Embed Size (px)
Citation preview

www.PRSJournal.com 907
Adequate correction of prominent ears requires analysis of the anatomical defects contributing to prominence so that the
appropriate surgical technique can be selected. Abnormalities causing prominent ears include underdefined antihelical fold, conchal hypertro-phy, increased conchomastoid angle, and ante-rior projection of the lobule.1 Correct diagnosis of these variations, accurate preoperative and perioperative measurements, and selection of the
appropriate technique are essential for avoiding unsatisfactory results after surgical correction.
The aim of the present study is to propose a sur-gical algorithm for revision otoplasty, based on an evaluation of patient concerns, desires, and clinical findings. This algorithm includes all of the surgical options available to address these abnormalities. A series of instructive cases is also presented.
PATIENTS AND METHODSThe clinical details of all patients who underwent
revision otoplasty at the Royal Hospital for Sick Children in Edinburgh and at St John’s Hospital in Livingston, within a 5-year period between May of 2006 and May of 2011, were retrieved from hospital records and from the medical photography database following audit approval. Exclusion criteria included surgical treatment of early complications or removal of protruding suture. Demographic data, complication occurrence, and indication for revision
Revision Otoplasty: An Algorithm Pawel Szychta, M.D., Ph.D.
Georgios Orfaniotis Ken J. Stewart, M.D.
Edinburgh, United Kingdom
Background: The purpose of this study was to propose a surgical algorithm for revision otoplasty, based on an evaluation of patient concerns, desires, and clinical findings. A series of instructive cases is presented.Methods: Thirty-six patients with an average age of approximately 15 years (range, 6 to 61 years), who underwent revision otoplasty between 2006 and 2011, were included. Demographic data, complications, indications for revision surgery, and operative details were retrieved from case notes and preopera-tive and postoperative photographs. Aesthetic outcomes were assessed by three independent plastic surgery consultants using a survey with 15 questions.Results: Indications for revision otoplasty included recurrent prominence/undercorrection, distortion of scaphoid fossa, distortion of antihelical fold, hypertrophic conchal bowl, and telephone ear. The relevant surgical technique was performed according to the patient’s concerns and aspirations in line with the proposed protocol of treatment and included the following: posterior suturing, conchal bowl reduction, reconstruction with conchal cartilage, or reconstruction with cost al cartilage.Conclusions: Otoplasty is performed frequently in young patients, and unsuc-cessful surgery can have a negative impact on their quality of life. Suturing techniques are safer than sculpting techniques, which can cause permanent ear deformity. Complications after sculpting techniques can lead to ear reconstruc-tion. The proposed algorithm for revision otoplasty addresses the whole variety of ear deformations, providing the surgical options available to address these abnormalities. (Plast. Reconstr. Surg. 130: 907, 2012.)CLINICAL QUESTION/LEVEL OF EVIDENCE: Therapeutic, IV.
Disclosure: The authors have no financial interest to declare in relation to the content of this article.
From the Department of Plastic and Reconstructive Surgery, Royal Hospital for Sick Children; and the Department of Oncological Surgery and Breast Diseases, Polish Mother’s Memorial Hospital-Research Institute.Received for publication November 7, 2011; accepted April 2, 2012.Presented at the Annual Meeting of the British Association of Aesthetic Plastic Surgeons, in Birmingham, United Kingdom, September 29 through 30, 2011, and at the 2011 Winter Meeting of the British Association of Plastic, Reconstructive and Aesthetic Surgeons, in London, United Kingdom, No-vember 30 through December 2, 2011.Copyright © 2012 by the American Society of Plastic Surgeons
DOI: 10.1097/PRS.0b013e31825dc363
Plastic and Reconstructive Surgery
Algorithm for Revision Otoplasty
October
2012
130
4
COSMETIC

908
Plastic and Reconstructive Surgery • October 2012
surgery and operative details were all retrieved from the case notes. A comparative analysis of the case report series was performed (Figs. 1 and 2). Patients were divided into four groups according to revision operation category. Detailed information about ear deformation was collected from photographs from before and after revision otoplasty; thus, patients required preoperative and postoperative photographs to be involved in the study.
