Embed Size (px)
Citation preview

Original Article
The contribution of diffusion tensorimaging and magnetic resonancespectroscopy for the differentiationof breast lesions at 3T
Ioannis Tsougos1, Patricia Svolos1, Evanthia Kousi1,Evangelos Athanassiou2, Kiriaki Theodorou1,Dimitrios Arvanitis4, Ioannis Fezoulidis3 andKaterina Vassiou3,4
AbstractBackground: Conventional breast magnetic resonance imaging (MRI), including dynamic contrast-enhanced MR mam-mography (DCE-MRM), may lead to ambiguous diagnosis and unnecessary biopsies.Purpose: To investigate the contribution of proton MR spectroscopy (1H-MRS) combined with diffusion tensor imaging(DTI) metrics in the discrimination between benign and malignant breast lesions.Material and Methods: Fifty-one women with known breast abnormalities from conventional imaging were examinedon a 3T MR scanner. DTI was performed during breast MRI, and fractional anisotropy (FA) and apparent diffusioncoefficient (ADC) were measured in the breast lesions and the contralateral normal breast. FA and ADC were comparedbetween malignant lesions, benign lesions, and normal tissue. 1H-MRS was performed after gadolinium administrationand choline peak was qualitatively evaluated.Results: In our study 1H-MRS showed a sensitivity of 93.5%, specificity 80%, and accuracy 88.2%. FA was significantlyhigher in breast carcinomas compared to benign lesions. However, no significant difference was observed in ADCbetween benign and malignant lesions. The combination of Cho presence and FA achieved higher levels of accuracyand specificity in discriminating malignant from benign lesions over Cho presence or FA alone.Conclusion: In conclusion, applying DTI and 1H-MRS together, adds incremental diagnostic value in the characterizationof breast lesions and may sufficiently improve the low specificity of conventional breast MRI.
KeywordsSpectroscopy, diffusion tensor imaging, breast tumor, 3T
Date received: 26 February 2013; accepted: 1 May 2013
Introduction
Conventional breast magnetic resonance imaging(MRI) has shown diagnostic sensitivities of 94–99%for screening breast lesions, whereas relatively low spe-cificities have been reported, resulting in many unneces-sary biopsies of benign lesions (1,2). Breast lesioncharacterization is based upon the combination of mor-phological features of the lesion and patterns ofdynamic contrast enhancement of gadolinium-based contrast agent. Despite the fact that dynamic
1Department of Medical Physics, University of Thessaly Medical School,Larissa, Greece2Department of Surgery, University of Thessaly Medical School, Larissa,Greece3Department of Diagnostic Radiology, University of Thessaly MedicalSchool, Larissa, Greece4Department of Anatomy-Histology-Embryology, University of ThessalyMedical School, Larissa, Greece
Corresponding author:
Ioannis Tsougos, Department of Medical Physics, University of ThessalyMedical School, Biopolis, 41110, Larissa, Greece.Email: [email protected]
Acta Radiologica
2014, Vol. 55(1) 14–23
! The Foundation Acta Radiologica
2013
Reprints and permissions:
sagepub.co.uk/journalsPermissions.nav
DOI: 10.1177/0284185113492152
acr.sagepub.com

contrast-enhanced MR mammography (DCE-MRM),has already gained acceptance as an important breastimaging modality, in many cases it may lead to ambigu-ous diagnosis, as its high sensitivity comes also with lowspecificity (3,4).
Besides morphologic criteria, the search for specificpredictors of malignant breast disease includes new MRtechniques like proton MR spectroscopy (1H-MRS)or di!usion-weighted imaging (DWI) (5–8). In-vivo1H-MRS of the breast has been previously reported(9–15). In all cases, breast lesion evaluation was princi-pally based on the level of choline-containing com-pounds (Cho) detected at 3.2 ppm in the breast tissuesamples. High levels of Cho have been observed inmalignant breast lesions, while benign lesions ornormal breast tissue revealed low levels or absence ofCho. Hence, these observations can be used for thedi!erentiation of malignant and benign breast lesionsstudied with 1H-MRS. Nevertheless, it has been shownthat the elevation of Cho levels is not the same in allbreast cancers may be due to di!erences on the biologicaggressiveness of the tumor. Thus, the ability of 1H-MRS to demonstrate abnormal Cho levels in breastcancer has been reported variable (13,15). Despite thepromising results of in-vivo 1H-MRS in the di!erenti-ation of benign and malignant breast lesions, a reviewof published studies shows that the method has a false-negative rate of approximately 4–18% and a false-positive rate of 14–18% (9,10,12,14,16).
DWI is a MRI technique that characterizes thethree-dimensional mobility of water in vivo and enablesindirect assessment of tissue microstructure. Recentstudies have demonstrated the potential dynamics ofDWI as a non-contrast technique for detecting andcharacterizing breast lesions (17–21). Results of thesestudies showed that carcinomas exhibit lower di!usivitythan benign lesions or normal breast tissue, attributedto a higher cell density of carcinomas. In those reports,the apparent di!usion coe"cient (ADC) was measured,with the general assumption that di!usion characteris-tics in the breast are isotropic (non-directional).
