Embed Size (px)
Citation preview
An Integrated Framework forDecision Making in NeurologicPhysical Therapist Practice
Decision-making frameworks are used by clinicians to guide patient manage-ment, communicate with other health care providers, and educate patientsand their families. A number of frameworks have been applied to guideclinical practice, but none are comprehensive in terms of patient manage-ment. This article proposes a unifying framework for application to decisionmaking in the management of individuals who have neurologic dysfunction.The framework integrates both enablement and disablement perspectives.The framework has the following attributes: (1) it is patient-centered, (2) it isanchored by the patient/client management model from the Guide for PhysicalTherapist Practice, (3) it incorporates the Hypothesis-Oriented Algorithm forClinicians (HOAC) at every step, and (4) it proposes a systematic approach totask analysis for interpretation of movement dysfunction. This frameworkprovides a mechanism for making clinical decisions, developing clinicalhypotheses, and formulating a plan of care. Application of the framework isillustrated with a case example of an individual with neurologic dysfunction.[Schenkman M, Deutsch JE, Gill-Body KM. An integrated framework fordecision making in neurologic physical therapist practice. Phys Ther. 2006;86:1681–1702.]
Key Words: Clinical decision making, Models, Neurologic dysfunction.
Margaret Schenkman, Judith E Deutsch, Kathleen M Gill-Body
Physical Therapy . Volume 86 . Number 12 . December 2006 1681
IIIST
EPSe
ries �
������������������������������������������������������������������������������������������������������������������������������
������
������
������
������
������
������
������
������
������
������
������
������
������
������
������
������
������
������
������
������
������
Dow
nloaded from https://academ
ic.oup.com/ptj/article/86/12/1681/2805124 by guest on 04 July 2022

Decision-making frameworks are instrumentalin guiding clinicians through a comprehen-sive process of patient management, commu-nicating with other health care providers, and
facilitating the educational process. A number of frame-works have been applied to clinical practice over the past2 decades for guiding clinical decision making.1–7 Earlyframeworks were based on disablement models.8–10 Sub-sequently, other frameworks were described based onenablement perspectives.11,12 Most recently, the Interna-tional Classification of Functioning, Disability and Health(ICF)13 was developed, integrating both enablement anddisablement perspectives.14 These various frameworkswere intended to organize aspects of the patient’s healthcondition for research, policy, and related decisions.However, for clinical care within physical therapy, no oneframework provides enough detail for decision making.For this purpose, it is important to separate out specificcomponents of enablement and disablement and to ana-lyze their implications for patient management.
The framework proposed in this article is designed tolink the larger concepts of health (enablement anddisablement) to the scope of physical therapist practice.The framework is intended to guide physical therapistpractice and to provide a structure for teaching clinicaldecision making to future clinicians. Specifically, thisarticle accomplishes the following:
(1) It presents a unifying framework for making clinicaldecisions by integrating and applying a variety ofconceptual models and analyses at different pointswithin the management process.
(2) It proposes a systematic approach to task analysis forsummarizing the movement problem.
(3) It illustrates how the generation of clinical hypoth-eses and their progressive refinement drives man-agement choices.
(4) It uses a case example to illustrate application of theunifying framework and systematic task analysis.
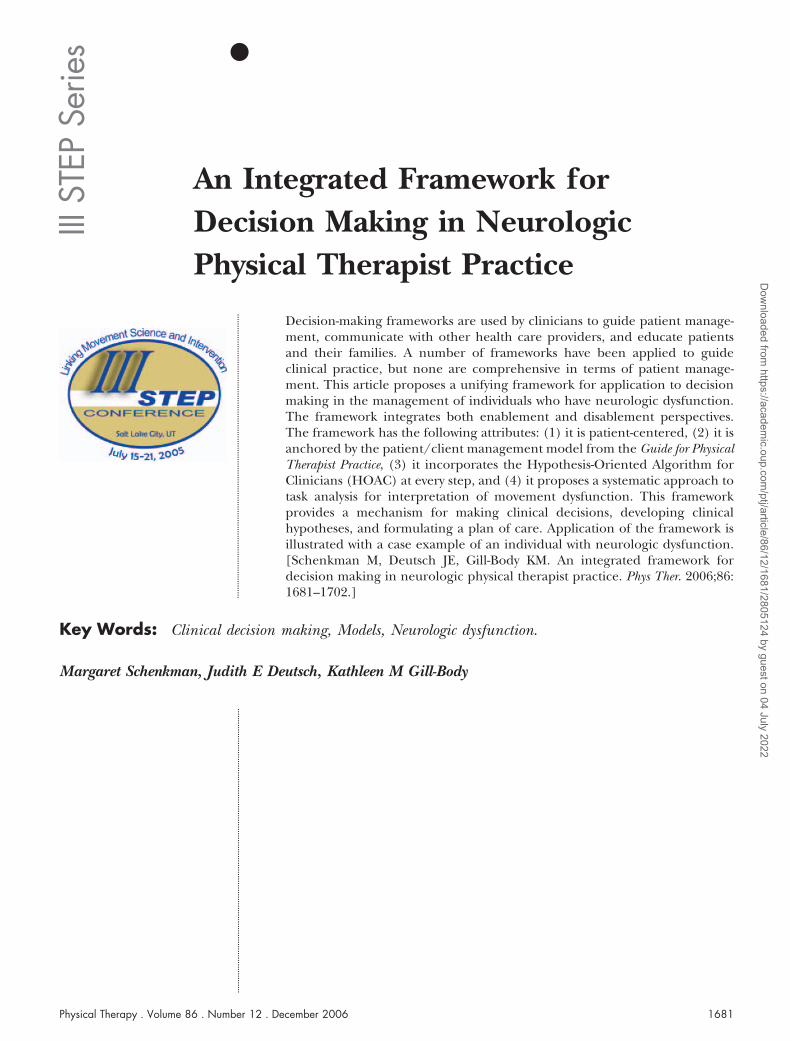
Overview of the FrameworkThe decision-making process we describe is patientcentered,15–18 which means that the whole process isfocused around the patient as depicted in Figure 1. Thispatient-centered approach contrasts with a pathology-driven approach in which the process is initiated withdisease and culminates in disablement. The patient-centered approach that we propose emphasizes rolesand functions of which the individual is capable and atthe same time identifies limitations in the individual’sabilities, with the goal of minimizing barriers to fullparticipation within society or the environment.
The framework that we describe has 4 distinct character-istics. First, it is anchored by the structure of the patient/
M Schenkman, PT, PhD, is Professor and Director, Physical Therapy Program, Department of Physical Medicine and Rehabilitation, University ofColorado at Denver and Health Sciences Center, Denver, CO 80262 (USA). Address all correspondence to Dr Schenkman at:[email protected].
JE Deutsch, PT, PhD, is Professor and Director of the Rivers Lab, Graduate Programs in Physical Therapy Program, Department of Developmentaland Rehabilitation Sciences, University of Medicine and Dentistry of New Jersey, Newark, NJ.
KM Gill-Body, PT, DPT, NCS, is Adjunct Clinical Associate Professor, Graduate Programs in Physical Therapy, MGH Institute of Health Professions,Boston, Mass.
All authors contributed to each part of the manuscript, including conceptualization, writing, and editing. The authors thank Jody Cormack, PT,DPT, for her insight and suggestions in the final drafts of the manuscript. They acknowledge substantive discussions with a number of colleaguesat the III STEP symposium and in particular thank James Gordon, PT, EdD, Lois Hedman, PT, MS, Lori Quinn, PT, EdD, and AnneShumway-Cook, PT, PhD. They also thank Jeffrey Lewis, who assisted with preparation of the figures.
This work was supported by National Institutes of Health grants #5 R01 HD 43770-03 and #M01 RR00051-44 and the University of Medicine andDentistry of New Jersey Master Educator Guild.
This article is based on a presentation at the III STEP Symposium on Translating Evidence Into Practice: Linking Movement Science andIntervention; July 15–21, 2005; Salt Lake City, Utah.
This article was received August 18, 2005, and was accepted July 14, 2006.
DOI: 10.2522/ptj.20050260
The proposed framework is intended
to guide physical therapist practice
and to provide a structure for teaching
clinical decision making to future
clinicians.
1682 . Schenkman et al Physical Therapy . Volume 86 . Number 12 . December 2006
Dow
nloaded from https://academ
ic.oup.com/ptj/article/86/12/1681/2805124 by guest on 04 July 2022
client management model, described in the Guide toPhysical Therapist Practice,19 and organizes patient man-agement from the initial encounter through the devel-opment and implementation of the plan of care andoutcomes measurement. Second, at each step of thepatient management process, clinical hypotheses aregenerated using the Hypothesis-Oriented Algorithm forClinicians (HOAC)1,20 to guide decision making. TheHOAC, which has been described elsewhere,1,20 ispatient centered, hypothesis driven, and iterative. Third,task analysis is used to examine and analyze problemswith performance of functional movement and then tosystematically summarize the movement problem.Finally, enablement and disablement models are appliedthroughout the management process, with particularemphasis on application of the enablement perspective,which we believe has been less well described in theliterature.
This framework was developed to provide a comprehen-sive approach to physical therapy, which can be used toguide clinical decisions and can be used to structure theeducation of future clinicians. In the following sectionsof this article, we elaborate on application of the frame-work for the management of individuals who haveneurologic disorders. Although this article focuses onpeople with neurologic dysfunction, the framework alsoshould be applicable across the life span to people whohave other conditions.
History and InterviewThe purpose of the history and interview is to gain anunderstanding of the patient as an individual, determinewhy the individual seeks physical therapy, identify whathe or she hopes to achieve through physical therapy, andbegin to formulate the examination strategy. The inter-view and history process initiates the collaborative rela-tionship between the patient and the physical therapist.
The interview begins by exploring questions such as thefollowing: What is the person’s role in society, and howis that affected by the current condition? Specifically,what does the person do vocationally and for recreation?What are the patient’s goals and identified problems?What is it that the patient wants to be able to do that heor she currently cannot do; in the patient’s view, what isneeded to overcome these functional limitations? Whatassistance does the patient expect from the clinician?What assistance does the patient need from the family orcaregivers? What assistance do the family or caregiversneed from the clinician? The patient is the primarysource for this information, but caregivers also contrib-ute; their perspective may be different from the patient’sperspective and also is important to include.21 Thisprocess begins during the interview and is further devel-oped during the examination.
In the proposed framework, the interview process drawson enablement and disablement perspectives as well as
Figure 1.Overview of the unifying framework demonstrating the steps in the clinical decision-making process. This framework is patient centered, integratesboth enablement and disablement perspectives, and incorporates a variety of existing conceptual models and analyses at various points in the patientmanagement process. HOAC�Hypothesis-Oriented Algorithm for Clinicians.
Physical Therapy . Volume 86 . Number 12 . December 2006 Schenkman et al . 1683
������
������
������
�����
Dow
nloaded from https://academ
ic.oup.com/ptj/article/86/12/1681/2805124 by guest on 04 July 2022

the HOAC. To understand the proposed framework, it isnecessary to highlight salient features from theseapproaches.
Application of the Enablement PerspectiveThe enablement model, as described by Quinn andGordon,7 guides the clinician to identify the individual’sparticipation and roles, including self-care, social, occu-pational, and recreational activities. The enablementmodel also explores the skills and resources that arerequired for fulfilling roles within different environmen-tal contexts (eg, the ability to achieve meaningful goalswith efficiency, flexibility, and consistency). Quinn andGordon defined resources as “physical and cognitivemechanisms, including musculoskeletal linkages, con-trol of basic movement types and the ability to plan.”7(p7)
In applying Quinn and Gordon’s enablement conceptsto our integrated framework, we broaden the concept ofresources to also include the social, emotional, andsocietal resources at the patient’s disposal.
Application of the Disablement PerspectiveThe disablement models begin the analysis from theunderlying disease or pathology.8,9 Relevant informationis revealed during the patient’s report of past medicalhistory, and review of the medical record guides specificquestions during the interview. Specific questions alsoare derived from knowledge about pathology and typicalor predicted signs, symptoms, and impairments associ-ated with these conditions. The clinician’s questionselicit information from the patient regarding the pres-ence and severity of these signs, symptoms, and impair-ments. This information guides the systems review andselection of examination procedures. Patients may iden-tify underlying impairments that they perceive as limit-ing (eg, weakness, stiffness, loss of feeling, pain). Theclinician may identify possible impairments throughobservation and communication (eg, faulty movementpatterns, cognitive impairments).
Application of the HOACThe HOAC1,20 is an algorithm that allows the clinician toexplore the patient’s concerns, referred to as the“patient-identified problems” (PIPs). The clinician alsoexplores problems not identified by the patient butrather by the clinician and caregivers. These problemsare referred to as “non–patient-identified problems”(N-PIPs). The clinician’s perspective can be particularlyimportant in identifying potential future problems (pre-vention) and in identifying functional limitations andunderlying impairments that have not risen to the levelof the patient’s awareness, but may become progressivelylimiting. The HOAC also prompts the clinician to beginto develop hypotheses surrounding identified problemsthroughout the interview process. These hypothesesshape the plan for further patient examination.
