Embed Size (px)
Citation preview

Predicting Support From an Intimate Partner After aTraumatic Injury1
Natalya C. Maisel2
VA Palo Alto Health Care SystemAmy J. Rauer
Department of Human Development andFamily Studies
Auburn University
Grant N. MarshallRAND Corporation
Benjamin R. KarneyUniversity of California, Los Angeles
Support from an intimate partner predicts recovery in individuals who have surviveda traumatic injury, but not all partners are willing or able to provide support. Toaccount for support provision after a traumatic injury, both members of 58 youngcouples were interviewed shortly after one member experienced a traumatic injury.Characteristics of the situation, the support recipient, and the support provideraccounted for unique variance in support provision. Specifically, partners of traumasurvivors reported providing more support when the injury was more severe, theywere more religious, and their partners were higher in neuroticism. Contrary toexpectations, no relationship variables were significantly associated with supportprovision. Results highlight the need to examine predictors of support in real-worldcontexts.jasp_792 2044..2075
In their lifetimes, approximately 50% to 60% of individuals in the UnitedStates will experience a traumatic event, such as a life-threatening accident ora physical assault (Kessler, 2000; Kessler, Sonnega, Bromet, Hughes, &Nelson, 1995; Resnick, Kilpatrick, Dansky, Saunders, & Best, 1993). Physi-cal injuries incurred as a result of the trauma may be lifelong problems (e.g.,back pain, bones that do not heal properly), but even if these injuries heal,survivors of traumatic events are also at increased risk for hypertension,diabetes, certain types of cancer, fatigue, and other physical problems (seeLutgendorf et al., 1995). In addition to the costs to their physical health,survivors of traumatic injuries are also at risk for a number of negative
1The research described here was supported by a grant from the Fetzer Institute, awardedto Benjamin R. Karney, and by grants from the National Institute of Mental Health(R01MH56122) and the National Institute on Alcohol Abuse and Alcoholism (R01AA014246),awarded to Grant N. Marshall. The views expressed herein are not necessarily those of theDepartment of Veteran Affairs.
2Correspondence concerning this article should be addressed to Natalya C. Maisel, Centerfor Health Care Evaluation, VA Palo Alto Health Care System (152MPD), 795 Willow Road,Menlo Park, CA 94025. E-mail: [email protected]
2044
Journal of Applied Social Psychology, 2011, 41, 8, pp. 2044–2075.© 2011 Wiley Periodicals, Inc.

mental health outcomes. In particular, trauma survivors are vulnerable todepression and post-traumatic stress disorder (PTSD), and these mentalhealth consequences are associated with further challenges, such as job loss,drug use, and suicide attempts (Michaels et al., 1999; Wilson, 2007).
Although everyone who experiences a trauma is at elevated risk for thesenegative outcomes, many who are injured will recover without lasting con-sequences. One of the resources that has been most strongly associated withmental and physical recovery from a trauma is the availability of socialsupport. Individuals who experience traumatic injuries require a wide rangeof support, including assistance with daily activities and medical regimens(i.e., instrumental support), as well as validation and expressions of care andcommitment (i.e., emotional support). A meta-analysis by Brewin, Andrews,and Valentine (2000) suggested that social support is one of the largestpredictors of PTSD symptom severity that has been examined.
Those who have experienced trauma may draw upon support from avariety of sources, but adults usually draw their most significant supportfrom their intimate partners (see Dehle, Larsen, & Landers, 2001). Indeed,the presence of a supportive intimate partner has been associated withimproved coping, and physical and mental health outcomes among indivi-duals with cancer or other chronic illnesses (e.g., Cutrona, 1996; Helgeson &Cohen, 1996). Married patients with supportive spouses recover morequickly and have better mental health outcomes, compared to unmarriedpatients and patients with unsupportive spouses (e.g., Berg & Upchurch,2007; Dehle et al., 2001). Social support from friends and family does notseem to compensate for poor support from a partner (Brown & Harris, 1978;Pistrang & Barker, 1995).
Yet, even among trauma survivors who have intimate partners, there is agreat deal of variability in the amount and quality of the support thatpartners provide (e.g., Bolger, Foster, Vinokur, & Ng, 1996; Rini, Dunkel-Schetter, Hobel, Glynn, & Sandman, 2006). As Bolger et al. (1996) noted, thestress of a crisis, such as a traumatic injury or chronic illness, can overwhelmcaregivers. Researchers have pointed specifically to the deterioration of socialsupport resources that can occur after a crisis (e.g., Norris & Kaniasty, 1996).For example, individuals may have to take over household duties that theirpartners previously handled, but not all spouses are able or willing to enactthis support (e.g., Revenson & Majerovitz, 1990). To date, research hassuccessfully documented the implications of this variability, but the sourcesof variability in support after a traumatic event remain an open question. Ina situation in which the successful exchange of support can be critical for anindividual’s health and recovery, accounting for the ability of partners tosupport each other after trauma is crucial. Moreover, interventions toimprove the outcomes of survivors will be strengthened to the extent that
SUPPORT AFTER TRAUMATIC INJURY 2045

they are grounded in a clear understanding of who gets support and whoprovides support after a traumatic injury.
The goal of the research described here is to examine the antecedents ofsupportive behavior in couples within which one partner has recently suffereda traumatic injury. In pursuit of this goal, the rest of this introduction isorganized into three sections. First, we review prior research on the determi-nants of social support receipt and provision, focusing on four broaddomains: the situation, the relationship, characteristics of the support recipi-ent, and characteristics of the support provider. Second, we identify specificlimitations in the existing literature affecting its ability to generalize to sur-vivors of traumatic injury. Finally, we provide an overview of the currentstudy, which draws upon a sample of 58 recent trauma survivors and theirpartners to examine the relative influence of each of the four broad domainson support provided shortly after an injury.
Who Gets Support and Who Provides It?
Survivors of traumatic injuries need support for the behaviors necessaryfor recovery and daily living (e.g., shopping, doctors’ appointments, con-tinuing medical regimens) and for the emotional needs that can be theconsequence of trauma (e.g., need for reassurance, companionship, orvalidation). Prior research has emphasized four broad domains to accountfor who is able to provide this support and who is most likely to receive it(Dunkel-Schetter & Skokan, 1990; Hobfoll & Lerman, 1989; Shumaker &Brownell, 1984).
Qualities of the Situation
In their seminal stage model of helping, Latané and Darley (1970) pro-posed that helping is determined more strongly by the structure of the situ-ation than by individual differences and personal values (e.g., a convictionthat helping other people is important). Given the opportunity to assist astranger in need, for example, Darley and Latané (1968) found that, regard-less of the composition of the bystanders, as the number witnessing anemergency increased, helping decreased, presumably because individuals feltless responsibility to help when there were other people available to providehelp in their place. In contrast, they found that individual differences (e.g.,personality, background factors) did not predict helping.
In the context of a trauma survivor with an intimate partner, the traumasurvivor’s partner will likely feel at least some responsibility to provide
2046 MAISEL ET AL.

support. Nevertheless, Latané and Darley’s (1970) model highlights otherelements of situations that should make a difference in predicting helpingbehavior directed toward trauma survivors. Specifically, research guided bythis model has found that helping declines when the need for help is ambigu-ous, and increases when the need is clear and unmistakable (e.g., Solomonet al., 1978). For trauma survivors, the key to determining need should be theseverity of the injury. The greater the injury, the more unambiguous theneeds of the survivor, and the more their partners should be motivated toprovide support. Indeed, previous researchers have found that the perceptionof problem severity is one of the “greatest direct predictors of helping”(George, Carroll, Kersnick, & Calderon, 1998, p. 685). In both strangersituations (e.g., bystander intervention) and cases in which friends and familyprovide support, people provide more support to individuals with moresevere injuries (Dunkel-Schetter & Skokan, 1990; George et al., 1998). Forexample, Bolger et al. (1996) found that the spouses of breast cancer patientsenacted more support as the severity of the patient’s physical impairmentincreased.
Qualities of the Relationship
Whereas Darley and Latané’s (1968) original work focused primarily onhelping between strangers, most significant support takes place in the contextof close relationships (Pasch, Bradbury, & Sullivan, 1997). As researchersbegan to examine this highly salient aspect of the helping situation, it hasbecome clear that the quality of the relationship—particularly the extent towhich partners feel attached and committed to each other—should predictthe extent to which they are motivated to respond to each other’s needs forsupport (e.g., Cutrona, 1996). Indeed, there are strong social norms dictatingthat people should care for those they love in times of illness or injury (e.g.,Feeney & Collins, 2003).
Models that directly address the role of relationship quality in socialsupport (e.g., Dunkel-Schetter & Skokan, 1990; Feeney & Collins, 2003)propose that caregivers in more satisfied relationships should be more likelyto provide support to their partners. Consistent with these perspectives,researchers have generally found associations between one’s own relationshipsatisfaction and the amount of support one provides (Acitelli, 1996). Forexample, in two daily diary studies of social support, Iida and colleagues(Iida, Seidman, Shrout, Fujita, & Bolger, 2008) found that on days whenindividuals were more satisfied with their relationships, they provided moresupport to their partners. In addition, caregivers who are more satisfied withtheir relationships report more altruistic motives for providing support (e.g.,
SUPPORT AFTER TRAUMATIC INJURY 2047

