.
Unauthorised copying
and distribution
is prohibited.
The possibility that some b-secretase inhi-bitors may be drug candidates has been bolsteredby the recent announcement that the US bio-tech company CoMentis has been reported tohave completed a phase I study of its orallybioavailable small molecule CTS-21166 (ASP-1702), described by CoMentis as a highly potent,highly selective and efficacious brain-penetratingb-secretase inhibitor.[85] The phase I trial in healthyvolunteers was designed as a dose-escalation studyto assess the safety, tolerability, pharmacokineticsand pharmacodynamics of CTS-21166 followingintravenous administration. Forty-eight subjectsreceived one of six different doses or placebo. Thestudy measured levels of CTS-21166 and levels ofplasma Ab. Single-dose administration of CTS-21166 produced a greater than 60% reductionin plasma Ab measured either by the area underthe plasma concentration-time curve (AUC) over24 hours or the maximal reduction relative topredose levels. The highest doses of CTS-21166further demonstrated a sustained reduction inAUC that exceeded 40% over 72 hours. Because ofthe urgent need for AD treatment, phase II stu-dies for CTS-21166 are planned for AD patients(table I).[85,86] Given the significant overall pro-gress in the knowledge base for b-secretase in-hibitors, it is likely that many other compoundswith appropriate efficacy and safety profiles willbe brought to the clinical stage soon.
4. c-Secretase Inhibitors and Modulators
4.1 c-Secretase Inhibitors
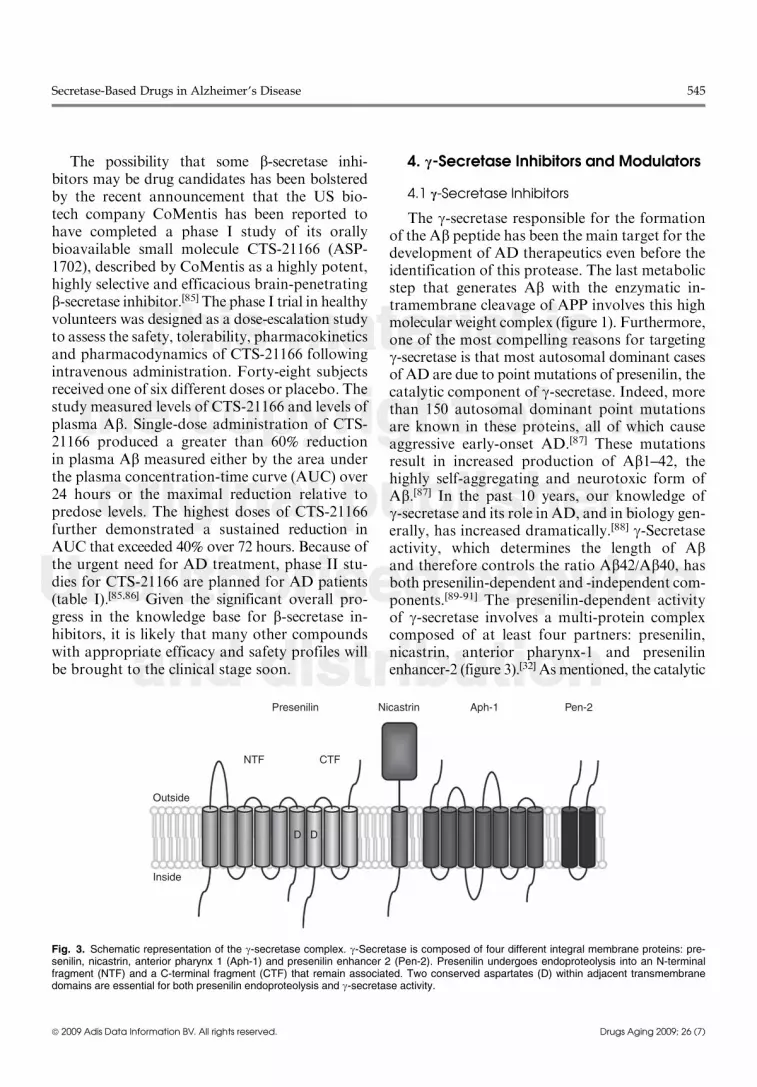
The g-secretase responsible for the formationof the Ab peptide has been the main target for thedevelopment of AD therapeutics even before theidentification of this protease. The last metabolicstep that generates Ab with the enzymatic in-tramembrane cleavage of APP involves this highmolecular weight complex (figure 1). Furthermore,one of the most compelling reasons for targetingg-secretase is that most autosomal dominant casesof AD are due to point mutations of presenilin, thecatalytic component of g-secretase. Indeed, morethan 150 autosomal dominant point mutationsare known in these proteins, all of which causeaggressive early-onset AD.[87] These mutationsresult in increased production of Ab1–42, thehighly self-aggregating and neurotoxic form ofAb.[87] In the past 10 years, our knowledge ofg-secretase and its role in AD, and in biology gen-erally, has increased dramatically.[88] g-Secretaseactivity, which determines the length of Aband therefore controls the ratio Ab42/Ab40, hasboth presenilin-dependent and -independent com-ponents.[89-91] The presenilin-dependent activityof g-secretase involves a multi-protein complexcomposed of at least four partners: presenilin,nicastrin, anterior pharynx-1 and presenilinenhancer-2 (figure 3).[32] As mentioned, the catalytic
Outside
NTF
D D
CTF
Presenilin Nicastrin Aph-1 Pen-2
Inside
Fig. 3. Schematic representation of the g-secretase complex. g-Secretase is composed of four different integral membrane proteins: pre-senilin, nicastrin, anterior pharynx 1 (Aph-1) and presenilin enhancer 2 (Pen-2). Presenilin undergoes endoproteolysis into an N-terminalfragment (NTF) and a C-terminal fragment (CTF) that remain associated. Two conserved aspartates (D) within adjacent transmembranedomains are essential for both presenilin endoproteolysis and g-secretase activity.
Secretase-Based Drugs in Alzheimer’s Disease 545
ª 2009 Adis Data Information BV. All rights reserved. Drugs Aging 2009; 26 (7)

This material is
the copyright of the
original publisher.
Unauthorised copying
and distribution
is prohibited.
component of the g-secretase complex is pre-senilin, with two aspartate residues forming theactive site. Inhibition of the catalytic unit of the g-secretase enzymatic complex appears a logicalstrategy for reducing Ab accumulation in pa-tients with AD.[92]
In 2001, the first in vivo testing of a g-secretaseinhibitor, the dipeptidic compoundDAPT (N-[N-(3,5-difluorophenacetyl)-L-alanyl]-S-phenylglycinet-butyl ester), developed by Elan and Eli Lilly,was reported.[93] Several other nonpeptidic, orallyavailable, g-secretase inhibitors have been syn-thesized.[94] Historically, the first g-secretaseinhibitor to reach clinical development appearsto be BMS-299897, a sulfonamide derivativesynthesized at Bristol-Myers Squibb and theformer SIBIA Neurosciences.[87] Human testingof BMS-299897 started in 2001, but clinicaldata have never been fully described. The con-tinuing lack of information on its clinical devel-opment may indicate that this agent has beenabandoned.[87] The benzodiazepine analogueLY-411575 and the benzolactam LY-450139 (se-magacestat), developed at Eli Lilly, are highlypotent g-secretase inhibitors that have been tes-ted extensively in vivo.[95,96] LY-450139 is themost well documented g-secretase inhibitorthat has reached clinical testing and for whichclinical studies have been fully published(table I).[96] At least five other g-secretase in-hibitors have progressed to clinical studies,and most of the information on these othercompounds derives from meeting abstracts:MK-0752,[97] E2012,[87] BMS-708163,[98] PF-3084014 (abandoned)[99] and GSI-953 (begace-stat)[100] [table I].
