Embed Size (px)
Citation preview

ORAL PAPERSThrombin-Activatable Fibrinolysis Inhibitor
O2A-1Identification of a protein factor that regulates humanthrombin-activatable fibrinolysis inhibitor mRNAstabilityKuo ACY1, Novakovic D2, Koschinsky ML2 and Boffa MB2
1Queen’s University, Kingston; 2University of Windsor, Windsor,
Canada
Thrombin-activatable fibrinolysis inhibitor (TAFI) is a basic carboxy-
peptidase zymogen that constitutes a molecular link between coagu-
lation and fibrinolysis, and between coagulation and inflammation.
The 3¢-untranslated region (UTR) of the human TAFI mRNA plays
a key role in regulating TAFI mRNA abundance. Three different
polyadenylation sites are used in TAFI mRNA processing with the
longest transcript being of the lowest stability and abundance and the
shortest transcript being of the highest stability and abundance.
Down-regulation of TAFI mRNA abundance by the inflammatory
cytokines IL-1b and IL-6 occurs through modulation of TAFI
mRNA stability. In the current study, we aimed to pinpoint cis-act-
ing elements in the TAFI 3¢-UTR and to identify protein factors
binding to these sites. We constructed a series of plasmids encoding
mRNAs containing rabbit b-globin sequences (as a reporter) fused to
sequences of the TAFI 3¢-UTR (encompassing 5¢ and internal dele-
tions). These plasmids were stably transfected into HepG2 (human
hepatoma) cells and the stability of the fusion transcripts measured.
We identified one element conferring stability and three elements con-
ferring instability. We then performed a series of gel mobility shift
analyses using RNA probes encompassing the three instability ele-
ments and HepG2 cell cytoplasmic extracts. Supershift assays identi-
fied the protein bound to the site between the second and third
polyadenylation sites as tristetraprolin (TTP). Mutation of the TTP
site abolished TTP binding in gel mobility shift assays and also stabi-
lized b-globin/TAFI fusion transcripts. TTP is a member of the
CCCH tandem zinc finger proteins and has been shown to regulate
the mRNA stability of a number of inflammatory proteins; TTP is
regulated by MAP kinase pathways, thus providing a plausible mech-
anism for the regulation of TAFI mRNA by inflammatory cytokines.
O2A-2Effect of TAFIa inhibition on tissue factor-inducedthromboembolism in the mouseRupin A, Vallez MO, Mennecier P, Richard I, Gloanec P andVerbeuren TJServier, Suresnes, France
Activated TAFI (TAFIa) or carboxypeptidase U cleaves C-terminal
lysine residues at the surface of partially degraded fibrin clots inhibit-
ing fibrinolysis before its propagation phase. The aim of this study
was to evaluate the role of TAFIa in an acute pulmonary thrombo-
embolism model induced by the systemic intravenous injection of
recombinant tissue factor (100 lL, Innovin�; Dade Behring) in the
tail vein of the mouse. Recombinant human tissue plasminogen acti-
vator (tPA, Alteplase, Boehringer Ingelheim) injected intravenously
(0.1 mL) 30 s before tissue factor increases survival of the mice in a
dose-dependent manner from 0.5 mg/kg (P < 0.05, Fisher test).
Interestingly, in the presence of an ineffective dose of tPA
(0.25 mg/kg), oral pretreatment of mice 1 h before tissue factor injec-
tion with a potent and selective TAFIa inhibitor (UK-396082, Ki
TAFIa = 12 nM and Ki Carboxypeptidase N > 100 lM) also
increases survival in a dose-dependent manner from 10 mg/kg
(P < 0.05, Fisher test). These results demonstrate that TAFIa plays
a role in acute pulmonary embolism induced by tissue factor in the
mouse. Moreover, our data confirm that prevention of TAFIa activ-
ity by an oral TAFIa inhibitor represents a novel therapeutic strategy
to prevent pulmonary thrombotic complications induced by activa-
tion of coagulation and fibrinolysis as found in patients with pulmo-
nary embolism.
O2A-3Evaluation of the profibrinolytic properties of ananti-TAFI monoclonal antibody in a mouse pulmonaryembolism modelVercauteren EB, Peeters M, Emmerechts J, Declerck PJ andGils AKatholieke Universiteit Leuven, Leuven, Belgium
Introduction Thrombin Activatable Fibrinolysis Inhibitor (TAFI)
plays an important role in the regulation of coagulation and fibrino-
lysis. Activated TAFI attenuates fibrinolysis by removing carboxyter-
minal lysines from partially degraded fibrin resulting in limited
plasmin formation.
Objective: To evaluate the profibrinolytic properties of MA-
TCK26D6.
Methods and Results: One-side ELISA and Surface Plasmon Reso-
nance analysis revealed that MA-TCK26D6, a monoclonal antibody
raised against human TAFI, cross-reacts with mouse TAFI. Chromo-
genic assays showed that MA-TCK26D6, using an 8-fold molar ratio
over TAFI, inhibits the plasmin-mediated activation of human and
mouse TAFI by 96 � 2% and 75 � 4%, respectively, and the throm-
bin/thrombomodulin-mediated activation by 26 � 17% and < 2%,
respectively. In in vitro clot lysis assays, MA-TCK26D6 (65 lg/mL)
reduces clot lysis time by 94 � 5% and 69 � 22% in human and
mouse plasma, respectively. The reduction of clot lysis time obtained
with the antibody is expressed relative to the reduction of clot lysis
time by potato tuber carboxypeptidase inhibitor (PTCI; 25 lg/mL), a
well-characterized TAFIa inhibitor. In a pulmonary embolism model,
mice were injected intravenously with a suboptimal concentration of
t-PA (0.1 mg/kg) before thromboplastin (2.5 mg/kg) injection to
induce thrombus formation in the lungs. Injection of MA-TCK26D6
(19 mg/kg) prior to t-PA and thromboplastin injections decreased
fibrin deposition in both lungs significantly, resulting in a significant
increase in the percentage of mice showing normal physical activity
(Table 1).
Conclusion: This is the first report on a monoclonal antibody that is
able to impair the activation of both human and mouse TAFI and
that can efficiently increase the percentage of mice with normal physi-
cal activity in a mouse pulmonary embolism model.
Table 1 for O2A-3
no MA MA-TCK26D6
Fibrin deposition left lungs 123 � 33 lg/mL 24 � 7 lg/mL*
Fibrin deposition right lungs 80 � 24lg/mL 33 � 9 lg/mL*
Mice with normal physical activity 26% 54%**
*P < 0.05; **P < 0.01, compared to control mice without MA
injection
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
ORAL PAPERS____________________________________________________________________________________

O2A-4Novel in vivo and in vitro profibrinolytic effect ofMMP-10 mediated by TAFIOrbe J1, Rodriguez JA1, Orset C2, Barrenetxe J1, Angles-Cano E2,Colucci M3, Vivien D2 and Paramo JA1
1CIMA University of Navarra, Pamplona, Spain; 2INSERM U9192
Serine Proteases and Pathophysiology of the Neurovascular Unit,
Caen, France; 3Section of General and Experimental Pathology,
University of Bary, Bari, Italy
Introduction: Extracellular proteolysis, mediated by the plasminogen/
plasmin and the metalloproteinase systems, plays a key role in many
pathophysiological processes. The role of metalloproteinases (MMPs)
on fibrinolysis has been scarcely studied. We examined the profibrin-
olytic effect of thrombin-activated MMP-10 (stromelysin-2) in vivo
and in vitro.
Methods: t-PA-mediated fibrinolysis was measured in human plasma
and blood by turbidimetry and thromboelastography, respectively.
Degradation of TAFI and other fibrinolytic proteins by MMP-10
was assessed on tricine gels. TAFI activity was determined with a
chromogenic substrate (Pentapharma). Tail-bleeding time and throm-
boembolic ischemic stroke induced by local injection of thrombin
(1 U/mL) in the middle cerebral artery were investigated in wild-type
(WT) and MMP-10 knockout (MMP-10-/-) mice.
Results: MMP-10 (1:10 ratio) degraded and inactivated purified
human TAFI but not other fibrinolytic proteins (plasminogen, t-PA
and u-PA). MMP-10 (100–400 nM) dose-dependently shortened the
lysis time of normal plasma clots (P < 0.05) but not of TAFI-defi-
cient clots. On the contrary, a monoclonal antibody anti-MMP-10
prolonged the lysis time of plasma clots, even in the absence of added
MMP-10, suggesting a role of the endogenous strmelysis-2. MMP-10
(200 nM) caused a significant and TAFI-dependent (PTCI-sensitive)
shortening of lysis time in whole blood (30.5 � 19.7%, P = 0.01).
Compared to WT animals, MMP-10-/- mice displayed higher levels
of circulating TAFI (P < 0.01) and delayed reperfusion after throm-
bin-induced thromboembolic stroke (40%, P < 0.05). Surprisingly,
MMP-10-/- mice showed a significantly shorter tail bleeding time that
was reverted by MMP-10 injection (2 nM).
Conclusions: We show for the first time that MMP-10 plays a previ-
ously unrecognized profibrinolytic effect favouring clot lysis in vivo
and in vitro. Our results indicate that inhibition of TAFI activity by
MMP-10 may contribute to enhanced clot lysis and support a profi-
brinolytic effect of this protease.
O2A-5Intact thrombomodulin-mediated regulation offibrinolysis during and after liver transplantation,despite a profoundly defective thrombomodulin-mediated regulation of coagulationLisman T1, Ruitenbeek K1, Adelmeijer J1, Hendriks HGD1,Meijers JCM2 and Porte RJ1
1University Medical Center Groningen, Groningen;2AMC, Amsterdam, The Netherlands
Liver disease is associated with substantial hemostatic changes, which
aggravate during liver transplantation. We have recently measured
thrombin generation in absence and presence of thrombomodulin in
plasma samples taken during and after liver transplantation and
observed a striking and as yet unexplained inability of thrombomod-
ulin to downregulate thrombin generation in patient plasma. Since
thrombomodulin is not only vital for the activation of protein C, but
also for activation of thrombin activatable fibrinolysis inhibitor
(TAFI), we investigated thrombomodulin-mediated regulation of
fibrinolysis during liver transplantation using a plasma-based clot
lysis assay. Ten adult patients undergoing liver transplantation and
eleven healthy volunteers from our laboratory were included in this
study. Blood samples from the patients were taken perioperatively
and at days 1, 5 and 10 after surgery. Clot lysis assays were per-
formed in the presence or absence of thrombomodulin and in the
presence or absence of the TAFI inhibitor CPI. During liver trans-
plantation, clot lysis time in the absence of thrombomodulin steadily
decreased and was shortest after reperfusion. At the end of surgery,
clot lysis time transiently increased and subsequently returned
towards normal in the postoperative period. In the presence of CPI,
clot lysis time decreased in controls and in patients at the start of
surgery, but was not different from clot lysis time in the absence of
CPI after reperfusion indicating that no TAFI activation takes place
in samples taken at this time point. Upon addition of thrombomodu-
lin, clot lysis time in controls and in patients at the start of surgery
doubled, and clot lysis time after reperfusion increased almost 5-fold,
and these increases were fully attributable to TAFI activation.
In conclusion, we have demonstrated intact thrombomodulin-medi-
ated regulation of fibrinolysis during liver transplantation, even
though thrombomodulin-mediated regulation of coagulation is pro-
foundly disturbed in these patients.
O2A-6Soluble thrombomodulin improves the hemostaticbalance in whole blood from canines with hemophiliaAFoley JH1, Petersen KU2, Lillicrap D1 and Nesheim ME1
1Queen’s University, Kingston, Canada; 2PAION Deutschland
GmbH, Aachen, Germany
Background: Hemophilia A is a debilitating disease that affects
approximately 1 in 5000 males. Severe hemophiliacs are prone to
spontaneous soft tissue, joint and intracranial bleeding which
increases the morbidity and mortality of the disease. Another major
complication of hemophilia is the development of inhibitors to fVIII
which makes the primary form of treatment ineffective. Soluble
thrombomodulin (Solulin), an indirect stabilizer of blood clots, may
stabilize the clot to an extent where less fVIII (or fIX, fVIIa, aPCC,
etc.) may be needed to control bleeding in hemophilia.
Methods: Clot-lysis experiments were conducted in normal and hem-
ophilic (�fVIII neutralizing inhibitors) dog plasma and whole blood
and clotting and fibrinolysis were monitored by turbidity and throm-
belastography, respectively.
Results: Canine TAFI exists in plasma at a concentration of 100 nM
and the half-life of canine TAFIa is 23 min. In hemophilic plasma,
the clot-lysis time and the TAFIa potential increased linearly with
the Solulin concentration. At 200 nM Solulin the TAFIa dependent
prolongation of lysis reached a plateau. In hemophilic whole blood,
the area under the clot-lysis curve (AUCL) can be used as a measure
of clot firmness and 100 nM Solulin increased this parameter by
greater than 5-fold. The clot lysis time in whole blood was increased
from 20 min in the absence of Solulin to > 3 h in the presence of
100 or 250 nM Solulin. Finally, in hemophilic whole blood with
fVIII-neutralizing inhibitors (> 150 BU), the AUCL was normalized
with 390 nM Solulin and the clot-lysis time was increased from 18 to
46 min.
Conclusions: Solulin increases both the clot lysis time and clot firm-
ness in hemophilic plasma and whole blood. This improvement in the
hemostatic balance suggests that Solulin may be used to suppress
fibrinolysis and stabilize clots in hemophilia.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
2 ORAL PAPERS____________________________________________________________________________________

Cellular Aspects
O2B-1Tissue-type plasminogen activator (t-PA) andtenecteplase but not urokinase or desmoteplasemodulate permeability across a human model of theblood-brain-barrierNiego B1, Medcalf RL1 and Petersen KU2
1Monash University, Melbourne, Australia; 2PAION Deutschland
GmBH, Aachen, Germany
t-PA is well-established for its role in the treatment of ischaemic
stroke in the CNS and can modulate blood brain barrier (BBB)
permeability in vitro and in vivo using rodent systems. This feature
of t-PA may be deleterious in patients with ischaemic stroke by
increasing the risk for haemorrhagic transformation during throm-
bolytic therapy. The mechanism underlying this effect of t-PA is
not fully understood, nor is it known if this phenomenon is shared
by other plasminogen activators. We have developed a human BBB
model whereby transformed human astrocytes are co-cultured for
72 h on the underside of a 3-micron porous membrane in contact
with primary human brain microvascular endothelial cells, seeded in
the inner (luminal) chamber. BBB permeability was estimated by
quantitating the transfer of FITC-labeled albumin across the mem-
brane. Addition of t-PA (0.1–1 lM) to the luminal side of the insert
caused a concentration-dependent increase in albumin transfer
within 8 h. Catalytic activity was required, as an inactive t-PA vari-
ant (ct-PA) produced no change in permeability. The t-PA effect
was blocked by a2-antiplasmin or aprotinin, indicating a require-
ment for plasmin generation. t-PA-induced increase in permeability
was also associated with changes in astrocyte morphology. The
t-PA variant, Tenecteplase (1 lM) also produced a significant
increase in permeability, although to a lesser extent than t-PA.
Reteplase, a variant consisting only of the second kringle and prote-
ase domains, was significantly less active. Urokinase, as well as des-
moteplase (both at 1 lM), were without effect and had no influence
on astrocyte morphology. Hence, the effect of t-PA on a human
model of the BBB requires plasmin generation, and is unique to
t-PA, its closest variant Tenecteplase and to a lesser extent retep-
lase. The lack of effect of desmoteplase is of particular interest as
this fibrin-selective thrombolytic is under phase-3 clinical develop-
ment for patients with ischaemic stroke
O2B-2Tissue-type plasminogen activator (t-PA) inducesintracranial bleeding through stromelysin-1 (MMP-3)induction in endothelial cells via low-densitylipoprotein receptor familySuzuki Y1, Nagai N2, Yamakawa K1, Kawakami J1, Lijnen HR3
and Umemura K1
1Hamamatsu University School of Medcine, Hamamatsu; 2Kinki
University School of Medicine, Osakasayama, Japan; 3KU
Leuven, Leuven, Belgium
Background: Tissue-type plasminogen activator (t-PA) is approved
for treatment of ischemic stroke patients, but it increases the risk of
intracranial bleeding (ICB). Here, we investigated the role of matrix
metalloproteinase -3 (MMP-3) in ICB increased by tPA.
Method: ICB was studied by a thrombotic middle cerebral artery
occlusion (MCAO) model in mice with genetic deficiencies of strom-
elysin-1 (MMP-3-/-) with or without intravenous t-PA (10 mg/kg)
administration 4 h after MCAO. Receptor-associated protein (RAP,
1 or 2 mg/kg), an antagonist of the low-density lipoprotein receptor
family (LDLRs) was also intravenously administered 5 min before
t-PA administration. In vitro, MMP-3 induction by t-PA treatment
(10 lg/mL) with or without RAP (200 nM) under 6 h oxygen-
glucose deprivation (OGD) followed by 18 h normoxia (Nor) was
assessed in bEnd.3, a mouse brain derived endothelial cell line.
Expression of LRP, a member of LDLRs, was measured both
in vitro and in vivo.
Results: In MMP-3+/+ WT mice given solvent, ICB was
4.3 � 2.9 mm3 (mean � SD, n = 7), which was significantly
increased with t-PA treatment to 9.7 � 4.7 mm3 (n = 9, P < 0.05),
whereas ICB in MMP-3-/- mice was not altered by t-PA treatment
(5.7 � 2.7 mm3, n = 9). Pretreatment with RAP prevented the
increased ICB induced by t-PA (2.0 � 2.0 and 1.9 � 1.1 mm2,
respectively, n = 8 each). In bEnd.3 cells, MMP-3 induction was
also significantly enhanced after OGD (1.7 � 0.14-fold increase),
which was further increased by t-PA treatment (2.4 � 0.16-fold,
P < 0.05 vs. OGD, n = 5). Furthermore, we observed upregulation
of LRP by ischemic stress, and suppression of MMP-3 induction
associated with t-PA by pretreatment with RAP, both in vitro and
in vivo.
Conclusion: These findings indicate that t-PA deteriorates ICB via
MMP-3 induction in endothelial cells and that antagonists of LDLRs
may have the potential to suppress ICB caused by t-PA treatment in
patients with stroke.
O2B-5Hypoxia and upregulation of hypoxia inducible factor1 alpha stimulate angiogenesis within resolvingvenous thrombiEvans CE, Humphries J, Mattock K, Waltham M, Wadoodi A,Saha P and Smith AKCL, London, UK
Objective: Angiogenesis is an important process in thrombus resolu-
tion, but the primary stimulus for neovascularisation is unknown.
Our aims were to determine whether: (i) hypoxia and hypoxia-induc-
ible factor (HIF) 1a are induced in resolving thrombus; (ii) this stim-
ulates production of factors that regulate angiogenesis; and (iii)
upregulating HIF1a enhances resolution.
Methods: The levels of hypoxia, HIF1a, and vascular endothelial
growth factor (VEGF) were measured in mouse thrombi at 1, 3, 7,
and 14 days after induction (n = 10/group). Oxygen tension was
measured with an oxygen sensor. HIF1a and VEGF were localised
by immunostaining and quantified by ELISA. An additional group
of thrombosed mice received daily intraperitoneal injections of either
L-mimosine, which prevents HIF1a degradation, or vehicle control
(n = 30/group). Expression of HIF1a, VEGF, and nine other HIF1-
mediated factors were measured by ELISA and proteome array at
days 1 and 7. Macrophage infiltration and thrombus resolution was
measured by image analysis at day 7.
Results: Oxygen tension in the thrombus was negatively correlated
with HIF1a (RS = -0.77, P < 0.0001); while HIF1a positively corre-
lated with VEGF (R = 0.85, P < 0.0005), during natural resolution.
HIF1a (P < 0.005) and VEGF (P < 0.005) was 2-fold greater in the
thrombus of mice treated with L-mimosine compared with controls,
and insulin-like growth factor binding protein 1 (IGFBP1, P < 0.01)
and stromal cell-derived factor 1 (SDF1, P < 0.04) were also
increased. Thrombus weight (P < 0.001) and volume (P < 0.05)
were reduced by a third in L-mimosine-treated mice compared with
controls; while vein recanalisation was 2-fold greater (P < 0.05),
which was associated with macrophage recruitment into the vein
wall.
Conclusions: Hypoxia and HIF1a induced in the naturally resolv-
ing thrombus are associated with angiogenic factor expression.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
ORAL PAPERS 3____________________________________________________________________________________

Accumulation of HIF1a increases the expression of factors that
regulate neovascularisation and enhances thrombus resolution.
HIF1a may represent a novel target for treatments that promote
resolution and reduce the incidence of post-thrombotic syndrome.
O2B-6Deficiency of thrombospondin-2 does not affectmurine adipose tissue angiogenesis or developmentvan Hul M and Lijnen HRKU Leuven, Leuven, Belgium
Thrombospondins (TSP) are large, secreted, multimodular, calcium-
binding glycoproteins that are believed to have in vivo anti-angiogenic
properties. Interestingly, TSP-2 is upregulated in gonadal adipose tis-
sue of obese mice and TSP-2 deficiency is associated with elevated
levels of MMP-2, that was recently shown to be involved in adipose
tissue development in mice. In this study we have evaluated the
potential contribution of TSP-2 to adipose tissue related angiogenesis
and fat development. Therefore, TSP-2 deficient (TSP-2-/-) and wild-
type littermate (TSP-2+/+) mice were kept on normal chow (SFD)
or on high fat diet (HFD) for 15 weeks, followed by analysis of sub-
cutaneous (SC) and gonadal (GON) fat.
TSP-2 deficiency had no significant effect on total body weight or on
SC or GON adipose tissue mass of mice kept on either SFD or
HFD. The composition of SC and GON adipose tissues of TSP-2-/-
and TSP-2+/+ mice was comparable in terms of size and density of
adipocytes or blood vessels. The lack of an effect of TSP-2 deficiency
could not be explained by compensatory increases of TSP-1 expres-
sion in the TSP-2-/- mice. TSP-2 deficiency had no effect on adipose
tissue mRNA expression of gelatinase A (MMP-2), whereas gelati-
nase B (MMP-9) was downregulated in SC and GON adipose tissues
of TSP-2-/- mice on HFD. Zymography with extracts of SC and
GON adipose tissues of both genotypes did, however, not reveal sig-
nificant differences in MMP-9 or MMP-2 activity.
Taken together, these data indicate that TSP-2 is not an important
mediator of adipose tissue associated angiogenesis or fat mass accu-
mulation.
O2B-7Polymerization of serine protease inhibitors iscritically dependent on structural stability of deeplyburied residues inside surface cavitiesSingh P, Jairajpuri MA and Khan MdSJMI, New Delhi, India
Serine proteinase inhibitors (Serpins) are a unique superfamily of
protease inhibitor whose native state is metastable state which trans-
forms into stable state when they inhibit target proteases. Serpins like
neuroserpin, antithrombin, alpha-1antitrypsin, alpha-antichymotryp-
sin,C1-inhibitors and plasminogen activator inhibitor are involved in
important biological processes like blood coagulation, fibrinolysis,
cell migration, cell differentiation, embryo implantation, competent
activation and tumour suppression. Mutation in serpins can lead to
aberrant intermolecular linkages that can compromise the specific
function and also lead to polymer formation. Polymerization of ser-
pin is associated with disease like emphysema/cirrhosis, angiodema,
familial dementia, chronic obstructive bronchitis and thrombosis.
Critical understanding of the factors and mechanisms promoting ser-
pin misfolding and those regulating serpins conformational changes
are essential for elucidating the etiology of serpin based diseases. In
this study we have taken a dataset of all the known naturally occur-
ring point mutants in serpins that are prone to polymerization. First
we did accessible surface area (ASA) analysis to know the status of
burial at these positions and showed that most of the amino acids
are completely buried residues in native state. A cavity based analysis
showed that these residues are generally present in cavities which
change in size during mechanism of inhibition and polymerization.
We calculated the corresponding free energy change due to point
mutation in these natural variants, and showed that overwhelming
majority of amino acids involved in polymerization destabilizes the
protein. A comprehensive cavity analysis of various conformational
states of serpin showed of a very large cavity in the shutter region of
polymerized and cleaved state but not in native, latent and cavity fill-
ing variants indicating their potential as target for hindering polymer-
ization. We further show that docking and experimental studies that
indeed cavities can be filled to retard the native to polymer transi-
tion.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
4 ORAL PAPERS____________________________________________________________________________________

Plenary Lectures (1)
O3-1The urokinase receptor: from structure-functionrelationships to in vivo imagingPloug MRigshospitalet, Copenhagen, Denmark
The urokinase-type plasminogen activator receptor (uPAR) is a gly-
colipid-anchored membrane glycoprotein that has been implicated in
a number of human pathologies, including dissemination of cancer.
uPAR belongs to the Ly-6/uPAR (LU) protein domain family and is
one of five multidomain members that are encoded by a small gene
cluster on chromosome 19q13 (1). The primary function of uPAR is
to focus uPA-mediated plasminogen activation to cell surfaces and
thus assist in extravascular fibrinolysis. Other proposed functions of
uPAR include stimulation of cell adhesion and migration by direct
interactions with the extracellular matrix. At the molecular level these
properties are accomplished by a high-affinity binding site for uPA
and a non-overlapping binding site for the somatomedin B domain in
vitronectin (Vn). A detailed structural insight into the molecular
interplay between uPAR, uPA and Vn has recently emerged from
crystallographic and biochemical studies on these complexes (2–5).
These studies clearly show that all three homologous LU-domains in
uPAR play important roles for the correct assembly of the composite
ligand-binding sites for uPA and Vn. Importantly, these studies also
define possible druggable target sites in uPAR for small molecules (5)
and provide guidelines for the development of small reporter probes
applicable for non-invasive imaging of uPAR expression in vivo by
positron emission tomography. In this presentation, I will review
recent advances in our knowledge of structure-function relationships
in the interaction between uPAR and its ligands (uPA and Vn) and
discuss how this information can guide translational research in pre-
clinical intervention studies of uPAR function.
1 Jacobsen & Ploug, Curr. Med. Chem. 2008; 15:2559–2573.
2 Llinas et al., EMBO J. 2005; 24:1655–1663.
3 Huai et al., Science 2006; 311:656–659.
4 Huai et al., Nat. Struct. Mol. Biol. 2008; 15:422–423.
5 Lin et al., J. Biol. Chem. 2010; 285:10982–10992.
O3-2Clinical relevance of fibrin structure for coagulationand fibrinolysisLord STUNC-Chapel Hill, Chapel Hill, NC, USA
The clinical relevance of fibrin structure has been demonstrated in
studies of populations with common diseases and individuals with
unusual diseases. The former, epidemiological studies link fibrin clot
structure to most, if not all, thrombotic diseases coronary artery dis-
ease, ischemic heart disease, stroke and thromboembolic disease. The
latter, represented by patients with Hemophilia where reduced throm-
bin generation manifests in an altered clot structure, link fibrin clot
structure to bleeding diseases. Studies of individuals with alterations
in fibrinogen structure and/or fibrinogen concentration link fibrin
structure to both bleeding and thrombotic diseases. Currently, how-
ever, the molecular pathophysiology that mediates these links
between fibrin structure and disease remains poorly defined. Bio-
chemical analyses have shown that many aspects of fibrin polymeriza-
tion influence clot structure. Polymerization is a kinetically controlled
process, influenced by the concentrations of thrombin and fibrinogen.
Understanding how the effective in vivo concentrations of thrombin
and fibrinogen are controlled and how these concentrations influence
polymerization provides a potential means to control clot structure.
Polymerization is mediated though specific interactions between fibrin
monomers and between early fibrin polymers. Identifying the nature
of these interactions may also provide a means to control clot struc-
ture. In addition, the link between structure and disease almost cer-
tainly reflects clot stability, but it is unknown whether susceptibility
to fibrinolysis or susceptibility to shear-induced fragmentation or
both is of greater consequence. Identifying the interactions that con-
trol clot endurance will provide opportunities to modify clot stability,
to enhance clot stability in bleeding diseases and control clot degra-
dation in thrombotic diseases.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
ORAL PAPERS 5____________________________________________________________________________________

