Embed Size (px)
Citation preview

PII S0360-3016(99)00500-3
CLINICAL INVESTIGATION Brain
DOSIMETRY AND DOSE–RESPONSE RELATIONSHIPS IN NEWLYDIAGNOSED PATIENTS WITH MALIGNANT GLIOMAS TREATED
WITH IODINE-131-LABELED ANTI-TENASCIN MONOCLONALANTIBODY 81C6 THERAPY
GAMAL AKABANI , PH.D.,* ILKCAN COKGOR, M.D.,† R. EDWARD COLEMAN, M.D.,*DINKO GONZALEZ TROTTER, PH.D.,* TERENCE Z. WONG, M.D.,* HENRY S. FRIEDMAN, M.D.,‡
ALLAN H. FRIEDMAN, M.D.,† ANA GARCIA-TURNER,§ JAMES E. HERNDON II, PH.D.,\
DAVID DELONG, PH.D.,* ROGER E. MCLENDON, M.D.,§ XIAO-GUANG ZHAO, M.D.,*CHARLES N. PEGRAM,§ JAMES M. PROVENZALE, M.D.,* DARELL D. BIGNER, M.D., PH.D.,§ AND
MICHAEL R. ZALUTSKY, PH.D.*
Departments of *Radiology,†Medicine,‡Surgery,§Pathology, and\Community and Family Medicine, Duke University Medical Center,Durham, NC
Purpose: The objective of this study was to perform the dosimetry and evaluate the dose–response relationshipsin newly diagnosed patients with malignant brain tumors treated by direct injections of 131I-labeled 81C6monoclonal antibody (MAb) into surgically created resection cavities (SCRCs).Methods and Materials: Absorbed doses to the 2-cm-thick shell as measured from the margins of the resectioncavity interface were estimated for 42 patients with primary brain tumors. MR images were used to assess theenhanced-rim volume as a function of time after radiolabeled MAb therapy. Biopsy samples were obtained from15 patients and 1 autopsy.Results: The average absorbed dose [range] to the 2-cm shell region was 32 [3–59] Gy. For the endpoint ofminimal time to MR contrast enhancement, the optimal absorbed dose and initial dose-rate were 436 16 Gy and0.41 6 0.10 Gy/h, respectively. There was a correlation between the absorbed dose and dose rate to the shellregion and biopsy outcome (tumor recurrence, radionecrosis, and tumor recurrence and/or radionecrosis). Inthis Phase I study, the maximum tolerated dose (MTD) was 120 mCi. At this MTD, the estimated averageabsorbed dose and initial dose rate to the 2-cm shell were 41 [9–89] Gy and 0.51 [0.24–1.13] Gy/h, respectively.These values are in agreement with the optimal values based on the time to MR lesion rim enhancement.Conclusions: The average absorbed dose to the 2-cm shell region varied considerably and mainly depended oncavity volume. In future clinical trials, the administered activity of 131I-labeled 81C6 MAb may be adjusted basedon cavity volume in order to deliver the optimal absorbed dose of 43 Gy rather than giving a fixed administeredactivity. © 2000 Elsevier Science Inc.
Radioimmunotherapy, Brain tumors, Dosimetry.
INTRODUCTION
Gliomas are the most common primary brain tumors, andrepresent the major cause of morbidity and mortality inneuro-oncological practice. Surgery, followed by externalbeam irradiation and chemotherapy, is the standard of carefor malignant gliomas. External beam radiation therapy isconsidered the most effective adjuvant therapy followingsurgery. The benefit of postoperative radiotherapy has beenwell established by Walkeret al., (1) where an improvementin median survival was found with increasing radiation dose
(1–4). However, in conventional radiotherapy with standardfractionation, absorbed doses above 60–70 Gy are avoidedbecause of the significant risk of normal brain tissue toxicityincluding delayed brain-tissue radionecrosis (5–8).
Most tumor progression and recurrence occurs within 2cm of the tumor margin (9). Delivering higher absorbeddoses within this 2-cm margin may provide a higher prob-ability of tumor control and a lower probability of recur-rence within that region. Radiosurgery and brachytherapyhave been used as a means of focally escalating the radia-
Reprint requests to: Gamal Akabani, Ph.D., Department ofRadiology, DUMC 3808, Durham, NC 27710. E-mail:[email protected]—This work was supported by the NationalCenter for Research Resources General Clinical Research Centers
Program, National Institutes of Health, Grants MO1-RR 30,NS20023, CA11898, CA70164, and CA42324; American CancerSociety Grant PDT-414; and U.S. Department of Energy GrantDE-FG02-96ER62150.
Accepted for publication 5 November 1999.
Int. J. Radiation Oncology Biol. Phys., Vol. 46, No. 4, pp. 947–958, 2000Copyright © 2000 Elsevier Science Inc.Printed in the USA. All rights reserved
0360-3016/00/$–see front matter
947

tion dose for newly diagnosed glioblastoma multiforme(GBM) patients, and as rescue therapy for patients withrecurrent disease (10, 11).
A randomized clinical trial in newly diagnosed malignantgliomas carried out by the Brain Tumor Cooperative Group(BTCG) established the efficacy of brachytherapy (12). Themedian survival for patients undergoing brachytherapy (60Gy), radiation therapy (60.2 Gy), and chemotherapy was 64weeks versus 52 weeks for those receiving only externalbeam therapy and chemotherapy. However, the reoperationrates for symptomatic radionecrosis for these two groups ofpatients were 50% and 42%, respectively.
Radiosurgery has been shown to improve survival whencompared to external beam radiation in different clinicaltrials (13, 14). The best results obtained were in GBMpatients treated with surgery, external beam radiation, and aradiosurgery boost of 10–35 Gy (average of 20 Gy) (15).However, reoperation to remove symptomatic radiation ne-crosis was required in more than 50% of patients. Theamount of postoperative tumor volume and target volumewere found to be the most important parameters associatedwith successful radiosurgery treatment and for complica-tions (16, 17). Unfortunately, the volume of normal braintissue receiving moderate to high radiation doses increasesas the target volume increases regardless of the boost tech-nique. Therefore, the larger the tumor volume, the lower theabsorbed dose that can safely be administered, and the lowerthe probability of tumor control (18).
Direct administration of radiolabeled monoclonal anti-bodies (MAbs) into surgically created resection cavities(SCRCs) can also be used as an adjuvant radioimmuno-therapy. This therapeutic modality delivers a highly local-ized radiation dose to residual tumor located at and near thecavity interface, with minimal dose to normal brain. Thistherapeutic modality emerges as an important means ofimproving the local control of brain tumors. This treatmentapproach has been used in preliminary studies by Papanas-tassiouet al. (19) and Rivaet al. (20), where patients weretreated by a single or multiple injections of131I-labeledMAbs. Absorbed doses to the cavity interface were esti-mated to be from 70 to 410 Gy. Similarly, Hopkinset al.(21) estimated absorbed doses to the cavity interface as afunction of mean cavity radius and antibody-binding frac-tion for 90Y-labeled anti-neural cell adhesion MAb (ERIC-1); a range of doses from 20 to 5000 Gy were calculated.
Previously, Bigneret al.performed a Phase I clinical trialfor 131I-labeled 81C6 in recurrent malignant glioma patientswho had prior external beam radiotherapy (22). These pa-tients received external beam therapy doses (56 to 63 Gy) atleast 4 months before undergoing radiolabeled MAb ther-apy. A maximum tolerated dose (MTD) of 3700 MBq (100mCi) was determined with neurotoxicity being the dose-limiting factor. The average absorbed doses to the cavityinterface and 2-cm shell region at the MTD were 1180 and39 Gy, respectively (23).
In this report, we present the dosimetry results and dose–response analysis of the second arm of this Phase I clinical
trial using intracystically administered131I-labeled 81C6MAb to treat newly diagnosed patients with malignant braintumors. An objective of this study was to evaluate therelationship between the dosimetry and contrast-enhancedmagnetic resonance imaging (MRI) and clinical symptoms.