Integration of Perspectives From Enablement,Disablement, and HOACTo illustrate how the models are integrated, we describethe following scenario where questions from each per-spective are asked. First, the physical therapist asks thepatient to identify his or her societal roles and anyproblems he or she has in fulfilling them (eg, problems,goals of treatment [enablement and HOAC]). Thephysical therapist also solicits input from family mem-bers and caregivers (HOAC). The physical therapistthen explores the specific abilities and skills that thepatient needs to fulfill the identified goals and ascertainsthose areas in which the patient experiences difficulty(enablement). This initial process is accomplished with-out consideration of the primary diagnosis or past med-ical history. When the physical therapist has completedthis portion of the history and interview, it should bepossible to answer the following questions:
• What are the patient’s needs in terms of participa-tion and activity?
• Why is the patient here (problem and goals)?• What can the family offer?• What are the perceived needs of the family?• What is the patient’s social, emotional, and physical
context?
The clinician should be able to answer the above ques-tions prior to analyzing the patient’s condition from adisablement perspective. From the disablement perspec-tive, the physical therapist explores underlying impair-ments that could contribute to the patient’s functionaldifficulties, based on knowledge of the pathology and itssequelae. For example, the physical therapist proceedswith specific questions aimed at detecting the patient’ssigns, symptoms, and impairments relevant to the disor-der. All of this information, taken together, informs theexamination strategy.
Transition From Interview to Systems ReviewDuring the history and interview, the clinician begins toformulate hypotheses that guide the transition into thesystems review and examination (HOAC). For example,the clinician may observe cognitive or perceptual limita-tions that indicate the need for a detailed examinationof these systems. The clinician may observe that a patienttransitions to and from a seated position and walks witha gait pattern typical of someone with intact sensory andmotor systems, suggesting that these systems need not beexamined in detail at the present time. Conversely, theclinician might observe that another individual alwaystransitions to a standing position by pushing up fromarm rests and does not take weight symmetricallythrough both lower extremities. Depending on thepatient’s diagnosis and premorbid and comorbid condi-tions, the patient’s task performance could suggest pain,
1684 . Schenkman et al Physical Therapy . Volume 86 . Number 12 . December 2006
Dow
nloaded from https://academ
ic.oup.com/ptj/article/86/12/1681/2805124 by guest on 04 July 2022

loss of lower-extremity range of motion, weakness,impaired sensory perception, or impaired motor organi-zation. These observations, along with knowledge of thedisorder, guide the clinician to specific choices of tests,measures, or activities to be included in the systemsreview.
Systems ReviewThe purpose of the systems review is to rule out thosebody systems with which the physical therapist need notbe concerned, identify systems that are resources for thepatient, guide choices regarding which aspects of theremaining systems to examine in detail, and determinewhether the physical therapist should proceed or shouldrefer the patient to other health care providers. Thesystems review can be conducted at the level of tasks orthe level of impairments, as is illustrated below.
The patient/client management model19 is used toorganize the overall systems review. Included is a reviewof arousal, attention, and cognition, as well as a mini-mum data set (eg, height, weight, heart rate after somespecific activity such as push-ups for an individual withspinal cord injury). Four major body systems arereviewed, related to the physical therapist practice pat-terns, including neurologic, musculoskeletal, cardio-pulmonary, and integumentary.
The systems review can be carried out at the level of tasksor level of impairments, or some combination of these 2levels. Reviewing of body systems at the level of tasks hasthe advantage of emphasizing the patient-centered focus.For this reason, we begin by describing that process.
Systems Review at the Level of TasksWhen beginning the systems review by examining tasks,the clinician analyzes the patient’s overall performanceon specific relevant tasks to develop hypotheses aboutwhich impairments should be examined in detail. If thepatient’s performance of a task is outside the typicalperformance range for the age and sex of the patient,the clinician proceeds to examine those specific under-lying impairments associated with problems with perfor-mance of the task (eg, strength [force-generating capac-ity of a muscle], range of motion, postural control). Inthe systems review, screening is conducted in a variety ofways, including the use of measurable tasks as well asobservational analyses.
With regard to quantitative approaches to screeningtasks, performance on a number of tasks has well-defined implications. For example, the Timed “Up &Go” Test, Functional Reach Test, and Berg Balance Testall can predict falls.22–24 If the patient has difficulty withperformance on these tasks, the clinician is alerted toperform a detailed examination of sensory and motor
organization. However, if performance is within thenormal range on any of these measures, it may not benecessary to assess specific elements of postural control(or balance) such as sensory organization. Similarly, theSix-Minute Walk Test25 can be used to identify potentialproblems with cardiovascular or musculoskeletal endur-ance that need to be further examined.
Observational task analysis also can be used in thesystems review. For example, requirements for the sit-to-stand task include force generation of specific musclegroups, range of motion at specific joints, and balanceand postural control.26–28 The clinician might ask apatient to stand from a low seat in order to quicklyobtain an assessment of lower-extremity strength andbalance control. If the patient has difficulty performingthe task, the clinician could be guided to include adetailed assessment of strength and postural control inthe examination. Alternatively, if the patient is able torise to a standing position successfully and smoothly, theclinician may logically conclude that lower-extremitystrength is, at a minimum, in the “fair” range and thatpostural control is adequate for this task. The clinicianthen may chose to defer detailed examination of theseareas.
Systems Review at the Level of ImpairmentsThe clinician also can choose to begin the systems reviewby examining specific impairments. Examination ofimpairments can draw on a variety of standard tests andmeasures (eg, reflexes, range of motion, muscle perfor-mance, sensory integrity), many of which are well artic-ulated in the Guide to Physical Therapist Practice.19 Impair-ments also can be measured using standardized testssuch as the Orpington test,29 which measures 4 areas:motor deficit of the arm, proprioception, balance, andcognition. The scores can be summarized to identifydisease severity. Additionally, looking at test scores ineach of the domains of the test may guide the clinicianto perform a more detailed examination.
Models That Inform the Systems ReviewIn contrast to the interview, where the enablementperspective leads off the process, the systems review ismore heavily focused on a disablement perspective. Thisis because a major purpose of the systems review is toidentify those systems that are impaired.
A number of disablement models provide guidanceregarding systems that are likely to be compromised withspecific diseases, injuries, or disorders. These disable-ment models include, but are not limited to, the WorldHealth Organization (WHO) model8 and the Nagi mod-el.9 The work of Verbrugge and Jette10 draws attention tofactors that should be reviewed as a result of previousmedical history (comorbid conditions). For example,
Physical Therapy . Volume 86 . Number 12 . December 2006 Schenkman et al . 1685
������
������
������
�����
Dow
nloaded from https://academ
ic.oup.com/ptj/article/86/12/1681/2805124 by guest on 04 July 2022
when an individual is admitted with a stroke and aprevious history of diabetes mellitus, it is particularlyimportant to screen for impairments associated withdiabetes (eg, sensory and integumentary integrity of thedistal extremities). When an individual has worked inthe mines throughout his adult life, it is particularlyimportant to carefully review the respiratory system.
Schenkman and Butler2 further elaborated on the dis-ablement models to make them applicable to clinicaldecision making for neurologic physical therapist prac-tice. To this end, the models of Schenkman and col-leagues2,3,5 draw attention to systems that may beimpaired as sequelae of the injury or disorder for whichthe patient seeks treatment. For example, an individualwho sustained a stroke some years ago and was sedentarythereafter is likely to have secondary cardiovasculardeconditioning.30 An individual with Parkinson disease(PD) is likely to have lost substantial range of motion inthe axial structures.31,32 Schenkman and colleagues haveapplied this model to patients with PD, and the modelhas been tested in several experimental studies, demon-strating relationships between range of motion and bothfunctional and kinematic measures of standing reach aswell as improvement of functional reach following use ofexercises to improve axial range of motion.31–33
In contrast, the enablement model draws attention tophysiologic reserves that may be resources to the patient.For example, compared with more sedentary individu-als, the distance runner may have substantial cardio-vascular reserve and the practitioner of yoga may haveenhanced flexibility. Hypotheses regarding the presenceand extent of physiological reserves can be tested in thesystems review or during the examination.
On completion of the initial systems review, the physicaltherapist should be able to accomplish the followingspecific tasks associated with disablement:
• Arousal, attention, and cognition:� Determine the appropriate style of interaction
with this patient and the need to modify furtherexamination or intervention procedures.
� Identify the need for further examination(eg, Mini-Mental State Exam).
• The primary disorder:� Rule out potential problems and issues that
could occur with patient’s primary disorder butdo not exist for this particular patient.
� Identify those body systems that are impaired andneed further examination to determine theseverity of involvement.
� Determine which specific impairments will beexamined.
• Impairments associated with comorbid conditions(pathology or disease)10:� Determine which specific impairments will be
examined in-depth, based on factors such as age,recreational activities, and work history.
• Secondary impairments2:� Identify which impairments are present among
those that typically occur as sequelae to theprimary disorder in systems other than the onefor which the patient sought physical therapycare.
With respect to the enablement model, the clinicianshould be able to accomplish the following tasks:
• Communication� Determine the patient’s preferred style of com-
munication and learning.
• Resources� Identify those systems that are particularly well
developed for the patient and can be or are usedto facilitate functional ability.
Transition From Systems Review to ExaminationAs information is gathered during the systems review,the clinician integrates findings with those obtainedduring the history and continues to develop clinicalhypotheses. These hypotheses may explain relationshipsamong existing impairments and functional abilities;hypotheses also may identify key issues that should beexamined related to the patient’s environment. Forexample, the clinician may make decisions about whichtasks to examine further and how to manipulate theenvironment during further examination. Additionally,the clinician often develops initial hypotheses aboutprognosis.
ExaminationThe specific purposes of the examination may vary anddepend on the reason for which it is carried out. Thelevel of examination is adjusted to reflect patient-identified problems and goals and can be drawn fromelements of the continuum of the ICF model. Forexample, the examination takes into account relevantresources (enablement), activities, participation, andquality of life, as well as underlying impairments (dis-ablement). For the purposes of this discussion, a distinc-tion is made between the initial examination and subse-quent re-examination, although examination takes placethroughout the patient management process.1,20
The initial examination provides data that can be used toaccomplish some or all of the following purposes:(1) perform triage (eg, to determine whether referral to
1686 . Schenkman et al Physical Therapy . Volume 86 . Number 12 . December 2006
Dow
nloaded from https://academ
ic.oup.com/ptj/article/86/12/1681/2805124 by guest on 04 July 2022

another health care professional is needed), (2)describe the movement problem for key tasks that aremeaningful to the patient within a relevant environmen-tal context (eg, walking in the dark; crawling across thecarpet), (3) identify patient’s resources and impair-ments, (4) test hypotheses from the history and systemsreview, and (5) formulate prognoses (eg, expecteddegree of recovery following a stroke, expected develop-mental problems following premature birth). In addi-tion, the examination leads to the ability to provide abasis from which to determine the approach to the planof care and to determine potential outcome measures.
Subsequent re-examination includes the following purpos-es: (1) test existing hypotheses, (2) develop and test newclinical hypotheses when the initial hypotheses are notsupported by the patient’s response to intervention, and(3) obtain specific outcome measurements.
As the clinician proceeds through the examinationprocess, there is an ongoing synthesis and analysis, asoutlined by the HOAC.1 Information from one set oftests provides guidance regarding the next logicalchoices of tests and measures. This ongoing analysiscomplements, but does not replace, the overall synthesisof findings that occurs in the evaluation.
The strategy and depth of the examination may vary,depending on the purposes. Relevant issues to considerinclude the patient’s level of function, the purposes ofthe examination (eg, prognosis, plan of care), and theclinician’s preferred style. The purposes of the examina-tion also set specific limits regarding what informationwill be obtained. For example, if the sole purpose is forformulation of a prognosis, the clinician may select aspecific focused examination approach (eg, the Fugl-Meyer examination to predict recovery from stroke,34
the Gross Motor Function Classification to predict func-tion in children with cerebral palsy,35 Glasgow ComaScale to predict outcome after traumatic brain injury36).If the purpose is to develop a plan of care and measureoutcomes, the clinician might chose measures such asthe Unified Parkinson’s Disease Rating Scale (UPDRS)37
or functional measures for children such as the PediatricEvaluation of Disability Inventory (PEDI) or the GrossMotor Function Measure (GMFM),34,38–41 all of whichare sensitive to change.
For purposes of developing a plan of care, the followinginformation should be obtained:
• Level of independence or dependence for func-tional activities of greatest importance to thepatient, including level of assistance needed, use ofexternal devices, or environmental modifications;
• Analysis of task performance for a variety of func-tional activities under various environmental condi-tions; and
• Possible reasons underlying the difficulty or inabil-ity to perform the task, including relevant impair-ments and environmental barriers.
The examination begins by observation of functionalactivities (eg, walking, getting up from a bed or a chair).The clinician decides the order in which the examina-tion data will be obtained. For example, the clinicianmight begin with a detailed task analysis of specificfunctional activities and work backward toward under-lying resources and impairments. Using this approach,the clinician performs the detailed task analysis, devel-ops hypotheses related to likely underlying impairments,and proceeds with the specific tests and measures thatare most likely to identify the presence and severity ofexisting impairments. This detailed task analysis is morespecific and systematic than the task analysis used duringthe systems review, as is illustrated below.