Quality of Fibrin: Sensitivity to Lysis
O4A-1Role of fibrin clot structure in susceptibility to lysisAriens RAS, Ajjan R, Standeven KF, Uitte de Willige S, Mutch NJand Philippou HUniversity of Leeds, Leeds, UK
A blood clot is composed of an intricate matrix of fibrin fibres,
which twist and branch out to form a three-dimensional network
that holds the clot together. The structure of the fibrin clot plays a
major role in the resistance of the clot to fibrinolysis by plasmin.
Several methods including turbidity and confocal microscopy have
been developed to investigate the relationship between fibrin struc-
ture and lysis. Studies on fibrinogen polymorphisms, fibrinogen gly-
cation, fibrin cross-linking by FXIIIa, and polyphosphates have
shed light on mechanisms involved in the modulation of fibrinolysis
by fibrin structure. Factors that influence fibrinolysis include: (i) the
density or porosity of the fibrin network determines the speed at
which fibrinolytic factors permeate the clot, (ii) the binding of tissue
plasminogen activator, plasminogen, and other factors to fibrin can
be modified by fibrin structure, and (iii) cross-linking of a2-antiplas-min to fibrin by FXIIIa contributes to resistance of the clot to lysis.
In turn, the process of fibrinolysis itself influences the structure and
quality of fibrin, thereby providing interplay between proteolysis
and fibrin structure. Further studies are required to develop a more
complete understanding of the relationship between fibrin structure
and fibrinolysis and its role in thrombosis. Modulation of the resis-
tance of fibrin to lysis could provide an important mechanism by
which to enhance (natural or therapeutic) thrombolysis and reduce
the risk for thrombosis.
O4A-2Effects of total fibrinogen and fibrinogen c’ onthrombin generation in plasmaCastoldi E1, Uitte de Willige S2, Dirven RJ3, Ariens RAS2,Rosing J1 and Bertina R3
1Maastricht University, Maastricht, The Netherlands; 2University
of Leeds, Leeds, UK; 3Leiden University, Leiden, The
Netherlands
Background: The fibrinogen c’ isoform is characterised by a nega-
tively charged C-terminal tail that binds with high affinity to throm-
bin exosite II, thereby inhibiting some of thrombin’s procoagulant
activities (e.g. factor VIII activation). Therefore, fibrinogen molecules
containing this isoform (cA/c’, 10–15% of total fibrinogen) have an
anticoagulant as well as a procoagulant function.
Aim: To investigate the effects of total fibrinogen and fibrinogen c’on thrombin generation in plasma.
Methods: Purified human fibrinogen was purchased from a commer-
cial source. cA/cA and cA/c’ fibrinogen were separated using anion
exchange chromatography and depleted of FXIII by ammonium sul-
phate precipitation. Thrombin generation was measured in: (i)
whole and defibrinated normal plasma; (ii) fibrinogen-deficient
plasma reconstituted with increasing amounts of cA/cA or cA/c’fibrinogen; and (iii) normal plasma before and after addition of c’-derived synthetic peptides (wild-type, mono-sulfated wild-type,
reverse and truncated). Thrombin generation was initiated with
either tissue factor (TF) or kaolin and monitored continuously using
a fluorogenic substrate for thrombin (Calibrated Automated Throm-
binography).
Results: Comparison of thrombin generation curves obtained in full
and defibrinated plasma indicated that fibrinogen prolongs the lag
time and increases the peak height of thrombin generation. The same
was observed when fibrinogen-deficient plasma was reconstituted with
total fibrinogen. Titrations of the individual fibrinogen isoforms in
fibrinogen-deficient plasma suggested that these effects were largely
attributable to cA/c’ fibrinogen. Accordingly, the wild-type c’ peptide(especially if sulfated) dose-dependently prolonged the lag time and
increased the peak height of thrombin generation, while the truncated
and reverse peptides were ineffective. All effects were more pro-
nounced when thrombin generation was initiated with kaolin or with
a low TF concentration, where the intrinsic pathway (factor VIII)
importantly contributes to thrombin formation. Differently, hardly
any effect of fibrinogen was observed at high TF concentrations. In
line with the effect of fibrinogen on the lag time of thrombin genera-
tion (which is a measure of the clotting time), the (sulfated) wild-type
c’ peptide also dose-dependently prolonged the aPTT but not the PT
of normal plasma.
Conclusions: Fibrinogen (particularly cA/c’) prolongs the lag time
and increases the peak height of thrombin generation initiated with
kaolin or with a low TF concentration. While the prolongation of
the lag time illustrates the anticoagulant action of fibrinogen, the
increase in peak height is likely due to the fact that fibrin-bound
thrombin is protected against inhibition by antithrombin.
O4A-3Clots formed from c’-fibrinogen are resistant to lysisbecause of impaired plasminogen activation by t-PAKim PYS, Leslie BA, Stafford AR, Vu T, Fredenburgh JC andWeitz JIThrombosis and Atherosclerosis Research Institute, McMaster
University, Hamilton, Canada
Background: About approximately 15% of circulating fibrinogen
contains a c-chain variant with an extended C-terminus and is desig-
nated c’-Fg. Although fibrin clots formed from c’-Fg have been
reported to be more resistant to lysis than those prepared from the
predominant cA-Fg, the mechanism responsible for this difference is
unknown.
Methods: Samples containing cA- or c’-Fg at various concentrations,
plasminogen, tissue-type plasminogen activator (t-PA) and a2-anti-plasmin were incubated with thrombin and CaCl2 at 37 �C and tur-
bidity was monitored at 400 nM. The time to half maximal decrease
in turbidity was designated as the lysis time. Similar experiments were
performed using (i) plasmin instead of plasminogen/t-PA, and (ii)
batroxobin, a snake venom extract that only releases fibrinopeptide-
A from fibrinogen, instead of thrombin, which releases both fibrino-
peptides-A and -B.
Results: t-PA-mediated lysis times increased with higher concentra-
tions of both cA- or c’-Fg, but the lysis times of clots formed from
c’-Fg were 1.4-fold longer than those from cA-Fg. This difference
was lost when plasmin was substituted for t-PA/plasminogen or
when batroxobin was substituted for thrombin. These findings sug-
gest that the slower lysis of clots formed from c’-Fg results from
reduced capacity to stimulate plasminogen activation by t-PA and
that this is attributable to impaired fibrinopeptide-B release from
c’-Fg.Conclusion: Our findings suggest that (i) fibrinopeptide-B release is
an important determinant of the capacity of fibrin to serve as a stim-
ulator of plasminogen activation by t-PA, thereby supporting the
concept that fibrinopeptide-B release exposes cryptic t-PA and/or
plasminogen binding sites on fibrin, and (ii) the relative resistance of
clots formed from c’-Fg to lysis reflects impaired fibrinopeptide-B
release. Therefore, these studies provide additional insight into the
stimulatory effects of fibrin on plasminogen activation by t-PA, and
suggest that c’-Fg levels may be an important determinant of the
resistance of thrombi to lysis.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
6 ORAL PAPERS____________________________________________________________________________________

O4A-4Hampered dissolution of fibrin formed undermechanical stressKolev K1, Varju I1, Szabo L2, Machovich R1, Silva M3 andLongstaff C3
1Semmelweis University, Budapest, Hungary; 2Chemical
Research Center, Hungarian Academy of Sciences, Budapest,
Hungary; 3National Institute for Biological Standards and
Control, South Mimms, Potters Bar, UK
Recent data indicate that stretching forces cause a dramatic decrease
in clot volume accompanied by gross conformational changes of
fibrin structure. The present study attempts to characterize the lytic
susceptibility of fibrin exposed to mechanical stress. The relevance of
these structural variants was substantiated by scanning electron
microscopic (SEM) evaluation of human thrombi removed during
surgery. In 40% of the examined thrombi the fibrin fibers on the sur-
face of the clot were oriented in the direction of the shear forces
resembling fibrin architecture observed under clot stretching, whereas
the interior fibers formed a random 3D spatial meshwork. For our in
vitro dissolution studies these structural variations were modelled
with fibrin prepared in elastic silicon rubber tubes, which allow
adjustable mechanical stress. Following 2- and 3-fold longitudinal
stretching (2 · S, 3 · S) the volume of the fibrin clot decreased by
90% and in parallel the median fiber diameter and pore area in the
SEM images of the fibrin network decreased 2- to 3-fold. Application
of tissue plasminogen activator (tPA) to the surface of the clot, which
contains plasminogen, resulted in plasmin generation which was mea-
sured in the fluid phase. After 30 min activation 12.6 pmol/mm2 plas-
min was released from the non-stretched clot (NS), 5.5 pmol/mm2
from 2 · S and 2.3 pmol/mm2 from 3 · S clot. In the initial 15 min
of tPA-initiated fibrin lysis 160 ng/mm2 fibrin degradation products
were released from NS fibrin and 47 ng/mm2 from both 2 · S and
3 · S clots. Confocal microscopic images of fibrin surfaces showed
that a green fluorescent protein-fusion variant of tPA accumulated in
the interfacial layer of NS fibrin but not stretched fibrin. In conclu-
sion, mechanical stress confers proteolytic resistance to fibrin, which
is related to hampered tPA binding and penetration in the denser
fibrin network and consequently modified plasminogen activation at
the fluid-gel interface.
O4A-5Composition of coronary thrombi in acute myocardialinfarctionSilvain J1, Collet JP1, Nagaswami C2, Beygui F1, Edmondson K2,Bellemain-Appaix A1, Pena A1, Barthelemy O1, Montalescot G1
and Weisel JW2
1INSERM CMR937, Pitie-Salpetriere Hospital (AP-HP),
Universite Paris 6, Paris, France; 2University of Pennsylvania
School of Medicine, Philadelphia, PA, USA
Background: The dynamic process of intracoronary thrombus forma-
tion in ST-elevation Myocardial Infarction (STEMI) patients is
poorly understood. While it is known that time is of the essence in
the treatment of these patients, the reasons are poorly understood.
Methods and Results: Intracoronary thrombi (n = 45) were obtained
by thromboaspiration in 288 consecutive STEMI patients presenting
for primary percutaneous intervention (PCI) within 12 h of symptom
onset. Thrombi were analyzed using high definition pictures taken
with a scanning electron microscope. Plasma biomarkers (TnI,
CRPus, IL-6, PAI-1, sCD40 ligand and TNF-a) and plasma fibrin
clot viscoelastic properties were measured simultaneously on periph-
eral blood.
Thrombi were composed of fibrin (55.918%), platelets (16.818%),
erythrocytes (11.59%), cholesterol crystal (5.28.4%) and leukocytes
(1.32.0%). The median ischemic time from symptom onset to PCI
was 175 min (IQR 140–297). Ischemic time impacted thrombi compo-
sition, resulting in a positive correlation with intracoronary thrombus
fibrin content, r = 0.38, P = 0.01 and a negative correlation with
platelet content r = -0.34, P = 0.02. Thus, fibrin content increased
with ischemic time, ranging from 48.421% (< 3 h) up to 66.99%
(> 6 h) (P = 0.02), while platelet content decreased from 24.923%
(< 3 h) to 9.16% (> 6 h) (P = 0.07). The platelet activation marker
sCD40 ligand was positively correlated to platelet content in the
thrombus (r = 0.40, P = 0.02) and negatively correlated with fibrin
content (r = -0.36; P = 0.04). Multivariate analysis indicated that
ischemic time was the only predictor of thrombus composition with a
2-fold increase of fibrin-rich thrombus per ischemic hour [adjusted
OR2 (1.03–3.7) P = 0.01].
Conclusions: In acute STEMI, platelet and fibrin contents of the
occlusive thrombus vary over time, which may have a direct impact
on the efficacy of drugs or devices used for coronary reperfusion. For
example, these results show that the decreased effectiveness of throm-
bolytic drugs with time from onset of symptoms is likely due to an
increase in fibrin content of the thrombi over time.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
ORAL PAPERS 7____________________________________________________________________________________

Fibrinolysis and Innate Immunity
O4B-1Fibrinolysis and innate immunityvan der Poll TAcademic Medical Center, University of Amsterdam,
Amsterdam, The Netherlands
Components of the fibrinolytic system have properties that go
beyond fibrinolysis. In this lecture the roles of several fibrinolytic
mediators in in vivo models of severe infection will be discussed.
Plasminogen activator inhibitor type I (PAI-1) has been implicated in
the pathogenesis of sepsis as elevated circulating PAI-1 levels are
highly predictive for an unfavourable outcome in sepsis patients.
Recently, studies using PAI-1 deficient mice and mice with transiently
enhanced expression of PAI-1 have pointed to a protective rather
than a detrimental role of this mediator in severe gram-negative
pneumonia and sepsis. PAI-1 deficiency impaired host defense during
Klebsiella pneumonia and sepsis as reflected by enhanced lethality and
increased bacterial growth and dissemination in mice with a targeted
deletion of the PAI-1 gene. Conversely, transgenic overexpression of
PAI-1 in the lung using a replication defective adenoviral vector
markedly improved host defense against Klebsiella pneumonia and
sepsis.
Tissue-type plasminogen activator (tPA) has been found to affect
antibacterial defense during abdominal sepsis caused by Escherichia
coli in mice: tPA deficient mice demonstrated an impaired defense
against E. coli peritonitis as indicated by higher bacterial loads and a
reduced survival. The protective function of tPA was independent of
its capacity to convert plasminogen into plasmin since plasminogen
gene deficient mice were indistinguishable from Wt mice in this
model. Similarly, pulmonary overexpression of human tPA markedly
improved host defense against Klebsiella pneumonia.
The urokinase-type plasminogen activator receptor (uPAR) mediates
leukocyte adhesion to the vascular wall or extracellular matrix com-
ponents. UPAR deficient mice demonstrated a strongly reduced neu-
trophil influx in models of bacterial pneumonia, which was
accompanied by an enhanced growth and dissemination of bacteria.
Conclusion: Mediators of the fibrinolytic system impact on innate
immunity by various mechanisms that at least in part are unrelated
to their function in lysis of fibrin clots.
O4B-2The occupancy of EPCR by protein C switches thePAR-1-dependent proinflammatory function ofthrombin to a protective responseRezaie RSt. Louis University School of Medicine, St. Louis, MO, USA
Thrombin is a multifunctional enzyme in plasma which clots fibrin-
ogen to stop bleeding during vascular injury. In addition to this
role, thrombin also regulates the anticoagulant and fibrinolytic path-
ways when it binds to its high affinity endothelial cell surface recep-
tor thrombomodulin (TM) to activate two plasma zymogens,
protein C and thrombin-activatable fibrinolysis inhibitor. Thrombin
also regulates inflammatory pathways when it activates the G-pro-
tein coupled receptor, protease-activated receptor 1 (PAR-1),
expressed on the surface of endothelial and other cell types. The
traditional view is that the activation of PAR-1 by thrombin on
vascular endothelial cells initiates a series of intracellular signaling
responses that culminate in the activation of the nuclear factor-jB(NF-jB) pathway, disruption of cellular permeability and expression
of proinflammatory molecules by endothelial cells. However, we
recently demonstrated that the PAR-1-dependent proinflammatory
signaling function of thrombin, observed in vitro in the endothelial
cell-culture systems, may not reflect a true physiological response
for thrombin based on the observation that the occupy of endothe-
lial protein C receptor (EPCR) by its natural ligand protein C
potently inhibited the PAR-1-dependent barrier enhancing and pro-
inflammatory functions of thrombin in the same cellular models.
Interestingly, we now demonstrate that the EPCR occupancy also
inhibits the PAR-1-dependent rapid release of P-selectin and
angiopoietin 2 (Ang2) from Weibel-Palade bodies, thereby down-
regulating the interaction of neutrophils with endothelium and up-
regulating the Ang1/Tie2 protective signaling pathway. Furthermore,
we demonstrate that the pretreatment of endothelial cells with the
catalytically inactive Ser-195 to Ser mutant of the zymogen protein
C leads to the PAR-1-dependent up-regulation of expression of
both Ang1 and Tie2 in endothelial, the same response which has
been attributed to activated protein C. Based on our results, we
hypothesize a PAR-1-dependent protective role for the low con-
centrations of thrombin in maintaining the integrity of the EPCR-
containing vasculature.
O4B-3The human fibrinolytic system is a target forproteases secreted by the pathogenic bacteriumPseudomonas aeruginosaMagdolen V, Seweryn P, Schmitt M and Beaufort NTechnical University Munich, Muenchen, Germany
A number of pathogenic bacteria interact with and engage the host
matrilytic and fibrinolytic plasminogen activation system. We hypoth-
esized that proteases secreted by Pseudomonas aeruginosa might con-
tribute to the activation of this major extracellular proteolytic
system, thereby participating in host tissue destruction and bacterial
dissemination.
We observed that the pseudomonal thermolysin-like metalloprotease
LasB converts the human zymogen of the urokinase-type plasmino-
gen activator (uPA), into its active form. Accordingly, while the sec-
retome from a LasB-expressing strain efficiently activates pro-uPA,
the secretome from an isogenic LasB-deficient strain is markedly less
potent in pro-uPA activation. Still, both secretomes induce some me-
talloprotease-independent activation of the human zymogen. This
later involves a trypsin-like protease, which we identified as the serine
protease ‘protease IV’(PIV).
Along with this, LasB converts plasminogen into mini-plasminogen
and angiostatin-related species, while, as previously reported, it pro-
cesses the uPA receptor, inactivates the plasminogen activator inhibi-
tor 1, and activates pro-matrix metalloproteinase 2. By contrast, PIV
does not target these factors at all.
To conclude, LasB and PIV, although belonging to different protease
families, both target and activate the host fibrinolytic system, a path-
way that is likely to contribute to bacterial virulence.
O4B-4Fibrinolysis impairs host defense during severemurine gram-negative sepsis (melioidosis)Kager M, Wiersinga WJ, Roelofs JJ, van t Veer C andvan der Poll TAcademic Medical Center, Amsterdam, The Netherlands
Background: Melioidosis, an endemic disease in Southeast Asia, is
caused by the gram-negative bacterium Burkholderia (B.) pseudomal-
lei. Melioidosis is associated with pneumonia and bacterial dissemina-
tion to distant sites, often leading to severe sepsis. Our previous work
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
8 ORAL PAPERS____________________________________________________________________________________

(Wiersinga et al. JTH 2008; 6: 32) revealed that infected patients
demonstrate evidence of coagulation activation with concurrent inhi-
bition of fibrinolysis. Mediators of fibrinolysis may not only influence
coagulation during infection but also leukocyte function.
Objective: To investigate the role of different proteins involved with
fibrinolysis during murine infection with B. pseudomallei, in particular
the role of tissue-type plasminogen activator, plasminogen activator
inhibitor type 1 (PAI-1) and a2-antiplasmin (A2AP).
Methods: Normal wild-type mice and mice deficient for either tPA,
PAI-1 or A2AP were infected intranasally with B. pseudomallei to
induce melioidosis. Mice were sacrificed after 24, 48 or 72 h and sur-
vival studies were performed. Lungs, liver, spleen and plasma were
harvested to measure bacterial loads, cellular influxes, pathology
scores, cytokine levels and coagulation parameters.
Results: tPA knockout (KO) mice, having less basal fibrinolysis, had
a strong survival advantage compared to wild-type mice. They also
had less bacterial outgrowth in liver and blood together with an anti-
inflammatory cytokine profile in the blood. On the contrary, both
PAI-1 KO mice and A2AP KO mice, that both have enhanced basal
fibrinolysis, showed significantly more bacterial outgrowth and a pro-
inflammatory cytokine profile in lungs and blood 48 and 72 h after
inoculation. Moreover, in PAI-1 KO mice a non-lethal bacterial load
appeared to be lethal during a survival study.
Conclusion: Fibrinolysis is an important component of the host
response during melioidosis. Our murine studies show that both tPA,
PAI-1 and A2AP play crucial roles, showing that less fibrinolysis
seems to be beneficial during this infection. Targeting fibrinolysis
could be a new therapy for this severe disease.
O4B-5Caveolin deficiency leads to increased activation ofcoagulation and decreased fibrinolysis in miceLupu F1, Lupu C1, Ivanciu L1 and Lijnen HR2
1Oklahoma Medical Research Foundation,Oklahoma City, USA;2Center for Molecular and Vascular Biology, Katholieke
Universiteit Leuven, Leuven, Belgium
Caveolin 1 (CAV1) is the main organizer of the specialized vesicular
microdomains of plasmalemma, named caveolae that are involved in
a variety of cellular processes. We have shown previously that caveo-
lae regulate the initiation of coagulation by controlling the endothe-
lial cell (EC)-bound TFPI. Here we used CAV1 deficient mice to
study the in vivo role of caveolin in the regulation of hemostasis in
normal and experimental inflammation. CAV1 knockout (CAV1-/-)
and wild type (WT) mice were challenged with LPS (1 mg/kg body
weight) or exposed to hypoxia. We observed that in contrast to WT
mice, non-challenged CAV1-/- animals have increased plasma fibrino-
gen consumption and fibrin deposition in the lung. Thrombin-anti-
thrombin and D-dimer levels confirmed that CAV1-/- mice have a
prothrombotic state that is further increased after LPS challenge.
In vitro analysis of immortalized lung microvascular EC from WT
and CAV1-/- mice incubated with/without LPS showed that EC of
CAV1-/- mice had less TFPI on the cell surface, and higher
TF-dependent coagulant activity than EC isolated from WT mice.
Zymography assay for plasmin generation on lung cryosections dem-
onstrated lower levels of t-PA dependent plasmin generation in
CAV-/- mice as compared to WT. Tissue and plasma analysis of
t-PA, u-PA and PAI1, measured at mRNA, protein and enzyme
activity levels suggest that the observed decrease in plasmin genera-
tion is due to decreased t-PA and increased PAI-1 production in
CAV1-/- mice. En-face confocal microscopy also showed less t-PA
staining. Quantitation of t-PA protein in lung homogenates con-
firmed that CAV1-/- mice have 2.5-fold less t-PA than WT mice. The
observed increased PAI-1 plasma levels correlate with higher PAI-1
mRNA expression in the liver of CAV1-/- mice.
In conclusion, our data demonstrate that CAV1 deficiency in mice
leads to increased activation of coagulation due to impaired TFPI
function and decreased t-PA dependent fibrinolysis.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
ORAL PAPERS 9____________________________________________________________________________________

Massive Hemorrhage in the Intensive Care: Treatment, Diagnostic
Methods and Basic Science
O5A-1Introduction: bleeding and thromboelastographyten Cate HDepartment of Internal Medicine and Cardiovascular Research
Institute Maastricht, Maastricht University Medical Center, The
Netherlands
Bleeding is a major source of health related morbidity and costs in
patients undergoing surgery and/or being treated with antithrombotic
medication. In addition, in rare congenital diseases like the hemophi-
lias, bleeding is a potential life threatening event. In all these situa-
tions, specific derangements of the blood coagulation system occur.
However, the attending physician is not always aware of these hemo-
static defects, which explains why major bleeding complications can
occur without adequate preparative measures being taken.
One of the laboratory methods that have been advocated for guiding
major surgical procedures, a major source of postoperative bleeding,
is thromboelastography (TEG). TEG, of which several commercial
applications have been developed (e.g. TEG� or ROTEM�), is one
of the so called capacity assays that reflect a major part of the blood
coagulation system ex vivo. This means that TEG quantifies both the
initiation, amplification and propagation phases of fibrin clot forma-
tion, but also gives options for measuring fibrinolysis upon addition
of clot lysing compounds. All these phases of blood clotting can be
expressed as specific variables, providing a pattern of clot formation
and lysis that reflects certain clinical conditions. TEG was already
clinically applied in 1985 and several algorithms have been published
in which clinical management after surgery was guided by TEG mea-
surements. However, in spite of its longtime application controlled
clinical studies are scarce. Such published small scale studies of mod-
erate quality suggest that there is some benefit to obtain when using
algorithm based TEG in the surgical arena, showing a tendency
towards reduced need for transfusion of blood products as a main
outcome. There remains however a strong need for properly designed
controlled trials to unequivocally demonstrate the clinical benefit in
terms of reduced bleeding and costs, for TEG, also in comparison to
other capacity assays like platelet function tests or thrombin genera-
tion assays.
O5A-2The clinical problem and trials with fibrinogenRahe-Meyer NHannover Medical School, Hannover, Germany
Until 2000 it was internationally agreed that the critical fibrinogen
plasma level in intraoperative bleeding were 1 g/L or even lower.
Fibrinogen concentrate was only available in some countries, fibrino-
gen therapy with plasma or cryo was tertiary after therapy with
platelets and thrombin generating enzymes, and observational data
seemed to confirm this. Since 2000 fibrinogen concentrate have
become more available, more clinicians experienced successful bleed-
ing therapy targeting at higher fibrinogen plasma levels, and corre-
sponding data were published.
The planning of clinical trials with fibrinogen is complicated by a set
of problems:
1 Intraoperatively acquired coagulation disorders are multi dimen-
sional – how can you examine only one coagulation factor?
2 Intraoperative bleeding situations are dynamic and standard labo-
ratory test take to much time – how can you rapidly measure the
fibrinogen level to guide your therapy?
3 How can you intraoperatively quantify bleeding to trigger the ther-
apy and to control its success?
4 Which target levels should be used and how can dosing be calcu-
lated?
Two recently published studies will be discussed. A FIBTEM-guided
post-cardiopulmonary bypass administration of fibrinogen concen-
trate in aortic surgery 1,2 as a first-line therapy of microvascular
bleeding had been performed there. In their study design answers
were given to the questions above. They have resulted in:
1 Improved intraoperative management of coagulopathic bleeding
2 Reduced requirements for allogeneic blood product transfusion
3 Reduced 24-h drainage volume
4 Efficacious first-line therapy (even under the conditions of reduced
thrombin generation and platelet function)
5 No thrombotic events even with fast, high dose administration of
fibrinogen concentrate.
There is emerging evidence that fibrinogen concentrate may prove
effective in the management of perioperative bleeding in cardiac
surgery. The application to other kinds of surgery is yet to be estab-
lished.
1 Rahe-Meyer N et al., J. Thorac. Cardiovasc. Surg. 2009; 138:694–
702.
2 Rahe-Meyer N et al., Br. J. Anaesth. 2009; 102:785–92.
O5A-3The effect of blood plasma substitutes on fibrinstructureFenger-Eriksen C1 and Sørensen B2
1Aarhus University Hospital, Aarhus, Denmark; 2Haemostasis
Research Unit, St. Thomas Hospital, London, UK
Introduction: Artificial plasma expanders like hydroxyethyl starch
(HES) or dextrans is often required in massively bleeding patients to
maintain haemodynamic stability. Blood loss and fluid resuscitation
dispose to development of dilutional coagulopathy through dilution,
loss and consumption of coagulation factors and cells involved in the
haemostatic procress. In addition specific adverse effect from HES
fluid resuscitation on fibrinogen function and fibrin polymerisation
has been reported in more studies.
Impact of colloids and crystalloids on fibrin polymerisation
An in vitro comparative analysis of whole blood haemodilution with
isotonic saline versus artificial colloids verified a coagulopathy char-
acterized by suppressed clot firmness, but unchanged clot initiation
and parameters of clot propagation, as evaluated by thromboelas-
tometry.
Similar thromboelastometric characteristics have been reported from
a study including 20 bleeding patients receiving fluid resuscitation
with HES until a dilution level at 30%. The same study reported that
levels of fibrinogen decreased significantly below the levels expected
from dilution. In another human study including 66 patients under-
going orthopaedic surgery fibrin polymerisation, as measured by
thromboelastometry, was significantly impaired in the group receiving
colloids as compared with Ringers lactate (1).
A series of laboratory, animal, retrospective as wells one randomized
controlled trial all have shown that fibrinogen concentrate restored
clot strength, re-established the architecture of the fibrin meshwork.
Intervention with fibrinogen concentrate has been shown to reduce
blood loss in a pig model of massive bleeding and to decrease trans-
fusion requirements in bleeding patients (2).
Conclusion: Artificial colloids impair haemostasis more than crystal-
loids. Acquired fibrinogen deficiency caused by fibrin polymerisation
defect seems to be the leading determinant in colloid induced dilu-
tional coagulopathy.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
10 ORAL PAPERS____________________________________________________________________________________

1 Mittermayr M, Streif W, Haas T, Fries D, Velik-Salchner C, Klin-
gler A, et al., Hemostatic changes after crystalloid or colloid fluid
administration during major orthopedic surgery: the role of fibrino-
gen administration. Anesth. Analg. 007 Oct;105(4):905–17.
2 Fenger-Eriksen C, Ingerslev J, Sorensen B. Fibrinogen concentrate
– a potential universal haemostatic agent. Expert Opin. Biol. Ther.
2009; 9(10).
O5A-4Thrombelastography-based monitoring for massiveblood loss in children during elective surgery forcraniosynostosis repair, TEG�versus ROTEM�
Machotta A1, Geerts J2, Grimminck B2, Stigter RL2, Poley MJ3,Al MJ3 and Appel IM2
1Department of Anaesthesiology; 2Department of Paediatirc
Oncology/Haematology; 3The institute for Medical Technology
Assessment (iMTA), Erasmus MC/ Sophia Children’s Hospital,
Erasmus University Medical Centre, Rotterdam, The Netherlands
The re-introduction of thromboelastography (TEG) has led to
decreased transfusions of blood products in adults. No systematic
studies on TEG and TEG-guided intervention during pediatric sur-
gery have been done. Using citrated blood, we compared TEG/Hae-
moscope and ROTEM/Pentapharm in a prospective study of 44
otherwise healthy children with craniosynostosis undergoing elective
surgery at the Sophia Children’s Hospital. Blood samples (5 mL from
an arterial line) for TEG and ROTEM measurement were obtained
after: induction of anesthesia (T1), Ringer’s LS 10 mL/kg (T2), Veno-
fundin to a maximum of 30 mL/kg (T3), transfusion of red blood
cells (T4), and FFP (T5). Between T2 and T3 all children demon-
strated a significant decline in Hb from mean 6.5 to 3.8 mmol/L
(P < 0.0005). The blood loss was mean 440 mL, requiring mean
220 mL transfusion of red blood cells. TEG and ROTEM parameters
pointed equally to dilutional coagulopathy, no signs of fibrinolysis.
Paired Students t-test demonstrated earlier significant changes in RO-
TEM, but most relevant changes from T2-T3 were equally highly sig-
nificant in both devices.
Table 1 for O5A-4
TEG� ROTEM�-INTEM ROTEM�-EXTEM
T1–T2R 6.3–6.0 min
K 1.9–1.7 min
a 65–66 �MA 62–61 mm
CT 159–154 s
CFT 62–69 s*
a 77–76 �MCF 63–61 mm*
CT 60–62 s
CFT 84–94 s*
a 73–71 �*MCF 61–59 mm*
MA-FF 19–19 FIBTEM-MCF 14–13*
T2–T3R 6.0–6.0
K 1.7–2.8*
a 66–58**
MA 61–48**
CT 154–170*
CFT 69–165**
a 76–62**
MCF 61–49**
CT 62–94**
CFT 94–170**
a 71 –60**
MCF 59–48**
MA-FF 19–6.2**FIBTEM-MCF 13–5.2**
T3–T4R 6.0–6.1
K 2.8–4.7*
a 58–42**
MA 48–42*
CT 170–193**
CFT 165–278*
a 62–54*
MCF 49–41**
CT 94–123*
CFT 170–302*
a 60–53*
MCF 48–41**
MA-FF 6.2–5.4* FIBTEM-MCF 5.2–4.5*
T4–T5R 6.1–5.9
K 4.7–3.1*
a 42–55**
MA 42–47*
CT 193–153*
CFT 278–195
a 54–59*
MCF 41–46*
CT 123–83*
CFT 302–212*
a 53–55*
MCF 41–46**
MA-FF 5.4–7.0* FIBTEM-MCF 4.5–5.6*
*P < 0.05 **P < 0.0001
O5A-5Fibrinogen and post-partum hemorrhage: fromprediction to treatmentDucloy-Bouthors AS, Pilla C, Bauters A, Wibaut B and Jude BCentre Hospitalier Regional et Universitaire, Lille, France
Post-partum hemorrhage (PPH) remains a major cause of maternal
morbidity and mortality. Charbit et al (1) have shown the decrease of
fibrinogen to be an early predictor of the severity of PPH. Early diag-
nosis of the hypofibrinogenemia is facilitated by thromboelastometry
ROTEM (Pentapharm Germany).(2). The correction of coagulation
disorders associated with the uterotonic treatment, could improve the
PPH evolution but it is not yet demonstrated (3). We report a clinical
observation illustrating the follow up of the coagulopathy’s treat-
ment.
Case report: Mrs H.M. was a 36 years. primiparus. A large fibroma
and anterior placenta praevia had been discovered during pregnancy.
Caesarean section had to be transplacental. Prophylactic uterine arte-
rial catheters were placed. The caesarean section lasted 90 min and
2500 mls bleeding was compensated by 2500 mls vascular loading
with colloids. Abdominal haemorrhage started again 3 h later. Embo-
lization was performed promptly and succeeded to stop the uterine
and hypogastric arterial flow but haemorrhage continued up to
4500 mls. Severe hypofibrinogenemia < 0.5 g/L (N: 2.9–7 g/L) and
nul FIBTEM amplitude (N: 20–35 mm) was treated gradually by
repeated injections of fibrinogen concentrate and antifibrinolytic
drug, then fresh frozen plasma, platelet concentrate and recombinant
activated factor seven (rFVIIa). Close biological and thromboelasto-
metric monitoring of each step of the procoagulant treatment was
realized. Although the ph, temperature, platelet count and calcium
had been maintained in normal range, rFVIIa failed to stop the
abdominal haemorrhage till the plasma fibrinogen level reached a
baseline range of 1.9 g/L and FIBTEM amplitude 11 mm.
Conclusion: In this PPH, a closed follow-up of the hypofibrinogen-
emia and its treatment efficacy has been useful for the clinician and
has contributed to complete the embolization and to avoid hysterec-
tomy.
1 Charbit D, Mandelbrot L, Samain E, Baron G, Haddaoui B et al.,
The decrease of fibrinogen is an early predictor of severity oh post-
partum haemorrhage. J.Thromb. Haemost. 2007; 5:266–73.
2 Huissoud C, Carrabin N, Audibert F, Levrat A, Massignon D,
Berland M, Rudigoz R-C. Bedside assessment of fibrinogen level in
postpartum haemorrhage by thrombelastometry. BJOG 2009;
116:1097–1102.
3 WHO guidelines for the management of post-partum haemorrhage
and retained placenta. WHO Library cataloguing 2009; WQ 330.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
ORAL PAPERS 11____________________________________________________________________________________