Although g-secretase has in many ways been anattractive target for AD therapeutics, g-secretaseinhibition may have safety drawbacks. Pre-senilin knockout in mice resulted in an early em-bryonal lethality with the phenotype presentingskeletal and CNS defects similar to those ofa Notch knockout.[101] Indeed, g-secretase in-hibitors block proteolysis of Notch-1, a parti-cular g-secretase substrate, by inhibiting cleavageat site 3 of the Notch receptor.[102] Physiologicalcleavage of Notch leads to release of the Notchintracellular domain, a protein fragment that is
translocated to the nucleus where it regulatestranscription of target genes involved in celldevelopment and the differentiation of adultself-renewing cells. Inhibition of Notch cleavagehas been associated with goblet cell hyperplasiain intestinal epithelium and changes in the im-mune system with a decrease in lymphocytes inthe spleen and thymus.[103,104] Recently, haircolour changes in animals have also been linkedto inhibition of Notch processing.[105] Use ofa Notch-related toxicity biomarker such as adip-sin may be useful for early detection of potentialtoxicity.[106]
LY-450139 is only 3-fold more selectivein inhibiting APP than Notch cleavage (APPconcentration that produces 50% inhibition[IC50] = 15 nmol/L, Notch concentration thatproduces a 50% effective response [EC50] = 49nmol/L).[96] In experimental animals, the effectsof LY-450139 on Ab levels in brain, CSF andplasma have been well characterized in transgenicmice,[107] non-transgenic mice,[108] guinea pigs[109]
and dogs.[110] However, the drug failed to showa statistically significant effect on brain plaquedeposition in long-term studies in transgenic miceexpressing mutated human APPV717F (PDAPP[platelet-derived growth factor promoter expres-sing APP] mice).[111] More importantly, no dataare available on the cognitive or behavioural ef-fects of the drug in animal models of AD.
In a phase I study, LY-450139 was adminis-tered to healthy men and women aged ‡45 yearsfor up to 14 days at doses of 5, 20, 40 and 50mgonce daily.[112] Two subjects in the 50-mg dosegroup developed possibly drug-related adverseevents (significant increases in serum amylase andlipase with moderate abdominal pain and diar-rhoea positive for occult blood) and discontinuedtreatment. The 50-mg dose caused a maximal40% reduction in total plasma Ab that returnedto baseline within 8 hours. However, after re-turning to baseline, plasma Ab levels increased toabout 300% of baseline values at 15 hours beforeslowly declining again. At lower doses, smallerand shorter decreases in plasmaAbwere observed,although the subsequent plasma Ab increaseswere similar. No significant changes in CSF Ablevels were detected.[112]
546 Panza et al.
ª 2009 Adis Data Information BV. All rights reserved. Drugs Aging 2009; 26 (7)

This material is
the copyright of the
original publisher.
Unauthorised copying
and distribution
is prohibited.
A second phase I study evaluated the safetyand tolerability and biomarker responses to sin-gle oral doses of LY-450139 60, 100 or 140mg in31 healthy male and female volunteers (aged ‡40years).[113] No clinically significant adverse eventsor laboratory changes were observed in thisstudy. However, many more data need to be ob-tained from human studies to establish the dif-ference between well tolerated and toxic doses ofg-secretase inhibitors in long-term treatment ofAD patients. Peak drug plasma concentrationsoccurred at 1 hour and then declined with a half-life of 2.5 hours.[113] A dose-dependent decreasein plasma Ab1–40 levels was also demonstratedwith maximum inhibition (-73%) at 6 hoursafter the administration of the 140-mg dose.A rebound effect on plasma Ab1–40 levels wasobserved at 8–12 hours after administration andthis persisted for at least 24 hours. CSF con-centrations of Ab were unchanged 4 hours afterdrug administration.[113] It is unknown if thebiphasic response of plasma Ab to LY-450139with a transient period of reduced Ab followed bya period of elevated Ab may induce a clinicalbenefit in AD patients.
LY-450139 has also been evaluated in AD pa-tients. In a randomized, placebo-controlled trial,70 patients received the drug for 6 weeks (30mgonce a day for 1 week followed by 40mg once aday for 5 weeks).[114] Six patients taking the drugreported diarrhoea and a 76-year-old man hadgastrointestinal bleeding associated with a Bar-rett’s oesophagus. Approximately 4 months afterdiscontinuing treatment, this patient developedendocarditis and died approximately 1 monththereafter. In the LY-450139-treated group, cir-culating CD69, T lymphocytes, eosinophils andserum concentrations of potassium and inorganicphosphorus showed statistically significant chan-ges. Plasma Ab1–40 concentrations of patients tak-ing the compound decreased significantly by 38%compared with baseline. Ab1–40 concentrationsin CSF did not decrease significantly.
Another phase II study evaluated the safety,tolerability and Ab response to LY-450139.[115]
Fifty-one individuals with mild to moderate ADwere randomized to receive placebo (n = 15) orLY-450139 (100mg [n = 22] or 140mg [n = 14]) for
14 weeks; 43 patients completed the treatmentphase. Patients randomized to LY-450139 received60mg/day for 2 weeks, followed by 100mg/dayfor 6 weeks, and then either 100 or 140mg/day for6 additional weeks. There were seven cases of skinrashes and three reports of hair colour change inthe drug treatment groups. There were also threeadverse event-related discontinuations, includingone transient bowel obstruction. Compared withplacebo, Ab1–40 plasma concentrations were re-duced by 58% in the 100-mg group and 65% in the140-mg group. No significant reduction in CSFAb levels was seen. No differences were seen incognitive or functional measures between placebo-and LY-450139-treated patients. No data werereported on the effects of LY-450139 on Ab1–42levels.[115]
Recently, the results of a study of the effectsof LY-450139 on Ab synthesis and clearance inthe CSF of AD patients were reported.[116] CSFwas collected hourly with a lumbar catheter.Fractional synthesis and clearance rates of CSFAb showed a significant inhibitory effect ofLY-450139 on newly synthesized Ab at dosesof 140 and 280mg. The maximum decrease inCSF Ab concentrations was seen 9 hours afterdrug administration.[116] The disconnection be-tween the timing of the peak inhibitory effectsof LY-450139 on CSF Ab levels (9 hours) andmaximum drug concentrations in CSF (4 hours)illustrates the complexity of the pharmacokinetic-pharmacodynamic relationship and need forprolonged CSF sampling to determine the effectsof g-secretase inhibitor on central Ab levels.
In April 2008, Eli Lilly initiated its firstphase III randomized, double-blind, placebo-controlled clinical trial of LY-450139 in patientswith mild to moderate AD, the IDENTITY (In-terrupting Alzheimer’s Dementia by EvaluatiNgTreatment of AmyloId PaThologY) trial.[87] Thetrial is to be conducted in the US and 21 addi-tional countries, with an enrolment goal of 1500AD patients for 21 months. An open-labelextension will be available to all participantscompleting the study. Patients who are takingcurrently available symptomatic drugs for ADwill be permitted to continue such treatments forthe duration of the study. The study incorporates
Secretase-Based Drugs in Alzheimer’s Disease 547
ª 2009 Adis Data Information BV. All rights reserved. Drugs Aging 2009; 26 (7)

This material is
the copyright of the
original publisher.
Unauthorised copying
and distribution
is prohibited.
a ‘randomized delayed start’ design with subjectsinitially assigned to the placebo arm and latertreated with LY-450139 to evaluate whether thedrug has effects on disease progression. Bothstudy subjects and investigators will be blinded tothe exact timing of this delayed start of studydrug administration.[87] g-Secretase inhibitorsmay represent the most advanced pharmacolo-gical class that provides opportunities to test theAb hypothesis of AD and modify the naturalhistory of the disease. Positive findings from theIDENTITY trial could confirm this hope.
