Embed Size (px)
Citation preview
Britannica LaunchPacks | The Treatment and Prevention of Disease
1 of 123© 2020 Encyclopædia Britannica, Inc.
The Treatment and Prevention of DiseaseFor Grades 9-12
This Pack contains:
5 ARTICLES1 IMAGE5 VIDEOS
Britannica LaunchPacks | The Treatment and Prevention of Disease
2 of 123© 2020 Encyclopædia Britannica, Inc.
infectious diseaseBritannica Note:
Infectious diseases are caused by microorganisms, and they spread in many ways. Infectious diseases may travel through food, air, and water; contact with animals; and person-to-person contact.
in medicine, a process caused by an agent, often a type of microorganism, that impairs a person’s health. In
many cases, infectious disease can be spread from person to person, either directly (e.g., via skin contact) or
indirectly (e.g., via contaminated food or water).
An infectious disease can differ from simple infection, which is the invasion of and replication in the body by any
of various agents—including bacteria, viruses, fungi, protozoans, and worms—as well as the reaction of tissues
to their presence or to the toxins that they produce. When health is not altered, the process is called a
subclinical infection. Thus, a person may be infected but not have an infectious disease. This principle is
illustrated by the use of vaccines for the prevention of infectious diseases. For example, a virus such as that
which causes measles may be attenuated (weakened) and used as an immunizing agent. The immunization is
designed to produce a measles infection in the recipient but generally causes no discernible alteration in the
state of health. It produces immunity to measles without producing a clinical illness (an infectious disease).
The most important barriers to invasion of the human host by infectious agents are the skin and mucous
membranes (the tissues that line the nose, mouth, and upper respiratory tract). When these tissues have been
broken or affected by earlier disease, invasion by infectious agents may occur. These infectious agents may
produce a local infectious disease, such as boils, or may invade the bloodstream and be carried throughout the
body, producing generalized bloodstream infection (septicemia) or localized infection at a distant site, such as
meningitis (an infection of the coverings of the brain and spinal cord). Infectious agents swallowed in food and
drink can attack the wall of the intestinal tract and cause local or general disease. The conjunctiva, which covers
the front of the eye, may be penetrated by viruses that cause a local inflammation of the eye or that pass into
the bloodstream and cause a severe general disease, such as smallpox. Infectious agents can enter the body
through the genital tract, causing the acute inflammatory reaction of gonorrhea in the genital and pelvic organs
or spreading out to attack almost any organ of the body with the more chronic and destructive lesions of
syphilis. Even before birth, viruses and other infectious agents can pass through the placenta and attack
developing cells, so that an infant may be diseased or deformed at birth.
From conception to death, humans are targets for attack by multitudes of other living organisms, all of them
competing for a place in the common environment. The air people breathe, the soil they walk on, the waters and
vegetation around them, the buildings they inhabit and work in, all can be populated with forms of life that are
potentially dangerous. Domestic animals may harbour organisms that are a threat, and wildlife teems with
agents of infection that can afflict humans with serious disease. However, the human body is not without
defenses against these threats, for it is equipped with a comprehensive immune system that reacts quickly and
specifically against disease organisms when they attack. Survival throughout the ages has depended largely on
these reactions, which today are supplemented and strengthened through the use of medical drugs.

Britannica LaunchPacks | The Treatment and Prevention of Disease
3 of 123© 2020 Encyclopædia Britannica, Inc.
Infectious agentsCategories of organisms
The agents of infection can be divided into different groups on the basis of their size, biochemical
characteristics, or manner in which they interact with the human host. The groups of organisms that cause
infectious diseases are categorized as bacteria, viruses, fungi, and parasites.
Bacteria
Bacteria can survive within the body but outside individual cells. Some bacteria, classified as aerobes, require
oxygen for growth, while others, such as those normally found in the small intestine of healthy persons, grow
only in the absence of oxygen and, therefore, are called anaerobes. Most bacteria are surrounded by a capsule
that appears to play an important role in their ability to produce disease. Also, a number of bacterial species
give off toxins that in turn may damage tissues. Bacteria are generally large enough to be seen under a light
microscope. Streptococci, the bacteria that cause scarlet fever, are about 0.75 micrometre (0.00003 inch) in
diameter. The spirochetes, which cause syphilis, leptospirosis, and rat-bite fever, are 5 to 15 micrometres long.
Bacterial infections can be treated with antibiotics.
Bacterial infections are commonly caused by pneumococci, staphylococci, and streptococci, all of which are
often commensals (that is, organisms living harmlessly on their hosts) in the upper respiratory tract but that can
become virulent and cause serious conditions, such as pneumonia, septicemia (blood poisoning), and meningitis.
The pneumococcus is the most common cause of lobar pneumonia, the disease in which one or more lobes, or
segments, of the lung become solid and airless as a result of inflammation. Staphylococci affect the lungs either
in the course of staphylococcal septicemia—when bacteria in the circulating blood cause scattered abscesses in
the lungs—or as a complication of a viral infection, commonly influenza—when these organisms invade the
damaged lung cells and cause a life-threatening form of pneumonia. Streptococcal pneumonia is the least
common of the three and occurs usually as a complication of influenza or other lung disease.
Pneumococci often enter the bloodstream from inflamed lungs and cause septicemia, with continued fever but
no other special symptoms. Staphylococci produce a type of septicemia with high spiking fever; the bacteria can
reach almost any organ of the body—including the brain, the bones, and especially the lungs—and destructive
abscesses form in the infected areas. Streptococci also cause septicemia with fever, but the organisms tend to
cause inflammation of surface lining cells rather than abscesses—for example, pleurisy (inflammation of the
chest lining) rather than lung abscess, and peritonitis (inflammation of the membrane lining the abdomen)
rather than liver abscess. In the course of either of the last two forms of septicemia, organisms may enter the
nervous system and cause streptococcal or staphylococcal meningitis, but these are rare conditions.
Pneumococci, on the other hand, often spread directly into the central nervous system, causing one of the
common forms of meningitis.
Staphylococci and streptococci are common causes of skin diseases. Boils and impetigo (in which the skin is
covered with blisters, pustules, and yellow crusts) may be caused by either. Staphylococci also can cause a
severe skin infection that strips the outer skin layers off the body and leaves the underlayers exposed, as in
severe burns, a condition known as toxic epidermal necrolysis. Streptococcal organisms can cause a severe
condition known as necrotizing fasciitis, commonly referred to as flesh-eating disease, which has a fatality rate
between 25 and 75 percent. Streptococci can be the cause of the red cellulitis of the skin known as erysipelas.

Britannica LaunchPacks | The Treatment and Prevention of Disease
4 of 123© 2020 Encyclopædia Britannica, Inc.
Some staphylococci produce an intestinal toxin and cause food poisoning. Certain streptococci settling in the
throat produce a reddening toxin that speeds through the bloodstream and produces the symptoms of scarlet
fever. Streptococci and staphylococci also can cause toxic shock syndrome, a potentially fatal disease.
Streptococcal toxic shock syndrome (STSS) is fatal in some 35 percent of cases.
Meningococci are fairly common inhabitants of the throat, in most cases causing no illness at all. As the number
of healthy carriers increases in any population, however, there is a tendency for the meningococcus to become
more invasive. When an opportunity is presented, it can gain access to the bloodstream, invade the central
nervous system, and cause meningococcal meningitis (formerly called cerebrospinal meningitis or spotted
fever). Meningococcal meningitis, at one time a dreaded and still a very serious disease, usually responds to
treatment with penicillin if diagnosed early enough. When meningococci invade the bloodstream, some gain
access to the skin and cause bloodstained spots, or purpura. If the condition is diagnosed early enough,
antibiotics can clear the bloodstream of the bacterium and prevent any from getting far enough to cause
meningitis. Sometimes the septicemia takes a mild, chronic, relapsing form with no tendency toward meningitis;
this is curable once it is diagnosed. The meningococcus also can cause one of the most fulminating of all forms
of septicemia, meningococcemia, in which the body is rapidly covered with a purple rash, purpura fulminans; in
this form the blood pressure becomes dangerously low, the heart and blood vessels are affected by shock, and
the infected person dies within a matter of hours. Few are saved, despite treatment with appropriate drugs.
Haemophilus influenzae is a microorganism named for its occurrence in the sputum of patients with influenza—
an occurrence so common that it was at one time thought to be the cause of the disease. It is now known to be a
common inhabitant of the nose and throat that may invade the bloodstream, producing meningitis, pneumonia,
and various other diseases. In children it is the most common cause of acute epiglottitis, an infection in which
tissue at the back of the tongue becomes rapidly swollen and obstructs the airway, creating a potentially fatal
condition. also is the most common cause of meningitis and pneumonia in children under five H. influenzaeyears of age, and it is known to cause bronchitis in adults. The diagnosis is established by cultures of blood,
cerebrospinal fluid, or other tissue from sites of infection. Antibiotic therapy is generally effective, although
death from sepsis or meningitis is still common. In developed countries where vaccine is used, there H. influenzahas been a great decrease in serious infections and deaths.
Chlamydial organisms
Chlamydia are intracellular organisms found in many vertebrates, including birds and humans and other
mammals. Clinical illnesses are caused by the species , which is a frequent cause of genital C. trachomatisinfections in women. If an infant passes through an infected birth canal, it can produce disease of the eye
(conjunctivitis) and pneumonia in the newborn. Young children sometimes develop ear infections, laryngitis, and
upper respiratory tract disease from . Such infections can be treated with erythromycin.Chlamydia
Another chlamydial organism, , produces psittacosis, a disease that results from exposure Chlamydophila psittacito the discharges of infected birds. The illness is characterized by high fever with chills, a slow heart rate,
pneumonia, headache, weakness, fatigue, muscle pains, anorexia, nausea, and vomiting. The diagnosis is
usually suspected if the patient has a history of exposure to birds. It is confirmed by blood tests. Mortality is rare,
and specific antibiotic treatment is available.
Rickettsias
The rickettsias are a family of microorganisms named for American pathologist Howard T. Ricketts, who died of
typhus in 1910 while investigating the spread of the disease. The rickettsias, which range in size from 250
nanometres to more than 1 micrometre and have no cell wall but are surrounded by a cell membrane, cause a

Britannica LaunchPacks | The Treatment and Prevention of Disease
5 of 123© 2020 Encyclopædia Britannica, Inc.
group of diseases characterized by fever and a rash. Except for , the cause of Q fever, they are Coxiella burnetiiintracellular parasites, most of which are transmitted to humans by an arthropod carrier such as a louse or tick.
, however, can survive in milk, sewage, and aerosols and can be transmitted to humans by a tick or by C. burnetiiinhalation, causing pneumonia in the latter case. Rickettsial diseases can be treated with antibiotics.
Humans contract most rickettsial diseases only when they break into a cycle in nature in which the rickettsias
live. In murine typhus, for example, is a parasite of rats conveyed from rat to rat by the Rickettsia mooseriOriental rat flea, ; it bites humans if they intrude into its environment. Scrub typhus is caused Xenopsylla cheopisby , but it normally parasitizes only rats and mice and other rodents, being carried from one to R. tsutsugamushithe other by a small mite, (previously known as ). This mite is fastidious in matters Leptotrombidium Trombiculaof temperature, humidity, and food and finds everything suitable in restricted areas, or “mite islands,” in South
Asia and the western Pacific. It rarely bites humans in their normal environment, but if people invade its territory
en masse it will attack, and outbreaks of scrub typhus will follow.
The spotted fevers are caused by rickettsias that spend their normal life cycles in a variety of small animals,
spreading from one to the other inside ticks; these bite human intruders and cause African, North Asian, and
Queensland tick typhus, as well as Rocky Mountain spotted fever. One other spotted fever, rickettsialpox, is
caused by , which lives in the body of the ordinary house mouse, , and spreads from one to R. akari Mus musculusanother inside the house mite (formerly ). This rickettsia Liponyssoides sanguineus Allodermanyssus sanguineusis probably a parasite of wild field mice, and it is perhaps only when cities push out into the countryside that
house mice catch the infection.
Mycoplasmas and ureaplasmas
Mycoplasmas and ureaplasmas, which range in size from 150 to 850 nanometres, are among the smallest known
free-living microorganisms. They are ubiquitous in nature and capable of causing widespread disease, but the
illnesses they produce in humans are generally milder than those caused by bacteria. Diseases due to
mycoplasmas and ureaplasmas can be treated with antibiotics.
Mycoplasma pneumoniae is the most important member of its genus. is associated with 20 M. pneumoniaepercent of all cases of pneumonia in adults and children over five years of age. Patients have fever, cough,
headache, and malaise and, upon physical examination, may be found to have pharyngitis (inflamed throat),
enlarged lymph nodes, ear or sinus infection, bronchitis, or croup. Diagnosis is established by chest X-rays and
blood tests. Although treatment with erythromycin or tetracycline may shorten the illness, it can last for weeks.
Mycoplasmas may also cause a red, bumpy rash—usually on the trunk or back—that is occasionally vesicular
(with blisters). Inflammation of the heart muscle and the covering of the heart (pericardium) is rare but can be
caused by mycoplasmas. About one-fourth of the people infected with these organisms experience nausea,
vomiting, diarrhea, and cramping abdominal pain. Inflammation of the pancreas (pancreatitis) or the liver
(hepatitis) may occur, and infection of the brain and spinal cord is a serious complication.
Ureaplasmas can be recovered frequently from the genital areas of healthy persons. The organism can cause
inflammation of the urethra and has been associated with infertility, low birth weight of infants, and repeated
stillbirths. In general, however, ureaplasma infections are mild. Tetracycline is the preferred treatment once the
organism has been established as the cause of infection by microscopic examination of urethral secretions.
Viruses
Viruses are not, strictly speaking, living organisms. Instead, they are nucleic acid fragments packaged within
protein coats that require the machinery of living cells to replicate. Viruses are visible by electron microscopy;
Britannica LaunchPacks | The Treatment and Prevention of Disease
6 of 123© 2020 Encyclopædia Britannica, Inc.
they vary in size from about 25 nanometres for poliovirus to 250 nanometres for smallpox virus. Vaccination has
been the most successful weapon against viral infection; some infections may be treated with antiviral drugs or
interferon (proteins that interfere with viral proliferation).
Viruses of the Herpesviridae family cause a multiplicity of diseases. Those causing infections in humans are the
varicella-zoster virus (VZV), which causes chickenpox and herpes zoster (shingles); the Epstein-Barr virus, which
causes infectious mononucleosis; the cytomegalovirus, which is most often associated with infections of
newborn infants and immunocompromised people; and herpes simplex virus, which causes cold sores and
herpetic venereal (sexually transmitted) diseases.
There are two serotypes of herpes simplex virus, HSV-1 and HSV-2. HSV-1 is the common cause of cold sores.
The primary infection usually occurs in childhood and is without symptoms in 50 to 80 percent of cases. Between
10 and 20 percent of infected individuals have recurrences precipitated by emotional stress or by other illness.
HSV-1 can also cause infections of the eye, central nervous system, and skin. Serious infections leading to death
may occur in immunocompromised persons. HSV-2 is associated most often with herpetic lesions of the genital
area. The involved area includes the vagina, cervix, vulva, and, occasionally, the urethra in females and the
head of the penis in males; it may also cause an infection at the site of an abrasion. The disease is usually
transmitted by sexual contact. In herpetic sexually transmitted diseases, the lesions are small, red, painful spots
that quickly vesiculate, become filled with fluid, and quickly rupture, leaving eroded areas that eventually
become scabbed. These primary lesions occur from two to eight days after exposure and may be present for up
to three weeks. Viral shedding and pain usually resolve in two weeks. When infections recur, the duration of the
pain, lesions, and viral shedding is approximately 10 days.
There are numerous other viruses that are transmitted between humans and that are significant causes of
illness and death. Seasonal influenza viruses, for example, circulate globally every year, causing illness in tens of
millions of people worldwide; an estimated 290,000 to nearly 650,000 people die from seasonal influenza each
year.
In addition, new types of infectious viruses emerge periodically. In many instances, these viruses “jump” to
humans from an animal reservoir, such as bats, pigs, or primates; this occurs when a human is in close contact
with an animal that carries the virus. Often the virus then evolves to become transmissible between humans.
Examples of infectious viruses that originated from animal reservoirs in the mid-20th or early 21st century and
went on to cause epidemics or pandemics of disease in humans include ebolaviruses, SARS coronavirus,
influenza A H1N1, human immunodeficiency virus (HIV/AIDS), and SARS-CoV-2 coronavirus.
Fungi
Fungi are large organisms that usually live on dead and rotting animal and plant matter. They are found mostly
in soil, on objects contaminated with soil, on plants and animals, and on skin, and they may also be airborne.
Fungi may exist as yeasts or molds and may alternate between the two forms, depending on environmental
conditions. Yeasts are simple cells, 3 to 5 micrometres (0.0001 to 0.0002 inch) in diameter. Molds consist of
filamentous branching structures (called hyphae), 2 to 10 micrometres in diameter, that are formed of several
cells lying end to end. Fungal diseases in humans are called mycoses; they include such disorders as
histoplasmosis, coccidioidomycosis, and blastomycosis. These diseases can be mild, characterized by an upper
respiratory infection, or severe, involving the bloodstream and every organ system. Fungi may cause
devastating disease in persons whose defenses against infection have been weakened by malnutrition, cancer,
or the use of immunosuppressive drugs. Specific types of antibiotics known as antifungals are effective in their
treatment.