The aesthetic result of the revision surgery was assessed by three independent plastic surgery con-sultants, using the Ear Reconstruction Aesthetics Survey, designed by the senior author of the study (K.J.S.). The questionnaire included detailed analysis of the ear shape, using a scale from 1 (very dissatisfied) to 5 (very satisfied) (Table 1). Statistical tests were used to analyze the results. The normality of the groups was assessed with the Shapiro-Wilk test. The parameters, analyzed from the preoperative and postoperative periods, were compared with a t test for dependent samples.
Patient AssessmentAs with any aesthetic surgical procedure,
careful exploration of the patient’s concerns and aspirations is pivotal to achieving a successful outcome. In patients seeking secondary surgery, the challenges of this process might have been
confounded by the disappointments with outcomes from previous operations. Careful evaluation of the patient’s motivations for secondary surgery should be balanced against a realistic assessment of the surgical probabilities. Furthermore, the complexity of the proposed secondary surgery should be balanced against the patient’s tolerance of secondary donor sites, length of surgery, and secondary scarring. Sometimes, for example, a patient will perceive an overcorrected midportion—the so-called telephone ear deformity—to be undercorrected upper and lower poles. Even when the reality of the deformity is demonstrated, patients may prefer a simple procedure to bring the upper and lower poles into planar harmony rather than subject themselves to a complex reconstruction with additional scars.
Many authors have discussed the high inci-dence of body dysmorphic disorder in patients seeking aesthetic surgery.2 We did not include patients in whom we did not undertake revision surgery in this series, but it is the senior author’s experience that there is a significant incidence of irrational body dissatisfaction in patients seeking secondary otoplasty. Young people with relative social instability and lack of functional interper-sonal relationships are classic examples. Patients who volunteer unjustified criticism of their
Fig. 1. Indications for revision otoplasty and the corresponding primary procedure.

Volume 130, Number 4 • Algorithm for Revision Otoplasty
909
previous surgeons are, virtually without excep-tion, poor candidates for further intervention.
Surgical TechniquesPosterior suturing technique with a fascial flap
as described by Horlock et al. was used.3 This was primarily indicated for recurrent prominence or planar disharmony between the upper, middle, or lower poles of the ear. The techniques used for revision otoplasty in essence involve address-ing the anatomical features requiring further set-back or contouring (Fig. 3).4,5 Local anesthesia is infiltrated to the posterior aspect of the ear. The previous posterior scar is incised or excised. Skin is dissected in the subdermal plane to the helical
rim and a fascial flap is raised after incision down to scaphoid cartilage. The above-mentioned com-posite flap of superficial musculoaponeurotic sys-tem and perichondrium is reflected posteriorly to the mastoid periosteum; raising this flap in secondary cases is actually fairly straightforward. Any previous suture material that is felt to be interfering is removed. Sutures are reinserted to adjust areas where there is either contour defi-ciency (e.g., inferior crus, superior crus, antihe-lix) or inadequate rotation (e.g., conchomastoid sutures for the conchal bowl). Therefore, 4-0 Ethibond sutures (Ethicon, Inc., Somerville, N.J.) on a round-bodied needle are placed to augment the antihelical fold (conchoscaphoid
Fig. 2. Algorithm of revision otoplasty techniques, based on the severity of the ear deformity.