Cellular Proteolysis
O5B-1Update on the clinical relevance of the plasminogenactivation system in cancerSchmitt MTechnical University of Munich, Munich, Germany
Today’s integration of cancer-associated biomarkers into disease
management of cancer patients differs from cancer policies several
years ago. Different than before, personalized, tailored patient care is
now in focus of cancer medicine, observing detailed information
about a patient’s gene and/or protein expression profile, to allow
identification of patients at risk. Substantial progress has come
through molecular biology techniques, providing gene and/or protein
signatures of molecular alterations in each patient’s tumor. Though,
to allow personalized treatment of cancer patients, we need signifi-
cant, validated biomarkers to determine the course of the disease and
to predict response to a given therapy.
Regarding this issue, the prognostic/predictive value of cancer bio-
markers uPA (urokinase-type plasminogen activator) and its inhibitor
PAI-1, which are key members of the plasminogen activation system,
determined by ELISA in tumor tissue extracts, to tailor individual-
ized cancer therapy, was convincingly shown for several cancer types
in numerous clinically relevant, validated retrospective and prospec-
tive studies. Most of the research on clinical utility of uPA, its recep-
tor uPAR (CD87), and its inhibitor PAI-1 has been centered on
breast cancer specimens, resulting in a multicenter breast cancer ther-
apy trial (Chemo-N0) and an international multicenter pooled analy-
sis surveying original follow-up data of patients with either high or
low uPA/PAI-1 antigen values. Consequently, for the first time ever
for any cancer biomarker, for breast cancer, uPA and PAI-1 were
awarded the highest level of evidence, LOE-1.
Another international clinical trial, NNBC3, aiming at treating 4150
high-risk breast cancer patients stratified by high uPA/PAI-1 has fin-
ished recruitment. A second, still ongoing large chemotherapy trial
(Plan B) is comparing the clinical effectiveness of uPA/PAI-1 versus
the 21-gene test Oncotype DX. An orally applicable small synthetic
molecule (Mesuprone) directed towards the proteolytic activity of
uPA is currently in phase II clinical trials in patients afflicted with
different types of advanced cancer.
O5B-2Extracts of echinococcus multilocularis cysts induceproliferation and protease expression of humanumbilical vein endothelial cells in vitroMahdy Ali K1, Kaun C1, Rychli K2, Hohensinner PJ3, Weiss T4,Auer H5 and Wojta J1
1Medical University of Vienna; 2University of Veterinary
Medicine, Vienna, Austria; 3Vesalius Research Center,
K.U. Leuven, Leuven, Belgium; 4Center for Clinical Heart
Research, Ulleval University Hospital, Oslo, Norway;5Department of Hygiene, Medical University of Vienna, Vienna,
Austria
Objective: Echinococcus multilocularis (E. multilocularis), one of the
most dangerous helminthic parasites, causes alveolar echinococcosis
affecting the liver and destroying the parenchyme. In alveolar echino-
coccosis tumor-like cysts grow beyond the organic borders and
invade attached organs. Vascularization is essential for tumor
growth, therefore induction of angiogenesis is a common feature of
many tumors. For angiogenesis to succeed proteolysis of extracellular
matrix is essential. The aim of our study was to investigate possible
angiogenic properties of E. multilocularis and to detect a possible
involvement of proteolytic proteins in this process.
Methods: Human umbilical vein endothelial cells (HUVEC) were
treated with the extract of homogenized E. multilocularis cysts grown
in mice at different concentrations for 72 h. Cell proliferation was
quantified using a proliferation assay (EZ4U�; Biomedica) Tube for-
mation of HUVEC grown on Matrigel� in the absence or presence
of echinococcal cyst extract was determined. Quantitative PCR analy-
sis was performed to detect specific mRNA for urokinase type of
plasminogen activator (uPA), uPA receptor (uPAR) and matrix me-
talloproteinase 1 (MMP-1) in stimulated HUVEC.
Results: HUVEC treated with the extract showed increased prolifera-
tion (up to 2.3-fold) and capillary tube formation in comparison to
untreated HUVEC. Quantitative PCR revealed a significant increase
in mRNA levels specific for uPA (up to 4-fold), uPAR (up to 4.6-
fold) and MMP-1 (up to 7.6-fold).
Conclusion: We could show for the first time that echinococcal cyst
extract induces proliferation and tube formation of HUVEC in vitro.
Furthermore we could show an increased expression of several prote-
olytic molecules in such treated HUVEC, namely uPA, uPAR and
MMP-1, which are known to modulate angiogenesis. We speculate
that the helminthic parasite E. multilocularis has the ability to induce
angiogenesis and that the uPA/uPAR system as well as the MMP
system may be critically involved in the tumor-like growth of this
parasite.
O5B-3Modulation of uPAR signaling to ERK/MAPK byendocytic receptors of the LDLR familyGeetha N1, Mihaly-Bison J1, Blasi F2 and Binder BR1
1Medical University of Vienna, Vienna, Austria; 2Molecular
Genetics Unit, DIBIT- San Raffaele Hospital, Milan, Italy
The interactions of uPA/uPAR/PAI-1 complex, with transmem-
brane receptors lead to the activation of intracellular signaling
machinery like MAP kinases. Active recombinant PAI 1 induces
uPA/uPAR dependent sustained activation of ERK1/2 in an other-
wise PAI-1 free system through LDLR family members. This
sustained ERK1/2 activation was accompanied by translocation of
ERK 1/2 into the nucleus and focal adhesions and led to increased
adhesion. Now we wanted to address the question whether
activation of the MAP Kinase pathway by RTK can also become
sustained by simultaneous LDLR signalling. Therefore we mim-
icked the PAI mediated sustained ERK1/2 activation by combining
a RTK type (EGF – EGFR) and a scavenger receptor type [Lac-
toferrin (LF) – LDLR] signalling. We found a RAP dependent
sustained activation of ERK 2, but not of ERK1, upon stimula-
tion with EGF & LF together in human fibrosarcoma cell line
HT-1080 in a time dependent manner leading to an increased
adhesion on Vitronectin through the redistribution of integrin b5into focal adhesions and it was happening through LRP1. This
happened by downregulating the expression DUSP6 in the cyto-
plasm & DUSP 1 in the nucleus with EGF/LF, via an increased
proteasomal degradation of the same DUSPs, in a RAP dependent
manner. Experiments with R3 monoclonal antibody against uPAR
showed that sustained ERK activation & DUSP downregulation
by EGF & LF is uPAR dependent. From these data we conclude
that LDLR signalling can in principle make MAP-Kinase signaling
induced by RTKs to become sustained but that uPAR-uPA-PAI-1
signaling is peculiar in so far as it induces sustained ERK1 activa-
tion that is in contrast to sutained ERK2 activation acompanied
by nuclear translocation of P-ERK and increased adhesion. We
find it promising as it may explain the mechanism of higher inci-
dence of cancer in hyperlipidemic patients or at the state of
inflammation.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
12 ORAL PAPERS____________________________________________________________________________________

O5B-4uPAR/LDLR interaction: a novel target for efficientendothelial cell migrationNovotny R, Unseld M, Bukowsky C, Poettler M, Binder BR,Zielinski CC and Prager GWMedical University of Vienna, Vienna, Austria
The urokinase plasminogen activator receptor (uPAR) system is
known to play a pivotal role in angiogenic endothelial cell behavior.
Recently, we have shown that in endothelial cells uPAR is redistrib-
uted to the leading edge of migrating cells upon VEGF stimulation
via a coordinated internalization and recycling mechanism, which
involves uPA:PAI-1:uPAR complex formation and LDLR-family
member mediated complex internalization. There is increasing evi-
dence that uPAR directly interacts with LDLR family members,
thereby linking integrin redistribution to the LDLR internalization
receptor.
In this study we have characterized the LDLR binding motif on
uPAR domain 3 in uPAR deficient HEK 293 cells or endothelial
cells, and studied the functional and biological consequences of sus-
pended uPAR/LDLR interaction by expression of either wild type
uPAR (wt) or mutated uPAR (mutL3) lacking LDLR binding capac-
ities. Additionally, we used a competitive interfering peptide (P1)
mimicking the binding domain of uPAR as well as chaperone Recep-
tor Associated Protein (RAP)-mediated inhibition of ligand binding
to LDLR family members.
Suspended uPAR/LRP interaction thereby led to reduced uPAR as
well as uPAR-dependent integrin internalization and redistribution
during cell migration. This was consistent with a decrease in integrin-
induced signal transduction such as pY576 FAK phosphorylation
most likely due to reduced integrin redistribution. As a consequence,
uPAR (mutL3) expressing cells revealed impaired cell spreading and
cell migration. Soluble as well as GPI-anchored uPAR domain 3,
however, was able to restore LDLR-mediated integrin internalization
during endothelial cell migration.
From these results we conclude that uPAR/LDLR interaction is
essential for uPAR-mediated integrin redistribution to the leading
edge of migrating endothelial cells during angiogenesis, which is a
prerequisite for efficient integrin-induced signal transduction. The
localization of the uPAR/LDLR binding motif will give novel
insights into a potential target for affecting endothelial cell behavior
in angiogenesis-related diseases.
O5B-5Growth factor induced endothelial cell migrationrequires urokinase receptor (uPAR)-dependent integrinredistributionPrager GW, Novotny R, Unseld M, Marina M, Mihaly J,Binder BR and Zielinski CCMedical University of Vienna, Vienna, Austria
Tumor angiogenesis is induced when the net balance of pro- and an-
tiangiogenic molecules is tipped in favor of angiogenesis, the so called
‘angiogenic switch’. Recently, we described a mechanism which
explains how the major angiogenic growth factor VEGF induces pro-
uPA activation via change of integrin beta-1 activity, which led to a
ternary complex formation between uPA/PAI-1 and uPAR, which
co-internalizes beta-1 integrins into the endosomal compartment.
Thereby, uPAR plays a central role for VEGF-induced endothelial
cell migration. However, limited treatment results of anti-angiogenic
therapies, which mainly aim to inhibit VEGF in malignancies(Cassidy
et al., 2008; Saltz et al., 2008), might lie in the fact that pro-angio-
genic endothelial cell behavior is not only induced by VEGF, but
also by a variety of other growth factors(Carmeliet, 2005).
Here we describe that uPAR associated pro-uPA activation, fol-
lowed by internalization and redistribution of uPAR and integrins,
is not specific for VEGF-induced endothelial cell activation, but
represents a more general pro-angiogenic mechanism, which is also
induced by others growth factors. We found that fibroblast growth
factor-2 (FGF-2), hepatocyte growth factor (HGF) as well as epi-
dermal growth factor (EGF), but not the VEGFR-1 ligand pla-
centa-like growth factor (PlGF) led to a PI3kinase dependent
activation of pro-uPA when bound to uPAR. As a consequence,
uPAR and integrins became internalized in an LDLR-like protein
dependent manner, while PlGF had no effect on uPAR redistribu-
tion. We found that domain-3 of uPAR is responsible and sufficient
to link integrin adhesion receptors to LDLR-family of internaliza-
tion receptors. Consistently, interference with the uPAR / integrin
internalization affected endothelial cell migration induced either by
VEGF, HGF, FGF-2, or EGF, but had no effect on PlGF-induced
endothelial cell migration.
From these data we conclude that uPAR represents a central mole-
cule in growth factor-induced endothelial cell behavior, which might
open a new avenue for therapeutic intervention in (tumor-)angiogene-
sis.
O5B-6Characterization of breast cancer cell linesoverexpressing the urokinase receptor splice variantuPAR-del4/5 or the GTP binding protein rab31Grismayer B1, Sato S1, Beaufort N1, Schmitt M1, Luther T2,Baretton G3, Magdolen V1 and Kotzsch M3
1Technical University Munich, Munchen; 2Medical Laboratory
Unit, Bautzen; 3Dresden University of Technology, Dresden,
Germany
The splice variant uPAR-del4/5 is a urokinase receptor form which
lacks domain DII. uPAR-del4/5 mRNA has been shown to be an
independent prognostic marker for distant metastasis-free survival in
node-negative breast cancer patients. Using microarray analyses to
identify differentially expressed genes associated with high uPAR-
del4/5 mRNA levels in breast tumors, the gene encoding rab31 was
one of seven genes found to be strongly up-regulated. Indeed, high
rab31 mRNA values were significantly associated, independent from
uPAR-del4/5, with worse outcome in breast cancer. Thus, rab31, a
member of the Rab family of small GTP-binding proteins involved in
intracellular transport, signal transduction and receptor internaliza-
tion/recycling, and uPAR-del4/5 may be components of associated,
tumor-relevant signaling pathways.
To analyze effects of uPAR-del4/5 and rab31 overexpression, respec-
tively, two different breast cancer cell lines, MDA-MB-231 and
MDA-MB-435, were stably transfected with expression plasmids
encoding uPAR-del4/5 or rab31.
FACS and Western blot analyses of transfected cell lines showed
an overexpression of both proteins about 3–10 times compared to
the vector control. The stably transfected cell lines were analyzed
regarding proliferation, and cell adhesion on several extracellular
matrix proteins. Interestingly, in highly metastatic MDA-MB-231
cells, proliferation was affected neither by overexpression of uPAR-
del4/5 nor of rab31, whereas overexpression of either proteins in
the only moderately metastatic MDA-MB-435 cells resulted in
enhanced proliferation. Furthermore, cells overexpressing uPAR-
del4/5 displayed reduced adhesion on several extracellular matrix
proteins. Strinkingly, a similar behavior was observed for cells over-
expressing rab31. In addition, cells overexpressing uPAR-del4/5
exhibit a significant decrease of tumor growth and metastasis in
vivo in comparison to the vector-transfected control cells. The
obtained results, and further experiments with single or combined
overexpression of both proteins concerning its invasive and migra-
tory potential may contribute to the further understanding of the
function/relation of uPAR-del4/5 and rab31 in tumor invasion and
metastasis.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
ORAL PAPERS 13____________________________________________________________________________________

O5B-7Matriptase induces formation of skin carcinomathrough activation of hepatocyte growth factor-dependent signaling pathwaySzabo R, Rasmussen AL, Moyer AB, Schafer JM, Molinolo AA,Gutkind JS and Bugge THNational Institutes of Health, Bethesda, USA
Matriptase is an epithelium-specific cell surface-associated serine pro-
tease that is overexpressed in a remarkable variety of human carcino-
mas. We have previously reported that dysregulated expression of
matriptase is sufficient to induce formation of highly invasive squa-
mous cell carcinoma (SCC) in mouse skin and also strongly potenti-
ates development of tumors induces by tobacco-related chemical
carcinogen DMBA (1). Here, we show that matriptase-induced
tumorigenesis is critically dependent on the proteolytic activation of
pro-hepatocyte growth factor (HGF), its receptor proto-oncogene
cMet, and the cMet-dependent signaling pathway that involves Akt
and mTor. Thus, we found that DMBA-induced tumor formation is
associated with the onset of matriptase expression in proliferating,
cMet-expressing keratinocytes of the basal layer of mouse skin and,
similarly, that matriptase and cMet colocalize in overwhelming
majority of human carcinomas of skin and head and heck region.
Genetic inactivation of cMet in mouse epidermis strongly suppressed
matriptase-induced hyperproliferation of epidermal keratinocytes, epi-
dermal hyperplasia, and carcinoma formation. Furthermore, matrip-
tase-dependent tumorigenesis was associated with overactivation of
Akt, one of the downstream targets of cMet signaling pathway, and
it could be completely prevented by the inhibition of an immediate
downstream target of Akt, mTOR. These data strongly suggest that
translocation of matriptase expression to proliferative compartment
of epidermis is linked to an increased activation of pro-hepatocyte
growth factor and an overactivation of cMet-dependent signaling
pathway, which critically contributes to the malignant transformation
of murine epidermis.
List, K., Szabo, R. et al., Genes Dev. 2005; 19: 1934–1950.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
14 ORAL PAPERS____________________________________________________________________________________

Plasminogen Activation and Fibrinolysis
O6A-1Polyphosphate modulates fibrin structure altering itssusceptibility to lysisMutch NJ, Engel E, Uitte de Willige S, Philippou H andAriens RASUniversity of Leeds, Leeds, UK
Upon activation by thrombin or other agonists platelets secrete a
negatively charged polymer, polyphosphate (polyP). We explored the
interaction of polyP with fibrin(ogen) and its impact on fibrin struc-
ture and fibrinolysis. Electrophoretic mobility and binding assays
indicate that polyP interacts directly with fibrinogen and soluble
fibrin. Clots formed in the presence of polyP displayed reduced tur-
bidity and permeability suggesting the formation of a tighter fibrin
network. These changes were independent of both cross-linking and
fibrinopeptide release. Microscopy revealed an altered pattern of
fibrin distribution in clots formed with polyP; with formation of tight
aggregates of fibrin fibers interspaced with large pores in contrast to
homogenous fiber distribution in control clots. Lysis by tPA and
plasminogen or pre-formed plasmin was delayed in clots formed in
the presence of polyP. These changes were dependent on both the
concentration of activator and polyP but were independent of throm-
bin. Addition of polyP to the clot after fibrin formation or to
repolymerising soluble fibrin did not affect lysis indicating that
changes induced by polyP occur at the level of conversion of fibrino-
gen to fibrin. Surface plasmon resonance revealed that the presence
of polyP during fibrin formation interfered with the binding of both
plasminogen and tPA but only after these surfaces were subjected to
partial-lysis by plasmin. Our data indicate that polyP produces pro-
thrombotic fibrin structures with increased resistance to fibrinolysis.
These effects result from architectural differences in the clot that
occur during conversion of fibrinogen to fibrin. The altered fibrin
structure generated in the presence of polyP is less susceptible to plas-
min cleavage, therefore reducing exposure of lysine binding sites. This
in turn modulates the cofactor capacity of fibrin in tPA-mediated
plasminogen activation.
O6A-2Fibrin structure and the regulation of tissueplasminogen activator (tPA) binding and potencyWilliams SC1, Kolev K2, Szabo L3, Silva M1 and Longstaff C1
1NIBSC, Potters Bar, UK; 2Semmelweis University, Budapest;3Chemical Research Centre, Budapest, Hungary
Regulation of tPA activity is highly dependent on fibrin binding and
tPA binds primarily by finger (F) and Kringle2 (K2) domains. How-
ever, rates of fibrinolysis are also affected by fibrin structure. We
have investigated structure/function and regulation of tPA activity in
fibrin formed at 10 IU/mL thrombin [fibrin(10), fine fibre mesh, small
pores] and 0.5 IU/mL thrombin [fibrin(0.5), thick fibres, large pores]
using domain variants of tPA. Parallel rate measurements of plasmin-
ogen activation in fibrin and fibrinolysis following clot turbidity were
made using domain variants. Kinetics studies on wild type tPA, (F-
G-K1-K2-P), K1K1tPA (F-G-K1-K1-P) and delFtPA (G-K1-K2-P)
showed a consistent trend for enzyme potency of tPA > K1K1tPA
> delFtPA with delFtPA up to 66% less potent than tPA in
fibrin(0.5), but differences reduced at high (PA) and in Fibrin(10).
Fibrin(10) was a better surface for plasminogen activation but more
resistant to lysis than fibrin(0.5). Reorganisation of fibrin(0.5) struc-
ture complicated turbidity measurements and SEM studies tied these
changes to reformation of large protein agglomerates during lysis.
Confocal microscopy using orange fluorescent fibrin with jellyfish
green fluorescent protein (GFP)-labelled tPA variants showed these
agglomerates strongly bind tPA. Movies and enzyme kinetics studies
highlight major differences in behaviour of tPA-GFP variants in
fibrin(10) and fibrin(0.5). Initial binding in fibrin(0.5) requires F
domain and delFtPA-GFP was less efficiently bound to agglomerates
so diffused through the clot ahead of the lysis zone. Poor initial bind-
ing and lag in plasminogen activation with delFtPA can be partially
compensated for by enhanced diffusion and fibrinolysis. Fibrinolysis
may be divided into three stages: (i) initial binding of tPA and activa-
tion of plasminogen; (ii) enhancement due to C-terminal lysine gener-
ation; (iii) tPA focalisation on large protein agglomerates. Stages (i)
and (iii) are more finger dependent, (ii) is K2 dependent, but fibrin
structure affects the three stages in different ways.
O6A-3Intra-vital analyses of plasminogen binding toplatelet-rich micro-thrombusTanaka A, Suzuki Y and Urano THamamatsu University School of Medicine, Hamamatsu, Japan
Aim: To elucidate the precise mechanism of thrombolysis in the
vasculature, we analyzed the process of plasminogen-binding to laser-
induced microthrombus in mice using intra-vital fluorescence micros-
copy. The binding of Glu-plg on activated platelets’ surface was also
analyzed in in-vitro experiment.
Method: Mesenteric vein of green fluorescent protein expressing
transgenic mouse (GFP-mouse) was irradiated by laser-beam through
objective lens of fluorescence confocal microscopy and platelet-rich
micro-thrombus was formed. The accumulation of GFP expressing
platelets as well as Alexafluor 568 labeled plasminogen (Glu- or
mini-plg) on injured vessel wall was measured as an increase in the
corresponding fluorescent intensity with time course, and their distri-
butions were analyzed.
Results: (i) Glu-plg accumulated in a time-dependent manner to the
center of micro-thrombus, where phosphatidylserine (PS) was
exposed on platelets surface and fibrin was formed. (ii) The bindings
of Glu-plg in the presence of EACA (approximately 20 mM) or after
treatment by carboxy-peptidase (approximately 10 U/mL), and of
mini-plg were significantly less than that of Glu-plg alone. (iii) Glu-
plg appeared to bind to the surface of calcium-ionophore treated
GFP-platelets, at the timing when GFP disappeared from the plate-
lets, which was possibly initiated as a result of sustained-elevation of
intra-cellular calcium ion concentration.
Discussion: Glu-plg appeared to accumulate in the center of micro-
thrombus in a time-dependent manner by binding to either activated
platelets’ surface or formed fibirn in a lysine binding site dependent
mechanism.
O6A-4Fibrinolysis regulation: Interaction of a2-antiplasminwith fibrin(ogen) and localization of the binding sitesMedved L1, Tsurupa G1, Yakovlev S1 and Mckee P2
1University of Maryland School of Medicine, Baltimore;2University of Oklahoma Health Science Center, Oklahoma, OK,
USA
Covalent incorporation of plasmin inhibitor a2-antiplasmin (a2-AP)
into fibrin clot results in effective inhibition of fibrinolysis. It is well
established that such incorporation is mediated by Factor XIIIa,
which cross-links a2-AP to the fibrin(ogen) Aa chain Lys303 located
in the aC-connector. We hypothesized that a2-AP may interact non-
covalently with fibrin prior to its covalent cross-linking. To test this
hypothesis, we studied the binding of a2-AP to immobilized fibrin(o-
gen) and its fragments by Surface Plasmon Resonance (SPR) and
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
ORAL PAPERS 15____________________________________________________________________________________

ELISA. SPR experiments revealed that a2-AP binds to fibrin while
no binding was observed with fibrinogen. To localize the a2-AP bind-
ing site(s), we studied the interaction of a2-AP with fibrin(ogen) D-D
and E3 fragments and the recombinant aC region (Aa221–610), whichtogether encompass practically the whole fibrin(ogen) molecule, as
well as with the aC-connector (Aa221–391) and aC-domain (aA392–
610) composing the aC region. In ELISA, a2-AP bound only to
immobilized D-D (Kd = 94 nM), Aa221–610 (Kd = 150 nM), and
aC-domain (Kd = 131 nM). The binding to both D-D and aC was
Lys-independent and was not inhibited by tPA or plasminogen. Fur-
thermore, the affinity of a2-AP to D-D was significantly increased in
the presence of plasminogen while that to aC remained unaffected.
Altogether, these results indicate that: (i) the D regions and aC-domains contain high affinity a2-AP binding sites which are cryptic
in fibrinogen and exposed in fibrin; (ii) these binding sites do not
overlap with the Lys303 cross-linking site; (iii) the presence of plas-
minogen facilitates the non-covalent binding of a2-AP to the fibrin D
region. The results also suggest that the non-covalent interaction of
a2-AP with fibrin and spatial separation of the non-covalent binding
sites may provide initial binding of a2-AP to fibrin and proper orien-
tation of the cross-linking sites to facilitate the covalent stage of the
interaction.
O6A-5Synthetic nonadecapeptide (SAK22-40) enhancesplasminogen activation and thrombolysisOkada KKinki University School of Medicine, Osakasayama, Osaka,
Japan
As we reported previously, a new synthetic nonadecapeptide
(SAK22-40) corresponding to Glu22-Leu40 of SAK (staphylokinase)
molecule bound to plasminogen and enhanced the activation of plas-
minogen by SAK-plasmin complex. We further investigate the mech-
anism in detail. SAK22-40 enhanced activation of plasminogen by
tissue-type plasminogen activator (t-PA), and enhanced also activa-
tion of plasminogen by t-PA on human endothelial cell. Analysis of
IAsys resonant mirror biosensor showed that SAK22-40 bound to
human and mouse Glu-plasminogen. This binding was completely
inhibited by synthetic peptide corresponding to C-terminal region of
plasmin B-chain. SAK22-40 bound to human endothelial cell through
Glu-plasminogen. The near-ultraviolet circular dichroism (CD)
spectra of the complex between SAK22-40 and Glu-plasminogen sig-
nificantly differed from Glu-plasminogen in the presence of �-amino-
caproic acid or Glu-plasminogen alone. Therefore, SAK22-40 binds
to Glu-plasminogen, and induces structural changes of Glu-plasmino-
gen. When SAK22-40 was administrated in mouse thrombosis model,
earlier recanalization was observed than in mice with vehicle adminis-
tration, and showed dose-dependent manner. However, SAK22-40
did not show the recanalization in t-PA gene deficient mice. Thus,
SAK22-40 enhanced plasminogen activation and induced effective
thrombolysis.
O6A-6Stable and reversible fusion protein conjugated to redblood cells for drug delivery in thromboprophylaxisMarcos-Contreras OA1, Gonzalez de la Fuente M2, Cines DB3,Muzykantov VR4 and Murciano JC5
1Fundacion Centro Nacional de Investigaciones
Cardiovasculares; 2Departamento de Farmacologia, Facultad de
Medicina, Universidad Complutense, Madrid, Spain;3Department of Pathology and Laboratory Medicine, University
of Pennsylvania; 4IFEM, University of Pennsylvania School of
Medicine, Philadelphia, PA, USA; 5Internal Medicin Department,
Hospital Ramon y Cajal, Madrid, Spain
Introduction: We developed a new thromboprophylactic agent by the
conjugation of plasminogen activators (PAs) to red blood cells
(RBCs). In order to bring this agent to clinics, we formulated fusion
proteins (FP) that combined a mutated streptavidin (SA) core, with a
limited capacity to tetramerized, with a thrombin-activatable uroki-
nase (UK-T). This results in a reversible conjugation between FP and
RBC, thus offering a thromboprophylactic agent with a controllable
duration.
Methods: S2 cells were trasfected with the construct of SA subunit
(13 kDa) with a single aminoacid mutation (D117A) and UK-T
(33 kDa). Produced FP was purified by affinity column chromatogra-
phy and analysed by western blot (WB). Its activity was tested by
biotinylated RBC (bRBC) binding and fibrinolytic activity. Revers-
ible binding to RBC was confirmed by FP displacement form the
bRBC surface using post-incubation with native SA.
Results: WB confirms the presence of two bands at 46 kDa (mono-
merized FP, 85% densitometric analysis) and 180 kDa (tetramerized
FP, 15%). FP fibrinolytic activity was confirmed by addition of
thrombin pre-activated FP over 125I-fibrin clots, resulting in a
99.7.�0.86% of lysis at 6 h, while non pre-activated one showed
23.5 � 3.1% and PBS control 6.5 � 0.4%. 125I-FP binds in a dose
dependent fashion over bRBC, peaking at 75 590 � 9003 molecules
per bRBC (606 � 135 over naıve RBC). RBC-FP remains stably
associated over 48 h in vitro (92 � 1.6% at 24 h and 64.4 � 1.5% at
48 h). RBC-FP efficiently dissolves fibrin clots (4 h) from within,
100 � 1.4% vs. 5.4 � 5% of FP pre-incubated with naıve RBC.
Interestingly, native SA displaced RBC-125I-FP over 53.6 � 5%,
resulting in a lack of RBC-FP fibrinolytic capacity 24.4 � 0.4%.
Conclusion: These data demonstrated that FP (i) stays mainly in a
monomeric form, (ii) binds specifically to bRBC, (iii) remains conju-
gated over days, (iv) get activated in the presence of thrombin and
(v) reversibly dissociates from the conjugate.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
16 ORAL PAPERS____________________________________________________________________________________

