Embed Size (px)
Citation preview

Simultaneous functional and fixed appliance therapy for growth modificationand dental alignment prior to prosthetic habilitation in hypohidroticectodermal dysplasia: A clinical report
Sunjay Suri, BDS, MDS,a Robert P. Carmichael, BSc, DMD, MSc,b and Bryan D. Tompson, DDSc
Oral Health Sciences Center, Post Graduate Institute of Medical Education and Research,Chandigarh, India; Department of Dentistry, Hospital for Sick Children, Toronto, Canada;University of Toronto, Toronto, Canada; The Bloorview MacMillan Children’s Centre,Toronto, Canada
This clinical report describes the simultaneous use of functional and fixed appliances to modify thepattern of dentofacial development and align teeth in preparation for prosthodontic habilitation ofa growing child with hypohidrotic ectodermal dysplasia. The treatment objective was to create a morefavorable starting point for the prosthodontic phase of habilitation by improving the sagittal and verticalskeletal relationships and facial esthetics. This was accomplished through growth modification withfunctional appliances conducted simultaneously with eruption of maxillary and mandibular molars,dental arch expansion, alignment, and space management using fixed orthodontic appliances.Orthodontic retention was accomplished by means of removable partial dentures. A second phase oforthodontics conducted closer to the age of skeletal maturation will aim at definitive tooth alignment inpreparation for dental implant-supported restorations. (J Prosthet Dent 2004;92:428-33.)
Ectodermal dysplasia (ED) is a congenital syndromecharacterized chiefly by abnormalities of tissues of ecto-dermal origin, namely skin, nails, hair, and teeth.1,2
There are more than 150 different variants of ED.3
Ectodermal dysplasia is usually described as being hy-pohidrotic or hidrotic, depending upon the degree ofsweat gland function. Hypohidrotic ectodermal dyspla-sia (HED) frequently exhibits the most severe dentalanomalies; thus, clinical management is of interest tothe prosthodontist and orthodontist. HED is character-ized by hypohidrosis, hypotrichosis, and hypodontiaand occurs with a frequency of 1/100,000 births.4 Itaffects men severely, while women carriers and hetero-zygotes usually show minor defects, although the com-plete syndrome has also been reported in women.1,5,6
The classical facial features of HED include frontalbossing, depressed nasal bridge, reduced vertical facialheight and facial depth, small palatal and cranial basewidths, small malar processes, and high-set orbits.7
The most striking oral feature of HED is the absenceof most deciduous and permanent teeth. The averagenumber of missing permanent teeth is reported as23.7.8 The maxillary central incisors, maxillary first mo-lars, mandibular first molars, and maxillary canines arethe teeth most often present.9,10 The maxillary central
aAssistant Professor, Division of Orthodontics, Oral Health SciencesCenter, Post Graduate Institute of Medical Education andResearch. Former Clinical Fellow, Division of Orthodontics,Department of Dentistry, Hospital for Sick Children.
bAssistant Professor, Discipline of Prosthodontics, University ofToronto; Coordinator of Prosthodontics, Hospital for SickChildren and The Bloorview MacMillan Children’s Centre.
cAssociate Professor and Head, Division of Orthodontics, De-partment of Dentistry, Hospital for Sick Children.
428 THE JOURNAL OF PROSTHETIC DENTISTRY
incisors and the maxillary and mandibular canines areusually conical in shape. The alveolar process fails to de-velop at edentulous sites11,12 and may be poorly devel-oped even at dentate sites.13 The deficient alveolargrowth and decreased vertical dimension of occlusionresults in a small lower vertical face height.14 Thesefeatures give the child a distinctly aged facial appearancesimilar to an edentulous patient. Diminished salivary se-cretion,11 dry oral mucosa, and hoarse voice quality havealso been reported.12,15 The psychological, psychoso-cial, and functional effects of HED can have a tremen-dous negative impact on a young individual.