Table 1. Detailed Assessment of the Ear Shape before and after Revision Surgery, Performed by Three Independent Plastic Surgery Consultants with Use of the Ear Reconstruction Aesthetics Survey
Before Revision Surgery After Revision Surgery Difference
Parameter Mean SD Mean SD t p*
Helical rim 3.21 0.77 4.54 0.52 –7.87 <0.00001Scaphoid fossa 3.02 0.93 4.61 0.54 –10.43 <0.00001Conchal bowl 2.76 0.92 4.42 0.61 –9.16 <0.00001Antitragus 3.09 0.86 4.42 0.56 –7.32 <0.00001Triangular fossa 3.00 0.88 4.10 0.69 –6.22 <0.00001Antihelix 3.12 0.87 4.58 0.47 –8.84 <0.00001Tragus 4.09 0.51 4.37 0.37 –2.51 <0.02Incisura 3.80 0.45 4.32 0.45 –4.95 <0.00005Lobe 4.06 0.50 4.24 0.51 –1.67 >0.05Size of ear 3.97 0.49 4.28 0.50 –2.58 <0.02Projection of ear 3.06 0.87 4.66 0.45 –9.45 <0.00001Rotation of ear 4.03 0.45 4.40 0.39 –4.66 <0.00005Quality of skin covering ear 4.14 0.45 4.05 0.69 0.66 >0.05Scars around ear 4.06 0.49 4.13 0.42 –0.71 >0.05*Statistically significant difference for values of p < 0.05.

910
Plastic and Reconstructive Surgery • October 2012
sutures), including the upper crus or occasion-ally the lower crus if required, and/or between the mastoid periosteum and the rim of the con-chal bowl (conchomastoid sutures).6,7 Sutures are tied with varying tension to create a progressively more obtuse antihelical fold in the upper pole. Repeated reference is made to the contralateral ear with ruler or caliper calibration as required. The fascial flap is placed back to the indwelling sutures with 5-0 Vicryl Rapide (Ethicon) and the skin is closed. Dressings and sutures are usually retained for 1 week.
Conchal reduction with posterior suturing is indicated either for recurrent ear prominence in the context of a preexistent but unrecognized conchal hypertrophy or for generally stiff carti-lage, the resistance of which is felt to contribute to recurrent prominence (Fig. 4). Local anesthesia is infiltrated to the anterior and posterior surfaces of the ear. Incision is performed on the posterior aspect of the concha, at the junction of the pos-terior conchal wall with the conchal floor.8 The fascial flap is raised as described before. Cartilage is dissected from the posterior conchal skin in the loose areolar plane. To estimate the degree of
conchal hypertrophy, the finger is placed on the antihelix and the ear is set back to its aesthetically pleasing position. The relevant crescent chondro-cutaneous portion of the ear is excised, leaving less cartilage and more skin to ensure tension-free closure. The concha is sutured with one row of 4-0 Ethibond sutures. Conchoscaphoid and concho-mastoid sutures are placed and the skin incision is closed.
Conchal cartilage graft reconstruction is indicated when the structural integrity of the ear is disrupted in a limited area.9 The technique involves graft harvest, usually from the contra-lateral but sometimes ipsilateral ear—usually by means of a posterior approach as described in the conchal reduction technique (Fig. 5). After exposure of the relevant area of cartilage using the anterior or posterior approach and shaving of any contour distortions, the graft is secured to best advantage with 5-0 nonabsorbable sutures.
Ear reconstruction with autologous costal cartilage is indicated for major disruption and deformity of ear cartilage and can consist of one or two stages (Figs. 6 and 7).10 First, an appro-priate amount of cartilage is harvested from
Fig. 3. Technique of posterior suturing otoplasty with fascial flap adjunct. (Above, left) Elliptical skin incision; (above, center) skin excised, fascia incised; (above, right) fascial flap raised; (below, left) conchoscaphoid sutures; and (below, right) conchomastoid sutures.