motivated by feelings of love, rather than an expectation of future reward;Feeney & Collins, 2003).
Qualities of the Trauma Survivor and the Partner
Although Latané and Darley’s (1970) classic theory emphasized the situ-ation, more recent models have recognized that support in ongoing relation-ships (e.g., caring for a chronically ill partner) is likely to depend oncharacteristics of both the provider and the recipient of support (Dunkel-Schetter & Skokan, 1990; Feeney & Collins, 2003; Pasch, Bradbury, & Sul-livan, 1997). With respect to the provider, individual differences should beassociated with the ability to determine appropriate forms of support, thewillingness to provide sustained support over time, and the way the providerunderstands and makes meaning from the situation. With respect to therecipient, individual differences should be associated with how support issolicited, and responses to support. A wide range of specific individual dif-ferences have been examined in this regard, but, in general, research hasfocused on personality traits, coping styles, and personal values.
Personality traits. Neuroticism, which is defined as the general tendencyto experience and express negative affect (Watson & Clark, 1984), has beenidentified as an important moderator of responses to stressful situations (e.g.,Gunthert, Cohen, & Armeli, 1999) and as a significant predictor of conflictand stability in intimate relationships (e.g., Rogge, Bradbury, Hahlweg,Engl, & Thurmaier, 2006). It follows that neuroticism should play a rolewhen intimate partners are coping with the stress of a traumatic injury, butresearch has observed different effects for the recipient and the provider. Forexample, although neuroticism is generally associated with negative relation-ship and health outcomes, husbands higher in neuroticism tend to receivemore emotional support from their wives (Pasch, Bradbury, & Davila, 1997).
To the extent that individuals who are more accustomed to expressingnegative affect are also more comfortable asking directly for support andreassurance, more neurotic individuals who have been injured may alsoreceive more support from their partners, at least in the short term. Withrespect to the provider, however, neuroticism has been shown to impair theability to offer support (e.g., Knoll, Burkert, & Schwarzer, 2006; Pasch,Bradbury, & Davila, 1997).
Coping style. Some people are more effective than are others at copingwith stress across situations. Dunkel-Schetter and Skokan (1990) suggestedthat individuals with more developed coping skills will have more resourcesavailable to provide support to their partners in any specific situation. Inparticular, research on emotion regulation has shown that those with a
2048 MAISEL ET AL.

weaker ability to regulate their negative emotions (e.g., suppressing theiremotions, rather than addressing them directly) describe more negative expe-riences providing and receiving support during times of stress (e.g., Gross,2002).
With respect to support recipients specifically, coping styles that empha-size suppression and avoidance have been associated with greater PTSDamong trauma survivors (e.g., Bryant & Harvey, 1995), whereas styles thatfocus on cognitive processing and problem solving seem to be beneficial(Lazarus, 1993). Being able to regulate one’s emotions effectively shouldallow both recipients and providers to communicate their needs more clearlyto each other (e.g., Gross, 2002).
Personal values. Darley and Latané’s (1968) work minimized the role ofpersonal values in helping, but more recent research has identified values thatdo appear to play a role in helping. Specifically, people who are religious aremore likely to volunteer to serve charitable causes (see Wilson & Musick,1997) and are more likely to help in studies in which confederates needassistance (Hansen, Vandenberg, & Patterson, 1995). Dunkel-Schetter,Folkman, and Lazarus (1987) found that people who are more religious weremore likely to receive support as well. Perhaps because they feel they mustanswer to a higher power or because of a desire to do the right thing, peoplewho report more spiritual feelings may be more motivated to exchangesupport with their partners in times of crisis, regardless of the characteristicsof the situation or the relationship.
Limitations of Prior Work
Although prior research has identified a broad range of situational,relational, and individual determinants of helping and support, severallimitations of the existing literature nevertheless suggest caution before gen-eralizing from the existing work to the context of intimate relationships aftertraumatic injuries. First, much of this research has focused on helpingdirected toward strangers (e.g., donating blood, volunteering one’s time; e.g.,Solomon et al., 1978) or hypothetical others (e.g., Weiner, 1995), for whomthe decision to help is a one-time choice with few lasting consequences. Incontrast, a partner who has experienced a traumatic injury requires ongoingcare, continual appraisal of the partner’s need, and considerable investmentfrom the support provider. Research on support in less impactful situationsmay not generalize to situations in which support is most common and mostconsequential (e.g., Dehle et al., 2001).
Second, even when studies have examined support in actual relationships,the samples have been limited primarily to couples who are White, middle-
SUPPORT AFTER TRAUMATIC INJURY 2049

class, and in long-term relationships (i.e., they are often married and have beentogether for many years). Traumatic injuries can happen to anyone, but ratesof traumatic injuries are especially high in more diverse and younger popula-tions. Non-White individuals tend to be at higher risk for trauma; for example,Breslau, Chilcoat, Kessler, and Davis (1999) found that minority individualsreported much higher exposure to assaultive violence. Trauma survivors alsotend to be younger. For example, in a random probability sample of LosAngeles adults, the average age of experiencing a traumatic event was 26 years(Ullman, 1995). Trauma survivors, therefore, are likely to be in shorter, lesscommitted relationships and, as a consequence, may have a different set ofresources to bring to bear on this situation, relative to the couples that havebeen studied more frequently. Thus, the findings from previous studies maynot easily generalize to the couples at greatest risk after experiencing trauma.
Finally, although Dunkel-Schetter and Skokan (1990) originally pro-posed that all four broad domains of predictors (i.e., situation, relationship,recipient, and provider) are required to understand support receipt and pro-vision, very few studies have examined all four domains at once. Instead,most research on support has focused on a single domain. In a noteworthyexception to this trend, Hobfoll and Lerman (1989) examined three of thesefactors (i.e., situation, relationship factors, and recipient characteristics) in astudy of women with children in the hospital. They found that chronic stress,relationship factors (e.g., intimacy), and personal characteristics (e.g., self-esteem) influenced the amount of general support they received. However,this study could not address the factors that specifically influence supportprovided by a partner, as it did not examine support from the partnerseparate from other network sources, and it did not measure specific supportprovider characteristics.
In another exception, Iida et al. (2008) examined multiple elements fromDunkel-Schetter and Skokan’s (1990) model in two daily diary studies ofcouples, and found that the recipient’s distress, aspects of the relationship(e.g., relationship anxiety), and measures taken from both partners (e.g.,daily mood) accounted for support provision. Yet, these studies examinedhealthy couples who were providing support with normative daily stressorsor with a professional stressor (i.e., taking the Bar exam). We are aware of nostudies to date that have adopted a similarly broad approach to account forsupport in couples experiencing a serious acute stressor like a traumaticinjury. As a consequence, whereas research on support in health-relatedcontexts has accumulated an increasingly lengthy list of significant predictorsof support, the relative influence of each class of predictors remains an openquestion. Without answers to this question, the accumulated research onsocial support is limited in its ability to inform interventions that target themost relevant predictors of support provision.
2050 MAISEL ET AL.

The Current Study
The goal of the current study is to address these gaps in the existingliterature through a study of couples in which one partner has recentlysurvived a traumatic injury (e.g., a gunshot wound, injuries from a caraccident). Survivors and their romantic partners were recruited from urbantrauma centers, and face-to-face interviews were conducted individually witheach partner in English or Spanish.
Our analyses of these interviews expand on previous research in threeways. First, whereas prior research on traumatic injuries has focused mostoften on the support recipient, we include data from both partners toexamine characteristics of both partners that may influence support. Second,whereas prior research on social support in health-related contexts has oftenfocused on White, middle-class couples, these data were drawn from a popu-lation including young, diverse, low socioeconomic status (SES) participants.Finally, whereas prior work has tended to examine specific domains of pre-dictors, these interviews gathered data on aspects of the situation, the cou-ple’s relationship, and the characteristics of both partners, allowing analysesof the unique ability of each of these domains to account for support in thissituation.
Based on the prior literature, we predict that elements drawn from each ofthe broad domains in Dunkel-Schetter and Skokan’s (1990) model willaccount for support behavior in these couples. Specifically, we propose thefollowing:
Hypothesis 1. With respect to the situation, partners willprovide more support to trauma survivors whose injuries aremore severe.
Hypothesis 2. With respect to the relationship, partners willprovide more support to trauma survivors to the extent thattheir relationships are more satisfied and more committed (e.g.,in longer relationships; married, rather than cohabiting ordating).
Hypothesis 3. With respect to personality, partners will provideless support to the extent that they are higher in neuroticism,but will provide more support to the extent that the survivor ishigher in neuroticism.
Hypothesis 4. With respect to coping style, partners will providemore support to the extent that they or their partners are moreeffective at regulating their emotions.
SUPPORT AFTER TRAUMATIC INJURY 2051