Dental management of ectodermal dysplasia patientstraditionally focuses on provision of a series of completeor removable partial dentures (RPDs) during the grow-ing years5,16-22 and definitive habilitation followingcompletion of jaw growth.10,23,24 The use of functionalorthopedic appliances to modify the pattern of jawgrowth in HED is usually not a part of the dental treat-ment protocol. The intent of this clinical report is tohighlight the simultaneous use of functional and fixedappliances to modify the pattern of dentofacial develop-ment and align teeth in preparation for prosthodontichabilitation of a child with hypohidrotic ectodermal dys-plasia.
CLINICAL REPORT
A 10-year-old Asian boy with HED was referred dueto multiple missing teeth. On examination, the patientpresented with the classical triad of hypohidrosis, hy-potrichosis, and hypodontia (Figs. 1 and 2). The mostremarkable facial features were decreased lower anteriorfacial height, flat mandibular plane, prominent chin anda resultant concave facial profile. There was insufficient
VOLUME 92 NUMBER 5
THE JOURNAL OF PROSTHETIC DENTISTRYSURI, CARMICHAEL, AND TOMPSON
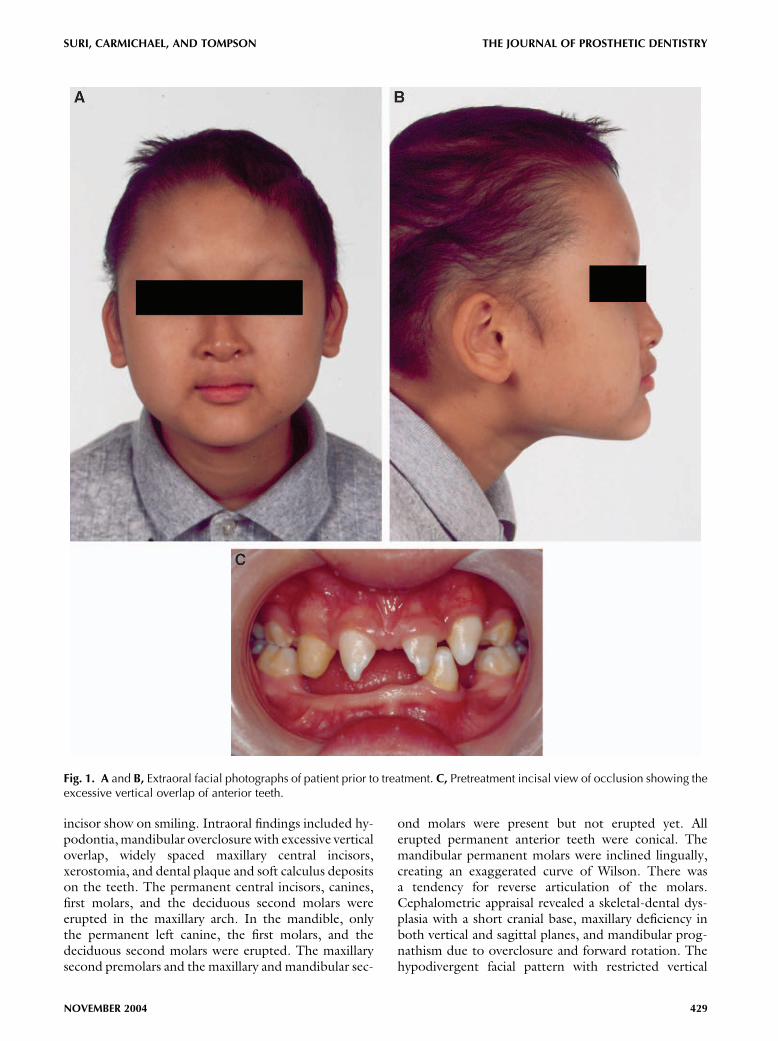
Fig. 1. A and B, Extraoral facial photographs of patient prior to treatment. C, Pretreatment incisal view of occlusion showing theexcessive vertical overlap of anterior teeth.