METHODS AND MATERIALS
Patient characteristicsForty-two patients were treated on this newly diagnosed
arm of the protocol: 14 were women and 28 were men, witha mean age of 47 years. Thirty-two patients had GBM, threehad anaplastic astrocytomas (AA), five had oligodendrogli-omas (AO), and two had mixed oligodendrogliomas (MO).All patients had a Karnofsky Performance Status (KPS)between 60 and 100, with the mean being 93. In this PhaseI protocol, patients were treated with an initial 20-mCi doseof 131I-labeled 81C6 MAb that was then escalated in 20-mCi increments up to 180 mCi. Patients diagnosed with AOdid not receive subsequent external beam therapy, and oneMO patient was not treated subsequently with externalbeam therapy. Two GBM patients refused external beamtherapy. The number of patients treated with131I-labeled81C6 MAb were as follows: 3 patients at 20 mCi/10 mg, 3at 40 mCi/10 mg, 5 at 60 mCi/10 mg, 6 at 80 mCi/10 mg,7 at 100 mCi/20 mg, 7 at 120 mCi/20 mg, 3 at 140 mCi/20mg, 7 at 160 mCi/20 mg, and 1 at 180 mCi/20 mg. As ofMay 1999, 26 patients were dead, 16 patients remainedalive and these are being followed.
Radiolabeled antibody characteristics81C6 is a murine IgG2B MAb that binds to tenascin, a
tumor-associated extracellular matrix glycoprotein presentin human gliomas but not in normal brain. Production of81C6 MAb was carried out in ascites fluid of athymic miceand it was purified by passage over a Sepharose-staphylo-coccal protein-A column, followed by polyethyleneimineion exchange chromatography. Radiolabeling of 81C6 MAbwith 131I was performed by the modified Iodo-Gen proce-dure (24). The radionuclide131I has a physical half-life of8.04 days and it emits beta particles with an average energyof 181.7 keV (100%) and a main gamma emission of 364.48keV (81.2%). The 90th percent distance (X90) of 131I betaparticles in liquid water is approximately 0.83 mm. Allpreparations had immunoreactivity of more than 50% (25),with more than 95% of the radioactivity eluting as IgG onhigh-pressure liquid chromatography, and more than 95%precipitating with trichloroacetic acid.
Toxicity determinationsPatients were monitored for toxicity and response for a
minimum of 1 year after radiolabeled MAb therapy or untildeath. Patients diagnosed with GBM and AA were subse-quently treated with external beam radiation therapy for 6weeks and, if they were stable, two cycles of adjuvantchemotherapy with chloroethylcyclohexylnitrosourea(CCNU), etoposide (VP-16), and tamoxifen, each were ad-
948 I. J. Radiation Oncology● Biology ● Physics Volume 46, Number 4, 2000
ministered. After adjuvant chemotherapy was completed,patients were evaluated every 3 months. At each evaluation,a complete physical and neurological examination, a KPSrating, and an MRI with contrast media administration wereperformed.
Serious toxicity was defined as Grade 3 or 4 nonhema-tological toxicity or major hematological toxicity, whichconsisted of more than 28 days of either an absolute neu-trophil count (ANC) of less than 500 cells/ml or a plateletcount of less than 20,000 cells/ml. Grade III or IV neuro-logical toxicity consisted of coma, severe confusion, intrac-table seizures, severe weakness or paralysis, sensory loss,and severe coordination problems. This definition wasbased on the National Cancer Institute Common ToxicityCriteria.
Radiation effects can be separated into acute and lateeffects. Such separation, however, is very imprecise anddoes not rely on the underlying pathophysiology and cellkinetic responses to radiation. Therefore, toxic effects ofradiation were categorized according to the time at whichthey became apparent and were divided in three categories:1) acute reactions, 2) subacute reactions, and 3) delayedreactions (26). Acute reactions occur at the time of radio-labeled MAb therapy. Subacute reactions were defined asthose occurring from the end of radiolabeled MAb therapyuntil 4 months after radiolabeled MAb therapy, and delayed
reactions were those occurring more than 4 months afterradiolabeled MAb therapy.
Brain imaging evaluationMRI was performed after radiolabeled MAb therapy to
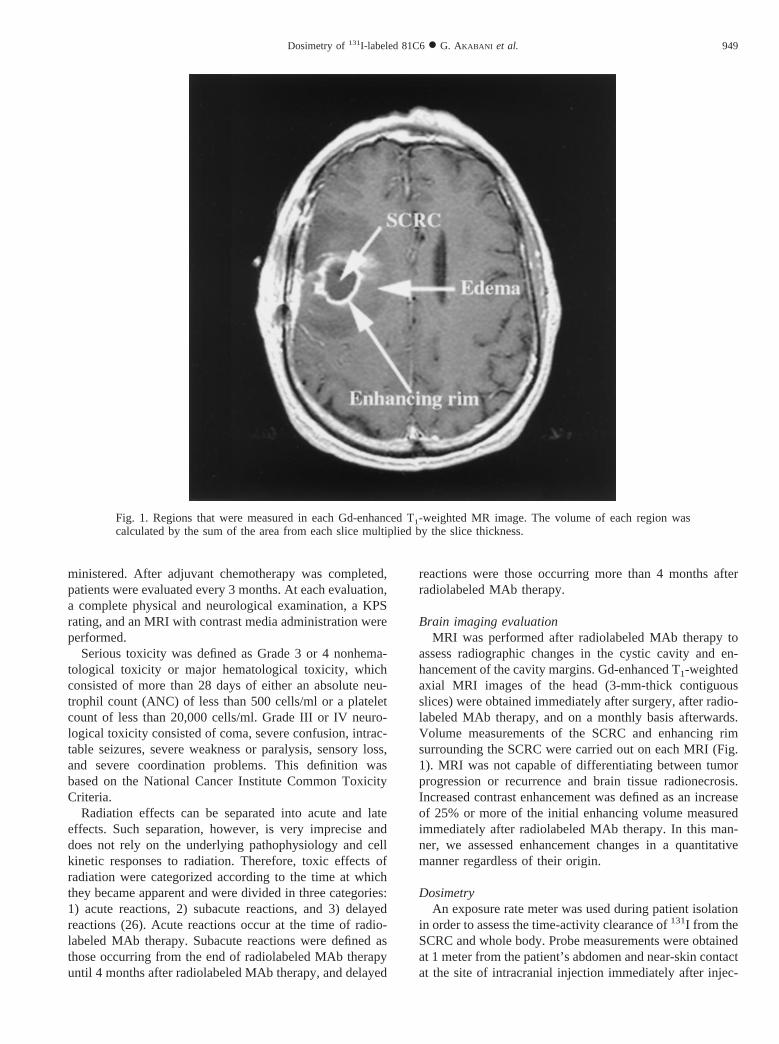
assess radiographic changes in the cystic cavity and en-hancement of the cavity margins. Gd-enhanced T1-weightedaxial MRI images of the head (3-mm-thick contiguousslices) were obtained immediately after surgery, after radio-labeled MAb therapy, and on a monthly basis afterwards.Volume measurements of the SCRC and enhancing rimsurrounding the SCRC were carried out on each MRI (Fig.1). MRI was not capable of differentiating between tumorprogression or recurrence and brain tissue radionecrosis.Increased contrast enhancement was defined as an increaseof 25% or more of the initial enhancing volume measuredimmediately after radiolabeled MAb therapy. In this man-ner, we assessed enhancement changes in a quantitativemanner regardless of their origin.
DosimetryAn exposure rate meter was used during patient isolation
in order to assess the time-activity clearance of131I from theSCRC and whole body. Probe measurements were obtainedat 1 meter from the patient’s abdomen and near-skin contactat the site of intracranial injection immediately after injec-
Fig. 1. Regions that were measured in each Gd-enhanced T1-weighted MR image. The volume of each region wascalculated by the sum of the area from each slice multiplied by the slice thickness.
949Dosimetry of131I-labeled 81C6● G. AKABANI et al.