Volume 130, Number 4 • Algorithm for Revision Otoplasty
911
the chest and placed as a graft to reconstruct the aesthetic appearance of the ear.11,12 Trans-verse incision is followed by exposure of fascia of the rectus abdominis muscle and the external oblique muscle. The two muscles are separated with dissecting scissors and the perichondrium is incised with the scalpel. The elevator is used to undermine the perichondrium, taking special care not to damage the pleura. A Doyen rib raspa-tory is inserted beneath the cartilage at the cos-tochondral junction and the cartilage is incised with the scalpel. Finally, the cartilage is harvested with the help of the raspatory and a hand. Sub-sequently, the harvested block of cartilage is carved and thinned into constructs to replace the deformed areas of anatomy. The remaining blocks of cartilage are cut into approximately 2-mm blocks. The perichondrium is closed with an absorbable suture and the blocks are applied inside the reconstructed cavity with the help of a small funnel. A drain is left behind the muscular layer. The muscle, muscular fascia, and skin are closed with 4-0 sutures. The recipient site is pre-pared after incision, usually from the posterior approach. The deformed portion of auricular cartilage is excised after careful degloving. The new construct is secured to overlapping auricu-lar cartilage with 5-0 nonabsorbable sutures. A drain is applied. The postauricular skin is closed. In cases of total ear reconstruction with insuffi-cient skin envelope or for cartilage atrophy after infection, the second stage of the reconstruction can be required to abduct the ear from the skull. After 6 months, the skin is incised posteriorly and the small skin graft is harvested and secured.
A not uncommon difficulty with revision oto-plasty was the tight skin envelope. This was partic-ularly the case with multiple previous operations. In cases with insufficient auricular skin, skin from the mastoid area or the temporal fascia flap could be used to cover the cartilage.1
RESULTSThirty-six patients met the inclusion criteria
for the study (15 male patients and 21 female patients). Sixty-nine ears in this group had under-gone primary otoplasty and 59 were revised. Patients requiring ear reconstruction with costal cartilage had an average age of 11.7 years (range, 5 to 60 years) at primary otoplasty and 16.34 years (range, 6 to 61 years) at final revision surgery. They waited for surgical correction of the unsuc-cessful primary otoplasty for approximately 4.68 years (range, 0 to 30 years). During this period, they underwent 1.25 operations on average (range, one to four operations).
Primary otoplasty and the final revision opera-tion were performed by different surgeons in 24 cases. The senior author (K.J.S.) performed 17 revision operations, including all ear recon-struction procedures. In four cases, where ear reconstruction with costal cartilage was required, another surgeon had performed the primary oto-plasty. The primary otoplasty techniques included scoring in 13 cases (26 ears) and suturing in 23 cases (43 ears).
Indications for revision otoplasty included recurrent prominence/undercorrection (54 percent), distortion of the scaphoid fossa (21
Fig. 4. Technique of conchal reduction with posterior suturing. (Left) Incision to the lateral aspect of the conchal bowl; (center) partial excision of the contralateral conchal bowl after adjusting the ear prominence with finger; and (right) suturing the cartilage.

912
Plastic and Reconstructive Surgery • October 2012
percent), telephone ear (13 percent), distortion of the antihelical fold (5 percent), and hypertro-phic conchal bowl (7 percent). The indications for revision otoplasty were assessed in relation to the performed primary operation and secondary procedure (Fig. 1). The chosen surgical tech-nique for each patient was performed according to an assessment of their concerns and aspira-tions in line with the proposed protocol of treat-ment. Posterior suturing with the fascial flap adjunct was used in 73 percent of revision oto-plasties, conchal bowl reduction was used in 11 percent, costal cartilage graft was used in 11 per-cent, conchal bowl graft was used in 3 percent, and shaving scaphoid fossa was used in 2 per-cent. Revision posterior suturing was performed for prominence in 46 percent, for telephone ear in 10 percent, for distortion of scaphoid fossa in
7 percent, and for distortion of antihelical fold in 5 percent. Conchal bowl grafting was per-formed for distortion of the scaphoid fossa in 2 percent. The most complex procedure of ear reconstruction was performed for distortion of scaphoid fossa in 10 percent and telephone ear in 3 percent. No complications were reported in the early postoperative period (14 days after surgery).
The average follow-up was 37 ± 11 months. All but two patients were delighted with the results of the revision surgery, including all patients sub-jected to ear reconstruction. Detailed assessment of the revision surgery aesthetic outcomes, per-formed by three independent plastic surgery con-sultants, is presented in Table 1.