Serpins
O6B-1Highly sensitive ELISA method for the determinationof alpha2-plasmin inhibitor antigen levelOrosz A, Muszbek L and Katona EUniversity of Debrecen, Medical and Health Science Center,
Debrecen, Hungary
Background: a2-plasmin inhibitor (a2-PI; a2-antiplasmin) is the pri-
mary inhibitor of plasmin-mediated fibrinolysis that forms an irre-
versible inhibitory complex with plasmin (plasmin-antiplasmin, PAP
complex). a2-PI is secreted into the plasma as a approximately
66 kDa single polypeptid chain with Met as the amino-terminus. In
the plasma it undergoes proteolytic cleavage to yield a 12 amino acid
shorter form with Asn as amino-terminus. Asn1-a2-PI becomes cross-
linked to fibrin by FXIIIa 13-times faster than Met1-a2-PI, thereby it
is more effective in the inhibitopn of fibrinolysis. There are also
C-terminal isoforms differing in 27 amino acids that cleaved by an
unidentified protease.
Methods: In this study we developed a two-step ELISA for the deter-
mination of total a2-PI using biotinylated monoclonal antibody
reacting with an epitope present in all isoforms of the protein and
peroxydase-labeled polyclonal antibody for capture and detection,
respectively. Samples and standards were incubated together with the
capture antibody in strepavidin-coated microplate in the first step.
After washing the detection antibody was applied and TMB substrate
was used for the quantification of the reaction.
Results: The limit of quantitation was 0.70 ng/mL, the measuring
range was 0.7–100 ng/mL. This high sensitivity allowed the determi-
nation of a2-PI in 1:2000 dilution of plasma samples. The assay
showed good precision with within run variability C = 4.6% at nor-
mal level (60.8 � 4.0 mg/L plasma), CV = 5.3% in the pathological
range (19.5 � 1.6 mg/L) and CV = 9.1% at extreme low level
(1.98 � 0.35 mg/L). Inter-assay reproducibility was CV = 5.8%,
7.3% and 16.6%, respectively. In normal citrated plasma samples
(n = 40) 69.3 � 8.0 mg/L (mean � SD) was measured.
Conclusion: Our method is suitable for the measurement of total a2-PI antigen level both in normal and pathologic range with good pre-
cision. Its high sensitivity makes it possible to detect very low level of
a2-PI present in body fluids other than plasma.
O6B-2The influence of alpha2-antiplasmin polymorphismArg407Lys on fibrinolysisUitte de Willige S, Miedzak M, Philippou H, Carter AM,Grant PJ and Ariens RASUniversity of Leeds, Leeds, UK
The main inhibitor of plasmin, alpha-2-antiplasmin, is secreted into
plasma as a 70 kDa protein of 464 amino acids. As a result of post-
translational proteolysis at the N- and C-termini, alpha-2-antiplasmin
circulates in functionally different molecular forms. In our search for
the position of C-terminal cleavage, we found that polymorphism
Arg407Lys (R407K; rs1057335) is located close to a potential cleav-
age site. This made us hypothesize that C-terminal cleavage of alpha-
2-antiplasmin, and thereby the lysis times of plasma clots, may be
modulated by this polymorphism.
To investigate this, we genotyped a group of 180 control samples by
RFLP and set up two ELISAs to measure (i) total alpha-2-antiplas-
min level and (ii) C-terminally intact alpha-2-antiplasmin level. To
determine the level of C-terminal cleavage of alpha-2-antiplasmin, we
calculated the ratio of C-terminal intact alpha-2-antiplasmin over
total alpha-2-antiplasmin.
Genotype frequencies were RR:60%, RK:35.6% and KK:4.4%,
allele frequencies were R:77.8% and K:22.2%. R407K did not asso-
ciate with C-terminal cleavage, as we found similar C-terminally
intact/total alpha-2-antiplasmin ratios for all three genotypes
(RR:0.96, RK:0.92, KK:0.94). However, total alpha-2-antiplasmin
level (90.8%) was lower in homozygous K-carriers compared to
RR-carriers (100%) or RK-carriers (102.6%), indicating that the
R407K polymorphism could be associated with diminished alpha-2-
antiplasmin expression. This was reflected in the time to 50% lysis,
with a shorter lysis time (8.66 min) for K-homozygotes compared to
RR-carriers (10.64 min) or RK-carriers (11.04 min). Intriguingly,
R407K also associated with the lagphase of clotting; RR:7.14 min,
RK:6.43 min, KK:4.80 min; P = 0.001), indicating that this poly-
morphism may influence the onset of coagulation. We next aim to
genotype alpha-2-antiplasmin R407K and measure alpha-2-antiplas-
min levels in 288 age- and sex-matched myocardial infarction (MI)
patient samples to investigate if this polymorphism influences MI
risk.
These data indicate that the alpha-2-antiplasmin R407K polymor-
phism influences alpha-2-antiplasmin expression and lysis times of
plasma clots, and possibly also the onset of coagulation.
O6B-3The adipokine vaspin inhibits smooth musclemigration in vitro and the development of coronaryin-stent restenosis in vivoKastl SP1, Katsaros KM1, Krychtiuk K1, Speidl WS1, Maurer G1,Huber K2 and Wojta J11Medical University of Vienna; 23rd Medical Department
Wilhelminenhospital, Vienna, Austria
Percutaneous coronary intervention (PCI) represents the most
important treatment modality of coronary artery stenosis. In-stent
restenosis (ISR) is still a limitation for the long-term outcome
despite the introduction of drug eluting stents. Adipokines may
directly influence vessel wall homeostasis by influencing the function
of endothelial cells and arterial smooth muscle cells (SMC). Visceral
adipose tissue-derived serpin (vaspin) was recently identified as a
member of serine protease inhibitor family and serveral studies
could demonstrate a relation to metabolic diseases like diabetes.
The aim of this study was to investigate a role of vaspin in SMC
migration in vitro and development of ISR in vivo. Human coronary
artery smooth muscle cell (HCASMC) migration was analyzed by
an in-vitro migration assay with different concentrations (0.004 ng/
mL up to 40 ng/mL) of vaspin. The development of ISR was stud-
ied in 57 patients with stable coronary artery disease who under-
went elective and successful percutaneous coronary intervention
(PCI) with implatation of drug eluting stents. Blood samples were
taken directly before PCI. Vaspin plasma levels were measured by
specific elisa. ISR was evaluated 8 months later by coronary angio-
graphy. During the follow up period, 13 patients developed ISR.
Patients with ISR had significantly lower vaspin plasma levels com-
pared to patients without ISR (0.205 ng/mL vs. 0.349 ng/mL;
P = 0.004). Further we could demonstrate that vaspin nearly abol-
ishes serum induced SMC migration (100% vs. 7%; P < 0.001) in
a biphasic manner. We were able to show for the first time that the
adipokine vaspin inhibits SMC migration in vitro. In addition, the
occurrence of ISR after PCI with implantation of DES was signifi-
cantly associated with low vaspin plasma levels before intervention.
Determination of vaspin plasma levels before PCI might be helpful
in the identification of patients with high risk for development of
ISR after stent implantation.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
ORAL PAPERS 17____________________________________________________________________________________

O6B-4PAI-1 as a furin convertase inhibitor: a potential rolein insulin resistanceBernot D, Canault M, Nalbone G, Alessi MC and Peiretti FINSERM, Marseille, France
Epidemiological studies showed that elevated plasma levels of SER-
PINE1/PAI-1 predict the risk of type 2 diabetes and metabolic syn-
drome. A direct role of PAI-1 in these pathologies has been
suggested, but not demonstrated. Among several hypotheses, inhibi-
tion by PAI-1 of furin convertase (a serine protease involved in the
processing of many potein precursors including insulin proreceptor)
has been proposed.
We studied this possibility, focusing on the consequences of furin
and PAI-1 overexpression on insulin proreceptor maturation and
insulin signaling.
We showed that PAI-1 efficiently associated with furin in a SDS-sta-
ble complex, in vitro and in vivo (transfected cells). Using a golgian
furin-activity reporter construct, we demonstrated intracellular furin
inhibition by PAI-1. Association between furin and PAI-1 most prob-
ably occurred intracellularly during transport/addressing, since a
PAI-1 lacking its signal peptide did not associate nor inhibit furin. In
furin-defective human LoVo cells (expressing low PAI-1 level), furin
overexpression induced insulin proreceptor maturation. Concomitant
overexpression of a stabilized form of PAI-1 inhibited this matura-
tion (-54.4%, significant), as well as insulin-stimulated phosphoryla-
tion of both insulin receptor and Akt. Analysis of hepatic tissue from
PAI-1 KO mice revealed an increase in insulin receptor mature form,
compared to wild type mice (+31.6%, significant).
In conclusion, our results show that PAI-1 potently inhibits furin
convertase, leading to a decrease in insulin receptor functionality that
can contribute to insulin resistance. In addition, we described an ori-
ginal intracellular effect of PAI-1 regulating serine protease activity.
O6B-5Metals exert an unexpected role in regulatingenzymes in the plasminogen activation cascadePeterson CB, Thompson LC and Goswami SUniversity of Tennessee, Knoxville, TN, USA
Proteases regulate many biological processes biology, including coag-
ulation and clot lysis, the immune response, and processes that remo-
del the extracellular matrix (ECM) during wound healing and cell
migration. Because of the importance of proteases, their activity must
be closely checked. This is accomplished in part by the serine prote-
ase inhibitors (serpins), which form inactive covalent complexes with
their target proteases. Plasminogen activator inhibitor-1 (PAI-1) is
the major inhibitor of both urokinase (uPA) and tissue plasminogen
activator (tPA) that lyse fibrin clots and also cleave ECM compo-
nents. The active conformation of PAI-1 is metastable and spontane-
ously converts to a latent form with a half-life of 1.1 h at 37 �C. Thehalf-life of the active conformation is extended to 1.5 h when PAI-1
is bound to the plasma protein vitronectin. Our recent work demon-
strates that the observed stabilization of PAI-1 by vitronectin is
metal-dependent. Human PAI-1 more rapidly converts to the latent
conformation in the presence of cobalt, nickel, and copper. Strik-
ingly, the half-life is much longer in the presence of vitronectin and
these metals. Steady-state binding measurements using surface plas-
mon resonance have been used to determine a dissociation constant
for the interaction with nickel. Stopped-flow measurements of
approach-to-equilibrium changes in intrinsic protein fluorescence
have been used in a complementary fashion to characterize binding
to a broader range of metals. These studies reveal distinct steps in
the mechanism for metal interaction with PAI-1, with a binding step
followed by a series of conformational changes. Measurements of the
observed rate constants of binding as a function of varying metal
concentrations allowed accurate determination of binding affinities
for cobalt, nickel, and copper, yielding dissociation constants of
about 40, 30, and 0.09 lM respectively. Identification of binding sites
for copper is being pursued using a structural informatics approach.
O6B-6Evaluation of a panel of plasminogen activatorinhibitor-1 inhibiting monoclonal antibodies in amouse pulmonary embolism modelvan de Craen B, Declerck PJ and Gils AKatholieke Universiteit Leuven, Leuven, Belgium
Introduction: Plasminogen activator inhibitor-1 (PAI-1) is an impor-
tant inhibitor of the plasminogen activation system. Elevated PAI-1
levels have been implicated in a wide variety of thrombotic and non-
thrombotic conditions. Pharmacological inhibition of PAI-1 activity
might therefore be an interesting therapeutic approach in different
pathologies.
Aim: The evaluation of a panel of inhibitory monoclonal antibodies
(MA) reacting with glycosylated mouse PAI-1 (mPAI-1) in a pulmo-
nary embolism model.
Methods and Results: Using hybridoma technology we were able to
generate MA that showed good reactivity towards glycosylated
mPAI-1 and inhibited at least 50% of PAI-1 activity at a 2-fold
molar excess of MA over PAI-1 in an in vitro enzymatic assay. These
antibodies were evaluated for their inhibitory potential in a mouse
pulmonary embolism model. In this model, 10 mg/kg of MA was
administered (i.v.) 5 min before i.v. injection of a suboptimal concen-
tration of t-PA (0.1 mg/kg). Pulmonary embolism was evoked by i.v.
injection of thromboplastin (3.3 mg/kg). Mice were evaluated after
15 min and gained a positive score if they displayed normal physical
activity. A negative score was obtained in case of paralysis of the
limbs or death.
For two of the evaluated antibodies, MA-MP6H6 and MA-MP26H2,
we could detect a statistically significant increase in the proportion of
mice showing normal physical activity compared to control mice to
which no monoclonal antibody was administered (Table 1).
Table 1 for O6B-6
MA Mice with normal physical activity (%) n
33% 103
MA-MP6H6 66%* 44
MA-MP26H2 60%* 30
MA-MP2D9** 34% 32
*P < 0.05 (Fisher’s exact test).
**Non-inhibitory MA reacting with glycosylated mPAI-1.
Conclusion: The increased survival rate obtained with MA-MP6H6
and MA-MP26H2 in this pulmonary embolism model indicates that
these PAI-1 inhibiting MA might be promising tools to further unra-
vel the complex role of PAI-1 in other thrombotic and non-throm-
botic mouse models.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
18 ORAL PAPERS____________________________________________________________________________________

Plenary Lectures (2)
O7-1The biochemistry of TAFINesheim MEQueen’s University, Kingston, Canada
TAFI, or thrombin activatable fibrinolysis inhibitor, is a 60 kDa
plasma zymogen that circulates at a concentration of about 100 nM.
It is activated to the basic carboxypepidase TAFIa by a single prote-
olytic cleavage at arginine 92. TAFIa down regulates the process of
fibrinolysis by removing the carboxy terminal lysine residues that
appear in fibrin as it is degraded. Because TAFI was discovered inde-
pendently and approximately contemporaneously by several groups it
has acquired other names which include plasma procarboxypeptidase
B (for basic), procarboxypeptidase U (for unstable) and procarboxy-
peptidase R(for arginine). TAFI can be activated by thrombin and
plasmin. The reaction with thrombin is enhanced 1250-fold by throm-
bomodulin. The mechanism for this enhancement is not known in
detail. Residues adjacent to the cleavage site appear not to be respon-
sible for the thrombomodulin dependence, whereas other key posi-
tively charged residues do, among them being three tandem lysine
residues in the activation peptide. TAFIa down regulates fibrinolysis
by eliminating the positive feedback steps comprising plasmin-
enhancement of the tPA cofactor activity of fibrin and plasmin-
catalyzed conversion of Glu-plasmingen to Lys-plasminogen. It also
suppresses the protection by partially cleaved fibrin of plasmin and
tPA from antiplasmin and PAI-1, respectively. TAFIa is down regu-
lated by spontaneous decay, with a half-life about 8 min at body
temperature. The human TAFI gene is located on chromosome 13.
Two common polymorphisms in the coding region have been identi-
fied. These translate as Ala147Thr and Thr325Ile in the protein. The
former has no known functional significance, but isoleucine at posi-
tion 325 doubles the half-life of TAFI and increases its antifibinolytic
potential. Numerous clinical studies indicate pathophysiologic roles
for TAFI. In addition, studies in the TAFI knockout mouse model
indicate that the TAFI pathway is relevant in inflammation and
pathologies associated with it.
O7-2Haemostasis and innate immunityGinsburg DUniversity of Michigan, Ann Arbor, MI, USA
Hemostasis is a critical component of the host response to microbial
pathogens and may be an important evolutionary selective pressure
underlying the wide variation in plasma level for many blood coagu-
lation factors. Work from our lab characterizing the interaction of
the microbial plasminogen activator, streptokinase, with host plas-
minogen will be reviewed, including recent efforts to modulate this
pathway as a novel approach to the therapy of Group A streptococ-
cal infection. Studies exploring the genetic basis for variability in
plasma von Willebrand factor levels and the potential implications of
these findings for the interaction between hemostasis and microbial
pathogens will also be discussed.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
ORAL PAPERS 19____________________________________________________________________________________

President’s Session: Young Investigators’ Presentations and the
D. Collen Young Investigators’ Awards
O8-1Allosteric activation of the DegS protease: designprinciples of stress-sensor proteasesSohn J, Grant R and Sauer RMassachusetts Institute of Technology, Cambridge, MA, USA
In the E. coli periplasm, disruption of protein folding is sensed by
the PDZ domains of the trimeric DegS protease, which bind C-termi-
nal peptides of misfolded outer-membrane porins (OMPs). This bind-
ing event triggers proteolytic cleavage of RseA, a transmembrane
regulator, and eventually leads to initiation of transcriptional activa-
tion of stress genes. We find that DegS is an allosteric enzyme.
OMP-peptide binding to the PDZ domain relieves inhibitory contacts
between the PDZ and protease domains, triggering reconfiguration of
the active-site oxyanion hole from inactive to active conformation.
Both RseA substrate and OMP peptides activate the protease by
binding preferentially but not exclusively to the active conformation
of DegS. Disrupting inhibitory interactions between the PDZ and
protease domains results in faster substrate cleavage and tighter
OMP-peptide binding. Likewise, stabilizing the active conformation
of the protease domain by mutagenesis results in the same phenotype.
Cocrystal structures of DegS in complex with different OMP peptides
and in multiple lattices also support the idea that the role of the
PDZ domain is inhibitory. Allostery is an intrinsic property of the
protease domain of DegS, as the isolated protease domain also equili-
brates between inactive and active trimeric conformations, similar to
those observed in the full-length enzyme. A set of conserved residues
in the protease domain mediates this allosteric transition. Mutations
on these residues result in substantially lower proteolytic activity, and
multiple crystal structures of these mutant DegS variants consistently
show the non-functional conformation. Overall, our biochemical and
structural results support a concerted two-state allosteric model,
which can be quantitatively modeled. This two-state mechanism is
biologically robust, allows rapid responses to protein-folding stress,
and allows DegS function to be precisely regulated by the affinity of
OMP peptides and substrate for its active and inactive conforma-
tions.
Reference: Sohn et al. Cell 2007; Mol. Cell 2009; Structure 2009.
O8-2TAFI regulates hepatocyte survival during liverregeneration independent from cell-associatedplasminogenOkumura NNihon University College of Bioresource Sciences, Fujisawa,
Japan
Background: Thrombin-activatable fibrinolysis inhibitor (TAFI) is
plasma procarboxypeptidase B secreted from the liver. We have dem-
onstrated that the expression of TAFI is suppressed by growth pro-
moted conditions during liver regeneration, and this down-regulation
promotes hepatocyte proliferation through cell surface plasmin(ogen).
In this study, we further investigated the role of TAFI in liver regen-
eration focusing on hepatocyte survival and death using TAFI defi-
cient mice as well as TAFI-gene silenced primary hepatocytes.
Methods: TAFI knock out mice (ko) and wild type mice (wt) under-
went 70% partial hepatectomy. The proliferation rate and the extent
of liver injury were measured during liver regeneration. Hepatocytes
were isolated from rat liver by collagenase perfusion and primary he-
patocytes were transfected with TAFI siRNA. The morphological
change of nuclei was observed by Hoechst33258 staining, and apop-
totic and survival signals were analyzed by western blotting.
Results: Liver regeneration was accelerated in TAFI ko in comparison
with wt. Liver injury after hepatectomy was milder in TAFI ko than
wt. TAFI siRNA suppressed TAFI mRNA expression in primary he-
patocytes by 90% of that in control hepatocytes. Apoptosis was
induced in control hepatocytes during primary culture; however, it
was reduced in TAFI-silenced hepatocytes. Cleaved caspase-3, which
is an executioner at the down stream of apoptosis, was decreased in
TAFI-silenced hepatocytes in comparison with control-hepatocytes.
Conversely, phosphorylated-Akt suppressing apoptosis and promoting
cell survival and proliferation was increased in TAFI-silenced hepato-
cytes. Treatment of hepatocytes with tranexamic acid failed to inhibit
the events induced by TAFI-gene silencing, suggesting that cell surface
associated plasmino(gen) was not involved in the signaling.
Conclusion: These results suggest a novel role for TAFI in the regula-
tion of hepatocyte survival and proliferation during liver regeneration
independent from cell-associated plasminogen.
O8-3Binding characteristics of thrombin-activatablefibrinolysis inhibitor to streptococcal surface collagen-like proteins A and BValls Seron M1, Marx PF2, Marquart JA2, Herwald H3, deGroot PG4 and Meijers JCM2
1Academic Medical Center (AMC); 2Academic Medical Center,
Amsterdam, The Netherlands; 3Biomedical Center, Lund
University, Lund, Sweden; 4University Medical Center, Utrecht
University, Utrecht, The Netherlands
Streptococcus pyogenes is an important human Gram-positive patho-
gen that mainly causes throat and skin infections, such us pharyngi-
tis, impetigo and cellulitis. Although the majority of streptococcal
infections are superficial, some cases may progress into invasive and
life threatening diseases with an extremely rapid progression, such as
sepsis and necrotizing fasciitis. Thrombin-Activatable Fibrinolysis
inhibitor (TAFI) binds to the collagen-like proteins SclA and SclB
found at the surface of Streptococcus pyogenes. Activation of TAFI
at this surface is thought to redirect inflammation from a transient to
a chronic state by modulation of the kallikrein/kinin system. Here,
Fig. 1. Initiation of the envelope-stress response.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
20 ORAL PAPERS____________________________________________________________________________________
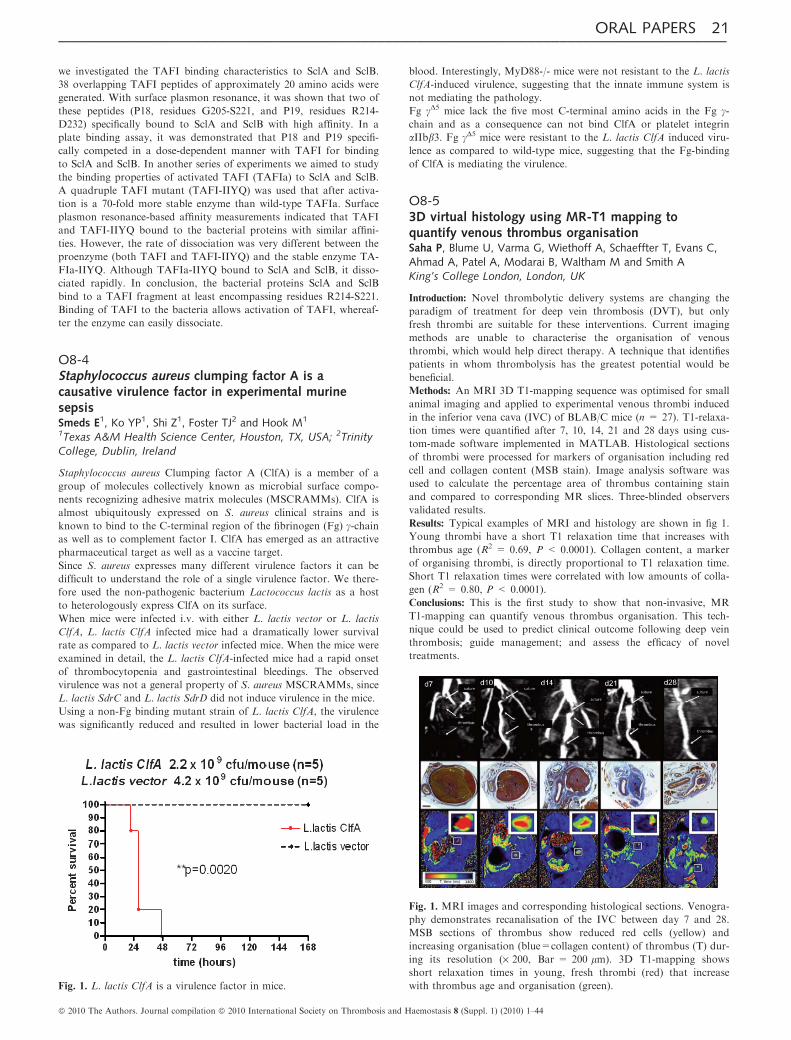
we investigated the TAFI binding characteristics to SclA and SclB.
38 overlapping TAFI peptides of approximately 20 amino acids were
generated. With surface plasmon resonance, it was shown that two of
these peptides (P18, residues G205-S221, and P19, residues R214-
D232) specifically bound to SclA and SclB with high affinity. In a
plate binding assay, it was demonstrated that P18 and P19 specifi-
cally competed in a dose-dependent manner with TAFI for binding
to SclA and SclB. In another series of experiments we aimed to study
the binding properties of activated TAFI (TAFIa) to SclA and SclB.
A quadruple TAFI mutant (TAFI-IIYQ) was used that after activa-
tion is a 70-fold more stable enzyme than wild-type TAFIa. Surface
plasmon resonance-based affinity measurements indicated that TAFI
and TAFI-IIYQ bound to the bacterial proteins with similar affini-
ties. However, the rate of dissociation was very different between the
proenzyme (both TAFI and TAFI-IIYQ) and the stable enzyme TA-
FIa-IIYQ. Although TAFIa-IIYQ bound to SclA and SclB, it disso-
ciated rapidly. In conclusion, the bacterial proteins SclA and SclB
bind to a TAFI fragment at least encompassing residues R214-S221.
Binding of TAFI to the bacteria allows activation of TAFI, whereaf-
ter the enzyme can easily dissociate.
O8-4Staphylococcus aureus clumping factor A is acausative virulence factor in experimental murinesepsisSmeds E1, Ko YP1, Shi Z1, Foster TJ2 and Hook M1
1Texas A&M Health Science Center, Houston, TX, USA; 2Trinity
College, Dublin, Ireland
Staphylococcus aureus Clumping factor A (ClfA) is a member of a
group of molecules collectively known as microbial surface compo-
nents recognizing adhesive matrix molecules (MSCRAMMs). ClfA is
almost ubiquitously expressed on S. aureus clinical strains and is
known to bind to the C-terminal region of the fibrinogen (Fg) c-chainas well as to complement factor I. ClfA has emerged as an attractive
pharmaceutical target as well as a vaccine target.
Since S. aureus expresses many different virulence factors it can be
difficult to understand the role of a single virulence factor. We there-
fore used the non-pathogenic bacterium Lactococcus lactis as a host
to heterologously express ClfA on its surface.
When mice were infected i.v. with either L. lactis vector or L. lactis
ClfA, L. lactis ClfA infected mice had a dramatically lower survival
rate as compared to L. lactis vector infected mice. When the mice were
examined in detail, the L. lactis ClfA-infected mice had a rapid onset
of thrombocytopenia and gastrointestinal bleedings. The observed
virulence was not a general property of S. aureus MSCRAMMs, since
L. lactis SdrC and L. lactis SdrD did not induce virulence in the mice.
Using a non-Fg binding mutant strain of L. lactis ClfA, the virulence
was significantly reduced and resulted in lower bacterial load in the
blood. Interestingly, MyD88-/- mice were not resistant to the L. lactis
ClfA-induced virulence, suggesting that the innate immune system is
not mediating the pathology.
Fg cD5 mice lack the five most C-terminal amino acids in the Fg c-chain and as a consequence can not bind ClfA or platelet integrin
aIIbb3. Fg cD5 mice were resistant to the L. lactis ClfA induced viru-
lence as compared to wild-type mice, suggesting that the Fg-binding
of ClfA is mediating the virulence.
O8-53D virtual histology using MR-T1 mapping toquantify venous thrombus organisationSaha P, Blume U, Varma G, Wiethoff A, Schaeffter T, Evans C,Ahmad A, Patel A, Modarai B, Waltham M and Smith AKing’s College London, London, UK
Introduction: Novel thrombolytic delivery systems are changing the
paradigm of treatment for deep vein thrombosis (DVT), but only
fresh thrombi are suitable for these interventions. Current imaging
methods are unable to characterise the organisation of venous
thrombi, which would help direct therapy. A technique that identifies
patients in whom thrombolysis has the greatest potential would be
beneficial.
Methods: An MRI 3D T1-mapping sequence was optimised for small
animal imaging and applied to experimental venous thrombi induced
in the inferior vena cava (IVC) of BLAB/C mice (n = 27). T1-relaxa-
tion times were quantified after 7, 10, 14, 21 and 28 days using cus-
tom-made software implemented in MATLAB. Histological sections
of thrombi were processed for markers of organisation including red
cell and collagen content (MSB stain). Image analysis software was
used to calculate the percentage area of thrombus containing stain
and compared to corresponding MR slices. Three-blinded observers
validated results.
Results: Typical examples of MRI and histology are shown in fig 1.
Young thrombi have a short T1 relaxation time that increases with
thrombus age (R2 = 0.69, P < 0.0001). Collagen content, a marker
of organising thrombi, is directly proportional to T1 relaxation time.
Short T1 relaxation times were correlated with low amounts of colla-
gen (R2 = 0.80, P < 0.0001).
Conclusions: This is the first study to show that non-invasive, MR
T1-mapping can quantify venous thrombus organisation. This tech-
nique could be used to predict clinical outcome following deep vein
thrombosis; guide management; and assess the efficacy of novel
treatments.
Fig. 1. L. lactis ClfA is a virulence factor in mice.
Fig. 1. MRI images and corresponding histological sections. Venogra-
phy demonstrates recanalisation of the IVC between day 7 and 28.
MSB sections of thrombus show reduced red cells (yellow) and
increasing organisation (blue=collagen content) of thrombus (T) dur-
ing its resolution (· 200, Bar = 200 lm). 3D T1-mapping shows
short relaxation times in young, fresh thrombi (red) that increase
with thrombus age and organisation (green).
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
ORAL PAPERS 21____________________________________________________________________________________

D-dimer and Fibrinolytic Markers
O9A-2D-dimer: the lack of comparability of test results andpossibilities for harmonizationMeijer PECAT Foundation, Leiden, The Netherlands
The measurement of D-Dimer largely contributes to the diagnostic
work-up of venous thromboembolism (VTE). Today more than 30
different commercial available test are used by clinical laboratories.
The numerical test result may differ between methods due to the het-
erogeneity of the analyte in the patient sample, the variation in the
specificity of antibodies and the kind of calibrator used in the test.
In a recent survey of the external quality assessment programme of
the ECAT Foundation this was clearly demonstrated by the use of a
highly positive patient sample (4–5 mg FEU/L) and a dilution of this
sample to a level close to the cut-off level. The ratio between these
two samples varied from 6 to 11 between the 11 most frequently used
methods in this survey.
This lack of standardization of D-Dimer results may be confusing in
daily laboratory and clinical practice.
Since 1995 several approaches for standardization and harmonization
towards D-Dimer methods were conducted, mostly within the frame
work of the SSC subcommittee on Fibrinolysis of the SSC. An over-
view will be given of the different standardization and harmonization
approaches, including the pros and cons of these approaches. Special
attention will be given to a model for harmonization which relies on
the transformation of an assay-specific regression line to a reference
regression line (P. Meijer et al. Thromb Haemost 2006; 95: 567–572).
This approach forms the basis for further development of a harmoni-
zation model within the SSC framework of the ISTH. An update will
be given on the current status.
O9A-3Performance of the Vidas D-dimer assay to rule outvenous thromboembolism across age categories in1004 consecutive out-patientsToulon P1, Claessens Y2, Allo JC2 and Dhainaut JF2
1CHU Cimiez, Laboratoire Hmatologie, Nice Cedex 1; 2Service
d’Accueil et de Traitement des Urgences, Hopital Cochin, Paris,
France
D-dimer levels below a well defined cut-off level enable to safely rule
out VTE in patients with a low or intermediate pre-test probability
of VTE, with a negative predictive value (NPV) around 100%. As
ageing is associated with increased concentrations of coagulation
markers including D-dimers, the question was raised of their useful-
ness to rule out VTE in elderly patients. We prospectively evaluated
the performance of Vidas D-dimer assay (BioMerieux), in 1004 con-
secutive out-patients with a low or intermediate pre-test probability
(Wells’ probability score). Standardized diagnostic procedures were
applied to assess VTE, with a 3 month-follow up.
VTE were confirmed in 70 patients: D-dimers level was above the
cut-off value (500 ng/mL) in 67 patients and below that level in three
patients, leading to NPV = 99.4% and sensitivity = 95.8%. D-dimer
assay specificity dramatically decreased in an age-dependent manner.
However, sensitivity and NPV remained nearly maximal in each age
category including older patients.
The Vidas D-dimer assay was found to perform well in 1004 unse-
lected patients suspected of VTE with an overall NPV = 99.4%.
However, the negative correlation between test specificity and age,
leading to high percentage of increased D-dimer test results in elderly
patients particularly those above 80 years old, raised the question of
its usefulness in those very old patients.
Table 1 for O9A-3
Age
(year)
Patients
(n)
VTE
(n)
Sensitivity
(95% CI)
Specificity
(95% CI)
NPV
(95% CI)
< 30 91 5 80% (28.4–99.5) 83.5% (74.3–90.5) 98.7% (93.0–100)
30–39 121 5 80% (28.4–99.5) 75.6% (67.0–83.0) 98.9% (94.0–100)
40–49 151 7 100% (59.0–100) 78.7% (71.3–84.9) 100% (96.9–100)
50–59 155 6 83.3% (35.9–99.6) 69.2% (61.4–76.4) 99.1% (95.0–100)
60–69 142 11 100% (71.5–100) 56.0% (47.1–64.5) 100% (95.2–100)
70–79 165 14 100% (76.8–100) 33.3% (26.1–41.1) 100% (93.4–100)
80–89 134 18 100% (81.5–100) 10.1% (5.3–17.0) 100% (73.5–100)
> 90 45 4 100% (39.8–100) 7.3% (4.0–20.0) 100% (29.2–100)
Total 1,004 70 95.8% (88.0–99.0) 57.4% (54.2–60.5) 99.4% (98.4–99.9)
O9A-4Different cut-off values of quantitative D-dimer (DD)assays to establish duration of oral anticoagulationtreatment (OAT) after venous thromboembolism (VTE)Legnani C, Cosmi B, Cini M and Palareti GUniversity Hospital S. Orsola-Malpighi, Bologna, Italy
The PROLONG study showed that continuing OAT in patients with
abnormal DD (evaluated by a qualitative assay, Clearview Simplify
D-dimer) resulted in a significant reduction of VTE recurrence. Theo-
retically, if the DD measurement has to be used to stratify the VTE
recurrence risk, each DD assay should be independently assessed in a
management study as the PROLONG. Nevertheless, several clinicians
have already adopted the DD-based risk stratification and implemen-
tation of OAT based on the PROLONG results, using quantitative
DD assays in the absence of method-specific validated cut-off values
for this clinical application.
The present study retrospectively analyzed a subgroup of patients
enrolled in the PROLONG study to define cut-off values of six quan-
titative D-dimer methods to predict the risk of VTE recurrence.
We measured DD levels by the VIDAS D-dimer Exclusion (Bio-
merieux), Biopool AutoDimer (Biopool), HemosIL D-dimer and He-
mosIL D-dimer HS (Instrumentation Laboratory), Innovance D-
dimer (Siemens) and STA Liatest D-dimer (Diagnostica Stago) in fro-
zen plasma aliquots sampled 30 � 10 days after OAT cessation in
321 patients enrolled in the PROLONG study who did not resumed
OAT.
During follow-up (542 year), 25 (7.8%) pts had recurrent VTE. Since
DD levels increase with age and are significantly higher in females
than in males, we calculated method specific cut-off values according
to age and gender. The criteria used to select these cut-off values (see
Table) were: 1) % of patients with altered DD between 36–40%; 2)
% of VTE recurrence as low as possible in patients with normal DD.
These data suggest that different cut-off values according to methods,
patient’s age and gender are indicated to identify patients at higher
risk for VTE recurrence. Furthermore, they are different than those
used in diagnostic strategies to rule out acute VTE. These method
specific cut-off values are being evaluated in the ongoing prospective
management multicenter DULCIS study.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
22 ORAL PAPERS____________________________________________________________________________________