However, the breast is a structured organ that pre-sents fibroglandular tissue orientated along tubularducts and Cooper ligaments, which may influence thedirectionality of di!usion and produce a measurablelevel of anisotropy (22,23).
Di!usion tensor imaging (DTI) extends DWI, prob-ing water motion in six or more directions, in order tomeasure the full di!usion tensor and characterize themotion of water in more detail. DTI provides measuresof di!usion anisotropy (or directionality) in addition toADC. Until now, only few published studies havereported DTI measures of fractional anisotropy (FA)and ADC or mean di!usivity (MD) in the breast(22,23). Partridge et al. demonstrated significantly
lower FA in breast cancer than normal tissue, whichmay reflect alterations in tissue organization. However,in comparisons between benign and malignant breastlesions, no significant di!erences in FA were found,while ADC significantly di!erentiated the two entities(22). On the contrary, Baltzer et al. revealed significantdi!erence on both FA and ADC values between malig-nant and benign breast lesions (23).
Hence, MRI has obviously shifted towards molecu-lar MRI, thus, promising to improve MR specificityand provide an insight into the underlying biologicalcharacteristics of tumors, going a step further fromconventional MRI. Over the last 10 years, it is evidentthat in brain tumor investigation the combination ofdi!usion characteristics and especially DTI metrics,such as FA, combined with MRS can yield the optimaloutcome regarding di!erential diagnosis (24). On theother hand, to our knowledge, no published studieshave integrated 1H-MRS and DTI to overall assesstheir contribution in breast lesion characterization.Therefore, the hypothesis of our study was that1H-MRS and DTI when applied together, may addincremental diagnostic value in the determination ofbreast lesion’s aggressiveness.
Material and Methods
Patients
In this study, 51 women were included ranging in agefrom 28 to 72 years (mean! SD, 51! 15 years). BreastMRI was performed on suspicious mammographic orultrasonographic abnormalities. Patients recruited forthe study presented at least one contrast-enhancingmass in bilateral breast MRI with the largest diameterbeing 10mm and at least 7mm in the remaining twodimensions. Patients who had received previous or cur-rent neoadjuvant chemotherapy or radiation therapy,previous needle biopsy or any other surgical proceduresin the 2 months preceding the breast examination, orhad any metallic clips from previous surgery and gen-eral contraindications to MRI or to the administrationof contrast agents were excluded from the study. Noneof the patients was a lactating mother, given that it hasbeen shown that Cho presence is substantially a!ected.All premenopausal patients were examined during thesecond week of the menstrual cycle and none of theenrolled postmenopausal women was under treatmentwith hormone replacement therapy. Fifty-one breastlesions were detected on the DCE-MRM. All lesionswere confirmed by surgically excised specimens (33/51) or by core needle biopsy and follow-up (18/51).Written informed consent was obtained from allsubjects.
Tsougos et al. 15

MRI, DTI, and 1H-MRS protocols
All MR scans were performed on a 3T MR scanner(GE Healthcare, Signa HDx, Milwaukee, WI, USA),using a dedicated phased array 8-channel breast coil.Patients were placed in the prone position, in order tominimize the e!ect of respiratory motion of the breasts.
Conventional MRI protocol. Our conventional MRI proto-col included axial T2-weighted fast spin echo imagingsequence (T2-FSE, TR/TE, 3600/100ms; slice thick-ness, 4mm; spacing, 0mm) and axial short TI inversionrecovery imaging sequence (STIR, TR/TE, 3875/90ms;slice thickness, 4mm; spacing, 0mm). DCE-MRMsequence was performed using fat-suppressed three-dimensional (3D) T1-weighted vibrant dynamicimages (flip angle, 10", 1mm3 isotropic voxel, oneunenhanced and five contrast-enhanced acquisitions).Gadolinium was automatically injected over approxi-mately 10 s.
1H-MRS protocol. For 1H-MRS performance a TE-aver-aged single-voxel point resolved spectroscopy (PRESS/vendor product name BREASE) was acquired aftercontrast administration. Before 1H-MRS procedurethe channels contralateral to the lesion were automat-ically switched o!. Automated parameter optimizationconsisted of frequency and receiver gain adjustmentand gradient tuning. An automatic shimming adjust-ment was also performed to reach a full width at halfmaximum (FWHM) of the unsuppressed water peak<25Hz as a quality parameter of the MR signal. Forvalues >25Hz, the voxel was readjusted to the region ofinterest and the automated shimming procedure wasrepeated. 1H-MRS sequence was acquired with the fol-lowing technical parameters: echo times, 4; TR/ aver-aged TE, 2000/155ms; 56 averages per echo for voxelsize of 3.375 cm3 (1.5# 1.5# 1.5 cm); and 32 averagesper echo for voxel size >3.375 cm3.
The relatively long averaged TE (155ms) was chosento increase the visibility of the Choline resonance due to
the longer T2 of Cho (>350ms) compared to that offatty tissue lipids ($100ms) (1).