Four instructive cases requiring ear recon-struction with costal cartilage are presented
Fig. 5. Technique of conchal cartilage graft. (Above, left) Left auricle with distorted scaphoid fossa in the upper pole; (above, right) harvested conchal bowl cartilage from the right ear (as presented in Fig. 4); (below, left) dressing of the posterior aspect of right auricle; and (below, right) placing the conchal cartilage graft to the posterior aspect of left auricle.

Volume 130, Number 4 • Algorithm for Revision Otoplasty
913
briefly here, all after the primary anterior scoring technique. The first patient had bilateral absence of the scaphoid fossa at the upper poles after anterior scoring. She presented with recurrent prominence at the upper poles with ear defor-mity. There was absence of scaphoid fossa at the upper poles, with very little support to the helical rims, leading to very constricted upper poles. The second patient had helical rim collapsed bilater-ally as the scaphoid fossa cartilage of each ear
bent over. Because of a lack of support, the heli-cal rim collapsed in its midportion. The patient had undergone two previous revision opera-tions. Extensive mastoid cutaneous scarring was observed. In the third case, recurrent telephone ears were observed after two revision operations. The fourth patient sustained bilateral loss of the upper lateral aspect of helical rims and sharp folding of scaphoid fossa on the right side. On examination, there was loss of the upper lateral
Fig. 6. Technique of ear reconstruction with costal cartilage. (Above, second row, and third row) First stage; (above, left) dissection of plane between rectus abdominis and external oblique mus-cles; (above, center) incision of the anterior aspect of the perichondrium; (above, right) under-mining the perichondrium from the anterior and posterior aspects of the ribs; (second row, left) incised costal cartilage, secured by Doyben rib raspatory, at the costochondral junction; (second row, center) removal of the dissected costal cartilage; (second row, right) cutting excessive pieces of the costal cartilage into 2-mm blocks and placing them into sutured cavity of the perichondrium; (below, left) usual donor site for ear reconstruction with costal cartilage; (below, right) carved piece of costal cartilage, which is placed beneath the skin envelope (if possible). (Reprinted from Kawa-nabe Y, Nagata S. A new method of costal cartilage harvest for total auricular reconstruction: Part I. Avoidance and prevention of intraoperative and postoperative complications and problems. Plast Reconstr Surg. 2006;117:2011–2018.).

914
Plastic and Reconstructive Surgery • October 2012
aspect of helical rim of both ears, with thinning of overlying skin.
DISCUSSIONMost primary otoplasty techniques fall into
two main categories: suturing and scoring.6,7,13,14 The most popular primary technique of the first group—anterior scoring—has a relatively high complication rate, including irreversible ear con-tour deformities caused by cartilage irregulari-ties, unpredictable scar tissue contraction, and cartilage remodeling.4,15,16 In the excellent study concerning ear reconstruction after otoplasty, Firmin et al. could draw no definitive correla-tion between the primary technique used and the resulting complication, because only one of the patients had referral records and details of the original operation.10 In our study, we could draw such conclusions because we had full records for each case. After primary anterior scoring, the incised scaphoid cartilage has a tendency to fold back onto itself. This leads to a loss of the width of the scaphoid, irregularities of the helical rim, and a narrow upper pole, and were observed in this series (Fig. 1). In addition, in all our cases requir-ing ear reconstruction with costal cartilage, ante-rior scoring was used as primary otoplasty.
In contrast, patients after primary otoplasty with suturing techniques had mostly reversible complications, such as prominence. The con-chal bowl hypertrophy was observed in the sec-ond group because there was no primary surgical interference to predefined enlarged cartilage. We have previously demonstrated a long-term recur-rence rate of 8.0 percent in prominent ears cor-rected by posterior suturing and 4.8 percent in those corrected by posterior suturing refined with a posterior fascial flap.4 This is generally a safe and simple method of revision otoplasty. Major cartilaginous irregularity or disruption was not seen with primary suturing otoplasty techniques and therefore complex reconstructions were not required (Fig. 1).