Hypothesis 5. With respect to personal values, partners willprovide more support to the extent that they or their partnersare more religious.
Importantly, the present analyses are able to evaluate the unique contri-butions of each of these elements in accounting for support after a traumaticinjury. Here, the existing literature did not support strong hypotheses for thispopulation. Our tentative hypothesis is that to the extent that trauma survi-vors tend to be young and, therefore, in newer relationships in which thereare fewer expectations that partners will provide for each other, we predictthat relationship qualities might play less of a role in accounting for supportin this population, compared to other populations in which the determinantsof support have been studied.
Method
Participants
Participants in the present study were approached following hospitaliza-tion at one of three Level I urban trauma centers in Los Angeles County. Allof the participants required treatment for injuries stemming from sudden,unexpected physical trauma, such as a car accident or a gunshot wound(injuries resulting from domestic violence and self-inflicted injuries wereexcluded).
The first 251 participants (192 males, 59 females) who were eligible andwho completed the interview comprise the original sample of trauma survi-vors in this study. The average time that these “target” participants spent inthe hospital after the injury was 8.75 days (SD = 8.40). The most commonreasons for being admitted were being shot by a gun (25.8%), being hit by amoving vehicle while driving (21.1%), hitting a non-moving object (e.g., awall) while driving (16.7%), being a passenger in a car accident (11.2%), andbeing stabbed with a knife or other sharp object (9.1%).
On average, the trauma survivors were 32.5 years old (SD = 11.8) and had12.16 years (SD = 2.71) of education. The sample was diverse: Approxi-mately 31.5% of the participants were African American, 42.2% wereLatino/a, 17.9% were White, and 8.4% were Asian/Pacific Islander. Althoughmost of the trauma survivors were male, an effort was made to recruit femalesurvivors as well (23.5% of the sample).
As part of their initial interview, all of the survivors were asked if they hadan intimate partner. Of the original 251 participants who were asked, 55.8%(n = 140) had a partner or spouse. If they had an intimate partner, survivors
2052 MAISEL ET AL.

were asked for permission to contact the partner to see if the partner wouldbe willing to be interviewed as well. Of the participants with partners, 71% ofthe trauma survivors gave the researchers permission to contact their part-ners. Of these partners, 13% could not be located, 13% were ineligible, and13% refused to participate. A total of 58 partners (41.4%) completed theinterview.3
We compared the characteristics of trauma survivors who had partnerswho participated in the study with the characteristics of trauma survivorswhose partners did not participate. Generally, we found very few differencesbetween these two groups. They did not differ in gender composition, age,years of education, relationship status (i.e., married, engaged, dating), rela-tionship length, or relationship satisfaction. Trauma survivors whose part-ners participated were more likely to be White, c2(1) = 3.30, p < .10; and wereless likely to be Asian, c2(1) = 4.38, p < .05. The survivors whose partnersparticipated also had slightly more severe injuries, t(138) = -2.52, p < .05.
We used the sample of 58 trauma survivors and their partners for theremainder of the analyses. The demographic characteristics of these traumasurvivors and their partners are presented in Table 1. The partners of thetrauma victims were primarily female (72.4%). On average, the partners were30.0 years of age (SD = 10.1), had 11.86 (SD = 2.47) years of education, andthey were diverse (32.8% were African American, 39.7% were Latino/a,25.9% were White, and 1.7% were Asian/Pacific Islander). Couples had beentogether an average of 6.7 months (SD = 10.2, range = less than 1 month to4.33 years). According to the partner’s report, approximately 48.3% weremarried or engaged, 13.8% were cohabiting, and 37.9% were dating.
Procedure
Trauma survivors were contacted in the hospital and were asked to par-ticipate in a study of coping with serious injury. Trained laypeople conductedthe face-to-face interviews in English or Spanish, either in the hospital or inthe survivor’s home. For the trauma survivor, the average number of daysthat elapsed from the time of hospitalization to the time of the interview was18.31 days (SD = 17.50). Participants were asked about the injury, theirdemographic characteristics, their mental health symptoms since the injury,their relationship status and relationship satisfaction, and other individual-difference measures (e.g., neuroticism).
3For more information on the full eligibility criteria for the study, see Shih, Schell,Hambarsoomian, Belzberg, and Marshall (2010).
SUPPORT AFTER TRAUMATIC INJURY 2053

Partners of trauma survivors were interviewed in their homes an averageof 27.47 days (SD = 20.54) after the trauma survivor’s injury. The interviewthat was given to partners was significantly shorter than the one that wasgiven to trauma survivors, and it contained several measures not adminis-tered to the survivor, most notably a measure of how much support they hadprovided to their partners since the injury. As with the trauma survivors,face-to-face interviews were conducted in English or Spanish.
Measures
Demographic Questions
Trauma survivors and their partners were asked to answer demographicquestions. These included their gender, age, race/ethnicity, and how manyyears of school they had completed (see Table 1).
Table 1
Characteristics of Trauma Survivors and Their Partners
Variable Trauma survivorsPartners of
trauma survivors
Female 27.6% 72.4%Age 30.7 (SD = 12.0) 30.0 (SD = 10.1)Ethnicity
African American 32.8% 32.8%Latino/a 46.6% 39.7%Caucasian/White 19.0% 25.9%Asian 1.7% 1.7%
Average years of education 11.79 (SD = 2.50) 11.86 (SD = 2.47)Relationship status
Married/engaged 44.8% 48.3%Cohabiting 17.2% 13.8%Dating 34.5% 37.9%
Relationship length (in months) 6.73 (SD = 10.15)Relationship satisfaction 5.48 (SD = 1.71) 5.79 (SD = 1.45)
Note. N = 58.
2054 MAISEL ET AL.

Support Provision
The main dependent variable of interest in these analyses was the supportprovided by the partner of the trauma survivor. To assess support provision,partners were asked to respond to items from the Caregiver Demands scale(Stetz, 1989). Originally designed to measure supportive behaviors in caregiv-ers of people with cancer, this scale asks how often the partner engages indifferent sorts of support activities. The instructions read “This group ofquestions asks about the tasks and activities that you may be doing to helpyour partner. For each of the activities I list, I am interested in knowing howmuch time you spend on that activity.”
Partners were asked about 15 specific behaviors, including “Helping yourpartner with medical care (e.g., giving medications, treatments, bandagingwounds),” and “Emotional support (e.g., being there for the partner).” Themajority of the questions pertain to helping with medical care, householdchores, and so forth. Partners rated their responses on a 5-point scale rangingfrom 0 (none) to 4 (a huge amount). Although the scale measures differentaspects of support (i.e., emotional, informational, instrumental), the coeffi-cient alpha for the whole scale was high (a = .90). Participants reportedproviding a “moderate amount” of support, on average (M = 2.28,SD = 0.91). This questionnaire was added to the study shortly after severalpartners had already been interviewed. Therefore, a total of 52 partnerscompleted this questionnaire.
Qualities of the Situation
Partners often disagree somewhat when rating the symptoms and severityof an injury or illness (e.g., Gallagher, Riggs, Byrne, & Weathers, 1998). Toexamine whether any results were specific to a single reporter, we assessed theseverity of the traumatic injury using reports from both the trauma survivorand the partner.
Trauma severity (trauma survivor report). Trauma survivors were askedseveral questions regarding the severity of the injury, including (a) “Whatpart(s) of your body were injured?” (list of options: chest, head, legs, etc.); (b)“Did you lose consciousness during the event?” (Yes or No); (c) “How long doyou think it will take you to fully physically recover from the injury?” (rated ona 6-point scale ranging from 1 [a few days] to 6 [you may not recover]); and (d)“How long do you think other people will be able to tell you have beeninjured?” (rated on a 6-point scale ranging from 1 [a few days] to 6 [more thana few years]). In addition, the interviewer reported (Yes or No) whether or notthere was evidence of recent trauma (e.g., cuts, bruises, burns, bandaging).
SUPPORT AFTER TRAUMATIC INJURY 2055