The use of task analysis to make judgments during theexamination requires knowledge of the literature link-ing performance and impairments and clinical experi-ence to recognize patterns of performance and theirimplications regarding underlying impairments. There-fore, this strategy may be difficult for the noviceclinician.
Alternatively, the clinician might begin by examiningthose impairments identified during the systems reviewas well as those known to occur with the specific under-lying disorder and its sequelae, as well as comorbidconditions. The clinician might proceed next to adetailed analysis of task performance. Using this routeinto the examination process, the clinician works for-ward from impairments to ability to perform functionaltasks.
Whatever examination approach is used, the clinician isjudicious in determining what should be examined sothat the maximum information can be obtained fromthe fewest possible tests and measures. To make judg-ments, the clinician draws from the patient’s problemsand goals, the clinician’s knowledge of the disorder, andpremorbid and comorbid conditions. In reality, exami-nation often proceeds as a combination of these 2approaches. For clarity, however, these 2 approaches arediscussed as distinct processes beginning with taskanalysis.
Examination at the Level of Task AnalysisTask analysis is a detailed observational analysis of thepatient’s total body movement patterns during taskperformance.42 Task analysis helps clinicians to deter-
Physical Therapy . Volume 86 . Number 12 . December 2006 Schenkman et al . 1687
������
������
������
�����
Dow
nloaded from https://academ
ic.oup.com/ptj/article/86/12/1681/2805124 by guest on 04 July 2022
mine whether the patient’s movement performance iswithin a range of typical performance and to determinewhere within the performance specific problems occur.The results of the task analysis shape the plan of care,which typically is focused around improvement offunction.
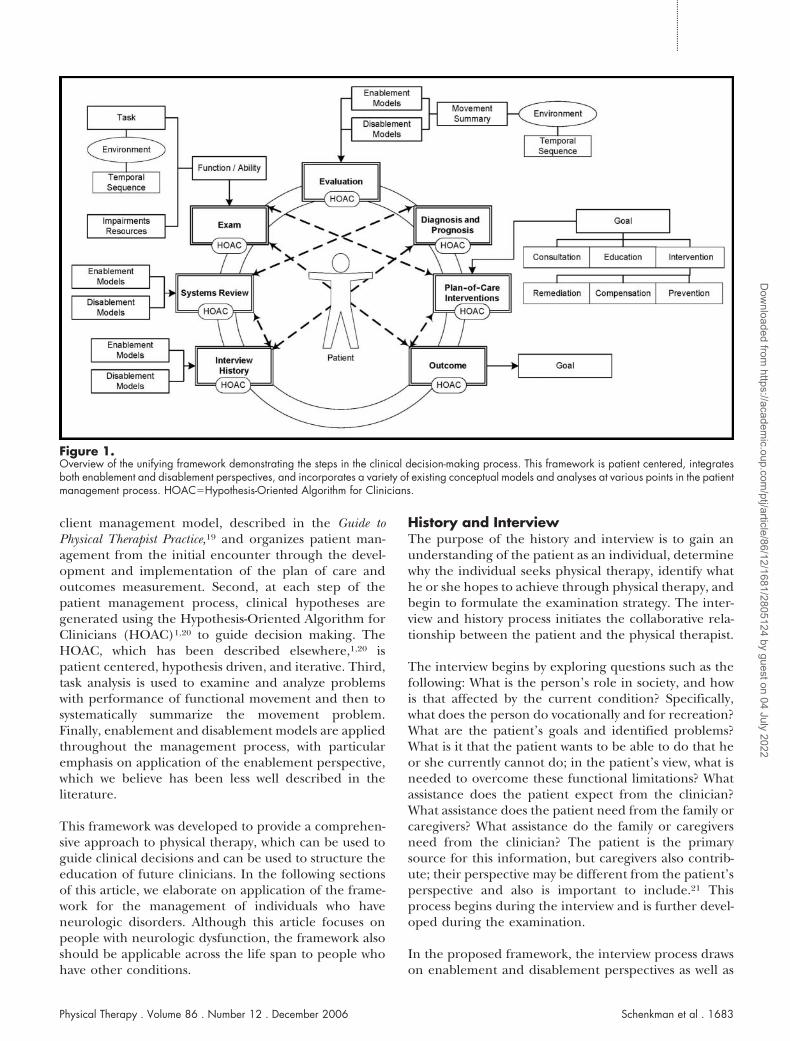
As movement specialists,43,44 it is incumbent upon phys-ical therapists to analyze movement. Task analysis(Fig. 2) is the route through which the physical therapistcarries out this central aspect of physical therapist prac-tice. Indeed, task analysis is one of the skills that definesthe physical therapist, and therefore synthesizes manyof the skills taught throughout the physical therapycurriculum.
In our framework, we propose a systematic approach totask analysis, based on work of Gentile45 and of Hedmanand colleagues.46,47 These 2 approaches to task analysiswere chosen because they are global in that they areapplicable to any task and because they give a compre-hensive description of task performance that is sufficientfor designing the plan of care. For specific tasks, thisinformation can be augmented by drawing from thegrowing body of available literature focused on move-ment analysis of particular tasks (see Shumway-Cook andWoollacott48 for examples). Specific application of theproposed task analysis is outlined below.
Task and environment. Performance of a task can varysubstantially, depending on the conditions under whichit is performed.49 For this reason, it is important toexamine tasks under conditions comparable to those in whichthe individual typically functions. Tasks can be described orcategorized in many ways. In the proposed model, thetask and environment are categorized as follows, basedon 4 conditions adapted and simplified from the work ofGentile.45 Two variables are manipulated: the individualand the environment. The 4 task and environmentcategories that we suggest using are:
(1) Stationary individual in a stationary environment(eg, sitting quietly on a treatment mat in a quiettreatment area).
(2) Moving individual in a stationary environment(eg, walking in a quiet treatment area).
(3) Stationary individual in a moving environment(eg, standing still in a busy clinic environment).
(4) Moving individual in a moving environment(eg, walking in a busy clinic environment).
We suggest that the first step in task analysis, then, is tocategorize the tasks included in the examination into 1of these 4 categories.
Other terms describing task attributes also may be usefulto consider as the clinician performs the systematic taskanalysis. For example, tasks can be categorized as dis-crete with a recognizable beginning and end (eg, com-ing from a standing position to a sitting position),continuous with no discernable beginning or end(eg, walking), or serial with discrete movements per-formed sequentially (eg, coming from sitting in anarmchair to standing, walking, turning, and sitting at thekitchen table).48(p5)
To categorize tasks using this simplified version ofGentile’s taxonomy,45 we consider all of the relevantattributes of the task and the environment that go intothe completion of the task. Included are considerationssuch as the support surface (eg, height, compliance),base of support, lighting, use of arms, and assistivedevices. For example, walking on the beach with a caneis very different in terms of environment and taskperformance than walking in the physical therapy gym;the relevant sensory, motor, perceptual, and cognitiveissues must be taken into account.
Categorization of the task and environment as we pro-pose provides critical information regarding the types oftasks and environmental conditions under which apatient may be experiencing difficulty with functional
Figure 2.The elements of task analysis. The environment and temporal sequenceare 2 elements of the task analysis that are applicable to all tasks.Strategies and phases of movement, elements that are task specific, mayadd useful information to the systematic task analysis.
1688 . Schenkman et al Physical Therapy . Volume 86 . Number 12 . December 2006
Dow
nloaded from https://academ
ic.oup.com/ptj/article/86/12/1681/2805124 by guest on 04 July 2022
abilities during daily activities. However, clinicians alsoneed to identify where within performance of the task thedifficulty occurs. For this purpose, we propose the use ofa temporal sequence to analyze the movements thatcomprise the task as outlined by Hedman and col-leagues.46,47 It is important to note that, as with the workof Gentile,45 we are highlighting selective aspects of theirwork.
Temporal sequence. Hedman and colleagues46,47 pro-posed that task analysis can be conducted by consideringthe temporal sequence of movements that comprise thetask. Use of this approach directs clinical decision mak-ing. Applying their concepts to our model, we ask thefollowing questions:
• What is the problem with completing the task?• Where along the movement continuum does the
problem interfere with function?• What are the underlying determinants of the
problem?• How do we intervene?
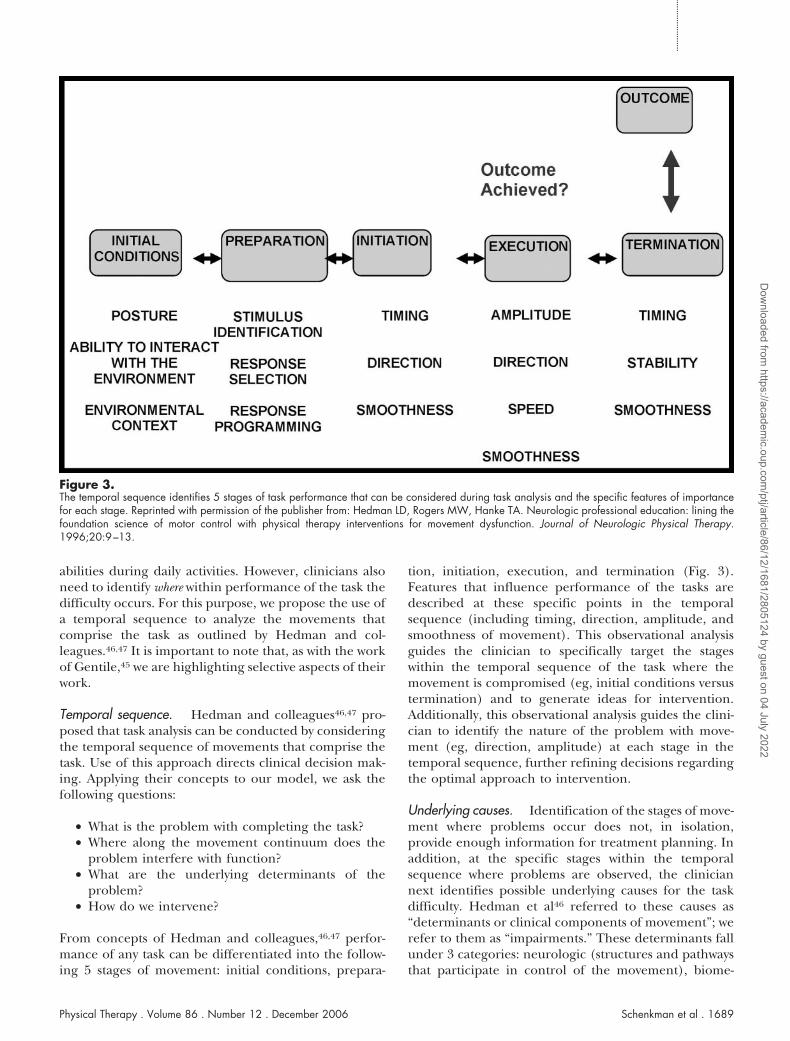
From concepts of Hedman and colleagues,46,47 perfor-mance of any task can be differentiated into the follow-ing 5 stages of movement: initial conditions, prepara-
tion, initiation, execution, and termination (Fig. 3).Features that influence performance of the tasks aredescribed at these specific points in the temporalsequence (including timing, direction, amplitude, andsmoothness of movement). This observational analysisguides the clinician to specifically target the stageswithin the temporal sequence of the task where themovement is compromised (eg, initial conditions versustermination) and to generate ideas for intervention.Additionally, this observational analysis guides the clini-cian to identify the nature of the problem with move-ment (eg, direction, amplitude) at each stage in thetemporal sequence, further refining decisions regardingthe optimal approach to intervention.
Underlying causes. Identification of the stages of move-ment where problems occur does not, in isolation,provide enough information for treatment planning. Inaddition, at the specific stages within the temporalsequence where problems are observed, the cliniciannext identifies possible underlying causes for the taskdifficulty. Hedman et al46 referred to these causes as“determinants or clinical components of movement”; werefer to them as “impairments.” These determinants fallunder 3 categories: neurologic (structures and pathwaysthat participate in control of the movement), biome-
Figure 3.The temporal sequence identifies 5 stages of task performance that can be considered during task analysis and the specific features of importancefor each stage. Reprinted with permission of the publisher from: Hedman LD, Rogers MW, Hanke TA. Neurologic professional education: lining thefoundation science of motor control with physical therapy interventions for movement dysfunction. Journal of Neurologic Physical Therapy.1996;20:9–13.
Physical Therapy . Volume 86 . Number 12 . December 2006 Schenkman et al . 1689
������
������
������
�����
Dow
nloaded from https://academ
ic.oup.com/ptj/article/86/12/1681/2805124 by guest on 04 July 2022

chanical (referring to structure and properties of mus-cles, joints, and soft tissue), and behavioral (referring tocognitive, motivational, perceptual, and emotionalaspects). These authors acknowledged that not all deter-minants can be identified by observing the patient’s taskperformance. However, 2 aspects of the determinantscan be considered as the patient is observed: (1) thepossible underlying sensory, motor, and musculoskeletalimpairments and (2) the synergistic coordination ofgroups of muscles during performance of tasks. These 2aspects are discussed below.