Voxel size was chosen to be >3.375 cm3 butnot >8 cm3, and it was carefully adjusted to thelesion. Additionally, a strong lipid and water spectralsuppression was applied using a frequency-selectiveinversion pulse surrounded by a spoiler gradient pulseof opposite signs, which also incorporates a motioncorrection. Cho resonance in breast spectra was quali-tatively determined. The criteria for determiningthe presence or absence of Cho were that apeak should be clearly identifiable at 3.2 ppm withinthe lesion (Fig. 1a).
A MR physicist and a radiologist qualitativelyassessed the presence of choline in a blinded review ofthe water suppressed spectra. A copy of the spectrafrom all patients was given to each reader, withoutany other information regarding MR images or voxelplacement. Consequently, the readers were asked toevaluate the spectra for the presence of choline reson-ance at 3.2 ppm, by responding yes or no.
DTI protocol. The DTI acquisition protocol included anaxial di!usion-weighted echo planar imaging (EPI)sequence and was performed before contrast injection.The sequence’s technical parameters were: TR/TE,6000/63.7ms; slice thickness, 4mm; and spacing,0mm. Di!usion gradients were applied in six directionswith b% 0 and 600 s/mm2. Data analysis and di!usionmeasurements were performed on an AdvantageLinux workstation using the Functool software pro-vided by the manufacturer (GE Healthcare). Priorto measurements, corrections for motion and eddy cur-rent artifacts were applied on the images using theBrainstat software. DTI parametric maps were thengenerated in order to extract FA and ADC values.Examples of ADC and FA parametric maps areshown in Fig. 1. The region of interest (ROI) wasplaced on the abnormal hyperintense area of theDCE-MRM images, which were used as a background
Fig. 1 Examples of Cho (a), ADC (b), and FA (c) measurements in a patient with breast carcinoma
16 Acta Radiologica 55(1)

reference image, fused on the parametric map (Fig. 1band 1c). DTI parameters for normal appearing fibro-glandular tissue were also measured in the contralateralbreast. ROI placement was performed without know-ledge of the histological information. The ADC and FAmeasurements were performed by two separatereaders (Radiologist and Medical Physicist). The totalscan time of the breast imaging process (conventionalMRI, DCE, DTI, and 1H-MRS) was 40minapproximately.
Finally, Cho levels, FA and ADC were comparedbetween neoplasms, benign lesions, and normal tissueby univariate and multivariate analyses.
It should be noted, that these techniques require theadjustment of several technical pre-acquisition param-eters, in order to ensure signal quality, therefore theyshould be optimally performed by an MR physicist.However, the metabolic and di!usion information pro-vided is highly correlated to the underlying pathophysi-ology. Hence, the overall evaluation of thespectroscopic and di!usion findings, in combinationwith the imaging characteristics of the tumor understudy, requires the cooperation of both the radiologistand the MR physicist.
Statistical analysis
Descriptive statistics consisted of means and SDsfor FA and ADC measurements. Data analysiswas performed using the Statistical Package for theSocial Sciences (SPSS, v13, IBM, New York, NY,USA) statistical software package. Non-parametricMann-Whitney U tests were used to evaluate the sig-nificance in the ADC and FA values between malignantand benign breast lesions, as well as between thea!ected (benign or malignant) and the contralateralareas. Pearson’s linear regression was employed todetermine whether the Cho presence was correlatedwith the DTI metrics.
Receiver-operating characteristic (ROC) curve ana-lysis based on logistic regression models was performedto compare the diagnostic performance of the multi-variate models to that of DTI metrics and Cho pres-ence. Statistical significance was set at P% 0.05.
Results
From the 51 lesions, 33 were malignant and 18 werebenign. Among the 33 malignant lesions, 25 were inva-sive ductal carcinomas, five were invasive lobular car-cinomas, and three were malignant phylloides tumors.Among the 18 benign lesions, 16 were fibroadenomasand two proved to be fibrocystic changes. Themean lesion size was 4.2 cm (range, 1–9 cm) for the
malignancies and 2.6 cm (range, 0.8–4.2 cm) for thebenign lesions, whereas for the two fibrocystic changesthe corresponding sizes were 0.8 cm and 0.9 cm in size,respectively.
1H-MRS
MRS was performed post contrast, on all 51 enhancedlesions that were detected on DCE-MRM. Fifty out ofthe 51 lesions were mass lesions and one was a non-mass lesion.