Table 1 for O9A-4
Cut-off values in ng/ml
Males Females
£ 70 year > 70 year £ 70 year > 70 year
VIDAS D-dimer exclusion* 490 1050 600 1300
Biopool autodimer & 90 190 111 240
HemosIL D-dimer & 205 300 225 330
HemosIL D-dimer HS & 170 345 215 430
Innovance D-dimer* 500 950 550 1150
STA Liatest D-dimer* 340 700 450 1050
*Results expressed in FEU; & results expressed in D-dimer units.
O9A-5Inflammatory and thrombotic markers in patients withST-elevation myocardial infarction treated withfibrinolysis and early PCIHalvorsen S, Seljeflot I, Bøhmer E and Arnesen HOslo University Hospital, Oslo, Norway
Background: The optimal treatment following fibrinolysis in patients
with ST-elevation myocardial infarction (STEMI) is still debated, but
several studies have shown improved outcomes with early transfer for
percutaneous coronary intervention (PCI). The aim of this study was
to investigate whether circulating levels of inflammatory and throm-
botic markers differ in patients treated with early versus late invasive
strategy following fibrinolysis.
Materials and Methods: This is a substudy of the NORwegian study
on District treatment of ST-elevation Myocardial Infarction (NOR-
DISTEM). Patients with STEMI of < 6 h duration and expected
time delay to PCI > 90 min were treated with tenecteplase, aspirin,
clopidogrel and enoxaparin, and randomized to early invasive
(n = 134) or ischemia-guided (late invasive) strategy (n = 132). Fast-
ing blood samples were collected in the morning 3 days and 3 months
after onset of STEMI for determinations of CRP, TNFa, IL- 6, IL-
10, IL-18, MCP-1, D-dimer, soluble TF and soluble CD40L. Com-
mercial available ELISA kits were used.
Results: After 3 days, D-dimer levels were higher and soluble CD40L
levels lower in the early compared to the late invasive group
(P = 0.001 and P = 0.008, respectively). The differences were abol-
ished after 3 months. No differences in other variables were observed.
The median change over time did not differ between groups, except
for D-dimer levels which were significantly more reduced in the early
invasive compared to the late invasive group (42% vs. 24% reduc-
tion, P = 0.002).
Conclusions: In STEMI patients treated with fibrinolysis and early
invasive strategy, D-dimer levels were higher after 3 days compared
to late invasive strategy, possibly due to early discontinuation of anti-
coagulation. No differences between treatment strategies were found
in other inflammatory markers. The clinical consequences of early
discontinuation of anticoagulation in these patients should be deter-
mined.
O9A-6Tissue plasminogen activator, fibrin D-dimer and VonWillebrand factor antigens and risk of future coronaryheart diseaseThompson A1, Lowe GD2, Rumley A2, Eiriksdottir G3, Danesh J1
and Gudnason V3
1University of Cambridge, Cambridge; 2University of Glasgow,
Glasgow, UK; 3Icelandic Heart Association, Reykjavik, Iceland
Background: Activation of blood coagulation and fibrinolysis may be
associated with increased risk of coronary heart disease (CHD).
Objectives: To assess associations of long-term circulating levels of
tissue plasminogen activator (t-PA), fibrin D-dimer and von Wille-
brand factor (vWF) antigens with CHD risk.
Methods: Measurements were made in 1925 people who had a
first-ever nonfatal myocardial infarction or died of CHD during
follow-up (median 19 years), and in 3616 controls nested within
the prospective population-based Reykjavik Study. Correction for
within-person variability was made using serial measurements taken
several years apart. Meta-analyses of published reports put the new
findings in context.
Results: The year-to-year variability of t-PA and D-dimer concentra-
tions within individuals was relatively high, yielding regression dilu-
tion ratios of 0.36 (95% CI: 0.26–0.47) for t-PA, and 0.28 (0.20–0.36)
for D-dimer. vWF was about as variable as total cholesterol, with a
regression dilution ratio of 0.54 (0.45–0.63). Ignoring such variability,
the odds ratios (ORs) for CHD adjusted for several vascular risk fac-
tors per 2 standard deviation (SD) higher measured levels were 1.06
(0.90–1.25) with t-PA, 1.12 (0.97–1.30) with D-dimer, and 1.19 (1.03–
1.37) with vWF. After correction for within-person variability, the
corresponding ORs were 0.89 (0.64–1.25), 1.11 (0.89–1.39), and 1.17
(1.01–1.36) respectively. When combined with the results from previ-
ous prospective studies, overall adjusted ORs were 1.44 (1.16–1.78)
with t-PA (11 studies, 4535 CHD cases); 1.57 (1.31–1.88) with
D-dimer (12 studies, 5123 cases); and 1.34 (1.13–1.59) with vWF
(10 studies, 4115 cases) per 2-SD higher baseline level.
Conclusions: Circulating levels of t-PA, D-dimer and vWF may be
more modestly associated with risk of CHD than previously reported,
particularly over the longer term. More detailed analyses, perhaps
involving pooling of individual data from prospective studies are
required to clarify the relevance of such markers to CHD.
O9A-7Plasma levels of fibrinolytic proteins and the risk ofmyocardial infarction in menLisman T1, Meltzer ME2, Meijers JCM3, de Groot PG4,Doggen CJM2 and Rosendaal FR2
1University Medical Center Groningen, Groningen; 2LUMC,
Leiden; 3AMC, Amsterdam; 4UMCU, Utrecht, The Netherlands
Hypofibrinolysis as measured with overall clot lysis assays is associ-
ated with an increased risk of arterial thrombosis. Individual com-
ponents of the fibrinolytic system, however, have not been studied
extensively in relation to arterial disease or results of studies were
inconsistent. The relation between plasminogen and a2-antiplasmin
levels and cardiovascular risk factors and the association between
plasminogen, a2-antiplasmin, thrombin-activatable fibrinolysis inhibi-
tor (TAFI), tissue-plasminogen activator (t-PA), and plasminogen
activator inhibitor-1 (PAI-1) and risk of myocardial infarction was
investigated in the Study of Myocardial Infarctions Leiden (555
men with a first myocardial infarction and 635 controls). a2-Anti-
plasmin was associated with age and lipid levels while plasminogen
correlated with lipids, C-reactive protein and smoking. Increased
levels of all fibrinolytic factors were associated with myocardial
infarction, except for TAFI which protected against myocardial
infarction at high levels. Age-adjusted odds ratios (OR) (95% confi-
dence interval) for quartile 4 compared with 1 were 1.7 (1.2–2.3)
for plasminogen, 1.9 (1.3–2.6) for a2-antiplasmin, 0.4 (0.3–0.5) for
TAFI, 1.7 (1.2–2.3) for t-PA, and 1.7 (1.2–2.4) for PAI-1. After
adjusting for cardiovascular risk factors, only a2-antiplasmin (OR
1.4 (1.0–2.0)) and TAFI levels (OR 0.3 (0.2–0.4)) remained associ-
ated with risk (OR 1.4 (1.0–2.0)). t-PA and PAI-1 levels predomi-
nantly reflected lipid levels whereas plasminogen reflected the
inflammatory state. Concluding, elevated a2-antiplasmin and
decreased TAFI levels are independently associated with risk of
myocardial infarction. We hypothesize that the protective effect of
high TAFI levels relates to its anti-inflammatory properties. t-PA,
PAI-1, and plasminogen levels appear to reflect other cardiovascular
risk factors.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
ORAL PAPERS 23____________________________________________________________________________________

Structure, Function and Regulation of the Plasminogen Activator
System
O9B-1Regulation of cell surface proteolysis and cellmigration by the novel plasminogen receptor, Plg-RKTMiles LA1, Lighvani S1, Baik N1, Diggs JE1, Parmer CM1,Kiosses WB1, Bai H2, Booth NA3, and Parmer RJ21The Scripps Research Institute; 2University of California San
Diego and Veterans Admin. San Diego Healthcare Sys., La Jolla,
USA; 3University of Aberdeen, Aberdeen, UK
The integral membrane plasminogen receptor, Plg-RKT, has a
unique cell surface orientation that facilitates cell surface proteoly-
sis. Plg-RKT exposes a C-terminal lysine on the cell surface allow-
ing interaction with the kringle domains of plasminogen. The C-
terminus of Plg-RKT also interacts, specifically, with t-PA. Further-
more, Plg-RKT is highly spatially co-localized with the uPAR as
revealed in confocal microscopy and co-immunoprecipitation stud-
ies. Cell surface-dependent plasminogen activation by either t-PA
or u-PA is markedly inhibited by antibodies directed against the C-
terminus of Plg-RKT. Differentiation of monocytes along the
monocyte/macrophage lineage results in the induction of Plg-RKT.
Therefore, we investigated the role of Plg-RKT in plasmin(ogen)-
dependent macrophage migration both in vitro and in vivo. U937
human myelomonocytic cells that express high levels of Plg-RKT
were used to study cell migration induced by monocyte chemoattr-
actant protein (MCP-1) in transwells. In the presence of plasmino-
gen, cell migration was markedly decreased by anti- Plg-RKT
mAb, compared to the isotype control. Anti-Plg-RKT mAb did
not significantly affect cell migration in the absence of plasmino-
gen. In a peritoneal inflammation model, C57BL/6 female mice
were injected intravenously with either anti-Plg-RKT mAb or iso-
type control prior to intraperitoneal injection with 3% thioglycol-
late, and a second intravenous injection of mAb. Cells were
harvested by peritoneal lavage. Anti-Plg-RKT mAb inhibited mac-
rophage recruitment in a dose-dependent manner [at the maximum
dose of 27 lg/g, 58 � 5.4% fewer macrophages were recovered
compared to the isotype control (P < 0.001, n = 5)]. Macrophage
recruitment was significantly decreased in plasminogen null mice
compared to wild type littermates, as previously reported. We
found no effect of anti-Plg-RKT mAb upon macrophage recruit-
ment in plasminogen null mice. These results suggest a major role
of Plg-RKT in plasmin(ogen)-dependent regulation of the inflam-
matory response.
O9B-2The novel plasminogen receptor, Plg-RKT, regulatescatecholaminergic functionParmer RJ1, Bai H2, Baik N3, Kiosses WB3, Krajewski S4 andMiles LA3
1University of California; 2Veterans Administration San Diego
Healthcare System, San Diego; 3The Scripps Research Institute;4Sanford/Burnham Medical Research Institute, La Jolla, CA, USA
Local generation of plasmin is markedly enhanced when plasmino-
gen is bound to the surface of catecholaminergic cells, and cate-
cholamine release by the sympathoadrenal system is negatively
regulated by prohormone cleavage products formed from plasmin-
mediated proteolysis. We recently identified a novel transmembrane
plasminogen receptor, Plg-RKT. Here, we investigated the expres-
sion and subcellular localization of Plg-RKT in catecholaminergic
cells and examined the role of Plg-RKT in catecholaminergic func-
tion. Prominent staining with anti-Plg-RKT mAb was observed in
adrenal medullary chromaffin cells of both human and murine tis-
sue. In western blotting, Plg-RKT was highly expressed in murine
adrenal gland, bovine adrenomedullary chromaffin cells, human
pheochromocytoma tissue, PC12 rat pheochromocytoma cells as
well as in purified rat hippocampal neurons. PC12 cells were
transfected with an expression vector encoding Plg-RKT fused in-
frame to GFP. Confocal analysis of the transfectants demonstrated
that the GFP signal was present at the cell membrane and
colocalized with wheat germ agglutinin, a surface marker
(79 � 5% colocalization). In phase partitioning experiments, Plg-
RKT partitioned to the detergent phase, consistent with Plg-RKT
behaving as an integral membrane protein. In the presence of anti-
Plg-RKT mAb, cell surface plasminogen activation was markedly
suppressed, compared to PC12 cells incubated with isotype control.
Correspondingly, cells stably overexpressing Plg-RKT exhibited
enhanced plasminogen binding and enhanced cell-surface plasmino-
gen activation, compared to cells stably expressing empty vector.
In functional secretion assays, cells overexpressing Plg-RKT exhib-
ited a marked decrease in nicotine-evoked 3H-norepinephrine
release (by 51 � 2%, P < 0.001), compared with control transfect-
ed cells. In conclusion, Plg-RKT is present on the surface of cate-
cholaminergic cells and functions to stimulate plasminogen
activation and modulate catecholamine release. This novel receptor
thus represents a new mechanism and novel control point for regu-
lating the interface between plasminogen activation and sympat-
hoadrenal function that may substantially influence
catecholaminergic stress responses.
O9B-3Effect of histone deacetylase inhibitors on tissue-typeplasminogen activator expression in humanendothelial cellsDunoyer-Geindre S and Kruithof EKOUniversity Hospital of Geneva, Geneva, Switzerland
Tissue-type plasminogen activator (t-PA) is produced by endothelial
cells (EC) and responsible for the removal of intravascular fibrin
deposits. We investigated the role of histone deacetylase (HDAC)
inhibitors on t-PA expression. HDAC are of major importance for
the epigenetic control of gene expression. Methylation analysis of
the proximal t-PA promoter revealed an island of unmethylated
CpG stretching from position -366 to +59, while upstream CpG’s
were all methylated. Acetylation of histones H3 and H4 by histone
acetyl transferases (HAT) is associated with active genes, whereas
removal of the acetyl groups by HDAC is associated with inactive
genes. Treatment of EC with HDAC inhibitors trichostatin (TSA)
and MS-275 resulted in a 7 and 13-fold increase of t-PA mRNA
expression, respectively, while expression of PAI-1 was increased
fourfold by MS-275, but not by TSA. As TSA inhibits both class I
and class II HDAC and MS-275 only class II HDAC, these results
imply a role for class I HDAC in the increased expression of t-PA
and PAI-1 and a role for a class II HDAC in PAI-1 reduction.
HDAC and HAT not only interact with histones but also with a
variety transcriptional regulators. To determine whether the effect
of the HDAC inhibitors on t-PA expression was related to changes
in histone acetylation we performed chromosome immunoprecipita-
tion analysis of the t-PA promoter using antibodies specific for acet-
ylated histone H3 or H4. We observed an increase in H3
acetylation of 10 � 3 and 44 � 14 -fold in EC treated with TSA or
MS-275, respectively, and in H4 acetylation of 7.7 � 1.4 and 16 � 3
- fold, respectively.
Thus, expression of t-PA by EC is suppressed by HDAC in a mecha-
nism that involves de-acetylation of histone H3 and H4. Reversal of
this epigenetic suppression increases t-PA expression by EC.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
24 ORAL PAPERS____________________________________________________________________________________

O9B-4Allelic imbalance of tissue-type plasminogen activator(tPA) gene expression in human brain tissueHultman K1, Tjarnlund-Wolf A1, Curtis M2, Faull R2, Medcalf RL3
and Jern C1
1Institute of Neuroscience and Physiology, Gothenburg, Sweden;2Department of Anatomy with Radiology, University of
Auckland, Auckland, New Zealand; 3Australian Centre for Blood
Diseases, Department of Clinical Haematology, Melbourne,
Australia
We have identified a single nucleotide polymorphism (SNP) at the
tPA locus (-7351C>T), which is associated with vascular tPA release
rates in humans and the risk of myocardial infarction. In vitro studies
demonstrated that this SNP is functional at the level of transcription,
and affects tPA gene regulation in endothelial cells. In the brain, tPA
has been implicated both in physiological and pathophysiological
processes. The aim of the present study was to examine the effect of
this SNP on tPA gene regulation in human brain tissue under in vivo
conditions. Human brain tissue was obtained from the Neurological
Foundation of New Zealand Human Brain Bank. Allelic expression
was determined in heterozygous samples by TaqMan assay using the
coding tPA 20 099T>C SNP as a marker for the -7351C>T SNP.
Thus, allele-specific gene expression is analysed in a normally func-
tioning nucleus where the different alleles are subjected to the same
genetic and environmental conditions. Protein-DNA interactions were
studied by EMSA and ChIP. In human brain tissue, a significantly
higher number of tPA mRNA transcripts were generated from chro-
mosomes expressing the wild-type C allele compared to the mutant
T allele (ratio C vs. T; mean � SEM, hippocampus 1.35 � 0.14,
P = 0.033, n = 12; cortex 1.25 � 0.10, P = 0.037, n = 12). EMSA
showed reduced neuronal and astrocytic nuclear protein binding
affinity to the mutant T-allele probe. Supershift experiments identified
Sp1 and Sp3 as the major transcription factors binding to the poly-
morphic site. ChIP analyses confirmed that Sp1 indeed recognised
the polymorphic enhancer in intact cells. The present study demon-
strates that the -7351C>T SNP affects tPA gene expression in
human brain tissue. As neurons are considered to be the major
source of tPA in the CNS, allele-specific tPA expression in these cells
may have a clinical impact in neurological conditions associated with
changes in plasminogen activation.
O9B-5Identification of proteins that selectively misfoldwithin the acutely injured brain and acceleratetPA-mediated plasmin formation: implications forischemic strokeSamson A, Borg RJ, Sashindranath M, Au AEL, Niego B,Cody SH and Medcalf RLMonash University, Melbourne, Australia
In the vasculature, fibrin acts as both a cofactor for tPA-mediated
plasmin formation and as a substrate for plasmin. An analogous situ-
ation arises in the brain whereby neuronal injury causes the forma-
tion of misfolded proteins. Like fibrin, these misfolded proteins
specifically bind tPA and plasminogen and act as a macromolecular
cofactor to promote tPA-mediated plasminogen activation (Samson
et al., Blood 2009).We have identified the intracellular proteins that
are most prone to aggregation during acute neuronal injury. Of the
proteins identified, we find that tubulin and GAPDH exhibit an espe-
cially strong propensity to misfold following a variety of in vivo (e.g.
traumatic brain injury) and in vitro (e.g. glutamate-induced excitotox-
icity) neuronal insults. One characteristic of misfolded proteins is
detergent-insolubility. Accordingly, we show that both tubulin and
GAPDH become detergent-insoluble following neuronal injury. Inter-
estingly, only the detergent-insoluble form of tubulin, and not the
soluble form, acts as a cofactor/substrate for tPA-mediated plasmin
formation. Another hallmark of misfolded proteins is their deposition
into spheroid-like structures within cells. We show that neuronal
injury causes the redistribution of tubulin from the cytoskeleton into
numerous intracellular spheroids which also act as a specific cofac-
tor/substrate for tPA-mediated plasmin formation.This is the first
description that GAPDH and tubulin can misfold and facilitate plas-
minogen activation following acute brain injury. Agents which block
the binding of tPA to aggregated tubulin and GAPDH would be
expected to specifically reduce plasminogen activation within the
injured brain whilst leaving fibrinolysis unperturbed. Such an
approach will likely improve the safety and efficacy of thrombolytic
therapy during ischemic stroke – a clinical situation where intravascu-
lar plasmin generation on fibrin is wanted, but where excessive tPA-
mediated plasmin formation in the injured brain is harmful.
O9B-6New functions of t-PA and factor XII in amyloid andprotein metabolismGebbink MCrossbeta Biosciences, Utrecht, The Netherlands
We identified in factor XII and t-PA a common domain, the fibro-
nectin-type I (or finger) domain, that could be shown to interact with
non-native proteins, including those comprising complex beta-sheet
structures such as crossbeta structure in amyloid. The consequences
of these interactions are multiple.
Stimulation of t-PA plasminogen activation was found common for
peptides and proteins that formed amyloid aggregates such as aggre-
gates of endostatin, amyloidbeta peptide, islet amyloid polypeptide
and fibrin peptides and fragments, ovalbumin, etc. The as such gener-
ated plasmin can be involved in processing amyloid-bound neuroen-
docrine factors, notably Chromogranin B and the neurosecretory
protein VGF, on the one hand, and in degradation of proteins/pep-
tides, most notably extracellular matrix components, such as fibrin
and vitronectin on the other hand.
Stimulation of the contact system (factor XII) can occur via protein
binding to surfaces. Traditional activators, such as kaolin, ellagic acid
and dextran sulphate do not induce factor-dependent kallikrein for-
mation in the absence of sufficient protein. Adsorption of protein can
result in unfolding into a non-native state. In agreement, non-native
proteins, including amyloid-beta can induce factor-FXII mediated
kallikrein formation in the absence of such traditional activator. This
route of non-native protein dependent activation can be exclusive for
kallikrein formation and leaves coagulation activation via factor XI
untouched. This process is considered of relevance for local oedema
formation involving bradykinin formation.
It is expected that in vivo several of these processes run in parallel
and may cooperate. The most appealing question is for each stimula-
tor of t-PA and contact system what is the exact profile of subse-
quent activation pathways.
It is concluded that a systematic study of stimulators is required to
overview the consequences of the newly discovered pathways of acti-
vation of t-PA and factor XII.
O9B-7Engineering Kunitz 1 domain (KD1) of human tissuefactor pathway inhibitor-2 to selectively inhibitfibrinolysis: properties of KD1-L17R variantBajaj MS1, Ogueli I1, Schmidt E2, Shanker S1, Velander W3,Calcaterra J3 and Bajaj SP1
1UCLA, Los Angeles, CA; 2Washinton University, St. Louis, MO;3University of Nebraska, Lincoln, NE, USA
Tissue factor pathway inhibitor-2 (TFPI-2) inhibits factor XIa, kallik-
rein and factor VIIa/tissue factor; accordingly, it has been proposed
for use as an anticoagulant. Full-length TFPI-2 or its isolated first
Kunitz domain (KD1) also inhibits plasmin and has been proposed
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
ORAL PAPERS 25____________________________________________________________________________________

for use as an antifibrinolytic agent. However, the anticoagulant prop-
erties of KD1 would diminish its antifibrinolytic function. In this
report, structure based investigations and analysis of the serine prote-
ases profiles revealed that coagulation enzymes prefer a hydrophobic
residue at the P2’ position in their substrates/inhibitors, whereas plas-
min prefers a positively charged residue at the corresponding posi-
tion. Thus, we changed the P2’ residue Leu17 in KD1 to Arg (KD1-
L17R) and compared its inhibitory properties with the wild-type
KD1 (KD1-WT). Both WT and KD1-L17R were expressed in E.
Coli, folded and purified to homogeneity. Amino-terminal sequences
and mass-spectra revealed proper folding of both proteins. Compared
to KD1-WT, the KD1-L17R neither prolonged aPTT of normal
plasma nor did it inhibit factor XIa, kallikrein or VIIa/tissue factor.
Further, KD1-L17R inhibited plasmin with ~5-fold increased affinity.
In mouse liver laceration model and tail transection bleeding model,
KD1-L17R was, respectively, ~6-fold and ~2-fold more effective than
KD1-WT in preventing blood loss. Importantly, in these bleeding
models, KD1-L17R was more effective than aprotinin (bovine pan-
creatic trypsin inhibitor), which has been used as an antifibrinolytic
agent to prevent blood loss during major surgery/trauma. Further, as
compared to aprotinin, renal toxicity was not observed with KD1-
WT or KD1-L17R. In rotational thromboelastography experiments,
KD1-WT and aprotinin increased the clotting time and clot forma-
tion time of whole blood whereas KD1-L17R had no effect. Plasmin-
induced fibrinolysis in whole blood or a purified system measured by
clot strength was prevented by KD1-L17R and aprotinin but not by
KD1-WT. KD1-L17R may be a superior therapeutic agent to prevent
fibrinolysis and blood loss in major surgery/trauma.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
26 ORAL PAPERS____________________________________________________________________________________

Fibrinolysis in Disease
O10A-1Plasminogen deficiency in mice causes periodontaldiseaseSulniute R1, Lindh T2, Li J1 and Ny T1
1Umea University, Umea; 2County Council of Vasterbotten, the
National Dental Service/Periodontics, Ume, Sweden
Periodontal disease involves bacterial infection, periodontium inflam-
mation, gum tissue degradation, and alveolar bone resorption leading
to teeth loss. In human, plasminogen deficiency causes ligneous peri-
odontitis. Therefore, we decided to examine oral health of plasmino-
gen deficient mice and their wild type littermates to establish a mouse
model for studying the roles of Plg activation system in periodontal
disease.
The periodontium in wild type mice was unaffected at all time points
studied whereas in plg deficient mice periodontitis progressed rapidly
within 20 weeks. Morphological studies revealed detachment of gingi-
val tissue, resorption of cementum layer, formation of necrotic tissue,
and severe alveolar bone degradation in plg deficient mice. The
immunohistochemical staining indicated a mass infiltration of neu-
trophils in the periodontal tissues. Interestingly, mice deficient in both
plasminogen activators, tPA and uPA, developed periodontal disease
similar to plg deficient mice, although mice lacking either of PAs
remained healthy in periodontium. Furthermore, supplementation
with human plasminogen for 10 days led to recovery of the periodon-
tium and removal of necrotic tissue in plg deficient mice. In addition,
quantification of alveolar bone revealed significant difference com-
pared to control mice, suggesting even possible alveolar bone
re-growth.
Our data demonstrated that plasminogen is essential to maintain
healthy periodontium and plays an important role against the sponta-
neous development of chronic periodontal disease. Moreover, revers-
ibility to the healthy status after supplementation suggests the
possibility of using plasminogen for a clinical therapy of periodontal
diseases.
O10A-2Biological variation in tPA-induced plasma clot lysistimeTalens S, Malfliet JJMC, Rudez G, de Maat MPM and Rijken DCErasmus Medical Center, Rotterdam, The Netherlands
Hypofibrinolysis is a risk factor for venous and arterial thrombosis,
and can be established by measuring the plasma fibrinolytic potential
in a turbidimetric tPA-induced clot lysis time assay. However, not
much is known about the biological variation in clot lysis time. It is
important to obtain information about the variation when clot lysis
time is tested as risk factor for thrombosis in future studies. Thus,
this study aimed to determine the analytical, within-subject and
between-subject variation. We collected blood samples from 40
healthy individuals throughout a period of 1 year (average 13 visits)
and determined the clot lysis time of each plasma sample in dupli-
cate. The mean (� SD) clot lysis time was 83.7 (� 10.9) min. The
coefficient of variations for total variation, analytical variation,
within-subject variation and between-subject variation were 13.0%,
3.7%, 8.0% and 10.0%, respectively. One measurement of clot lysis
time was sufficient to establish the habitual value which does not
deviate more than 20% from its true value with a probability of
95%. The contribution of analytical imprecision to the within-subject
variation was 10.2%, the index of individuality was 0.88 and the ref-
erence change value was 24.4%. We observed that the clot lysis time
was prolonged in the morning compared to the afternoon and was
slightly higher in older individuals compared to younger individuals.
There was no seasonal variation observed. This study provides
insight into the biological variation of clot lysis time, which can be
used in future studies using clot lysis time as a potential risk factor
for thrombosis.
O10A-3Plasma fibrinolytic capacity and the risk of arterialthrombosis in young womenSiegerink B1, Meltzer M1, de Groot PG2, Algra A2, Lisman JA3
and Rosendaal FR1
1LUMC, Leiden; 2UMC Utrecht, Utrecht; 3UMC Groningen,
Groningen, The Netherlands
Background: Recently, reduced overall fibrinolytic capacity has been
shown to increase the risk of arterial thrombosis, especially coronary
heart disease and myocardial infarction in young men. The role of
fibrinolysis in clinical ischaemic stroke is unclear. So far, studies on
fibrinolysis and atrial disease have mainly been focussed on men.
Objectives: With this study we aim to determine the risk of both
hyper- and hypofibrinolysis on the risk of myocardial infarction and
ischaemic stroke in young women.
Methods: The RATIO study is a population based case control study
including women (18–50 years) with myocardial infarction (MI;
N = 205), ischaemic stroke (IS; N = 175) and 638 healthy controls,
frequency matched on age, year of event and area of residence. Over-
all fibrinolytic potential was determined with a tissue factor and tis-
sue plasminogen activator induced clot lysis assay. Clot lysis time
(CLT) was divided into quintiles based on the levels found in the
control group (Q1–Q5), with the middle quintile (Q3) as reference.
Odds ratios, obtained from a logistic regression model, adjusted for
the matching factors and cardio vascular risk factors were calculated
as a measure of rate ratios.
Results: Hypofibrinolysis was associated with an increase in risk of
myocardial infarction (Q4, odds ratio 1.5; 95% CI 0.8–2.9 and Q5,
2.3; 1.2–4.4). Hyperfibrinolysis had no clear effect (Q2, 0.8; 0.4–1.8
and Q1, 1.8; 0.9–3.8). Hypofibrinolysis did not affect the risk of is-
chaemic stroke (Q4 0.8; 0.3–2.0 and Q5, 1.1; 0.5–2.5), whereas hyper-
fibrinolysis increased this risk fourfold (Q2 1.6; 95%CI 0.7–3.7 and
Q1, 3,9; 1.7–8.8).
Discussion: These results show that hypofibrinolysis is a risk factor
for myocardial infarction in young women, which is similar to find-
ings in men and mixed populations. Surprisingly, hyperfibrinolysis
increased the risk of ischaemic stroke fourfold.
O10A-4Venous thrombosis risk associated with plasmahypofibrinolysis is explained by elevated plasmalevels of TAFI and PAI-1Lisman T1, Meltzer ME2, de Groot PG3, Meijers JCM4, LeSessie S2, Doggen CJM2 and Rosendaal FR2
1University Medical Center Groningen, Groningen; 2LUMC,
Leiden; 3UMCU, Utrecht; 4AMC, Amsterdam, The Netherlands
Elevated plasma clot lysis time (CLT) as measured with a plasma-
based assay increases risk of venous and arterial thrombosis. It is,
however, unclear which fibrinolytic factors contribute to thrombosis
risk. In 743 healthy controls we investigated determinants of CLT.
By comparison with 770 patients with a first venous thrombosis we
assessed plasma levels of fibrinolytic proteins as risk factors for
thrombosis. Plasminogen activator inhibitor-1 (PAI-1) levels were the
main determinants of CLT, followed by plasminogen, thrombin acti-
vatable fibrinolysis inhibitor (TAFI), prothrombin, and a2-antiplas-min. Fibrinogen, factor VII, X, and XI contributed minimally. These
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
ORAL PAPERS 27____________________________________________________________________________________