It is noteworthy that a straw poll of the interna-tional community of ear reconstruction surgeons shows nearly universal preference for suturing techniques as the preferred primary otoplasty method. In other words, those called on most fre-quently to rectify the most severe complications of otoplasty recognize the greater potential for harm with an anterior scoring technique.
Indications for revision surgery of the auricle include ear deformations after primary otoplasty.
In our study, the majority of patients wanted sec-ondary treatment because of prominence or undercorrection. However, technique-related ear deformities were also observed bilaterally, such as distortion of scaphoid fossa, distortion of antihe-lical fold, hypertrophic conchal bowl, and tele-phone ear.
The surgical technique required for revision otoplasty depends on the severity of the ear defor-mity (Fig. 2). Clearly, individual surgeons should offer only surgical techniques with which they are experienced and competent. If a more complex procedure such as costal cartilage reconstruction is indicated, appropriate referral may be consid-ered. Other authors have suggested algorithms to treat the complications after primary otoplasty that do not extend to the use of costal cartilage.17 In our series, we proposed a wide range of options concerning revision surgery of the auricle, which allowed us to achieve pleasing aesthetic outcomes (Table 1). The majority of revision operations included otoplasty with posterior suturing tech-nique and fascial flap. Moreover, patients were subjected to conchal bowl reduction, shaving of scaphoid fossa, conchal cartilage graft, and ear reconstruction with costal cartilage. Based on the obtained results, an algorithm is suggested that addresses the variety of postotoplasty ear deforma-tions, including the most severe along with sug-gested interventions (Fig. 2).
In revision surgery, undercorrection, recur-rence, and overcorrection shortly after primary otoplasty are usually addressed with simple tech-niques such as suture revision and conchal reduc-tion (Figs. 3 and 4).6,8 In all revision otoplasties with posterior suturing, good postoperative results were obtained. Conchal bowl reduction is indicated in cases where stiff cartilage contributes to recurrent prominence or where an enlarged conchal bowl is diagnosed (Fig. 4).18
Overcorrection deformities and minor car-tilage irregularities after primary otoplasty can necessitate conchal cartilage grafting (Fig. 5). Isolated deformities of the helix or scapha are considered here. Lentz et al. performed ear reconstruction with conchal cartilage that was harvested using the anterior approach.17 We believe that the posterior approach is sufficient for both harvesting and placing the conchal car-tilage and avoids any scarring in the anterior aspect of the ear. In our study, only one patient was treated with the above-mentioned type of ear reconstruction for isolated unilateral distortion of the scaphoid fossa.
Volume 130, Number 4 • Algorithm for Revision Otoplasty
915
Severe complications require ear reconstruc-tion with autologous costal cartilage (Figs. 6 and 7). Costal cartilage grafting is the most complex, challenging type of ear reconstruction, and requires excellence in understanding the ear shape and the importance of the overlying skin. Firmin at al. used costal cartilage grafts for vari-ous defects of the ear, including the antihelix, helix, combined helix and antihelix; posterior wall of the concha; and combined scapha, helix, and antihelix.10 In the present report, ear recon-struction was necessary because of severe defor-mity of the helical rim, scaphoid fossa, triangular fossa, antihelix, conchal bowl, or a combination of the above.
Conclusions with regard to the epidemiologic relationship between the primary technique and the necessity for revision surgery cannot be derived from these data.4 A local preference for primary otoplasty over the past decade has been posterior suturing. The relative incidence of recurrence reflects the practice of correcting this issue locally. The senior author offers an ear reconstruction service to patients for the whole of Scotland and receives referrals from elsewhere in the United Kingdom. Patients referred from this wider catchment area tended to have more severe complications and by virtue of locally
preferred practice may have had anterior scoring techniques.