4.2 g-Secretase Modulators
While a number of highly potent g-secretaseinhibitors have been identified and g-secretasehas in many ways been an attractive target forAD therapeutics, interference with Notch pro-cessing and signalling may lead to toxicities thatmay preclude the clinical use of inhibitors of thisprotease.[117] The ability to selectively block APPproteolysis by g-secretase without affecting pro-teolysis of Notch is a major goal to be achieved inefforts to identify safe and effective therapeuticsforAD. This could be realized bymodulating ratherthan inhibiting g-secretase. g-Secretasemodulationwas first observed in 2001 with certain NSAIDsthat were capable of altering the cleavage prop-erties of g-secretase to lower the production ofAb42, both in cultured cells and in transgenicmouse models, and increase the formation of ashorter 38-residue species (Ab38);[118,119] theseNSAIDs include ibuprofen, sulindac sulfide, indo-metacin and flurbiprofen. The ability of theseNSAIDs to modulate Ab production is not re-lated to their inhibition of cyclo-oxygenase.Binding of these NSAIDs to APP is more effi-cient than to Notch and, thus, their effects onNotch processing are minor.[120] These NSAIDsdo not reduce Ab production very potently andstructural modifications to these molecules havebeen proposed.[121] In transgenic mouse modelsof CNS amyloid deposition, treatment with theseagents significantly reduced amyloid accumula-tion.[122] Unfortunately, in humans, the toxicityof high doses of such NSAIDs limits the feasi-bility of this approach.
However, the g-secretase modulator taren-flurbil (MPC-7869; former non-proprietary nameR-flurbiprofen, Flurizan�) reduced brain con-centrations of Ab1–42 in a mouse model of AD,and long-term dosing of this agent in this modelprevented defects in learning and memory.[122,123]
Treatment with tarenflurbil 200, 400 or 800mgtwice daily for 3 weeks was well tolerated inhealthy elderly volunteers but did not sig-nificantly modify Ab1–40 or Ab1–42 levels inplasma or CSF.[124] A phase II trial of tarenflurbilwas designed to show slowing of cognitive andfunctional decline in mild to moderate AD; 210patients were enrolled in this 1-year trial.[125] Aseparate analysis with patients grouped accord-ing to whether they had mild or moderate cogni-tive impairment at baseline showed a favourableeffect of treatment on activities of daily living(Alzheimer’s Disease Cooperative Study Activ-ities of Daily Living scale, ADCS-ADL) andglobal function (Clinical Dementia RatingSum of Boxes, CDR-SB) in the subgroup of pa-tients with mild AD.[126] The results of a 12-monthblinded extension to the trial suggested long-term tolerability, and perhaps efficacy, of taren-flurbil 800mg twice daily in patients with mildAD.[125]
However, after these encouraging results, alarge phase III study of 18 months’ duration in1684 mildly affected AD patients yielded com-pletely negative results.[127] The reasons for thismajor failure are unclear but preclinical studieshave shown that tarenflurbil has low potency ininhibiting the secretion of Ab1-42 in vitro andpoor CNS penetration in rodents with inade-quate brain concentrations achieved in vivo.[125,128]
The promising pharmacological results obtainedwith tarenflurbil by the Mayo Clinic group(owner of the patent) after short-term adminis-tration in transgenic mice[122] have never beenconfirmed by other groups.[128] The neuropatho-logical and behavioural effects of tarenflurbilafter long-term administration in the transgenicmouse are inconsistent and questionable froma methodological point of view.[123] From aclinical point of view, an accurate examinationof the results of the phase II study[125] revealthat the apparent positive effects of the drug
548 Panza et al.
ª 2009 Adis Data Information BV. All rights reserved. Drugs Aging 2009; 26 (7)

This material is
the copyright of the
original publisher.
Unauthorised copying
and distribution
is prohibited.
in mildly affected patients at a dosage of 800mgtwice daily on theADCS-ADL andCDR-SB scaleswere likely due to an anomalous deteriorationrate observed in patients treated with placebo,rather than to the drug itself.[128] Interestingly,no significant effects of tarenflurbil were observedon the cognitive measure Alzheimer’s DiseaseAssessment Scale – Cognitive Subscale (ADAS-Cog), which showed consistent mean decreasesfor patients with mild and moderate AD whoreceived placebo. Accordingly, there were noeffects at all of tarenflurbil on Mini-MentalStage Examination (MMSE), another measureof cognition.
Other promising g-secretase modulators arebeing developed and have reached or are approa-ching clinical testing. E2012 is a diarylcinnamidederivative for which the exact structure has notbeen disclosed.[129] This compound has beenclaimed to lower Ab by modulating g-secretasewithout interfering with Notch processing. E2012was developed by Eisai in a partnership withTorreyPines Therapeutics. In mid 2006, thecompound entered phase I clinical development;in February 2007, a 13-week preclinical safetystudy in rats was put on hold because lenticularopacity was observed in a high-dose group. Atthe time the study was suspended, no medicalconcerns were reported. Lenticular opacity wasnot observed in a subsequent 13-week safetystudy in monkeys. An additional 13-week multi-ple dosing study in rats also did not reveal oculartoxicity and the clinical hold on E2012 was liftedin April 2008. The drug is now moving again to-ward phase I clinical trials.
Merck is developing a g-secretase modulator(GSM-1). In Tg2576 mice, this compound dose-dependently reduced brain Ab42 levels (maximumreduction of 69% with 30mg/kg). No significanteffects on brain Ab40 were observed while Ab38levels increased dose-dependently, as would beexpected for a g-secretase modulator.[130] Inrhesus monkeys, GSM-1 was shown to dose-dependently decrease Ab42 levels in CSF, leavingunmodified Ab40 levels in plasma and CSF.[131]
Unfortunately, the effects of the drug on plasmaAb42 were not described. It is not clear if GSM-1is progressing to human testing.
Chiesi is also developing a promising g-secretasemodulator (CHF5074).[132] In human neuro-glioma cells over-expressing the Swedish mutatedAPP (H4swe), CHF5074 preferentially loweredAb42 secretion with an IC50 of 3.6 mmol/L.[133] At5 mmol/L, no effects on Notch intracellular clea-vage in human embryonic kidney 293swe cellswere observed. At 100mmol/L, CHF5074 does notalter the expression profile of several Notchintracellular domain-responsive genes.[134] In rats,CHF5074 is well absorbed after oral administra-tion (50%) and is slowly eliminated from plasma(half life » 20 hours).[135] In transgenic mice ex-pressing the human Swedish APP mutation,long-term treatment with CHF5074 markedlyreduces brain Ab burden without histologicalsigns of peripheral Notch-mediated toxicity.[133]
Long-term treatment with CHF5074 in an ag-gressive transgenic mouse model of AD (humanAPP [hAPP] mice) attenuated brain Ab patho-logy and associated behavioural deficit in theseanimals.[136] CHF5074 drug is approaching clin-ical testing.
5. Conclusions
Drugs currently used in the treatment of pa-tients with AD have a very limited therapeuticeffect on both cognitive symptoms and psychia-tric and behavioural disturbances. Un-fortunately, these drugs do not interfere with thepathophysiological mechanisms of the disease.The ‘amyloid cascade hypothesis’ of AD hasdriven most of the drug discovery efforts in thelast 15 years. Hundreds of compounds have beengenerated with different ways of targeting Ab;however, unfortunately, until now they have notbeen clinically successful with major initiativesinvolving Ab aggregation inhibitors (tramipro-sate) and immunologically mediated Ab clearanceenhancers (pre-aggregated Ab1-42 [AN1792]).