proteins explained 77% of variation in CLT. Levels of these proteins
allowed accurate prediction of CLT. Levels of the fibrinolytic factors
were associated with thrombosis risk (odds ratios, highest quartile
versus lowest, adjusted for age, sex, and BMI: 1.6 for plasminogen,
1.2 for a2-antiplasmin, 1.6 for TAFI, 1.6 for PAI-1, 1.8 for tissue
plasminogen activator (t-PA)). Adjusting for acute-phase proteins
attenuated the risk associated with elevated plasminogen levels. The
risk associated with increased t-PA nearly disappeared after adjusting
for acute-phase proteins and endothelial activation. TAFI and PAI-1
remained associated with thrombosis after extensive adjustment. Con-
cluding, CLT reflects levels of all fibrinolytic factors except t-PA.
Plasminogen, TAFI, PAI-1, and t-PA are associated with venous
thrombosis. However, plasminogen and t-PA levels may reflect
underlying risk factors.
O10A-5Clot lysis time (CLT) of PRP and PPP inhypercholesterolemia. Effect of atorvastatin andrelationships with inflammatory markersMezzano D, Acevedo M, Pereira J, Matus V and Panes OSchool of Medicine, P. Universidad Catolica de Chile, Santiago,
Chile
The role of platelet fibrinolytic components in hemostatic balance is
largely ignored. A decrease in fibrinolysis is postulated in the patho-
genesis of arterial thrombosis in hypercholesterolemia and athero-
thrombosis, but studies reporting effect of statins on total fibrinolytic
capacity (FC) are controversial. Our aim was to study the contribu-
tion of platelets on clot lysis time in patients with hypercholesterol-
emia, before and after atorvastatin (80 mg/day, 1 month). We used
the CLT-PPP described by Lisman et al (Blood, 2005) and developed
an assay using PRP (CLT-PRP) to assess FC. In healthy controls,
(LDL-Chol = 108 � 27 mg/dL), lysis times with both assays were
essentially identical (25 � 12 min vs. 24 � 12 min, P = NS, n = 9),
denoting no influence of platelets in FC. In 7 hypercholesterolemic
patients (LDL-Chol = 193 � 46 mg/dL), FC was significantly
decreased, with prolongation of CLT’s in both assays. CLT-PRP val-
ues were higher than those of CLT-PPP (81 � 34 vs. 68 � 29 min,
respectively, P = 0.015), suggesting higher sensitivity of CLT-PRP
and enhanced platelet-derived hypofibrinolytic effect. CLT-PRP and
CLT-PPP were correlated with LDL-Chol (r = 0.62, P = 0.01), tri-
glycerides (r = 0.81, P = 0.0002) and PAI-1 concentration
(r = 0.74, P = 0.006, n = 16). CLT-PRP, but not for CLT-PPP,
was significantly correlated with acute-phase reactants (APhR): usC-
reactive protein (r = 0.81, P = 0.0002), fibrinogen (r = 0.55,
P = 0.029), VWF:Ag (r = 0.64, P = 0.014). After atorvastatin,
LDL-Chol decreased to 88 � 21 mg/dL. This was accompanied with
decreases, though not normalization, of CLT’s in both assays: CLT-
PPP to 44 � 22 min (P = 0.012) and CLT-PRP to 64 � 29 min
(P = NS). No significant changes in inflammatory markers resulted
from atorvastatin treatment.
Conclusions: (i) FC, assessed by CLT-PRP, is decreased in hypercho-
lesterolemia, and is closely related with plasma cholesterol, PAI-1
and inflammatory markers. (ii) FC improves after atorvastatin treat-
ment. (iii) CLT-PRP appears more sensitive than CLT-PPP to assess
the abnormal FC of hypercholesterolemia. (iv) Further studies will
determine the role of the platelet fibrinolysis components in states of
enhanced/decreased fibrinolysis.
O10A-6Leukocyte- and endothelial-derived microparticles: acirculating source for fibrinolysisLacroix R1, Plawinski L2, Robert S1, Doeuvre L3, Sabatier F1,Anfonso F1, Leroyer A1, Boulanger C1, Angles-Cano E3 andDignat-George F1
1INSERM U608, Marseille; 2CNRS; 3INSERM U919, Caen, France
Membrane microparticles (MPs) derived from activated platelets, leu-
kocytes and endothelial cells, are well described for their procoagu-
lant activity. We recently assigned a new fibrinolytic function to
endothelial-derived MPs (Blood 2007, 110: 2432). Since the relevance
of this novel mechanism of plasmin formation remains unsolved, we
investigated whether circulating MPs found in healthy subjects and in
pathological situations could be a source of fibrinolysis.
We first compared the ability of circulating MPs, isolated from blood
of patients (atherosclerotic and auto-immune diseases, thrombotic
thrombocytopenic purpura: TTP) and healthy subjects to generate
plasmin activity. Plasmin generation on circulating MPs was signifi-
cantly higher in patients compared to healthy controls. Circulating
MPs from patients with TTP generate a range of plasmin activity
indicating a variable content in either urokinase- (uPA) or tissue-type
plasminogen activator (tPA). Complexes between tPA and plasmino-
gen activator inhibitor-1 (PAI-1) were also identified. In all cases,
plasmin generation was consistent with a lysine-dependent mechanism
for plasminogen binding and activation.
To determine the origin of MPs bearing this fibrinolytic activity, we
generated MPs from circulating blood subpopulations and from dif-
ferent human endothelial cell types. Plasmin generation was detected
on endothelial- and leukocyte-derived MPs, but was absent on plate-
lets- or erythrocyte-derived MPs. These findings were confirmed by
depletion of target MPs from plasma of patients with TTP. Leuko-
cyte-derived MPs express uPA and its receptor uPAR, but not tPA.
By contrast, tPA and tPA/PAI-1 complexes were detected in endothe-
lial-derived MPs with variations according to their anatomical origin
while uPA remained undetectable.
In conclusion, our study suggests that the fibrinolytic activity in the
circulation is supported by MP-borne uPA or tPA, derived from leu-
kocyte or endothelial cells. The fibrinolytic activity of these MPs is
modulated in pathological settings.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
28 ORAL PAPERS____________________________________________________________________________________

Fibrin(ogen) and Repair
O10B-1Two cases of dysfibrinogenemia associated withthrombosisKotlin R, Khaznadar T, Suttnar J, Riedel T, Salaj P and Dyr JEInstitute of Hematology and Blood Transfusion, Praha 2, Czech
Republic
Fibrinogen, a 340 kDa glycoprotein, is synthesized by hepatocytes
and secreted to the circulation at a level in the range 2–4 g/L. Fibrin-
ogen plays an important role in many physiological processes, espe-
cially in blood coagulation; but it is also known thrombotic risk
factor. After injury, fibrinogen undergoes conversion into fibrin clot.
Fibrin network, if not needed anymore, undergoes proteolytic diges-
tion called fibrinolysis. Fibrinolysis is catalysed by the serine protease
plasmin. Inherited mutations in fibrinogen, causing congenital dysfi-
brinogenemia, may affect fibrinolysis what may lead to thrombosis.
Fibrinogens of two unrelated patients, both with history of throm-
botic events, pulmonary embolism and indication of dysfibrinogen-
emia, were studied. No common thrombotic risk factors were found.
Both dysfibrinogens showed remarkably delayed fibrin polymeriza-
tion after addition of either thrombin or reptilase. tPA-mediated
fibrinolysis was significantly slower than control. The most noticeable
delay occurred during the final stages of what appeared as a diphasic
lysis. DNA sequencing showed the heterozygous mutations c Tyr363-
Asn in one patient and Aa Asn106Asp in the second one. Both
abnormal fibrinogens caused the decrease of platelet aggregation.
Morphologies of both clots, studied by electron microscopy, showed
abnormal fibrin network with narrower fibers and abrupt fibril termi-
nations. Mutation c Tyr363Asn is situated in polymerization pocket
‘a’ in loop III in the P-domain of the c-nodule and is highly con-
served across species. The mutation Aa Asn106Asp is situated in the
coiled-coil connector of fibrinogen and the importance of Aa Asn106
is strengthened by its conservation.
This work was supported by a grant of The Internal Grant Agency
of The Ministry of Health of the Czech Republic, number NS 9636-
3/2008; by a grant of The Ministry of Health of the Czech Republic,
number 2373601; and by a grant of The Academy of Sciences of the
Czech Republic, number KAN200670701.
O10B-2Biologically active human fibrinogen produced in themilk of transgenic cowsCalcaterra J1, Vancott KE1, Forsberg EJ2, Inan M1, Germano M3,van Veen HV3, Nelson K2 and Velander WH1
1University of Nebraska-Lincoln, Lincoln, NE; 2Pharming
Healthcare, Inc., Deforest, WI USA; 3Pharming Technologies
B.V., Leiden, The Netherlands
In the future, hemostatic therapies will likely include recombinant
human fibrinogen (r-F1) as a preferred alternative to human plasma-
derived (pd-) fibrinogen (pd-F1) products. Here we characterize r-F1
purified from the milk of cloned, transgenic cows producing 2 to
4-fold higher concentrations than the pd-F1 found in human plasma.
Three transgenes consisting of genomic A-alpha, B-beta and gamma
fibrinogen genes under the control of the bovine alpha s1-casein pro-
moter were co-inserted into a female somatic cell lineage which was
used to make founder animals by nuclear transfer. The stoichiometric
ratio and molecular weights of alpha, beta and gamma chains as
judged by mass spectroscopy and SDS-PAGE were similar for pd-F1
and r-F1. The phosphorylation content at Ser-3 in fibrinopeptide
FpB is complete in r-F1 whereas only 30% of Ser-3 is phosphory-
lated in pd-F1. Glycosylation of r-F1 features mostly neutral, milk
protein-like glycoforms relative to the more acidic pd-F1. In vitro
findings indicate that the molecular and viscoelastic properties of
r-F1 clot formation are similar to those of pd-F1 when treated with
pd-thrombin (FIIa) and Factor XIII (FXIII). No contaminating
transglutaminase or fibrinolytic activity was found in r-F1 prepara-
tions. Proteolytic cleavage of r-F1 alpha and beta chains by thrombin
was similar to pd-F1. Formation of gamma-gamma dimers in the
presence of FXIII was faster for r-F1 compared with pd-F1. Throm-
boelastographic (TEG) analyses of fibrin formation confirmed similar
formation kinetics and maximum amplitudes between r-F1 and
pd-F1. These molecular properties make r-F1 desirable for use in
fibrinogen replacement therapy and as fibrin sealants.
O10B-3The density of surface bound fibrinogen effects therelease of fibrinopeptidesDyr JE1, Medved L2, Riedel T1 and Suttnar J11Institute of Hematology and Blood Transfusion, Prague, Czech
Republic; 2University of Maryland School of Medicine,
Baltimore, MD, USA
Fibrinogen and fibrin play overlapping roles in blood clotting, fibri-
nolysis, cellular and matrix interactions, the inflammatory response,
wound healing, and neoplasia. Fibrin polymerization is initiated by
thrombin cleveage of the fibinopeptides A and B (FPA, FPB), con-
verting fibrinogen to fibrin monomer. During fibrin polymerization in
solution the release of FPA occurs very rapidly while the release of
FPB is delayed and reaches its maximum when fibrin formation is
almost completed. Numerous studies demonstrated that fibrinogen in
solution and fibrinogen adsorbed on various surfaces exhibit different
properties.We previously reported that fibrinogen adsorbs on artifical
surfaces in basically two different orientation, side-on and end-on.
While side-on orientation prevails during adsorption from low fibrin-
ogen concentrations, the other orientation, in which adsorbed fibrino-
gen is close-packed, occurs at high fibrinogen concentrations. The
adsorbed fibrinogen molecules in both cases have reduced accessibil-
ity for thrombin to the E region suggesting their thrombin binding
properties and fibrinopeptide release may also be altered. Therefore,
the major aim of the present study was to estimate fibrinopeptides
release from fibrinogen and growing fibrin layers at different surface
densities and modes.
We found that the side-on adsorbed fibrinogen released FPB with no
lag phase, and the final concentration of both fibrinopeptides (A, B)
was the same. The initial rate of FpB and FpA release from fibrino-
gen adsorbed at high concentration of Fbg was approximately the
same, however, the final amount of relased FpB was substantially
higher as compared with the amount of FpA. Fibrinopeptide B is
known as a potent chemoattractant, therefore its preferential release
may indicate the physiological meaning in the attraction of cells to
the site of injury.
This work was supported by Grants NS10633-3/2009 and MZ
02373601 from the Ministry of Health, Czech Republic, by Grant
KAN200670701 from the Academy of Sciences, Czech Republic.
O10B-4New evidence for fibrinogen-boundalpha2-antiplasmin in bloodMosesson M, Holyst T and Hernandez IBlood Center of Wisconsin, Milwaukee, WI, USA
Alpha2-plasmin inhibitor (a2AP) occurs mainly as a single-chain pro-
tein in blood, although existing evidence indicates that a2AP is also
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
ORAL PAPERS 29____________________________________________________________________________________

covalently linked to plasma fibrinogen. First, Mosesson and Finlay-
son identified a plasmin inhibitory activity in purified fibrinogen (JCI
42:747,1963). Years later a2AP was shown by immunoelectrophoresis
to be present in purified fibrinogen (BC&F 11:293,2000). More
recently, we developed an ELISA for estimating fibrinogen-bound
a2AP (JTH 6:1565,2008), but the technique was not applicable to
plasma. Thus, to develop evidence for fibrinogen-bound a2AP in
plasma, we prepared Western Blots using near-infrared fluorescent
dye-labeled secondary antibodies (LI-COR Biosciences) to identify
primary antibody-labeled antigens. We labeled PVDF-membrane
bound plasma a2AP or fibrinogen with goat anti-a2AP or rabbit
anti-human achain, respectively. Then we reacted (i) with anti-goat
IgG tagged with green fluorescent dye (IRdye800) or, (ii) with anti-
rabbit IgG tagged with red fluorescent dye (IRdye700). Non-reduced
plasma showed four IRdye800-labeled a2AP-reactive bands: (i) in the
cathodal region of the IRdye700-stained 340 kD fibrinogen band; (ii)
at ~120–125 kD co-migrating with an IRdye700-stained band, proba-
bly a fibrinogen a chain/a2AP heterodimer; (iii) one corresponding to
‘free’ a2AP (~55–60 kD); (iv) a band at ~25 kD of unknown origin.
The IRdye800/IRdye700-stained fibrinogen band was absent from
serum, but the other IRdye800-stained bands remained.
The IRdye800-fibrinogen band was absent from disulfide-bridge
reduced plasma samples, but the other IRdye800 bands remained: (i)
a less intense 120–125 kD a2AP-stained band, co-staining with IR-
dye700; (ii) an a2AP band overlapping red IRdye700-stained a chain
bands; (iii) the 25 kD band. These observations show that (i) a2AP is
covalently linked to the fibrinogen in plasma, (ii) a heterodimeric
a2AP/Aa polypeptide chain exists in plasma. The role that plasma
fibrinogen-bound a2AP plays in regulating the fibrinolytic process
should be investigated.
O10B-5Early factor XIII activation and delayed fibrinolysis inindividuals with Factor V Leiden; a novel mechanismcontributing to increased thrombosis riskBagoly Z, Koncz Z, Haramura G, Mezei ZA and Muszbek LUniversity of Debrecen, Medical and Health Science Center,
Debrecen, Hungary
Background: Factor V Leiden mutation (FVLeiden) increases the risk
of venous thromboembolism by enhancing thrombin formation. It
has been also shown that FVLeiden inhibits fibrinolysis, however,
underlying mechanisms have not been fully elucidated. We investi-
gated the effect of FVLeiden on factor XIII (FXIII) activation, on
the cross-linking of fibrin and a2 plasmin inhibitor (a2PI) and studied
the effect of cross-linking on the rate of clot-lysis.
Methods: Clotting was initiated in plasma samples of fifteen healthy
individuals with known FVLeiden genotypes and wild type for FXIII
A subunit (FXIII-A) Val34Leu polymorphism by recombinant
human tissue factor and phospholipids with/without recombinant
human thrombomodulin (rhTM). Clots were recovered and analyzed
by SDS-PAGE and Western blotting for FXIII-A and a2PI. The
extent of FXIII activation, the cross-linking of fibrin c-chains and the
incorporation of a2PI into the clot were evaluated by quantitative
densitometry. In-vitro clot-lysis experiments with/without rhTM were
also performed.
Results: The presence of rhTM significantly slowed down the activa-
tion of FXIII in the plasma of wild type individuals as compared to
FVLeiden carriers. Time required for half maximal FXIII activation
was approximately 1.5-fold prolonged in wild types (mean � SEM:
629 � 75.3 s) in the presence of rhTM as compared to carriers of
FVLeiden (mean � SEM: 437 � 43.6 s). The delay of FXIII activa-
tion caused by rhTM in wild type individuals was more than 4-fold
reduced in heterozygotes and more than 8-fold in homozygotes. The
inefficiency of rhTM in delaying FXIII activation in FVLeiden carri-
ers resulted in earlier cross-linking of fibrin c-chain and a2PI to
fibrin; the rate of clot lysis in the presence of rhTM was slowed down
in carriers of FVLeiden.
Conclusion: Earlier FXIII activation and, as a consequence, earlier
cross-linking reactions resulting in earlier inhibition of fibrinolysis
might represent a novel mechanism contributing to the increased
thrombosis risk in FVLeiden carriers.
O10B-6Global health risk associated with the use ofrecombinant streptokinase as a biosimilar forthrombolytic therapyThelwell CNIBSC, Potters Bar, UK
Worldwide, streptokinase (SK) remains the most used thrombolytic
agent for the treatment of myocardial infarction (MI). Recombinant
SK expressed in E. coli is increasingly used in developing countries as
a biosimilar of native SK, but potency assignments against the WHO
International Standard (IS) are highly variable with potentially dan-
gerous consequences. A proportion of recombinant SK appears to be
incompletely processed, retaining the N-terminal Met engineered for
E. coli expression. The N-terminal residue of secreted mature native
SK (Ile) is known to be critical in the ‘molecular sexuality’ mecha-
nism of action of SK. Other sequence variations have been reported
including products that appear to be derived from different strepto-
coccus groups. Commercial SK is derived from the H46A isolate of
S. equisimilis (Group C); strains of S. pyogenes (Group A) are
reported to have differing plasminogen activation characteristics. We
have cloned and expressed commercial SK in E. coli (rSK), con-
structed a novel variant with an N-terminal Met (rSK-Met), and
expressed rSK from the M1 strain of S. pyogenes (rSK-M1GAS).
SKs are expressed as N-terminal fusions with SUMOstar (Life Sen-
sors). Crucially SUMOstar1 protease cleaves the fusion tag without
leaving behind unwanted residues, providing complete control over
the SK N-terminus. The potency of each recombinant SK was deter-
mined relative to the WHO IS using a chromogenic solution assay,
and in a fibrin-based assay. In solution, relative to the IS, rSK and
rSK-Met potencies are equivalent, however in the presence of fibrin
rSK-Met loses ~80% of its potency compared to ~30% loss for rSK.
Conversely rSK-M1GAS has <10% of rSK activity in solution,
which increases ~3-fold in fibrin. This apparent difference in activity
and fibrin selectivity highlights dangers in the unregulated clinical use
of biosimilars, and has serious health implications. Improved under-
standing of the detailed mechanism of SK-fibrin specificity will help
improve global thrombolytic therapy.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
30 ORAL PAPERS____________________________________________________________________________________

Plenary Lectures (3)
O11-1ISFP Prize Lecture 2010. From PAI-1 to PDGF in thebrain, a series of fortunate eventsLawrence DAUniversity of Michigan, Ann Arbor, MI, USA
Fibrinolysis has been studied for well over 100 years, and the enzy-
matic components of the plasminogen activator (PA) system have
been known since the 1940’s. However, it was only in the 1990’s that
it began to be appreciated that plasminogen activators might be act-
ing on substrates other than plasminogen, and that their regulation
of physiologic systems may occur through pathways other than fibri-
nolysis. Our work has focused on understanding the non-traditional
roles of plasminogen activators and their inhibitors in normal and
pathologic physiology. Studies have included characterization of the
inhibitory mechanism of Serpins and demonstration of how this
mechanism provides conformational control of both protease and
non-protease ligand interactions, which in-turn regulate complex cel-
lular and physiologic functions. Studies have also investigated plas-
minogen independent roles of PAs and their inhibitors in the central
nervous system (CNS). This work has demonstrated that tissue-type
PA (tPA) can directly regulate the blood brain barrier (BBB) through
interactions with the neurovascular unit (NVU). In vivo results indi-
cate that this occurs through tPA-mediated activation of latent plate-
let-derived growth factor CC (PDGF-CC). Specific proteolysis of
PDGF-CC by tPA generates active PDGF-CC capable of triggering
PDGF receptor alpha (PDGFRa) signaling in perivascular astrocytes
within the NVU, which in-turn controls BBB permeability. The
regulation of BBB integrity after stroke plays a critical role in stroke
progression and in hemorrhagic transformation. Understanding this
pathway may hold the key to developing better treatments for stroke
and potentially other CNS disorders where BBB integrity is
disrupted.
O11-2Clinical value of D-dimer testingPalareti GUniversity Hospital of Bologna, Bologna, Italy
Venous thromboembolism (VTE) requires prolonged treatment to
prevent recurrences. However, the optimal duration of anticoagula-
tion is still controversial. The more recent guidelines of the American
College of Chest Physicians recommend that patients with unpro-
voked VTE should receive at least 3 months of anticoagulation and
then should all be evaluated for the risk-benefit ratio of long-term
therapy. Our line of clinical research is aiming to find criteria to dis-
tinguish subjects at high or low risk of recurrence, to avoid an indefi-
nite anticoagulation in the latter. Prospective studies involving
patients with VTE have consistently shown that the D-dimer (Dd)
levels after anticoagulation have a high predictive value -positive or
negative – for VTE recurrence. These findings suggested a possible
role of Dd assay in regulating the duration of anticoagulation in
VTE patients. The PROLONG trial showed that patients with abnor-
mal Dd 1 month after VKA withdrawal for unprovoked VTE who
were randomized to not resume anticoagulation had a high rate of
recurrences (15.0%), while those with normal Dd had a lower rate of
recurrences (6.2%). It was however unknown whether Dd normal
1 month after VKA withdrawal may change subsequently and
whether this may be associated with an increased risk of recurrence.
The prospective multicenter PROLONG II study was then performed
to assess Dd time course in these patients and its relation with late
recurrences. Patients with normal Dd 1 month after stopping antico-
agulation repeated Dd testing every 2 months for 1 year. Patients in
whom Dd became abnormal at the third month and remained abnor-
mal afterward had a higher risk of recurrence (27% p-y) than
patients in whom Dd remained always normal during followup
(2.9% p-y; adjusted hazard ratio: 7.9; P < 0.002). Repeated D-d test-
ing after anticoagulation suspension for a first episode of unprovoked
VTE could help tailor the duration of treatment.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
ORAL PAPERS 31____________________________________________________________________________________

Thrombin-activatable Fibrinolysis Inhibitor
O12A-1Carboxypeptidase U (TAFIa): a new drug target forfibrinolytic therapy?Hendriks DFUniversity of Antwerp, Antwerp, Belgium
Procarboxypeptidase U (TAFI) is a plasma procarboxypeptidase that
upon activation by thrombin or thrombin-thrombomodulin turns
into a potent antifibrinolytic enzyme once its activity surpasses a cer-
tain threshold value. Its prominent bridging function between coagu-
lation and fibrinolysis raised the interest of several research groups
and pharmaceutical industry to develop carboxypeptidase U inhibi-
tors as profibrinolytic agents. Several studies have been performed
with small synthetic and naturally occurring CPU inhibitors in differ-
ent animal models of thrombosis, and many of these studies show
beneficial effects leading to an improvement of endogenous fibrinoly-
sis. Moreover, treatment with an oral CPU inhibitor has also been
used in a proof-of-principle clinical study in patients with pulmonary
embolism, indicating an improved rate of resolution of pulmonary
emboli and increased endogenous fibrinolysis.
Another approach is the use of CPU inhibitors combined with t-PA
thereby increasing the efficiency of pharmacological thrombolysis
allowing lower dosing of t-PA and subsequently fewer bleeding com-
plications.
In this presentation we will focus on the benefits/risks of targeting
carboxypeptidase U for the treatment of thrombotic disorders. We
will also discuss the advantages and pittfals of measuring proCPU
and active CPU – not only as a risk factor for thrombotic disease,
but also as a possible biomarker for therapy – in patient plasma sam-
ples both with published assays and with several commercially avail-
able immuno- and activity based assays.
O12A-2The role of activation peptide residues Lys42, Lys43,and Lys44 of TAFI in its activation by thethrombin-thrombomodulin complexWu C1, Kim PY2, Foley JH1, Gils A3, Declerck P3 andNesheim ME1
1Queen’s University, Kingston; 2David Braley Cardiac, Vascular
& Stroke Research Institute, Hamilton, Canada; 3Katholieke
Universiteit Leuven, Leuven, Belgium
Thrombin-activable Fibrinolysis Inhibitor (TAFI) is activated to TA-
FIa by thrombin-thrombomodulin complex with a 1250-fold higher
catalytic efficiency than thrombin alone. TAFIa is a potent antifibrin-
olytic enzyme, which significantly prolongs clot lysis time in vitro.
TAFI has three exclusive consecutive lysine residues at positions 42,
43, and 44, in its activation peptide that are not found in rattus,
bovine or human tissue procarboxypeptidases A and B. We previ-
ously reported an 8-fold decrease in catalytic efficiency for TAFI acti-
vation when the three lysine residues were all mutated to alanine
(K42/43/44A).
We constructed and expressed combinations of mutations of the three
lysine residues in order to identify which one (s) is key for TAFI acti-
vation. We activated TAFI wild-type and mutants with thrombin for
10 min in the presence or absence of TM and then added the syn-
thetic TAFIa substrate AAFR to quantify levels of TAFIa formed.
The activation rates were used to determine kinetic parameters of
TAFI activation. We also tested the antifibrinolytic potential of each
mutant activated in situ using an in vitro plasma clot lysis assay. The
time to 50% clot lysis was determined as the midpoint between maxi-
mum turbidity of a clot and the minimum turbidity when a clot was
completely lysed.
kcat values (1/s) ranged from 1.09 � 0.25 (WT) to 8.53 � 4.58 (K43/
44A). Km values (lM) ranged from 0.58 � 0.05 (WT) to
19.87 � 14.08 (K43/44A). Compared to wild-type, the catalytic effi-
ciencies for TAFI activation decreased by 2.3-fold (K43A) to 4.1-fold
(K43/44A). The TAFI concentration required to achieve the half-
maximal effect on attenuation of clot lysis increased from 2.2-fold
(K43A) to 14.8-fold (K42/43/44A).
Our data show that each of the three lysine residues contributes to the
efficiency of activation of TAFI. The increases in kcat suggest that
product (TAFIa) release may be rate limiting in TAFI activation.
O12A-3Identification and characterization of monoclonalantibodies that impair the activation of human TAFIthrough different mechanismsMishra N, Vercauteren EB, Develter J, Bammens R, Declerck PJand Gils AKatholieke Universiteit Leuven, Leuven, Belgium
Introduction: Thrombin activatable fibrinolysis inhibitor (TAFI)
forms a molecular link between coagulation and fibrinolysis and
therefore it is a promising target to develop profibrinolytic drugs.
Objective: To characterize functional properties of three monoclonal
antibodies (MA) raised against a stable TAFI variant (TAFI-AI-
CIYQ; Ceresa et al. JTH, 2007; 5:418–420) with the focus on their
inhibitory properties and mode of action and to elucidate their
respective epitopes.
Methods and Results: Out of a panel of MA raised against a stable
TAFI variant, MA-TCK11A9, MA-TCK22G2 and MA-TCK27A4
revealed high affinity towards human TAFI-TI-wt, but no affinity
towards either mouse or rat TAFI-wt. Even at a 16-fold molar excess
of MA over TAFI, none of these MA was able to reduce TAFIa
activity (Table 1). However, using an 8-fold molar excess of MA over
TAFI, MA-TCK11A9 was able to inhibit plasmin-mediated activa-
tion, MA-TCK22G2 inhibited plasmin- and thrombin-mediated
TAFI activation and MA-TCK27A4 inhibited TAFI activation by
plasmin, thrombin and thrombin/thrombomodulin (Table 1). Using
an 8-fold molar excess of MA over TAFI, all three MA were able to
reduce clot lysis time significantly (Table 1). Phe113 was identified as
the major residue interacting with MA-TCK27A4. Using a sandwich-
type ELISA, we could deduce that this epitope is distinct from the
epitopes of MA-TCK11A9 and MA-TCK22G2, which are currently
being elucidated.
Conclusion: We identified three MA that impair the activation of
TAFI through different mechanisms and demonstrated that MA-
TCK11A9 which exclusively impairs plasmin-mediated TAFI activa-
tion can also significantly reduce clot lysis time in vitro.
Table 1 for O12A-3
MA
% Reduction
on TAFIa
activity
% Reduction on
TAFI activation
% Reduction on
clot-lysis time
By
T/TM
By
plasmin
By
T
Expressed relative
to reduction
by PTCI
TCK11A9 < 2% < 2% 64 � 4.3 < 2% 84 � 27*
TCK22G2 < 2% < 2% 58 � 4.0 41 � 7.0 99 � 15*
TCK27A4 < 2% 98 � 2.0 98 � 4.0 97 � 2.0 128 � 8.0*
Mean � SD, n ‡ 3; *P < 0.05 versus no TAFI inhibitor.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
32 ORAL PAPERS____________________________________________________________________________________