tion and 24 hr afterwards. Whole-body planar images andprobe measurements were compared in order to assess theirlinear correlation (23). This analysis yielded relative clear-ance curves for the SCRC and whole body. Blood sampleswere obtained at approximately 1, 2, 4, 8, 12, 24, 72, 120,and 360 hours after131I-labeled 81C6 administration tomeasure the activity concentration in blood as a function oftime. Hopkins et al. have investigated the diffusion ofradiolabeled MAb into brain parenchyma resulting in alimited diffusion of a few millimeters. This dosimetricmodel assumes that there is a limited diffusion of theradiolabeled MAb into brain parenchyma (27). Therefore,most of the administered activity remained in the SCRC,and the absorbed dose to the whole body was calculatedbased on two sources: activity located in the SCRC and thatdistributed in the whole body. A serial two-compartmentsystem was used to model the pharmacokinetics of131I-labeled 81C6, where the SCRC and the whole body (notincluding the activity located in the SCRC) were assumed tobe the first and second compartments, respectively. Assum-ing a monoexponential clearance for the SCRC and wholebody, the functional solution for the SCRC and whole-body(WB) activity can be expressed as
ASCRC5 A0e2~lp1lSCRC!t
, (1)
AWB 5 A0
lSCRC
lWB 2 lSCRC~e2lSCRCt 2 e2lWBt!e2lpt (2)
whereA0 is the initial administered activity,lp representsthe physical decay constant for131I, andlSCRCandlWB arethe biological clearance constants for the SCRC and wholebody, respectively. The residence time for the SCRC(tSCRC) and whole body (tWB) were estimated from theseclearance curves. The whole-body absorbed dose was ex-pressed as
DWB 5 A0~tWBS~WB4WB! 1 tSCRCS~WB4 SCRC!! (3)
whereS(WB4 WB) andS(WB4 SCRC) are the corre-sponding S-values.
Radiation absorbed-dose estimates for bone marrow werebased on the activity in whole blood as a function of timepostadministration. The activity concentration of131I-la-beled 81C6 in blood samples was measured in a calibratedwell-scintillation counter. A factor of 0.3 was used to relateactivity in blood to that in marrow (28). The dose contri-bution from the SCRC to bone marrow was also estimatedby means of photon Monte Carlo transport (23). The esti-mated S-value for SCRC to bone marrow was 83 1025
(cGy/MBq-h).Knowledge of the range of absorbed doses as a function
of depth from the SCRC interface is of importance ingaining an understanding of the MRI evaluations, normaltissue toxicity (radionecrosis), and tumor control after treat-ment with 131I-labeled 81C6 MAb. Gd-enhanced T1-
weighted axial MRI images of the patient’s head wereobtained immediately after surgery and immediately afterdischarge from isolation. Using these images, a three-di-mensional reconstruction of the SCRC was generated andthe volume of the SCRC was calculated using image anal-ysis software (Voxel View 2.5.4, Vital Images, St. Paul,MN). This volume was used to estimate the initial activityconcentration in the SCRC at the time of administrationwhen a uniform activity concentration was assumed. Ab-sorbed doses to the cavity interface and shell region wereestimated using the corresponding S-values as a function ofcavity volume; S-values were calculated by means of betaand photon Monte Carlo transport based on the methodsdescribed previously (29). S-values are based on cavityvolume and therefore are patient-specific. The absorbeddose to a given target region was expressed as
D~target! 5 A0tSCRCS~target4 SCRC! (4)
and the corresponding S-values are
S~interface4 SCRC! 5 5.473 1022 V20.97, (5)
S~shell4 SCRC! 5 3.013 1024 V20.36, (6)
S~shellmin4 SCRC!
5 H 5.9023 1023 2 5.8443 1024 log~V! 25.5993 1023 V20.03571 1.4203 1025 V0.4538J , (7)
whereD is expressed in Gy,A0 in MBq, t in h, V in cm3,and the S-values in Gy/MBq-h.S(shellmin 4 SCRC) pro-vides the minimum S-value for the 2-cm shell region. Doserates at the cavity interface and shell region were expressedas
D~target! 5 A0S~target4 SCRC!e2~lp1lSCRC!t, (8)
whereD is expressed in Gy/h. Single-photon emission com-puted tomography (SPECT) scans were performed in sevenpatients immediately after discharge from isolation to es-tablish the distribution of131I activity within the SCRC andsurrounding brain tissue.
Estimates of absorbed doses per unit administered activ-ity to normal organs were calculated in a previous studywith 9 patients (23). The absorbed doses per unit adminis-tered activity for normal brain, liver, spleen, thyroid, stom-ach, bone marrow, and whole body were 0.18, 0.03, 0.08,0.05, 0.02, 0.02, and 0.01 cGy/MBq, respectively.
RESULTS
Dosimetry estimatesAbsorbed dose estimates to the cavity interface, 2-cm
shell region, whole body, and bone marrow were based onthe methods described previously by Akabaniet al., (23).The average [range] residence-time for the SCRC was 79
950 I. J. Radiation Oncology● Biology ● Physics Volume 46, Number 4, 2000

[10–113] h. The average [range] absorbed dose from131I-labeled 81C6 to the SCRC interface and 2-cm shell regionwas 1435 [46–9531] Gy and 32 [3–59] Gy, respectively. Ananalysis based on absorbed dose per unit administered ac-tivity (Gy/MBq) among all 42 patients to the cavity inter-face and 2-cm shell region with cavity volume resulted inthe following relationships
D interface5 4.143 V20.95 (9)
Dshell 5 0.0283 V20.40 (10)
whereV is expressed in cm3, with a correlation coefficientof r 5 0.9 andr 5 0.8, respectively. These expressionsindicate that the absorbed dose depended primarily on cav-ity volume. The initial average [range] dose rate to thecavity interface and 2-cm shell region for all patients was 20[1–121] Gy/h and 0.41 [0.04–0.75] Gy/h, respectively. Atthe maximum tolerated dose of 4440 MBq (120 mCi), theestimated initial dose rate and absorbed dose to the 2-cmshell region was 0.5 [0.3–0.9] Gy/h and 41 [9–89] Gy,respectively. The variability in absorbed dose was primarilydue to a large variation in SCRC size.
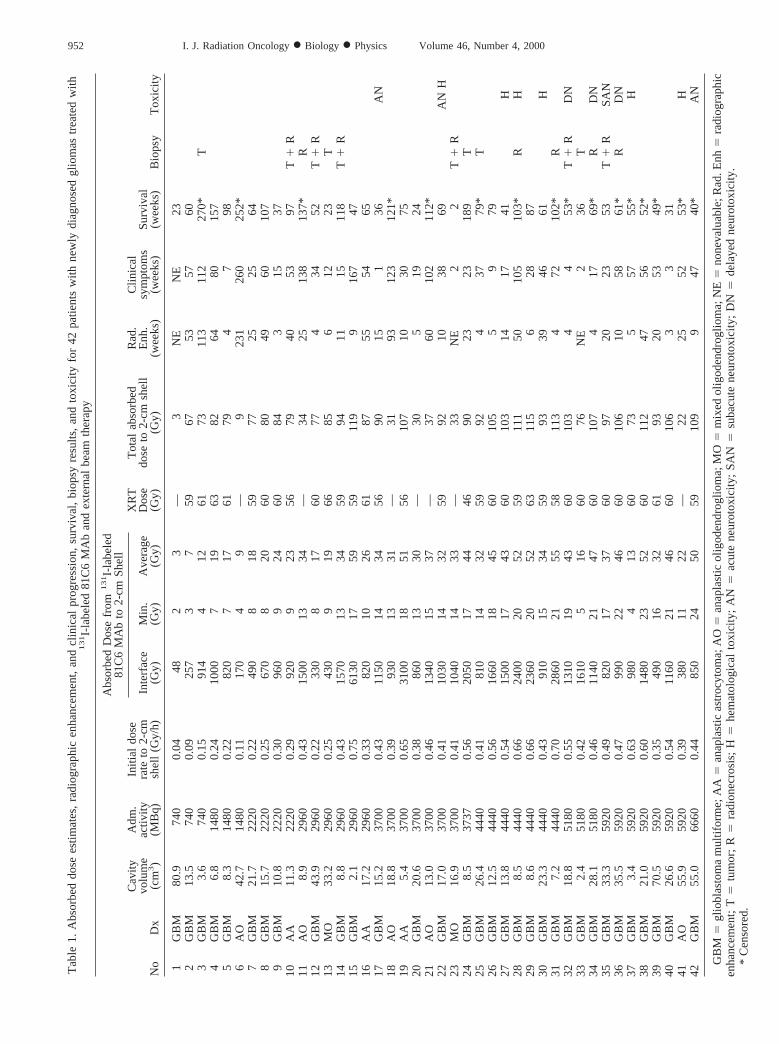
The average [range] residence time for the whole bodywas 35 [20–55] h. The average whole-body dose was 42[9–87] cGy, with an average absorbed per unit adminis-tered activity of 1.15 [0.39–1.67]3 1024 cGy/MBq. Theaverage absorbed dose to bone marrow was 42 [8–90] cGywith an average absorbed dose per unit administered activ-ity of 0.011 cGy/MBq. Only one of 42 patients treated with131I-labeled 81C6 developed major hematological toxicity(Patient 40). This patient was treated with 5920 MBq (160mCi) of 131I-labeled 81C6 MAb and developed neutropeniaand thrombocytopenia within 2 weeks after treatment. Theestimated residence time for131I-labeled 81C6 in the SCRCand whole body for this patient was 10 and 55 h, respec-tively. The estimated absorbed dose to the whole body andbone marrow was 87 and 90 cGy, respectively. Table 1presents a summary for all 42 patients of the histologicaldiagnosis, administered activity of131I-labeled 81C6 MAb,initial dose rate, radiolabeled MAb absorbed dose to theshell region, absorbed dose from external beam radiother-apy, total absorbed dose to the shell region, time to radio-graphic enhancement, time to clinical symptomatology, sur-vival, biopsy results, and clinical toxicity.