Because these questions include categorical and continuous variables, wecreated a cumulative-risk variable to determine the severity of the injury.Participants were assigned a 1 for each severe characteristic he or she reported(e.g., if they had lost consciousness during the event and if the interviewerreported evidence of recent trauma). They received a 1 on the continuousmeasures if they scored above the median (i.e., on the number of body partsinjured, the time they thought it would take to recover, and the time they thoughtthat people would be able to tell they were injured). A sum of these items wasused for the cumulative-risk variable (M = 2.79, SD = 1.32, range = 0–5).
Trauma severity (partner report). The partners were asked “How long doyou think it will take your partner to fully physically recover from theinjury?” (rated on a 6-point scale ranging from 1 [a few days] to 6 [partner maynot recover]). The mean response was 2.86 (SD = 1.21), which means thatpartners reported that it would take the trauma survivors about a year, onaverage, to recover physically. These two reports of severity (i.e., from thetrauma survivor and from the partner) were not highly correlated (r = .10,p = .44), so we examined them as two separate scales. On the one item thatboth partners completed (i.e., how long it will take the partner to recoverphysically), there was no significant mean difference between ratings of thetrauma survivors (M = 2.71, SD = 1.14) and ratings of the partners(M = 2.86, SD = 1.21), t(114) = -0.71, p > .10. However, these reports werenot significantly correlated within couples (r = .19, p = .16).
Qualities of the Relationship
Relationship length. Trauma survivors were asked how long they hadbeen in a relationship with their current partners (see Table 1).
Relationship status. Trauma survivors were asked about their relation-ship status, including whether they were married, not married but living witha long-term partner, widowed, separated, divorced, or never married. If theywere not married or were cohabiting with a partner, they were asked if theyhave a “main romantic involvement, a man or a woman you think of as asteady, a lover, a girlfriend or boyfriend, a partner, or the like.” If theyanswered Yes to this question, they were asked about the status of therelationship: dating casually (i.e., free to see other people), dating exclusively(i.e., not seeing other people), engaged but haven’t set the date, or engagedwith a wedding date set (see Table 1).
Partners of the trauma survivors were also asked if they were married,engaged, living together, dating exclusively, or dating casually (see Table 1).Not all of the couples agreed on the status of the relationship (34.5% did notagree), but this may have been a result of the time lapse between the interview
2056 MAISEL ET AL.

of the trauma survivor and the interview of the partner (i.e., some people whowere dating exclusively may have moved in together or become engaged inthe time between the interviews). In all cases, we used the partner’s report ofthe relationship status, as this was the most recent report and was taken at thesame time as the measure of support provision.
Relationship satisfaction. Trauma survivors and their partners were eachasked about their relationship quality with a single satisfaction item: “Takingthings all together, how would you describe your current relationshipwith your partner?” This was rated on a 7-point scale ranging from 1 (veryunhappy) to 7 (very happy; see Table 1). This is the same item that was usedto assess relationship satisfaction in the General Social Survey (Davis,Smith, & Marsden, 2006) and the National Survey of Families and House-holds (Sweet, Bumpass, & Call, 1988), and it has been found to perform aswell as longer measures of the same construct (Johnson, 1995).
Qualities of the Trauma Survivor and Partner
Personality. In both the survivor and the partner interviews, level ofneuroticism was measured with five items that were selected from the NEOFive Factor Inventory (NEO-FFI; Costa & McCrae, 1992). Participants werespecifically asked to describe themselves as they were before the injury,through items such as “I often felt inferior,” and “I often got angry,” on a5-point scale ranging from 1 (strongly disagree) to 5 (strongly agree). Themean for trauma survivors (a = .81) was 2.42 (SD = 0.91), while the mean forpartners (a = .79) was 2.48 (SD = 0.93), with higher scores indicating higherlevels of neuroticism.
Coping style. Trauma survivors and their partners were asked how theyusually handle themselves when they are upset, using five items taken fromthe shortened Ruminative Responses Scale (Treynor, Gonzalez, & Nolen-Hoeksema, 2003). These include items such as “When you feel upset, howoften do you . . . analyze recent events to try to understand why you areupset?” The items were rated on a 5-point scale ranging from 1 (never) to 5(always). These items represent the “reflection” aspect of dealing with nega-tive emotions, which includes “a purposeful turning inward to engage incognitive problem solving to alleviate one’s depressive symptoms” (Treynoret al., 2003, p. 256). This type of reflective processing captures a person’stendency to regulate emotions and reflect on problems (see Kross, Ayduk, &Mischel, 2005). These items are distinct from worrying or brooding about theproblem and being depressed about the problem (see Treynor et al., 2003).The mean for trauma survivors (a = .77) was 2.47 (SD = 0.85), while themean for partners (a = .80) was 2.55 (SD = 0.99).
SUPPORT AFTER TRAUMATIC INJURY 2057

Personal values. Survivors were asked two questions about their religios-ity. The first is “Currently, how important is religion in your daily life?” Thiswas rated on a 4-point scale ranging from 1 (very important) to 4 (not at allimportant; reverse-scored). The second question is “How much do yourreligious beliefs influence the way you live?” This was rated on a 4-point scaleranging from 1 (not at all ) to 4 (very much). For the trauma survivors, thesetwo questions were averaged together (a = .77), with a mean of 3.15(SD = 0.84).
The partners of the trauma survivors were given a larger scale to measurereligiosity and spirituality. The Daily Spiritual Experiences (DSE) scale(Underwood & Teresi, 2002) is a 16-item scale that assesses everyday reli-gious experience (e.g., “I feel guided by God in the midst of daily activities”)and that has demonstrated adequate reliability and validity (Underwood &Teresi, 2002). Participants rated the items on a 6-point scale ranging from0 (never or almost never) to 5 (many times a day). The alpha for the scale was.96, with a mean of 2.91 (SD = 1.36). We used the two religiosity questionsfor the trauma survivor and the DSE scale for the partners to measure eachperson’s religiosity.
Analytic Strategy
Our primary outcome of interest is the support provided by the traumasurvivor’s partner after the injury. Our preliminary analyses included exam-ining the correlations among the predictors of interest, and examining theeffects of potential control variables (e.g., demographic factors) on supportprovision. For our main analyses, we examined different groups of predictorsin stages through hierarchical regression, which allowed us to assess howmuch unique variance each new set of variables added to our prediction ofsupport provision. We conducted three separate analyses predicting supportprovision: The first examined situational variables, the second examinedrelationship variables, and the third examined individual-difference vari-ables. Finally, an omnibus analysis considered all of the previously significantpredictors simultaneously, to see which variables remained significant.
Results
Preliminary Analyses
Correlations Among Predictors
The correlations among all of the independent variables described inthese analyses are reported in Table 2. As the table reveals, there was little
2058 MAISEL ET AL.

Tab
le2
Cor
rela
tion
sA
mon
gS
itua
tion
al,R
elat
ions
hip,
and
Indi
vidu
al-D
iffer
ence
Var
iabl
es
Mea
sure
12
34
56
78
9
1.T
raum
ase
veri
ty(s
urvi
vor’
sre
port
)—
2.T
raum
ase
veri
ty(p
artn
er’s
repo
rt)
.10
—3.
Rel
atio
nshi
psa
tisf
acti
on(s
urvi
vor)
-.10
.03
—4.
Rel
atio
nshi
psa
tisf
acti
on(p
artn
er)
.01
-.13
.02
—5.
Neu
roti
cism
(sur
vivo
r)-.
07.0
3-.
21-.
27*
—6.
Neu
roti
cism
(par
tner
).0
4.2
9†-.
04-.
46**
.34*
*—
7.R
eflec
tive
proc
essi
ng(s
urvi
vor)
.01
-.06
-.07
.04
.20
-.02
—8.
Refl
ecti
vepr
oces
sing
(par
tner
)-.
25†
.01
.07
.09
.07
.29*
.23
—9.
Rel
igio
sity
(sur
vivo
r)-.
14.1
7-.
09.1
6.0
5.0
5.1
2-.
06—
10.
Rel
igio
sity
(par
tner
)-.
33*
.02
-.07
.09
-.00
.17
.14
.42*
*.4
7**
Not
e.N
sra
nged
from
51to
58.
†p<
.10.
*p<
.05.
**p
<.0
1.
SUPPORT AFTER TRAUMATIC INJURY 2059