CONCLUSIONSDetermining the patient’s hopes and expec-
tations is essential. Therefore, a variety of tech-niques should be used, based on how best to address patient desires. However, surgeons should be aware of body dysmorphic disorder. In relation to the surgical technique of primary otoplasty, correction of the irreversible complications after anterior scoring is far more difficult. For severe cases of deformity, reconstruction with costal cartilage may even be indicated. In all cases, ade-quacy of the skin envelope is a major determinant of outcome. The algorithm for revision surgery after primary otoplasty, proposed in our article, addresses the whole variety of ear deformations, providing the surgical options available to address these abnormalities.
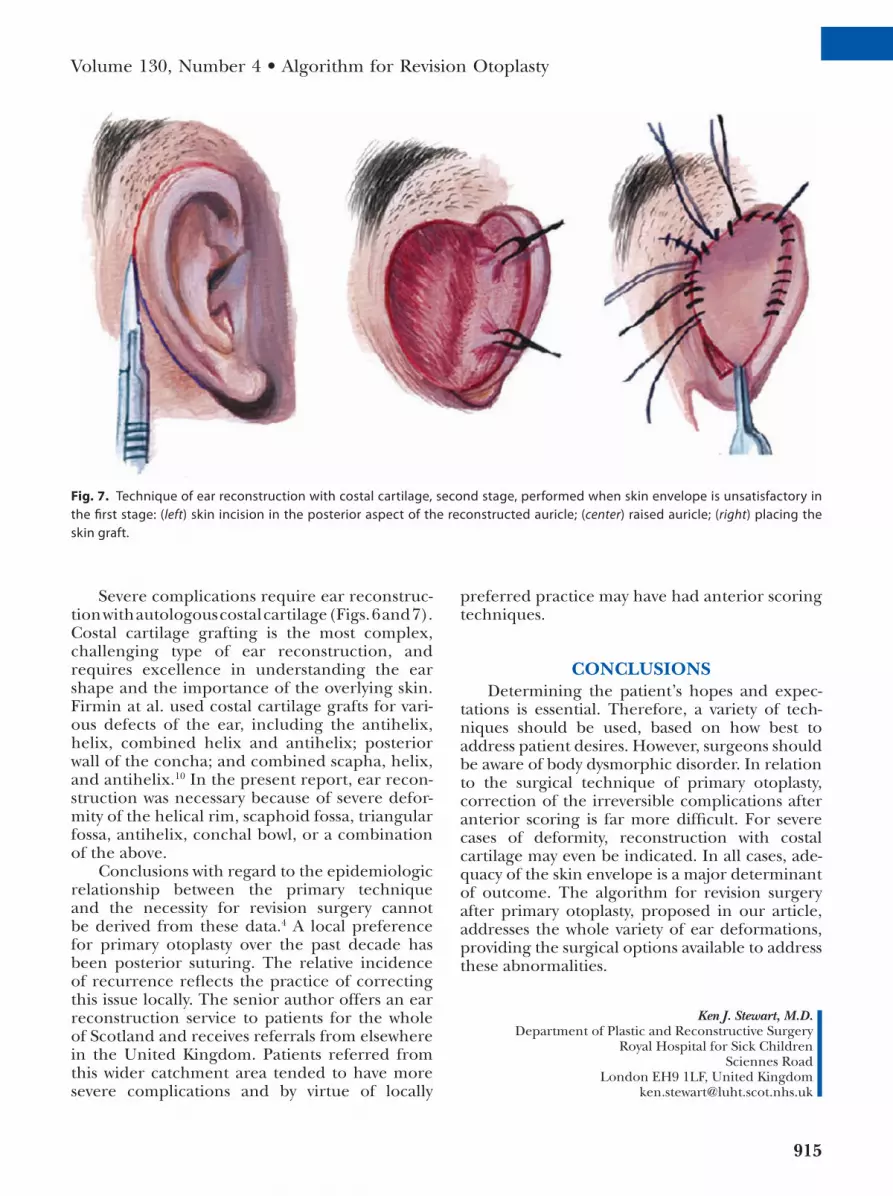
Fig. 7. Technique of ear reconstruction with costal cartilage, second stage, performed when skin envelope is unsatisfactory in the first stage: (left) skin incision in the posterior aspect of the reconstructed auricle; (center) raised auricle; (right) placing the skin graft.