Manipulation of the enzymes responsible forthe generation of Ab (a-, b- and g-secretase) hasbeen aggressively pursued and several compoundshave reached clinical testing. A weak, poorlybrain-penetrant, g-secretase modulator inhibitor(tarenflurbil) has recently experienced a majorsetback in the largest ever controlled clinical trial
Secretase-Based Drugs in Alzheimer’s Disease 549
ª 2009 Adis Data Information BV. All rights reserved. Drugs Aging 2009; 26 (7)

This material is
the copyright of the
original publisher.
Unauthorised copying
and distribution
is prohibited.
in AD patients. These negative results raise thepossibility that targeting Ab may not be clinicallyefficacious in AD patients, given the suggestedalternative non-pathogenic roles of Ab.[137,138]
Indeed, the hypothesis that Ab is the key patho-logical factor affecting the disease process hasbeen strongly questioned by a recently publishedpaper showing that although immunization withAN1792 resulted in almost complete clearance ofSPs from the brain of patients with AD, thisplaque removal did not prevent progressive neu-rodegeneration.[139] Ab may play a physiologicalrole in modulating synaptic plasticity[140] andhippocampal neurogenesis.[141] Ab deposition couldsimply represent a host response to an upstreampathophysiological process[24] or serve a protectivefunction,[142] probably as an antioxidant/metalchelator.[143,144] Nevertheless, the fight againstAb is continuing with more effective compounds.
The way forward appears likely to be pro-tracted when we consider that 20 years elapsedfollowing generation of the cholinergic hypoth-esis in 1976[145] before the effective and safe cho-linergic agent donepezil could be developed.[146]
The ‘amyloid cascade hypothesis’ was initiallyproposed in 1991[22] and we may similarly need towait until 2011 to obtain an effective and safeanti-Ab agent. The issue is further complicatedby the fact that Ab-interfering therapies are con-sidered by definition ‘disease-modifying’ drugsand need much longer clinical trials comparedwith ‘symptomatic drugs’ such as ChEIs or mem-antine. However, accurate evaluation of theeffects of the most promising drugs on biomarkerlevels (Ab40 and Ab42) in plasma and in CSFduring the early clinical development phases mayguide rational selection of the doses to be tested inlarge, long-term, phase III studies. One g-secre-tase inhibitor (LY-450139) has been adequatelycharacterized with respect to its pharmaco-dynamic features in initial phase I and II studiesand now is in phase III clinical testing. We willknow if LY-450139 is effective within the nextcouple of years. b-Secretase inhibitors anda-secretase activators are at early stages of clinicaldevelopment and they need 3–5 years to be fullytested. The hope for an effective therapy of thisdevastating disease is still alive.
Acknowledgements
This work was supported by the Italian LongitudinalStudy on Aging (ILSA) [Italian National Research Council-CNR-Targeted Project on Ageing –Grants 9400419PF40 and95973PF40]. The funding agencies had no role in the design orconduct of the review. The authors have no conflicts of in-terest that are directly relevant to the content of this review.
References1. Brookmeyer R, Johnson E, Ziegler-Graham K, et al.
Forecasting the global burden of Alzheimer’s disease.Alzheimer’s Dement 2008 Sep; 4 (5): 316-23
2. Visser PJ, Scheltens P, Verhey FR. DoMCI criteria in drugtrials accurately identify subjects with predementia Alz-heimer’s disease? J Neurol Neurosurg Psychiatry 2005Oct; 76 (10): 1348-54
3. Aisen PS. Treatment for MCI: is the evidence sufficient?Neurology 2008 May 27; 70 (22): 2020-1
4. Panza F, D’Introno A, Colacicco AM, et al. Current epi-demiology of mild cognitive impairment and other pre-dementia syndromes. Am J Geriatr Psychiatry 2005 Aug;13 (8): 633-44
5. Panza F, D’Introno A, Colacicco AM, et al. Cognitivefrailty: predementia syndrome and vascular risk factors.Neurobiol Aging 2006 Jul; 27 (7): 933-40
6. Giacobini E. Cholinesterase in human brain: the effectof cholinesterase inhibitors on Alzheimer’s disease andrelated disorders. In: Giacobini E, Pepeu G, editors.The brain cholinergic system in health and disease. Oxon:Informa Healthcare, 2006: 235-64
7. Hull M, Berger M, Heneka M. Disease-modifying thera-pies in Alzheimer’s disease: how far have we come? Drugs2006; 66 (16): 2075-93
8. Maelicke A, Samochocki M, Jostock R, et al. Allostericsensitization of nicotinic receptors by galantamine, a newtreatment strategy for Alzheimer’s disease. Biol Psy-chiatry 2001 Feb 1; 49 (3): 279-88
9. Greig NH, Utsuki T, Yu Q, et al. A new therapeutic targetin Alzheimer’s disease treatment: attention to butyr-ylcholinesterase. Curr Med Res Opin 2001; 17 (3): 159-65
10. Wilkinson DG, Francis PT, Schwam E, et al. Cholinester-ase inhibitors used in the treatment of Alzheimer’s disease:the relationship between pharmacological effects andclinical efficacy. Drugs Aging 2004; 21 (7): 453-78
11. Raina P, Santaguida P, Ismaila A, et al. Effectiveness ofcholinesterase inhibitors and memantine for treatingdementia: evidence review for a clinical practice guideline.Ann Intern Med 2008 Mar 4; 148 (5): 379-97
12. Raschetti R, Albanese E, Vanacore N, et al. Cholinesteraseinhibitors in mild cognitive impairment: a systematic re-view of randomised trials. PLoSMed 2007 Nov 27; 4 (11):e338
13. Imbimbo BP. The potential role of non-steroidal anti-inflammatory drugs in treating Alzheimer’s disease. Ex-pert Opin Investig Drugs 2004 Nov; 13 (11): 1469-81
14. Henderson VW. Estrogen-containing hormone therapyand Alzheimer’s disease risk: understanding discrepant
550 Panza et al.
ª 2009 Adis Data Information BV. All rights reserved. Drugs Aging 2009; 26 (7)

This material is
the copyright of the
original publisher.
Unauthorised copying
and distribution
is prohibited.