Figure 2 presents a three-dimensional image of the reg-istered MR and SPECT images for a patient who receivedan initial administered activity of 4440 MBq. A good cor-relation was obtained between the boundaries of the SCRCin MRI scans and131I activity distribution in SPECT im-ages.
Imaging observationsThirty-nine of the patients had sufficient images for com-
plete radiographic analysis (31: GBM; 2: AA; 5: AO; 1:MO). The volume of the enhancing rim was measured as afunction of time after131I-labeled 81C6 MAb therapy. The
cavity and rim-enhancing volumes were calculated fromimages obtained immediately after surgery, and these vol-umes were used as a reference for subsequent MR studies.The average [range] cavity volume and enhancing volumeof these 39 patients was 21 [2–81] and 7 [0–22] cm3,respectively. Within approximately 1 to 3 weeks after131I-labeled 81C6 MAb therapy, MR images from all patientsshowed a well-defined enhancing rim contiguous to theSCRC except in one patient with AO. The thickness of thisenhancing rim was approximately 2 to 3 mm, similar to themaximum range of131I beta particles in tissue. This enhanc-ing rim most likely represents an acute reaction caused byimmediate coagulation necrosis of brain tissue contiguousto the SCRC because of the extremely high doses to thecavity interface delivered by131I-labeled 81C6 MAb ther-apy; however, it was asymptomatic.
Similar to brachytherapy, these observations suggest thatacute reactions of normal brain tissue to131I-labeled 81C6MAb were related to dose rate and total dose (30). However,none of the patients treated with131I-labeled 81C6 exceededthe threshold dose for acute radiation necrosis of 180 Gy tothe 2-cm shell region (30). The median time to radiographicenhancement among all and GBM patients was 15 (5–39,95% confidence interval [CI]) weeks and 10 (4–23, 95%CI) weeks, respectively.
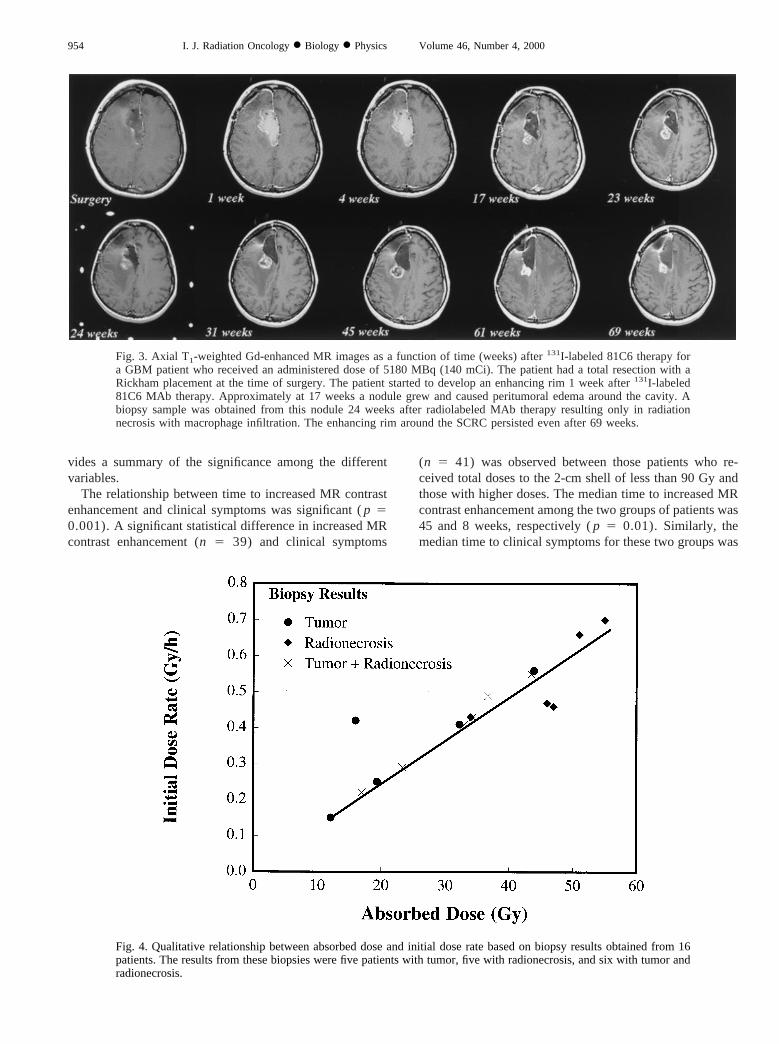
Figure 3 presents the radiographic progression for Patient34 diagnosed with GBM who received an administeredactivity of 5180 MBq (140 mCi). The absorbed dose to thecavity interface and 2-cm shell region in this patient was1145 and 47 Gy, respectively. Immediately after treatment,this patient suffered from acute neurotoxicity that consistedof focal motor seizures. External beam radiotherapy (60 Gy)started 4 weeks after131I-labeled 81C6 MAb therapy. Acontrast-enhancing nodule developed between 4 and 17weeks after131I-labeled 81C6 MAb, and a biopsy from thisregion at 24 weeks showed frank radiation necrosis withmacrophage infiltration. Furthermore, the enhancing rimpersisted up to 69 weeks after131I-labeled 81C6 MAbtherapy. As of this date, the patient has not required reop-eration for symptomatic radiation necrosis. However, herKPS score has been declining and her clinical status hasbeen deteriorating, as evidenced by memory loss, seizures,and severe confusion.
Acute and late reactions from low-dose-rate irradiationare dose-rate and total-dose related (30). The initial averageabsorbed dose rate to the shell region among all patients was0.41 [0.04–0.75] Gy/h. It has been suggested that a dose-rate higher than 0.8 Gy/h and boost dose higher than 60 Gylead to irreparable damage to the brain vasculature. Ananalysis of the median time to increased contrast for these39 patients based on a minimum131I-labeled 81C6 MAbdose and dose rate was carried out to assess their respectiveoptimal values. This analysis yielded an optimal radiola-beled MAb dose of 436 16 Gy with a dose rate of 0.4160.10 Gy/h to the shell region.
951Dosimetry of131I-labeled 81C6● G. AKABANI et al.
Tab
le1.
Abs
orbe
ddo
sees
timat
es,
radi
ogra
phic
enha
ncem
ent,
and
clin
ical
prog
ress
ion,
surv
ival
,bi
opsy
resu
lts,
and
toxi
city
for
42pa
tient
sw
ithne
wly
diag
nose
dgl
iom
astr
eate
dw
ith1
31 I-
labe
led
81C
6M
Ab
and
exte
rnal
beam
ther
apy
No
Dx
Cav
ityvo
lum
e(c
m3)
Adm
.ac
tivity
(MB
q)
Initi
aldo
sera
teto
2-cm
shel
l(G
y/h)
Abs
orbe
dD
ose
from
13
1 I-la
bele
d81
C6
MA
bto
2-cm
She
llX
RT
Dos
e(G
y)
Tot
alab
sorb
eddo
seto
2-cm
shel
l(G
y)
Rad
.E
nh.
(wee
ks)
Clin
ical
sym
ptom
s(w
eeks
)S
urvi
val
(wee
ks)
Bio
psy
Tox
icity
Inte
rfac
e(G
y)M
in.
(Gy)
Ave
rage
(Gy)
1G
BM
80.9
740
0.04
482
3—
3N
EN
E23
2G
BM
13.5
740
0.09
257
37
5967
5357
603
GB
M3.
674
00.