incisor show on smiling. Intraoral findings included hy-podontia,mandibular overclosure with excessive verticaloverlap, widely spaced maxillary central incisors,xerostomia, and dental plaque and soft calculus depositson the teeth. The permanent central incisors, canines,first molars, and the deciduous second molars wereerupted in the maxillary arch. In the mandible, onlythe permanent left canine, the first molars, and thedeciduous second molars were erupted. The maxillarysecond premolars and the maxillary and mandibular sec-
NOVEMBER 2004
ond molars were present but not erupted yet. Allerupted permanent anterior teeth were conical. Themandibular permanent molars were inclined lingually,creating an exaggerated curve of Wilson. There wasa tendency for reverse articulation of the molars.Cephalometric appraisal revealed a skeletal-dental dys-plasia with a short cranial base, maxillary deficiency inboth vertical and sagittal planes, and mandibular prog-nathism due to overclosure and forward rotation. Thehypodivergent facial pattern with restricted vertical
429
THE JOURNAL OF PROSTHETIC DENTISTRY SURI, CARMICHAEL, AND TOMPSON
development of the lower anterior face height, coupledwith the forward rotation and prognathic mandible,compounded the skeletal Class III pattern. Dentally,the maxillary and mandibular molars and the maxillaryincisors were undererupted. Both upper and lower lipswere protruded, and the chin was prominent.
Treatment options considered for this child includedconstructing removable partial dentures after reshapingthe conical maxillary central incisors with composite.However, the excessive vertical overlap, the wide spacebetween the central incisors, the undereruptedmaxillaryand mandibular molars, and the lingually inclined man-dibular molars with tendency for reverse articulation ofthe molars militated against this as the preferred choiceof treatment. It was considered that osseointegrated im-plants would play a significant role in the definitive res-toration of the occlusion. However, as the youngpatient was growing, it was decided to defer the defini-tive restorative phase, including the placement ofimplants, until after the completion of jaw growth andalignment of the existing natural teeth in desiredpositions. To use the facial growth in this growing childto advantage, functional appliance therapy was selectedto redirect and modify mandibular growth. It was deter-mined that this would be conducted simultaneouslywith orthodontic eruption of the maxillary and mandib-ular molars, maxillary dental alignment, and