inferences from observational and experimental research.Neuroscience 2006; 138 (3): 1031-9
15. Panza F, D’Introno A, Colacicco AM, et al. Lipid meta-bolism in cognitive decline and dementia. Brain Res Rev2006 Aug; 51 (2): 275-92
16. Salerno-Kennedy R, Cashman KD. Relationship betweendementia and nutrition-related factors and disorders: anoverview. Int J Vitam Nutr Res 2005 Mar; 75 (2): 83-95
17. Alzheimer A. Uber eine eigenartige Erkrankung der Hirn-rinde. Allg Zeitschrift Psych 1907; 64: 146-8
18. Terry RD. Alzheimer’s disease at mid century (1927–1977).In: Jucker M, Beyreuther K, Haas C, et al., editors. Alz-heimer: 100 years and beyond. Berlin: Springer-Verlag,2006: 58-61
19. Giacobini E, Becker RE. One hundred years after the dis-covery of Alzheimer’s disease: a turning point for therapy?J Alzheimers Dis 2007 Aug; 12 (1): 37-52
20. Walter J, Kaether C, Steiner H, et al. The cell biology ofAlzheimer’s disease: uncovering the secrets of secretases.Curr Opin Neurobiol 2001 Oct; 11 (5): 585-90
21. Ohyagi Y, Asahara H, Chui DH, et al. Intracellular abe-ta42 activates p53 promoter: a pathway to neurodegen-eration in Alzheimer’s disease. FASEB J 2005 Feb; 19 (2):255-7
22. Hardy J, Allsop D. Amyloid deposition as the central eventin the aetiology of Alzheimer’s disease. Trends PharmacolSci 1991 Oct; 12 (10): 383-8
23. Hardy J, Selkoe DJ. The amyloid hypothesis of Alzhei-mer’s disease: progress and problems on the road totherapeutics. Science 2002 Jul 19; 297 (5580): 353-6
24. Castellani RJ, Lee HG, Zhu X, et al. Alzheimer diseasepathology as a host response. J Neuropathol Exp Neurol2008 Jun; 67 (6): 523-31
25. Crystal HA, DicksonDW, SliwinskiMJ, et al. Pathologicalmarkers associated with normal aging and dementia in theelderly. Ann Neurol 1993 Oct; 34 (4): 566-73
26. Knopman DS, Parisi JE, Salviati A, et al. Neuropathologyof cognitively normal elderly. J Neuropathol Exp Neurol2003 Nov; 62 (11): 1087-95
27. Wisniewski T,KonietzkoU.Amyloid-beta immunisation forAlzheimer’s disease. Lancet Neurol 2008 Sep; 7 (9): 805-11
28. Doody RS, Gavrilova SI, Sano M, et al., Dimebon In-vestigators. Effect of dimebon on cognition, activities ofdaily living, behaviour, and global function in patientswith mild-to-moderate Alzheimer’s disease: a random-ised, double-blind, placebo-controlled study. Lancet2008 Jul; 372 (9634): 207-15
29. Vincent B, Cisse MA, Sunyach C, et al. Regulation of be-taAPP and PrPc cleavage by alpha-secretase: mechanisticand therapeutic perspectives. Curr Alzheimer Res 2008Apr; 5 (2): 202-11
30. Sisodia SS. b-amyloid precursor protein cleavage by amembrane bound protease. Proc Natl Acad Sci U S A1992 Jul 1; 89 (13): 6075-9
31. Shin RW, Saido TC, Maeda M, et al. Novel a-secretasecleavage of Alzheimer’s amyloid b precursor protein inthe endoplasmic reticulum of COS7 cells. Neurosci Lett2005 Mar 7; 376 (1): 14-9
32. Imbimbo BP, Speroni F. b-Amyloid therapeutic strategiesfor Alzheimer’s disease. In: Abraham DJ, editor. Burger’s
medicinal chemistry and drug discovery. 6th ed. Hoboken(NJ): John Wiley & Sons Inc., 2005: 1-115
33. Furukawa K, Sopher BL, Rydel RE, et al. Increasedactivity-regulating and neuroprotective efficacy of alpha-secretase-derived secreted amyloid precursor proteinconferred by a C-terminal heparin-binding domain.J Neurochem 1996 Nov; 67 (5): 1882-96
34. MezianeH, Dodart JC,Mathis C, et al.Memory-enhancingeffects of secreted forms of the b-amyloid precursor pro-tein in normal and amnestic mice. Proc Natl Acad SciU S A 1998 Oct 13; 95 (21): 12683-8
35. Kojro E, Fahrenholz F. The non-amyloidogenic pathway:structure and function of alpha-secretases. Subcell Bio-chem 2005; 38: 105-27
36. Allinson TM, Parkin ET, Turner AJ, et al. ADAMs familymembers as amyloid precursor protein alpha-secretases.J Neurosci Res 2003 Nov 1; 74 (3): 342-52
37. Seals DF, Courtneidge SA. The ADAMs family of me-talloproteases: multidomain proteins with multiple func-tions. Genes Dev 2003 Jan 1; 17 (1): 7-30
38. Postina R, Schroeder A, Dewachter I, et al. A disintegrin-metalloproteinase prevents amyloid plaque formationand hippocampal defects in an Alzheimer disease mousemodel. J Clin Invest 2004 May; 113 (10): 1456-64
39. Lichtenthaler SF, Haass C. Amyloid at the cutting edge:activation of alpha-secretase prevents amyloidogenesis inan Alzheimer disease mouse model. J Clin Invest 2004May; 113 (10): 1384-7
40. Lopez-Perez E, Zhang Y, Frank SLJ, et al. Constitutivea-secretase cleavage of the b-amyloid precursor proteinin the furin-deficient LoVo cell line: involvement of thepro-hormone convertase 7 and the disintegrin ADAM10.J Neurochem 2001 Mar; 76 (5): 1532-9
41. Kojro E, Gimpl G, Lammich S, et al. Low cholesterol sti-mulates the nonamyloidogenic pathway by its effect onthe alpha-secretase ADAM 10. Proc Natl Acad Sci U S A2001 May 8; 98 (10): 5815-20
42. Parvathy S, Ehrlich M, Pedrini S, et al. Atorvastatin-induced activation of Alzheimer’s secretase is resistant tostandard inhibitors of protein phosphorylation-regulatedectodomain shedding. J Neurochem 2004 Aug; 90 (4):1005-10
43. Pedrini S, Carter TL, Prendergast G, et al. Modulation ofstatin-activated shedding of Alzheimer APP ectodomainby ROCK. PLoS Med 2005 Jan; 2 (1): e18
44. Famer D, Crisby M. Rosuvastatin reduces caspase-3activity and up-regulates a-secretase in human neuro-blastoma SH-SY5Y cells exposed to A beta. Neurosci Lett2004 Nov 23; 371 (2-3): 209-14
45. Hoglund K, Thelen KM, Syversen S, et al. The effect ofsimvastatin treatment on the amyloid precursor proteinand brain cholesterol metabolism in patients with Alz-heimer’s disease. Dement Geriatr Cogn Disord 2005;19 (5-6): 256-65
46. Kinouchi T, Sorimachi H, Maruyama K, et al. Conven-tional protein kinase C (PKC)-alpha and novel PKCepsilon, but not -delta, increase the secretion of an N-terminal fragment of Alzheimer’s disease amyloid pre-cursor protein from PKC cDNA transfected 3Y1fibroblasts. FEBS Lett 1995 May 8; 364 (2): 203-6
Secretase-Based Drugs in Alzheimer’s Disease 551
ª 2009 Adis Data Information BV. All rights reserved. Drugs Aging 2009; 26 (7)

This material is
the copyright of the
original publisher.
Unauthorised copying
and distribution
is prohibited.