1591
44
1261
7311
311
227
0*T
4G
BM
6.8
1480
0.24
1000
719
6382
6480
157
5G
BM
8.3
1480
0.22
820
717
6179
47
986
AO
42.7
1480
0.11
170
49
—9
231
260
252*
7G
BM
21.7
2220
0.22
490
818
5977
2525
648
GB
M15
.722
200.
2567
08
2060
8049
6010
79
GB
M10
.822
200.
3096
09
2460
843
1537
10A
A11
.322
200.
2992
09
2356
7940
5397
T1
R11
AO
8.9
2960
0.43
1500
1334
—34
2513
813
7*R
12G
BM
43.9
2960
0.22
330
817
6077
434
52T
1R
13M
O33
.229
600.
2543
09
1966
856
1223
T14
GB
M8.
829
600.
4315
7013
3459
9411
1511
8T
1R
15G
BM
2.1
2960
0.75
6130
1759
5911
99
167
4716
AA
17.2
2960
0.33
820
1026
6187
5554
6517
GB
M15
.237
000.
4311
5014
3456
9015
136
AN
18A
O18
.837
000.
3993
013
31—
3193
123
121*
19A
A5.
437
000.
6531
0018
5156
107
1030
7520
GB
M20
.637
000.
3886
013
30—
305
1924
21A
O13
.037
000.
4613
4015
37—
3760
102
112*
22G
BM
17.0
3700
0.41
1030
1432
5992
1038
69A
NH
23M
O16
.937
000.
4110
4014
33—
33N
E2
2T1
R24
GB
M8.
537
370.
5620
5017
4446
9023
2318
9T
25G
BM
26.4
4440
0.41
810
1432
5992
437
79*
T26
GB
M12
.544
400.
5616
6018
4560
105
59
7927
GB
M13
.844
400.
5415
0017
4360
103
1417
41H
28G
BM
8.5
4440
0.66
2400
2052
5911
150
105
103*
RH
29G
BM
8.6
4440
0.66
2360
2052
6311
56
2887
30G
BM
23.3
4440
0.43
910
1534
5993
3946
61H
31G
BM
7.2
4440
0.70
2860
2155
5811
34
7210
2*R
32G
BM
18.8
5180
0.55
1310
1943
6010
34
453
*T
1R
DN
33G
BM
2.4
5180
0.42
1610
516
6076
NE
236
T34
GB
M28
.151
800.
4611
4021
4760
107
417
69*
RD
N35
GB
M33
.359
200.
4982
017
3760
9720
2353
T1
RS
AN
36G
BM
35.5
5920
0.47
990
2246
6010
610
5861
*R
DN
37G
BM
3.4
5920
0.63
980
413
6073
557
55*
H38
GB
M21
.059
200.
6014
8023
5260
112
4756
52*
39G
BM
70.5
5920
0.35
490
1632
6193
2053
49*
40G
BM
26.6
5920
0.54
1160
2146
6010
63
331
41A
O55
.959
200.
3938
011
22—
2225
5253
*H
42G
BM
55.0
6660
0.44
850
2450
5910
99
4740
*A
N
GB
M5
glio
blas
tom
am
ultif
orm
e;A
A5an
apla
stic
astr
ocyt
oma;
AO5
anap
last
icol
igod
endr
oglio
ma;
MO5
mix
edol
igod
endr
oglio
ma;
NE5
none
valu
able
;Rad
.Enh5
radi
ogra
phic
enha
ncem
ent;
T5tu
mor
;R
5ra
dion
ecro
sis;
H5he
mat
olog
ical
toxi
city
;A
N5
acut
ene
urot
oxic
ity;
SA
N5su
bacu
tene
urot
oxic
ity;
DN5
dela
yed
neur
otox
icity
.*
Cen
sore
d.
952 I. J. Radiation Oncology● Biology ● Physics Volume 46, Number 4, 2000

Clinical observationsTwelve patients had toxicity after131I-labeled 81C6 MAb
therapy; five patients had Grade II or III hematologicaltoxicity (H), seven patients had neurological toxicity (onepatient had both hematological and neurological toxicity)which was dose-limiting. Among those patients with hema-tological toxicity, the average [range] whole body dose andbone marrow dose was 58 [40–83] cGy and 87 [60–110]cGy, respectively. For those patients who developed neuro-logical toxicity, three had acute neurological toxicity (AN),one had subacute neurological toxicity (SAN), and three haddelayed neurological toxicity (DN). Among the seven pa-tients with neurological toxicity, the average radiolabeledMAb absorbed dose and initial dose rate to the 2-cm shellregion was 41 [37–55] Gy and 0.46 [0.46–0.7] Gy/h, re-spectively. Only one patient required reoperation for symp-tomatic radionecrosis (Patient 36).
Stereotactic biopsy samples were obtained from theSCRC interface region that received the highest radiationdose in 15 patients and one autopsy (Table 1). The necroticregion was firm and avascular and was easily separatedfrom the surrounding brain tissue. Histologically, the mate-rial was comprised of variable proportions of tumor and/ornecrotic tissue. Biopsy results were divided into three cat-egories: 1) tumor (T), 2) radionecrosis (R), and 3) mixedtumor and radionecrosis (T1 R). The results from these
biopsies were: five tumor, five radionecrosis, and six mixedtumor and radionecrosis.
The mean131I-labeled 81C6 MAb dose [range] and doserate [range] to the 2-cm shell region among the five patientswith radionecrosis was 47 [34–55] Gy, and 0.54 [0.43–0.7]Gy/h, respectively. One patient developed acute and de-layed neurotoxicity, and two developed delayed neurotox-icity. The five patients whose stereotactic biopsies indicatedtumor had an average dose [range] and average dose rate[range] to the 2-cm shell region of 25 [12–44], and 0.36[0.15–0.56] Gy/h, respectively. None of these patients hadany type of toxicity. Those patients diagnosed with mixedviable tumor and radionecrosis received an average131I-labeled 81C6 MAb dose [range] and average [range] doserate of 31 [17–44] Gy, and 0.4 [0.22–0.55] Gy/h, respec-tively. Two of these six patients had neurotoxicity.
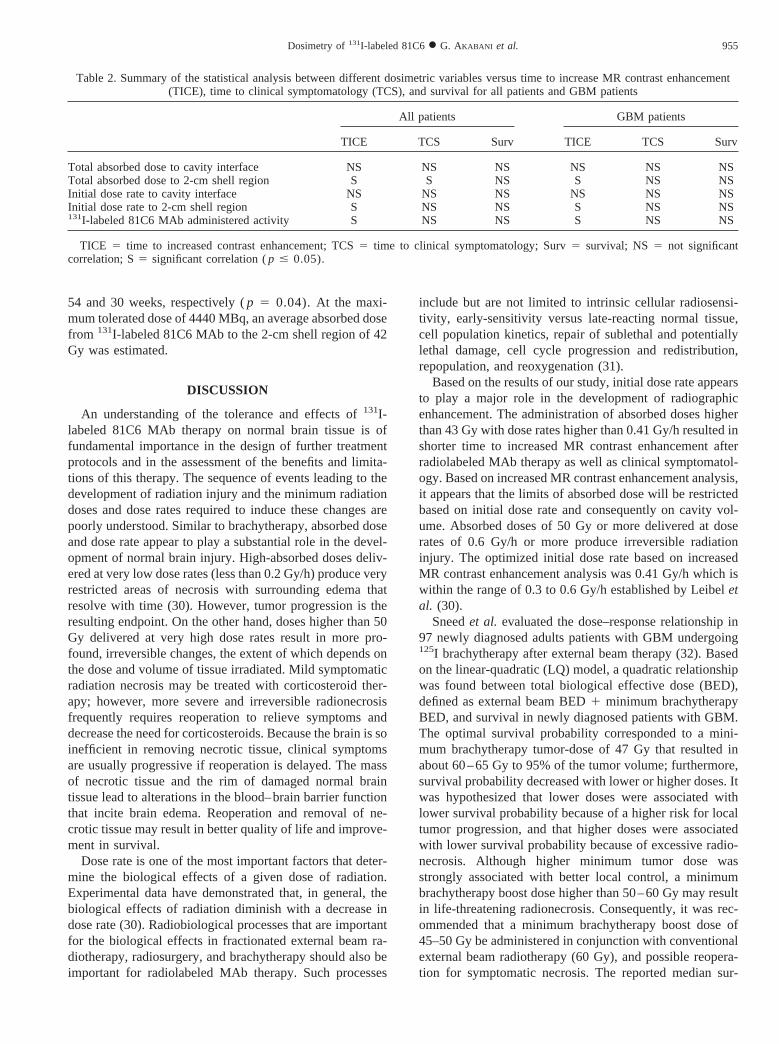
Comparing the dosimetric results among these threegroups, there is a qualitative relationship between absorbeddose and dose rate to the 2-cm shell region from131I-labeled81C6 MAb and clinical and pathological outcome (Fig. 4).It can be inferred that the most probable outcome for thosepatients who received an absorbed-dose and initial absorbeddose rate below 27 Gy and 0.34 Gy/h, respectively, is tumorrecurrence with no sign of radionecrosis and no treatment-related toxicity. For those patients that received an ab-sorbed-dose and initial absorbed dose rate higher than 47Gy and 0.54 Gy/h, respectively, the most probable outcomeis symptomatic radionecrosis with possible clinical neuro-toxicity. The most probable outcome for those patients whoreceived doses between 27 and 47 Gy and initial absorbeddose rates between 0.34 and 0.54 Gy/h is a mixture of tumorand radiation necrosis with possible signs of clinical neu-rotoxicty. The qualitative results obtained from these biopsysamples are in accordance with the optimal values of 43 Gyand 0.41 Gy/h for absorbed dose and dose rate, respectively,obtained from the previous analysis of MRI contrast en-hancement.