Britannica LaunchPacks | The Treatment and Prevention of Disease
7 of 123© 2020 Encyclopædia Britannica, Inc.
Parasites
Among the infectious parasites are the protozoans, unicellular organisms that have no cell wall, that cause such
diseases as malaria. The various species of malarial parasites are about 4 micrometres (0.0002 inch) in
diameter. At the other extreme, the tapeworm can grow to several metres in length; treatment is designed
either to kill the worm or to dislodge it from its host.
The worm causes ascariasis, one of the most prevalent infections in the world. lives Ascaris lumbricoides Ascarisin the soil, and its eggs are ingested with contaminated food. The eggs hatch in the human intestine, and the
worms then travel through the bloodstream to the liver, heart, and lungs. They can cause pneumonia,
perforations of the intestine, or blockage of the bile ducts, but infected people usually have no symptoms
beyond the passage of worms in the stool. Specific treatment is available and prognosis is excellent.
Infections are also caused by whipworms, genus , and pinworms, , each Trichuris Enterobius vermicularispopularly named for its shape. The former is parasitic in the human large intestine and may cause chronic
diarrhea. The latter can be found throughout the gastrointestinal tract, especially in children, and can cause poor
appetite, loss of weight, anemia, and itching in the anal area (where it lays its eggs). Both conditions are easily
diagnosed and treated with drugs.
Modes of survival
Infectious agents have various methods of survival. Some depend on rapid multiplication and rapid spread from
one host to another. For example, when the measles virus enters the body, it multiplies for a week or two and
then enters the bloodstream and spreads to every organ. For several days before a rash appears, the surface
cells of the respiratory tract are bursting with measles virus, and vast quantities are shed every time the
infected person coughs or sneezes. A day or two after the rash appears, the amount of antibody (protein
produced in response to a pathogen) rises in the bloodstream, neutralizing the virus and stopping further
shedding. The patient rapidly becomes noninfectious but already may have spread the virus to others. In this
way an epidemic can rapidly occur. Many other infectious agents—for example, influenza virus—survive in this
manner. How such viruses exist between epidemics is, in some cases, less clear.
Learn why tuberculosis is still a threat to the human population.
© American Chemical Society
The picture is different in more-chronic infections. In tuberculosis there is neither overwhelming multiplication
nor rapid shedding of the tubercle bacillus. Rather, the bacilli remain in the infected person’s body for a long
period, slowly forming areas of chronic inflammation that may from time to time break down and allow them to
escape.
Some organisms form spores, a resting or dormant stage that is resistant to heat, cold, drying, and chemical
action. Spore-forming organisms can survive for months or years under the most adverse conditions and may
Britannica LaunchPacks | The Treatment and Prevention of Disease
8 of 123© 2020 Encyclopædia Britannica, Inc.
not, in fact, be highly infectious. The bacterium that causes tetanus, , is present everywhere in Clostridium tetanithe environment—in soil, in dust, on window ledges and floors—and yet tetanus is an uncommon disease,
especially in developed countries. The same is true of the anthrax bacterium, . Although Bacillus anthracisusually present in abundance in factories in which rawhides and animal wool and hair are handled, it rarely
causes anthrax in employees. , the cause of botulism, produces one of the most lethal Clostridium botulinumtoxins that can afflict humans, and yet the disease is one of the rarest because the microorganism depends for
its survival on its resistant spore.
In contrast to these relatively independent organisms, there are others that cannot exist at all outside the
human body. The germs of syphilis and gonorrhea, for example, depend for survival on their ability to infect and
their adaptation to the human environment.
Some organisms have complicated life cycles and depend on more than one host. The malarial parasite must
spend a portion of its life cycle inside a mosquito, while the liver fluke , an occasional human Fasciola hepaticaparasite, spends part of its life in the body of a land animal such as a sheep, part in a water snail, and part in the
open air as a cyst attached to grass.
Commensal organisms
All of the outer surfaces of the human body are covered with agents that normally do no harm and may, in fact,
be beneficial. Those commensal organisms on the skin help to break down dying skin cells or to destroy debris
secreted by the many minute glands and pores that open on the skin. Many of the organisms in the
intestinaltract break down complex waste products into simple substances, and others help in the manufacture
of chemical compounds that are essential to human life.
The gastrointestinal tract is considered in this regard to be one of these “outer” surfaces since it is formed by
the intucking, or invagination, of the ectoderm, or outer surface, of the body. The mouth, nose, and sinuses
(spaces inside the bones of the face) are also considered to be external structures because of their direct
contact with the outside environment. Both the gastrointestinal tract and the mouth, nose, and sinuses are
heavily populated with microorganisms, some of which are true commensals—living in humans and deriving
their sustenance from the surface cells of the body without doing any harm—and others of which are
indistinguishable from disease germs. The latter may live like true commensals in a particular tract in a human
and never cause disease, despite their potential to do so. When the environment is altered, however, they are
capable of causing severe illness in their host, or, without harming their host, they may infect another person
with a serious disease.
It is not known why, for example, the hemolytic streptococcus bacterium can live for months in the throat
without causing harm and then suddenly cause an acute attack of tonsillitis or how an apparently harmless
pneumococcus gives rise to pneumonia. Similarly, it is not understood how a person can harmlessly carry
type B in the throat but then become ill when the organism invades the body and Haemophilus influenzaecauses one of the most severe forms of meningitis. It may be that external influences, such as changes in
temperature or humidity, are enough to upset the balance between host and parasite or that a new microbial
invader enters and, by competing for some element in the environment, forces the original parasite to react
more violently with its host. The term , often used to describe conditions at the onset of lowered resistanceinfectious disease, is not specific and simply implies any change in the immune system of the host.
A microorganism’s environment can be changed radically, of course. If antibiotics are administered, the body’s
commensal organisms can be killed, and other, less-innocuous organisms may take their place. In the mouth and
throat, penicillin may eradicate pneumococci, streptococci, and other bacteria that are sensitive to the drug,

Britannica LaunchPacks | The Treatment and Prevention of Disease
9 of 123© 2020 Encyclopædia Britannica, Inc.
while microorganisms that are insensitive, such as , may then proliferate and cause thrush (an Candida albicansinflammatory condition of the mouth and throat). In the intestinal tract, an antibiotic may kill most of the
bacterial microorganisms that are normally present and allow dangerous bacteria, such as Pseudomonas , to multiply and perhaps to invade the bloodstream and the tissues of the body. If an infectious aeruginosa
agent—for example, —reaches the intestinal tract, treatment with an antibiotic may have an effect Salmonellathat differs from what was intended. Instead of attacking and destroying the salmonella, it may kill the normal
inhabitants of the bowel and allow the salmonella to flourish and persist in the absence of competition from
other bacterial microorganisms.
Effects of environment on human diseaseHuman activity
Family patterns
Humans are social animals. As a result, human social habits and circumstances influence the spread of infectious
agents. Crowded family living conditions facilitate the passage of disease-causing organisms from one person to
another. This is true whether the germs pass through the air from one respiratory tract to another or whether
they are bowel organisms that depend for their passage on close personal hand-to-mouth contact or on lapses of
sanitation and hygiene.
The composition of the family unit is also important. In families with infants and preschool children, infection
spreads more readily, for children of this age are both more susceptible to infection and, because of their
undeveloped hygiene habits, more likely to share their microbes with other family members. Because of this
close and confined contact, infectious agents are spread more rapidly.
Distinction must be made between disease and infection. The virus of poliomyelitis, for example, spreads easily
in conditions of close contact (infection), but it usually causes no active disease. When it does cause active
disease, it attacks older people much more severely than the young. Children in more-crowded homes, for
example, are likely to be infected at an early age and, if illness results, it is usually mild. In less-crowded
conditions, young children are exposed less often to infection; when they first encounter the virus at an older
age, they tend to suffer more severely. The difference between infection and disease is seen even more rapidly
in early childhood, when infection leads more often to immunity than to illness. Under high standards of hygiene,
young children are exposed less frequently, and fewer develop immunity in early life, with the result that
paralytic illness, a rarity under the former conditions, is seen frequently in older children and adults. The pattern
of infection and disease, however, can be changed. In the case of the poliomyelitis virus, only immunization can
abolish both infection and disease.
Population density
Density of population does not of itself determine the ease with which infection spreads through a population.
Problems tend to arise primarily when populations become so dense as to cause overcrowding. Overcrowding is
often associated with decreases in quality of living conditions and sanitation, and hence the rate of agent
transmission is typically very high in such areas. Thus, overcrowded cities or densely populated areas of cities
can potentially serve as breeding grounds for infectious agents, which may facilitate their evolution, particularly
in the case of viruses and bacteria. Rapid cycling between humans and other hosts, such as rats or mice, can
result in the emergence of new strains capable of causing serious disease.
Britannica LaunchPacks | The Treatment and Prevention of Disease
10 of 123© 2020 Encyclopædia Britannica, Inc.
Social habits
The vampire bats of Brazil, which transmit paralytic rabies, bite cattle but not ranchers, presumably because
ranchers are few but cattle are plentiful on the plains of Brazil. Bat-transmitted rabies, however, does occur in
humans in Trinidad, where herdsmen sleep in shacks near their animals. The mechanism of infection is the same
in Brazil and Trinidad, but the difference in social habits affects the incidence of the disease.
During the early 20th century in Malta, goats were milked at the customers’ doors, and a species in the Brucellamilk caused a disease that was common enough to be called Malta fever. When the pasteurization of milk
became compulsory, Malta fever almost disappeared from the island. (It continued to occur in rural areas where
people still drank their milk raw and were in daily contact with their infected animals.)
Important alterations in environment also occur when children in a modern community first go to school. Colds,
coughs, sore throats, and swollen neck glands can occur one after the other. In a nursery school, with young
children whose hygiene habits are undeveloped, outbreaks of dysentery and other bowel infections may occur,
and among children who take their midday meal at school, foodborne infection caused by a breakdown in
hygiene can sweep through entire classes of students. These are dangers against which the children are
protected to some extent at home but against which they have no defense when they move to the school
environment.
Changing food habits among the general population also affect the environment for humans and microbes.
Meals served in restaurants, for example, offer a greater danger of food poisoning if the standard of hygiene for
food preparation is flawed. The purchase and preparation of poultry—which is often heavily infected with
—present a particular danger. If chickens are bought fresh from a farm or shop and cooked in an oven Salmonellaat home, food poisoning from eating them is rare. If poultry is purchased while it is deep-frozen and then not
fully thawed before it is cooked, there is a good chance that insufficient heat penetration will allow the
—which thrive in the cold—to survive in the meat’s centre and infect the people who eat it.Salmonella
Temperature and humidity
At a social gathering, the human density per square yard may be much greater than in any home, and humidity
and temperature may rise to levels uncomfortable for humans but ideal for microbes. Virus-containing droplets
pass easily from one person to another, and an outbreak of the common cold may result.
In contrast, members of scientific expeditions have spent whole winters in the Arctic or Antarctic without any
respiratory illness, only to catch severe colds upon the arrival of a supply ship in the early summer. This is
because viruses, not cold temperatures, cause colds. During polar expeditions, the members rapidly develop
immunity to the viruses they bring with them, and, throughout the long winter, they encounter no new ones.
Their colds in the summer are caused by viruses imported by the crew of the supply ship. When the members of
the expedition return on the ship to temperate zones, they again come down with colds, this time caught from
friends and relatives who have spent the winter at home.

Britannica LaunchPacks | The Treatment and Prevention of Disease
11 of 123© 2020 Encyclopædia Britannica, Inc.
Movement
Refugees from Kyrgyzstan waiting in a refugee camp near the village of Erkishlok, Uzbekistan, June…
Anvar Ilyasov—AP/Shutterstock.com
Movement into a new environment often is followed by an outbreak of infectious disease. On pilgrimages and in
wars, improvised feeding and sanitation lead to outbreaks of such intestinal infections as dysentery, cholera, and
typhoid fever, and sometimes more have died in war from these diseases than have been killed in the fighting.
People entering isolated communities may carry a disease such as measles with them, and the disease may
then spread with astonishing rapidity and often with enhanced virulence. A traveler from Copenhagen carried
measles virus with him to the Faroe Islands in 1846, and 6,000 of the 8,000 inhabitants caught the disease. Most
of those who escaped were old enough to have acquired immunity during a measles outbreak 65 years earlier.
In Fiji a disastrous epidemic of measles in 1875 killed one-fourth of the population. In these cases, the change of
environment favoured the virus. Nearly every person in such “virgin” populations is susceptible to infection, so
that a virus can multiply and spread unhindered. In a modern city population, by contrast, measles virus mainly
affects susceptible young children. When it has run through them, the epidemic must die down because of a lack
of susceptible people, and the virus does not spread again until a new generation of children is on hand. With
the use of measles vaccine, the supply of susceptible young children is reduced, and the virus cannot spread
and multiply and must die out.
An innocent change in environment such as that experienced during camping can lead to infection if it brings a
person into contact with sources of infection that are absent at home. Picnicking in a wood, a person may be
bitten by a tick carrying the virus of one of several forms of encephalitis; as he swims in a canal or river, his skin
may be penetrated by the organisms that cause leptospirosis. He may come upon some watercress growing wild
in the damp corner of a field and may swallow with the cress almost invisible specks of life that will grow into
liver flukes in his body, giving him fascioliasis, an illness that is common in cattle and sheep but that can spread
to humans when circumstances are in its favour.
Occupation and commerce
In occupational and commercial undertakings, people often manipulate their environment and, in so doing,
expose themselves to infection. A farmer in his fields is exposed to damp conditions in which disease
microorganisms flourish. While clearing out a ditch, he may be infected with leptospires passed into the water in
rats’ urine. In his barns he may be exposed to brucellosis if his herd of cattle is infected or to salmonellosis or Q
fever. Slaughterhouse workers run similar risks, as do veterinarians. A worker in a dock or tannery may get
anthrax from imported hides; an upholsterer may get the disease from wool and hair; and a worker mending
sacks that have contained bone meal may contract the disease from germs still clinging to the sack.
Britannica LaunchPacks | The Treatment and Prevention of Disease
12 of 123© 2020 Encyclopædia Britannica, Inc.
Workers in packing plants and shops often are infected from the raw meat that they handle; they are sometimes
regarded as carriers and causes of outbreaks of food poisoning, but as often as not they are victims Salmonellarather than causes. Workers in poultry plants can contract salmonellosis, more rarely psittacosis or a viral
infection of the eye, from the birds that they handle. Forestry workers who enter a reserve may upset the
balance of nature of the area and expose themselves to attack from the undergrowth or the trees by insect
vectors of disease that, if undisturbed, would never come into contact with humans. Whenever people
manipulate the environment—by herding animals, by importing goods from abroad, by draining a lake, or by
laying a pipe through swampy land, and in many other seemingly innocent ways—they run the chance of
interfering with microbial life and attracting into their own environment agents of disease that they might not
otherwise ever encounter.
The inanimate environment
Dust cannot cause infectious disease unless it contains the living agents of the infection. Yet the term inanimateis a convenient one to use when infectious disease arises from contact with an environment in which there is no
obvious direct living contact between the source and the victim of an infection. A pencil is an inanimate object,
but if it is sucked by a child with scarlet fever and then by a second child, the organisms causing the disease can
be conveyed to the second child. Many such objects—a handkerchief or a towel, for example—may convey
infection under favourable conditions, and, when they do so, they are known as fomites.
Dust is perhaps one of the most common inanimate elements capable of conveying disease. Organisms present
in dust may get on food and be swallowed, settle on the skin and infect it, or be breathed into the respiratory
passages. Some germs—the causative agents of anthrax and tetanus, of Q fever, brucellosis, and psittacosis, for
example—can live for long periods dried in dust. Under certain conditions all may be dangerous, but under
different conditions there may be no danger. The germ that causes tetanus, , is one of the Clostridium tetanimost common germs in dust, but the incidence of tetanus varies greatly in different parts of the world. In many
countries it is rare, in others common, and the difference may be related to slight differences in human
behaviour or custom. The wearing of shoes in temperate climates protects the wearer against many wounds,
while the barefoot child in the tropics sustains many puncture wounds of the feet that, although minor, may yet
carry tetanus spores into the tissues of the foot, where conditions may be ideal for germination and the
production of toxin. Obstetrical practices in some parts of the world can lead to infection of the newborn child.
Other, more subtle influences, such as changes of temperature or humidity, may affect the spread of diseases
by dust. A long wet winter followed by a dry summer may encourage the growth of molds in hay, and the dust,
when the hay is disturbed, may lead to infection of the farmer’s lungs.
Water is not a favourable medium for the growth and multiplication of microorganisms, and yet many can
survive in it long enough to carry infection to humans. Cholera and typhoid fever are both waterborne diseases,
and the virus of hepatitis A also can survive in water. But the mere presence of a microorganism in water does
not necessarily lead to the spread of disease. People have swum in water polluted with without Salmonella typhigetting typhoid fever, while others eating shellfish from the same water have developed the disease. The same
may be true of hepatitis; the eating of clams from infected water has often caused the disease, whereas
swimming has not proved to be a hazard. Shellfish concentrate germs in their tissues, which is probably why
they can transmit diseases.
Water is carried to humans in pipes for drinking, but it is also carried away in pipes as sewage. Defects in these
systems may permit water to pass from one to the other, and microorganisms from sewage may get into
drinking water. Wells and other water sources can be contaminated by badly sited septic tanks, manure heaps,
or garbage dumps. Properly treated, such water is safe to drink; if drunk untreated, disease may follow.
Britannica LaunchPacks | The Treatment and Prevention of Disease
13 of 123© 2020 Encyclopædia Britannica, Inc.
The soil of gardens and farmlands can harbour disease organisms, as can food. Smoke, fog, and tobacco can
affect the human respiratory tract and render it more vulnerable to disease. Air is probably the most common
source of infectious agents. The whole of the environment is, in fact, filled with organisms and objects that can
transmit infectious agents to humans.
Immune response to infectionWhen a pathogenic (disease-causing) microorganism invades the body for the first time, the clinical (observable)
response may range from nothing at all, through various degrees of nonspecific reactions, to specific infectious
disease. Immunologically, however, there is always a response, the purpose of which is defense. If the defense is
completely successful, there is no obvious bodily reaction; if it is partially successful, the affected person
exhibits symptoms but recovers from an infectious disease; if unsuccessful, the person may be overwhelmed by
the infectious process and die.
The two responses—the clinical and the immunologic—can be illustrated by the natural history of the disease
poliomyelitis. When the virus of this disease enters the body for the first time, it multiplies in the throat and in
the intestinal tract. In some people, it gets no farther; virus is shed to the outside from the throat and the bowel
for a few weeks, and then the shedding ceases and the infection is over. The host, however, has responded and
has developed circulating antibodies to a type of poliovirus. These antibodies are specific antipoliovirus proteins
in the blood and body fluids that subsequently prevent disease should the poliovirus again be encountered. In
addition, the infected individual develops an antipoliovirus response in a subset of white blood cells known as T
cells. Antipoliovirus T cells persist throughout the individual’s lifetime.
In other people, the same process occurs but some virus also gets into the bloodstream, where it circulates for a
short time before being eliminated. In a few individuals, the virus passes from the bloodstream into the central
nervous system, where it circulates for a short time before being eliminated. Finally, in some individuals, the
virus passes from the bloodstream into the central nervous system, where it may enter and destroy some of the
nerve cells that control movement in the body and so cause paralysis. Such paralysis is the least-common result
of infection with poliomyelitis virus; most infected persons have no symptoms at all. Those whose bloodstream
contains virus often have a mild illness, consisting of no more than malaise, slight headache, and possibly a sore
throat. This so-called minor illness of poliomyelitis is unlikely to be recognized except by those in close contact
with someone later paralyzed by the disease.
If the nervous system becomes invaded by the virus, the infected person has a severe headache and other
symptoms suggesting meningitis. Such persons are acutely ill, but most recover their normal health after about
one week. Only a few of those with this type of infection have paralysis. Of all the people infected with
poliomyelitis virus, not more than 1 in 100, possibly as few as 1 in 1,000, has paralysis, though paralysis is the
dominant feature of the fully developed clinical picture of poliomyelitis. This poliomyelitis is actually an
uncommon complication of poliovirus infection.
This wide range of response to the poliomyelitis virus is characteristic of most infections, though the proportions
may vary. Influenza virus, for example, may cause symptoms ranging from a mild cold to a feverish illness,
severe laryngitis (inflammation of the larynx, or voice box) or bronchitis, or an overwhelming and fatal
pneumonia. The proportions of a population with these differing outcomes may vary from one epidemic to
another. There is perhaps more uniformity of pattern in the operation of the defense mechanisms of the body,
called the immune response.