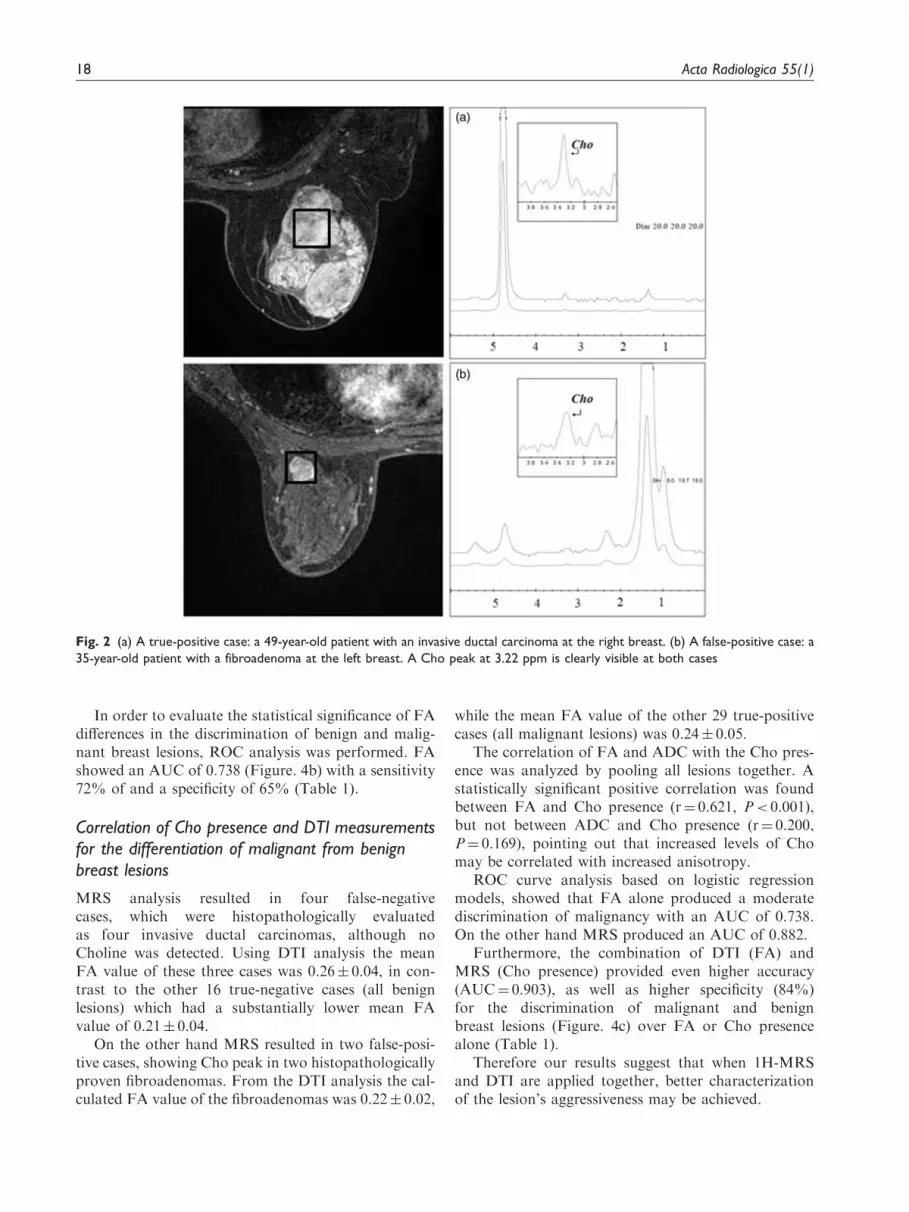
1H-MRS was positive for Cho detection at 31lesions and negative at 20 lesions. From the 31 Cho-positive lesions, 29 were malignant (true-positive) andtwo proved benign (false-positive) (Fig. 2). These 29malignant lesions were 21 invasive ductal carcinomas,five invasive lobular carcinomas, and three malignantphylloides tumors. The Cho-positive benign lesionswere two fibroadenomas.
From the 20 Cho-negative lesions, 16 were benign(true-negative) and four were malignant (false-negative)(Fig. 3). All four malignant lesions proved to be inva-sive ductal carcinomas. From the 16 benign Cho-negative lesions, 14 were fibroadenomas and twoproved to be fibrocystic changes. Overall, 1H-MRS sig-nificantly di!erentiated malignant from benign breastlesions (P< 0.05).
Hence in our study 1H-MRS showed a sensitivity of93.5%, specificity 80%, and accuracy 88.2% (Fig. 4A).The aforementioned 1H-MRS results are summarizedin Table 1.
DTI
Paired DTI measurements for all breast lesions andcontralateral normal tissue were performed for eachpatient. The mean FA values for carcinomas, benignlesions, and the contralateral normal tissue were0.24! 0.05, 0.21! 0.04, and 0.30! 0.05, respectively.The mean ADC for carcinomas, benign lesions, andthe contralateral normal tissue were 1.54! 0.59(*10&3 mm2/s), 1.67! 0.62 (*10&3mm2/s), and0.99! 0.68 (*10&3mm2/s), respectively.
FA and ADC values for both malignant and benignbreast lesions were significantly di!erent from thenormal breast tissue (Table 2).
Concerning the characterization of breast lesions,FA was higher in breast carcinomas compared tobenign lesions. On the contrary, there were no signifi-cant di!erences observed in ADC values betweenmalignant and benign breast lesions (Table 2).However, ADC showed a tendency towards lowervalues for malignant (1.54! 0.59 *10&3mm2/s) com-pared to benign (1.67! 0.62 *10&3mm2/s) breastlesions.