Statistical analysisThe median survival (95% CI) after radiolabeled MAb
therapy for all newly diagnosed patients and for those withGBM tumors was 75 (61–106, 95% CI) and 69 (52–106,95% CI) weeks, respectively. The median time to increasedMR contrast enhancement (TICE) among all patients andGBM patients was 15 (6–39, 95% CI) and 10 (4–23, 95%CI) weeks, respectively. The median time to clinical symp-tomatology (TCS) for all patients and GBM patients was 38weeks (19–58, 95% CI) and 30 weeks (17–57, 95% CI),respectively.
A Cox proportional hazard model was used to examinethe effect of the following variables on time to increasedMR contrast enhancement, clinical symptomatology, andsurvival: 1) total absorbed dose to the cavity interface, 2)total absorbed dose to the shell region, 3) initial absorbeddose rate to the cavity interface and shell region, and 4)131I-labeled 81C6 MAb administered activity. Table 2pro-
Fig. 2. Three-dimensional view of registered MRI and SPECTimages of a patient immediately after being discharged fromisolation where the estimated activity in the SCRC was 1554 MBq(42 mCi). The administered activity of131I-labeled 81C6 was 4440MBq. Notice the well-defined Rickham reservoir over the surfaceof the skull.
953Dosimetry of131I-labeled 81C6● G. AKABANI et al.
vides a summary of the significance among the differentvariables.
The relationship between time to increased MR contrastenhancement and clinical symptoms was significant (p 50.001). Asignificant statistical difference in increased MRcontrast enhancement (n 5 39) and clinical symptoms
(n 5 41) was observed between those patients who re-ceived total doses to the 2-cm shell of less than 90 Gy andthose with higher doses. The median time to increased MRcontrast enhancement among the two groups of patients was45 and 8 weeks, respectively (p 5 0.01). Similarly, themedian time to clinical symptoms for these two groups was
Fig. 3. Axial T1-weighted Gd-enhanced MR images as a function of time (weeks) after131I-labeled 81C6 therapy fora GBM patient who received an administered dose of 5180 MBq (140 mCi). The patient had a total resection with aRickham placement at the time of surgery. The patient started to develop an enhancing rim 1 week after131I-labeled81C6 MAb therapy. Approximately at 17 weeks a nodule grew and caused peritumoral edema around the cavity. Abiopsy sample was obtained from this nodule 24 weeks after radiolabeled MAb therapy resulting only in radiationnecrosis with macrophage infiltration. The enhancing rim around the SCRC persisted even after 69 weeks.
Fig. 4. Qualitative relationship between absorbed dose and initial dose rate based on biopsy results obtained from 16patients. The results from these biopsies were five patients with tumor, five with radionecrosis, and six with tumor andradionecrosis.
954 I. J. Radiation Oncology● Biology ● Physics Volume 46, Number 4, 2000
54 and 30 weeks, respectively (p 5 0.04). At themaxi-mum tolerated dose of 4440 MBq, an average absorbed dosefrom 131I-labeled 81C6 MAb to the 2-cm shell region of 42Gy was estimated.
DISCUSSION
An understanding of the tolerance and effects of131I-labeled 81C6 MAb therapy on normal brain tissue is offundamental importance in the design of further treatmentprotocols and in the assessment of the benefits and limita-tions of this therapy. The sequence of events leading to thedevelopment of radiation injury and the minimum radiationdoses and dose rates required to induce these changes arepoorly understood. Similar to brachytherapy, absorbed doseand dose rate appear to play a substantial role in the devel-opment of normal brain injury. High-absorbed doses deliv-ered at very low dose rates (less than 0.2 Gy/h) produce veryrestricted areas of necrosis with surrounding edema thatresolve with time (30). However, tumor progression is theresulting endpoint. On the other hand, doses higher than 50Gy delivered at very high dose rates result in more pro-found, irreversible changes, the extent of which depends onthe dose and volume of tissue irradiated. Mild symptomaticradiation necrosis may be treated with corticosteroid ther-apy; however, more severe and irreversible radionecrosisfrequently requires reoperation to relieve symptoms anddecrease the need for corticosteroids. Because the brain is soinefficient in removing necrotic tissue, clinical symptomsare usually progressive if reoperation is delayed. The massof necrotic tissue and the rim of damaged normal braintissue lead to alterations in the blood–brain barrier functionthat incite brain edema. Reoperation and removal of ne-crotic tissue may result in better quality of life and improve-ment in survival.
Dose rate is one of the most important factors that deter-mine the biological effects of a given dose of radiation.Experimental data have demonstrated that, in general, thebiological effects of radiation diminish with a decrease indose rate (30). Radiobiological processes that are importantfor the biological effects in fractionated external beam ra-diotherapy, radiosurgery, and brachytherapy should also beimportant for radiolabeled MAb therapy. Such processes
include but are not limited to intrinsic cellular radiosensi-tivity, early-sensitivity versus late-reacting normal tissue,cell population kinetics, repair of sublethal and potentiallylethal damage, cell cycle progression and redistribution,repopulation, and reoxygenation (31).
Based on the results of our study, initial dose rate appearsto play a major role in the development of radiographicenhancement. The administration of absorbed doses higherthan 43 Gy with dose rates higher than 0.41 Gy/h resulted inshorter time to increased MR contrast enhancement afterradiolabeled MAb therapy as well as clinical symptomatol-ogy. Based on increased MR contrast enhancement analysis,it appears that the limits of absorbed dose will be restrictedbased on initial dose rate and consequently on cavity vol-ume. Absorbed doses of 50 Gy or more delivered at doserates of 0.6 Gy/h or more produce irreversible radiationinjury. The optimized initial dose rate based on increasedMR contrast enhancement analysis was 0.41 Gy/h which iswithin the range of 0.3 to 0.6 Gy/h established by Leibeletal. (30).
Sneedet al. evaluated the dose–response relationship in97 newly diagnosed adults patients with GBM undergoing125I brachytherapy after external beam therapy (32). Basedon the linear-quadratic (LQ) model, a quadratic relationshipwas found between total biological effective dose (BED),defined as external beam BED1 minimum brachytherapyBED, and survival in newly diagnosed patients with GBM.The optimal survival probability corresponded to a mini-mum brachytherapy tumor-dose of 47 Gy that resulted inabout 60–65 Gy to 95% of the tumor volume; furthermore,survival probability decreased with lower or higher doses. Itwas hypothesized that lower doses were associated withlower survival probability because of a higher risk for localtumor progression, and that higher doses were associatedwith lower survival probability because of excessive radio-necrosis. Although higher minimum tumor dose wasstrongly associated with better local control, a minimumbrachytherapy boost dose higher than 50–60 Gy may resultin life-threatening radionecrosis. Consequently, it was rec-ommended that a minimum brachytherapy boost dose of45–50 Gy be administered in conjunction with conventionalexternal beam radiotherapy (60 Gy), and possible reopera-tion for symptomatic necrosis. The reported median sur-
Table 2. Summary of the statistical analysis between different dosimetric variables versus time to increase MR contrast enhancement(TICE), time to clinical symptomatology (TCS), and survival for all patients and GBM patients
All patients GBM patients
TICE TCS Surv TICE TCS Surv
Total absorbed dose to cavity interface NS NS NS NS NS NSTotal absorbed dose to 2-cm shell region S S NS S NS NSInitial dose rate to cavity interface NS NS NS NS NS NSInitial dose rate to 2-cm shell region S NS NS S NS NS131I-labeled 81C6 MAb administered activity S NS NS S NS NS
TICE 5 time to increased contrast enhancement; TCS5 time to clinical symptomatology; Surv5 survival; NS 5 not significantcorrelation; S5 significant correlation (p # 0.05).