Determinants (impairments) are considered at eachstage in the temporal sequence of the task to guidedecisions regarding which impairments to examine indetail. Identification of the contributing impairmentseventually helps the clinician to determine optimalinterventions. For example, if force production is one ofthe main causes of difficulty with the execution stageduring the sitting-to-standing activity, it may be necessaryto include interventions that improve force production.
Analysis of individual impairments in isolation may onlypartially explain difficulty with task performance. Forexample, just because a muscle can fire, does not meanthat it will fire in the appropriate synergistic combina-tion during performance of a task. Appropriate synergis-tic firing of muscles can be problematic for any patientand can be of particular concern for those with under-lying neurologic dysfunction. For this reason, it can beimportant to examine synergistic coordination of musclegroups.
The coordination of synergistic groups of muscles hassome overlap with Hedman and colleagues’ concept ofdeterminants of movement,46,47 but goes beyond thoseconcepts. From a kinesiological perspective, purposeful,functional movement is accomplished by coordinationof muscle groups throughout the body. Included areprime movers, secondary movers, synergists (helpingand stabilizing), and whole-body stabilizers.50 With neu-rologic injury, appropriate coordination of these variousmuscle groups is frequently disrupted. At times, individ-uals have the ability to produce adequate force whenmuscles are examined in isolation, but they are unable toproduce force in appropriate synergistic combinationsduring functional activities. Conversely, it may be possi-ble to produce force in a muscle group only duringwhole-body movements (or in combination with othermuscle groups) but not during isolated limb or jointmovements. Thus, examination of force production inisolation may not be adequate to fully identify theunderlying causes of movement dysfunction. When pat-terns of movement appear inappropriate or inefficientfor the task, the clinician can use observational andmanual skills to determine which muscles within a
synergistic combination are likely participating andwhich are not. This important part of the analysis ofmovement has not received much attention in recentliterature and, as a consequence, may be overlooked.
The coordination of synergistic activity can be analyzedin a systematic fashion, drawing from principles ofbiomechanics and kinesiology, beginning with the abilityto stabilize against gravity, move while in relativelysupported positions (eg, recumbent, sitting), and movewhile in relatively unsupported positions (eg, standing),and progressing to the coordination of complex transi-tional movements (eg, walking, reading). Results of theanalysis of synergistic coordination can guide the clini-cian in making decisions about which aspects of thecoordination of synergistic activity to emphasize withinthe intervention (ie, the ability to stabilize, shift weightwhile remaining stable, shift weight while in less stablepositions, or coordinate complex transitional move-ments). The clinician determines whether problemswith synergistic coordination are observed at only one orat several of the following points in the temporalsequence: initiation, execution, and termination of themovement.
In summary, on completion of this systematic task anal-ysis as we propose, the clinician can identify the task andenvironmental conditions under which the patient hasdifficulty, identify the stages in the temporal sequence ofmovement where the difficulty is most evident, andhypothesize about the underlying determinants of thedifficulty. The underlying determinants may includeimpairments (eg, force production, coordination) aswell as coordination of synergistic groups of muscles.This proposed approach to task analysis is generic in thatit can be used with any patient for analyzing perfor-mance of any task.
The clinician can augment this generic analysis of taskperformance by drawing from the extensive body ofliterature that is task specific. This task-specific literaturefocuses around strategies of task performance. The term“strategies” refers to those motor patterns that are usedto accomplish the task, including how a person organizessensory and perceptual information.48(p123) Strategiesprovide an overall description of the way the task isperformed. Strategies have been described for a numberof important activities under a variety of environmentaland task conditions. For some of these tasks, strategiesare broken down into component parts or phases(eg, sit to stand,51 reach and grasp52) or into neuro-physiological descriptions.53 The following examples areprovided to illustrate this point, but are by no meanscomprehensive.
1690 . Schenkman et al Physical Therapy . Volume 86 . Number 12 . December 2006
Dow
nloaded from https://academ
ic.oup.com/ptj/article/86/12/1681/2805124 by guest on 04 July 2022

Phases have been described by a number of authors forwhole-body activities (eg, gait,54–56 sit to stand51) and forupper-extremity reaching tasks.52 Strategies that are usedby healthy individuals of various ages have beendescribed as typical for getting up from the floor orbed.57–59 These and other approaches to stages andstrategies can be used to focus the clinician’s observationand analysis of these specific tasks. As another example,when working with individuals who have balance dys-function associated with vestibular damage, identifica-tion of sensory organization strategies may be critical fordesigning effective interventions.60–62 When workingwith an individual after a cerebrovascular accident, itmay be helpful to determine whether the individualtransitions from a sitting position to a standing positionat a fast speed, utilizing momentum (momentum strat-egy), or moves at a slow speed, relying primarily onlower-extremity force (stabilization strategy).63
Examination at the Level of ImpairmentsWhether the clinician begins with task analysis or withimpairment testing, at some point in the examination,the clinician may need to test specific impairments. Aswith the systems review, examination of impairments candraw on a variety of standard tests and measures(eg, reflexes, range of motion, muscle performance,sensory integrity), many of which are well articulated inthe Guide to Physical Therapist Practice.19 Additionally,many resources are available to direct the clinician toexamine specific impairments.64,65
SummaryTo summarize, task analysis and impairment testing areused by clinicians to perform the patient examination.Although the clinician can chose either entry point intothe examination, task analysis, in our opinion, is anessential component of the process. Task analysisinforms the general approach to intervention as well asthose specific elements that will be incorporated into theplan of care. This process is further elaborated on in thenext section on evaluation.
EvaluationThe evaluation consists of an interpretation of findingsin order to develop a realistic plan of care. The plan ofcare is based on a synthesis of the information from all ofthe previous steps, including the patient’s goals andexpectations, task performance, the patient’s resourcesand impairments, and the medical diagnosis and prog-nosis for the condition. This synthesis results in thefollowing: (1) identification of the most important prob-lems for the patient (including both PIPs and N-PIPs),1(2) evaluation from both enablement and disablementperspectives, and (3) summary of the movement prob-lem. This information leads to the clinician’s ability to:(1) develop a diagnosis and prognosis, (2) develop
realistic goals and selection of appropriate outcomesmeasures, and (3) determine the overall approach tointervention as well as selection of the specific elementsfor the plan of care. Each of these elements is discussedbelow.
One of the first steps to the evaluation is for the clinicianto determine whether the patient’s goals are realistic andappropriate. If they are inappropriate, it is necessary forthe patient and clinician to negotiate goals that aremeaningful to the patient as well as realistic.
Next, the clinician synthesizes all available informationin relation to the patient’s main concerns, aspirations,and life circumstances. Included is an evaluation ofrelationships among all findings. This evaluation weighsthe patient’s resources and impairments and analyzesrelationships among direct and indirect effects of thedisorder.
The plan of care is patient centered and often is focusedaround task performance. Therefore, an important stepin the evaluation process is the analysis and summary ofthe movement problem. This information allows theclinician to design an overall approach to interventionand to determine how to implement the intervention.
Specifically, the analysis of the task and environmentrelationship allows the clinician to determine whetherthe patient has difficulty with all tasks in all environ-ments (eg, cannot even sit unsupported on a stationarymat), has difficulty with only more demanding tasks andenvironments (eg, moving in a moving environment), orhas some combination of these difficulties. This analysisguides the clinician’s choice of the environment inwhich to work. The nature of the task (eg, discrete versusserial) with which the patient has problems furtherinforms the clinician’s decisions regarding the specificplan of care. Identification of where the problem iswithin the temporal sequence assists in the determination ofwhether to focus the intervention on initial conditions,initiation, execution, or termination of the task (or somecombination thereof). Finally, the clinician’s choicesregarding how best to focus the intervention are guidedby identifying the underlying impairments influencingtask performance.
This overall approach to evaluation flows directly fromthe task analysis and should be fairly consistent acrossphysical therapists. For example, if the movement prob-lem for a patient occurs when the patient moves instationary environments, is most apparent during initia-tion and execution of a specified task, and relates toproblems with postural control, then the overallapproach to intervention should address each of theseissues. The specific treatment techniques that the indi-
Physical Therapy . Volume 86 . Number 12 . December 2006 Schenkman et al . 1691
������
������
������
�����
Dow
nloaded from https://academ
ic.oup.com/ptj/article/86/12/1681/2805124 by guest on 04 July 2022
vidual clinicians choose may vary, but the focus must beon the issues identified (ie, execution of tasks within astationary environment, difficulty with postural control).
In summary, at the end of the evaluation of relevant tasksand impairments, the clinician should be able to answerthe following questions:
(1) In what environmental contexts does this individualhave difficulty performing the task(s)?45
(2) Within the environmental context, what other issuesare of importance (eg, height of the chair seat, baseof support, lighting, compliance of the supportsurfaces)?
(3) How does the movement problem manifest itselfwith regard to the temporal sequence of movementsthat comprise the task?46,47
(4) Which key underlying impairments likely affect spe-cific or multiple stages within the temporalsequence of task performance?
(5) Does the patient have difficulty coordinating syner-gistic groups of muscles and under what conditions?
Using these elements of the task analysis, the cliniciandevelops a summary of the movement problem. Twoexamples that illustrate this process follow.
Task Analysis for an Individual Who Sus-tained a Cerebrovascular Accident (CVA)
A patient with a chronic CVA with residual loss ofupper-extremity control seeks physical therapy tobe able to increase the use of the affected upperextremity under a variety of environmental condi-tions. One difficulty that the therapist identifies isdifficulty with the grasp and manipulation phasesof the task of taking a tissue out of box. (Thisdifficulty was environment neutral). The therapistobserves that the initial conditions of the move-ment may not be biomechanically optimal becausethe person’s trunk alignment may subsequentlyproduce abnormal scapular movements. The exe-cution of the task is most affected because theperson does not seem to generate the force pro-duction or the precision of finger movements toremove the tissue. The compensatory trunk move-ments have created a pattern of distal upper-extremity control that interferes with achieving thetask. The therapist identifies initial conditions andexecution as the 2 phases to work on.
Task Analysis for an Individual Who HasUnilateral Vestibular Disorder
A patient 6 weeks after the onset of labrynthitisseeks physical therapy to improve his balance andbe able to resume commuting to work on the bus.The patient appears unstable when walking andclimbing stairs, often holding on to a rail ortouching the wall to maintain balance. Task anal-ysis reveals that the patient’s primary difficultiesare with execution and termination of movementin standing and walking in all environments, withthe most difficulty when he is moving in a busyenvironment. He is malaligned in standing, whichmay contribute to difficulties with balance. Thepatient appears to have difficulty stabilizing bodysegments, moving within and between postures,and coordinating between postures and move-ments to accomplish functional activities. Impair-ments in flexibility, sensory organization, andmotor control also are likely contributing to hisoverall balance problem. He is visually reliant withvery limited use of vestibular inputs for posturalcontrol. The therapist identifies execution andtermination as the 2 phases to concentrate on.
Diagnosis and PrognosisThe diagnosis and prognosis are critical to shaping thefinal plan of care. For example, a patient with a neuro-degenerative disorder may have signs and symptomsquite similar to those of a patient with a nonprogressiveneurologic injury. However, the course of the 2 disor-ders can be quite different, which has a great effect onappropriate goal setting and the overall plan of care.
Diagnosis, as performed by a physical therapist, refers tothe cluster of signs and symptoms, syndromes, or cate-gories and is used to guide the physical therapist indetermining the most appropriate intervention strategyfor each patient.19 The physical therapy profession hasgrappled for some time with the best means by which tosummarize diagnosis but has not yet reached a consen-sus for individuals with neurologic dysfunction. This hasbeen a source of discussion across the profession and inneurologic physical therapist practice in particular.66–68
As a first approach to diagnosis, the clinician can identifythe practice patterns under which this condition falls,using the Guide to Physical Therapist Practice.19 The pre-ferred practice patterns describe the elements of themanagement process for patients with specific medicaldiagnoses as well as strategies for primary preventionand reduction of risk factors. Identification of the prac-tice pattern, however, is not sufficient. As an evolvingapproach to the diagnosis made by the physical thera-pist, one of the important elements is diagnosis of themovement problem.44 Ultimately, given the role of phys-ical therapists as movement specialists, task analysis
1692 . Schenkman et al Physical Therapy . Volume 86 . Number 12 . December 2006
Dow
nloaded from https://academ
ic.oup.com/ptj/article/86/12/1681/2805124 by guest on 04 July 2022
should form the basis of the diagnosis. It is our hope thatthis framework will stimulate further discussion andeventual application of task analysis for diagnosticpurposes.
Prognosis for physical therapist practice refers to thepredicted optimal level of functional improvement thatcan be expected and the amount of time required forthe patient to reach that level.19 The preferred practicepatterns in the Guide to Physical Therapist Practice19 pro-vide a range of the number of visits required to managethis condition.19 The clinician can narrow this rangethrough analysis of literature specifically related to prog-nosis for the condition.