O12A-4The role of TAFI and Factor XI in platelet-mediatedresistance to fibrinolysisColucci M, Carrieri C, Galasso R, Incampo F, Semeraro F,Ammollo CT and Semeraro NUniversity of Bari, Bari, Italy
While it is well documented that platelets make thrombi resistant to
fibrinolysis through clot retraction and PAI-1 release, little is known
about the involvement of TAFI in platelet-mediated resistance to
fibrinolysis. We investigated the contribution of TAFI to the antifi-
brinolytic effect of platelets in whole blood by thromboelastography.
Platelet-poor (PP-WB, < 40 · 103/lL) and platelet-rich (PR-WB,
> 400 · 103/lL) blood samples were obtained from normal blood
(N-WB, 150–220 · 103/lL). Clot lysis time was measured by throm-
boelastography (Haemoscope), using recalcified human blood supple-
mented with t-PA (100 ng/mL) and tissue factor (1/1000 diluted
Recombiplastin).
t-PA-induced lysis time increased proportionally to platelet concen-
tration (from 21.5 � 8.9 to 60.1 � 18.4 min, in PP-WB and PR-WB,
respectively). Neutralization of TAFIa activity (by PTCI) or inhibi-
tion of thrombin-mediated TAFI activation (by a specific monoclonal
antibody) shortened lysis time by 52.3% in PR-WB and by 6.3% in
PP-WB, suggesting that the contribution of TAFI was substantial
only in the presence of platelets. Qualitatively similar results were
obtained when clot retraction was prevented by cytochalasin D or
when PAI-1 was inhibited by a neutralizing antibody. Assay of pro-
thrombin F1 + 2 and TAFIa generation during clot lysis confirmed
that platelets enhanced both thrombin generation and TAFI activa-
tion. Addition of a neutralizing anti-FXI antibody had little effect on
clot formation but shortened the lysis time by 38% in PR-WB and
by < 5% in PP-WB. A significant shortening of lysis time (27%)
was also observed when N-WB collected on CTI (corn trypsin inhibi-
tor, an inhibitor of FXIIa) was supplemented with the anti-FXI, but
not with an anti-FXII antibody. Our data indicate that TAFI activa-
tion is one major mechanism whereby platelets make clots resistant
to fibrinolysis and suggest that FXII-independent activation of FXI
plays an important role in platelet-mediated enhancement of throm-
bin and TAFIa generation.
O12A-5Internalization of thrombin-activatable fibrinolysisinhibitor in keratinocytes by receptor-mediatedendocytosisVerkleij CJN, Reits EAJ, Plug T, Marx PF and Meijers JCMAcademic Medical Center, University of Amsterdam,
Amsterdam, The Netherlands
Introduction: Mice that are deficient for thrombin-activatable fibrino-
lysis inhibitor (TAFI) have delayed wound healing due to impaired
keratinocyte migration. We hypothesized that TAFI may affect
wound healing via direct interactions with keratinocytes. The aim of
this study was to elucidate interactions between TAFI and keratino-
cytes by studying endogenous TAFI in, and internalization of TAFI
by these cells.
Methods: The presence of TAFI in the skin was studied by immuno-
histochemical staining of skin tissue. Direct interactions of TAFI
with keratinocytes were determined in HaCaT cells, a keratinocyte
cell-line. Endogenously generated TAFI was studied at protein level,
whereas TAFI internalization was studied using fluorescently labeled
TAFI.
Results: Immunohistochemical staining for TAFI indicated interac-
tions of TAFI with keratinocytes, while endogenous TAFI was
detected in keratinocytes on protein level, which was dependent on
the phase of the cell cycle. Live-cell imaging showed that keratino-
cytes internalize TAFI via receptor-mediated endocytosis.
Conclusions: This study shows that TAFI can bind to and becomes
internalized in keratinocytes. The enhanced endogenous TAFI pro-
tein levels in mitotic cells suggest that TAFI is involved keratinocyte
proliferation.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
ORAL PAPERS 33____________________________________________________________________________________

Proteases in the Brain
O12B-1Antibodies based immunotherapy for strokeVivien D, Ali C and Macrez RINSERM, Caen, France
Tissue-type plasminogen activator (tPA, endogenous and exogenous)
has two faces in acute ischemic stroke: beneficial fibrinolysis in the
vascular bed, but damaging effects on the neurovascular unit and the
brain parenchyma. To improve this profile, we used our knowledge
of the underlying molecular (patho)physiology to develop a novel
treatment strategy for stroke, relying on antibodies targeting the pro-
neurotoxic effects of tPA. Based on a dedicated model of murine
thrombo-embolic stroke, we demonstrate the efficiency of immuno-
therapy in a complete pre-clinical screen: after a single administration
(alone or with late thrombolysis), antibodies dramatically reduce
ischemic brain injuries, improve long-term neurological outcome and,
in parallel, attenuate critical ischemic events including blood-brain
barrier leakage and activation of MMP-3, MMP-9, and the PDGF-
CC pathway. Thus, the prospect of this immunotherapy is an exten-
sion of the range of treatable patients, whether used as a monothera-
py or, in combinations, to extend the therapeutic window for
thrombolysis.
O12B-2Role of tPA in the rewarding effect of abused drugsNagai TNagoya University Graducate School of Medicine, Nagoya,
Japan
Activation of the mesocorticolimbic dopamine system, which origi-
nates in the midbrain ventral tegmental area and projects to the
nucleus accumbens (NAc) has been implicated in the positive rein-
forcing (rewarding) effects of nicotine and other drugs of abuse.
Recently, it has been proposed that activity-dependent synaptic plas-
ticity and remodeling of the mesolimbic dopaminergic system play a
crucial role in the development of drug dependence. Tissue plasmino-
gen activator (tPA) is a serine protease that catalyzes the conversion
of plasminogen to plasmin. In our previous study, it has been demon-
strated that the tPA-plasmin system participates in the rewarding
effect of opiate and psychostimulant. Here we show that the tPA-
plasmin system regulates nicotine-induced reward and dopamine
release. In vivo microdialysis revealed that microinjection of either
tPA or plasmin into the NAc significantly potentiated whereas plas-
minogen activator inhibitor-1 reduced the nicotine-induced dopamine
release in the NAc in a dose-dependent manner. Nicotine-induced
dopamine release was markedly diminished in tPA-deficient (tPA-/-)
mice, and the defect of dopamine release in tPA-/- mice was restored
by microinjection of either exogenous tPA or plasmin into the NAc.
Nicotine increased tPA protein levels and promoted the release of
tPA into the extracellular space in the NAc. Activation of postsynap-
tic dopamine D1 receptors in the NAc leads to an increase in extra-
cellular tPA activity via PKA signaling. Immunohistochemistry
revealed that protease activated receptor-1 (PAR1)-immunoreactivity
was localized to the nerve terminals positive for tyrosine hydroxylase
in the NAc. Furthermore, we demonstrated that nicotine-induced
conditioned place preference and dopamine release were diminished
in PAR1-deficient (PAR1-/-) mice. Our findings suggest that the tPA-
plasmin-PAR1 system plays a crucial role in the rewarding effects of
nicotine.
O12B-3MMP-10: a new fibrinolytic agent in ischemic stroke?Paramo JA, Orbe JO and Rodriguez JACIMA (University of Navarra), Pamplona (Navarra), Spain
The fibrinolytic and metalloprotease (MMP) systems act in concert to
degrade extracellular matrix proteins and also fibrin, a main structural
component of most thrombi. We have investigated the pathophysio-
logical relevance of vascular MMP-10 (stromelysin-2) expression and
our recent results lead us to postulate a new role for MMP-10 in fibri-
nolysis. After testing different pro-atherosclerotic/proinflammatory
molecules, we found that thrombin strongly induced endothelial
MMP-10 expression in vitro and in vivo. This led us to assess the
effects of MMP-10 on thrombosis and fibrinolysis, and we observed
that MMP-10 significantly enhanced t-PA-induced fibrinolysis in vitro,
either in turbidimetric-based plasma tests, on fibrin plates, and in
whole blood by thromboelastography, while MMP-10 inhibition pre-
vented t-PA-induced fibrinolysis. These results were confirmed in vivo
in the MMP-10 KO mouse. We first assessed thrombus formation
and lysis in the carotid artery after rose bengal infusion and laser
injury, and found that MMP-10 KO exhibited faster thrombus devel-
opment and delayed fibrinolysis compared with wild type mice, sug-
gesting an important role of MMP-10 in thrombus formation and
lysis in vivo. In a murine model of stroke by thrombin microinjection
in the middle cerebral artery, spontaneous reperfusion was severely
impaired in MMP-10 KO animals. We also used this model of stroke
to show in wild type mice that MMP-10 administration significantly
reduced brain lesion volume as compared to controls (P < 0.01), with
no increase in bleeding. Finally, we found that MMP-10 exerts its
profibrinolytic effect at least in part by cleaving thrombin activatable
fibrinolysis inhibitor (TAFI), thus preventing its activation.
We propose that MMP-10 administration, alone or in combination
with t-PA, can become a new profibrinolytic strategy in arterial
thrombosis, particularly useful in the treatment of ischemic stroke.
O12B-4Roles of urokinase receptor (uPAR) on ischemic strokeNagai N1, Okada K1, Kawao N1, Ishida C1, Ueshima S2 andMatsuo O1
1Kinki Univ School of Med, Osaka; 2Kinki Univ School of
Agriculture, Nara, Japan
Urokinase-type plasminogen activator receptor (uPAR) is a key com-
ponent of the plasminogen activation system at the cell surface. Recent
studies showed that uPAR is expressed in the ischemic damaged brain,
suggesting its involvement in brain damage. To evaluate the roles of
uPAR, we evaluated the role of uPAR in ischemic brain damage
induced by permanent middle cerebral artery (MCA) occlusion in mice
with genetic deficiency of uPAR (uPAR-/-) or of uPA (uPA-/-). Brain
damage on day 3 was smaller in uPAR-/- mice (4.5 � 1.0 mm3) than
in littermate wild-type mice (uPAR+/+) (9.1 � 1.8 mm3, P < 0.05),
whereas it was comparable in uPA-/- (8.0 � 4.1 mm3) and uPA+/+
(6.9 � 2.6 mm3) mice. uPAR expression was upregulated in the ipsilat-
eral cerebral cortex of control mice within 12 h, and remained elevated
for up to 3 days. On day 1 or 2 after MCA occlusion, uPAR expres-
sion was selectively localized in vessels at the border of the damaged
area. It was also found that uPAR-/- mice showed less blood-brain bar-
rier disruption than uPAR+/+ on day 1. In bEnd.3, an endothelial cell
line derived from mice brain, uPAR expression was upregulated at
24 h after 2 h of oxygen-glucose deprivation mimicking ischemia or
after 24 h serum deprivation, indicating that both hypoxic stress and
starvation of trophic factors by ischemia induced uPAR on endothelial
cells. These findings suggest that uPAR expressed by endothelial cells
augments of the ischemic brain damage via failure of endothelial cell
function by uPA-independent mechanism.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
34 ORAL PAPERS____________________________________________________________________________________

Clinical and Basic Aspects of Thrombolysis
O13A-1Clinical thrombolysisVerheugt FWAOnze Lieve Vrouwe Gasthuis, Amsterdam, The Netherlands
Reperfusion therapy for ST-elevation myocardial infarction (STEMI)
aims at early and complete recanalization of the infarct-related artery
in order to salvage myocardium and improve both early and late clin-
ical outcomes. The benefit rises exponentially the earlier therapy is
initiated. Both coronary fibrinolysis (formerly called coronary throm-
bolysis) and primary coronary angioplasty can achieve full reperfu-
sion. Angioplasty is more successful, but has severe logistic
constraints, whereas fibrinolysis can be administered everywhere.
Time to treatment can be shortened by prehospital diagnosis and
treatment. The optimal site for STEMI diagnosis is the patient’s home
or place where the infarction occurs. Prehospital ECG diagnosis has
shown to increase the number of patients treated earlier in hospital by
either fibrinolysis or primary coronary angioplasty (1). Furthermore,
prehospital initiation of fibrinolysis shows a gain in time to treatment
of about one hour and results in 15% relative risk reduction of early
mortality (2). Compared to primary angioplasty prehospital fibrino-
lytic therapy may be not inferior to primary angioplasty because of
this gain in time to treatment (3). Finally, prehospital diagnosis fol-
lowed by direct transfer to a hospital with PCI facilities rather than
to a hospital without reduces time-to-treatment with at least 1 h in
Denmark. Four Administration of fibrinolytic therapy in the emer-
gency room is superior to starting fibrinolysis in the Coronary care
Unit (5). In patients transferred for primary angioplasty direct trans-
fer to the catheterization laboratory saves time to treatment in com-
parison to admission to the emergency department or Coronary Care
Unit (6). The ideal strategy is prehospital triage with direct transfer to
the catheterization laboratory (7, 8). Thus, ambulance diagnosis and
triage as well as direct transfer to a catheterization laboratory are the
major leaps forward in the reduction in time-to-treatment in STEMI.
The several advantages and disadvantages of fibrinolysis and primary
coronary intervention are summarized in the table.
References
1 Curtis JP, Portnay EL, McNamara EL, et al. The pre-hospital elec-
trocardiogram and time to reperfusion in patients with acute myo-
cardial infarction, 2000–2002: findings from the National Registry
of Myocardial Infarction-4. J Am Coll Cardiol. 2006; 17:1544–1552.
2 Morrison LJ, Verbeek PR, McDonald AC, Sawadsky BV, Cook
DJ. Mortality and prehospital thrombolysis for acute myocardial
infarction. JAMA. 2000; 283:2686–2692.
3 Steg PG, Bonnefoy E, Chabaud S, et al. Impact of time to treat-
ment on mortality after prehospital fibrinolysis or primary angio-
plasty: data from the CAPTIM randomized clinical trial.
Circulation 2003; 103:2851–2856.
4 Terkelsen CJ, Lassen JF, Norgaard BL, et al. Reduction of treat-
ment delay in patients with ST-elevation myocardial infarction:
impact of pre-hospital diagnosis and direct referral to primary per-
cutaneous coronary intervention. Eur Heart J. 2005; 26:770–777.
5 Verheugt FWA, Funke Kupper AJ, Sterkman LGW, Meijer A,
Peels CH, Roos JP. Emergency room infusion of intravenous strep-
tokinase in acute myocardial infarction: feasibility, safety end he-
modynamic consequences. Am Heart J. 1989; 117:1018–1022.
6 Bradley EH, Herrin J, Wang Y, et al. Strategies for reducing the
door-to-balloon time in acute myocardial infarction. N Engl J
Med. 2006; 355:2308–2320.
7 Vermeulen RP, Jaarsma T, Hanenburg FGA, Nannenberg, Jessu-
run GAJ, Zijlstra F. Prehospital diagnosis in STEMI patients trea-
ted by primary PCI: the key to rapid reperfusion. Neth Heart J.
2008; 16:5–9.
8 Liem S, Dieker H, Keuper W, Clappers N, Brouwer MA, Aeng-
evaeren WRM, Verheugt FWA. The impact of ambulance-based
triage for primary angioplasty.on treatment intervals and clinical
outcome. J Am Coll Cardiol Int. 2010 in press.
O13A-2Optimizing thrombolytic efficacy and safety bypreventing non-specific plasminogen activationGurewich V and Pannell RBeth Israel Deaconess Medical Center, Cambridge, MA, USA
The shortcomings of available thrombolytics include their limited effi-
cacy and bleeding risk. Consequently, thrombolysis is being replaced
by angioplasty (AMI) or used with reluctance (stroke). The maximum
efficacy of all plasminogen activators is a function of the rate of
fibrin degradation by plasmin. This rate, however, is unattainable
clinically because of dose-dependent hemorrhagic complications due
to non-specific plasminogen activation or direct lysis of hemostatic
fibrin. At safer fibrin specific doses, the clot lysis rate is only ~50%
of the maximum with either tPA or prouPA. These activators have
distinctly different properties. TPA is promoted by intact fibrin (D-
domain), which corresponds to hemostatic fibrin, and thereby can
induce bleeding directly by fibrinolysis. ProuPA is promoted by the
fibrin E-domain, which is absent in hemostatic fibrin. Unfortunately,
at therapeutic concentrations, prouPA proved vulnerable to activa-
tion by plasmin with loss of fibrin-specificity (a reaction amplified by
positive feedback) leading to a bleeding diathesis, which deterred
EMEA from granting approval. Mutant prouPA, M5, is more stable
in plasma due both to a lower intrinsic activity and an unusual inhi-
bition of two-chain M5 by plasma C1-inhibitor (C1I), a negligible
inhibitor of tPA or tcuPA. When plasma was enriched with C1I in vi-
tro, stability of M5 was further enhanced, enabling the maximum rate
of lysis with fibrin-specificity. C1I selectively inhibited only non-spe-
cific plasminogen activation. Other serpins (PAI-1, AT, a2AP) inhib-
ited both fibrin-specific and non-specific plasminogen activation. This
M5/C1I phenomenon was tested in vivo in dogs with thromboembo-
lism given high-dose M5 � C1I. Lysis and bleeding from hemostatic
injury sites were quantitated. Equivalent, rapid lysis (100% in
30 min) occurred in both groups, but extensive bleeding was inhibited
only with C1I supplementation.
C1I is already an approved drug. Used as adjunctive therapy with
M5, C1I can make therapeutic thrombolysis optimally effective and
safe for the first time.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
ORAL PAPERS 35____________________________________________________________________________________

O13A-3Exploring the sensitivity of fibrinolysis rates toinhibition of tissue plasminogen activator (tPA)-fibrinbinding and plasminogen-fibrin bindingSilva M, Thelwell C and Longstaff CNIBSC-HPA, Potters Bar, UK
As part of our efforts to model the kinetics of plasminogen activation
and fibrinolysis we have investigated plasminogen- fibrin-tPA ternary
complex formation and the mechanism of stimulation of fibrinolysis
by C-terminal lysines. Generation of C-terminal lysines by plasmin in
fibrin upregulates binding of plasminogen and tPA (via Kringle
domains) and stimulates further generation of plasmin. This positive
feedback can be damped by carboxypeptidases (e.g. CPB and TAFI)
and binding can be inhibited by lysine analogues such as tranexamic
acid. To dissect out the relative importance of C-terminal lysine bind-
ing for tPA and plasminogen we have compared tPA (F-G-K1-K2-P)
and a domain-switched variant K1K1tPA (F-G-K1-K1-P) that lacks
the K2 lysine binding domain but retains normal tPA structure. Pre-
cise measurements using high throughput methods of plasminogen
activation in fibrin and of fibrinolysis show that tranexamic acid
affects rates with both variant enzymes across a range of conditions.
In fibrin, 50% inhibition of plasminogen activation and fibrinolysis
was achieved by tranexamic acid at 0.3 or 0.075 mM, for lys- and
glu-plasminogen, respectively. Fibrinolysis rates with tPA were only
up to 10% more affected than K1K1tPA, indicating tranexamic acid
acts on plasminogen binding, rather than tPA. Clots incorporating
dose ranges of CPB behaved in a similar way. At 2 U/mL CPB, inhi-
bition of plasminogen activation and fibrinolysis was around 25%
and 70% for lys- and glu-plasminogen, respectively. Assays with tPA
were maximally only 10% more inhibited than K1K1tPA assays, by
CPB, indicating the importance of C-terminal lysine-plasminogen
binding in regulating fibrinolysis. Significant inhibition of fibrinolysis
using an inactive ser-> ala active site tPA variant was not observed
at concentrations up to 200 nM in the clot, a 5000-fold excess over
active tPA. All these results highlight the greater sensitivity of fibri-
nolysis rates to blocking plasminogen (substrate) binding to fibrin,
over tPA binding.
O13A-4A multi-scale mathematical model of fibrinolysis:from fiber cross sections to whole clotsBannish BE, Fogelson AL and Keener JPUniversity of Utah, Salt Lake City, UT, USA
Mathematical models can be very useful for making predictions
about biological processes that are difficult to quantify experimen-
tally. Models give insight to underlying mechanisms and provide
explanations for phenomena seen in experimental results. We study
fibrinolysis using a multi-scale mathematical model intended to
answer the following question: Why do coarse clots composed of
thick fibers lyse more quickly than fine clots composed of thin fibers,
despite the fact that individual thin fibers lyse more quickly than
individual thick fibers? We use stochastic methods to model lytic pro-
cesses on scales ranging from individual fiber cross section to whole
clot. The biochemistry is contained in the fiber cross-section model,
which we use to predict the average time it takes plasmin to cut
through single fibers of varying diameter, the average amount of
plasmin produced by a single tPA molecule, and the spatial and tem-
poral concentration profiles of fibrin-bound plasminogen and plas-
min. This information is used in a fibrin clot model to investigate the
pattern and speed of lysis induced by tPA added to the surrounding
plasma. Concentration profiles of the lytic enzymes are obtained in
different regions of the clot, and the lysis of coarse and fine clots are
contrasted. An advantage of studying fibrinolysis mathematically is
the ability to cheaply and (relatively) easily change the experiment of
interest. We can test hypothesized clinical therapies by adding the
effect of a proposed drug into our system, for example. In the future,
we intend to build upon the model to address questions arising from
current research.
O13A-5Lysis of thrombi formed in the Chandler loop orBadimon chamberMostefai HA1, Baeten KM1, Langrish JP2, Lucking AJ2,Newby DE2 and Booth NA1
1University of Aberdeen, Aberdeen; 2University of Edinburgh,
Edinburgh, UK
Thrombus stability is central to stroke, heart attack and deep venous
thrombosis. Some thrombi are removed by naturally-occurring fibri-
nolytic activity, and we explored the potential of endogenous fibrino-
lysis, caused by tissue-plasminogen activator (tPA) released from the
endothelium. Model thrombi were formed from blood in vitro in
Chandler loops and ex vivo using the Badimon chamber, with FITC
labelled fibrinogen as a tracer for quantitative analysis of lysis. In
addition, tPA was introduced to blood at final concentrations of 0–
50 ng/mL, accurately mimicking stimulated endogenous t-PA release.
Added tPA was successfully incorporated into the forming Chandler
model thrombus over the entire concentration range. Zymography
showed that all tPA and plasminogen activator inhibitor type 1 (PAI-
1) incorporated in the thrombus was free, whereas tPA in serum was
predominantly in complex with inhibitors. When preformed tPA-
PAI-1 complex was added to the blood, this was only recovered in
the serum and not in extracts of model thrombi, showing that it was
not incorporated into the forming thrombus. Addition of increasing
concentrations of tPA resulted in marked increases in thrombus lysis,
as shown by fluorescence release and D-dimer measurements. Similar
data were generated from thrombi formed in the Chandler loop and
those formed in the Badimon chamber at high or low shear rates.
Incorporated tPA was much more efficient than tPA added to bath-
ing fluid, to the extent that some lysis already occurred during forma-
tion, such that the rotation time for formation of Chandler model
thrombi was decreased from 90 min, as published, to 30 min. In con-
clusion, tPA at physiological concentrations was incorporated during
thrombus formation in a free and active form, despite the presence of
PAI-1 and other inhibitors. Once incorporated within the thrombus,
tPA was effective in lysis, confirming the importance of endogenous
tPA localized inside the thrombus.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
36 ORAL PAPERS____________________________________________________________________________________

Tissue Remodeling and Matrix Metalloproteinases
O13B-1Tissue remodeling and matrix metalloproteinasesLijnen HRCenter for Molecular and Vascular Biology, Leuven, Belgium
Matrix metalloproteinases (MMPs) and their tissue inhibitors (TIM-
Ps) play a role in most biological processes requiring tissue remodel-
ing. In general, the net proteolytic activity is determined by a delicate
balance between MMP and TIMP activity. TIMP-1 is a main physio-
logical inhibitor of most MMPs. In murine atherosclerosis models,
TIMP-1 deficiency is associated with reduced plaque area but
enhanced occurrence and severity of aneurysms. MMP activity (e.g.
MMP-3, -9, -12, -13) develops via activation of proMMPs by plasmin
that is generated via plasminogen activation by macrophage derived
urokinase. Extracellular matrix proteolysis is also required for expan-
sion of adipose tissue. We have used a nutritionally induced obesity
model in transgenic mice to study the role of the MMP system. In
this model, stromelysin-1 (MMP-3) or stromelysin-3 (MMP-11) but
not stromelysin-2 (MMP-10) deficiency promoted adipose tissue
development, whereas deficiency of gelatinase A (MMP-2) but not
gelatinase B (MMP-9) impaired it by contributing to adipocyte hypo-
trophy. Deficiency of TIMP-1 induced impaired adipose tissue devel-
opment associated with adipocyte hypotrophy. However, adenoviral
overexpression of TIMP-1 in mice had no significant effect on body
weight or developing adipose tissue mass. Administration to wild-
type mice kept on a high fat diet of broad-spectrum MMP inhibitors
or of relatively gelatinase-specific inhibitors resulted in moderate to
significant reduction of adipose tissue weight. Thus, studies in trans-
genic mouse models as well as pharmacologic studies support a role
of the MMP system in adipogenesis and obesity; the role of specific
members of this family, however, remains to be determined in more
detail.
O13B-2Plasminogen-dependent mobilization of hematopoieticstem cells-induced by G-CSF requires twoindependent pathways, activation of MMP-9 and SDF-1/CXCR-4 regulationHoover-Plow JL and Gong YLerner Research Institute Cleveland Clinic, Cleveland, OH, USA
Ischemic heart diseases including myocardial infarction (MI) are the
leading causes of death in the USA. Use of hematopoietic stem cells
(HSC) to improve recovery of the injured heart after MI is an impor-
tant emerging therapeutic strategy. The plasminogen (Plg) system, an
inflammatory mediator, is critical for tissue repair after injuries. Plg
deficiency (Plg-/-) significantly decreases HSC mobilization from bone
marrow (BM) to the circulation induced by granulocyte colony-stim-
ulating factor (G-CSF). After G-CSF treatment, there was no differ-
ence in proMMP-9 between Plg+/+ and Plg deficient mice, but
actMMP-9 was higher in Plg+/+ mice than Plg-/- mice. Reconstitu-
tion of actMMP-9 activity, but not proMMP-9, rescued HSC mobili-
zation in Plg-deficient mice. Thus, Plg-dependent HSC requires
MMP-9 activation. SDF-1 is a key chemoattractant for HSC mobili-
zation from BM, and G-CSF decreases SDF-1 in BM of Plg+/+
mice creating a gradient of SDF-1 between BM and blood. Our data
show that Plg deficiency abolishes the gradient of SDF-1 and pro-
motes the expression of CXCR-4, a major receptor of SDF-1 on
HSC, and suggests that Plg may regulate stem cell mobilization by
modulating SDF-1/CXCR-4 signal. In MMP-9 deficient mice, SDF-1
was not different compared to MMP-9+/+ after G-CSF treatment
indicating a distinct and novel mechanism by which Plg regulates
HSC mobilization through SDF-1. In addition, our data show that
Plg deficiency inhibits G-CSF-induced neovascularization in the
infarcted area, a key step of cardiac repair. Taken together, these
data suggest that Plg may enhance HSC recruitment by regulating
both MMP-9 activation and BM SDF-1/CXCR-4 function. Those
pathway cascades may also contribute to cardiac repair after MI.
This pathway cascade may also be involved in the cardiac repair after
MI.
O13B-3Activated protein C prevents neuronal apoptosis atexcitotoxicity via inhibition of p53Gorbacheva L1, Savinkova I1, Pinelis V2, Ishiwata S3, Reiser G4
and Strukova S1
1Lomonosov Moscow State University; 2Scientific Centre for
Children‘s Health, Moscow, Russian Federation; 3School of
Science and Engineering, Waseda University, Tokyo, Japan;4Institute for Neurobiochemistry, Otto-von-Guericke University,
Magdeburg, Germany
Brain ischemic stroke led to glutamate (Glu)-induced toxicity which
can initiate the cascade of mitochondrial dysfunctions and induction
of apoptosis. It was shown that one of the key molecular regulators
of neuronal survival and death can be the tumor suppressor protein
p53. Activated protein C (APC) exerts the direct cytoprotective
effects on neurons via EPCR activation of protease activated receptor
1. However, the molecular mechanisms of APC neuroprotective
effects at Glu-toxicity have not been elucidated. We suggested that
APC can suppress the molecular cascade responsible for neuronal
apoptosis at Glu-induced toxicity via inhibition of p53 or blocked the
activation of caspases and NF-kB. This is the focus of the current
investigation.
Studies were performed using primary culture of neurons from cortex
or hippocampus of brain of Wistar rat pups. Cell death was deter-
mined by biochemical (LDH) and morphological methods (Hoe-
chst33342, Ethidium bromide and Syto-3). By immunostaining and
Western blot the nucleus and cytoplasm levels of pro-apoptotic pro-
teins (p53, AIF and caspase-3) and NF-kBp65 were assessed during
Glu-toxicity and incubation with APC.
APC at low concentrations was shown to have the protective effect
on neurons survival at Glu-toxicity. Hippocampal neurons sensitivity
to APC was higher than one to cortical neurons. In hippocampal
neurons APC inhibits Glu-induced caspase-3 activity with maximum
effect 24 h after treatment. APC inhibits AIF translocation into
nucleus. Incubation of neurons with APC blocks the increase of
nuclear level of p53 as well as 4 h and 24 h after exposure cells to
Glu. APC protects neurons from Glu-toxicity due to blockage of
both caspase-dependent and -independent apoptosis. APC reduces of
the nuclear level of NF-jBp65 at Glu-toxicity.
Thus APC can suppress the molecular cascade responsible for
neuronal apoptosis at Glu-induced toxicity via inhibition of p53 or
blockage the activation of caspases and NF-kB. (RFBR grant 08-04-
01123a)
O13B-4Tissue-type plasminogen activator (tPA) andplasmin(ogen) participate in the removal of dead cellsBorg RJ, Samson A, Schlozen A, Plebanski M and Medcalf RLMonash University, Melbourne, Australia
Fibrin is the classic cofactor that promotes tPA-mediated plasmin
formation, which in turn leads to fibrinolysis. We have shown that
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
ORAL PAPERS 37____________________________________________________________________________________

dead cells, regardless of their background lineage, also provide a co-
factor for tPA-mediated plasmin formation (Samson et al. Blood
2009) and we considered the possibility that tPA-mediated plasmin
formation participates in the proteolytic clearance of dead cells. We
show that a brief treatment of dead cells with both tPA and plas-
minogen leads to their proteolytic degradation (n = 4) suggesting
that tPA and plasminogen indeed participate in dead cell break-
down and clearance. Phagocytosis is also a key element of dead cell
clearance. Dendritic cells (DCs) are antigen presenting phagocytes
that link the innate and adaptive immune system. We show that
tPA-mediated plasmin formation induces profound morphological
changes in monocyte-derived DCs (MoDCs), whereby MoDCs
become more adherent and develop long extended appenditures.
These plasmin-induced changes in MoDC adherence and morphol-
ogy were rapid (‡ 3 h; n = 3) and persistent (£ 48 h; n = 3) and
were blocked by aprotinin, indicating a dependency on plasmin for-
mation. No effect was observed when MoDCs were treated with the
closely-related protease thrombin (n = 3). Cell-surface marker stud-
ies showed that plasmin treatment did not induce MoDC matura-
tion (n = 4). These findings align with those of Li and co-workers
(2010) who showed that plasmin induces MoDC chemotaxis. Collec-
tively, plasmin influence dead cell removal via direct proteolysis of
dead cell proteins and may also engage dendritic cells. We are cur-
rently determining whether plasmin promotes DC-induced phagocy-
tosis and conducting experiments to assess the effect of tPA-
mediated plasmin formation in systems where dead cell proteolytic
degradation, phagocytosis, and DC activation/migration occur con-
currently.
O13B-5Plasminogen as a novel therapeutic agent to treattympanic membrane perforationsShen Y1, Guo Y1, Li J1, Wilczynska M1, Hellstrom S2 and Ny T1
1Umea University, Umea; 2Karolinska Universitetssjukhuset,
Stockholm, Sweden
Tympanic membrane (TM) perforations are commonly seen in clini-
cal practice, e.g. after trauma to the ear or during episodes of acute
otitis media. So far there is no effective treatment to TM perforation
except tympanoplasty, a surgical procedure. It has been shown previ-
ously that healing of TM perforation is completely arrested in plas-
minogen-deficient mice. Inflammatory cells were recruited to the
wounded area but there were no signs of tissue debridement. In addi-
tion, removal of fibrin, keratinocyte migration and in-growth of con-
nective tissue were impaired. Here we show that topical application
of purified human plasminogen in plasminogen-deficient mice success-
fully restores the normal TM perforation healing in these mice and
speeds up the healing of a hydrocortisone-induced chronic TM perfo-
ration model in rats. The healing is dependent on the concentration
of the plasminogen solution used as well as the time length of appli-
cation. Also by local injection, purified human plasminogen shows
sufficient healing effect. In conclusion these results indicate that puri-
fied human plasminogen can be locally used as a novel therapeutic
agent to treat TM perforations. Future clinical studies will elucidate
whether local treatment by plasminogen can replace surgical tympa-
noplasty.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
38 ORAL PAPERS____________________________________________________________________________________