Tsougos et al. 17
In order to evaluate the statistical significance of FAdi!erences in the discrimination of benign and malig-nant breast lesions, ROC analysis was performed. FAshowed an AUC of 0.738 (Figure. 4b) with a sensitivity72% of and a specificity of 65% (Table 1).
Correlation of Cho presence and DTI measurementsfor the differentiation of malignant from benignbreast lesions
MRS analysis resulted in four false-negativecases, which were histopathologically evaluatedas four invasive ductal carcinomas, although noCholine was detected. Using DTI analysis the meanFA value of these three cases was 0.26! 0.04, in con-trast to the other 16 true-negative cases (all benignlesions) which had a substantially lower mean FAvalue of 0.21! 0.04.
On the other hand MRS resulted in two false-posi-tive cases, showing Cho peak in two histopathologicallyproven fibroadenomas. From the DTI analysis the cal-culated FA value of the fibroadenomas was 0.22! 0.02,
while the mean FA value of the other 29 true-positivecases (all malignant lesions) was 0.24! 0.05.
The correlation of FA and ADC with the Cho pres-ence was analyzed by pooling all lesions together. Astatistically significant positive correlation was foundbetween FA and Cho presence (r% 0.621, P< 0.001),but not between ADC and Cho presence (r% 0.200,P% 0.169), pointing out that increased levels of Chomay be correlated with increased anisotropy.
ROC curve analysis based on logistic regressionmodels, showed that FA alone produced a moderatediscrimination of malignancy with an AUC of 0.738.On the other hand MRS produced an AUC of 0.882.
Furthermore, the combination of DTI (FA) andMRS (Cho presence) provided even higher accuracy(AUC% 0.903), as well as higher specificity (84%)for the discrimination of malignant and benignbreast lesions (Figure. 4c) over FA or Cho presencealone (Table 1).
Therefore our results suggest that when 1H-MRSand DTI are applied together, better characterizationof the lesion’s aggressiveness may be achieved.
Fig. 2 (a) A true-positive case: a 49-year-old patient with an invasive ductal carcinoma at the right breast. (b) A false-positive case: a35-year-old patient with a fibroadenoma at the left breast. A Cho peak at 3.22 ppm is clearly visible at both cases
18 Acta Radiologica 55(1)

Discussion
Conventional breast MRI, even with the addition ofDCE MRM techniques, reaches high levels of sensitiv-ity but still exhibits relatively low specificity, which
remains a drawback in the di!erential diagnosis, espe-cially in small size breast lesions.
1H-MRS of the breast was proposed to be used as anadjunctive tool to the MRI examination for the
Fig. 3 (a) A false-negative case: a 67-year-old patient with an invasive ductal carcinoma at the left breast. (b) A true-negative case: a53-year-old patient with a fibroadenoma at the left breast. 1H-MRS measurements show no Cho peak at 3.22 ppm at both cases
Fig. 4 ROC curve for differentiating malignant from benign breast lesions using Cho presence (a), FA (b), and the combination of both(c) as discriminators
Tsougos et al. 19

improvement of specificity. Although specificity wasindeed improved as several studies have shown(7,8,15,25–27), there are still limitations such as thevoxel size, or the accurate localization on the lesion,thus biopsy unavoidably is the ultimate gold standardin the di!erential diagnosis between malignant andbenign lesions. Hence, the need for further improve-ment of specificity by non-invasive techniques stillremains.
Towards this direction, the current study investi-gated the contribution of DTI with 1H-MRS appliedtogether, in order to provide additional information inthe di!erential diagnosis of breast cancer. The contri-bution of DTI in breast tumor characterization hasonly recently been investigated by a few groups(22,23). To our knowledge, no previous study has com-bined spectroscopy with DTI analysis, and our resultsindicate that a multi-parametric approach using 1H-MRS and DTI can provide important informationabout the metabolic and structural status of breasttissue, which may increase the specificity of MRI forbreast cancer diagnosis.
It should be mentioned that 1H-MRS is not amethod for detecting breast lesions but rather amethod for their characterization. Taking into accountthat DCE-MRM shows a wide range of specificities(37–97%) (28–31), 1H-MRS is a method which shiftsthat range towards higher values. As choline containingcompounds are believed to be precursors of thephospholipids that compose cell membranes, increasesin Cho signals are thought to reflect increased mem-brane synthesis. Elevated levels of Cho have beenreported in many studies of excised human breast
tumors, cultured human breast cancer cells, andanimal models (27). The phosphocholine content inhuman breast cancer cells was found to be 10-foldhigher than that of normal human mammary epithelialcells (27,32–34). Previous investigators have reportedsensitivities of 70–100% and specificities of 67–100%for breast MR spectroscopy (35).