space distri-bution using fixed orthodontic appliances. Insertion ofRPDs was planned following the completion of the or-thodontic phase, whichwould also serve to retain the or-thodontic result. In addition, a second phase oforthodontics aimed at definitive tooth alignment wouldbe undertaken after the complete eruption of the perma-nent dentition, in preparation for dental implant–supported prostheses.
Treatment was initiated by cementing bands(American Orthodontics, Sheboygan, Wis) with lingualbuttons on the permanent first molars. The maxillarycentral incisors were recontoured with composite(Single Bond Dental Adhesive; 3M composite Z100Restorative; 3M ESPE, St. Paul, Minn) bonded to theteeth. A wax interocclusal record providing 4mm poste-rior clearance was made to construct a maxillary func-
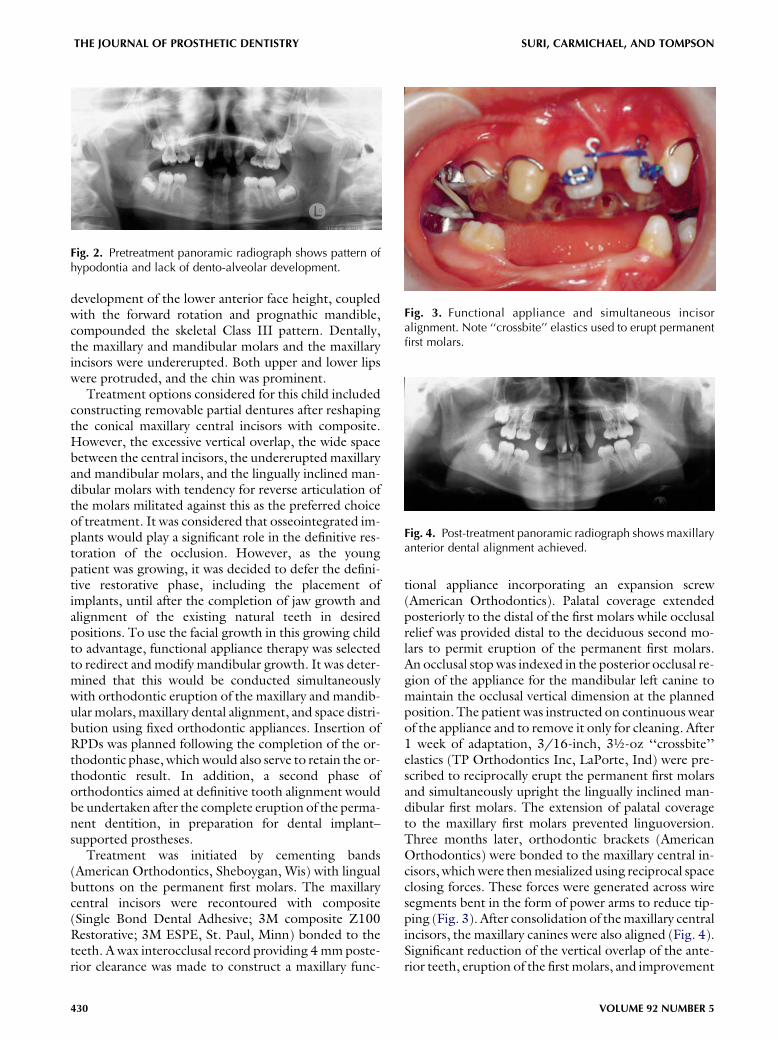
Fig. 2. Pretreatment panoramic radiograph shows pattern ofhypodontia and lack of dento-alveolar development.
430
tional appliance incorporating an expansion screw(American Orthodontics). Palatal coverage extendedposteriorly to the distal of the first molars while occlusalrelief was provided distal to the deciduous second mo-lars to permit eruption of the permanent first molars.An occlusal stopwas indexed in the posterior occlusal re-gion of the appliance for the mandibular left canine tomaintain the occlusal vertical dimension at the plannedposition. The patient was instructed on continuous wearof the appliance and to remove it only for cleaning. After1 week of adaptation, 3/16-inch, 3½-oz ‘‘crossbite’’elastics (TP Orthodontics Inc, LaPorte, Ind) were pre-scribed to reciprocally erupt the permanent first molarsand simultaneously upright the lingually inclined man-dibular first molars. The extension of palatal coverageto the maxillary first molars prevented linguoversion.Three months later, orthodontic brackets (AmericanOrthodontics) were bonded to the maxillary central in-cisors, whichwere thenmesialized using reciprocal spaceclosing forces. These forces were generated across wiresegments bent in the form of power arms to reduce tip-ping (Fig. 3). After consolidation of themaxillary centralincisors, the maxillary canines were also aligned (Fig. 4).Significant reduction of the vertical overlap of the ante-rior teeth, eruption of the first molars, and improvement
Fig. 3. Functional appliance and simultaneous incisoralignment. Note ‘‘crossbite’’ elastics used to erupt permanentfirst molars.
Fig. 4. Post-treatment panoramic radiograph shows maxillaryanterior dental alignment achieved.