Educational Workshop on Technologies
O14A-1An in silico model for haemostasis: computationalmethods and algorithmsBakker B, van den Ham R and van Ooijen HPhillips Research, Eindhoven, The Netherlands
A correct haemostatic balance is essential for human health. A vast
and increasing number of people require support in maintaining this
balance through anti-coagulants like Warfarin on the one hand and
monitoring of their current haemostatic balance on the other. The
current standard tool for such monitoring is the INR (International
Normalized Ratio) test which is based on prothrombin time. This
tool is sensitive for only a small subsection of the full haemostatic
system and is for example unaffected by influences from fibrinolysis,
platelet reactions or the endothelium. Improvement on the accuracy
of the INR, the use of new anti-coagulants and a number of specific
clinical questions require the development of a more comprehensive
test panel which encompasses all relevant aspects of haemostasis.
To identify the components of such a test panel, Philips Research has
started the development of a computer model that describes (within
reason) all the aspects of haemostasis. The finished model will feature
modules on the coagulation cascade, fibrin network formation and
fibrinolysis, endothelial and platelet reactions, blood flow and to
some extent also inflammation. The qualitative part of such a model
is obtained from literature. Examples of such qualitative knowledge
are the many protein-protein reactions that feature in the coagulation
cascade, fibrinolysis and on the platelet and endothelial surface. The
quantitative part, e.g. the rate constants involved in the aforemen-
tioned reactions, is less well known. We have developed a number of
methods to identify important model parameters, set up in vitro
experiments and estimate model parameters based on experimental
observations.
I will describe our approach in building a computer model for hae-
mostasis from literature and in vitro experiments, the estimation of
model parameters and the identification of the most important model
parts. I will show examples of these techniques applied to the coagu-
lation cascade part of the model and demonstrate the results in the
form of an on-line demo.
O14A-2Global fibrinolysis assaysColucci MUniversity of Bari, Bari, Italy
Intravascular fibrinolysis is a complex process and is heavily influ-
enced by thrombin generation which reduces clot lysability directly
(by altering clot architecture) and indirectly (by activating FXIII and
TAFI). It is therefore practically impossible to judge the overall func-
tion of the system from the concentration of single components.
Attempts to develop global assays date back to the 50s. Because
in vitro a plasma or blood clot will not lyse spontaneously due to the
excess of inhibitors, earlier methods either removed the inhibitors
(euglobulin lysis time) or reduced their effect (diluted blood clot lysis
time). Obviously, none of these methods reflected the physiological
condition. A more recent and widely adopted alternative is to chal-
lenge plasma with a fixed concentration of exogenous plasminogen
activator (generally t-PA) prior to clot induction and to measure the
‘lysis time’ by the changes in optical density. The method is quite
simple and is sensitive to the main fibrinolytic components and to
thrombin generation. It can be regarded as an estimate of the fibrino-
lytic ‘potential’, assuming that in vivo, at sites of vessel occlusion,
enough t-PA is released to overcome PAI-1. This method has been
successfully used for basic research and clinical studies. Each labora-
tory, however, uses its own version of the assay so that there are
many variations on the theme. This is a critical point because analyti-
cal conditions have a great impact on the results and may even com-
promise the test’s ability to unmask some fibrinolytic alterations. To
better approximate the in vivo condition, the assay can be performed
on platelet-rich plasma and may include elements of the vessel wall
(e.g. thrombomodulin). Assays in whole blood, in which fibrinolysis
is monitored by thromboelastography or through the release of
D-dimer, have also been proposed. The pros and the cons of each
method will be discussed.
O14A-3Cell culture technology and stem cells in research:emphasis on proteolysisvan Hinsbergh VWM and Koolwijk PVU University Medical Center, Amsterdam, The Netherlands
The use of cultured cells has facilitated previous studies on the regu-
lation of fibrinolysis and proteolysis. Cells provide a versatile tool to
study the effect of many stresses on the gene and activity regulation
of proteases, their inhibitors and their receptors. These stresses
include inflammation, hypoxia, ageing, metabolic stresses, angiogenic
factors and inhibitors, and others. They can be studied in single cells,
but the three-dimensional embedding of the cell has major effects on
their regulation. In addition to the classical assays of mRNAs, pro-
tein antigens and protein activities and regulation parameters such as
transcription factors and micro-RNAs, cultured cells provide a plat-
form for deletion and overexpression of genes and factors. Sophisti-
cated imaging techniques provide new clues about the cellular
localization of specific proteases as well as that of activities of specific
regulators within the cell. The availability of in vivo models enables
to verify the in vitro observations so that misinterpretations based on
vitro artifacts can be avoided. This is discussed on the basis of differ-
ent types of endothelial cells, various types of cells indicated as endo-
thelial progenitors cells, and stem cells that can be obtained in
different ways. The latter provide a versatile system to investigate
differentiation and to monitor the adaptive responses in a variety of
settings.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
ORAL PAPERS 39____________________________________________________________________________________

Neurovascular Dysfunction
O14B-1Neurovascular-derived microparticles: potentialbiomarkers and fibrinolytic messenger in strokeAngles-Cano E1, Doeuvre L2, Plawinski L3, Dejouvencel T2,Nicole O3, Goux D4, Lacroix R5, Dignat-George F5 andBraeckmans K6
1Inserm; 2Inserm U919; 3CNRS UMR6232; 4CMABIO Universite
de Caen, Caen; 5Inserm U608, Marseille, France6University of
Ghent, Ghent, Belgium
Cells of the neurovascular unit and circulating leukocytes express
plasminogen activators and generate plasmin at their membrane.
Membrane microparticles (MPs) released upon stimulation/activation
of these cells may therefore convey plasminogen activators and the
plasmin generated at their surface (Blood 2007, 110: 2432). MPs are
vesicles of 100–1000 nm size released by activated cells under the
influence of a variety of stimuli including proteases. Data presented
here indicate that plasmin formed at the surface of neurons by the
tPA they express may also elicit the release of MPs. The plasmin
formed rapidly induces a calcium influx that could be inhibited by a
selective PAR-1 antagonist. This is an important feature preceding
membrane blebbing and followed by the release of membrane MPs
of about 300 nm in diameter (shown by electron microscopy and
fluorescent single particle tracking). These MPs as those of endothe-
lial and leukocyte origin bear plasminogen activators and have the
potential to generate plasmin de novo when in contact with plasmin-
ogen. The proteolytic activity they convey may participate in fibrino-
lysis, matrix remodeling and cell migration or angiogenesis. Indeed, it
has been recently shown that endothelial- or leukocyte-derived MPs
bearing uPA activate plasminogen bound to fibrin or to platelets
unveiling thereby a new mechanism for plasmin formation: the fibri-
nolytic cross-talk (Blood 2010, 115: 2048).
The in vivo pathophysiological relevance of these phenomena is under
study. Since MPs display molecular signatures from the parent cells it
is possible to identify their origin within the neurovascular complex.
Furthermore, beyond their well-characterized procoagulant activity it
is now possible to characterize their fibrinolytic/proteolytic activity as
well as other biomolecules. MPs are therefore evolving as characteris-
tic biomarkers of affected distinct cell subpopulations and could be
considered a direct message from a specific tissue undergoing activa-
tion or damage, e.g. ischemic stroke.
O14B-2Tissue-type plasminogen activation, the blood brainbarrier and traumatic brain injuryMedcalf RL, Sashindranath M, Sales E and Niego BMonash University, Melbourne, Australia
The human plasminogen activating (PA) system is well known for its
role in the turnover of the extracellular matrix and in the removal of
blood clots. However, over the past 15 years, there has been an
explosion of information linking this enzyme cascade with important
proteolytic and non-proteolytic events within the central nervous sys-
tem. Tissue-type plasminogen activator (t-PA) is arguably the most
relevant member of the PA system in this context. While a positive
role for t-PA has been linked with learning and memory under nor-
mal conditions, a deleterious role for t-PA is now well established in
brain pathology, notably following ischaemic stroke and traumatic
brain injury (TBI). While much effort has been devoted to under-
standing the molecular basis for these effects, a pattern is emerging
to suggest that a major component of these unwanted effects of t-PA
is linked to its effect on the blood brain barrier (BBB). We have
established in vitro models of the BBB to explore the means by which
t-PA modulates permeability across the BBB and if this effect is
unique to t-PA or shared by other plasminogen activators. We have
also established a reliable mouse model of TBI where we have com-
pared the degree of protein extravasation, lesion volume and motor
function post-TBI in mice under- or over-expressing t-PA in neurons.
Results from these in vivo experiments provide unambiguous evidence
that the degree of injury severity post-TBI is positively correlated
with the level of endogenous neuronal t-PA and its downstream
effects on BBB permeability. These results further suggest that thera-
pies directed at blocking the ability of t-PA to modulate the BBB
without compromising its classical fibrinolytic role will be of benefit
in TBI patients as well as patients with ischaemic stroke.
O14B-3Quantitation of net tissue-type plasminogen activatoractivity following CNS stimulation and injury using arapid and reliable amidolytic assaySashindranath M1, Samson AL1, Abdella E1, Lawrence AJ2,Tarlac V1, Downes CE3, Crack PJ3 and Medcalf RL1
1Monash University; 2Howard Florey Institute, Melbourne;3Department of Pharmacology, University of Melbourne,
Melbourne, Australia
Tissue-type plasminogen activator (tPA) is best known as an initiator
of fibrinolysis via its cleavage of plasminogen into active plasmin.
tPA is also widely expressed in the central nervous system where it
mediates numerous physiological and pathological processes. Most
studies to date have only used in situ and gel-based zymography
assays to monitor in vivo changes in neural tPA activity. Here we
describe an amidolytic assay which we have termed the ‘FAStPA’
assay (fibrin-accelerated S2251 hydrolysis by tPA) to quantitate
changes in net tPA proteolytic activity in brain tissues. Using tPA-/-
and wildtype mice we show that this assay can be used selectively to
detect changes in net tPA activity in the brain. The FAStPA assay
offers several advantages over zymography in that it is fully quantita-
tive, rapid and high-throughput, whilst maintaining a high degree of
sensitivity. We used this assay to quantitate alterations in net tPA
activity in various brain structures including the cortex, sub-cortical
structures and cerebella following systemic morphine treatment and
subsequent to a controlled cortical impact model of traumatic brain
injury and middle cerebral artery occlusion (MCAo)-mediated ische-
mic stroke. A role for tPA has been described in each of these
instances, and significant and compartment-specific alterations in net
tPA activity (up to 30%) were observed using the FAStPA assay
(P < 0.05). Finally, we also show that net tPA activity is increased
in both the cortex (P < 0.05) and cerebellum (P = 0.07) of mice
expressing a pathogenic form of Ataxin-1, the mutant protein respon-
sible for spinocerebellar ataxia type-1 (SCA1). This finding corrobo-
rates previous reports linking increased cerebellar tPA activity to
degeneration and dysfunction. In summary, we describe a practical
and accurate method for monitoring in vivo changes in net tPA activ-
ity in brain tissue. Our results shed further light on tPA as a complex
mediator of CNS function and dysfunction.
O14B-4Brain plasminogen systemDoeuvre L1, Chimienty G2, Orset C1, Mezzapesa A2, Mata S3,Pepe G2 and Angles-Cano E1
1Inserm, Caen, France; 2Department of Biochemistry and
Molecular Biology, University of Bari, Bari; 3Department of
Neurology, Careggi Hospital, Florence, Italy
Endothelial cells, glial and neuronal cells, representing the princi-
pal sources of plasminogen activator (tPA and uPA), are in close
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
40 ORAL PAPERS____________________________________________________________________________________

interaction in the neurovascular unit. Formation of plasmin at the
surface of endothelial cells and neurons has important consequences
on these cells (apoptosis of endothelial cells and detachment/aggrega-
tion of neurons). The plasminogen activation system is also known to
participate in various inflammatory conditions of the central nervous
system. In such pathologies, beyond circulating plasminogen, the ori-
gin of plasminogen is still a matter of debate.
First, we have investigated the presence of plasminogen in human
cerebro-spinal fluids. The presence of plasminogen and the activity of
plasmin, tPA and uPA in inflammatory diseases (GBS, Guillain Barre
Syndrome patients, n = 14; MS, Multiple sclerosis, n = 9) and also
in non-inflammatory diseases (n = 13) were studied. Western blot-
ting, zymography and chromogenic detection were used to evaluate
antigens and activity of plasmin(ogen), uPA and tPA.
In human, plasminogen was detectable in both inflammatory (66%)
and non-inflammatory (65%) patients. Plasminogen was found in
larger concentration in inflammatory diseases (4.6 nM in GBS,
6.5 nM in MS and 2.2 nM in non inflammatory diseases). Active
plasmin was detected in GBS and MS patients (3.55 nM vs.
2.6 nM). uPA was detectable in a minority of patients (15% of
GBS, 20% if MS and 7% of non-inflammatory diseases), and tPA
was not detect.
To further investigate the origin of plasminogen in the central ner-
vous system, we are currently exploring the presence of plasminogen
in mouse parenchyma in physiological and inflammatory conditions
by immuno-histochemistry.
In conclusion, we have shown that a plasminogen activation system
is detectable in CSF of patient with inflammatory and non-inflamma-
tory diseases. The role of these proteolytic messengers in diseases out-
come remains to be determined.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
ORAL PAPERS 41____________________________________________________________________________________

Thrombolytic Therapy
O15A-1Combination of intra-arterial thrombolysis andmechanical treatment for acute ischemic strokeDippel DWJErasmus MC University Medical Center, Rotterdam, The
Netherlands
Acute ischemic stroke leads to death or disability in more than half
of all patients. National and international guidelines recommend
thrombolysis with intravenous rtPA in patients who can be treated
within 4.5 h and have no contra-indications. In the one fifth of
patients who have a proximal occlusion of an intracranial artery,
symptoms are often more severe and outcome is even less favorable.
Treatment with i.v. thrombolysis leads to recanalization in a minority
of these patients. Three small randomized clinical trials suggest that
local intra-arterial thrombolysis with delivery of the thrombolytic
agent through a microcatheter leads to better results: recanalization
in more than half of the patients. Mechanical treatment with a local
device may consist of aspiration, stenting, or thrombectomy with or
without ultrasound enhancement. Uncontrolled studies suggest that
these approaches may lead to recanalization in more than 60% of
treated patients. Complications of i.a. thrombolysis consist of reper-
fusion edema and hemorrhage, often leading to neurological deterio-
ration or death. Mechanical treatment is associated with similar and
with device-related complications such as dissection, vessel wall rup-
ture and local ischemia.
Prompt recanalization does not ensure improved neurological out-
come. The frequent complications cast doubt on the overall effect of
this treatment. The challenge for the coming years will be to assess
the effect of intra-arterial thrombolysis and mechanical treatment on
functional outcome after stroke, and to assess its safety in various
combinations, dosages and time windows. Large ongoing clinical tri-
als are the Interventional Management of Stroke trial 3 (IMS3) and
the Multicenter CLinical trial of Endovascular treatment for Acute
ischemic stroke in the Netherlands (MR CLEAN).
We will describe state of the art in intra-arterial treatment for acute
ischemic stroke, and discuss the results of published studies, as well
as the ethics and design of new and ongoing clinical trials.
O15A-2Improving stroke thrombolysis (tPA) safety throughthe use of plasma biomarkersMontaner JVall d’Hebron Hospital, Barcelona, Spain
The use of blood biomarkers is getting increasingly popular in the
field of cerebrovascular diseases, since biomarkers might aid physi-
cians in several steps of stroke evaluation. Although thrombolytic
therapy using tissue plasminogen activator (t-PA) in acute stroke is
effective since it accelerates clot lyses and earlier restoration of blood
flow, up to 40–50% of treated patients do not recanalize or do it too
late, and between 6% and 15% suffer hemorrhagic transformations
with high death rates. In the context of the neurovascular unit, t-PA
may degrade extracellular matrix integrity and increase risks of neu-
rovascular cell death, blood-brain barrier leakage, edema and hemor-
rhage. We have shown that t-PA treatment increases and activates
MMP-9 in human stroke, our data suggest that neutrophils are good
candidates to be the main source of MMP-9 following t-PA stroke
treatment and, in consequence, partially responsible of brain bleed-
ings. In humans, biomarkers such as matrix metalloproteinase-9
(MMP-9), vascular adhesion protein-1 (VAP-1) or fibronectin, which
might be used to select patients at higher risk of hemorrhagic trans-
formation, and high plasminogen activator inhibitor-1 (PAI-1) inter-
fering with tPA-induced recanalization, thus predicting clot-lyses
resistance and poor outcome, have been recently identified. More-
over, high levels of MMP-9 and MMP-13 are involved in DWI lesion
growth in spite of thrombolytic therapy suggesting its ultra-early role
in brain injury. Other biomarkers such as C-reactive protein may
accurately predict stroke mortality following reperfusion therapies.
Finally, we will also show that genetic background of stroke patients
may condition plasma levels of some of these biomarkers and influ-
ence therapeutic response in t-PA-treated patients.
O15A-3Thromboprophylaxis by cell-bound thrombolyticsMuzykantov VRUniversity of Pennsylvania, Philadelphia, PA, USA
Efficacy and safety of current thromboprophylaxis are limited, espe-
cially in acute settings associated with a short-term propensity for
thrombosis in post-surgical patients, among other potentially eligible
cohorts. In theory, timely delivery of thrombolytics into the interior
of nascent pathological clots could provide their rapid dissolution
preventing occlusion, if such a maneuver can be performed without
damaging hemostatic mural clots formed shortly after surgery. How-
ever, plasminogen activators have insufficient time of circulation,
attack preexisting hemostatic clots and penetrate into tissues includ-
ing the CNS where they exert adverse effects. Coupling plasminogen
activators to carrier red blood cells (RBC) does not affect negatively
RBC, yet prolongs tPA circulation time by several orders of magni-
tude, as well as prevents dissolution of hemostatic clots and side
effects in tissues. RBC glycocalyx protects RBC-bound tPA from
plasma inhibitors. Further, recombinant proteins fusing mutant
thrombin-activated plasminogen activators with a single chain frag-
ment of a monoclonal antibody to glycophorin A safely bind to cir-
culating RBC after injection in animals, circulate for many hours and
prevent formation of occlusive venous and arterial clots in animal
models. Results of recent and ongoing studies in models of cerebral
and peripheral thrombosis and ischemia in mice, rats and pigs indi-
cate that using RBC as a carrier for prophylactic delivery of fibrino-
lytics provides immediate and safe short-term thromboprophylaxis,
unattainable with free tPA causing severe side effects.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
42 ORAL PAPERS____________________________________________________________________________________

New Factors, Functions, Mechanisms
O15B-1Epithelial development and homeostasis requirecomplex interactions between matriptase and theKunitz-type transmembrane serine protease inhibitors,HAI-1 and HAI-2Bugge TH1, Szabo R1, Kosa P1 and List K2
1NIH, Bethesda, MD; 2Wayne State University, Detroit, MI, USA
Matriptase (a.k.a., MT-SP1 and epithin) is an autoactivating type II
transmembrane serine protease that is constitutively expressed in
many developing and adult epithelia. We show that postnatal abla-
tion of matriptase from epithelia of diverse origin and function leads
to a spectrum of abnormalities ranging from impaired barrier func-
tion and loss of secretory function to complete de-differentiation and
malignant transformation. This epithelial demise was often preceded
by loss of tight junction function, increased paracellular permeability,
and mislocation of tight junction-associated proteins. Hepatocyte
growth factor activator inhibitor (HAI)-1 and HAI-2 are Kunitz-type
transmembrane serine protease inhibitors that display potent inhibi-
tory activity towards matriptase in vitro. We found that both HAI-1
and HAI-2 display near-ubiquitous co-localization with matriptase in
embryonic as well as adult epithelial tissues. Disruption of either the
HAI-1 or the HAI-2 gene in mice led to embryonic lethality, which
was associated with loss of epithelial cell polarity. However, simulta-
neous genetic inactivation of matriptase in either HAI-1- or HAI-2-
deficient embryos completely rescued this embryonic lethality, identi-
fying matriptase as the primary developmental protease target for
both protease inhibitors. Moreover, HAI-1-deficient mice with low
matriptase levels (1–15%) not only completed embryonic develop-
ment, but displayed normal long-term survival. Combined heterozy-
gosity for HAI-1 and HAI-2 also caused embryonic lethality
(nonallelic noncomplementation), which could be rescued by the loss
of just a single matriptase allele. Taken together, these data show
that epithelial development and homeostasis is enabled by complex
interactions between the membrane serine protease, matriptase, and
the Kunitz-type transmembrane serine protease inhibitors, HAI-1
and HAI-2.
O15B-2Protease signaling contributes to neural tube closureCamerer E1, Barker A2 and Coughlin SR2
1Inserm U970, Paris Cardiovascular Research Center, Paris,
France; 2Cardiovascular Research Institute, University of
California San Francisco, San Francisco, CA, USA
Protease-activated receptors (PARs) are G protein-coupled receptors
that mediate cellular responses to proteases. Mice with single deficien-
cies in PARs displayed defects in vascular development and hemosta-
sis, most likely reflecting a disruption in the ability of mutant
endothelial cells and platelets to sense active coagulation proteases.
To identify roles for protease signaling beyond the vasculature and
seek evidence for additional physiological PAR agonists, we gener-
ated mice with combined deficiencies in all PARs. We thus revealed
an unexpected role for protease signaling in neural tube closure and
formation of the central nervous system. Mouse embryos lacking
PARs 1&2 showed defective hindbrain and posterior neuropore clo-
sure and developed exencephaly and spina bifida. Par1 and Par2 were
expressed in surface ectoderm, Par2 selectively along the line of clo-
sure. Ablation of Gi/z and Rac1 function in these Par2-expressing
cells disrupted neural tube closure, further implicating G protein-cou-
pled receptors and identifying a likely effector pathway. Cluster anal-
ysis of protease and Par2 expression patterns revealed a group of
membrane-tethered proteases often co-expressed with Par2. Among
these, matriptase activated Par2 with picomolar potency, and hepsin
and prostasin activated matriptase. Together, our results suggest a
role for protease-activated receptor signaling in neural tube closure
and identify a local protease network that may trigger Par2 signaling
and monitor and regulate epithelial integrity in this context.
O15B-3Proteolysis of human Factor IX and FIXa:gla-dependant conformational specificity in itsinactivation by plasminSutton A1, Fatemi M1, Vancott KE1, Bajaj SP2 and Velander WH1
1University of Nebraska-Lincoln, Lincoln, NE; 2University of
California Los Angeles, Los Angeles, CA, USA
The biosynthesis of recombinant human Factor IX (rhFIX) creates
major subpopulations that differ in post-translational modification
(PTM). We have compared differences in PTM between subpopula-
tions of rhFIX made in transgenic pig milk (tg-rhFIX) and rhFIX
made in CHO cells (CHO-rhFIX) to human plasma-derived Factor
IX (pd-hFIX). Differences occur in the content of gamma-carboxy-
glutamic acid (gla) that affect procoagulation activity. Interestingly,
similar proteolytic degradation products were found in rhFIX and
pd-FIX preparations. The proteolysis pattern of tg-rhFIX is consis-
tent with plasmin’s established role as a predominant milk protease.
This is the first report of gla-dependant conformational effects upon
plasmin cleavage of Factor IX. in vitro treatment by plasmin of
CHO-rhFIX, pd-hFIX, and tg-rhFIX subpopulations having different
gla contents showed contrasting degradation in the presence of cal-
cium or EDTA. Higher gla content rhFIX or pd-FIX species (11 or
12 gla) showed a bias towards plasmin mediated proteolysis to form
rFIX-alpha in the presence of Ca2+. This indicates a gla-dependant
presentation of the Arg 145 cleavage site on the NH2-terminus of
activation peptide. In contrast, lower gla content (average nine) spe-
cies showed increased production of rhFIX-gamma indicating
increased accessibility of Arg 318 cleavage site in the catalytic domain
of Factor IX relative to Arg 145. While rhFIX- or pd-FIX-alpha
retain procoagulation activity, their gamma proteolysis products are
inactive due to Factor X exosite disruption by plasmin cleavage.
Fully activated Factor IX exhibited resistance to hydrolysis by plas-
min in either Ca2+ or EDTA indicating that it less efficiently pre-
sents the Arg 318 cleavage site than does Factor IX zymogen and
Factor IX alpha. Based upon this data, we hypothesize that Factor
IX activity consumption in blood circulation by plasmin is affected
by Factor IX gla-content. For example, a more rapid inactivation of
lower gla content Factor IX by plasmin could arise from warfarin
therapy.
O15B-4Thresholding behaviour in prothrombin activation byprothrombinaseCook PM, Colizza K and Nesheim MEQueen’s University, Kingston, Canada
In systems that are initiated by stimuli and have both positive feed-
back and inhibition, thresholding can exist, depending on the relative
kinetics of feedback and inhibition. Two manifestations of threshold-
ing are steep dose-response curves and ‘all or none’ responses. These
studies were carried out to determine whether prothrombin activation
exhibits thresholding, when the dose is defined as the input factor Xa
concentration and the response is defined as the area under the
thrombin concentration time course (thrombin potential). Factor Xa
was added to prothrombin, factor V, antithrombin, phosphatidylcho-
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
ORAL PAPERS 43____________________________________________________________________________________

line and phosphatidylserine vesicles, CaCl2, and the fluorogenic
thrombin substrate Z-Gly-Gly-Arg-7-amido-4-methylcoumarin (Z-
GGR-AMC). The free thrombin concentration over time was calcu-
lated from rates of Z-GGR-AMC hydrolysis. In the above condi-
tions, the thrombin potential was nearly zero from 0 pM to 0.5 pM
factor Xa, increased approximately linearly from 0.5 pM to 3 pM
factor Xa, and plateaued thereafter. This relationship demonstrates
the existence of thresholding with respect to the dose of factor Xa in
prothrombin activation. Activated protein C addition (0–5 nM)
raised the threshold factor Xa dose from 0.5 pM to 10 pM. Similarly,
heparin (0–2 lg/mL), enoxaparin (0–100 nM), and fondaparinux (0–
100 nM) increased the threshold factor Xa dose from 0.5 pM to 50,
150, and 200 pM, respectively. The thrombin time courses were fit to
a computer model of prothrombin activation which includes inhibi-
tion of thrombin and factor Xa by antithrombin and antithrombin-
heparin, positive feedback activation of factor V by thrombin and
factor Xa, and factor Va inactivation by activated protein C. The
model predicted the experimental data well, which suggests that
thresholding is a property intrinsic to this system of components. The
experimental data and model both show that prothrombin activation
is threshold dependent and the threshold dose of factor Xa changes
with changes in the kinetics of feedback and inhibition.
O15B-5Reduced thromboxane production in morbidly obesesubjects: another facet of the ‘obesity paradox’Cialdella P1, Graziani F1, Biasucci LM1, Giubilato S1, Liuzzo G1,Della Bona R1, Pulcinelli FM2, Iaconelli A1, Mingrone G1 andCrea F1
1Universita Cattolica del Sacro Cuore; 2Universita La Sapienza,
Roma, Italy
Purpose: Post-mortem studies have demonstrated that morbidly
obese subjects (MO) surprisingly show less coronary atherosclerosis
than obese subjects (O), but the reasons for this apparent protection
from atherosclerosis are not clear yet. Thromboxane A2 (TxA2), a
marker of platelet activation, is higher in O compared to lean sub-
jects (L) and this might represent a clue to their increased cardiovas-
cular risk. However, data on TxA2 in MO are still lacking, therefore
we hypothesized that lower levels of TxA2 in MO might play a role
in their lower atherosclerotic burden.
Methods: We measured serum levels of Thromboxane B2(TxB2), a
stable metabolite of TxA2, high-sensitivity C-reactive protein(hs-
CRP)and leptin in 17 L (BMI 22.9 � 1.6), 25 O (BMI 32.6 � 2.4)
and 23 MO (BMI 48.6 � 7.1), without insulin resistance, diabetes
and overt cardiovascular diseases.
Results: Serum TxB2 levels were lower in L versus O (P = 0.046),
and in MO versus L and O (P = 0.03 and P < 0.001 respectively).
In contrast, hs-CRP and leptin levels were higher in O versus L (hs-
CRP P < 0.001; leptin P = 0.002) and MO versus L (P < 0.001 for
both). Leptin was also higher in MO versus O (P < 0.001). TxB2
negatively correlated with leptin and BMI. Hs-CRP correlated with
leptin, and both of them were also correlated with waist circumfer-
ence, BMI and HOMA-IR.
Conclusions: Insulin sensitive MO show lower levels of TxB2 as com-
pared with O and L, suggesting that a reduced platelet activation
could play a role in the paradoxical protection of MO from athero-
sclerosis, despite higher levels of leptin.
ª 2010 The Authors. Journal compilation ª 2010 International Society on Thrombosis and Haemostasis 8 (Suppl. 1) (2010) 1–44
44 ORAL PAPERS____________________________________________________________________________________





