Britannica LaunchPacks | The Treatment and Prevention of Disease
14 of 123© 2020 Encyclopædia Britannica, Inc.
Natural and acquired immunity
Every animal species possesses some natural resistance to disease. Humans have a high degree of resistance to
foot-and-mouth disease, for example, while the cattle and sheep with which they may be in close contact suffer
in the thousands from it. Rats are highly resistant to diphtheria, whereas unimmunized children readily contract
the disease.
What such resistance depends on is not always well understood. In the case of many viruses, resistance is
related to the presence on the cell surface of protein receptors that bind to the virus, allowing it to gain entry
into the cell and thus cause infection. Presumably, most causes of absolute resistance are genetically
determined; it is possible, for example, to produce by selective breeding two strains of rabbits, one highly
susceptible to tuberculosis, the other highly resistant. In humans there may be apparent racial differences, but it
is always important to disentangle such factors as climate, nutrition, and economics from those that might be
genetically determined. In some tropical and subtropical countries, for example, poliomyelitis is a rare clinical
disease, though a common infection, but unimmunized visitors to such countries often contract serious clinical
forms of the disease. The absence of serious disease in the residents is due not to natural resistance, however,
but to resistance acquired after repeated exposure to poliovirus from infancy onward. Unimmunized visitors from
other countries, with perhaps stricter standards of hygiene, are protected from such immunizing exposures and
have no acquired resistance to the virus when they encounter it as adults.
Natural resistance, in contrast to acquired immunity, does not depend upon such exposures. The human skin
obviously has great inherent powers of resistance to infection, for most cuts and abrasions heal quickly, though
often they are smothered with potentially pathogenic microorganisms. If an equal number of typhoid bacteria
are spread on a person’s skin and on a glass plate, those on the skin die much more quickly than do those on
the plate, suggesting that the skin has some bactericidal property against typhoid germs. The skin also varies in
its resistance to infectious organisms at different ages: impetigo is a common bacterial infection of children’s
skin but is rarer in adults, and acne is a common infection of the skin of adolescents but is uncommon in
childhood or in older adults. The phenomenon of natural immunity can be illustrated equally well with examples
from the respiratory, intestinal, or genital tracts, where large surface areas are exposed to potentially infective
agents and yet infection does not occur.
If an organism causes local infection or gains entry into the bloodstream, a complicated series of events ensues.
These events are described in detail in the article immune system, but they can be summarized as follows:
special types of white blood cells called polymorphonuclear leukocytes or granulocytes, which are normally
manufactured in the bone marrow and which circulate in the blood, move to the site of the infection. Some of
these cells reach the site by chance, in a process called random migration, since almost every body site is
supplied constantly with the blood in which these cells circulate. Additional granulocytes are attracted and
directed to the sites of infection in a process called directed migration, or chemotaxis.
When a granulocyte reaches the invading organism, it attempts to ingest the invader. Ingestion of bacteria may
require the help of still other components of the blood, called opsonins, which act to coat the bacterial cell wall
and prepare it for ingestion. An opsonin generally is a protein substance, such as one of the circulating
immunoglobulins or complement components.
Once a prepared bacterium has been taken inside the white blood cell, a complex series of biochemical events
occurs. A bacterium-containing vacuole (phagosome) may combine with another vacuole that contains bacterial-
degrading proteins (lysozymes). The bacterium may be killed, but its products pass into the bloodstream, where
they come in contact with other circulating white blood cells called lymphocytes. Two general types of

Britannica LaunchPacks | The Treatment and Prevention of Disease
15 of 123© 2020 Encyclopædia Britannica, Inc.
lymphocytes—T cells and B cells—are of great importance in protecting the human host. When a T cell
encounters bacterial products, either directly or via presentation by a special antigen-presenting cell, it is
sensitized to recognize the material as foreign, and, once sensitized, it possesses an immunologic memory. If the
T cell encounters the same bacterial product again, it immediately recognizes it and sets up an appropriate
defense more rapidly than it did on the first encounter. The ability of a T cell to function normally, providing what
is generally referred to as cellular immunity, is dependent on the thymus gland. The lack of a thymus, therefore,
impairs the body’s ability to defend itself against various types of infections.
After a T cell has encountered and responded to a foreign bacterium, it interacts with B cells, which are
responsible for producing circulating proteins called immunoglobulins or antibodies. There are various types of B
cells, each of which can produce only one of the five known forms of immunoglobulin (Ig). The first
immunoglobulin to be produced is IgM. Later, during recovery from infection, the immunoglobulin IgG, which can
specifically kill the invading microorganism, is produced. If the same microorganism invades the host again, the
B cell immediately responds with a dramatic production of IgG specific for that organism, rapidly killing it and
preventing disease.
In many cases, acquired immunity is lifelong, as with measles or rubella. In other instances, it can be short-lived,
lasting not more than a few months. The persistence of acquired immunity is related not only to the level of
circulating antibody but also to sensitized T cells (cell-mediated immunity). Although both cell-mediated
immunity and humoral (B-cell) immunity are important, their relative significance in protecting a person against
disease varies with particular microorganisms. For example, antibody is of great importance in protection
against common bacterial infections such as pneumococcal pneumonia or streptococcal disease and against
bacterial toxins, whereas cell-mediated immunity is of greater importance in protection against viruses such as
measles or against the bacteria that cause tuberculosis.
Immunization
Antibodies are produced in the body in response to either infection with an organism or, through vaccination, the
administration of a live or inactivated organism or its toxin by mouth or by injection. When given alive, the
organisms are weakened, or attenuated, by some laboratory means so that they still stimulate antibodies but do
not produce their characteristic disease. However stimulated, the antibody-producing cells of the body remain
sensitized to the infectious agent and can respond to it again, pouring out more antibody. One attack of a
disease, therefore, often renders a person immune to a second attack, providing the theoretical basis for active
immunization by vaccines.
Antibody can be passed from one person to another, conferring protection on the antibody recipient. In such a
case, however, the antibody has not been produced in the body of the second person, nor have his antibody-
producing cells been stimulated. The antibody is then a foreign substance and is eventually eliminated from the
body, and protection is short-lived. The most common form of this type of passive immunity is the transference
of antibodies from a mother through the placenta to her unborn child. This is why a disease such as measles is
uncommon in babies younger than one year. After that age, the infant has lost all of its maternal antibody and
becomes susceptible to the disease unless protective measures, such as measles vaccination, are taken.
Sometimes antibody is extracted in the form of immunoglobulin from blood taken from immune persons and is
injected into susceptible persons to give them temporary protection against a disease, such as measles or
hepatitis A.
Generally, active immunization is offered before the anticipated time of exposure to an infectious disease. When
unvaccinated people are exposed to an infectious disease, two alternatives are available: active immunization
may be initiated immediately in the expectation that immunity can be developed during the incubation period of

Britannica LaunchPacks | The Treatment and Prevention of Disease
16 of 123© 2020 Encyclopædia Britannica, Inc.
the disease, or passive immunity can be provided for the interim period and then active immunization given at
an appropriate time. The antigens (foreign substances in the body that stimulate the immune defense system)
introduced in the process of active immunization can be live attenuated viruses or bacteria, killed
microorganisms or inactivated toxins (toxoids), or purified cell wall products (polysaccharide capsules, protein
antigens).
There are five basic requirements for an ideal vaccine. The agents used for immunization should not in
themselves produce disease. The immunizing agent should induce long-lasting, ideally permanent, immunity.
The agent used for immunization should not be transmissible to susceptible contacts of the person being
vaccinated. The vaccine should be easy to produce, its potency easy to assess, and the antibody response to it
measurable with common and inexpensive techniques. Finally, the agent in the vaccine should be free of
contaminating substances. It is also recognized, however, that vaccine transmissibility can be helpful—e.g., in
the case of live polio vaccine, which can be spread from vaccinated children to others who have not been
vaccinated.
The route by which an antigen is administered frequently determines the type and duration of antibody
response. For example, intramuscular injection of inactivated poliomyelitis virus (Salk vaccine) generates less
production of serum antibody and induces only a temporary systemic immunity; it may not produce substantial
local gastrointestinal immunity and, therefore, may not prevent the carrying of the virus in the gastrointestinal
tract. Live, attenuated, oral poliomyelitis virus (Sabin vaccine) induces both local gastrointestinal and systemic
antibody production; thus, immunization by mouth is preferred.
The schedule by which a vaccine is given depends upon the epidemiology of the naturally occurring disease, the
duration of immunity that can be induced, the immunologic status of the host, and, in some cases, the
availability of the patient. Measles, for example, is present in many communities and poses a potential threat to
many children over 5 months of age. A substantial number of infants, however, are born with measles antibody
from their mothers, and this maternal antibody interferes with an adequate antibody response until they are
between 12 and 15 months of age. Generally, the immunization of infants after the age of 15 months benefits
the community at large. In measles outbreaks, however, it may be advisable to alter this schedule and immunize
all infants between 6 and 15 months of age.
Diphtheria toxoid
The introduction of diphtheria toxoid in the early 20th century led to a dramatic reduction in the incidence of the
disease in many parts of the world. Primary prevention programs consisting of communitywide routine
immunization of infants and children have largely eliminated the morbidity and mortality previously associated
with diphtheria. Although the reported annual incidence of diphtheria has been relatively constant since the
1960s, local epidemics continue to occur. A complacent attitude toward immunization in some nations largely
reflects a lack of awareness of the public health hazard that can arise if the proportion of susceptible individuals
is significant enough to allow renewed outbreaks. Also, adequate immunization does not completely eliminate
the potential for transmission of the bacterium . Carriage of in the Corynebacterium diphtheriae C. diphtheriaenose or throat has been well documented in fully immunized persons who clearly may transmit the disease to
susceptible individuals.
The vaccine—prepared by the treatment of toxin with formaldehyde—is available in both fluid and C. diphtheriaeadsorbed forms, the latter being recommended. Diphtheria toxoid is also available combined with tetanus toxoid
and pertussis vaccine (DPT), combined with tetanus toxoid alone (DT), and combined with tetanus toxoid for
adults (Td). The Td preparation contains only 15 to 20 percent of the diphtheria toxoid present in the DPT
vaccine and is more suitable for use in older children and adults.
Pertussis vaccine
Britannica LaunchPacks | The Treatment and Prevention of Disease
17 of 123© 2020 Encyclopædia Britannica, Inc.
Pertussis vaccine
The number of cases of pertussis (whooping cough), a serious disease that is frequently fatal in infancy, can be
dramatically reduced by the use of the pertussis vaccine. The pertussis immunizing agent is included in the DPT
vaccine. Active immunity can be induced by three injections given eight weeks apart.
Tetanus toxoid
The efficacy of active immunization against tetanus was illustrated most dramatically during World War II, when
the introduction of tetanus toxoid among military personnel virtually eliminated the occurrence of the disease as
a result of war-related injuries. Since then, the routine immunization of civilian populations with tetanus toxoid
has resulted in the decreased incidence of tetanus. In the United States, for example, 50 or fewer cases of
tetanus are reported each year, the majority of deaths occurring in persons more than 60 years of age. In
virtually all cases, the disease has been reported in unimmunized or inadequately immunized individuals.
Because it provides long-lasting protection and relative safety in humans, tetanus toxoid has proved to be an
ideal vaccine. Tetanus toxoid is available in both vaccine fluid and alum-precipitated preparations.
Commercially, tetanus toxoid is available in DPT, Td, and T (tetanus toxoid, adsorbed) preparations. DPT is
recommended for infants, while the Td form is recommended at 12 and again at 18 years of age and only once
every 10 years thereafter. If a person sustains a wound prone to tetanus (such as a puncture wound or a wound
contaminated with animal excreta), Td is given along with tetanus immune globulin (TIG) to prevent occurrence
of the disease.
Polio vaccine
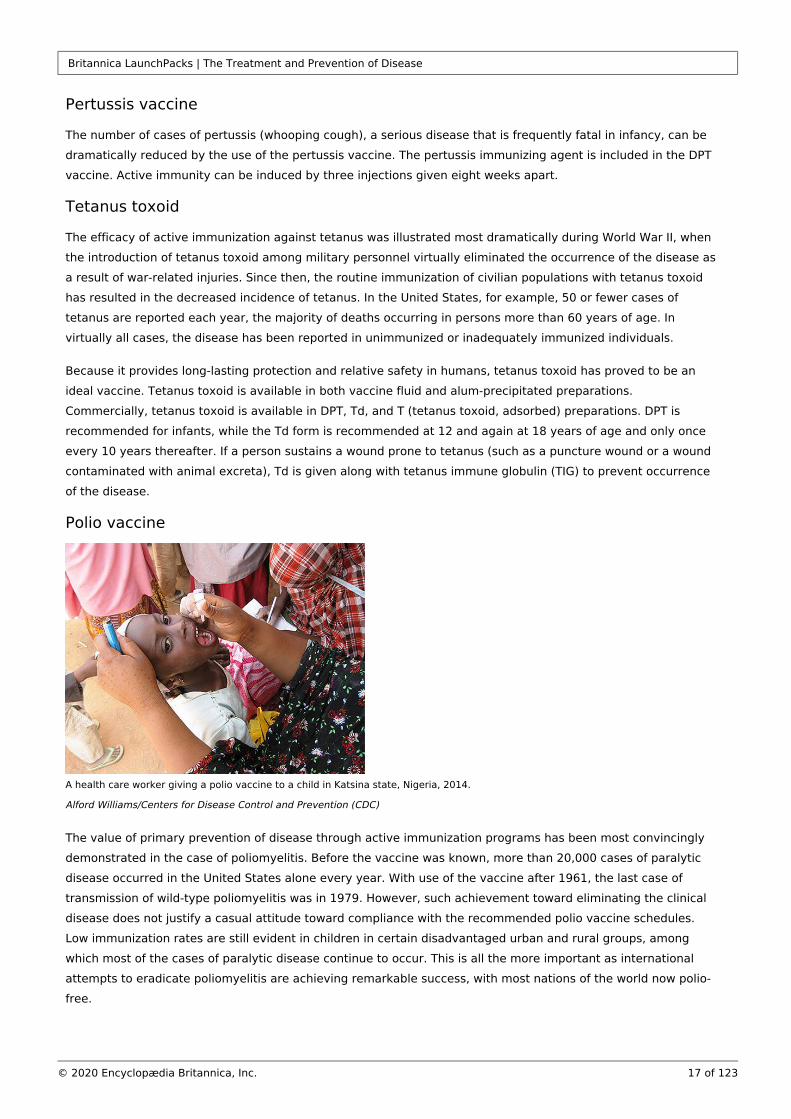
A health care worker giving a polio vaccine to a child in Katsina state, Nigeria, 2014.
Alford Williams/Centers for Disease Control and Prevention (CDC)
The value of primary prevention of disease through active immunization programs has been most convincingly
demonstrated in the case of poliomyelitis. Before the vaccine was known, more than 20,000 cases of paralytic
disease occurred in the United States alone every year. With use of the vaccine after 1961, the last case of
transmission of wild-type poliomyelitis was in 1979. However, such achievement toward eliminating the clinical
disease does not justify a casual attitude toward compliance with the recommended polio vaccine schedules.
Low immunization rates are still evident in children in certain disadvantaged urban and rural groups, among
which most of the cases of paralytic disease continue to occur. This is all the more important as international
attempts to eradicate poliomyelitis are achieving remarkable success, with most nations of the world now polio-
free.