VOLUME 92 NUMBER 5
THE JOURNAL OF PROSTHETIC DENTISTRYSURI, CARMICHAEL, AND TOMPSON
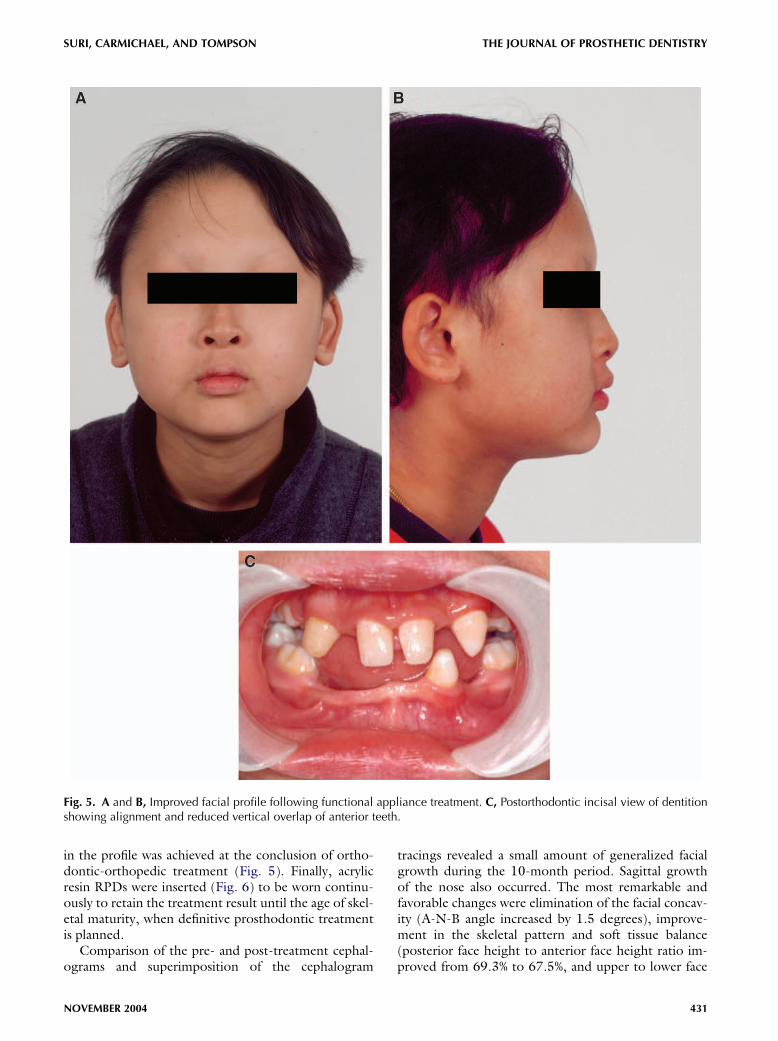
Fig. 5. A and B, Improved facial profile following functional appliance treatment. C, Postorthodontic incisal view of dentitionshowing alignment and reduced vertical overlap of anterior teeth.
in the profile was achieved at the conclusion of ortho-dontic-orthopedic treatment (Fig. 5). Finally, acrylicresin RPDs were inserted (Fig. 6) to be worn continu-ously to retain the treatment result until the age of skel-etal maturity, when definitive prosthodontic treatmentis planned.
Comparison of the pre- and post-treatment cephal-ograms and superimposition of the cephalogram
NOVEMBER 2004
tracings revealed a small amount of generalized facialgrowth during the 10-month period. Sagittal growthof the nose also occurred. The most remarkable andfavorable changes were elimination of the facial concav-ity (A-N-B angle increased by 1.5 degrees), improve-ment in the skeletal pattern and soft tissue balance(posterior face height to anterior face height ratio im-proved from 69.3% to 67.5%, and upper to lower face
431
THE JOURNAL OF PROSTHETIC DENTISTRY SURI, CARMICHAEL, AND TOMPSON
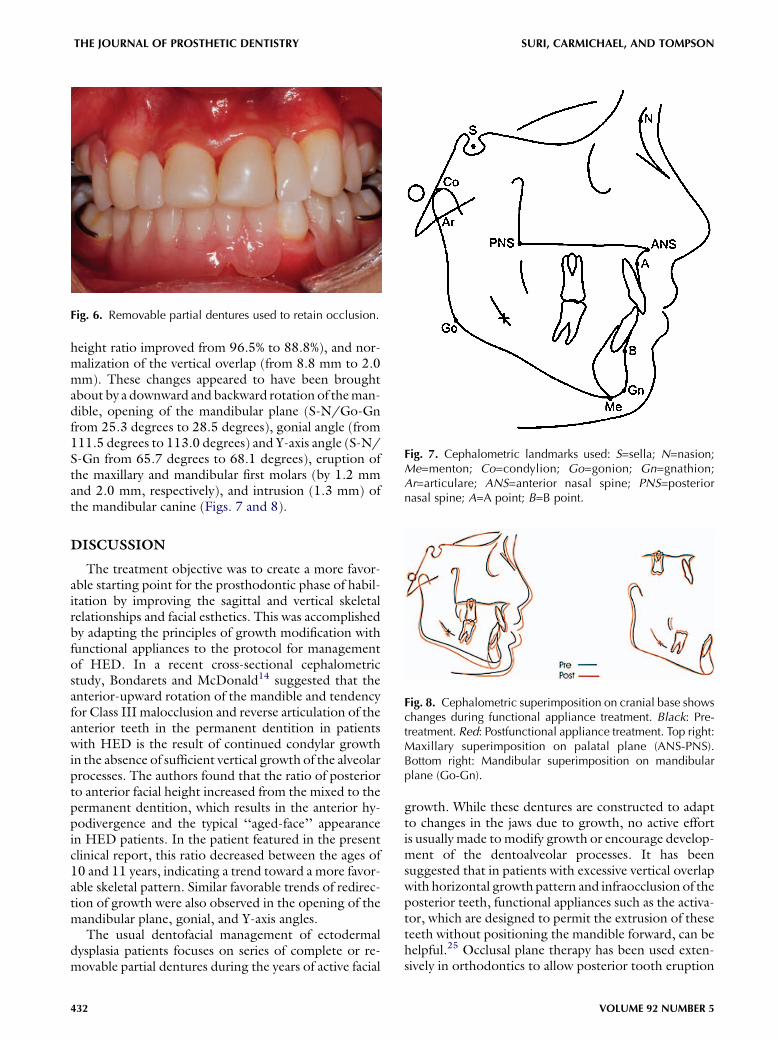
height ratio improved from 96.5% to 88.8%), and nor-malization of the vertical overlap (from 8.8 mm to 2.0mm). These changes appeared to have been broughtabout by a downward and backward rotation of theman-dible, opening of the mandibular plane (S-N/Go-Gnfrom 25.3 degrees to 28.5 degrees), gonial angle (from111.5 degrees to 113.0 degrees) and Y-axis angle (S-N/S-Gn from 65.7 degrees to 68.1 degrees), eruption ofthe maxillary and mandibular first molars (by 1.2 mmand 2.0 mm, respectively), and intrusion (1.3 mm) ofthe mandibular canine (Figs. 7 and 8).
DISCUSSION