955Dosimetry of131I-labeled 81C6● G. AKABANI et al.
vival for this group of patients was 83 weeks (32). Therewas no statistical correlation between any dosimetric vari-able and time to clinical symptomatology and survival; thislack of correlation may have been because these patientswere treated with chemotherapy.
Both brachytherapy and131I-labeled 81C6 MAb therapygenerate a sharp dose gradient at the field edges and cavityinterface, respectively. This effect may be responsible forthe fact that the majority of these patients recur in theimmediate periphery to the tumor cavity (23). Total ab-sorbed doses used in brachytherapy range between 100 and120 Gy. In contrast, the total absorbed doses using com-bined131I-labeled 81C6 and external beam therapy were inthe range of 63 to 115 Gy with an average of 80 Gy. Thislower absorbed dose may be the reason why only onepatient required reoperation.
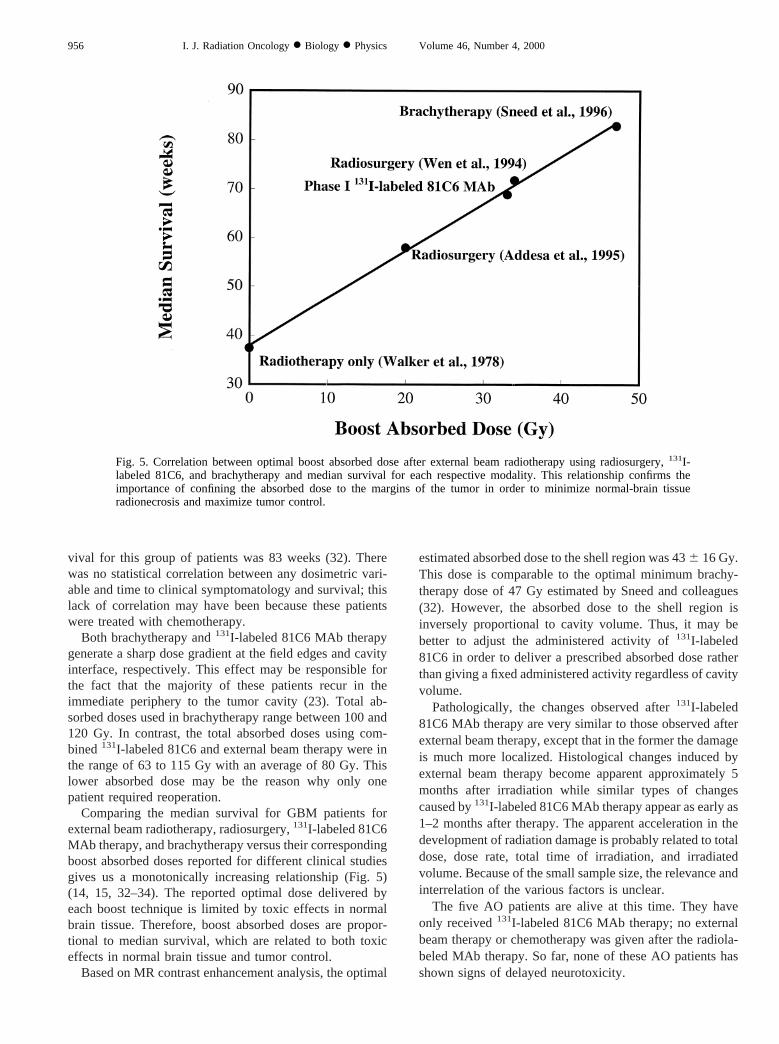
Comparing the median survival for GBM patients forexternal beam radiotherapy, radiosurgery,131I-labeled 81C6MAb therapy, and brachytherapy versus their correspondingboost absorbed doses reported for different clinical studiesgives us a monotonically increasing relationship (Fig. 5)(14, 15, 32–34). The reported optimal dose delivered byeach boost technique is limited by toxic effects in normalbrain tissue. Therefore, boost absorbed doses are propor-tional to median survival, which are related to both toxiceffects in normal brain tissue and tumor control.
Based on MR contrast enhancement analysis, the optimal
estimated absorbed dose to the shell region was 436 16 Gy.This dose is comparable to the optimal minimum brachy-therapy dose of 47 Gy estimated by Sneed and colleagues(32). However, the absorbed dose to the shell region isinversely proportional to cavity volume. Thus, it may bebetter to adjust the administered activity of131I-labeled81C6 in order to deliver a prescribed absorbed dose ratherthan giving a fixed administered activity regardless of cavityvolume.
Pathologically, the changes observed after131I-labeled81C6 MAb therapy are very similar to those observed afterexternal beam therapy, except that in the former the damageis much more localized. Histological changes induced byexternal beam therapy become apparent approximately 5months after irradiation while similar types of changescaused by131I-labeled 81C6 MAb therapy appear as early as1–2 months after therapy. The apparent acceleration in thedevelopment of radiation damage is probably related to totaldose, dose rate, total time of irradiation, and irradiatedvolume. Because of the small sample size, the relevance andinterrelation of the various factors is unclear.
The five AO patients are alive at this time. They haveonly received131I-labeled 81C6 MAb therapy; no externalbeam therapy or chemotherapy was given after the radiola-beled MAb therapy. So far, none of these AO patients hasshown signs of delayed neurotoxicity.
Fig. 5. Correlation between optimal boost absorbed dose after external beam radiotherapy using radiosurgery,131I-labeled 81C6, and brachytherapy and median survival for each respective modality. This relationship confirms theimportance of confining the absorbed dose to the margins of the tumor in order to minimize normal-brain tissueradionecrosis and maximize tumor control.
956 I. J. Radiation Oncology● Biology ● Physics Volume 46, Number 4, 2000

CONCLUSIONS
An understanding of the tolerance and effects of radiola-beled MAb on normal brain tissue is of fundamental im-portance in the design of treatment protocols and in theassessment of its benefits and limitations. Total dose anddose rate play a substantial role in the development ofirreversible brain injury and focal radiation necrosis that,unfortunately, may be mistaken for tumor progression orrecurrence when the usual imaging criteria are used. Thedose–response data obtained from this Phase I study deter-mined the minimum dose and dose rate required to mini-mize or eradicate tumor cells but spare normal brain tissue.Furthermore, the careful manipulation of dose rates andtotal doses to the shell margins can help minimize the toxiceffects of radiolabeled MAb therapy and maximize tumorcontrol. The administered activity of131I-labeled 81C6 infuture studies will probably be adjusted based on cavityvolume in order to deliver an optimal absorbed dose rather
than delivering a fixed administered activity regardless ofcavity volume.
The use of131I-labeled 81C6 as an adjuvant therapy is anaggressive therapeutic approach for the management ofmalignant gliomas. The optimal estimated radiolabeledMAb boost dose and initial dose rate that minimize braininjury and maximize tumor control were 436 16 Gy and0.416 0.10 Gy/h, respectively. This value for radiolabeledMAb dose is comparable to that estimated by Sneedet al.(32) for brachytherapy of 476 19 Gy (estimated uncertain-ty). This approach may increase the risk of radiation-in-duced damage to normal brain tissue. However, the likeli-hood of such risk is outweighed by the benefits in increasedmedian survival and quality of life of malignant gliomapatients. This risk is acceptable based on current mediansurvival of 69 weeks for GBM patients. This treatmentappears to prolong survival for newly diagnosed malignantgliomas and has a lower reoperative rate for symptomaticradionecrosis than does brachytherapy or radiosurgery.
REFERENCES
1. Walker MD, Strike TA, Sheline GE. An analysis of dose–response relationship in the radiotherapy of malignant glio-mas.Int J Radiat Oncol Biol Phys1979;5:1725–1731.