Britannica LaunchPacks | The Treatment and Prevention of Disease
18 of 123© 2020 Encyclopædia Britannica, Inc.
Live trivalent oral poliovirus vaccine (OPV) is used for routine mass immunization but is not recommended for
patients with altered states of immunity (for example, those with cancer or an immune deficiency disease or
those receiving immunosuppressive therapy) or for children whose siblings are known to have an immune
deficiency disease. Inactivated poliovirus vaccine (IPV) is used for immunodeficient or immunosuppressed
patients and for the primary immunization of adults because of their greater susceptibility to paralytic disease.
In 2000, as poliomyelitis eradication appeared imminent, the United States switched from OPV to IPV as a
routine recommended infant vaccine.
Rubella (German measles) vaccine
A major epidemic in the United States in 1964 resulted in more than 20,000 cases of congenital rubella. In
consequence, active immunization programs with attenuated rubella vaccine were initiated in 1969 in an
attempt to prevent an expected epidemic in the early 1970s. The immunization of all children from 1 to 12 years
of age was aimed at reducing the reservoir and transmission of wild rubella virus and, secondarily, at diminishing
the risk of rubella infection in susceptible pregnant women. This national policy contrasts with that of the United
Kingdom, where only girls from 10 to 14 years of age who do not have detectable antibody levels to rubella virus
are immunized. Proponents of the British policy have argued that natural rubella infection, which confers lifelong
immunity, is more effective than vaccine-induced protection of uncertain duration and that continued outbreaks
of rubella in the United States (largely in older children and young adults) since the introduction of rubella
vaccines attest to the difficulty of achieving herd (group) immunity for this disease.
Live attenuated rubella vaccine is available in combination with measles vaccine (MR) and in combination with
measles and mumps vaccines (MMR). For routine infant immunization, MMR is given one time at about 15
months of age. Rubella vaccination can be accompanied by mild joint pain and fever in 5 percent of those who
receive it. Vaccination is recommended for all children between the ages of 12 months and puberty. Vaccination
is not recommended for pregnant women. A number of women, however, have inadvertently received rubella
vaccine during pregnancy with no harm to their fetuses being noted.
Measles (rubeola) vaccine
The licensing and distribution of killed measles vaccine in 1963, followed by the development and widespread
use of live attenuated vaccine, have sharply reduced the prevalence of measles and its related morbidity and
mortality in many parts of the world. Additional attenuated vaccine preparations have been developed; though
not fully evaluated, they appear to be safe and highly effective and to confer prolonged, if not lifelong,
protection.
Despite the introduction of effective immunizing agents, measles continues to be a major public health concern.
The continued occurrence of outbreaks of measles, especially among young adults, emphasizes the probable
failure of herd immunity to eliminate measles transmission, despite high local immunization rates in young
children. The outbreaks also indicate the possibility that a small number of appropriately immunized individuals
may not develop solid immunity. It is estimated that about 700,000 to 800,000 people, mostly children, die of
measles each year.
Measles vaccine is commercially available in live attenuated form and is used routinely in the MMR preparation
for infant immunization at about 15 months of age. Susceptible older children or adults who have not had
measles or have not previously received measles vaccine also should receive a single dose.
Britannica LaunchPacks | The Treatment and Prevention of Disease
19 of 123© 2020 Encyclopædia Britannica, Inc.
Mumps vaccine
Mumps is generally a self-limited disease in children but occasionally is moderately debilitating. A live
attenuated mumps vaccine is available alone or in combination with measles and rubella vaccines. No serious
adverse reactions have been reported following mumps immunization.
Pneumococcal vaccine
Streptococcus pneumoniae (pneumococcus) is the most frequent cause of bloodstream infection, pneumonia,
and ear infection and is the third most common cause of bacterial meningitis in children. Pneumococcal infection
is particularly serious among the elderly and among children with sickle-cell anemia, with congenital or acquired
defects in immunity, without spleens, or with abnormally functioning spleens.
Immunity after pneumococcal disease is type-specific and lifelong. The pneumococcal vaccine now available
consists of polysaccharide antigens from many of the most common types of pathogenic pneumococci. It can be
given to children two years of age or older or to adults in a single intramuscular injection. The duration of
protection is unknown.
Meningococcal vaccine
Neisseria meningitidis can cause meningitis (infection of the coverings of the brain and spinal cord) or severe
bloodstream infection known as meningococcemia. In the general population, less than 1 per 400,000 persons is
attacked by the bacterium, while among those younger than one year, the ratio rises to 1 per 100,000. In a day-
care centre in which a primary case of meningococcal disease has occurred, the ratio has been reported at 2 to
100 per 100,000, and the danger from household contact from an infected person is believed to be 200 to 1,000
times greater than that of the general population. Because of these statistics, anyone who has had contact with
the disease in a home, day-care centre, or nursery school should receive prophylactic antibiotic treatment as
soon as possible, preferably within 24 hours of the diagnosis of the primary case of the disease.
Group-specific meningococcal polysaccharide vaccines can be used to control outbreaks of disease and may
benefit travelers to countries where these diseases are endemic. Certain of the vaccines are administered
routinely to military recruits in the United States.
Hepatitis B vaccine
Hepatitis B virus (HBV) produces an illness characterized by jaundice, poor appetite, malaise, and nausea.
Chronic liver disease may follow the infection. Hepatitis B vaccine is recommended for infants and for persons
who are at a greater risk of contracting the disease because of their lifestyles or jobs. These include health care
personnel who are exposed to blood products, hemodialysis patients, institutionalized patients and their staffs,
patients receiving multiple transfusions, prostitutes and the sexual partners of individuals with the disease,
users of illicit intravenous drugs, and homosexual males.
Hepatitis B vaccine consists of recombinant viral surface antigen particles and is given in a three-dose series.
Britannica LaunchPacks | The Treatment and Prevention of Disease
20 of 123© 2020 Encyclopædia Britannica, Inc.
Influenza vaccine
Searching for a universal flu vaccine.
© American Chemical Society
The manufacture of influenza vaccine is complicated by the many influenza viruses and by the major changes in
antigenic composition that these viruses continually undergo. Routine immunization against influenza viruses is
recommended for all healthy individuals before the respiratory disease season commences (in the fall) and may
be recommended throughout the year for travelers to a different hemisphere (e.g., from North to South America,
because their winter seasons are reversed).
Haemophilus influenzae type B vaccine
The bacterium is a major cause of morbidity and mortality in children, particularly in Haemophilus influenzaethose under six years of age. Because it is highly contagious among people in close contact with one another,
antibiotics were traditionally used to prevent infection. In 1990 a powerful vaccine called a conjugate vaccine
was licensed, and it has caused a dramatic decrease in disease in many countries.H. influenzae
Chickenpox (varicella) vaccine
The low morbidity of chickenpox in healthy children does not arguably support the universal use of vaccine. In
certain persons, especially those with immunodeficiency disease or cancer, however, chickenpox can be
devastating. A live attenuated vaccine has been found to be safe and immunogenic in healthy children and has
recently been licensed, although its use has been questioned.
Passive immunity
Passive immunity is the administration of antibodies to an unimmunized person from an immune subject to
provide temporary protection against a microbial agent or toxin. This type of immunity can be conferred on
persons who are exposed to measles, mumps, whooping cough, poliomyelitis, rabies, rubella (German measles),
tetanus, chickenpox, and herpes zoster (shingles). The process is also used in the treatment of certain disorders
associated with bites (snake and spider) and as a specific (Rho-GAM) or nonspecific (antilymphocyte serum)
immunosuppressant. Other antibody preparations are available under specific conditions for specific disorders.
Passive immunization is not always effective; the duration of immunity provided is brief and variable, and
undesirable reactions may occur, especially if the antiserum is of nonhuman origin. Several preparations are
available for use as passive immunizing agents.
Britannica LaunchPacks | The Treatment and Prevention of Disease
21 of 123© 2020 Encyclopædia Britannica, Inc.
HISG
Human immune serum globulin (HISG) is prepared from human serum. Special treatment of the serum removes
various undesirable proteins and infectious viruses, thus providing a safe product for intramuscular injection.
HISG is used for the treatment of antibody deficiency conditions and for the prevention of hepatitis A and
hepatitis B viral infections, measles, chickenpox, rubella, and poliomyelitis.
The most widespread use of HISG is in the prevention of hepatitis A infection, a disease for which active
immunization has only recently become available, in individuals known to have had intimate exposure to the
disease. Hepatitis B immunoglobulin should be given immediately to susceptible persons who are exposed to
contaminated blood or who have had intimate physical contact with a person who has hepatitis B infection.
Because of the scarcity of the product, hepatitis B immune globulin is not recommended routinely for those who
are continuously at high risk of exposure to hepatitis B. It should be given, however, in conjunction with
vaccination, to infants born to mothers who have serological evidence of hepatitis B viral infection.
Several investigators have claimed a beneficial effect of HISG in persons with HIV infection and AIDS, as well as
in persons with asthma and other allergic disorders; evidence confirming its efficacy in these conditions is
lacking, however. Monthly HISG is not beneficial in the prevention of upper respiratory infections, otitis, skin
infections, gastrointestinal disorders, or fever of undetermined cause. HISG has been used inconclusively in the
treatment of infants with significantly low levels of immunoglobulins and patients with severe burns who are at
an increased risk of infection. Antivenoms derived from horses are used effectively to treat snake or spider bites,
but not without significant risk of reaction to the equine antibody preparation.
Rho-GAM
Rho-GAM is a human anti-RhD immune serum globulin used in the prevention of Rh hemolytic disease of the
newborn. Rho-GAM is given to Rh-negative mothers after the delivery of Rh-positive infants or after miscarriage
or abortion to prevent the development of anti-Rh antibodies, which could cause hemolysis (red blood cell
destruction) in the infant of a subsequent pregnancy.
Antitoxins
Botulism, a severe paralytic poisoning, results from the ingestion or absorption of the toxin of the bacterium
. As a preventive measure, antitoxin can be given to individuals known to have ingested Clostridium botulinumcontaminated food and to patients with symptoms as soon as possible after exposure.
Most of the damaging effect of diphtheria results from the toxin produced by the bacterium Corynebacterium . This toxin not only has local effects but also is distributed through the blood to the heart, nervous diphtheriae
system, kidneys, and other organs. Diphtheria antitoxin of animal origin remains the principal treatment, along
with antibiotics.
Gas gangrene is caused by infection with clostridial organisms, usually following a traumatic injury that has
caused extensive local tissue damage. An antitoxin derived from horses is available as an adjunct to surgical and
other treatment of these infections.
Ralph D. FeiginRenu GargAndrew Barnett Christie
Britannica LaunchPacks | The Treatment and Prevention of Disease
22 of 123© 2020 Encyclopædia Britannica, Inc.
Additional ReadingGeneral information
GERALD L. MANDELL, , and (eds.), JOHN E. BENNETT RAPHAEL DOLIN Mandell, Douglas, and Bennett’s Principles
, 7th ed. (2010), is a modern textbook that the general reader may find and Practice of Infectious Diseasesinformative and useful. and , , 4th ed. H.A.K. ROWLAND PHILIP D. WELSBY A Color Atlas of Infectious Diseases
(2003), reveals through the use of colour photographs the actual clinical features associated with various
infectious diseases. , LAURIE GARRETT The Coming Plague: Newly Emerging Diseases in a World out of
(1994), is a Pulitzer Prize-winning account that focuses on emerging infectious diseases. Balance RICHARD
(ed.), (1998, reissued 2000), is an excellent M. KRAUSE Emerging Infections: Biomedical Research Reports
collection of articles edited by the former director of the U.S. National Institute of Allergy and Infectious
Diseases. (ed.), , 4th ed. (2008), is a well-written text on a KING K. HOLMES Sexually Transmitted Diseases
facet of infectious disease that is assuming increasing importance in society. , PAUL W. EWALD Evolution of
(1993, reissued 1996), an accessible work, was the first to present a Darwinian Infectious Diseaseperspective on infectious disease.
History of infectious disease
ANDRÉ SIEGFRIED, (also published as Routes of Contagion Germs and Ideas: Routes of Epidemics and
, 1965; originally published in French, 1960); and , Ideologies HENRY E. SIGERIST Civilization and Disease
(1943, reissued 1970), deal with the effect of disease on human life and history; both are nontechnical.
, (1976, reissued 1998), is a modern classic that looks at the role of WILLIAM H. MCNEILL Plagues and Peoples
epidemics in human history from an interdisciplinary perspective. Two other excellent books on the
history of infectious disease are , CHARLES-EDWARD AMORY WINSLOW The Conquest of Epidemic Disease: A
(1943, reprinted 1980); and , (1935, Chapter in the History of Ideas H. ZINSSER Rats, Lice, and History
reissued 2000).
Citation (MLA style):
"Infectious disease." , Encyclopædia Britannica LaunchPacks: The Treatment and Prevention of DiseaseBritannica, 1 May. 2020. packs-ngl.eb.com. Accessed 6 Apr. 2022.
While every effort has been made to follow citation style rules, there may be some discrepancies. Please refer to the appropriate style manual or other sources if you have any questions.
genetic testingany of a group of procedures used to identify gene variations associated with health, disease, and ancestry and
to diagnose inherited diseases and disorders. A genetic test is typically issued only after a medical history, a
physical examination, and the construction of a family pedigree documenting the genetic diseases present in the
past three generations have been considered. The pedigree is especially important, since it aids in determining
whether a disease or disorder is inherited and likely to be passed on to subsequent generations. Genetic testing
is increasingly being used in genealogy, the study of family origins and history.
Genetic mutations

Britannica LaunchPacks | The Treatment and Prevention of Disease
23 of 123© 2020 Encyclopædia Britannica, Inc.
Genetic mutationsA genetic disorder can occur in a child with parents who are not affected by the disorder. This situation arises
when a gene mutation occurs in the egg or sperm (germinal mutation) or following conception, when
chromosomes from the egg and sperm combine. Mutations can occur spontaneously or be stimulated by
environmental factors, such as radiation or carcinogens (cancer-causing agents). Mutations occur with increasing
frequency as people age. In men this may result from errors that occur throughout a lifetime as DNA
(deoxyribonucleic acid) replicates to produce sperm. In women nondisjunction of chromosomes becomes more
common later in life, increasing the risk of aneuploidy (too many or too few chromosomes). Long-term exposure
to ambient ionizing radiation may cause genetic mutations in either gender. In addition to these exposure
mutations, there also exist two broad classes of genes that are prone to mutations that give rise to cancer.
These classes include oncogenes, which promote tumour growth, and tumour-suppressor genes, which suppress
tumour growth.
Types of diagnostic genetic testsChemical, radiological, histopathologic, and electrodiagnostic procedures can diagnose basic defects in patients
suspected of genetic disease. Genetic tests may involve cytogenetic analyses to investigate chromosomes,
molecular assays to investigate genes and DNA, or biochemical assays to investigate enzymes, hormones, or
amino acids. Tests such as amino acid chromatography of blood and urine, in which the amino acids present in
these fluids are separated on the basis of certain chemical affinities, can be used to identify specific hereditary
or acquired gene defects. There also exist numerous genetic tests for blood and blood typing and antibody
determination. These tests are used to isolate blood or antibody abnormalities that can be traced to genes
involved in the generation of these substances. Various electrodiagnostic procedures such as electromyography
are useful for identifying defects in muscle and nerve function, which often result from inherited gene mutations.
Prenatal diagnosis
Prenatal screening is performed if there is a family history of inherited disease, the mother is at an advanced
age, a previous child had a chromosomal abnormality, or there is an ethnic indication of risk. Parents can be
tested before or after conception to determine whether they are carriers.
A common prenatal test involves screening for alpha-fetoprotein (AFP) in maternal serum. Elevated levels of AFP
are associated with neural tube defects in the fetus, including spina bifida (defective closure of the spine) and
anencephaly (absence of brain tissue). When AFP levels are elevated, a more specific diagnosis is attempted,
using ultrasound and amniocentesis to analyze the amniotic fluid for the presence of AFP. Fetal cells contained in
the amniotic fluid also can be cultured and the karyotype (chromosome morphology) determined to identify
chromosomal abnormality. Cells for chromosome analysis also can be obtained by chorionic villus sampling, the
direct needle aspiration of cells from the chorionic villus (future placenta).
Women who have had repeated in vitro fertilization failures may undergo preimplantation genetic diagnosis
(PGD). PGD is used to detect the presence of embryonic genetic abnormalities that have a high likelihood of
causing implantation failure or miscarriage. In PGD a single cell is extracted from the embryo and is analyzed by
fluorescence in situ hybridization (FISH), a technique used to identify structural abnormalities in chromosomes
that standard tests such as karyotyping cannot detect. In some cases DNA is isolated from the cell and analyzed
by polymerase chain reaction (PCR) for the detection of gene mutations that can give rise to certain disorders
such as Tay-Sachs disease. Another technique, known as comparative genomic hybridization (CGH), may be
used alongside PGD to identify chromosomal abnormalities.
Britannica LaunchPacks | The Treatment and Prevention of Disease
24 of 123© 2020 Encyclopædia Britannica, Inc.
Advances in DNA sequencing technologies have enabled scientists to reconstruct the human fetal genome from
genetic material found in maternal blood and paternal saliva. This in turn has raised the possibility for
development of prenatal diagnostic tests that are noninvasive to the fetus but capable of accurately detecting
genetic defects in fetal DNA. Such tests are desirable because they would significantly reduce the risk of
miscarriage that is associated with procedures requiring cell sampling from the fetus or chorionic villus.
Karyotyping
Chromosomal karyotyping, in which chromosomes are arranged according to a standard classification scheme, is
one of the most commonly used genetic tests. To obtain a person’s karyotype, laboratory technicians grow
human cells in tissue culture media. After being stained and sorted, the chromosomes are counted and
displayed. The cells are obtained from the blood, skin, or bone marrow or by amniocentesis or chorionic villus
sampling, as noted above. The standard karyotype has approximately 400 visible bands, and each band contains
up to several hundred genes.
When a chromosomal aberration is identified, it allows for a more accurate prediction of the risk of its recurrence
in future offspring. Karyotyping can be used not only to diagnose aneuploidy, which is responsible for Down
syndrome, Turner syndrome, and Klinefelter syndrome, but also to identify the chromosomal aberrations
associated with solid tumours such as nephroblastoma, meningioma, neuroblastoma, retinoblastoma, renal-cell
carcinoma, small-cell lung cancer, and certain leukemias and lymphomas.
Karyotyping requires a great deal of time and effort and may not always provide conclusive information. It is
most useful in identifying very large defects involving hundreds or even thousands of genes.
DNA tests
Techniques such as FISH, CGH, and PCR have high rates of sensitivity and specificity. These procedures provide
results more quickly than traditional karyotyping because no cell culture is required. FISH can detect genetic
deletions involving one to five genes. It is also useful in detecting moderate-sized deletions, such as those
causing Prader-Willi syndrome. CGH is more sensitive than FISH and is capable of detecting a variety of small
chromosomal rearrangements, deletions, and duplications. The analysis of individual genes also has been
greatly enhanced by the development of PCR and recombinant DNA technology. In recombinant DNA
technology, small DNA fragments are isolated and copied, thereby producing unlimited amounts of cloned
material. Once cloned, the various genes and gene products can be used to study gene function both in healthy
individuals and those with disease. Recombinant DNA and PCR methods can detect any change in DNA, down to
a one-base-pair change, such as a point mutation or a single nucleotide polymorphism, out of the three billion
base pairs in the human genome. The detection of these changes is facilitated by DNA probes that are labeled
with radioactive isotopes or fluorescent dyes. Such methods can be used to identify persons who are carriers for
inherited conditions, such as hemophilia A, polycystic kidney disease, sickle cell anemia, Huntington disease,
cystic fibrosis, and hemochromatosis.
Biochemical tests
Biochemical tests primarily detect enzymatic defects such as phenylketonuria, porphyria, and glycogen-storage
disease. Although testing of newborns for all these abnormalities is possible, it is not cost-effective, because
some of these conditions are quite rare. Screening requirements for these disorders vary and depend on
whether the disease is sufficiently common, has severe consequences, and can be treated or prevented if
diagnosed early and whether the test can be applied to the entire population at risk.
Genetic testing and genealogy

Britannica LaunchPacks | The Treatment and Prevention of Disease
25 of 123© 2020 Encyclopædia Britannica, Inc.
Genetic testing and genealogyOnce the domain of oral traditions and written pedigrees, genealogy in the modern era has become grounded in
the science of genetics. Increased rigour in the field has been made possible by the development and ongoing
refinement of methods to accurately trace genes and genetic variations through generations. Genetic tests used
in genealogy are mainly intended to identify similarities and differences in DNA between living humans and their
ancestors. In some instances, however, in the process of tracing genetic lineages, gene variations associated
with disease may be detected.
Methods used in genealogical genetics analysis include Y chromosome testing, mitochondrial DNA (mtDNA)
testing, and detection of ancestry-associated genetic variants that occur as single nucleotide polymorphisms
(SNPs) in the human genome. Y chromosome testing is based on genetic comparison of Y chromosomes, from
males. Because males with a common male ancestor have matching Y chromosomes, scientists are able to trace
paternal lineages and thereby determine distant relationships between males. Such analyses allow genealogists
to confirm whether males with the same surname are related. Likewise, maternal lineages can be traced
genetically through mtDNA testing, since the mitochondrial genome is inherited only from the mother. Maternal
lineage tests typically involve analysis of a segment in mtDNA known as hypervariable region 1; comparison of
this segment against reference mtDNA sequences (e.g., Cambridge Reference Sequence) enables scientists to
reconstruct an individual’s maternal genetic lineage.
Following the completion of the Human Genome Project in 2003, it became possible to more efficiently scan the
human genome for SNPs and to compare SNPs occurring in the genomes of human populations in different
geographical regions of the world. The analysis of this information for genetic testing and genealogical purposes
forms the basis of biogeographical ancestry testing. These tests typically make use of panels of ancestry
informative markers (AIMs), which are SNPs specific to human populations and their geographical areas that can
be used to infer ancestry. In 2010 a study using genome-wide SNP analysis incorporating ancestral information
successfully traced persons in Europe to the villages in which their grandparents lived. The technique was
expected to advance genetic testing intended to map an individual’s geographical ancestry.
Citation (MLA style):
"Genetic testing." , Encyclopædia Britannica, 8 Britannica LaunchPacks: The Treatment and Prevention of DiseaseJun. 2012. packs-ngl.eb.com. Accessed 6 Apr. 2022.
While every effort has been made to follow citation style rules, there may be some discrepancies. Please refer to the appropriate style manual or other sources if you have any questions.
medicinethe practice concerned with the maintenance of health and the prevention, alleviation, or cure of disease.