The treatment objective was to create a more favor-able starting point for the prosthodontic phase of habil-itation by improving the sagittal and vertical skeletalrelationships and facial esthetics. This was accomplishedby adapting the principles of growth modification withfunctional appliances to the protocol for managementof HED. In a recent cross-sectional cephalometricstudy, Bondarets and McDonald14 suggested that theanterior-upward rotation of the mandible and tendencyfor Class III malocclusion and reverse articulation of theanterior teeth in the permanent dentition in patientswith HED is the result of continued condylar growthin the absence of sufficient vertical growth of the alveolarprocesses. The authors found that the ratio of posteriorto anterior facial height increased from the mixed to thepermanent dentition, which results in the anterior hy-podivergence and the typical ‘‘aged-face’’ appearancein HED patients. In the patient featured in the presentclinical report, this ratio decreased between the ages of10 and 11 years, indicating a trend toward a more favor-able skeletal pattern. Similar favorable trends of redirec-tion of growth were also observed in the opening of themandibular plane, gonial, and Y-axis angles.
The usual dentofacial management of ectodermaldysplasia patients focuses on series of complete or re-movable partial dentures during the years of active facial
Fig. 6. Removable partial dentures used to retain occlusion.
432
growth. While these dentures are constructed to adaptto changes in the jaws due to growth, no active effortis usually made tomodify growth or encourage develop-ment of the dentoalveolar processes. It has beensuggested that in patients with excessive vertical overlapwith horizontal growth pattern and infraocclusion of theposterior teeth, functional appliances such as the activa-tor, which are designed to permit the extrusion of theseteeth without positioning the mandible forward, can behelpful.25 Occlusal plane therapy has been used exten-sively in orthodontics to allow posterior tooth eruption
Fig. 7. Cephalometric landmarks used: S=sella; N=nasion;Me=menton; Co=condylion; Go=gonion; Gn=gnathion;Ar=articulare; ANS=anterior nasal spine; PNS=posteriornasal spine; A=A point; B=B point.