threat of collinearity among the set of predictors examined here. Of the 45possible bivariate correlations, only 9 were statistically significant or mar-ginally significant. Moreover, the size of even the significant correlationswas moderate (rs ranged from -.46 to .47), although all were in predicteddirections (e.g., partners’ reports of relationship satisfaction were negativelyassociated with their own and the survivors’ levels of neuroticism).However, the failure to observe a significant correlation between the rela-tionship satisfaction scores of survivors and their partners (r = .02, ns) isworth noting.
In established couples, the satisfaction of the two partners is oftenstrongly correlated (e.g., Sprecher, 1988). The lack of a correlation here maybe a result of the fact that these are young relationships, on average; or thefact that the partners and survivors reported on their relationships at differ-ent times, during a period of change in the relationship. In general, thevariables assessed here were performing as expected and were associated inways that justify examining them as separate predictors of support provisionin subsequent regression analyses.
Analysis of Control Variables
Next, we examined potential control variables that might account forvariance in support provision. We conducted a multiple regression analysiswith the following demographic variables assessed in both the trauma survi-vors and their partners: gender, age, race/ethnicity, and education. Addition-ally, because partners varied in the length of time that had elapsed betweenthe injury and the interview, we examined this as a potential control variable(because less support might be required as the time since the injury increases).We entered all of these predictors into the equation simultaneously, as thesewere not our main variables of interest. From this analysis, the only signifi-cant predictor of support provision was gender (b = .35, p < .05). Femalepartners provided more support to the trauma survivor than did male part-ners. Therefore, in the results that follow, we controlled for the partner’sgender in Step 1 of each analysis.
Situational Factors
In the first hierarchical regression analysis, we entered the control variableof gender in Step 1. We entered the severity of the injury as a predictor ofsupport in Step 2 (see Table 3).
2060 MAISEL ET AL.
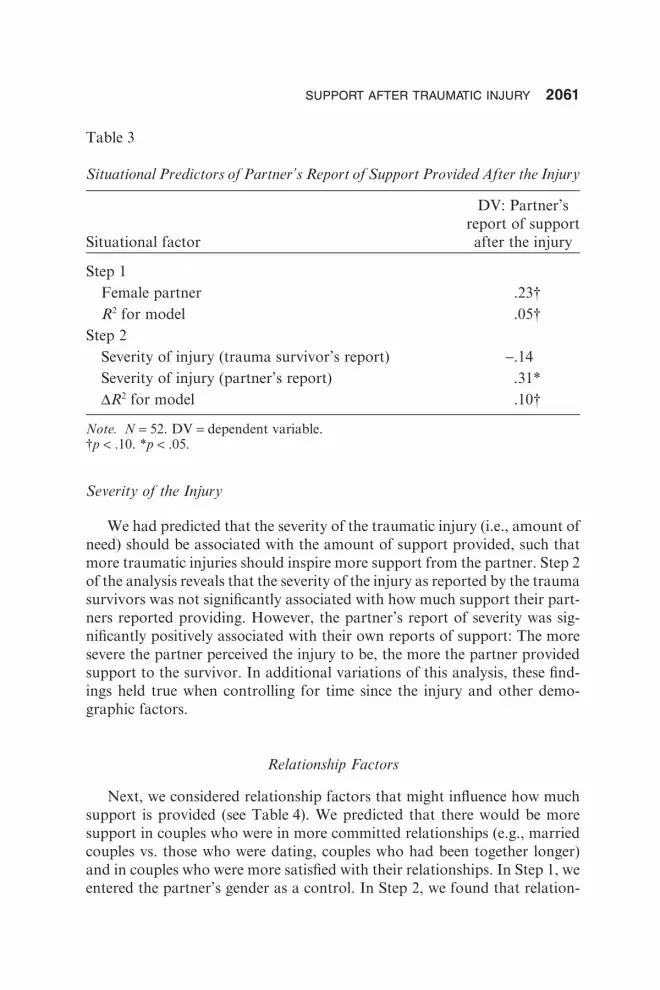
Severity of the Injury
We had predicted that the severity of the traumatic injury (i.e., amount ofneed) should be associated with the amount of support provided, such thatmore traumatic injuries should inspire more support from the partner. Step 2of the analysis reveals that the severity of the injury as reported by the traumasurvivors was not significantly associated with how much support their part-ners reported providing. However, the partner’s report of severity was sig-nificantly positively associated with their own reports of support: The moresevere the partner perceived the injury to be, the more the partner providedsupport to the survivor. In additional variations of this analysis, these find-ings held true when controlling for time since the injury and other demo-graphic factors.
Relationship Factors
Next, we considered relationship factors that might influence how muchsupport is provided (see Table 4). We predicted that there would be moresupport in couples who were in more committed relationships (e.g., marriedcouples vs. those who were dating, couples who had been together longer)and in couples who were more satisfied with their relationships. In Step 1, weentered the partner’s gender as a control. In Step 2, we found that relation-
Table 3
Situational Predictors of Partner’s Report of Support Provided After the Injury
Situational factor
DV: Partner’sreport of supportafter the injury
Step 1Female partner .23†R2 for model .05†
Step 2Severity of injury (trauma survivor’s report) -.14Severity of injury (partner’s report) .31*DR2 for model .10†
Note. N = 52. DV = dependent variable.†p < .10. *p < .05.
SUPPORT AFTER TRAUMATIC INJURY 2061

ship status was not significantly associated with the amount of supportprovided. In Step 3, we similarly found that relationship length was notsignificantly associated with support. In Step 4, we found that neither thesurvivor’s nor the partner’s reports of relationship satisfaction were signifi-cantly associated with support either. In additional variations of this analy-sis, these findings held true when controlling for time since the injury, injuryseverity, and other demographic factors.
Individual-Difference Factors
Finally, we examined three individual-difference variables in both thetrauma survivors and their partners (see Table 5). In Step 1 of the regressionanalysis, we entered the control variable of gender. In Step 2, we entered
Table 4
Relationship Predictors of Partner’s Report of Support Provided After theInjury
Relationship factorDV: Partner’s report
of support after the injury
Step 1Female partner .24†R2 for model .02†
Step 2Married/engaged .12DR2 for model .01
Step 3Relationship length -.20DR2 for model .03
Step 4Relationship satisfaction (trauma survivor) -.04Relationship satisfaction (partner) -.02DR2 for model .00
Note. N = 51. DV = dependent variable.†p < .10.
2062 MAISEL ET AL.

neuroticism for both partners; in Step 3, we added reflective processing forboth partners; and in Step 4, we added religiosity for both partners.
Personality
Consistent with prior research, the neuroticism of the trauma survivorwas positively associated with support. Trauma survivors who reported moreneuroticism had partners who reported providing more support. Neuroticismof the partner was not significantly associated with support. These findingsheld true, controlling for time since the injury, injury severity, and otherdemographic factors.
Table 5
Individual-Difference Predictors of Partner’s Report of Support Provided Afterthe Injury
Individual-difference factorDV: Partner’s report
of support after the injury
Step 1Female partner .23†R2 for model .05†
Step 2Neuroticism (trauma survivor) .34*Neuroticism (partner) .04DR2 for model .13*
Step 3Reflective processing (trauma survivor) -.08Reflective processing (partner) .25DR2 for model .05
Step 4Religiosity (trauma survivor) -.02Religiosity (partner) .34*DR2 for model .09†
Note. N = 52. DV = dependent variable.†p < .10. *p < .05.
SUPPORT AFTER TRAUMATIC INJURY 2063

Coping Style
Reflective processing of the trauma survivor was not significantly associ-ated with support provision, nor was reflective processing of the partner.These findings held true, controlling for time since the injury, injury severity,and other demographic factors.
Religiosity
Religiosity of the trauma survivor was not significantly associated withsupport provision. However, the partner’s report of religiosity was positivelyassociated with the amount of support he or she provided. In other words,the more a partner reported feeling spiritual and religious (i.e., feeling close toGod), the more likely he or she was to provide support to the traumasurvivor. These findings held true, controlling for time since the injury, injuryseverity, and other demographic factors.
All Predictors
To evaluate the relative ability of variables from each of the four broaddomains to account for support, the final analysis entered all of the previoussignificant predictors (i.e., partner’s report of trauma severity, trauma survi-vor’s neuroticism, partner’s religiosity) into one multiple regression analysis.While controlling for gender, all three variables remained significant.
The partner’s report of the severity of the injury (b = .28, p = .019), thetrauma survivor’s neuroticism (b = .34, p = .005), and the partner’s religiosity(b = .36, p = .004) all remained significant predictors of support. In a finalmodel with only these three predictors, the partner’s report of the severity ofthe injury accounted for a 10% increase in R2 ( p = .022), the trauma survi-vor’s neuroticism accounted for an 11% increase in R2 ( p = .013), and thepartner’s religiosity accounted for a 15% increase in R2 ( p = .001). Together,these significant predictors accounted for 36% of the total variance insupport. When all of the variables (i.e., all demographic, situational, rela-tionship, and individual characteristic variables) were entered into a singleregression analysis, these three predictors remained the only significant pre-dictors of support.
Discussion
For individuals who have recently suffered a traumatic injury, the supportthat intimate partners provide can make the difference between recovery and
2064 MAISEL ET AL.