Britannica LaunchPacks | The Treatment and Prevention of Disease
26 of 123© 2020 Encyclopædia Britannica, Inc.
Surgeons performing a laparoscopy.
© s4svisuals/Shutterstock.com
The World Health Organization at its 1978 international conference held in the Soviet Union produced the Alma-
Ata Health Declaration, which was designed to serve governments as a basis for planning health care that would
reach people at all levels of society. The declaration reaffirmed that
health, which is a state of complete physical, mental and social well-being, and not merely the absence of
disease or infirmity, is a fundamental human right and that the attainment of the highest possible level of health
is a most important world-wide social goal whose realization requires the action of many other social and
economic sectors in addition to the health sector.
In its widest form, the practice of medicine—that is to say, the promotion and care of health—is concerned with
this ideal.
Organization of health servicesIt is generally the goal of most countries to have their health services organized in such a way to ensure that
individuals, families, and communities obtain the maximum benefit from current knowledge and technology
available for the promotion, maintenance, and restoration of health. In order to play their part in this process,
governments and other agencies are faced with numerous tasks, including the following: (1) They must obtain as
much information as is possible on the size, extent, and urgency of their needs; without accurate information,
planning can be misdirected. (2) These needs must then be revised against the resources likely to be available
in terms of money, manpower, and materials; developing countries may well require external aid to supplement
their own resources. (3) Based on their assessments, countries then need to determine realistic objectives and
draw up plans. (4) Finally, a process of evaluation needs to be built into the program; the lack of reliable
information and accurate assessment can lead to confusion, waste, and inefficiency.
Health services of any nature reflect a number of interrelated characteristics, among which the most obvious,
but not necessarily the most important from a national point of view, is the curative function; that is to say,
caring for those already ill. Others include special services that deal with particular groups (such as children or
pregnant women) and with specific needs such as nutrition or immunization; preventive services, the protection
of the health both of individuals and of communities; health education; and, as mentioned above, the collection
and analysis of information.
Levels of health care
In the curative domain there are various forms of medical practice. They may be thought of generally as forming
a pyramidal structure, with three tiers representing increasing degrees of specialization and technical

Britannica LaunchPacks | The Treatment and Prevention of Disease
27 of 123© 2020 Encyclopædia Britannica, Inc.
sophistication but catering to diminishing numbers of patients as they are filtered out of the system at a lower
level. Only those patients who require special attention either for diagnosis or treatment should reach the
second (advisory) or third (specialized treatment) tiers where the cost per item of service becomes increasingly
higher. The first level represents primary health care, or first contact care, at which patients have their initial
contact with the health-care system.
Primary health care is an integral part of a country’s health maintenance system, of which it forms the largest
and most important part. As described in the declaration of Alma-Ata, primary health care should be “based on
practical, scientifically sound and socially acceptable methods and technology made universally accessible to
individuals and families in the community through their full participation and at a cost that the community and
country can afford to maintain at every stage of their development.” Primary health care in the developed
countries is usually the province of a medically qualified physician; in the developing countries first contact care
is often provided by nonmedically qualified personnel.
The vast majority of patients can be fully dealt with at the primary level. Those who cannot are referred to the
second tier (secondary health care, or the referral services) for the opinion of a consultant with specialized
knowledge or for X-ray examinations and special tests. Secondary health care often requires the technology
offered by a local or regional hospital. Increasingly, however, the radiological and laboratory services provided
by hospitals are available directly to the family doctor, thus improving his service to patients and increasing its
range. The third tier of health care, employing specialist services, is offered by institutions such as teaching
hospitals and units devoted to the care of particular groups—women, children, patients with mental disorders,
and so on. The dramatic differences in the cost of treatment at the various levels is a matter of particular
importance in developing countries, where the cost of treatment for patients at the primary health-care level is
usually only a small fraction of that at the third level; medical costs at any level in such countries, however, are
usually borne by the government.
Ideally, provision of health care at all levels will be available to all patients; such health care may be said to be
universal. The well-off, both in relatively wealthy industrialized countries and in the poorer developing world,
may be able to get medical attention from sources they prefer and can pay for in the private sector. The vast
majority of people in most countries, however, are dependent in various ways upon health services provided by
the state, to which they may contribute comparatively little or, in the case of poor countries, nothing at all.
Costs of health care
The costs to national economics of providing health care are considerable and have been growing at a rapidly
increasing rate, especially in countries such as the United States, Germany, and Sweden; the rise in Britain has
been less rapid. This trend has been the cause of major concerns in both developed and developing countries.
Some of this concern is based upon the lack of any consistent evidence to show that more spending on health
care produces better health. There is a movement in developing countries to replace the type of organization of
health-care services that evolved during European colonial times with some less expensive, and for them, more
appropriate, health-care system.
In the industrialized world the growing cost of health services has caused both private and public health-care
delivery systems to question current policies and to seek more economical methods of achieving their goals.
Despite expenditures, health services are not always used effectively by those who need them, and results can
vary widely from community to community. In Britain, for example, between 1951 and 1971 the death rate fell
by 24 percent in the wealthier sections of the population but by only half that in the most underprivileged
Britannica LaunchPacks | The Treatment and Prevention of Disease
28 of 123© 2020 Encyclopædia Britannica, Inc.
sections of society. The achievement of good health is reliant upon more than just the quality of health care.
Health entails such factors as good education, safe working conditions, a favourable environment, amenities in
the home, well-integrated social services, and reasonable standards of living.
In the developing countries
The developing countries differ from one another culturally, socially, and economically, but what they have in
common is a low average income per person, with large percentages of their populations living at or below the
poverty level. Although most have a small elite class, living mainly in the cities, the largest part of their
populations live in rural areas. Urban regions in developing and some developed countries in the mid- and late
20th century developed pockets of slums, which were growing because of an influx of rural peoples and
immigrants. Slums persisted into the 21st century, though newer, cheaper construction techniques greatly
facilitated the development of affordable housing, alleviating some housing problems in densely populated
places such as New York City and cities in India. Nonetheless, many urban areas are simply overcrowded, which
is problematic for maintaining public health. For lack of even the simplest measures, vast numbers of urban and
rural poor die each year of preventable and curable diseases, often associated with poor hygiene and sanitation,
impure water supplies, malnutrition, vitamin deficiencies, and chronic preventable infections. The effect of these
and other deprivations is reflected by the finding that in the 1980s the life expectancy at birth for men and
women was about one-third less in Africa than it was in Europe; similarly, infant mortality in Africa was about
eight times greater than in Europe. The extension of primary health-care services is therefore a high priority in
the developing countries.
The developing countries themselves, lacking the proper resources, have often been unable to generate or
implement the plans necessary to provide required services at the village or urban poor level. It has, however,
become clear that the system of health care that is appropriate for one country is often unsuitable for another.
Research has established that effective health care is related to the special circumstances of the individual
country, its people, culture, ideology, and economic and natural resources.
The rising costs of providing health care have influenced a trend, especially among the developing nations, to
promote services that employ less highly trained primary health-care personnel who can be distributed more
widely in order to reach the largest possible proportion of the community. The principal medical problems to be
dealt with in the developing world include undernutrition, infection, gastrointestinal disorders, and respiratory
complaints, which themselves may be the result of poverty, ignorance, and poor hygiene. For the most part,
these are easy to identify and to treat. Furthermore, preventive measures are usually simple and cheap. Neither
treatment nor prevention requires extensive professional training: in most cases they can be dealt with
adequately by the “primary health worker,” a term that includes all nonprofessional health personnel.
In the developed countries
Those concerned with providing health care in the developed countries face a different set of problems. The
diseases so prevalent in the Third World have, for the most part, been eliminated or are readily treatable. Many
of the adverse environmental conditions and public health hazards have been conquered. Social services of
varying degrees of adequacy have been provided. Public funds can be called upon to support the cost of medical
care, and there are a variety of private insurance plans available to the consumer. Nevertheless, the funds that a
government can devote to health care are limited and the cost of modern medicine continues to increase, thus
putting adequate medical services beyond the reach of many. Adding to the expense of modern medical
practices is the increasing demand for greater funding of health education and preventive measures specifically
directed toward the poor.
Harold Scarborough

Britannica LaunchPacks | The Treatment and Prevention of Disease
29 of 123© 2020 Encyclopædia Britannica, Inc.
Administration of primary health care
A health care worker in surgical scrubs.
Creatas/Getty Images Plus
In many parts of the world, particularly in developing countries, people get their primary health care, or first-
contact care, where available at all, from nonmedically qualified personnel; these cadres of medical auxiliaries
are being trained in increasing numbers to meet overwhelming needs among rapidly growing populations. Even
among the comparatively wealthy countries of the world, containing in all a much smaller percentage of the
world’s population, escalation in the costs of health services and in the cost of training a physician has
precipitated some movement toward reappraisal of the role of the medical doctor in the delivery of first-contact
care.
In advanced industrial countries, however, it is usually a trained physician who is called upon to provide the first-
contact care. The patient seeking first-contact care can go either to a general practitioner or turn directly to a
specialist. Which is the wisest choice has become a subject of some controversy. The general practitioner,
however, is becoming rather rare in some developed countries. In countries where he does still exist, he is being
increasingly observed as an obsolescent figure, because medicine covers an immense, rapidly changing, and
complex field of which no physician can possibly master more than a small fraction. The very concept of the
general practitioner, it is thus argued, may be absurd.
The obvious alternative to general practice is the direct access of a patient to a specialist. If a patient has
problems with vision, he goes to an eye specialist, and if he has a pain in his chest (which he fears is due to his
heart), he goes to a heart specialist. One objection to this plan is that the patient often cannot know which organ
is responsible for his symptoms, and the most careful physician, after doing many investigations, may remain
uncertain as to the cause. Breathlessness—a common symptom—may be due to heart disease, to lung disease,
to anemia, or to emotional upset. Another common symptom is general malaise—feeling run-down or always
tired; others are headache, chronic low backache, rheumatism, abdominal discomfort, poor appetite, and
constipation. Some patients may also be overtly anxious or depressed. Among the most subtle medical skills is
the ability to assess people with such symptoms and to distinguish between symptoms that are caused
predominantly by emotional upset and those that are predominantly of bodily origin. A specialist may be capable
of such a general assessment, but, often, with emphasis on his own subject, he fails at this point. The generalist
with his broader training is often the better choice for a first diagnosis, with referral to a specialist as the next
option.
It is often felt that there are also practical advantages for the patient in having his own doctor, who knows about
his background, who has seen him through various illnesses, and who has often looked after his family as well.

Britannica LaunchPacks | The Treatment and Prevention of Disease
30 of 123© 2020 Encyclopædia Britannica, Inc.
This personal physician, often a generalist, is in the best position to decide when the patient should be referred
to a consultant.
The advantages of general practice and specialization are combined when the physician of first contact is a
pediatrician. Although he sees only children and thus acquires a special knowledge of childhood maladies, he
remains a generalist who looks at the whole patient. Another combination of general practice and specialization
is represented by group practice, the members of which partially or fully specialize. One or more may be general
practitioners, and one may be a surgeon, a second an obstetrician, a third a pediatrician, and a fourth an
internist. In isolated communities group practice may be a satisfactory compromise, but in urban regions, where
nearly everyone can be sent quickly to a hospital, the specialist surgeon working in a fully equipped hospital can
usually provide better treatment than a general practitioner surgeon in a small clinic hospital.
Medical practice in developed countriesBritain
Before 1948, general practitioners in Britain settled where they could make a living. Patients fell into two main
groups: weekly wage earners, who were compulsorily insured, were on a doctor’s “panel” and were given free
medical attention (for which the doctor was paid quarterly by the government); most of the remainder paid the
doctor a fee for service at the time of the illness. In 1948 the National Health Service began operation. Under its
provisions, everyone is entitled to free medical attention with a general practitioner with whom he is registered.
Though general practitioners in the National Health Service are not debarred from also having private patients,
these must be people who are not registered with them under the National Health Service. Any physician is free
to work as a general practitioner entirely independent of the National Health Service, though there are few who
do so. Almost the entire population is registered with a National Health Service general practitioner, and the vast
majority automatically sees this physician, or one of his partners, when they require medical attention. A few
people, mostly wealthy, while registered with a National Health Service general practitioner, regularly see
another physician privately; and a few may occasionally seek a private consultation because they are
dissatisfied with their National Health Service physician.
A general practitioner under the National Health Service remains an independent contractor, paid by a capitation
fee; that is, according to the number of people registered with him. He may work entirely from his own office,
and he provides and pays his own receptionist, secretary, and other ancillary staff. Most general practitioners
have one or more partners and work more and more in premises built for the purpose. Some of these structures
are erected by the physicians themselves, but many are provided by the local authority, the physicians paying
rent for using them. Health centres, in which groups of general practitioners work have become common.
In Britain only a small minority of general practitioners can admit patients to a hospital and look after them
personally. Most of this minority are in country districts, where, before the days of the National Health Service,
there were cottage hospitals run by general practitioners; many of these hospitals continued to function in a
similar manner. All general practitioners use such hospital facilities as X-ray departments and laboratories, and
many general practitioners work in hospitals in emergency rooms (casualty departments) or as clinical assistants
to consultants, or specialists.
General practitioners are spread more evenly over the country than formerly, when there were many in the
richer areas and few in the industrial towns. The maximum allowed list of National Health Service patients per
doctor is 3,500; the average is about 2,500. Patients have free choice of the physician with whom they register,
Britannica LaunchPacks | The Treatment and Prevention of Disease
31 of 123© 2020 Encyclopædia Britannica, Inc.
with the proviso that they cannot be accepted by one who already has a full list and that a physician can refuse
to accept them (though such refusals are rare). In remote rural places there may be only one physician within a
reasonable distance.
Until the mid-20th century it was not unusual for the doctor in Britain to visit patients in their own homes. A
general practitioner might make 15 or 20 such house calls in a day, as well as seeing patients in the office or
“surgery,” often in the evenings. This enabled him to become a family doctor in fact as well as in name. In
modern practice, however, a home visit is quite exceptional and is paid only to the severely disabled or seriously
ill when other recourses are ruled out. All patients are normally required to go to the doctor.
It has also become unusual for a personal doctor to be available during weekends or holidays. His place may be
taken by one of his partners in a group practice, a provision that is reasonably satisfactory. General
practitioners, however, may now use one of several commercial deputizing services that employs young doctors
to be on call. Although some of these young doctors may be well experienced, patients do not generally
appreciate this kind of arrangement.
John Walford ToddHarold Scarborough
United States
Whereas in Britain the doctor of first contact is regularly a general practitioner, in the United States the nature of
first-contact care is less consistent. General practice in the United States was in a state of decline in the second
half of the 20th century, especially in metropolitan areas. Increasingly, the general practitioner was replaced by
the growing field of family practice. In 1969 family practice was recognized as a medical specialty after the
American Academy of General Practice (later the American Academy of Family Physicians) and the American
Medical Association created the American Board of General Practice (later American Board of Family Medicine).
Since that time the field has become one of the larger medical specialties in the United States. The family
physicians were the first group of medical specialists in the United States for whom recertification was required.
There is no national health service, as such, in the United States. Most physicians in the country have
traditionally been in some form of private practice, whether seeing patients in their own offices, clinics, medical
centres, or another type of facility and regardless of the patients’ income. Doctors are usually compensated by
such state and federally supported agencies as Medicaid (for treating the poor) and Medicare (for treating the
elderly); not all doctors, however, accept poor patients. There are also some state-supported clinics and
hospitals where the poor and elderly may receive free or low-cost treatment, and some doctors devote a small
percentage of their time to treatment of the indigent. Veterans may receive free treatment at Veterans
Administration hospitals, and the federal government through its Indian Health Service provides medical services
to American Indians and Alaskan natives, sometimes using trained auxiliaries for first-contact care.
In the rural United States first-contact care is likely to come from a generalist. The middle- and upper-income
groups living in urban areas, however, have access to a larger number of primary medical care options. Children
are often taken to pediatricians, who may oversee the child’s health needs until adulthood. Adults frequently
make their initial contact with an internist, whose field is mainly that of medical (as opposed to surgical)
illnesses; the internist often becomes the family physician. Other adults choose to go directly to physicians with
narrower specialties, including dermatologists, allergists, gynecologists, orthopedists, and ophthalmologists.
Patients in the United States may also choose to be treated by doctors of osteopathy. These doctors are fully
qualified, but they make up only a small percentage of the country’s physicians. They may also branch off into
specialties, but general practice is much more common in their group than among M.D.’s.