Fig. 8. Cephalometric superimposition on cranial base showschanges during functional appliance treatment. Black: Pre-treatment. Red: Postfunctional appliance treatment. Top right:Maxillary superimposition on palatal plane (ANS-PNS).Bottom right: Mandibular superimposition on mandibularplane (Go-Gn).
VOLUME 92 NUMBER 5

THE JOURNAL OF PROSTHETIC DENTISTRYSURI, CARMICHAEL, AND TOMPSON
and development of the dentoalveolar process.26,27
Extrusion of themaxillary andmandibularmolars resultsin opening of the Y axis and increase of the A-N-Bangle.28 For patients in whom anterior rotation is tobe expected, the goal of orthodontic treatment shouldbe to establish and maintain normal horizontal overlapand vertical overlap. Retention of the occlusion at theend of treatment is necessary, and in extreme situations,must be continued until growth at the condyles is com-pleted.29 In the presented patient, withmissingmandib-ular incisors, a positive incisal contact was providedthrough the mandibular denture teeth occluding withthe maxillary incisors. The RPDs will be worn until thecompletion of facial growth, at which time a secondphase of treatment to prepare for dental implant-supported restorations will be initiated. During the in-tervening period, the patient will be followed up clini-cally, with cephalometric growth assessment asnecessary, and any orthodontic or orthopedic guidancewill be reinstituted if required.
SUMMARY
Individuals with hypohidrotic ectodermal dysplasiaare routinely managed by a series of dentures duringthe growing years and definitive habilitation followingthe completion of jaw growth. Functional and fixed or-thodontic appliances were used to modify the pattern ofdentofacial development and to align teeth in prepara-tion for prosthodontic habilitation of a growing childwithHED. Sagittal and vertical dentofacial relationshipsand facial esthetics were significantly improved withgrowth modification, controlled eruption of the maxil-lary and mandibular molars, and dental alignment andspace management using limited fixed and removableappliances. This treatment sequence was helpful in max-imizing the treatment outcome and addressing thepatient’s functional and esthetic needs.
REFERENCES
1. Gorlin RJ, Cohen MM, Hennekam RCM, editors. Syndromes of the head
and neck. 4th ed. New York: Oxford University Press; 2001. p. 540-5.
2. Bergsma D, editor. Birth defects compendium. 2nd ed. New York: Alan
Liss; 1979. p. 92.
3. Pinheiro M, Freire-Maia N. Ectodermal dysplasias: a clinical classification
and a causal review. Am J Med Genet 1994;53:153-62.
4. Clarke A. Hypohidrotic ectodermal dysplasia. J Med Genet 1987;24:
659-63.
5. Herer PD. Treatment of anhidrotic ectodermal dysplasia: report of case.
J Dent Child 1975;42:133-6.
6. Ali G, Kumar M, Verma R, Khajuria V, Wadhwa MB. Anhidrotic ectoder-
mal dysplasia (Christ-Seimens-Touraine syndrome)—case report with a re-
view. Indian J Med Sci 2000;54:541-4.
7. Bixler D, Saksena SS, Ward RE. Characterization of the face in hypohi-
drotic ectodermal dysplasia by cephalometric and anthropometric analy-
sis. Birth Defects Orig Artic Ser 1988;24:197-203.
8. Crawford PJ, Aldred MJ, Clarke A. Clinical and radiographic dental find-
ings in X-linked hypohidrotic ectodermal dysplasia. J Med Genet 1991;
28:181-5.
NOVEMBER 2004
9. Nakata M, Koshiba H, Eto K, Nance WE. A genetic study of anodontia in
X-linked hypohidrotic ectodermal dysplasia. Am J Hum Genet 1980;32:
908-19.
10. Guckes AD, Roberts MW, McCarthy GR. Pattern of permanent teeth pres-
ent in individuals with ectodermal dysplasia and severe hypodontia sug-
gests treatment with dental implants. Pediatr Dent 1998;20:278-80.
11. Everett FG, Jump EB, Sutherland WF, Savara BS, Suher T. Anhidrotic ecto-
dermal dysplasia with anodontia: a study of two families. J Am Dent Assoc
1952;44:173-86.