lasting physical and mental scars (e.g., Halford, Scott, & Smythe, 2000). Yet,research on the antecedents of support has not been applied toward under-standing couples in this context. Existing research on support may not gen-eralize to the context of a traumatic injury, as trauma survivors’ partners varyon dimensions that may be related to the sorts of support they are able andwilling to provide (e.g., they tend to be younger, more diverse, and in lesscommitted relationships).
In this study, we attempted to account for the support that intimatepartners provide after a traumatic injury. In particular, these analyses exam-ined the unique contributions of variables drawn from four domains: situ-ational factors (i.e., severity of the injury), relationship factors (i.e., status,length, satisfaction), and individual differences (i.e., neuroticism, reflectiveprocessing, religiosity) in the support recipient and the support provider.These four domains emerged from models of support provision (e.g., Dunkel-Schetter & Skokan, 1990). Such models have not been tested previously in apopulation of trauma survivors. Moreover, most research has neglected toassess all four domains, leaving their relative importance in applied settings anopen question. One of the central contributions of the current study is theability to address all of these domains at once to examine their independentassociations with support after traumatic injury. Variables from three of thefour domains accounted for significant variance in partner support, even aftercontrolling for the other significant predictors examined here.
With respect to the situation, partners’ reports of their own support weresignificantly associated with their own perceptions of the severity of thesurvivors’ injuries, but were not associated with the survivors’ reports ofinjury severity. It is worth recalling that partner and survivor reports of theseverity of the injury were not significantly correlated—their ratings of sever-ity were largely subjective. Thus, partners were supporting survivors whenthey thought the survivors needed support, not necessarily when the survi-vors thought they needed support. This highlights the need to consider theperspectives of the provider and the recipient independently in models andinterventions addressing support. Although we did not study it directly here,the lack of a shared understanding of the injury seems likely to impede thequality and effectiveness of the support that the partners of trauma survivorsprovide.
Additionally, in our analysis of demographic predictors, we found thatthe gender of the support provider was associated with support, such thatwomen provided more support than did men. This finding is consistent withother research on social support that has found that women tend to providemore support than do men, particularly when self-report measures are used(e.g., Verhofstadt, Buysse, & Ickes, 2007). Controlling for this gender differ-ence did not substantially change any of the other effects reported here.
SUPPORT AFTER TRAUMATIC INJURY 2065

With respect to the relationship, neither relationship status, nor relation-ship length, nor relationship satisfaction accounted for significant variance inthe support that partners provided to survivors after the injury. This wassurprising, given prior studies that have reported significant links between thesupport that partners exchange and qualities of both marital and datingrelationships (e.g., Gurung, Sarason, & Sarason, 1997; Pasch, Bradbury, &Sullivan, 1997).
Two important differences between the current study and prior ones mayhave combined to account for the failure to replicate past results. First,despite some variability in duration, the relationships assessed in this studywere, on average, relatively short-lived at the time that the injury occurred(for over half of the sample, the relationship was less than 3 months old).Even couples in the sample who were married had not been together verylong (the mean relationship length for married couples was 12 months).These short relationships may be quite different from the relationships oftenstudied in the social support literature. For example, couples in new relation-ships are often quite satisfied (i.e., the “honeymoon” phase; e.g., Huston,McHale, & Crouter, 1986). Indeed, only 19% of our sample reported averagerelationship satisfaction or lower. Thus, the simple lack of variance in satis-faction may have limited our power to observe covariance between satisfac-tion and anything else. Given greater variability in the length and satisfactionof the relationship, we might have found a greater impact of relationshipcharacteristics on helping.
Second, the event examined here was, by design, a highly impactful one.In contrast, prior studies of social support in couples have examined eitherless committed relationships facing relatively mild stressors (e.g., Collins &Feeney, 2000) or well established relationships facing severe health challenges(e.g., Bolger et al., 1996). In both of these sorts of studies, the supportrequired in the situation was well calibrated to the level of commitment in thecouples being studied: minimal support in the dating couples, and substantiallife changes in the longstanding couples. The couples examined here,however, faced a mismatch. Most were not married and had been togetheronly briefly; yet, they faced a situation requiring the sorts of support thatmuch more involved partners typically provide. In these young relationships,trauma survivors may have drawn upon other sources of support, and thequalities of the relationship may have been less relevant.
With respect to individual differences, characteristics of both the survivorand the partner were independently associated with support. Consistent withother research on support provision (in particular, the finding that displayingmore distress elicits more support; Hobfoll & Lerman, 1988), survivors whoscored higher on a measure of neuroticism had partners who provided moresupport after the injury. Although neuroticism is typically associated with
2066 MAISEL ET AL.

more negative outcomes, it makes sense that individuals with a tendency toworry across situations may be especially in tune with their own needs in asituation that actually warrants concern.
It is worth noting, however, that the current findings examined supportonly in the short term. Given the negative interpersonal consequences ofneuroticism (Rogge et al., 2006; Tucker, Kressin, Spiro, & Ruscio, 1998), it ispossible that in the long term, those who support more neurotic survivorsmay be more vulnerable to burning out and eventually withdrawingtheir support. Future longitudinal research might profitably explore thispossibility.
With respect to the support provider, partners who reported higher levelsof religiosity provided more support. This finding is consistent with otherresearch demonstrating that religiosity is associated with greater supportprovision. In particular, individuals who have intrinsic or “internal” religi-osity (e.g., viewing religion as an end and not as a means for social status)have reported a greater desire to provide support to others (Batson & Gray,1981). The association between religiosity and support may be a result ofseveral aspects of religiosity. Religious people tend to report greater moralcommitment to providing support (Lam, 2002), and research on long-termcaregiving has shown that more religious people derive more rewards fromcaregiving (Pinquart & Sorensen, 2005) and report greater well-being, even inthe face of caregiver stress (Burgener, 1994).
These findings on religiosity highlight the unique challenge that the part-ners faced: It would be difficult to just walk away after a partner is injured;however, in these new relationships, the extent of partners’ obligation toprovide support can be ambiguous. In this context, partners may be morelikely to fall back on their own values. Partners whose religious valuesemphasize caregiving may be likely to fall back on these beliefs when deter-mining how to provide support. Latané and Darley (1970) proposed a modelof helping in which the situation should determine whether or not a personhelps. However, the current study demonstrates that when there is a clearneed for support but the norms are unclear, individual factors such as reli-giosity do play a role.
Overall, the results of the current study have two implications for multi-domain models of social support (e.g., Dunkel-Schetter & Skokan, 1990). Onone hand, the fact that aspects of the situation, the survivor, and the partnereach contributed independently toward understanding support providedafter a traumatic injury highlights the generalizability of these models. Acomprehensive understanding of who provides and who receives supportafter trauma seems likely to require the broad focus that these perspectivesendorse. On the other hand, these results also highlight the need to assesssocial support as it occurs in specific contexts.
SUPPORT AFTER TRAUMATIC INJURY 2067

Whereas most research on social-support exchanges in couples hasobserved strong associations between social support and relationship qualityand commitment, sometimes what goes on within a couple has little to dowith the dynamics of the couple. The period after a traumatic injury may beone of those times, when the demands of events external to the relationshipare so sudden and extreme that members of the couple respond according totheir individual dispositions, without reference to the nature of the relation-ship. Future research might further pursue how and why different contextsand challenges emphasize different elements of multi-domain models ofsocial support.
Strengths and Limitations
Our confidence in the results of this study is enhanced by a number ofstrengths in its methodology and design. First, in contrast to the majority ofresearch on support that is filtered through the eyes of the support recipient(see Kaul & Lakey, 2003), much of the data analyzed here were obtainedfrom both members of the couples. The fact that measures from each partneraccounted for support after the injury alleviates concerns that the associa-tions reported here depend on shared-method variance. Second, these datawere collected within a few weeks after couples had experienced a traumaticevent. Thus, their responses were collected during a time when the event wasstill current and likely to be highly salient, reducing opportunities for recallbias to affect the data. Third, the sample was young and diverse, more similarto the population of trauma survivors than to the populations that typicallyparticipate in research on illness and social support. Fourth, although each ofthe variables examined in our study has been examined in prior research onsupport and helping, they have rarely been examined in the same studies, andnever in the context of a severe and sudden stressor like a traumatic injury.Finally, the dependent variable assessed specific support behaviors that thepartner provided. Our measure of specific support behaviors avoids anumber of the pitfalls (e.g., recall bias, subjectivity) of more global measuresof support (see Wills & Shinar, 2000).
Despite these strengths, however, several factors nevertheless limit inter-pretations of the current findings. First, data from each partner were col-lected at a single assessment, limiting the ability of these analyses to addressissues of temporal or causal order. That said, because the dependent variablehere was support behavior, it remains far more likely that aspects of theinjury and stable characteristics of the partners affected support than viceversa. Second, all of the data described here were obtained through self-reports. Although the measurement and the comparison of data across
2068 MAISEL ET AL.