Britannica LaunchPacks | The Treatment and Prevention of Disease
32 of 123© 2020 Encyclopædia Britannica, Inc.
It used to be more common in the United States for physicians providing primary care to work independently,
providing their own equipment and paying their own ancillary staff. In smaller cities they mostly had full hospital
privileges, but in larger cities these privileges were more likely to be restricted. Physicians, often sharing the
same specialties, are increasingly entering into group associations, where the expenses of office space, staff,
and equipment may be shared; such associations may work out of suites of offices, clinics, or medical centres.
The increasing competition and risks of private practice have caused many physicians to join Health
Maintenance Organizations (HMOs), which provide comprehensive medical care and hospital care on a prepaid
basis. The cost savings to patients are considerable, but they must use only the HMO doctors and facilities.
HMOs stress preventive medicine and out-patient treatment as opposed to hospitalization as a means of
reducing costs, a policy that has caused an increased number of empty hospital beds in the United States.
While the number of doctors per 100,000 population in the United States has been steadily increasing, there has
been a trend among physicians toward the use of trained medical personnel to handle some of the basic
services normally performed by the doctor. So-called physician extender services are commonly divided into
nurse practitioners and physician’s assistants, both of whom provide similar ancillary services for the general
practitioner or specialist. Such personnel do not replace the doctor. Almost all American physicians have
systems for taking each other’s calls when they become unavailable. House calls in the United States, as in
Britain, have become exceedingly rare.
EB Editors
Russia
In Russia general practitioners are prevalent in the thinly populated rural areas. Pediatricians deal with children
up to about age 15. Internists look after the medical ills of adults, and occupational physicians deal with the
workers, sharing care with internists.
Teams of physicians with experience in varying specialties work from polyclinics or outpatient units, where many
types of diseases are treated. Small towns usually have one polyclinic to serve all purposes. Large cities
commonly have separate polyclinics for children and adults, as well as clinics with specializations such as
women’s health care, mental illnesses, and sexually transmitted diseases. Polyclinics usually have X-ray
apparatus and facilities for examination of tissue specimens, facilities associated with the departments of the
district hospital. Beginning in the late 1970s was a trend toward the development of more large, multipurpose
treatment centres, first-aid hospitals, and specialized medicine and health care centres.
Home visits have traditionally been common, and much of the physician’s time is spent in performing routine
checkups for preventive purposes. Some patients in sparsely populated rural areas may be seen first by
feldshers (auxiliary health workers), nurses, or midwives who work under the supervision of a polyclinic or
hospital physician. The feldsher was once a lower-grade physician in the army or peasant communities, but
feldshers are now regarded as paramedical workers.
Japan
In Japan, with less rigid legal restriction of the sale of pharmaceuticals than in the West, there was formerly a
strong tradition of self-medication and self-treatment. This was modified in 1961 by the institution of health
insurance programs that covered a large proportion of the population; there was then a great increase in visits
to the outpatient clinics of hospitals and to private clinics and individual physicians.
When Japan shifted from traditional Chinese medicine with the adoption of Western medical practices in the
1870s, Germany became the chief model. As a result of German influence and of their own traditions, Japanese
Britannica LaunchPacks | The Treatment and Prevention of Disease
33 of 123© 2020 Encyclopædia Britannica, Inc.
physicians tended to prefer professorial status and scholarly research opportunities at the universities or
positions in the national or prefectural hospitals to private practice. There were some pioneering physicians,
however, who brought medical care to the ordinary people.
Physicians in Japan have tended to cluster in the urban areas. The Medical Service Law of 1963 was amended to
empower the Ministry of Health and Welfare to control the planning and distribution of future public and
nonprofit medical facilities, partly to redress the urban-rural imbalance. Meanwhile, mobile services were
expanded.
The influx of patients into hospitals and private clinics after the passage of the national health insurance acts of
1961 had, as one effect, a severe reduction in the amount of time available for any one patient. Perhaps in
reaction to this situation, there has been a modest resurgence in the popularity of traditional Chinese medicine,
with its leisurely interview, its dependence on herbal and other “natural” medicines, and its other traditional
diagnostic and therapeutic practices. The rapid aging of the Japanese population as a result of the sharply
decreasing death rate and birth rate has created an urgent need for expanded health care services for the
elderly. There has also been an increasing need for centres to treat health problems resulting from
environmental causes.
Other developed countries
On the continent of Europe there are great differences both within single countries and between countries in the
kinds of first-contact medical care. General practice, while declining in Europe as elsewhere, is still rather
common even in some large cities, as well as in remote country areas.
In The Netherlands, departments of general practice are administered by general practitioners in all the medical
schools—an exceptional state of affairs—and general practice flourishes. In the larger cities of Denmark, general
practice on an individual basis is usual and popular, because the physician works only during office hours. In
addition, there is a duty doctor service for nights and weekends. In the cities of Sweden, primary care is given by
specialists. In the remote regions of northern Sweden, district doctors act as general practitioners to patients
spread over huge areas; the district doctors delegate much of their home visiting to nurses.
In France there are still general practitioners, but their number is declining. Many medical practitioners advertise
themselves directly to the public as specialists in internal medicine, ophthalmologists, gynecologists, and other
kinds of specialists. Even when patients have a general practitioner, they may still go directly to a specialist.
Attempts to stem the decline in general practice are being made by the development of group practice and of
small rural hospitals equipped to deal with less serious illnesses, where general practitioners can look after their
patients.
Although Israel has a high ratio of physicians to population, there is a shortage of general practitioners, and only
in rural areas is general practice common. In the towns many people go directly to pediatricians, gynecologists,
and other specialists, but there has been a reaction against this direct access to the specialist. More general
practitioners have been trained, and the Israel Medical Association has recommended that no patient should be
referred to a specialist except by the family physician or on instructions given by the family nurse. At Tel Aviv
University there is a department of family medicine. In some newly developing areas, where the doctor shortage
is greatest, there are medical centres at which all patients are initially interviewed by a nurse. The nurse may
deal with many minor ailments, thus freeing the physician to treat the more seriously ill.

Britannica LaunchPacks | The Treatment and Prevention of Disease
34 of 123© 2020 Encyclopædia Britannica, Inc.
Nearly half the medical doctors in Australia are general practitioners—a far higher proportion than in most other
advanced countries—though, as elsewhere, their numbers are declining. They tend to do far more for their
patients than in Britain, many performing such operations as removal of the appendix, gallbladder, or uterus,
operations that elsewhere would be carried out by a specialist surgeon. Group practices are common.
Medical practice in developing countriesChina
Health services in China since the Cultural Revolution have been characterized by decentralization and
dependence on personnel chosen locally and trained for short periods. Emphasis is given to selfless motivation,
self-reliance, and to the involvement of everyone in the community. Campaigns stressing the importance of
preventive measures and their implementation have served to create new social attitudes as well as to break
down divisions between different categories of health workers. Health care is regarded as a local matter that
should not require the intervention of any higher authority; it is based upon a highly organized and well-
disciplined system that is egalitarian rather than hierarchical, as in Western societies, and which is well suited to
the rural areas where about two-thirds of the population live. In the large and crowded cities an important
constituent of the health-care system is the residents’ committees, each for a population of 1,000 to 5,000
people. Care is provided by part-time personnel with periodic visits by a doctor. A number of residents’
committees are grouped together into neighbourhoods of some 50,000 people where there are clinics and
general hospitals staffed by doctors as well as health auxiliaries trained in both traditional and Westernized
medicine. Specialized care is provided at the district level (over 100,000 people), in district hospitals and in
epidemic and preventive medicine centres. In many rural districts people’s communes have organized
cooperative medical services that provide primary care for a small annual fee.
Throughout China the value of traditional medicine is stressed, especially in the rural areas. All medical schools
are encouraged to teach traditional medicine as part of their curriculum, and efforts are made to link colleges of
Chinese medicine with Western-type medical schools. Medical education is of shorter duration than it is in
Europe, and there is greater emphasis on practical work. Students spend part of their time away from the
medical school working in factories or in communes; they are encouraged to question what they are taught and
to participate in the educational process at all stages. One well-known form of traditional medicine is
acupuncture, which is used as a therapeutic and pain-relieving technique; requiring the insertion of brass-
handled needles at various points on the body, acupuncture has become quite prominent as a form of
anesthesia.
The vast number of nonmedically qualified health staff, upon whom the health-care system greatly depends,
includes both full-time and part-time workers. The latter include so-called barefoot doctors, who work mainly in
rural areas, worker doctors in factories, and medical workers in residential communities. None of these groups is
medically qualified. They have had only a three-month period of formal training, part of which is done in a
hospital, fairly evenly divided between theoretical and practical work. This is followed by a varying period of on-
the-job experience under supervision.
India
Āyurvedic medicine is an example of a well-organized system of traditional health care, both preventive and
curative, that is widely practiced in parts of Asia. Āyurvedic medicine has a long tradition behind it, having
originated in India perhaps as long as 3,000 years ago. It is still a favoured form of health care in large parts of
the Eastern world, especially in India, where a large percentage of the population use this system exclusively or

Britannica LaunchPacks | The Treatment and Prevention of Disease
35 of 123© 2020 Encyclopædia Britannica, Inc.
combined with modern medicine. The Indian Medical Council was set up in 1971 by the Indian government to
establish maintenance of standards for undergraduate and postgraduate education. It establishes suitable
qualifications in Indian medicine and recognizes various forms of traditional practice including Āyurvedic, Unani,
and Siddha. Projects have been undertaken to integrate the indigenous Indian and Western forms of medicine.
Most Āyurvedic practitioners work in rural areas, providing health care to at least 500,000,000 people in India
alone. They therefore represent a major force for primary health care, and their training and deployment are
important to the government of India.
Like scientific medicine, Āyurvedic medicine has both preventive and curative aspects. The preventive
component emphasizes the need for a strict code of personal and social hygiene, the details of which depend
upon individual, climatic, and environmental needs. Bodily exercises, the use of herbal preparations, and Yoga
form a part of the remedial measures. The curative aspects of Āyurvedic medicine involves the use of herbal
medicines, external preparations, physiotherapy, and diet. It is a principle of Āyurvedic medicine that the
preventive and therapeutic measures be adapted to the personal requirements of each patient.
Other developing countries
A main goal of the World Health Organization (WHO), as expressed in the Alma-Ata Declaration of 1978, is to
provide to all the citizens of the world a level of health that will allow them to lead socially and economically
productive lives by the year 2000. By the late 1980s, however, vast disparities in health care still existed
between the rich and poor countries of the world. In developing countries such as Ethiopia, Guinea, Mali, and
Mozambique, for instance, governments in the late 1980s spent less than $5 per person per year on public
health, while in most western European countries several hundred dollars per year was spent on each person.
The disproportion of the number of physicians available between developing and developed countries is similarly
wide.
Along with the shortage of physicians, there is a shortage of everything else needed to provide medical care—of
equipment, drugs, and suitable buildings, and of nurses, technicians, and all other grades of staff, whose
presence is taken for granted in the affluent societies. Yet there are greater percentages of sick in the poor
countries than in the rich countries. In the poor countries a high proportion of people are young, and all are
liable to many infections, including tuberculosis, syphilis, typhoid, and cholera (which, with the possible
exception of syphilis, are now rare in the rich countries), and also malaria, yaws, worm infestations, and many
other conditions occurring primarily in the warmer climates. Nearly all of these infections respond to the
antibiotics and other drugs that have been discovered since the 1920s. There is also much malnutrition and
anemia, which can be cured if funding is available. There is a prevalence of disorders remediable by surgery.
Preventive medicine can ensure clean water supplies, destroy insects that carry infections, teach hygiene, and
show how to make the best use of resources.
In most poor countries there are a few people, usually living in the cities, who can afford to pay for medical care,
and in a free market system the physicians tend to go where they can make the best living; this situation causes
the doctor–patient ratio to be much higher in the towns than in country districts. A physician in Bombay or in Rio
de Janeiro, for example, may have equipment as lavish as that of a physician in the United States and can earn
an excellent income. The poor, however, both in the cities and in the country, can get medical attention only if it
is paid for by the state, by some supranational body, or by a mission or other charitable organization. Moreover,
the quality of the care they receive is often poor, and in remote regions it may be lacking altogether. In practice,
hospitals run by a mission may cooperate closely with state-run health centres.
Because physicians are scarce, their skills must be used to best advantage, and much of the work normally done
by physicians in the rich countries has to be delegated to auxiliaries or nurses, who have to diagnose the
Britannica LaunchPacks | The Treatment and Prevention of Disease
36 of 123© 2020 Encyclopædia Britannica, Inc.
common conditions, give treatment, take blood samples, help with operations, supply simple posters containing
health advice, and carry out other tasks. In such places the doctor has time only to perform major operations
and deal with the more difficult medical problems. People are treated as far as possible on an outpatient basis
from health centres housed in simple buildings; few can travel except on foot, and, if they are more than a few
miles from a health centre, they tend not to go there. Health centres also may be used for health education.
Although primary health-care service differs from country to country, that developed in Tanzania is
representative of many that have been devised in largely rural developing countries. The most important feature
of the Tanzanian rural health service is the rural health centre, which, with its related dispensaries, is intended
to provide comprehensive health services for the community. The staff is headed by the assistant medical officer
and the medical assistant. The assistant medical officer has at least four years of experience, which is then
followed by further training for 18 months. He is not a doctor but serves to bridge the gap between medical
assistant and physician. The medical assistant has three years of general medical education. The work of the
rural health centres and dispensaries is mainly of three kinds: diagnosis and treatment, maternal and child
health, and environmental health. The main categories of primary health workers also include medical aids,
maternal and child health aids, and health auxiliaries. Nurses and midwives form another category of worker. In
the villages there are village health posts staffed by village medical helpers working under supervision from the
rural health centre.
In some primitive elements of the societies of developing countries, and of some developed countries, there
exists the belief that illness comes from the displeasure of ancestral gods and evil spirits, from the malign
influence of evilly disposed persons, or from natural phenomena that can neither be forecast nor controlled. To
deal with such causes there are many varieties of indigenous healers who practice elaborate rituals on behalf of
both the physically ill and the mentally afflicted. If it is understood that such beliefs, and other forms of
shamanism, may provide a basis upon which health care can be based, then primary health care may be said to
exist almost everywhere. It is not only easily available but also readily acceptable, and often preferred, to more
rational methods of diagnosis and treatment. Although such methods may sometimes be harmful, they may
often be effective, especially where the cause is psychosomatic. Other patients, however, may suffer from a
disease for which there is a cure in modern medicine.
In order to improve the coverage of primary health-care services and to spread more widely some of the benefits
of Western medicine, attempts have sometimes been made to find a means of cooperation, or even integration,
between traditional and modern medicine (see above Medical practice in developing countries: India). In Africa,
for example, some such attempts are officially sponsored by ministries of health, state governments,
universities, and the like, and they have the approval of WHO, which often takes the lead in this activity. In view,
however, of the historical relationships between these two systems of medicine, their different basic concepts,
and the fact that their methods cannot readily be combined, successful merging has been limited.
Alternative or complementary medicinePersons dissatisfied with the methods of modern medicine or with its results sometimes seek help from those
professing expertise in other, less conventional, and sometimes controversial, forms of health care. Such
practitioners are not medically qualified unless they are combining such treatments with a regular (allopathic)
practice, which includes osteopathy. In many countries the use of some forms, such as chiropractic, requires
licensing and a degree from an approved college. The treatments afforded in these various practices are not
always subjected to objective assessment, yet they provide services that are alternative, and sometimes
complementary, to conventional practice. This group includes practitioners of homeopathy, naturopathy,
acupuncture, hypnotism, and various meditative and quasi-religious forms. Numerous persons also seek out

Britannica LaunchPacks | The Treatment and Prevention of Disease
37 of 123© 2020 Encyclopædia Britannica, Inc.
some form of faith healing to cure their ills, sometimes as a means of last resort. Religions commonly include
some advents of miraculous curing within their scriptures. The belief in such curative powers has been in part
responsible for the increasing popularity of the television, or “electronic,” preacher in the United States, a
phenomenon that involves millions of viewers. Millions of others annually visit religious shrines, such as the one
at Lourdes in France, with the hope of being miraculously healed.
Special practices and fields of medicineSpecialties in medicine
At the beginning of World War II it was possible to recognize a number of major medical specialties, including
internal medicine, obstetrics and gynecology, pediatrics, pathology, anesthesiology, ophthalmology, surgery,
orthopedic surgery, plastic surgery, psychiatry and neurology, radiology, and urology. Hematology was also an
important field of study, and microbiology and biochemistry were important medically allied specialties. Since
World War II, however, there has been an almost explosive increase of knowledge in the medical sciences as
well as enormous advances in technology as applicable to medicine. These developments have led to more and
more specialization. The knowledge of pathology has been greatly extended, mainly by the use of the electron
microscope; similarly microbiology, which includes bacteriology, expanded with the growth of such other
subfields as virology (the study of viruses) and mycology (the study of yeasts and fungi in medicine).
Biochemistry, sometimes called clinical chemistry or chemical pathology, has contributed to the knowledge of
disease, especially in the field of genetics where genetic engineering has become a key to curing some of the
most difficult diseases. Hematology also expanded after World War II with the development of electron
microscopy. Contributions to medicine have come from such fields as psychology and sociology especially in
such areas as mental disorders and mental handicaps. Clinical pharmacology has led to the development of
more effective drugs and to the identification of adverse reactions. More recently established medical specialties
are those of preventive medicine, physical medicine and rehabilitation, family practice, and nuclear medicine. In
the United States every medical specialist must be certified by a board composed of members of the specialty in
which certification is sought. Some type of peer certification is required in most countries.
Magnetic resonance imaging (MRI) is a powerful diagnostic technique that is used to visualize organs …
© Corbis
Expansion of knowledge both in depth and in range has encouraged the development of new forms of treatment
that require high degrees of specialization, such as organ transplantation and exchange transfusion; the field of
anesthesiology has grown increasingly complex as equipment and anesthetics have improved. New technologies
have introduced microsurgery, laser beam surgery, and lens implantation (for cataract patients), all requiring the
specialist’s skill. Precision in diagnosis has markedly improved; advances in radiology, the use of ultrasound,
Britannica LaunchPacks | The Treatment and Prevention of Disease
38 of 123© 2020 Encyclopædia Britannica, Inc.
computerized axial tomography (CAT scan), and nuclear magnetic resonance imaging are examples of the
extension of technology requiring expertise in the field of medicine.
To provide more efficient service it is not uncommon for a specialist surgeon and a specialist physician to form a
team working together in the field of, for example, heart disease. An advantage of this arrangement is that they
can attract a highly trained group of nurses, technologists, operating room technicians, and so on, thus greatly
improving the efficiency of the service to the patient. Such specialization is expensive, however, and has
required an increasingly large proportion of the health budget of institutions, a situation that eventually has its
financial effect on the individual citizen. The question therefore arises as to their cost-effectiveness.
Governments of developing countries have usually found, for instance, that it is more cost-efficient to provide
more people with basic care.
Teaching
Physicians in developed countries frequently prefer posts in hospitals with medical schools. Newly qualified
physicians want to work there because doing so will aid their future careers, though the actual experience may
be wider and better in a hospital without a medical school. Senior physicians seek careers in hospitals with
medical schools because consultant, specialist, or professorial posts there usually carry a high degree of
prestige. When the posts are salaried, the salaries are sometimes, but not always, higher than in a nonteaching
hospital. Usually a consultant who works in private practice earns more when on the staff of a medical school.
In many medical schools there are clinical professors in each of the major specialties—such as surgery, internal
medicine, obstetrics and gynecology, and psychiatry—and often of the smaller specialties as well. There are also
professors of pathology, radiology, and radiotherapy. Whether professors or not, all doctors in teaching hospitals
have the two functions of caring for the sick and educating students. They give lectures and seminars and are
accompanied by students on ward rounds.
Industrial medicine
The Industrial Revolution greatly changed, and as a rule worsened, the health hazards caused by industry, while
the numbers at risk vastly increased. In Britain the first small beginnings of efforts to ameliorate the lot of the
workers in factories and mines began in 1802 with the passing of the first factory act, the Health and Morals of
Apprentices Act. The factory act of 1838, however, was the first truly effective measure in the industrial field. It
forbade night work for children and restricted their work hours to 12 per day. Children under 13 were required to
attend school. A factory inspectorate was established, the inspectors being given powers of entry into factories
and power of prosecution of recalcitrant owners. Thereafter there was a succession of acts with detailed
regulations for safety and health in all industries. Industrial diseases were made notifiable, and those who
developed any prescribed industrial disease were entitled to benefits.
The situation is similar in other developed countries. Physicians are bound by legal restrictions and must report
industrial diseases. The industrial physician’s most important function, however, is to prevent industrial
diseases. Many of the measures to this end have become standard practice, but, especially in industries working
with new substances, the physician should determine if workers are being damaged and suggest preventive
measures. The industrial physician may advise management about industrial hygiene and the need for safety
devices and protective clothing and may become involved in building design. The physician or health worker
may also inform the worker of occupational health hazards.
Modern factories usually have arrangements for giving first aid in case of accidents. Depending upon the size of
the plant, the facilities may range from a simple first-aid station to a large suite of lavishly equipped rooms and
may include a staff of qualified nurses and physiotherapists and one or perhaps more full-time physicians.