12. Soderholm AL, Kaitila I. Expression of X-linked hypohidrotic ectodermal
dysplasia in six males and in their mothers. Clin Genet 1985;28:136-44.
13. Tape MW, Tye E. Ectodermal dysplasia: literature review and a case re-
port. Compend Contin Educ Dent 1995;16:524-8.
14. Bondarets N, McDonald F. Analysis of the vertical facial form in patients
with severe hypodontia. Am J Phys Anthropol 2000;111:177-84.
15. Peterson-Falzone SJ, Caldarelli DD, Landahl KL. Abnormal laryngeal vo-
cal quality in ectodermal dysplasia. Arch Otolaryngol 1981;107:300-4.
16. Sarnat BG, Brodie AG, Kubacki WH. Fourteen-year report of facial growth
in case of complete anodontia with ectodermal dysplasia. AMA Am J Dis
Child 1953;86:162-9.
17. Tocchini JJ, West FT, Bartlett RW. An unusual developmental pattern in
a case of hypohidrotic ectodermal dysplasia. ASDC J Dent Child 1970;
37:158-9.
18. Nortje CJ, Farman AG, Thomas CJ, Watermeyer GJ. X-linked hypohidrotic
ectodermal dysplasia- An unusual prosthetic problem. J Prosthet Dent
1978;40:137-42.
19. Shaw RM. Prosthetic management of hypohidrotic ectodermal dysplasia
with anodontia. Case report. Austr Dent J 1990;35:113-6.
20. Boj JR, Duran J, Cortada M, Jimenez A, Golobart J. Cephalometric
changes in a patient with ectodermal dysplasia after placement of den-
tures. J Clin Pediatr Dent 1993;17:217-20.
21. Franchi L, Branchi R, Tollaro I. Craniofacial changes following early pros-
thetic treatment in a case of hypohidrotic ectodermal dysplasia with com-
plete anodontia. ASDC J Dent Child 1998;65:116-21.
22. Itthagarun A, King NM. Oral rehabilitation of a hypohidrotic ectodermal
dysplasia patient: a 6-year follow-up. Quintessence Int 2000;31:642-8.
23. Guckes AD, Brahim JS, McCarthy GR, Rudy SF, Cooper LF. Using endo-
sseous dental implants for patients with ectodermal dysplasia. J Am Dent
Assoc. 1991;122:59-62.
24. Davarpanah M, Moon JW, Yang LR, Celletti R, Martinez H. Dental im-
plants in the oral rehabilitation of a teenager with hypohidrotic ectoder-
mal dysplasia: report of a case. Int J Oral Maxillofac Implants 1997;12:
252-8.
25. Graber TM, Rakosi T, Petrovic AG. Dentofacial orthopedics with func-
tional appliances. 2nd ed. St. Louis: Mosby; 1997. p. 182.
26. Hemley S. Bite Plates: Their application and action. Am J Orthod 1938;
24:721-36.
27. Sleichter CG. Effects of maxillary bite plane therapy in orthodontics. Am J
Orthod 1954;40:850-70.
28. Stockli PW, Teuscher UM. Combined activator headgear orthopedics. In:
Graber TM, Vanarsdall RL, editors. Orthodontics: Current Principles and
Techniques. 2nd ed. St. Louis: Mosby; 1994. p. 440.
29. Nielsen IL. Growth considerations in stability of orthodontic treatment. In:
Nanda R, Burstone CJ, editors. Retention and stability in orthodontics.
Philadelphia: WB Saunders; 1993. p. 9-34.
Reprint requests to:
DR ROBERT P. CARMICHAEL
BLOORVIEW MACMILLAN CHILDREN’S CENTRE
350 RUMSEY ROAD
TORONTO, ONTARIO M5R 1Y2
CANADA
FAX: 416-424-3839
E-MAIL: [email protected]
0022-3913/$30.00
Copyright � 2004 by The Editorial Council of The Journal of Prosthetic
Dentistry
doi:10.1016/j.prosdent.2004.07.014
433





