47. Gabuzda D, Busciglio J, Yankner BA. Inhibition ofb-amyloid production by activation of protein kinase C.J Neurochem 1993 Dec; 61 (6): 2326-9
48. Savage MJ, Trusko SP, Howland DS, et al. Turnover ofamyloid b-protein in mouse brain and acute reduction ofits level by phorbol ester. J Neurosci 1998 Mar 1; 18 (5):1743-52
49. Garrido JL, Godoy JA, Alvarez A, et al. Protein kinase Cinhibits amyloid peptide neurotoxicity by acting onmembers of the Wnt pathway. FASEB J 2002 Dec;16 (14): 1982-4
50. Kozikowski AP, Nowak I, Petukhov PA, et al. New amide-bearing benzolactam-based protein kinase C modulatorsinduce enhanced secretion of the amyloid precursor pro-tein metabolite sAPPa. J Med Chem 2003 Jan 30; 46 (3):364-73
51. Ibarreta D, Duchen M, Ma D, et al. Benzolactam (BL)enhances sAPP secretion in fibroblasts and in PC12 cells.Neuroreport 1999 Apr 6; 10 (5): 1035-40
52. Etcheberrigaray R, Tan M, Dewachter I, et al. Thera-peutic effects of PKC activators in Alzheimer’s diseasetransgenic mice. Proc Natl Acad Sci U S A 2004 Jul 27;101 (30): 11141-6
53. Clarke H, Ginanni N, Laughlin KV, et al. The transientincrease of tight junction permeability induced by bryo-statin 1 correlates with rapid downregulation of proteinkinase C-alpha. Exp Cell Res 2000 Nov 25; 261 (1): 239-49
54. National Institute on Aging. Safety, efficacy, pharmacoki-netics, and pharmacodynamics study of bryostatin 1 inpatients with Alzheimer’s disease [ClinicalTrial.gov iden-tifier NCT00606164]. US National Institutes of Health.ClinicalTrial.gov [online]. Available from URL: http://www.clinicaltrials.gov [Accessed 2009 Jun 23]
55. Fahrenholz F. Activation of alpha-secretase as an ap-proach for treatment of Alzheimer’s disease. In: JuckerM,Beyreuther K, Haas C, et al., editors. Alzheimer: 100 yearsand beyond. Berlin: Springer-Verlag, 2006: 255-9
56. Hock C, Maddalena A, Heuser I, et al. Treatment with theselective muscarinic agonist talsaclidine decreases cere-brospinal fluid levels of total amyloid beta-peptide inpatients with Alzheimer’s disease. Ann N Y Acad Sci2000; 920: 285-91
57. Hock C, Maddalena A, Raschig A, et al. Treatment withthe selective muscarinic M1 agonist talsaclidine decreasescerebrospinal fluid levels of Ab42 in patients with Alz-heimer’s disease. Amyloid 2003 Mar; 10 (1): 1-6
58. Nitsch RM, Deng M, Tennis M, et al. The selective mus-carinic M1 agonist AF102B decreases levels of total Ab incerebrospinal fluid of patients with Alzheimer’s disease.Ann Neurol 2000 Dec; 48 (6): 913-8
59. Caccamo A, Oddo S, Billings LM, et al. M1 receptors playa central role in modulating AD like pathology in trans-genic mice. Neuron 2006 Mar 2; 49 (5): 671-82
60. Obregon DF, Rezai-Zadeh K, Bai Y, et al. ADAM10activation is required for green tea (-)-epigallocatechin-3-gallate-induced alpha-secretase cleavage of amyloid pre-cursor protein. J Biol Chem 2006 Jun 16; 281 (24): 16419-27
61. Marcello E, Gardoni F, Mauceri D, et al. Synapse-associated protein-97 mediates a-secretase ADAM10trafficking and promotes its activity. J Neurosci 2007 Feb14; 27 (7): 1682-91
62. Desire L, Buee L, Lambeng N, et al. EHT-0202: a neuro-protective and procognitive alpha-secretase stimulatortargeted towards Alzheimer disease therapy [abstract no.O3-05-02]. Alzheimers Dement 2008; 4 (4): T168
63. Lin X, Koelsch G, Wu S, et al. Human aspartic proteasememapsin 2 cleaves the beta-secretase site of beta-amyloidprecursor protein. Proc Natl Acad Sci U S A 2000 Feb 15;97 (4): 1456-60
64. Vassar R, Bennett BD, Babu-Khan S, et al. Beta-secretasecleavage of Alzheimer’s amyloid precursor protein by thetransmembrane aspartic protease BACE. Science 1999;286: 735-41
65. Ghosh AK, Gemma S, Tang J. beta-Secretase as a ther-apeutic target for Alzheimer’s disease. Neurotherapeutics2008 Jul; 5 (3): 399-408
66. Roberds SL, Anderson J, Basi G, et al. BACE knockoutmice are healthy despite lacking the primary beta-secre-tase activity in brain: implications for Alzheimer’s diseasetherapeutics. HumMolGenet 2001 Jun 1; 10 (12): 1317-24
67. Willem M, Garratt AN, Novak B, et al. Control of per-ipheral nerve myelination by the beta-secretase BACE1.Science 2006 Oct; 314 (5799): 664-6
68. Gruninger-Leitch F, Schlatter D, Kung E, et al. Substrateand inhibitor profile of BACE (b-secretase) and compar-ison with other mammalian aspartic proteases. J BiolChem 2002 Feb 15; 277 (7): 4687-93
69. Marciniszyn Jr J, Huang JS, Hartsuck JA, et al. Mode ofinhibition of acid proteases by pepstatin. J Biol Chem1976 Nov 25; 251 (22): 7095-102
70. Hills ID, Vacca JP. Progress toward a practical BACE-1inhibitor. Curr Opin Drug Discov Devel 2007 Jul; 10 (4):383-91
71. Ghosh AK, Kumaragurubaran N, Hong L, et al. Memap-sin 2 (beta-secretase) inhibitors: drug development. CurrAlzheimer Res 2008 Apr; 5 (2): 121-31
72. Hussain I. The potential for BACE1 inhibitors in thetreatment of Alzheimer’s disease. IDrugs 2004 Jul; 7 (7):653-8
73. Ghosh AK, Shin DW, Downs D, et al. Design of potentinhibitors for human brain memapsin 2 (beta-secretase).J Am Chem Soc 2000; 122 (14): 3522-3
74. Ghosh AK, Bilcer G, Harwood C, et al. Structure-baseddesign: potent inhibitors of human brain memapsin 2(beta-secretase). J Med Chem 2001 Aug 30; 44 (18): 2865-8
75. Asai M, Hattori C, Iwata N, et al. The novel beta-secretaseinhibitor KMI-429 reduces amyloid beta peptide pro-duction in amyloid precursor protein transgenic and wild-type mice. Neurochem 2006 Jan; 96 (2): 533-40
76. Park ICH, Jeon SY, Lee HJ, et al. A b-secretase (BACE1)inhibitor hispidin from the mycelial cultures of Phellinuslinteus. Planta Med 2004; 70 (2): 143-6
77. Jeon SY, Bae K, Seong YH, et al. Green tea catechins as aBACE1 (b-secretase) inhibitor. Bioorg Med Chem Lett2003 Nov 17; 13 (22): 3905-8
78. Ghosh AK, Devasamudram T, Hong L, et al. Structure-based design of cycloamide-urethane-derived novel inhib-itors of human brain memapsin 2 (b-secretase). BioorgMed Chem Lett 2005 Jan 3; 15 (1): 15-20
79. Turner 3rd RT, Hong L, Koelsch G, et al. Structurallocations and functional roles of new subsites S(5), S(6),
552 Panza et al.
ª 2009 Adis Data Information BV. All rights reserved. Drugs Aging 2009; 26 (7)

This material is
the copyright of the
original publisher.
Unauthorised copying
and distribution
is prohibited.