Prognosis represents a synthesis, based on an under-standing of the pathology, foundational knowledge,theory, evidence, experience, and examination findingsand takes into account the patient’s social, emotional,and motivational status. Included in the synthesis are thefollowing: prognosis for this disorder (eg, a patient withamyotrophic lateral sclerosis is likely to live 3–5 years),69
prognosis for neurologic recovery (eg, following stroke,initial change scores on the Fugl-Meyer examinationpredict eventual neurologic recovery),70 and prognosisfor functional change (eg, even years after an incompletespinal cord injury or stroke, some patients can makesubstantial and meaningful functional recovery.)71,72
The patient’s aspirations and PIPs determine the focusof the goals. Priorities are based on patient-identifiedpriorities for participation, functional ability, and taskperformance. Non-PIPs also are considered by the clini-cian, who should weigh the relative importance ofproblems that he or she identifies, as well as thoseidentified by family members and caregivers. Taking allof this information into account, the clinician andpatient come to an agreement regarding the mostimportant problems around which care should befocused and together establish relevant goals. Goalsmust be realistic and able to be achieved within theconstraints of the health care system.
Outcome measures reflect the patient’s goals. Outcomecan be measured in terms of qualitative changes directlyrelated to the patient’s goals (eg, patient’s goal is to feelsatisfied with his or her level of physical independence)and quantitative changes related to task performance orfunctional abilities that are interpreted as being essentialto meet the patient’s goals.
In summary, the evaluation draws on information from avariety of frameworks and models. The HOAC1,20 is usedto understand the patient’s perceived problems andrelated goals. The enablement perspective7,11 drawsattention to the patient’s resources, desires, and skills.
The disablement perspective2,8–10 is used to interpretunderlying causes of dysfunction and prognosis, and taskanalysis provides a summary of specific movement prob-lems. By synthesizing all of this information, the clinicianand patient together arrive at goals that are meaningfulto the patient and a plan of care that is appropriate tothe goals. This synthesis guides the clinician’s decisionsregarding when to use rehabilitative approaches, whento teach compensatory strategies, and when to usepreventive approaches. The HOAC1,20 guides the physi-cal therapist to continuously test and modify hypothesesused to drive intervention choices as the plan of careevolves.
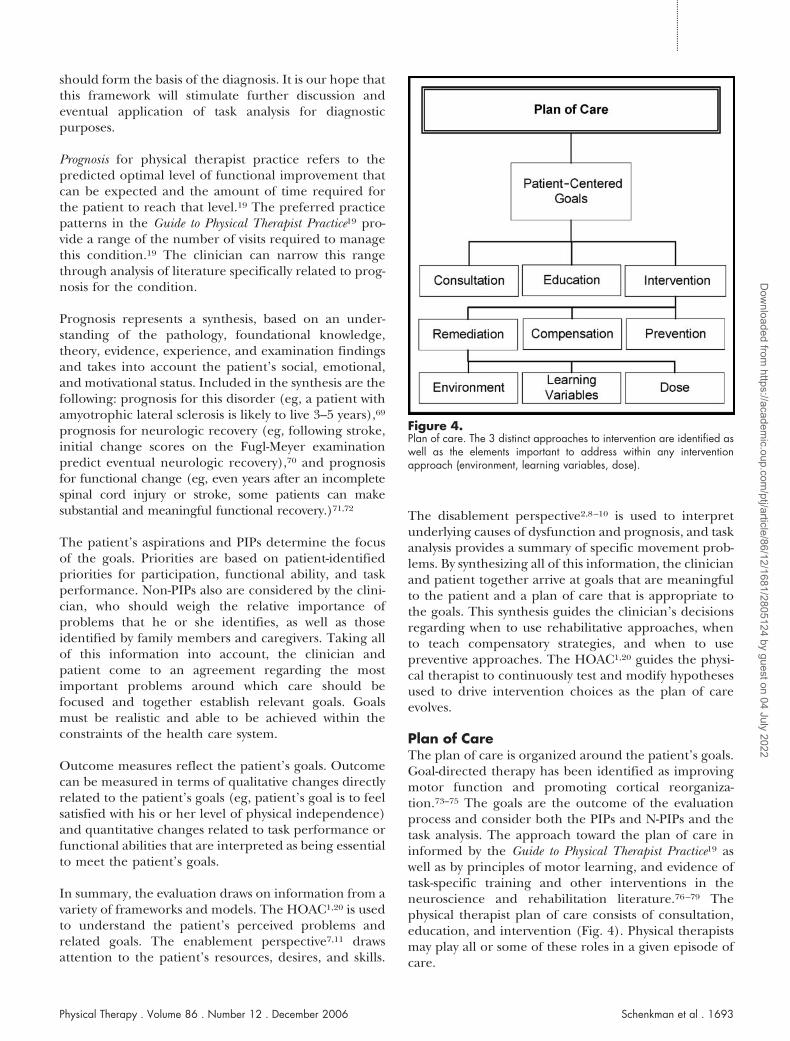
Plan of CareThe plan of care is organized around the patient’s goals.Goal-directed therapy has been identified as improvingmotor function and promoting cortical reorganiza-tion.73–75 The goals are the outcome of the evaluationprocess and consider both the PIPs and N-PIPs and thetask analysis. The approach toward the plan of care ininformed by the Guide to Physical Therapist Practice19 aswell as by principles of motor learning, and evidence oftask-specific training and other interventions in theneuroscience and rehabilitation literature.76–79 Thephysical therapist plan of care consists of consultation,education, and intervention (Fig. 4). Physical therapistsmay play all or some of these roles in a given episode ofcare.
Figure 4.Plan of care. The 3 distinct approaches to intervention are identified aswell as the elements important to address within any interventionapproach (environment, learning variables, dose).
Physical Therapy . Volume 86 . Number 12 . December 2006 Schenkman et al . 1693
������
������
������
�����
Dow
nloaded from https://academ
ic.oup.com/ptj/article/86/12/1681/2805124 by guest on 04 July 2022

To elaborate on how these roles are performed, inter-vention is organized into 3 categories: (1) remediation,(2) compensation or adaptation, and (3) prevention.The terms “remediation,” “compensation” or “adapta-tion,” and “prevention” have been used by otherauthors.48(p125) Remediation consists of enhancing skillsand resources or reversing impairments. A remediationapproach assumes that potential for change exists in thesystem and the person (eg, neurologic plasticity, abilityof muscles to become stronger or to lengthen). Use ofbody weight–supported treadmill training for a personwith a stroke80 is an example of remediation. Compensa-tion or adaptation refers to the alteration of the environ-ment or the task. This intervention approach is takenwhen it is determined that remediation is not possible.Examples include the use of a walker to widen the baseof support for a patient with balance problems, avoidingmultitask activities for patients with motor planningproblems, and the use of prism lenses for patients withvisual deficits. Prevention refers to the management ofanticipated problems (or N-PIPs in the HOAC model).An example of a preventive intervention related to theintegumentary system in a person with spinal cord injuryis the use of a combined educational program regardingthe need for frequent skin inspection with direct inter-vention for training in ischial weight relief to preventskin breakdown.
Interventions are rendered based on manipulation ofthe environment and principles of exercise and motorlearning. The specific components of the interventionare directly related to the results of the task analysis, inwhich tasks, environments, and movement problemswere identified. The therapist uses the task analysisfindings to consider the environmental context underwhich the person should practice the task in order toacquire and generalize the skill. Task-specific traininghas been advocated as the unit of therapy.48,81,82 Learn-ing variables serve as an outline for the specific treat-ment. Therapists select the appropriate schedule ofpractice and type of feedback given the goal and thestate of the learner. The final consideration is dose,which includes frequency, intensity, and duration. Doseis an important variable of therapy and is included inthe framework based on the knowledge that intensivepractice (goal-directed) is an important factor is rehabil-itation.83
A case example is provided to illustrate the process bywhich these models and frameworks are integrated forpatient care. This case example is not intended to becomprehensive, but rather is used to illustrate certainfeatures of the decision-making process, up through thedevelopment of the initial plan of care.
Case Example
History and InterviewMr C was an 88-year-old man who sought physicaltherapy following a diagnosis of PD. He lived in a lifecare community with his wife of 60 years. He was thepresident of a company and drove himself to the officeevery day, although his son effectively ran the company.
Mr C reported that he was diagnosed with PD approxi-mately a year previously and that since that time every-thing has become more difficult for him, takes time, andis “just plain slow.” He traversed the length of his office(36.6 m [120 ft]) several times daily, and this was a slowprocess. He had severe osteoarthritis, especially of theknees and lumbar spine. Getting up from the seatedposition could be quite painful, and the crepitus wasloud enough to hear from several feet away. Getting inand out of cars was difficult (“a contortionist activity”).When he returned from the office, he ate dinner andwent to bed by 7:30 pm.
On probing by the clinician, Mr C reported that he hasdifficulty with balance control on uneven surfaces andthat, when walking from his apartment to the elevator,he uses the walls for support. He reported frequent nearfalls, which he indicated tended to occur in the morn-ing. He also reported difficulty getting out of the bed inthe morning. Mr C’s goal in seeking treatment was to beable to function more easily, including the ability tocomplete his daily activities more efficiently, with lesspainful knees, and with greater stability.
At present, Mr C’s medical management includedcarbidopa-levodopa for the PD. He reported that hissymptoms did not vary according to time of dosage;therefore, it would not be necessary to plan the inter-vention around his medication schedule. He also hadongoing treatment for the osteoarthritis, including ibu-profen daily and injections of hyaline G-F 20 every 4months.
The clinician summarized Mr C’s history and interviewfrom both enablement and disablement perspectives(Fig. 5). From the enablement perspective, it was impor-tant to assess his roles, the skills that he needs to fulfillthese roles, and his resources. From the disablementperspective, it was important to assess those factors thatlimited his ability to fulfill his roles and to identifypotential contributing impairments.
Systems ReviewBased on the history and interview, as well as knowledgeof PD, the clinician determined choices and the ratio-nale for the systems review. Two tasks were included: bedmobility and sit to stand. These tasks were chosen both
1694 . Schenkman et al Physical Therapy . Volume 86 . Number 12 . December 2006
Dow
nloaded from https://academ
ic.oup.com/ptj/article/86/12/1681/2805124 by guest on 04 July 2022

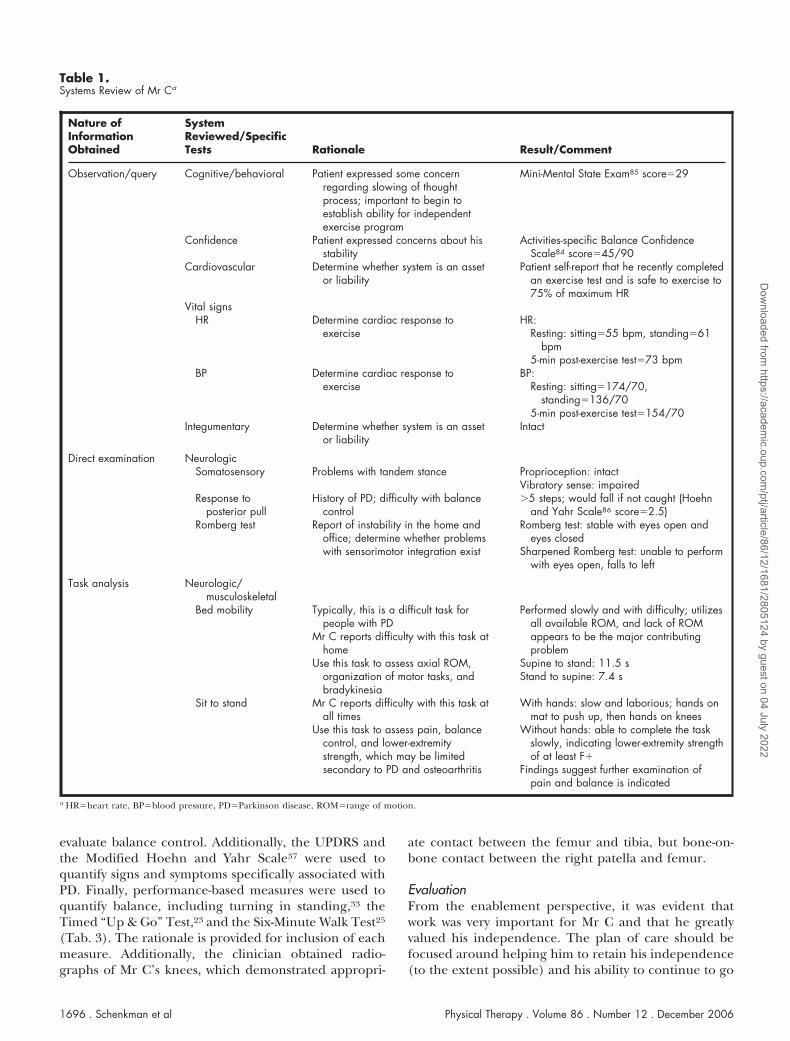
because they were problematic for Mr C and becausethey could be used to assess trunk range of motion andlower-extremity strength and for motor planning. TheActivities-specific Balance Confidence (ABC) Scale84 wasused to quantify confidence, given his report of instabil-ity, and to identify other areas that would be importantto examine. The Mini-Mental State Exam85 was used toquantify the cognitive/behavioral system, and theHoehn and Yahr Scale86 was used to quantify response toposterior pull. Rationale for choices and results of thesystems review are provided in Table 1.