spouses were designed to minimize the role of perceptual biases, convergentfindings using more objective sources of data (e.g., medical records) wouldhave strengthened the conclusions. Third, although the focus on the intimatepartnership was justified by prior research on the unique effects of socialsupport from a partner, it would have provided an important context forthese results to know about the amount of support that the trauma survivorsreceived from other sources, such as family, friends, and community organi-zations. Fourth, the main dependent variable in this study was assessed in thepartners only, preventing analyses of agreement between partners and survi-vors on the extent of support provided. Indeed, prior research has shown thatpartners’ reports of support exchanged within their relationships often do notagree, although the level of agreement tends to be highest when the questionsrefer to specific behaviors, as they did in the present study (e.g., Norton &Manne, 2007). To the extent that the survivors may have had a differentperception of the support they received from their partners, those perceptionsmight have had unique predictors as well. Future research would benefit fromassessing all variables of interest in both members of the couple.
Finally, the sample examined here was relatively small, limiting the sta-tistical power of these analyses. In particular, although the results describedhere were not moderated by sources of heterogeneity in our sample (e.g., thepattern of results described here did not vary by gender, age, race/ethnicity,relationship length, relationship status, or severity of the trauma), some ofthese moderating effects might have been significant in a larger sample.Nonetheless, given that young, urban, low-SES individuals are widely under-studied, even data from a smaller sample of this difficult-to-reach populationexpand on the generalizability of existing models of support.
Future Directions
The current study did not address the effectiveness of the support thatpartners provided to survivors, only whether or not partners made the effortto provide support. Research would be enhanced by examining what supportwas most effective in these situations (and for whom), and by understandinghow responsive the support was to the person’s needs (Reis, Clark, &Holmes, 2004; Rini et al., 2006). It seems likely that the factors that accountfor efforts to provide support may be different from the factors that accountfor whether or not the support is effective and is perceived as supportive. Inparticular, whereas aspects of the relationship did not predict the extent towhich partners provided support in this study, aspects of the relationshipmay well affect the impact of that support on the survivor (e.g., Frazier,Tix, & Barnett, 2003).
SUPPORT AFTER TRAUMATIC INJURY 2069

A second worthwhile direction would be to examine how support changesover time in couples in which one partner needs extended or chronic care. Allfour of the domains we examined here may matter, but they may predictsupport differently over time. In particular, some of these domains may bemore or less predictive of who will experience caregiver burnout. Forexample, in a study of ongoing care in which one partner had cancer ormultiple sclerosis, Ybema, Kuijer, Hagedoorn, and Buunk (2002) found thatnegative relationship qualities—specifically, perceptions of inequity in therelationship—led to greater burnout and dissatisfaction. As the demand on acaregiver continues over a long period of time, it seems likely that a person’ssatisfaction with the relationship will predict the extent to which partnerssustain their efforts to provide care and support (e.g., Steadman, Tremont, &Davis, 2007).
In conclusion, although existing models of social support describe thelandscape of possible influences on social-support behavior, what we knowabout the relative importance of different domains in one context may notgeneralize to a context with different needs and different expectations. Inthe case of traumatic injuries, survivors tend to be young, so they are likelyto be in shorter, more recent relationships. Whereas social support incouples has often been linked to qualities of their relationships, in thiscontext partners responded more as individuals, relying on their own valuesand appraisals of the injury to determine the level of support they provided.Interventions to promote support in couples after a traumatic injury, there-fore, will need to take the perspective and values of the partner intoaccount.
References
Acitelli, L. K. (1996). The neglected links between marital support andmarital satisfaction. In G. R. Pierce, B. R. Sarason, & I. G. Sarason(Eds.), Handbook of social support and the family (pp. 83–103). New York:Plenum.
Batson, C. D., & Gray, R. A. (1981). Religious orientation and helpingbehavior: Responding to one’s own or the victim’s needs? Journal ofPersonality and Social Psychology, 40, 511–520.
Berg, C. A., & Upchurch, R. (2007). A developmental-contextual model ofcouples coping with chronic illness across the adult life span. Psychologi-cal Bulletin, 133, 920–954.
Bolger, N., Foster, M., Vinokur, A. D., & Ng, R. (1996). Close relationshipsand adjustment to life crisis: The case of breast cancer. Journal of Person-ality and Social Psychology, 70, 283–294.
2070 MAISEL ET AL.

Breslau, N., Chilcoat, H. D., Kessler, R. C., & Davis, G. C. (1999). Previousexposure to trauma and PTSD effects of subsequent trauma: Results fromthe Detroit Area Survey of Trauma. American Journal of Psychiatry, 156,902–907.
Brewin, C. R., Andrews, B., & Valentine, J. D. (2000). Meta-analysis of riskfactors for posttraumatic stress disorder in trauma-exposed adults.Journal of Consulting and Clinical Psychology, 68, 748–766.
Brown, G. W., & Harris, T. O. (1978). Social origins of depression: A study ofpsychiatric disorder in women. New York: Free Press.
Bryant, R. A., & Harvey, A. G. (1995). Avoidant coping style and post-traumatic stress following motor vehicle accidents. Behaviour Researchand Therapy, 33, 631–635.
Burgener, S. C. (1994). Caregiver religiosity and well-being in dealing withAlzheimer’s dementia. Journal of Religion and Health, 33, 175–189.
Collins, N. L., & Feeney, B. C. (2000). A safe haven: An attachment theoryperspective on support seeking and caregiving in intimate relationships.Journal of Personality and Social Psychology, 78, 1053–1073.
Costa, P. T., & McCrae, R. R. (1992). Revised NEO Personality Inventory(NEO PI-RTM) and NEO Five-Factor Inventory (NEO-FFI): Profes-sional manual. Odessa, FL: Psychological Assessment Resources.
Cutrona, C. E. (1996). Social support in couples: Marriage as a resource intimes of stress. Thousand Oaks, CA: Sage.
Darley, J. M., & Latané, B. (1968). Bystander intervention in emergencies:Diffusion of responsibility. Journal of Personality and Social Psychology,8, 377–383.
Davis, J. A., Smith, T. W., & Marsden, P. V. (2006). General social surveys,1972–2006: Cumulative codebook. Chicago: National Opinion ResearchCenter.
Dehle, C., Larsen, D., & Landers, J. E. (2001). Social support in marriage.American Journal of Family Therapy, 29, 307–324.
Dunkel-Schetter, C., Folkman, S., & Lazarus, R. S. (1987). Correlates ofsocial support receipt. Journal of Personality and Social Psychology, 53,71–80.
Dunkel-Schetter, C., & Skokan, L. A. (1990). Determinants of social supportprovision in personal relationships. Journal of Social and Personal Rela-tionships, 7, 437–450.
Feeney, B. C., & Collins, N. L. (2003). Motivations for caregiving inadult intimate relationships: Influences on caregiving behavior and rela-tionship functioning. Personality and Social Psychology Bulletin, 29, 950–968.
Frazier, P. A., Tix, A. P., & Barnett, C. L. (2003). The relational context ofsocial support: Relationship satisfaction moderates the relations between
SUPPORT AFTER TRAUMATIC INJURY 2071

enacted support and distress. Personality and Social Psychology Bulletin,29, 1133–1146.
Gallagher, J. G., Riggs, D. S., Byrne, C. A., & Weathers, F. W. (1998).Female partners’ estimations of male veterans’ combat-related PTSDseverity. Journal of Traumatic Stress, 11, 367–374.
George, D. M., Carroll, P., Kersnick, R., & Calderon, K. (1998). Gender-related patterns of helping among friends. Psychology of Women Quar-terly, 22, 685–704.
Gross, J. J. (2002). Emotion regulation: Affective, cognitive, and social con-sequences. Psychophysiology, 39, 281–291.
Gunthert, K. C., Cohen, L. H., & Armeli, S. (1999). The role of neuroticismin daily stress and coping. Journal of Personality and Social Psychology,77, 1087–1100.
Gurung, R. A. R., Sarason, B. R., & Sarason, I. G. (1997). Personal charac-teristics, relationship quality, and social support perceptions and behaviorin young adult romantic relationships. Personal Relationships, 4, 319–339.
Halford, W. K., Scott, J. L., & Smythe, J. (2000). Couples and coping withcancer: Helping each other through the night. In K. B. Schmaling & T. G.Sher (Eds.), The psychology of couples and illness: Theory, research, and prac-tice (pp. 135–170). Washington, DC: American Psychological Association.
Hansen, D. E., Vandenberg, B., & Patterson, M. L. (1995). The effects ofreligious orientation on spontaneous and nonspontaneous helping behav-iors. Personality and Individual Differences, 19, 101–104.
Helgeson, V. S., & Cohen, S. (1996). Social support and adjustment tocancer: Reconciling descriptive, correlational, and intervention research.Health Psychology, 15, 135–148.
Hobfoll, S. E., & Lerman, M. (1988). Personal relationships, personalattributes, and stress resistance: Mothers’ reactions to their child’s illness.American Journal of Community Psychology, 16, 565–589.
Hobfoll, S. E., & Lerman, M. (1989). Predicting receipt of social support: Alongitudinal study of parents’ reactions to their child’s illness. HealthPsychology, 8, 61–77.
Huston, T. L., McHale, S. M., & Crouter, A. C. (1986). When the honey-moon’s over: Changes in the marriage relationship over the first year. InR. Gilmore & S. Duck (Eds.), The emerging field of personal relationships(pp. 109–132). Hillsdale, NJ: Lawrence Erlbaum.
Iida, M., Seidman, G., Shrout, P. E., Fujita, K., & Bolger, N. (2008). Mod-eling support provision in intimate relationships. Journal of Personalityand Social Psychology, 94, 460–478.
Johnson, D. R. (1995). Assessing marital quality in longitudinal and lifecourse studies. In J. C. Conoley & E. B. Werth (Eds.), Family assessment(pp. 155–202). Lincoln, NE: Buros Institute of Mental Measurements.
2072 MAISEL ET AL.