2. Walker MD, Alexander E, Hunt WE,et al. Evaluation ofBCNU and/or radiotherapy in the treatment of anaplasticgliomas; a co-operative clinical trial.J Neurosurg1978;49:333–343.
3. Sheline GE. Radiotherapy for high grade gliomas.Int J RadiatOncol Biol Phys1990;18:793–803.
4. Davies E, Clarke C, Hopkins A. Malignant cerebral glio-ma—I: Survival, disability, and morbidity after radiotherapy.Br Med J1996;313:1507–1512.
5. Chang CH, Horton J, Schoenfeld D, Salazer O, Perez-TamayoR, Kramer S, Weinstein A, Nelson JS, Tsukada Y. Compari-son of postoperative radiotherapy and combined postoperativeradiotherapy and chemotherapy in the multidisciplinary man-agement of malignant gliomas: A joint Radiation TherapyOncology Group and Eastern Cooperative Oncology Groupstudy.Cancer1983;52:997–1007.
6. Miller PJ, Hassanein RS, Giri PG, Kimler BF, O’Boynick P,Evans RG. Univariate and multivariate statistical analysis ofhigh-grade gliomas: The relationship of radiation dose andother prognostic factors.Int J Radiat Oncol Biol Phys1990;19:275–280.
7. Sheline GE, Wara WM, Smith V. Therapeutic irradiation andbrain injury.Int J Radiat Oncol Biol Phys1980;6:1215–1228.
8. Marks JE, Baglan RJ, Prassad SC, Blank WF. Cerebral radio-necrosis: Incidence and risk in relation to dose, time, fraction-ation and volume.Int J Radiat Oncol Biol Phys1981;7:243–252.
9. Burger PC, Heinz ER, Shibata T, Kleihues P. Topographicanatomy and CT correlations in the untreated glioblastomamultiforme.J Neurosurg1988;68:698–704.
10. Leibel SA, Gutin PH, Wara WM,et al.Survival and quality oflife after interstitial implantation of removable high-activityiodine-125 sources for the treatment of patients with recurrentmalignant gliomas.Int J Radiat Oncol Biol Phys1989;17:1129–1139.
11. Leibel SA, Scott CB, Loeffler JS. Contemporary approachesto the treatment of malignant gliomas with radiation therapy.Semin Oncol1994;21:198–219.
12. Green SB, Shapiro WR, Burger PC, Selker RG, VanGilder JC,Saris S, Malkin MG, Mealy J, Neal J, Robertson JT, Olson J.A randomized trial of interstitial radiotherapy (RT) boost fornewly diagnosed malignant glioma: Brain Tumor CooperativeGroup (BTCG) Trial 8701. Proceedings of the AmericanSociety of Clinical Oncology, Dallas, TX; 1994. p. 174.
13. Shrieve DC, Alexander E III, Wen PY,et al. Comparison ofstereotactic radiosurgery and brachytherapy in the treatment ofrecurrent glioblastoma multiforme.Neurosurgery1995;36:275–284.
14. Wen PY, Alexander E III, Black PM,et al. Long term resultsof stereotactic brachytherapy used in the initial treatment ofpatients with glioblastomas.Cancer1994;73:3029–3036.
15. Addesa AE, Shrieve DC, Alexander A III,et al. Stereotacticradiosurgery as primary adjuvant treatment for glioblastoma:The JCRT update. Proceedings Am Society Clin Oncol 31stAnnual Meeting. Los Angeles, 144, 1995.
16. Wood JR, Green SB, Shapiro WR. The prognostic importanceof tumor size in malignant gliomas: A computed topographicscan study by the Brain Tumor Cooperative Group.J ClinOncol 1988;6:338–343.
17. Marks LB, Specnce DP. The influence of volume on thetolerance of the brain to radiosurgery.J Neurosurg1991;75:177–180.
18. Larson DA, Wara WM. Radiotherapy of primary malignantbrain tumors.Semin Surg Oncol1998;14:34–42.
19. Papanastassiou V, Pizer BL, Coakham HB,et al.Treatment ofrecurrent and cystic malignant gliomas by a single intracavityinjection of 131I monoclonal antibody: Feasibility, pharmaco-kinetics and dosimetry.Br J Cancer1993;67:144–151.
20. Riva P, Arista A, Tison V,et al. Intralesional radioimmuno-therapy of malignant gliomas: An effective treatment in re-current tumors.Cancer1994;73:1076–1082.
21. Hopkins K, Chandler C, Bullimore J,et al.A pilot study of thetreatment of patients with recurrent malignant gliomas withintratumoral yttrium-90 radioimmunoconjugates.RadiotherOncol 1995;34:121–131.
22. Bigner DD, Brown MT, Friedman AH,et al. Iodine-131-labeled anti-tenascin monoclonal antibody 81C6 treatment ofpatients with recurrent malignant gliomas: Phase I trial results.J Clin Oncol1998;16:2202–2212.
957Dosimetry of131I-labeled 81C6● G. AKABANI et al.

23. Akabani G, Reist CJ, Cokgor I, Friedman AH, Friedman HS,Coleman RE, Zhao XG, Bigner DD, Zalutsky MR. Dosimetryof I-131 labeled 81C6 monoclonal antibody administered intosurgically created resection cavities in malignant brain tumorpatients.J Nucl Med1999;40:631–638.
24. Zalutsky MR, Moseley RP, Coakham HB, Coleman RE, Big-ner DD. Pharmacokinetics and tumor localization of 131I-labeled anti-tenascin monoclonal antibody 81C6 in patientswith gliomas and other intracranial malignancies.Cancer Res1989;49:2807–2813.
25. Lindmo T, Boven E, Cuttitta F, Fedorko J, Bunn PA Jr.Determination of the immunoreactive fraction of radiolabeledmonoclonal antibodies by linear extrapolation to binding atinfinite antigen excess.J Immunol Methods1984;72:77–89.
26. Rubin P, Casarett GW. Central nervous system. In: Rubin P,Casarett GW, editors. Clinical radiation pathology, Vol. II.Philadelphia, London, Toronto: W. B. Saunders; 1968. p.609–661.
27. Hopkins K, Chandler C, Eatough J, Moss T, Kemshead JT.Direct injection of 90Y MoAbs into glioma tumor resectioncavities leads to limited diffusion of the radioimmunoconju-gates into normal brain parenchyma: A model to estimateabsorbed radiation dose.Int J Radiat Oncol Biol Phys1998;40:835–844.
28. Sgouros G. Bone marrow dosimetry for radioimmunotherapy:Theoretical considerations.J Nucl Med1993;34:689–694.
29. Akabani G, Poston JW Sr, Bolch WE. Estimates of absorbedfractions in small volumes for selected radionuclides.J NuclMed 1991;32:835–839.
30. Leibel SA, Gutin PH, Davis RL. Factors affecting radiationinjury after interstitial brachytherapy for brain tumors. In:Gutin PH, Leibel SA, Sheline GE, editors. Radiation injury tothe nervous system. New York: Raven Press; 1991.
31. Hoshino T. A commentary on the biology and growth kineticsof low grade and high grade gliomas.J Neurosurg1984;61:895–900.
32. Sneed PK, Lamborn KR, Larson DA, Prados MD, Malec MK,McDermott MW, Weaver KA, Phillips TL, Wara WM, GutinPH. Demonstration of brachytherapy boost dose–response re-lationships in glioblastoma multiforme.Int J Radiat OncolBiol Phys1996;35:37–44.
33. Mehta MP, Masciopinto J, Rozental J, Levin A, Chappell R,Bastin K, Miles J, Turski P, Kubsad S, Mackie T,et al.Stereotactic radiosurgery for glioblastoma multiforme: Reportof a prospective study evaluating prognostic factors and ana-lyzing long-term survival advantage.Int J Radiat Oncol BiolPhys1994;30:541–549.
34. Barker FG 2nd, Prados MD, Chang SM, Gutin PH, LambornKR, Larson DA, Malec MK, McDermott M, Sneed PK, WaraWM, Wilson CB. Radiation response and survival time inpatients with glioblastoma multiforme.J Neurosurg1996;84:442–448.
958 I. J. Radiation Oncology● Biology ● Physics Volume 46, Number 4, 2000





