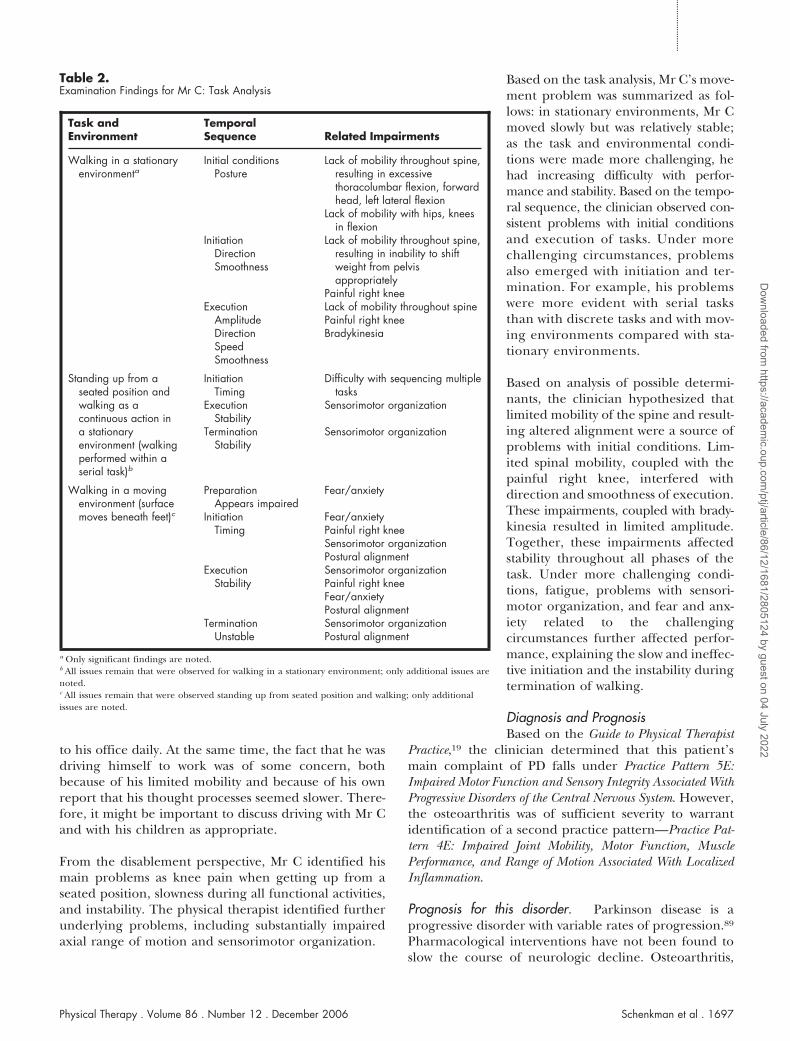
ExaminationThe examination strategy was based on Mr C’s goals aswell as the findings from the systems review. He reportedfunctional problems due to difficulty with bed mobility,coming from a sitting position to a standing position,and walking. Therefore, the examination strategyfocused on understanding the causes for difficulty withthese functional activities. The clinician chose to beginthe examination using task analysis. The 3 tasks wereanalyzed in detail and under a variety of environmentaland task conditions, which were made progressivelymore difficult to elicit Mr C’s underlying difficulty withfunctional movement. Findings are presented in Table 2.
The task of walking is used to illustrate the application ofthe models and frameworks. Walking first was examinedin a quiet clinic area (stationary environment). The taskthen was made more challenging by asking Mr C to walkin context of a serial task. He was asked to stand up froma seated position and walk to a black mat. Walking also
was made more challenging by asking Mr C to walk in anenvironment in which the surface was moving. This wasaccomplished by having Mr C walk across a black matthat covered large stones and foam (the support surfaceshifted under his weight). Finally, Mr C walked in a busyarea with people passing by quickly and unexpectedly(moving environment). The patient’s typical perfor-mance is described below.
Initial conditions revealed that he was consistently inexcessive thoracolumbar flexion, with some asymmetry(lateral flexion to the right). Initiation was typically in thesagittal plane only, without appropriate movement incoronal plane to initiate gait. Notably, preparationappeared normal, and initiation was not delayed(ie, there was no evidence of akinesia). Executionrevealed the following: amplitude was low (eg, smallsteps, small base of support), direction typically was inthe sagittal plane without shifting of weight from thepelvis and without transverse-plane movement of thethorax relative to the pelvis, and speed was slow. Termi-nation was stable in less-demanding situations, but he wasunstable in moving environments and when tasks wereperformed serially. Findings from the task analysis forwalking are summarized in Table 2.
The clinician next examined several impairments basedon hypotheses formed during the task analysis andmeasured performance based on functions of impor-tance for Mr C (Tab. 3). The visual analog scale87 wasused to assess knee pain, and the Modified Clinical Testfor Sensory Interaction of Balance (CTSIB)88 was used to
Figure 5.The enablement and disablement perspective for Mr C. PD�Parkinson disease, ROM�range of motion.
Physical Therapy . Volume 86 . Number 12 . December 2006 Schenkman et al . 1695
������
������
������
�����
Dow
nloaded from https://academ
ic.oup.com/ptj/article/86/12/1681/2805124 by guest on 04 July 2022
evaluate balance control. Additionally, the UPDRS andthe Modified Hoehn and Yahr Scale37 were used toquantify signs and symptoms specifically associated withPD. Finally, performance-based measures were used toquantify balance, including turning in standing,33 theTimed “Up & Go” Test,23 and the Six-Minute Walk Test25
(Tab. 3). The rationale is provided for inclusion of eachmeasure. Additionally, the clinician obtained radio-graphs of Mr C’s knees, which demonstrated appropri-
ate contact between the femur and tibia, but bone-on-bone contact between the right patella and femur.
EvaluationFrom the enablement perspective, it was evident thatwork was very important for Mr C and that he greatlyvalued his independence. The plan of care should befocused around helping him to retain his independence(to the extent possible) and his ability to continue to go
Table 1.Systems Review of Mr Ca
Nature ofInformationObtained
SystemReviewed/SpecificTests Rationale Result/Comment
Observation/query Cognitive/behavioral Patient expressed some concernregarding slowing of thoughtprocess; important to begin toestablish ability for independentexercise program
Mini-Mental State Exam85 score�29
Confidence Patient expressed concerns about hisstability
Activities-specific Balance ConfidenceScale84 score�45/90
Cardiovascular Determine whether system is an assetor liability
Patient self-report that he recently completedan exercise test and is safe to exercise to75% of maximum HR
Vital signsHR Determine cardiac response to
exerciseHR:
Resting: sitting�55 bpm, standing�61bpm
5-min post-exercise test�73 bpmBP Determine cardiac response to
exerciseBP:
Resting: sitting�174/70,standing�136/70
5-min post-exercise test�154/70Integumentary Determine whether system is an asset
or liabilityIntact
Direct examination NeurologicSomatosensory Problems with tandem stance Proprioception: intact
Vibratory sense: impairedResponse to
posterior pullHistory of PD; difficulty with balance
control�5 steps; would fall if not caught (Hoehn
and Yahr Scale86 score�2.5)Romberg test Report of instability in the home and
office; determine whether problemswith sensorimotor integration exist
Romberg test: stable with eyes open andeyes closed
Sharpened Romberg test: unable to performwith eyes open, falls to left
Task analysis Neurologic/musculoskeletal
Bed mobility Typically, this is a difficult task forpeople with PD
Mr C reports difficulty with this task athome
Use this task to assess axial ROM,organization of motor tasks, andbradykinesia
Performed slowly and with difficulty; utilizesall available ROM, and lack of ROMappears to be the major contributingproblem
Supine to stand: 11.5 sStand to supine: 7.4 s
Sit to stand Mr C reports difficulty with this task atall times
Use this task to assess pain, balancecontrol, and lower-extremitystrength, which may be limitedsecondary to PD and osteoarthritis
With hands: slow and laborious; hands onmat to push up, then hands on knees
Without hands: able to complete the taskslowly, indicating lower-extremity strengthof at least F�
Findings suggest further examination ofpain and balance is indicated
a HR�heart rate, BP�blood pressure, PD�Parkinson disease, ROM�range of motion.
1696 . Schenkman et al Physical Therapy . Volume 86 . Number 12 . December 2006
Dow
nloaded from https://academ
ic.oup.com/ptj/article/86/12/1681/2805124 by guest on 04 July 2022
to his office daily. At the same time, the fact that he wasdriving himself to work was of some concern, bothbecause of his limited mobility and because of his ownreport that his thought processes seemed slower. There-fore, it might be important to discuss driving with Mr Cand with his children as appropriate.
From the disablement perspective, Mr C identified hismain problems as knee pain when getting up from aseated position, slowness during all functional activities,and instability. The physical therapist identified furtherunderlying problems, including substantially impairedaxial range of motion and sensorimotor organization.
Based on the task analysis, Mr C’s move-ment problem was summarized as fol-lows: in stationary environments, Mr Cmoved slowly but was relatively stable;as the task and environmental condi-tions were made more challenging, hehad increasing difficulty with perfor-mance and stability. Based on the tempo-ral sequence, the clinician observed con-sistent problems with initial conditionsand execution of tasks. Under morechallenging circumstances, problemsalso emerged with initiation and ter-mination. For example, his problemswere more evident with serial tasksthan with discrete tasks and with mov-ing environments compared with sta-tionary environments.
Based on analysis of possible determi-nants, the clinician hypothesized thatlimited mobility of the spine and result-ing altered alignment were a source ofproblems with initial conditions. Lim-ited spinal mobility, coupled with thepainful right knee, interfered withdirection and smoothness of execution.These impairments, coupled with brady-kinesia resulted in limited amplitude.Together, these impairments affectedstability throughout all phases of thetask. Under more challenging condi-tions, fatigue, problems with sensori-motor organization, and fear and anx-iety related to the challengingcircumstances further affected perfor-mance, explaining the slow and ineffec-tive initiation and the instability duringtermination of walking.
Diagnosis and PrognosisBased on the Guide to Physical Therapist
Practice,19 the clinician determined that this patient’smain complaint of PD falls under Practice Pattern 5E:Impaired Motor Function and Sensory Integrity Associated WithProgressive Disorders of the Central Nervous System. However,the osteoarthritis was of sufficient severity to warrantidentification of a second practice pattern—Practice Pat-tern 4E: Impaired Joint Mobility, Motor Function, MusclePerformance, and Range of Motion Associated With LocalizedInflammation.
Prognosis for this disorder. Parkinson disease is aprogressive disorder with variable rates of progression.89
Pharmacological interventions have not been found toslow the course of neurologic decline. Osteoarthritis,
Table 2.Examination Findings for Mr C: Task Analysis
Task andEnvironment
TemporalSequence Related Impairments
Walking in a stationaryenvironmenta
Initial conditionsPosture
Lack of mobility throughout spine,resulting in excessivethoracolumbar flexion, forwardhead, left lateral flexion
Lack of mobility with hips, kneesin flexion
InitiationDirectionSmoothness
Lack of mobility throughout spine,resulting in inability to shiftweight from pelvisappropriately
Painful right kneeExecution
AmplitudeDirectionSpeedSmoothness
Lack of mobility throughout spinePainful right kneeBradykinesia
Standing up from aseated position andwalking as acontinuous action ina stationaryenvironment (walkingperformed within aserial task)b
InitiationTiming
ExecutionStability
TerminationStability
Difficulty with sequencing multipletasks
Sensorimotor organization
Sensorimotor organization
Walking in a movingenvironment (surface
PreparationAppears impaired
Fear/anxiety
moves beneath feet)c InitiationTiming
Fear/anxietyPainful right kneeSensorimotor organizationPostural alignment
ExecutionStability
Sensorimotor organizationPainful right kneeFear/anxietyPostural alignment
TerminationUnstable
Sensorimotor organizationPostural alignment
a Only significant findings are noted.b All issues remain that were observed for walking in a stationary environment; only additional issues arenoted.c All issues remain that were observed standing up from seated position and walking; only additionalissues are noted.
Physical Therapy . Volume 86 . Number 12 . December 2006 Schenkman et al . 1697
������
������
������
�����
Dow
nloaded from https://academ
ic.oup.com/ptj/article/86/12/1681/2805124 by guest on 04 July 2022

likewise, is progressive in nature. Interventions such asinjections of hyaline G-F 20 can be beneficial in reducingthe pain associated with the condition. Total kneereplacement most likely is not indicated for this man dueto his age and to the PD. Clinical experience suggeststhat patients with PD frequently experience severeincreases in symptoms following surgery.
Prognosis for functional change. Some studies90,91 sug-gest that functional change is possible. Evidence suggeststhat trunk range of motion specifically is limiting tobalance control and can improve.31,33 Mr C’s age, thelength of time that musculoskeletal changes haveexisted, and his questionable commitment and ability tocarry out a home program all may limit the extent offunctional improvement. Evidence also indicates thatchanges can occur with interventions directed towardsensorimotor organization.92 Finally, improved biome-chanics of transitioning from a sitting position to astanding position can diminish the pain that Mr Cexperiences and can slow down further degenerativeprocesses.