Britannica LaunchPacks | The Treatment and Prevention of Disease
39 of 123© 2020 Encyclopædia Britannica, Inc.
Periodic medical examination
Physicians in industry carry out medical examinations, especially on new employees and on those returning to
work after sickness or injury. In addition, those liable to health hazards may be examined regularly in the hope
of detecting evidence of incipient damage. In some organizations every employee may be offered a regular
medical examination.
The industrial and the personal physician
When a worker also has a personal physician, there may be doubt, in some cases, as to which physician bears
the main responsibility for his health. When someone has an accident or becomes acutely ill at work, the first aid
is given or directed by the industrial physician. Subsequent treatment may be given either at the clinic at work
or by the personal physician. Because of labour-management difficulties, workers sometimes tend not to trust
the diagnosis of the management-hired physician.
Industrial health services
During the epoch of the Soviet Union and the Soviet bloc, industrial health service generally developed more
fully in those countries than in the capitalist countries. At the larger industrial establishments in the Soviet
Union, polyclinics were created to provide both occupational and general care for workers and their families.
Occupational physicians were responsible for preventing occupational diseases and injuries, health screening,
immunization, and health education.
In the capitalist countries, on the other hand, no fixed pattern of industrial health service has emerged.
Legislation impinges upon health in various ways, including the provision of safety measures, the restriction of
pollution, and the enforcement of minimum standards of lighting, ventilation, and space per person. In most of
these countries there is found an infinite variety of schemes financed and run by individual firms or, equally, by
huge industries. Labour unions have also done much to enforce health codes within their respective industries.
In the developing countries there has been generally little advance in industrial medicine.
Family health care
In many societies special facilities are provided for the health care of pregnant women, mothers, and their young
children. The health care needs of these three groups are generally recognized to be so closely related as to
require a highly integrated service that includes prenatal care, the birth of the baby, the postnatal period, and
the needs of the infant. Such a continuum should be followed by a service attentive to the needs of young
children and then by a school health service. Family clinics are common in countries that have state-sponsored
health services, such as those in the United Kingdom and elsewhere in Europe. Family health care in some
developed countries, such as the United States, is provided for low-income groups by state-subsidized facilities,
but other groups defer to private physicians or privately run clinics.
Prenatal clinics provide a number of elements. There is, first, the care of the pregnant woman, especially if she is
in a vulnerable group likely to develop some complication during the last few weeks of pregnancy and
subsequent delivery. Many potential hazards, such as diabetes and high blood pressure, can be identified and
measures taken to minimize their effects. In developing countries pregnant women are especially susceptible to
many kinds of disorders, particularly infections such as malaria. Local conditions determine what special
precautions should be taken to ensure a healthy child. Most pregnant women, in their concern to have a healthy
child, are receptive to simple health education. The prenatal clinic provides an excellent opportunity to teach the
mother how to look after herself during pregnancy, what to expect at delivery, and how to care for her baby. If
the clinic is attended regularly, the woman’s record will be available to the staff that will later supervise the

Britannica LaunchPacks | The Treatment and Prevention of Disease
40 of 123© 2020 Encyclopædia Britannica, Inc.
delivery of the baby; this is particularly important for someone who has been determined to be at risk. The same
clinical unit should be responsible for prenatal, natal, and postnatal care as well as for the care of the newborn
infants.
Most pregnant women can be safely delivered in simple circumstances without an elaborately trained staff or
sophisticated technical facilities, provided that these can be called upon in emergencies. In developed countries
it was customary in premodern times for the delivery to take place in the woman’s home supervised by a
qualified midwife or by the family doctor. By the mid-20th century women, especially in urban areas, usually
preferred to have their babies in a hospital, either in a general hospital or in a more specialized maternity
hospital. In many developing countries traditional birth attendants supervise the delivery. They are women, for
the most part without formal training, who have acquired skill by working with others and from their own
experience. Normally they belong to the local community where they have the confidence of the family, where
they are content to live and serve, and where their services are of great value. In many developing countries the
better training of birth attendants has a high priority. In developed Western countries there has been a trend
toward delivery by natural childbirth, including delivery in a hospital without anesthesia, and home delivery.
Postnatal care services are designed to supervise the return to normal of the mother. They are usually given by
the staff of the same unit that was responsible for the delivery. Important considerations are the matter of
breast- or artificial feeding and the care of the infant. Today the prospects for survival of babies born
prematurely or after a difficult and complicated labour, as well as for neonates (recently born babies) with some
physical abnormality, are vastly improved. This is due to technical advances, including those that can determine
defects in the prenatal stage, as well as to the growth of neonatology as a specialty. A vital part of the family
health-care service is the child welfare clinic, which undertakes the care of the newborn. The first step is the
thorough physical examination of the child on one or more occasions to determine whether or not it is normal
both physically and, if possible, mentally. Later periodic examinations serve to decide if the infant is growing
satisfactorily. Arrangements can be made for the child to be protected from major hazards by, for example,
immunization and dietary supplements. Any intercurrent condition, such as a chest infection or skin disorder,
can be detected early and treated. Throughout the whole of this period mother and child are together, and
particular attention is paid to the education of the mother for the care of the child.
A part of the health service available to children in the developed countries is that devoted to child guidance.
This provides psychiatric guidance to maladjusted children usually through the cooperative work of a child
psychiatrist, educational psychologist, and schoolteacher.
Geriatrics
Since the mid-20th century a change has occurred in the population structure in developed countries. The
proportion of elderly people has been increasing. Since 1983, however, in most European countries the
population growth of that group has leveled off, although it is expected to continue to grow more rapidly than
the rest of the population in most countries through the first third of the 21st century. In the late 20th century
Japan had the fastest growing elderly population.
Geriatrics, the health care of the elderly, is therefore a considerable burden on health services. In the United
Kingdom about one-third of all hospital beds are occupied by patients over 65; half of these are psychiatric
patients. The physician’s time is being spent more and more with the elderly, and since statistics show that
women live longer than men, geriatric practice is becoming increasingly concerned with the treatment of
women. Elderly people often have more than one disorder, many of which are chronic and incurable, and they
need more attention from health-care services. In the United States there has been some movement toward
making geriatrics a medical specialty, but it has not generally been recognized.

Britannica LaunchPacks | The Treatment and Prevention of Disease
41 of 123© 2020 Encyclopædia Britannica, Inc.
Support services for the elderly provided by private or state-subsidized sources include domestic help, delivery
of meals, day-care centres, elderly residential homes or nursing homes, and hospital beds either in general
medical wards or in specialized geriatric units. The degree of accessibility of these services is uneven from
country to country and within countries. In the United States, for instance, although there are some federal
programs, each state has its own elderly programs, which vary widely. However, as the elderly become an
increasingly larger part of the population their voting rights are providing increased leverage for obtaining more
federal and state benefits. The general practitioner or family physician working with visiting health and social
workers and in conjunction with the patient’s family often form a working team for elderly care.
In the developing world, countries are largely spared such geriatric problems, but not necessarily for positive
reasons. A principal cause, for instance, is that people do not live so long. Another major reason is that in the
extended family concept, still prevalent among developing countries, most of the caretaking needs of the elderly
are provided by the family.
Public health practice
Ministry of Public Health worker administering water-purifying tablets in Kabul, 2005.
Tomas Munita/AP
The physician working in the field of public health is mainly concerned with the environmental causes of ill
health and in their prevention. Bad drainage, polluted water and atmosphere, noise and smells, infected food,
bad housing, and poverty in general are all his special concern. Perhaps the most descriptive title he can be
given is that of community physician. In Britain he has been customarily known as the medical officer of health
and, in the United States, as the health officer.
The spectacular improvement in the expectation of life in the affluent countries has been due far more to public
health measures than to curative medicine. These public health measures began operation largely in the 19th
century. At the beginning of that century, drainage and water supply systems were all more or less primitive;
nearly all the cities of that time had poorer water and drainage systems than Rome had possessed 1,800 years
previously. Infected water supplies caused outbreaks of typhoid, cholera, and other waterborne infections. By
the end of the century, at least in the larger cities, water supplies were usually safe. Food-borne infections were
also drastically reduced by the enforcement of laws concerned with the preparation, storage, and distribution of
food. Insect-borne infections, such as malaria and yellow fever, which were common in tropical and semitropical
climates, were eliminated by the destruction of the responsible insects. Fundamental to this improvement in
health has been the diminution of poverty, for most public health measures are expensive. The peoples of the
developing countries fall sick and sometimes die from infections that are virtually unknown in affluent countries.
Britannica LaunchPacks | The Treatment and Prevention of Disease
42 of 123© 2020 Encyclopædia Britannica, Inc.
Britain
Public health services in Britain are organized locally under the National Health Service. The medical officer of
health is employed by the local council and is the adviser in health matters. The larger councils employ a
number of mostly full-time medical officers; in some rural areas, a general practitioner may be employed part-
time as medical officer of health.
The medical officer has various statutory powers conferred by acts of Parliament, regulations and orders, such
as food and drugs acts, milk and dairies regulations, and factories acts. He supervises the work of sanitary
inspectors in the control of health nuisances. The compulsorily notifiable infectious diseases are reported to him,
and he takes appropriate action. Other concerns of the medical officer include those involved with the work of
the district nurse, who carries out nursing duties in the home, and the health visitor, who gives advice on health
matters, especially to the mothers of small babies. He has other duties in connection with infant welfare clinics,
crèches, day and residential nurseries, the examination of schoolchildren, child guidance clinics, foster homes,
factories, problem families, and the care of the aged and the handicapped.
United States
Federal, state, county, and city governments all have public health functions. Under the U.S. Department of
Health and Human Services is the Public Health Service, headed by an assistant secretary for health and the
surgeon general. State health departments are headed by a commissioner of health, usually a physician, who is
often in the governor’s cabinet. He usually has a board of health that adopts health regulations and holds
hearings on their alleged violations. A state’s public health code is the foundation on which all county and city
health regulations must be based. A city health department may be independent of its surrounding county
health department, or there may be a combined city-county health department. The physicians of the local
health departments are usually called health officers, though occasionally people with this title are not
physicians. The larger departments may have a public health director, a district health director, or a regional
health director.
The minimal complement of a local health department is a health officer, a public health nurse, a sanitation
expert, and a clerk who is also a registrar of vital statistics. There may also be sanitation personnel, nutritionists,
social workers, laboratory technicians, and others.
Japan
Japan’s Ministry of Health and Welfare directs public health programs at the national level, maintaining close
coordination among the fields of preventive medicine, medical care, and welfare and health insurance. The
departments of health of the prefectures and of the largest municipalities operate health centres. The integrated
community health programs of the centres encompass maternal and child health, communicable-disease
control, health education, family planning, health statistics, food inspection, and environmental sanitation.
Private physicians, through their local medical associations, help to formulate and execute particular public
health programs needed by their localities.
Numerous laws are administered through the ministry’s bureaus and agencies, which range from public health,
environmental sanitation, and medical affairs to the children and families bureau. The various categories of
institutions run by the ministry, in addition to the national hospitals, include research centres for cancer and
leprosy, homes for the blind, rehabilitation centres for the physically handicapped, and port quarantine services.
Britannica LaunchPacks | The Treatment and Prevention of Disease
43 of 123© 2020 Encyclopædia Britannica, Inc.
Former Soviet Union
In the aftermath of the dissolution of the Soviet Union, responsibility for public health fell to the governments of
the successor countries.
The public health services for the U.S.S.R. as a whole were directed by the Ministry of Health. The ministry,
through the 15 union republic ministries of health, directed all medical institutions within its competence as well
as the public health authorities and services throughout the country.
The administration was centralized, with little local autonomy. Each of the 15 republics had its own ministry of
health, which was responsible for carrying out the plans and decisions established by the U.S.S.R. Ministry of
Health. Each republic was divided into , or provinces, which had departments of health directly oblastiresponsible to the republic ministry of health. Each , in turn, had (municipalities), which have their oblast rayonyown health departments accountable to the health department. Finally, each was subdivided into oblast rayonsmaller (districts).uchastoki
In most rural the responsibility for public health lay with the chief physician, who was also medical rayonydirector of the central hospital. This system ensured unity of public health administration and rayonimplementation of the principle of planned development. Other health personnel included nurses, feldshers, and
midwives.
For more information on the history, organization, and progress of public health, see below.
Military practice
The medical services of armies, navies, and air forces are geared to war. During campaigns the first requirement
is the prevention of sickness. In all wars before the 20th century, many more combatants died of disease than of
wounds. And even in World War II and wars thereafter, although few died of disease, vast numbers became
casualties from disease.
The main means of preventing sickness are the provision of adequate food and pure water, thus eliminating
starvation, avitaminosis, and dysentery and other bowel infections, which used to be particular scourges of
armies; the provision of proper clothing and other means of protection from the weather; the elimination from
the service of those likely to fall sick; the use of vaccination and suppressive drugs to prevent various infections,
such as typhoid and malaria; and education in hygiene and in the prevention of sexually transmitted diseases, a
particular problem in the services. In addition, the maintenance of high morale has a striking effect on casualty
rates, for, when morale is poor, soldiers are likely to suffer psychiatric breakdowns, and malingering is more
prevalent.
The medical branch may provide advice about disease prevention, but the actual execution of this advice is
through the ordinary chains of command. It is the duty of the military, not of the medical, officer to ensure that
the troops obey orders not to drink infected water and to take tablets to suppress malaria.
Army medical organization
The medical doctor of first contact to the soldier in the armies of developed countries is usually an officer in the
medical corps. In peacetime the doctor sees the sick and has functions similar to those of the general
practitioner, prescribing drugs and dressings, and there may be a sick bay where slightly sick soldiers can
remain for a few days. The doctor is usually assisted by trained nurses and corpsmen. If a further medical
opinion is required, the patient can be referred to a specialist at a military or civilian hospital.
Britannica LaunchPacks | The Treatment and Prevention of Disease
44 of 123© 2020 Encyclopædia Britannica, Inc.
In a war zone, medical officers have an aid post where, with the help of corpsmen, they apply first aid to the
walking wounded and to the more seriously wounded who are brought in. The casualties are evacuated as
quickly as possible by field ambulances or helicopters. At a company station, medical officers and medical
corpsmen may provide further treatment before patients are evacuated to the main dressing station at the field
ambulance headquarters, where a surgeon may perform emergency operations. Thereafter, evacuation may be
to casualty clearing stations, to advanced hospitals, or to base hospitals. Air evacuation is widely used.
In peacetime most of the intermediate medical units exist only in skeleton form; the active units are at the
battalion and hospital level. When physicians join the medical corps, they may join with specialist qualifications,
or they may obtain such qualifications while in the army. A feature of army medicine is promotion to
administrative positions. The commanding officer of a hospital and the medical officer at headquarters may have
no contacts with actual patients.
Although medical officers in peacetime have some choice of the kind of work they will do, they are in a chain of
command and are subject to military discipline. When dealing with patients, however, they are in a special
position; they cannot be ordered by a superior officer to give some treatment or take other action that they
believe is wrong. Medical officers also do not bear or use arms unless their patients are being attacked.
Naval and air force medicine
Naval medical services are run on lines similar to those of the army. Junior medical officers are attached to ships
or to shore stations and deal with most cases of sickness in their units. When at sea, medical officers have an
exceptional degree of responsibility in that they work alone, unless they are on a very large ship. In peacetime,
only the larger ships carry a medical officer; in wartime, destroyers and other small craft may also carry medical
officers. Serious cases go to either a shore-based hospital or a hospital ship.
Flying has many medical repercussions. Cold, lack of oxygen, and changes of direction at high speed all have
important effects on bodily and mental functions. Armies and air forces may share the same medical services.
A developing field is aerospace medicine. This involves medical problems that were not experienced before
spaceflight, for the main reason that humans in space are not under the influence of gravity, a condition that has
profound physiological effects.
Clinical researchThe remarkable developments in medicine brought about in the 20th and 21st centuries, especially after World
War II, were based on research either in the basic sciences related to medicine or in the clinical field. Advances
in the use of radiation, nuclear energy, and space research have played an important part in this progress. Some
laypersons often think of research as taking place only in sophisticated laboratories or highly specialized
institutions where work is devoted to scientific advances that may or may not be applicable to medical practice.
This notion, however, ignores the clinical research that takes place on a day-to-day basis in hospitals and
doctors’ offices.
Historical notes
Although the most spectacular changes in the medical scene during the 20th century, and the most widely
heralded, was the development of potent drugs and elaborate operations, another striking change included the
abandonment of most of the remedies of the past. In the mid-19th century, persons ill with numerous maladies
were starved (partially or completely), bled, purged, cupped (by applying a tight-fitting vessel filled with steam
to some part and then cooling the vessel), and rested, perhaps for months or even years. Much more recently

Britannica LaunchPacks | The Treatment and Prevention of Disease
45 of 123© 2020 Encyclopædia Britannica, Inc.
they were prescribed various restricted diets and were routinely kept in bed for weeks after abdominal
operations, for many weeks or months when their hearts were thought to be affected, and for many months or
years with tuberculosis. The abandonment of these measures may not be thought of as involving research, but
the physician who first encouraged persons who had peptic ulcers to eat normally (rather than to live on the
customary bland foods) and the physician who first got his patients out of bed a week or two after they had had
minor coronary thrombosis (rather than insisting on a minimum of six weeks of strict bed rest) were as much
doing research as is the physician who first tries out a new drug on a patient. This research, by observing what
happens when remedies are abandoned, has been of inestimable value, and the need for it has not passed.
Clinical observation
Much of the investigative clinical field work undertaken in the present day requires only relatively simple
laboratory facilities because it is observational rather than experimental in character. A feature of much
contemporary medical research is that it requires the collaboration of a number of persons, perhaps not all of
them doctors. Despite the advancing technology, there is much to be learned simply from the observation and
analysis of the natural history of disease processes as they begin to affect patients, pursue their course, and
end, either in their resolution or by the death of the patient. Such studies may be suitably undertaken by
physicians working in their offices who are in a better position than doctors working only in hospitals to observe
the whole course of an illness. Disease rarely begins in a hospital and usually does not end there. It is notable,
however, that observational research is subject to many limitations and pitfalls of interpretation, even when it is
carefully planned and meticulously carried out.
Drug research
The administration of any medicament, especially a new drug, to a patient is fundamentally an experiment: so is
a surgical operation, particularly if it involves a modification to an established technique or a completely new
procedure. Concern for the patient, careful observation, accurate recording, and a detached mind are the keys
to this kind of investigation, as indeed to all forms of clinical study. Because patients are individuals reacting to a
situation in their own different ways, the data obtained in groups of patients may well require statistical analysis
for their evaluation and validation.
One of the striking characteristics in the medical field in the 20th century, and which continued in the 21st
century, was the development of new drugs, usually by pharmaceutical companies. Until the end of the 19th
century, the discovery of new drugs was largely a matter of chance. It was in that period that Paul Ehrlich, the
German scientist, began to lay down the principles for modern pharmaceutical research that made possible the
development of a vast array of safe and effective drugs. Such benefits, however, bring with them their own
disadvantages: it is estimated that as many as 30 percent of patients in, or admitted to, hospitals suffer from the
adverse effect of drugs prescribed by a physician for their treatment (iatrogenic disease). Sometimes it is
extremely difficult to determine whether a drug has been responsible for some disorder. An example of the
difficulty is provided by the thalidomide disaster between 1959 and 1962. Only after numerous deformed babies
had been born throughout the world did it become clear that thalidomide taken by the mother as a sedative had
been responsible.
In hospitals where clinical research is carried out, ethical committees often consider each research project. If the
committee believes that the risks are not justified, the project is rejected.
After a potentially useful chemical compound has been identified in the laboratory, it is extensively tested in
animals, usually for a period of months or even years. Few drugs make it beyond this point. If the tests are
satisfactory, the decision may be made for testing the drug in humans. It is this activity that forms the basis of