and S(7) in memapsin 2 (b-secretase). Biochemistry 2005Jan 11; 44 (1): 105-12
80. Chang WP, Koelsch G, Wong S, et al. In vivo inhibition ofAbeta production by memapsin 2 (betasecretase) in-hibitors. J Neurochem 2004 Jun; 89 (6): 1409-16
81. Chang WP, Downs D, Huang XP, et al. Amyloid-beta re-duction by memapsin 2 (beta-secretase) immunization.FASEB J 2007 Oct; 21 (12): 3184-96
82. He X, Cooley K, Chung CH, et al. Apolipoprotein receptor2 and X11 a/b mediate apolipoprotein E-induced endo-cytosis of amyloid-b precursor protein and b-secretase,leading to amyloid-b production. J Neurosci 2007 Apr 11;27 (15): 4052-60
83. Ghosh AK, Kumaragurubaran N, Hong L, et al. Potentmemapsin 2 (beta-secretase) inhibitors: design, synthesis,protein-ligand X-ray structure, and in vivo evaluation.Bioorg Med Chem Lett 2008 Feb 1; 18 (3): 1031-6
84. Lukiw WJ. Emerging amyloid beta (Ab) peptide mod-ulators for the treatment of Alzheimer’s disease (AD).Expert Opin Emerg Drugs 2008 Jun; 13 (2): 255-71
85. CoMentis announces proof-of-activity-data from its phaseI study of disease-modifying Alzheimer’s disease therapy.CoMentis News Room [online]. Available from URL:http://www.athenagen.com/index.php?/athenagen/press_releases/48 [Accessed 2008 Nov 30]
86. CoMentis receives FDA clearance to begin human clinicaltrials for its disease-modifying Alzheimer’s therapy. Co-Mentis News Room [online]. Available fromURL: http://www.athenagen.com/index.php?/athenagen/press_releases/45 [Accessed 2008 Nov 30]
87. Imbimbo BP. Alzheimer’s disease: gamma-secretase inhib-itors. Drug Discov Today Ther Strateg 2008; 5 (3): 169-75
88. Wolfe MS. Gamma-secretase: structure, function, andmodulation for Alzheimer’s disease. Curr TopMed Chem2008; 8 (1): 2-8
89. Armogida M, Petit A, Vincent B, et al. Endogenousb-amyloid production in presenilin deficient embryonicmouse fibroblasts. Nature Cell Biol 2001 Nov; 3 (11):1030-3
90. Wilson CA, Doms RW, Zheng H, et al. Presenilins are notrequired for Ab42 production in the early secretorypathway. Nature Neurosci 2002 Sep; 5 (9): 849-55
91. Lai MT, Crouthamel MC, DiMuzio J, et al. A presenilin-independent aspartyl protease prefers the gamma-42 sitecleavage. J Neurochem 2006 Jan; 96 (1): 118-25
92. Imbimbo BP. Therapeutic potential of gamma-secretaseinhibitors and modulators. Curr Top Med Chem 2008;8 (1): 54-61
93. Dovey HF, John V, Anderson JP, et al. Functionalg-secretase inhibitors reduce b-amyloid peptide levels inbrain. J Neurochem 2001 Jan; 76 (1): 173-81
94. Olson RE, Albright CF. Recent progress in the medicinalchemistry of g-secretase inhibitors. Curr Top Med Chem2008; 8 (1): 17-33
95. Best JD, Jay MT, Otu F, et al. Quantitative measurementof changes in amyloid-b(40) in the rat brain and cere-brospinal fluid following treatment with the g-secretaseinhibitor LY-411575 [N2-[(2S)-2-(3,5-difluorophenyl)-2-hydroxyethanoyl]-N1-[(7S)-5-methyl-6-oxo-6,7-dihydro-
5H-dibenzo[b,d]azepin-7-yl]-L-alaninamide]. J PharmacolExp Ther 2005 May; 313 (2): 902-8
96. Gitter BD, Czilli DL, Li W, et al. Stereoselective inhibitionof amyloid b peptide secretion by LY450139 dihydrate, anovel functional gamma secretase inhibitor [abstract no.P4.339]. Neurobiol Aging 2004; 25 (2S): S571
97. Rosen LB, Stone JA, Plump A, et al. The b secretaseinhibitor MK-0752 acutely and significantly reduces CSFAb40 concentrations in humans [abstract no. O4-03-02].Alzheimers Dement 2006; 2 (3) Suppl. 1: S79
98. Albright CF, Dockens R, Olson RE, et al. BMS-708163,a potent and selective g-secretase inhibitor, decreases CSFAb at safe and tolerable doses in animals and humans[abstract no. HT-01-05]. International Conference onAlzheimer’s Disease; 2008 Jul 26-31; Chicago
99. Wood KM, Lanz TA, Coffman KJ, et al. Efficacy of thenovel g-secretase inhibitor, Pf-3084014, in reducing ab inbrain, CSF, and plasma in guinea pigs and Tg2576 mice[abstract no. P2-375]. Alzheimers Dement 2008; 4 (4)Suppl. 2: T482
100. Frick G, Raje S, Wan H, et al. GSI-953, a potent and se-lective g-secretase inhibitor: modulation of b amyloidpeptides and plasma and cerebrospinal fluid pharmaco-kinetic/pharmacodynamic relationships in humans [ab-stract no. P4-366]. Alzheimers Dement 2008; 4 (4 Suppl.2): T781
101. Shen J, Bronson RT, Chen DF, et al. Skeletal and CNSdefects in presenilin-1-deficient mice. Cell 1997 May 16;89 (4): 629-39
102. Lewis HD, Perez Revuelta BI, Nadin A, et al. Catalyticsite-directed g-secretase complex inhibitors do not dis-criminate pharmacologically between Notch S3 and beta-APP cleavages. Biochemistry 2003 Jun 24; 42 (24): 7580-6
103. Maillard I, Adler SH, Pear WS. Notch and the immunesystem. Immunity 2003 Dec; 19 (6): 781-91
104. Stanger BZ, Datar R, Murtaugh LC, et al. Direct regula-tion of intestinal fate by Notch. Proc Natl Acad Sci U S A2005 Aug 30; 102 (35): 12443-8
105. Schouwey K, Beermann F. The Notch pathway: hairgraying and pigment cell homeostasis. Histol Histopathol2008 May; 23 (5): 609-19
106. Searfoss GH, Jordan WH, Calligaro DO, et al. Adipsin, abiomarker of gastrointestinal toxicity mediated by afunctional g-secretase inhibitor. J Biol Chem 2003Nov 14;278 (46): 46107-16
107. Boggs LN, Fuson KS, Gitter BD, et al. In vivo character-ization of LY450139, a novel, stereoselective, functionalg-secretase inhibitor [abstract]. Neurobiol Aging 2004;25 Suppl. 2: 218
108. May PC, Yang Z, Li W-Y, et al. Multi-compartmentalpharmaco-dynamic assessment of the functional g-secre-tase inhibitor LY450139 in PDAPP transgenic mice andnontransgenic mice [abstract no. 03-06-08]. NeurobiolAging 2004; 25 (S2): S65
109. Lanz TA,KarmilowiczMJ,WoodKM, et al. Concentration-dependent modulation of Ab in vivo and in vitro using theg-secretase inhibitor, LY- 450139. J Pharmacol Exp Ther2006 Nov; 319 (2): 924-33
110. Cocke PJ, Boggs LN, Ness DK, et al. Comparison of cis-ternal and lumbar cerebrospinal fluid amyloid beta con-
Secretase-Based Drugs in Alzheimer’s Disease 553
ª 2009 Adis Data Information BV. All rights reserved. Drugs Aging 2009; 26 (7)

This material is
the copyright of the
original publisher.
Unauthorised copying
and distribution
is prohibited.