A number of investigations have been conducted, spe-cifically examining exercise and PD. Findings of theseinvestigations, most of which had small sample sizes,suggest that balance, gait, and overall function canimprove with a variety of interventions.90,91 The evalua-tion above indicated to the physical therapist that rangeof motion and altered alignment had a major effect on
this patient’s performance. Therefore, interventionsare specifically indicated that focus directly on theseproblems.
Finally, some studies93,94 provide guidance regardingintervention directly focused toward osteoarthritis of theknees. These studies demonstrated the effectiveness ofinterventions including fitness walking, aerobic exercise,and strength training as well as mobilization and manip-ulation of the lumbar spine, knee, and ankle.
Goals and Outcome MeasuresThe following were determined to be meaningfulchanges for Mr C: ability to conduct daily functionalactivities with less painful knees, greater stability, and lessfatigue. Goals were set that were focused around theseidentified changes. These goals were deemed to berealistic and achievable within the constraints of thehealth care system (Tab. 4).
Outcome measures were identified that reflected hisgoals and also that reflected the hypothesized steps toachieve those goals. Proposed outcome measures for MrC are shown in Table 4. The first column synthesizes hisgoals and the qualitative indicators of success. Themiddle column summarizes the analysis of necessarychanges to reach these goals and gives insight into thenecessary intervention. The last column lists the quanti-tative indicators of success, which are more specificmeasures that are related to his goals.
Table 3.Examination Findings for Mr C: Impairments and Outcome Measuresa
Measures Rationale Findings
ImpairmentPain (visual analog scale, 0–10)85 Knee pain may be limiting function, provides baseline
data for future comparisonKnee pain during sit-to-stand
task�4Functional axial rotation33 Loss of axial mobility may be limiting function,
provides baseline data for future comparisonRight: X�82.5°, SD�3.5°Left: X�87.5°, SD�3.5°
Modified CTSIB88 Allows for further evaluation of problems withbalance control, findings will inform approach tointervention
On foam, eyes open�20 sOn foam, eyes closed�unable
Summary measureUnified Parkinson’s Disease Rating Scale37 Reviews impairments and functional limitations
associated with PD (combination of directexamination and self-report), 0�no problems
Overall score�44.5/124ADL subscale score�17/52Motor subscale score�27/56Mentation�0/16
Performance-based measuresFunctional Reach Test22 Outcome measure for standing balance control 15.2 cm (6 in)360° turn33 Outcome measure chosen due to difficulty associated
with PD in making turns while standingRight: 14 steps, 6.4 sLeft: 14 steps, 6.5 s
Six-Minute Walk Test25 Outcome measure will be interpreted based onendurance, pain, bradykinesia
175.6 m (576 ft)
Timed “Up & Go” Test (with hands)23 Outcome measure will be interpreted in context ofbradykinesia, stability, and knee pain; assesses fallrisk
31.6 s
a CTSIB�Modified Clinical Test for Sensory Interaction of Balance, PD�Parkinson disease, ADL�activities of daily living.
1698 . Schenkman et al Physical Therapy . Volume 86 . Number 12 . December 2006
Dow
nloaded from https://academ
ic.oup.com/ptj/article/86/12/1681/2805124 by guest on 04 July 2022

Implications for Treatment Planning and theInitial Plan of CareTaking all of this information into account, it wasdeemed important to work with Mr C in progressivelymore demanding environments (moving support sur-faces and people moving around him). It also wouldbe important to use tasks of increasing complexity(eg, serial versus discrete tasks). The focus of these tasksshould be on improving range of motion and posture inorder to improve the initial conditions, execution, andtermination of task performance.
Based on a full analysis of Mr C’s problems, their underly-ing causes, and overall prognosis, a combined interventionapproach was recommended that includes remediation,compensation, and prevention. To provide adequate phys-iological support for function, it would be important toimprove trunk range of motion to the extent possible(remediation) and to assist Mr C to use more biome-chanically favorable strategies for the sitting-to-standingtask (remediation), thereby lessening the demand on hisknees and decreasing the pain. Clinical experiencesuggests that exercises for trunk range of motion shouldbe practiced in stationary environments to allow Mr C tofocus on range of motion. Improved transitioning froma sitting position to a standing position should be practicedfrom higher chair seats with a firm surface initially to workon the organization of the task and moving to progressivelylower seats and less firm surfaces.
Improved sensorimotor organization also was needed toprovide Mr C with greater stability while moving instanding positions (remediation). Sensorimotor organi-zation should be practiced in progressively moredemanding environments (eg, standing on foam witheyes open, then eyes closed; walking across a moving
surface) and with progressively more demanding tasks(eg, walking in the context of serial tasks).
Compensatory strategies also were indicated to assist MrC with his endurance and to protect his knees. Forexample, he should be encouraged to use a cane whilewalking and to obtain an electric tri-cart for locomotionover longer distances (eg, from his apartment to hisparking space). He should be encouraged to have adriver take him to and from his office.
Finally, preventive strategies were important both inlight of the PD and the osteoarthritis. With PD (as well asincreasing age), Mr C was at risk for further loss of rangeof motion. An exercise program was indicated to retardthese further losses. Prevention of further damage to theknees and back is needed (eg, the use of the tri-cart or acane), and general conditioning is important to retainoverall health and wellness.95
Summary of the Framework andIts ApplicationA framework is proposed to guide physical therapistpractice and to provide a structure for teaching clinicaldecision making to future clinicians. The frameworkintegrates enablement and disablement perspectives andhypothesis generation and refinement at each step ofpatient care, and it incorporates systematic task analysisfor examination, evaluation, and intervention. The pro-cess is cyclical and iterative. The framework is illustratedusing a case example.
It is important to note that this framework is not meantto be prescriptive in nature. That is, the order andemphasis of application of the elements of the frame-work depend on factors such as the clinician’s level of skill,
Table 4.Proposed Outcome Measures for Mr C
Patient-Desired Outcome Hypothesized Necessary Changes Indicators
Sit to stand with less pain, greater speedand stability
Improved stability and speed Timed “Up & Go” Test, change �10 s
Less pain Visual analog scale for knee pain,change ��3
Improved axial mobility and mechanics Functional axial rotation change, �7°Anterior excursion of lumbar spine/pelvis
Stable and safe for all tasks Improved balance control No reported loss of balance in morningIncreased capacity for balance controlFunctional Reach Test, change,
�1.27 cm (0.5 in)Improved sensory processing Stable on foam, eyes closed �20 sCompensation for loss of vibratory sense,
sensory processingAppropriate use of caneUse of electric tri-cart for distances
Overall physical improvement Adopt and adhere to appropriateexercise program
Self-report of improved well-beingSelf-report of increased exercise habits
Physical Therapy . Volume 86 . Number 12 . December 2006 Schenkman et al . 1699
������
������
������
�����
Dow
nloaded from https://academ
ic.oup.com/ptj/article/86/12/1681/2805124 by guest on 04 July 2022

experience, and preferred choices. However, the elementsthat are included are meant to be comprehensive.
Many of the elements of this framework are familiar andused with increasing frequency in both clinical andeducational settings (eg, Guide to Physical Therapist Prac-tice,19 disablement models8,9). This framework differsfrom prior work in that we propose that other criticalelements also be included (eg, task analysis, a patient-centered enablement approach, algorithms for makingdecisions). In particular, we propose that task analysisintegrates the entire framework and is critical for effec-tive decision making in the clinic. Such a systematicapproach as we describe should be emphasized in theprocess of educating physical therapists.
It also is important to note that this framework isproposed as a working document. The framework willcontinue to evolve as the scientific basis for movementanalysis and rehabilitation evolves. Additionally, theframework should be evaluated and refined by applyingit to clinical decision making across a wide variety ofdiagnostic conditions and populations, including thosewith non-neurologic disorders. For example, focusgroups can be used to examine the utility of this approachfor structuring neurologic physical therapist education,and case analyses can be used to test the clarity and utilityof the approach for patient management.
The complete framework, depicted in Figure 1, is arepresentation of actual clinical practice for many expe-rienced clinicians. By building from simple principles tothe entire framework, experienced clinicians and educa-tors can use this framework to assist students and noviceclinicians to better understand and incorporate all aspectsof decision making necessary for effective care of patients.This framework also provides the experienced clinicianwith a structure for articulating intuitive decisions.
References1 Echternach JL, Rothstein JM. Hypothesis-oriented algorithms. PhysTher. 1989;69:559–564.
2 Schenkman M, Butler RB. A model for multisystem evaluation,interpretation and treatment of individuals with neurologic dysfunc-tion. Phys Ther. 1989;69:538–547.
3 Schenkman M, Donovan J, Tsubota J, et al. Management of individ-uals with Parkinson’s disease: rationale and case studies. Phys Ther.1989;69:944–955.
4 Scheets PK, Sahrmann SA, Norton JB. Diagnosis for physical therapyfor patients with neuromuscular conditions. Neurology Report. 1999;23:158–169.
5 Schenkman M, Bliss S, Day L, et al. A model for management ofpatients with neurological dysfunction: update and case analysis.Neurology Report. 1999;23:145–157.
6 Bello-Haas VD. A framework for rehabilitation for neurodegenera-tive diseases: managing progression and maximizing quality of life.Neurology Report. 2002;26:115–129.
7 Quinn L, Gordon J. Functional Outcomes Documentation for Rehabilita-tion. Philadelphia, Pa: WB Saunders Co; 2003:6–7.
8 International Classification of Impairments, Disabilities, and Handicaps: AManual of Classification Relating to the Consequences of Disease. Geneva,Switzerland: World Health Organization; 1980.
9 Nagi S. Some conceptual issues in disability and rehabilitation. In:Sussman M, ed. Sociology and Rehabilitation. Washington, DC: AmericanSociological Association; 1965:100–113.
10 Verbrugge LM, Jette AM. The disablement process. Soc Sci Med.1994;38:1–14.
11 Enabling America: Assessing the Role of Rehabilitation Science and Engi-neering. Washington, DC: National Academies Press; 1997.
12 Gordon J. A top-down model for neurologic rehabilitation. Presen-tation at the III STEP Symposium on Translating Evidence IntoPractice: Linking Movement Science and Intervention; July 15–21,2005; Salt Lake City, Utah.
13 International Classification of Functioning, Disability and Health: ICF.Geneva, Switzerland: World Health Organization; 2001.
14 Jette AM. Toward a common language for function, disability, andhealth. Phys Ther. 2006;86:726–734.
15 Platt F, Gasper DL, Coulehan JL, et al. “Tell me about yourself”: Thepatient-centered interview. Ann Intern Med. 2001;134:1079–1085.
16 Smyth FS. The place of humanities and social sciences in educationof physicians. J Med Educ. 1962;37:495–499.
17 Kravitz RL, Callahan EJ, Paterniti D, et al. Prevalence and sources ofpatients’ unmet expectations for care. Ann Intern Med. 1996;125:730–737.
18 Delbanco TL. Enriching the doctor-patient relationship by invitingthe patient’s perspective. Ann Intern Med. 1992;116:414–418.
19 Guide to Physical Therapist Practice. 2nd ed. Phys Ther. 2001;81:9–746.
20 Rothstein JM, Riddle DL, Echternach JL. The Hypothesis-OrientedAlgorithm for Clinicians II (HOAC II): a guide for patient manage-ment. Phys Ther. 2003;83:455–470.
21 Cutson TM, Zhu C, Whetten K, Schenkman M. Observations ofspouse-patient dyads with Parkinson’s disease over five years. Journal ofNeurologic Physical Therapy. 2004;28:122–128.
22 Duncan PW, Studenski S, Chandler J, Prescott B. Functional reach:predictive validity in a sample of elderly male veterans. J Gerontol.1992;47:M93–M98.
23 Shumway-Cook A, Brauer S, Woollacott M. Predicting the probabil-ity for falls in community-dwelling older adults using the Timed Up &Go Test. Phys Ther. 2000;80:896–903.
24 Shumway-Cook A, Baldwin M, Polissar NS, Gruber W. Predictingthe probability for falls in community-dwelling older adults. Phys Ther.1997;77:812–819.
25 Enright P, Sherrill D. Reference equations for the six-minute walkin healthy adults. Am J Resp Crit Care Med. 1998;158:1384–1387.
26 Hughes MA, Myers BS, Schenkman ML. The role of strength inrising from a chair in the frail elderly. J Biomech. 1996;12:1509–1513.
27 Schenkman M, Hughes MA, Samsa G, Studenski SA. The relativeimportance of strength and balance in the performance of sitting tostanding by functionally impaired older individuals. J Am Geriatr Soc.1996;44:1441–1446.
28 Eriksrud O, Bohannon RW. Relationship of knee extension force toindependence in sit-to-stand performance in patients receiving acuterehabilitation. Phys Ther. 2003;83:544–551.
1700 . Schenkman et al Physical Therapy . Volume 86 . Number 12 . December 2006
Dow
nloaded from https://academ
ic.oup.com/ptj/article/86/12/1681/2805124 by guest on 04 July 2022

29 Lai SM, Duncan PW, Keighely J. Prediction of functional outcomesafter stroke: comparison of the Orpington Prognostic Scale and NIHStroke Scale. Stroke. 1998;29:1838–1842.