In our study the sensitivity of 1H-MRS was 93.5%,the specificity was 80%, and the accuracy was 88.2%.The MRS analysis provided four false-negative casesand two false-positive cases. The four false-negativecases were invasive ductal carcinomas although noCholine was detected. One possible cause of this draw-back could be that at least one dimension of thesetumors was <1.5 cm, while the minimum voxel dimen-sion, used for such lesions, was not <1.5 cm in order tohave su"cient signal. As a result, a significant amountof the surrounding fatty breast parenchyma wasincluded inside the voxel and may have contributed tothe overall signal, masking the Cho presence in thesecases. Such inclusion deteriorates the field homogeneityin the region of interest, due to the di!erent magneticpermeability of fat and lesion tissue interface. Hence, itseems that the sensitivity of breast 1H-MRS is stronglydependent on tumor size, as previously reported byother studies (14,36). This dependency appears to bemainly based on the technical issues related to thedetection of smaller quantities of composite Cho.Moreover, previous single voxel 1H-MRS studieshave reported false-negative results either because ofrecent hemorrhage of the lesion, since blood productscan degrade the local field homogeneity, or because ofmotion artifacts due to the extended length of theexamination (14).
Another possible drawback of MRS is that lobularbreast carcinomas may include enough lipids in acqui-sition voxels that could mask the choline resonance (8),nevertheless this was not observed in our study, as allthree lobular carcinomas exhibited a discriminant Chosignal.
The two false-positive cases, in which a misleadingCho peak was detected, proved to be two fibroaden-omas. The reason that some fibroadenomas showCho is unknown, and it could refer to the limitations
Table 2. FA and ADC mean values with their corresponding SD and comparison results between malignant, benign, and contralateralnormal area.
Malignant Benign Contralateral normal tissue P values
FA 0.24! 0.05* 0.21! 0.04* 0.30! 0.05 <0.05
ADC (*10-3 mm2/s) 1.54! 0.59* 1.67! 0.62* 0.99! 0.68 0.373
P values represent Mann-Whitney U test for the comparison of the ADC and FA between malignant and benign breast lesions*The parameter significant difference between ADC and FA of the lesions from the corresponding contralateral normal tissue (P< 0.05)
Table 1. Measures of overall accuracy, sensitivity and specificityusing Cho presence, FA, and the combination of both for thediscrimination of benign from malignant breast lesions.
Metrics Accuracy (%) Sensitivity (%) Specificity (%)
Cho presence 88.2 93.5 80
FA 73.8 72 65
Cho*FA 90.3 80 84
20 Acta Radiologica 55(1)

of the method in the diagnosis of benign tumors (27).This has been previously reported, although themost common reported false-positive cases arehistologically tubular adenomas or fibrocystic changes(9,12). Indicatively, in our study there were two cases offibrocystic change which were correctly shown astrue-negative.
A previous di!usion study has shown that breastpathologies result in decreased structuring and thus, asignificant reduction of di!usion anisotropy comparedto normal breast parenchyma is expected (23).
Our results verify the aforementioned hypothesis,showing significantly lower di!usion anisotropy in can-cers than normal tissue, which may indeed reflect alter-ations in the organization of breast tissue. The meanFA value for malignant, benign, and normal tissue was0.24! 0.05, 0.21! 0.04, and 0.30! 0.05, respectively.These results reflect the distinct discrimination betweenthe normal and pathological breast tissue, and furtherindicate a potential di!erentiation between the benignand malignant lesions per se. This may also be observedin the results of ROC analysis using FA alone, wherethe computed accuracy, sensitivity, and specificity are73.8%, 72%, and 65% respectively. In one of the fewstudies that investigate measures of anisotropy in breasttumors, Partridge et al. (22) reported similar observa-tions regarding the discrimination between breastcancer and normal tissue, but not between malignantand benign lesions. On the other hand, Baltzer et al.demonstrated significantly lower FA values for benignbreast lesions over carcinomas, which is in compliancewith our observations (23).
Regarding tumor cellularity, previous studies havereported that in a variety of cancers, lower ADCvalues in malignancies correlate with increased celldensity, compared to benign lesions (37,38). Our resultsseem to be in agreement with these observations, as themean ADC value for malignant tumors was 1.54! 0.59(*10–3mm2/s), whereas for benign lesions 1.67! 0.62(*10–3mm2/s), however these di!erences did not reacha statistical significance. The decreased di!usivity inbreast carcinomas may be explained by their increasedcell density, which might cause water molecules to dif-fuse with a higher degree of directionality, in contrastto benign lesions. Therefore, increased anisotropy andreduced di!usivity are expected in malignant breastlesions, as reported by a previous study fromPartridge et al. (22).
All the evaluated metrics (metabolic and di!usion)di!erentiate normal tissue from breast carcinomas.However, the di!erentiation of benign and malignanttissue was feasible only by Cho presence and FA, andnot ADC.
A multiple logistic regression model combiningFA and Cho presence achieved high accuracy
(AUC% 0.903), as well as high specificity (84%)(Table 1). On the contrary, Cho presence aloneachieved a lower discrimination, with an AUC of0.882, whereas FA alone resulted only in a moderatediscrimination with an AUC of 0.738, which might beexplained by the overlapping FA values between malig-nant and benign tissue.