centrations following oral administration of LY450139dihydrate to beagle dogs [abstract no. P1-017]. AlzheimersDement 2008; 4 (4 Suppl. 2): T210
111. NessDK, Boggs LN,HepburnDL, et al. Reducedb-amyloidburden, increased C-99 concentrations and evaluation ofneuropathology in the brains of PDAPP mice givenLY450139 dihydrate daily by gavage for 5 months [ab-stract no. P2-053]. Neurobiol Aging 2004; 25 (S2): S238
112. Siemers E, Skinner M, Dean RA, et al. Safety, tolerability,and changes in amyloid beta concentrations after admin-istration of a g-secretase inhibitor in volunteers. ClinNeuropharmacol 2005 May-Jun; 28 (3): 126-32
113. Siemers ER, Dean RA, Friedrich S, et al. Safety, toler-ability, and effects on plasma and cerebrospinal fluidamyloid-beta after inhibition of gamma-secretase. ClinNeuropharmacol 2007 Nov-Dec; 30 (6): 317-25
114. Siemers ER, Quinn JF, Kaye J, et al. Effects of a g-secretaseinhibitor in a randomized study of patients with Alzhei-mer disease. Neurology 2006 Feb 28; 66 (4): 602-4
115. Fleisher AS, Raman R, Siemers ER, et al. Phase 2 safetytrial targeting amyloid beta production with a gamma-secretase inhibitor in Alzheimer disease. Arch Neurol2008 Aug; 65 (8): 1031-8
116. Bateman RJ. Ab turnover in human subjects [abstract no.S2-01-04]. Alzheimers Dement 2008; 4 (4 Suppl. 2): T123
117. Wolfe MS. Inhibition and modulation of gamma-secretasefor Alzheimer’s disease. Neurotherapeutics 2008 Jul; 5 (3):391-8
118. Weggen S, Eriksen JL, Das P, et al. A subset of NSAIDslower amyloidogenic Abeta42 independently of cyclooxy-genase activity. Nature 2001 Nov 8; 414 (6860): 212-6
119. Kukar TL, Ladd TB, Bann MA, et al. Substrate-targetingg-secretase modulators. Nature 2008 Jun 12; 453 (7197):925-9
120. Kukar T, Golde TE. Possible mechanisms of action ofNSAIDs and related compounds that modulate g-secretasecleavage. Curr Top Med Chem 2008; 8 (1): 47-53
121. Peretto I, La Porta E. g-Secretase modulation and its pro-mise for Alzheimer’s disease: a medicinal chemistry per-spective. Curr Top Med Chem 2008; 8 (1): 38-46
122. Eriksen JL, Sagi SA, Smith TE, et al. NSAIDs and enan-tiomers of flurbiprofen target gamma-secretase and lowerAbeta 42 in vivo. J Clin Invest 2003 Aug; 112 (3): 440-9
123. Kukar T, Prescott S, Eriksen JL, et al. Chronic adminis-tration of R-flurbiprofen attenuates learning impairmentsin transgenic amyloid precursor protein mice. BMCNeurosci 2007 Jul 24; 8: 54
124. Galasko DR, Graff-Radford N, May S, et al. Safety, tol-erability, pharmacokinetics and Abeta levels after short-term administration of R-flurbiprofen in healthy elderlyindividuals. Alzheimer Dis Assoc Disord 2007 Oct-Dec;21 (4): 292-9
125. Wilcock GK, Black SE, Hendrix SB, et al., TarenflurbilPhase II Study investigators. Efficacy and safety oftarenflurbil in mild to moderate Alzheimer’s disease; arandomised phase II trial. Lancet Neurol 2008 Jun; 7 (6):483-93
126. Aisen PS. Tarenflurbil: a shot on goal. Lancet Neurol 2008Jun; 7 (6): 468-9
127. Green RC, Schneider LS, Hendrix SB, et al. Safety andefficacy of tarenflurbil in subjects with mild Alzheimer’sdisease: results from an 18-month multi-center phase 3trial. Alzheimers Dement 2008; 4 (4 Suppl. 2): T165
128. Imbimbo BP. Why did Flurizan fail? J Alzheimers Dis.Epub 2009 Jun 19
129. Kimura T, Kawano K, Doi E, et al. Cinnamide compound[patent no. US 2006/0004013 A1]. 2006 Jan 5
130. Page RM, Baumann K, Tomioka M, et al. Generation ofAb38 and Ab42 is independently and differentially af-fected by familial Alzheimer disease-associated presenilinmutations and gamma-secretase modulation. J Biol Chem2008 Jan 11; 283 (2): 677-83
131. Michener MS, Holahan MA, Gilberto DB, et al. Nonhu-man primate model for prediction of human Ab effects:targeting g-secretase – effects of enzyme inhibition vsmodulation of cleavage specificity on CSF and plasma Abin conscious rhesus monkeys [abstract no. P2-069]. Alz-heimers Dement 2006; 2 Suppl. 1: S252-3
132. Lindsley CW.Molecule of themonth. Curr TopMedChem2008; 8 (12): 1100
133. Imbimbo BP, Del Giudice E, Colavito D, et al. 1-(30,40-Dichloro-2-fluoro[1,10-biphenyl]-4-yl)-cyclopropanecarb-oxylic acid (CHF5074), a novel g-secretase modulator,reduces brain b-amyloid pathology in a transgenic mousemodel of Alzheimer’s disease without causing peri-pheral toxicity. J Pharmacol Exp Ther 2007 Dec; 323 (3):822-30
134. Imbimbo BP, Del Giudice E, Cenacchi V, et al. In vitroand in vivo profiling of CHF5022 and CHF5074, twob-amyloid1–42 lowering agents. Pharmacol Res 2007Apr; 55 (4): 318-28
135. Peretto I, Radaelli S, Parini C, et al. Synthesis and biolo-gical activity of flurbiprofen analogues as selective in-hibitors of b-amyloid1–42 secretion. J Med Chem 2005Sep 8; 48 (18): 5705-20
136. Imbimbo BP, Hutter-Paier B, Villetti G, et al. CHF5074, anovel g-secretase modulator, attenuates brain b-amyloidpathology and learning deficit in a mouse model of Alz-heimer’s disease. Br J Pharmacol 2009Mar; 156 (6): 982-93
137. Castellani RJ, Lee HG, Zhu X, et al. Neuropathology ofAlzheimer disease: pathognomonic but not pathogenic.Acta Neuropathol 2006 Jun; 111 (6): 503-9
138. Lee HG, Zhu X, Castellani RJ, et al. Amyloid-beta inAlzheimer disease: the null versus the alternate hy-potheses. J Pharmacol Exp Ther 2007 Jun; 321 (3): 823-9
139. Holmes C, Boche D, Wilkinson D, et al. Long-term effectsof Ab42 immunisation in Alzheimer’s disease: follow-upof a randomised, placebo-controlled phase I trial. Lancet2008 Jul; 372 (9634): 216-23
140. Puzzo D, Privitera L, Leznik E, et al. Picomolar amyloid-bpositively modulates synaptic plasticity and memory inhippocampus. J Neurosci 2008 Dec; 28 (53): 14537-45
141. Chen Y, Dong C. Ab40 promotes neuronal cell fate inneural progenitor cells. Cell Death Differ 2009 Mar; 16(3): 386-94
142. Lee HG, Zhu X, Nunomura A, et al. Amyloid beta: thealternate hypothesis. Curr Alzheimer Res 2006 Feb; 3 (1):75-80
554 Panza et al.
ª 2009 Adis Data Information BV. All rights reserved. Drugs Aging 2009; 26 (7)

This material is
the copyright of the
original publisher.
Unauthorised copying
and distribution
is prohibited.
143. Hayashi T, Shishido N, Nakayama K, et al. Lipid perox-idation and 4-hydroxy-2-nonenal formation by copperion bound to amyloid-beta peptide. Free Radic Biol Med2007 Dec; 43 (11): 1552-9
144. Nakamura M, Shishido N, Nunomura A, et al. Three his-tidine residues of amyloid-beta peptide control the redoxactivity of copper and iron. Biochemistry 2007 Nov 6; 46(44): 12737-43
145. Davies P, Maloney AJ. Selective loss of central cholinergicneurons in Alzheimer’s disease. Lancet 1976 Dec 25; II(8000): 1403
146. Rogers SL, Friedhoff LT. The efficacy and safety of do-nepezil in patients with Alzheimer’s disease: results ofa US multicentre, randomized, double-blind, placebo-controlled trial. The Donepezil Study Group. Dementia1996 Nov-Dec; 7 (6): 293-303
Correspondence: Dr Francesco Panza, Department of Ger-iatrics, Center for Aging Brain, Memory Unit, University ofBari, Policlinico, Piazza Giulio Cesare, 11-70124 Bari, Italy.E-mail: [email protected]
Secretase-Based Drugs in Alzheimer’s Disease 555
ª 2009 Adis Data Information BV. All rights reserved. Drugs Aging 2009; 26 (7)









![[Contemporary treatment with disease-modifying treatment in multiple sclerosis] Съвременно лечение с модифициращи хода на заболяването](https://img.pdfslide.net/doc/110x75/633338d3a290d455630a0a29/contemporary-treatment-with-disease-modifying-treatment-in-multiple-sclerosis.jpg)



