30 Macko RF, Smith GV, Dobrovolny L, et al. Treadmill trainingimproves fitness reserve in chronic stroke patients. Arch Phys MedRehabil. 2001;82:879–884.
31 Schenkman M, Morey M, Kuchibhatla M. Spinal flexibility andphysical performance of community-dwelling adults with and withoutParkinson’s disease. J Gerontol A Biol Sci Med Sci. 2000;55:M441–M445.
32 Schenkman M, Clark K, Xie T, et al. Spinal flexibility and perfor-mance of standing reach task: participants with and without Parkin-son’s disease. Phys Ther. 2001;81:1400–1411.
33 Schenkman M, Cutson TM, Kuchibhatla M, et al. A randomizedcontrolled exercise trial in patients with Parkinson’s disease. J AmGeriatric Soc. 1998;46:1207–1216.
34 Duncan PW, Goldstein LB, Matcher D, et al. Measurement of motorrecovery after stroke. outcome assessment and sample size require-ments. Stroke. 1992;23:1084–1089.
35 Wood E, Rosenbaum P. The gross motor function classificationsystem for cerebral palsy: a study of reliability and stability over time.Dev Med Child Neurol. 2000;42:292–296.
36 Woischneck D, Firsching R. Efficiency of the Glasgow OutcomeScale (GOS)-Score for the long-term follow-up after severe braininjuries. Acta Neurochirurgica Suppl. 1998;71:138–141.
37 Fahn S, Elton RL, and members of the UPDRS DevelopmentCommittee. Unified Parkinson’s Disease Rating Scale. In: Fahn S,Marsden CD, Calne D, Goldstein M, eds. Recent Developments in Parkin-son’s Disease, Volume 2. Florham Park, NJ: Macmillan HealthcareInformation; 1987:153–163.
38 Haley SM, Coster WJ, Ludlow LH, et al. Pediatric Evaluation ofDisability Inventory (PEDI): Development, Standardization and Administra-tion Manual. Boston, Mass: PEDI Research Group, New EnglandMedical Center Hospitals; 1992.
39 Russell DJ, Rosenbaum PL, Avery LM, Lane M. Gross Motor FunctionMeasure (GMFM-66 and GMFM-88) User’s Manual. London, UnitedKingdom: Mac Keith Press; 2002.
40 Nordmark E. Jarnlo G. Hagglund G. Comparison of the GrossMotor Function Measure and Pediatric Evaluation of Disability Inven-tory in assessing motor function in children undergoing selectivedorsal rhizotomy. Dev Med Child Neurol. 2000;42:245–252.
41 Palisano R, Rosenbaum P, Walter S, et al. Development and reli-ability of a system to classify gross motor function in children withcerebral palsy. Dev Med Child Neurol. 1997;39:214–223.
42 Ling SS, Fisher BE. Functional improvements using observationalmovement analysis and task specific training for an individual withchronic severe upper extremity hemiparesis. Journal of NeurologicPhysical Therapy. 2004;28:91–99.
43 Philosophical statement on diagnosis in physical therapy. In: Pro-ceedings of the House of Delegates. Washington, DC, American PhysicalTherapy Association; 1983.
44 Sahrmann SA. The Twenty-Ninth Mary McMillan Lecture: Movingprecisely? Or taking the path of least resistance? Phys Ther. 1998;78:1208–1218.
45 Gentile AM. Skill acquisition: action, movement, and neuromotorprocesses. In: Carr JH, Shepherd RB, eds. Movement Science: Foundationsfor Physical Therapy in Rehabilitation. 2nd ed. Gaithersburg, Md: AspenPublishers Inc; 2000:111–187.
46 Hedman LD, Rogers MW, Hanke TA. Neurologic professionaleducation: lining the foundation science of motor control with physi-cal therapy interventions for movement dysfunction. Journal of Neuro-logic Physical Therapy. 1996;20:9–13.
47 Hedman LD, Sullivan JE. Acute rehabilitation post stroke. In: RioloL, ed. Topics in Physical Therapy: Neurology. Alexandria, Va: AmericanPhysical Therapy Association; 2002: lesson 4.
48 Shumway-Cook A, Woollacott MH. Motor Control: Theory and PracticalApplications. 2nd ed. Philadelphia, Pa: Lippincott Williams & Wilkins;2001.
49 Shumway-Cook A, Patla AE, Stewart A, et al. Environmentaldemands associated with community mobility in older adults with andwithout mobility disabilities. Phys Ther. 2002;82:670–681.
50 Schenkman M, Rugo de Cartaya V. Kinesiology of the shouldercomplex. J Orthop Sports Phys Ther. 1987;8:438–450.
51 Janssej WG, Bussmann HB, Stam HJ. Determinants of the sit-to-stand movement: a review. Phys Ther. 2002;82:866–879.
52 Kamper DG, McKenna-Cole AN, Kahn LE, Reinkensmeyer DJ. Alter-ations in reaching after stroke and their relation to movement directionand impairment severity. Arch Phys Med Rehabil. 2002;83:702–707.
53 Runge CF, Shupert CL, Horak FB, Zajac FE. Ankle and hip posturalstrategies defined by joint torques. Gait Posture. 1999;10:161–170.
54 Wolfson L, Whipple R, Amerman P, Tobin JN. Gait assessment inthe elderly: a gait abnormality rating scale and its relation to falls.J Gerontol. 1990;45:M12–M19.
55 Winter DA. Biomechanics and Motor Control of Human Movement. 2nded. New York, NY: John Wiley & Sons Inc; 1990.
56 Perry J. Gait Analysis: Normal and Pathological Function. Thorofare,NJ: Slack Inc; 1992.
57 Cohen BG, Cardillo ER, Lugg D, et al. Description of movementpatterns of young adults moving supine from the foot to the head ofthe bed. Phys Ther. 1998;78:999–1006.
58 Ford-Smith CD, VanSant AF. Age differences in movement patternsused to rise from a bed in subjects in the third through fifth decadesof age. Phys Ther. 1993;73:300–309.
59 Marsala G, VanSant AF. Age-related differences in movementpatterns used by toddlers to rise from a supine position to erect stance.Phys Ther. 1998;78:149–159.
60 Gill-Body KM, Krebs DE, Parker SW, Riley PO. Physical therapymanagement of peripheral vestibular dysfunction: two clinical casereports. Phys Ther. 1994;74:129–142.
61 Gill-Body KM, Popat RA, Parker SW, Krebs DE. Rehabilitation ofbalance in two patients with cerebellar dysfunction. Phys Ther. 1997;77:534–552.
62 Gill-Body KM, Beninato M, Krebs DE. Relationship among balanceimpairments, functional performance and disability in subjects withvestibular hypofunction. Phys Ther. 2000;80:748–758.
63 Hughes MA, Wiener DK, Schenkman ML, et al. Chair rise strategiesin the elderly. Clin Biomech. 1994;9:187–192.
64 O’Sullivan SB, Schmitz TJ, eds. Physical Medicine and Rehabilitation:Assessment and Treatment. 4th ed. Philadelphia, Pa: FA Davis Co; 2001.
65 Umphred D, ed. Neurological Rehabilitation. 4th ed. St Louis, Mo:Mosby; 2001.
66 Sahrmann SA. Diagnosis by the physical therapist: a prerequisite fortreatment (special communication). Phys Ther. 1988;68:1303–1307.
Physical Therapy . Volume 86 . Number 12 . December 2006 Schenkman et al . 1701
������
������
������
�����
Dow
nloaded from https://academ
ic.oup.com/ptj/article/86/12/1681/2805124 by guest on 04 July 2022

67 Deutsch J. Editor’s note: Confused about physical therapy diagnosisand differential diagnosis? Journal of Neurologic Physical Therapy. 2004;28:153.
68 Sullivan KJ, Hershberg J, Howard R, Fisher BE. Neurologic differ-ential diagnosis for physical therapy. Journal of Neurologic PhysicalTherapy. 2004;28:162–168.
69 Bello-Haas VD, Kloos AD, Mitsumoto H. Physical therapy for apatient through six stages of amyotrophic lateral sclerosis. Phys Ther.1998;78:1312–1324.
70 Duncan PW, Goldstein LB, Matcher D, et al. Measurement of motorrecovery after stroke: outcome assessment and sample size require-ments. Stroke. 1992;23:1084–1089.
71 Wirz M, Zemon DH, Rupp R, et al. Effectiveness of automatedlocomotor training in patients with chronic incomplete spinal cordinjury: a multicenter trial. Arch Phys Med Rehabil. 2005;86:672–680.
72 Peurala SH, Tarkka IM, Pitkanen K, Sivenius J. The effectiveness ofbody weight-supported gait training and floor walking in patients withchronic stroke. Arch Phys Med Rehabil. 2005;86:1557–1564.
73 Nudo RJ, Wise BM, SiFuentes F, Milliken GW. Neural substrates forthe effects of rehabilitative training on motor recovery after ischemicinfarct. Science. 1996;272:1791–1794.
74 Liepert J, Bauder H, Miltner WHR, et al. Treatment-induced corti-cal reorganization after stroke in humans. Stroke. 2000;31:1210–1216.
75 Jang SH, You SH, Hallett M, et al. Cortical reorganization andassociated functional motor recovery after virtual reality in patientswith chronic stroke: an experimenter-blind preliminary study. ArchPhys Med Rehabil. 2005;86:2218–2223.
76 Halsband U, Lange RK. Motor learning in man: a review offunctional and clinical studies. J Physiol (Paris). 2006;99(4–6):414–424.
77 Dean CM, Richards CL, Malouin F. Task-related circuit trainingimproves performance of locomotor tasks in chronic stroke: a random-ized, controlled pilot trial. Arch Phys Med Rehabil. 2000;81:409–417.
78 Plautz EJ, Milliken GW, Nudo RJ. Effects of repetitive motortraining on movement representations in adult squirrel monkeys: roleof use versus learning. Neurobiol Learn Mem. 2000;74:27–55.
79 Ottawa Panel Evidence-Based Clinical Practice Guidelines for Post-Stroke Rehabilitation. Stroke Rehabilitation. 2006;13(2):1–267.
80 Sullivan KJ, Knowlton BJ, Dobkin BH. Step training with body weightsupport: effect of treadmill speed and practice paradigms on poststrokelocomotor recovery. Arch Phys Med Rehabil. 2002;83:683–691.
81 Carr JH, Shepherd RB, eds. Motor Relearning Program for Stroke.Gaithersburg, Md: Aspen Publishers Inc; 1986.
82 Carr JH, Shepherd RB. Stroke Rehabilitation: Guidelines for Exercise andTraining to Optimize Motor Skill. Newton, Mass: Butterworth-Heinemann;2003.
83 Kwakkel G, van Peppen R, Wagenaar RC, et al. Effects of aug-mented exercise therapy time after stroke: a meta-analysis. Stroke.2004;35:2529–2539.
84 Powell LE, Myers AM. The Activities-specific Balance Confidence(ABC) Scale. J Gerontol A Bio Sci Med Sci. 1995;50:M28–M34.
85 Folstein MF, Folstein SE, McHugh PR. “Mini-Mental State”: Apractical method for grading the cognitive state of patients for theclinician. J Psychiat Res. 1975;12:189–198.
86 Hoehn MM, Yahr MD. Parkinsonism: onset, progression, andmortality. Neurology. 1967;17:427–442.
87 Von Korff M, Jensen MP, Karoly P. Assessing global pain severity byself-report in clinical and health services research. Spine. 2000;25:3140–3151.
88 Horak FB. Clinical measurement of postural control in adults. PhysTher. 1987;67:1881–1885.
89 Zetusky WJ, Jankovic, J, Pirozzolo FJ. The heterogeneity of Parkinson’sdisease: clinical and prognostic implications. Neurology. 1985;35:522–526.
90 de Goede CJT, Keus SHJ, Kwakkel G, Wagenaar RC. The effects ofphysical therapy in Parkinson’s disease: a research synthesis. Arch PhysMed Rehabil. 2001;82:509–515.
91 Deane KH, Jones D, Ellis-Hill C, et al. A comparison of physiother-apy techniques for patients with Parkinson s disease [CochraneReview]. Cochrane Database Syst Rev. 2001;1:CD002815.
92 Badke MB, Shea TA, Miedaner JA, Grove CR. Outcomes afterrehabilitation for adults with balance dysfunction. Arch Phys MedRehabil. 2004;85:227–233.
93 Puett DW Griffin MR. Published trials of nonmedicinal and noninva-sive therapies for hip and knee osteoarthritis. Clin Ther. 1992;14:336–346.
94 Deyle GD, Allison SC, Matekel RL, et al. Physical therapy treatmenteffectiveness for osteoarthritis of the knee: a randomized comparisonof supervised clinical exercise and manual therapy procedures versus ahome exercise program. Phys Ther. 2005;85:1301–1317.
95 King AC, Rejeski WJ, Buchner DM. Physical activity interventionstargeting older adults: a critical review and recommendations. Am JPrev Med. 1998;15:316–333.
1702 . Schenkman et al Physical Therapy . Volume 86 . Number 12 . December 2006
Dow
nloaded from https://academ
ic.oup.com/ptj/article/86/12/1681/2805124 by guest on 04 July 2022





