Hence our preliminary results, indicate a positivecorrelation between Cho presence and FA (r% 0.621,P< 0.001), and suggest that the combination of FAwith Cho presence adds incremental diagnostic valueover FA or Cho presence alone, in the discriminationof malignant from benign tissue.
This correlation between Cho and FA may beexplained based on two factors: (a) Cho is associatedwith active cell proliferation; and (b) tumor growth,results in higher cell density, which might cause watermolecules to di!use with a higher degree of direction-ality, in contrast to benign lesions.
Thus, it seems that the combination of these twocellular and molecular variables may lead to an opti-mum non-invasive discrimination. Therefore, there is ahigh probability of a breast lesion to be correctly clas-sified if both Cho and FA parameters are taken intoaccount. Hence, if 1H-MRS and DTI are appliedtogether, better characterization of the lesion’s aggres-siveness is expected.
Our study presents some limitations that have to betaken into account. One limitation is that the minimumlesion size which can be examined by MRS is1.5*1.5*1.5 cm, consequently the acquisition voxelmay include surrounding, normal, adipose tissueobscuring the Cho resonance (8). Moreover, the rela-tively long acquisition time of the 1H-MRS sequence(nearly 10 min) may reduce the spectral resolution, dueto the probability of artifacts from respiratory andother patient’s motion.
Almost all lesions in this study were masses. Thismight be a limitation of this study since MRS andDTI may not perform as well in non-mass lesions,which are indeed common false-positives in MRI.
Advanced MRI techniques such as 1H-MR spectros-copy and DTI can be incorporated in the clinical rou-tine to improve specificity, and provide an insight intothe underlying biological characteristics of breasttumors.
Our preliminary results suggest that the combinationof DTI and MRS metrics provided the highest accuracyand specificity, in the di!erentiation of malignant frombenign breast lesions, compared to each techniqueapplied separately.
In conclusion, applying DTI and 1H-MRS together,adds incremental diagnostic value in the characteriza-tion of breast lesions and may su"ciently improve thelow specificity of conventional breast MRI.
Tsougos et al. 21

Funding
This research received no specific grant from any fundingagency in the public, commercial, or not-for-profit sectors.
References
1. Heywang-Kobrunner SH, Viehweg P, Heinig A, et al.Contrast-enhanced MRI of the breast: accuracy, value,controversies, solutions. Eur J Radiol 1997;24:94–108.
2. Orel SG, Schnall MD. MR imaging of the breast for thedetection, diagnosis, and staging of breast cancer.Radiology 2001;220:13–30.
3. Nunes LW, Schnall MD, Orel SG, et al. Correlation oflesion appearance and histological findings for the nodesof a breast MR imaging interpretation model.Radiographics 1999;19:79–92.
4. Yen Y, Han K, Daniel B, et al. Dynamic breast MRI withspiral trajectories: 3D versus 2D. J Magn Reson Imaging2000;11:351–359.
5. Malich A, Fischer DR, Wurdinger S, et al. Potential MRIinterpretation model: differentiation of benign frommalignant breast masses. Am J Roentgenol2005;185:964–970.
6. Schnall MD, Blume J, Bluemke DA, et al. Diagnosticarchitectural and dynamic features at breast MR ima-ging: multicenter study. Radiology 2006;238:42–53.
7. Tozaki M, Fukuma E. 1H MR spectroscopy and diffu-sion-weighted imaging of the breast: are they useful toolsfor characterizing breast lesions before biopsy? Am JRoentgenol 2009;193:840–849.
8. Mountford C, Ramadan S, Stanwell P, et al. ProtonMRS of the breast in the clinical setting. NMR Biomed2009;22:54–64.
9. Kvistad KA, Bakken IJ, Gribbestad IS, et al.Characterization of neoplastic and normal humanbreast tissues with in vivo (1)H MR spectroscopy. JMagn Reson Imaging 1999;10:159–164.
10. Gribbestad IS, Singstad TE, Nilsen G, et al. In vivo (1) HMRS of normal breast and breast tumors using a dedi-cated double breast coil. J Magn Reson Imaging1998;8:1191–1197.
11. Sijens PE, Wijrdeman HK, Moerland MA, et al. Humanbreast cancer in vivo: H-1 and P-31 MR spectroscopy at1.5 T. Radiology 1988;169:615–620.
12. Yeung DK, Cheung HS, Tse GM. Human breastlesions: characterization with contrast enhanced in vivoproton MR spectroscopy-initial results. Radiology2001;220:40–46.
13. Yeung DK, Yang WT, Tse GM. Human breast cancer:in vivo proton MR spectroscopy in the characterizationof histopathological subtypes and preliminary observa-tions in axillary node metastases. Radiology2002;225:190–197.
14. Cecil KM, Schnall MD, Siegelman ES, et al. The evalu-ation of human breast lesions with magnetic resonanceimaging and proton magnetic resonance spectroscopy.Breast Cancer Res Treat 2001;68:45–54.