Kaul, M., & Lakey, B. (2003). Where is the support in perceived support? Therole of generic relationship satisfaction and enacted support in perceivedsupport’s relation to low distress. Journal of Social and Clinical Psychol-ogy, 22, 59–78.
Kessler, R. C. (2000). Posttraumatic stress disorder: The burden to the indi-vidual and to society. Journal of Clinical Psychiatry, 61, 4–14.
Kessler, R. C., Sonnega, A., Bromet, E., Hughes, M., & Nelson, C. B. (1995).Posttraumatic stress disorder in the National Comorbidity Survey.Archives of General Psychiatry, 52, 1048–1060.
Knoll, N., Burkert, S., & Schwarzer, R. (2006). Reciprocal support provi-sion: Personality as a moderator? European Journal of Personality, 20,217–236.
Kross, E., Ayduk, O., & Mischel, W. (2005). When asking “why” does nothurt. Distinguishing rumination from reflective processing of negativeemotions. Psychological Science, 16, 709–715.
Lam, P. Y. (2002). As the flocks gather: How religion affects voluntaryassociation participation. Journal for the Scientific Study of Religion, 41,405–422.
Latané, B., & Darley, J. M. (1970). The unresponsive bystander: Why doesn’the help? New York: Appleton-Century-Crofts.
Lazarus, R. S. (1993). Coping theory and research: Past, present, and future.Psychosomatic Medicine, 55, 234–247.
Lutgendorf, S. K., Antoni, M. H., Ironson, G., Fletcher, M. A., Penedo, F.,Baum, A., et al. (1995). Physical symptoms of chronic fatigue syndromeare exacerbated by the stress of Hurricane Andrew. Psychosomatic Medi-cine, 57, 310–323.
Michaels, A. J., Michaels, C. E., Zimmerman, M. A., Smith, J. S., Moon,C. H., & Peterson, C. (1999). Posttraumatic stress disorder in injuredadults: Etiology by path analysis. Journal of Trauma, 47, 867–873.
Norris, F. H., & Kaniasty, K. (1996). Received and perceived social supportin times of stress: A test of the social support deterioration deterrencemodel. Journal of Personality and Social Psychology, 71, 498–511.
Norton, T. R., & Manne, S. L. (2007). Support concordance among couplescoping with cancer: Relationship, individual, and situational factors.Journal of Social and Personal Relationships, 24, 675–692.
Pasch, L. A., Bradbury, T. N., & Davila, J. (1997). Gender, negative affec-tivity, and observed social support behavior in marital interaction. Per-sonal Relationships, 4, 361–378.
Pasch, L. A., Bradbury, T. N., & Sullivan, K. T. (1997). Social support inmarriage: An analysis of intraindividual and interpersonal components. InG. R. Pierce, B. Lakey, I. G. Sarason, & B. R. Sarason (Eds.), Sourcebookof social support and personality (pp. 229–256). New York: Plenum.
SUPPORT AFTER TRAUMATIC INJURY 2073

Pinquart, M., & Sorensen, S. (2005). Ethnic differences in stressors,resources, and psychological outcomes of family caregiving: A meta-analysis. Gerontologist, 45, 90–106.
Pistrang, N., & Barker, C. (1995). The partner relationship in psychologicalresponse to breast cancer. Social Science and Medicine, 40, 789–797.
Reis, H. T., Clark, M. S., & Holmes, J. G. (2004). Perceived partner respon-siveness as an organizing construct in the study of intimacy and closeness.In D. J. Mashek (Ed.), Handbook of closeness and intimacy (pp. 201–225).Mahwah, NJ: Lawrence Erlbaum.
Resnick, H. S., Kilpatrick, D. G., Dansky, B. S., Saunders, B. E., & Best,C. L. (1993). Prevalence of civilian trauma and posttraumatic stress dis-order in a representative national sample of women. Journal of Consultingand Clinical Psychology, 61, 984–991.
Revenson, T. A., & Majerovitz, S. D. (1990). Spouses’ support provision tochronically ill patients. Journal of Social and Personal Relationships, 7,575–586.
Rini, C., Dunkel-Schetter, C., Hobel, C. J., Glynn, L. M., & Sandman, C. A.(2006). Effective social support: Antecedents and consequences of partnersupport during pregnancy. Personal Relationships, 13, 207–229.
Rogge, R. D., Bradbury, T. N., Hahlweg, K., Engl, J., & Thurmaier, F.(2006). Predicting marital distress and dissolution: Refining the two-factor hypothesis. Journal of Family Psychology, 20, 156–159.
Shih, R. A., Schell, T. L., Hambarsoomian, K., Belzberg, H., & Marshall,G. N. (2010). Prevalence of posttraumatic stress disorder and major depres-sion after trauma center hospitalization. Journal of Trauma, 69, 1560–1566.
Shumaker, S. A., & Brownell, A. (1984). Toward a theory of social support:Closing conceptual gaps. Journal of Social Issues, 40(4), 11–36.
Solomon, L. Z., Solomon, H., & Stone, R. (1978). Helping as a function ofnumber of bystanders and ambiguity of emergency. Personality and SocialPsychology Bulletin, 4, 318–321.
Sprecher, S. (1988). Investment model, equity, and social support determi-nants of relationship commitment. Social Psychology Quarterly, 51, 318–328.
Steadman, P. L., Tremont, G., & Davis, J. D. (2007). Premorbid relationshipsatisfaction and caregiver burden in dementia caregivers. Journal of Geri-atric Psychiatry and Neurology, 20, 115–119.
Stetz, K. M. (1989). The relationship among background characteristics,purpose in life, and caregiving demands on perceived health of spousecaregivers. Scholarly Inquiry for Nursing Practice, 3, 133–153.
Sweet, J. A., Bumpass, L. L., & Call, V. (1988). The design and content of theNational Survey of Families and Households. Madison, WI: Center forDemography and Ecology, University of Wisconsin–Madison.
2074 MAISEL ET AL.

Treynor, W., Gonzalez, R., & Nolen-Hoeksema, S. (2003). Ruminationreconsidered: A psychometric analysis. Cognitive Therapy and Research,27, 247–259.
Tucker, J. S., Kressin, N. R., Spiro, A., & Ruscio, J. (1998). Intrapersonalcharacteristics and the timing of divorce: A prospective investigation.Journal of Social and Personal Relationships, 15, 211–225.
Ullman, S. E. (1995). Adult trauma survivors and post-traumatic stresssequelae: An analysis of reexperiencing, avoidance, and arousal criteria.Journal of Traumatic Stress, 8, 179–188.
Underwood, L. G., & Teresi, J. (2002). The Daily Spiritual Experience scale:Development, theoretical description, reliability, exploratory factoranalysis, and preliminary construct validity using health-related data.Annals of Behavioral Medicine, 24, 22–33.
Verhofstadt, L. L., Buysse, A., & Ickes, W. (2007). Social support in couples:An examination of gender differences using self-report and observationalmethods. Sex Roles, 57, 267–282.
Watson, D., & Clark, L. A. (1984). Negative affectivity: The disposition toexperience aversive emotional states. Psychological Bulletin, 96, 465–490.
Weiner, B. (1995). Judgments of responsibility: A foundation for a theory ofsocial conduct. New York: Guilford.
Wills, T. A., & Shinar, O. (2000). Measuring perceived and received socialsupport. In S. Cohen, L. G. Underwood, & B. H. Gottlieb (Eds.), Socialsupport measurement and intervention: A guide for health and social scien-tists (pp. 86–135). New York: Oxford University Press.
Wilson, J. F. (2007). Posttraumatic stress disorder needs to be recognized inprimary care. Annals of Internal Medicine, 146, 617–620.
Wilson, J., & Musick, M. (1997). Who cares? Toward an integrated theory ofvolunteer work. American Sociological Review, 62, 694–713.
Ybema, J. F., Kuijer, R. G., Hagedoorn, M., & Buunk, B. P. (2002).Caregiver burnout among intimate partners of patients with a severeillness: An equity perspective. Personal Relationships, 9, 73–88.
SUPPORT AFTER TRAUMATIC INJURY 2075





