Ken J. Stewart, M.D.Department of Plastic and Reconstructive Surgery
Royal Hospital for Sick ChildrenSciennes Road
London EH9 1LF, United [email protected]

916
Plastic and Reconstructive Surgery • October 2012
REFERENCES 1. Hackney FL. Plastic surgery of the ear. Select Read Plast Surg.
2001;16:1–31. 2. Gorney M. Recognition and management of the patient
unsuitable for aesthetic surgery. Plast Reconstr Surg. 2010;126:2268–2271.
3. Horlock N, Misra A, Gault DT. The postauricular fascial flap as an adjunct to Mustardé and Furnas type otoplasty. Plast Reconstr Surg. 2001;108:1487–1490.
4. Mandal A, Bahia H, Ahmad T, Stewart KJ. Comparison of cartilage scoring and cartilage sparing otoplasty: A study of 203 cases. J Plast Reconstr Aesthet Surg. 2006;59: 1170–1176.
5. Schaverien MV, Al-Busaidi S, Stewart KJ. Long-term results of posterior suturing with postauricular fascial flap otoplasty. J Plast Reconstr Aesthet Surg. 2010;63:1447–1451.
6. Mustarde JC. The correction of prominent ears using simple mattress sutures. Br J Plast Surg. 1963;16:170–178.
7. Furnas DW. Correction of prominent ears by buried con-chamastoid sutures. Plast Reconstr Surg. 1968;42:189–193.
8. Bauer BS, Margulis A, Song DH. The importance of conchal resection in correcting the prominent ear. Aesthet Surg J. 2005;25:72–79.
9. Han K, Kim J, Son D, Park B. How to harvest the maximal amount of conchal cartilage grafts. J Plast Reconstr Aesthet Surg. 2008;61:1465–1471.
10. Firmin F, Sanger C, O’Toole G. Ear reconstruction following severe complications of otoplasty. J Plast Reconstr Aesthet Surg. 2008;61(Suppl 1):S13–S20.
11. Kawanabe Y, Nagata S. A new method of costal cartilage har-vest for total auricular reconstruction: Part I. Avoidance and prevention of intraoperative and postoperative complica-tions and problems. Plast Reconstr Surg. 2006;117:2011–2018.
12. Kawanabe Y, Nagata S. A new method of costal cartilage har-vest for total auricular reconstruction: Part II. Evaluation and analysis of the regenerated costal cartilage. Plast Reconstr Surg. 2007;119:308–315.
13. Kelley P, Hollier L, Stal S. Otoplasty: Evaluation, technique, and review. J Craniofac Surg. 2003;14:643–653.
14. Widgerow AD. Revision otoplasty: The contracted antihelical fold. Plast Reconstr Surg. 2002;110:827–830.
15. Rubino C, Farace F, Figus A, Masia DR. Anterior scoring of the upper helical cartilage as a refinement in aesthetic oto-plasty. Aesthetic Plast Surg. 2005;29:88–93; discussion 94.
16. Limandjaja GC, Breugem CC, Mink van der Molen AB, Kon M. Complications of otoplasty: A literature review. J Plast Reconstr Aesthet Surg. 2009;62:19–27.
17. Lentz AK, Plikaitis CM, Bauer BS. Understanding the unfa-vorable result after otoplasty: An integrated approach to cor-rection. Plast Reconstr Surg. 2011;128:536–544.
18. Elliott RA Jr. Complications in the treatment of prominent ears. Clin Plast Surg. 1978;5:479–490.





