15. Kousi E, Tsougos I, Vasiou K, et al. Magnetic resonancespectroscopy of the breast at 3T: pre- and post-contrast
evaluation for breast lesion characterization. ScientificWorld Journal 2012;2012:754380.
16. Gribbestad IS, Bakken IJ, Singstad TE, et al.Determination of choline content in breast tumors withH-1 MR spectroscopy: an external standard method. In:Proceedings of the 7th meeting of ISMRM, Berkeley,1999.
17. Yoshikawa MI, Ohsumi S, Sugata S, et al. Comparisonof breast cancer detection by diffusion-weighted magneticresonance imaging and mammography. Radiat Med2007;25:218–223.
18. Yabuuchi H, Matsuo Y, Okafuji T, et al. Enhanced masson contrast-enhanced breast MR imaging: lesion charac-terization using combination of dynamic contrast-enhanced and diffusion-weighted MR images. J MagnReson Imaging 2008;28:1157–1165.
19. Woodhams R, Matsunaga K, Kan S, et al. ADC map-ping of benign and malignant breast us. Magn ResonMed Sci 2005;4:35–42.
20. Rubesova E, Grell AS, De Maertelaer V, et al.Quantitative diffusion imaging in breast cancer: a clinicalprospective study. J Magn Reson Imaging2006;24:319–24.
21. Kuroki-Suzuki S, Kuroki Y, Nasu K, et al. Detectingbreast cancer with non-contrast MR imaging: combiningdiffusion-weighted and STIR imaging. Magn Reson MedSci 2007;6:21–27.
22. Partridge SC, Ziadloo A, Murthy R, et al. Diffusiontensor MRI: preliminary anisotropy measures and map-ping of breast tumors. J Magn Reson Imaging2010;31:339–347.
23. Baltzer PA, Schafer A, Dietzel M, et al. Diffusion tensormagnetic resonance imaging of the breast: a pilot study.Eur Radiol 2011;21:1–10.
24. Tsougos I, Svolos P, Kousi E, et al. Differentiation ofglioblastoma multiforme from metastatic brain tumorusing proton-MRS, diffusion and perfusion metrics at3T. Cancer Imaging 2012;26:423–436.
25. Sardanelli F, Fausto A, Di Leo G, et al. In vivo protonMR spectroscopy of the breast using the total cholinepeak integral as a marker of malignancy. Am JRoentgenol 2009;192:1608–1617.
26. Hu J, Yu Y, Kou Z, et al. A high spatial resolution 1Hmagnetic resonance spectroscopic imaging technique forbreast cancer with a short echo time. Magn ResonImaging 2008;26:360–366.
27. Katz-Brull R, Lavin PT, Lenkinski RE. Clinical utilityof proton magnetic resonance spectroscopy incharacterizing breast lesions. J Natl Cancer Inst2002;94:1197–1203.
28. Robson ME, Offit K. Breast MRI for women with her-editary cancer risk. JAMA 2004;292:1368–1370.
29. Kriege M, Brekelmans CT, Boetes C, et al. Efficacy ofMRI and mammography for breast-cancer screening inwoman with familial or genetic predisposition. N Engl JMed 2004;351:427–437.
30. Daniel BL, Yen YF, Glover GH, et al. Breast dis-ease: dynamic spiral MR imaging. Radiology1998;209:499–509.
22 Acta Radiologica 55(1)

31. Liberman L, Morris EA, Lee MJ, et al. Breast lesionsdetected on MR imaging: features and positive predictivevalue. Am J Roentgenol 2002;179:171–178.
32. Aboagye EO, Bhujwalla ZM. Malignant transformationalters membrane choline phospholipid metabolism ofhuman mammary epithelial cells. Cancer Res1999;59:80–84.
33. Singer S, Souza K, Thilly WG. Pyruvate utilization,phosphocholine and adenosine triphosphate (ATP) aremarkers of human breast tumor progression: a 31P and13C-nuclear magnetic resonance (NMR) spectroscopystudy. Cancer Res 1995;55:5140–5145.
34. Ting YT, Sherr D, Degani H. Variations in the energyand phospholipid metabolism in normal and cancerhuman mammary epithelial cells. Anticancer Res1996;16:1381–1388.
35. Bartella L, Morris EA, Dershaw DD, et al. Proton MRspectroscopy with choline peak as malignancy markerimproves positive predictive value for breast cancer diag-nosis: preliminary study. Radiology 2006;239:686–692.
36. Roebuck JR, Cecil KM, Schnall MD, et al. Humanbreast lesions: characterization with proton MR spectros-copy. Radiology 1998;209:269–275.
37. Hatakenaka M, Soeda H, Yabuuchi H, et al. Apparentdiffusion coefficients of breast tumors: clinical applica-tion. Magn Reson Med Sci 2008;7:23–29.
38. Guo Y, Cai YQ, Cai ZL, et al. Differentiation ofclinically benign and malignant breast lesions using diffu-sion-weighted imaging. J Magn Reson Imaging2002;16:172–178.
Tsougos et al. 23




