Britannica LaunchPacks | The Treatment and Prevention of Disease
46 of 123© 2020 Encyclopædia Britannica, Inc.
much clinical research. In most countries the first step is the study of its effects in a small number of health
volunteers. The response, effect on metabolism, and possible toxicity are carefully monitored and have to be
completely satisfactory before the drug can be passed for further studies, namely with patients who have the
disorder for which the drug is to be used. Tests are administered at first to a limited number of these patients to
determine effectiveness, proper dosage, and possible adverse reactions. These searching studies are
scrupulously controlled under stringent conditions. Larger groups of patients are subsequently involved to gain a
wider sampling of the information. Finally, a full-scale clinical trial is set up. If the regulatory authority is satisfied
about the drug’s quality, safety, and efficacy, it receives a license to be produced. As the drug becomes more
widely used, it eventually finds its proper place in therapeutic practice, a process that may take years.
An important step forward in clinical research was taken in the mid-20th century with the development of the
controlled clinical trial. This sets out to compare two groups of patients, one of which has had some form of
treatment that the other group has not. The testing of a new drug is a case in point: one group receives the
drug, the other a product identical in appearance, but which is known to be inert—a so-called placebo. At the
end of the trial, the results of which can be assessed in various ways, it can be determined whether or not the
drug is effective and safe. By the same technique two treatments can be compared, for example a new drug
against a more familiar one. Because individuals differ physiologically and psychologically, the allocation of
patients between the two groups must be made in a random fashion; some method independent of human
choice must be used so that such differences are distributed equally between the two groups.
In order to reduce bias and make the trial as objective as possible the double-blind technique is sometimes used.
In this procedure, neither the doctor nor the patients know which of two treatments is being given. Despite such
precautions the results of such trials can be prejudiced, so that rigorous statistical analysis is required. It is
obvious that many ethical, not to say legal, considerations arise, and it is essential that all patients have given
their informed consent to be included. Difficulties arise when patients are unconscious, mentally confused, or
otherwise unable to give their informed consent. Children present a special difficulty because not all laws agree
that parents can legally commit a child to an experimental procedure. Trials, and indeed all forms of clinical
research that involve patients, must often be submitted to a committee set up locally to scrutinize each proposal.
Surgery
Surgeons operating on a patient.
© gchutka/iStock.com
In drug research the essential steps are taken by the chemists who synthesize or isolate new drugs in the
laboratory; clinicians play only a subsidiary part. In developing new surgical operations clinicians play a more
important role, though laboratory scientists and others in the background may also contribute largely. Many new
Britannica LaunchPacks | The Treatment and Prevention of Disease
47 of 123© 2020 Encyclopædia Britannica, Inc.
operations have been made possible by advances in anesthesia, and these in turn depend upon engineers who
have devised machines and chemists who have produced new drugs. Other operations are made possible by
new materials, such as the alloys and plastics that are used to make artificial hip and knee joints.
Whenever practicable, new operations are tried on animals before they are tried on patients. This practice is
particularly relevant to organ transplants. Surgeons themselves—not experimental physiologists—transplanted
kidneys, livers, and hearts in animals before attempting these procedures on patients. Experiments on animals
are of limited value, however, because animals do not suffer from all of the same maladies as do humans.
Many other developments in modern surgical treatment rest on a firm basis of experimentation, often first in
animals but also in humans; among them are renal dialysis (the artificial kidney), arterial bypass operations,
embryo implantation, and exchange transfusions. These treatments are but a few of the more dramatic of a
large range of therapeutic measures that have not only provided patients with new therapies but also have led
to the acquisition of new knowledge of how the body works. Among the research projects of the late 20th and
early 21st centuries was that of gene transplantation, which had the potential of providing cures for cancer and
other diseases.
Screening proceduresDevelopments in modern medical science have made it possible to detect morbid conditions before a person
actually feels the effects of the condition. Examples are many: they include certain forms of cancer; high blood
pressure; heart and lung disease; various familial and congenital conditions; disorders of metabolism, like
diabetes; and acquired immune deficiency syndrome (AIDS). The consideration to be made in screening is
whether or not such potential patients should be identified by periodic examinations. To do so is to imply that
the subjects should be made aware of their condition and, second, that there are effective measures that can be
taken to prevent their condition, if they test positive, from worsening. Such so-called specific screening
procedures are costly since they involve large numbers of people. Screening may lead to a change in the life-
style of many persons, but not all such moves have been shown in the long run to be fully effective. Although
screening clinics may not be run by doctors, they are a factor of increasing importance in the preventive health
service.
Periodic general medical examination of various sections of the population, business executives for example, is
another way of identifying risk factors that, if not corrected, can lead to the development of overt disease.
John Walford ToddHarold Scarborough
Additional ReadingWebster’s Medical Desk Dictionary (1986), is a reference source for the layman. The Oxford Companion to
, 2 vol., edited by , , and (1986), is a comprehensive text Medicine JOHN WALTON PAUL B. BEESON RONALD BODLEY SCOTT
of 20th-century developments and persons.
GEORGE ROSEN, (1983), is a historical study. Particular The Structure of American Medical Practice, 1875–1941
kinds of medical practice are explored in and (eds.), WESLEY FABB JOHN FRY Principles of Practice Management in
(1984); , edited by Primary Care SIR DOUGLAS BLACKet al., Inequalities in Health: The Black Report PETER TOWNSEND
and (1982); and , NICK DAVIDSON DAVID SANDERS RICHARD CARVER The Struggle for Health: Medicine and the Politics of
(1985); and and (eds.), Underdevelopment V. DJUKANOVIC E.P. MACH Alternative Approaches to Meeting Basic
(1975). Also see the articles of such journals Health Needs in Developing Countries: A Joint UNICEF/WHO Study
Britannica LaunchPacks | The Treatment and Prevention of Disease
48 of 123© 2020 Encyclopædia Britannica, Inc.
as (monthly) and (semimonthly). For a view of alternative medicine, see Private Practice Modern Healthcare and (eds.), (1985); and , DOUGLAS STALKER CLARK GLYMOUR Examining Holistic Medicine RICHARD GROSSMAN The Other
(1985). The variety of roles in the health-care profession are the subject of , Medicines LOUISE SIMMERS Diversified
(1983); , , and , Health Occupations C. WESLEY EISELE WILLIAM R. FIFER TOMA C. WILSON The Medical Staff and the
(1985); and (ed.), Modern Hospital ELI GINZBERG From Physician Shortage to Patient Shortage: The Uncertain
(1986).Future of Medical Practice
Citation (MLA style):
"Medicine." , Encyclopædia Britannica, 21 Mar. Britannica LaunchPacks: The Treatment and Prevention of Disease2022. packs-ngl.eb.com. Accessed 6 Apr. 2022.
While every effort has been made to follow citation style rules, there may be some discrepancies. Please refer to the appropriate style manual or other sources if you have any questions.
nutritional diseaseany of the nutrient-related diseases and conditions that cause illness in humans. They may include deficiencies
or excesses in the diet, obesity and eating disorders, and chronic diseases such as cardiovascular disease,
hypertension, cancer, and diabetes mellitus. Nutritional diseases also include developmental abnormalities that
can be prevented by diet, hereditary metabolic disorders that respond to dietary treatment, the interaction of
foods and nutrients with drugs, food allergies and intolerances, and potential hazards in the food supply. All of
these categories are described in this article. For a discussion of essential nutrients, dietary recommendations,
and human nutritional needs and concerns throughout the life cycle, nutrition, human.see
Children with rickets. The disease, which most commonly strikes children, causes bone deformities…
Robin Laurance/Alamy
Nutrient deficienciesAlthough the so-called diseases of civilization—for example, heart disease, stroke, cancer, and diabetes—will be
the focus of this article, the most significant nutrition-related disease is chronic undernutrition, which plagues
Britannica LaunchPacks | The Treatment and Prevention of Disease
49 of 123© 2020 Encyclopædia Britannica, Inc.
more than 925 million people worldwide. Undernutrition is a condition in which there is insufficient food to meet
energy needs; its main characteristics include weight loss, failure to thrive, and wasting of body fat and muscle.
Low birth weight in infants, inadequate growth and development in children, diminished mental function, and
increased susceptibility to disease are among the many consequences of chronic persistent hunger, which
affects those living in poverty in both industrialized and developing countries. The largest number of chronically
hungry people live in Asia, but the severity of hunger is greatest in sub-Saharan Africa. At the start of the 21st
century, approximately 20,000 people, the majority of them children, died each day from undernutrition and
related diseases that could have been prevented. The deaths of many of these children stem from the poor
nutritional status of their mothers as well as the lack of opportunity imposed by poverty.
Only a small percentage of hunger deaths is caused by starvation due to catastrophic food shortages. During the
1990s, for example, worldwide famine (epidemic failure of the food supply) more often resulted from complex
social and political issues and the ravages of war than from natural disasters such as droughts and floods.
Launching a cookbook for Irish cancer patients with involuntary weight loss.
University College Cork, Ireland
Malnutrition is the impaired function that results from a prolonged deficiency—or excess—of total energy or
specific nutrients such as protein, essential fatty acids, vitamins, or minerals. This condition can result from
fasting and anorexia nervosa; persistent vomiting (as in bulimia nervosa) or inability to swallow; impaired
digestion and intestinal malabsorption; or chronic illnesses that result in loss of appetite (e.g., cancer, AIDS).
Malnutrition can also result from limited food availability, unwise food choices, or overzealous use of dietary
supplements.
Select nutrient-deficiency diseasesSelected nutrient-deficiency diseases are listed in the table.
Protein-energy malnutrition
Chronic undernutrition manifests primarily as protein-energy malnutrition (PEM), which is the most common form
of malnutrition worldwide. Also known as protein-calorie malnutrition, PEM is a continuum in which people—all
too often children—consume too little protein, energy, or both. At one end of the continuum is kwashiorkor,
characterized by a severe protein deficiency, and at the other is marasmus, an absolute food deprivation with
grossly inadequate amounts of both energy and protein.
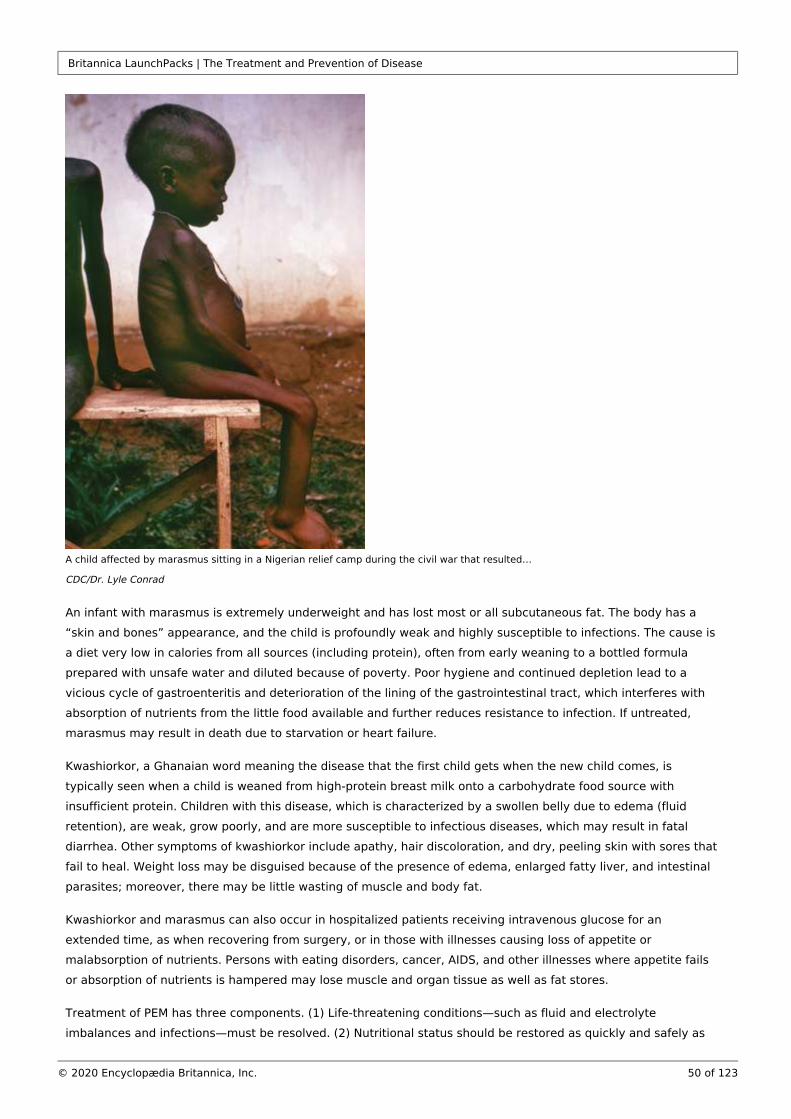
Britannica LaunchPacks | The Treatment and Prevention of Disease
50 of 123© 2020 Encyclopædia Britannica, Inc.
A child affected by marasmus sitting in a Nigerian relief camp during the civil war that resulted…
CDC/Dr. Lyle Conrad
An infant with marasmus is extremely underweight and has lost most or all subcutaneous fat. The body has a
“skin and bones” appearance, and the child is profoundly weak and highly susceptible to infections. The cause is
a diet very low in calories from all sources (including protein), often from early weaning to a bottled formula
prepared with unsafe water and diluted because of poverty. Poor hygiene and continued depletion lead to a
vicious cycle of gastroenteritis and deterioration of the lining of the gastrointestinal tract, which interferes with
absorption of nutrients from the little food available and further reduces resistance to infection. If untreated,
marasmus may result in death due to starvation or heart failure.
Kwashiorkor, a Ghanaian word meaning the disease that the first child gets when the new child comes, is
typically seen when a child is weaned from high-protein breast milk onto a carbohydrate food source with
insufficient protein. Children with this disease, which is characterized by a swollen belly due to edema (fluid
retention), are weak, grow poorly, and are more susceptible to infectious diseases, which may result in fatal
diarrhea. Other symptoms of kwashiorkor include apathy, hair discoloration, and dry, peeling skin with sores that
fail to heal. Weight loss may be disguised because of the presence of edema, enlarged fatty liver, and intestinal
parasites; moreover, there may be little wasting of muscle and body fat.
Kwashiorkor and marasmus can also occur in hospitalized patients receiving intravenous glucose for an
extended time, as when recovering from surgery, or in those with illnesses causing loss of appetite or
malabsorption of nutrients. Persons with eating disorders, cancer, AIDS, and other illnesses where appetite fails
or absorption of nutrients is hampered may lose muscle and organ tissue as well as fat stores.
Treatment of PEM has three components. (1) Life-threatening conditions—such as fluid and electrolyte
imbalances and infections—must be resolved. (2) Nutritional status should be restored as quickly and safely as

Britannica LaunchPacks | The Treatment and Prevention of Disease
51 of 123© 2020 Encyclopædia Britannica, Inc.
possible; rapid weight gain can occur in a starving child within one or two weeks. (3) The focus of treatment then
shifts to ensuring nutritional rehabilitation for the long term. The speed and ultimate success of recovery depend
upon the severity of malnutrition, the timeliness of treatment, and the adequacy of ongoing support. Particularly
during the first year of life, starvation may result in reduced brain growth and intellectual functioning that cannot
be fully restored.
Carbohydrates
Under most circumstances, there is no absolute dietary requirement for carbohydrates—simple sugars, complex
carbohydrates such as starches, and the indigestible plant carbohydrates known as dietary fibre. Certain cells,
such as brain cells, require the simple carbohydrate glucose as fuel. If dietary carbohydrate is insufficient,
glucose synthesis depends on the breakdown of amino acids derived from body protein and dietary protein and
the compound glycerol, which is derived from fat. Long-term carbohydrate inadequacy results in increased
production of organic compounds called ketones (a condition known as ketosis), which imparts a distinctive
sweet odour to the breath. Ketosis and other untoward effects of a very-low-carbohydrate diet can be prevented
by the daily consumption of 50 to 100 grams of carbohydrate; however, obtaining at least half of the daily
energy intake from carbohydrates is recommended and is typical of human diets, corresponding to at least 250
grams of carbohydrate (1,000 calories in a 2,000-calorie diet). A varied diet containing fruits, vegetables,
legumes, and whole-grain cereals, which are all abundant in carbohydrates, also provides a desirable intake of
dietary fibre.
Essential fatty acids
There is also a minimum requirement for fat—not for total fat, but only for the fatty acids linoleic acid (a so-
called omega-6 fatty acid) and alpha-linolenic acid (an omega-3 fatty acid). Deficiencies of these two fatty acids
have been seen in hospitalized patients fed exclusively with intravenous fluids containing no fat for weeks,
patients with medical conditions affecting fat absorption, infants given formulas low in fat, and young children
fed nonfat milk or low-fat diets. Symptoms of deficiency include dry skin, hair loss, and impaired wound healing.
Essential fatty acid requirements—a few grams a day—can be met by consuming approximately a tablespoon of
polyunsaturated plant oils daily. Fatty fish also provides a rich source of omega-3 fatty acids. Even individuals
following a low-fat diet generally consume sufficient fat to meet requirements.
Vitamins
Although deficiency diseases have been described in laboratory animals and humans deprived of single
vitamins, in human experience multiple deficiencies are usually present simultaneously. The eight B-complex
vitamins function in coordination in numerous enzyme systems and metabolic pathways; thus, a deficiency of
one may affect the functioning of others.
Vitamin A
Vitamin A deficiency is the leading cause of preventable blindness in children and is a major problem in the
developing world, especially in Africa and Southeast Asia; in the poorest countries hundreds of thousands of
children become blind each year due to a deficiency of the vitamin. Even a mild deficiency can impair immune
function, thereby reducing resistance to disease. Night blindness is an early sign of vitamin A deficiency,
followed by abnormal dryness of the eye and ultimately scarring of the cornea, a condition known as
xerophthalmia. Other symptoms include dry skin, hardening of epithelial cells elsewhere in the body (such as
mucous membranes), and impaired growth and development. In many areas where vitamin A deficiency is

Britannica LaunchPacks | The Treatment and Prevention of Disease
52 of 123© 2020 Encyclopædia Britannica, Inc.
endemic, the incidence is being reduced by giving children a single large dose of vitamin A every six months. A
genetically modified form of rice containing beta-carotene, a precursor of vitamin A, has the potential to reduce
greatly the incidence of vitamin A deficiency, but the use of this so-called golden rice is controversial.
Vitamin D
Vitamin D (also known as vitamin D hormone) is synthesized in the body in a series of steps, starting in the skin
by the action of sunlight’s ultraviolet rays on a precursor compound; thus, without adequate food sources of
vitamin D, a deficiency of the vitamin can occur when exposure to sunlight is limited. Lack of vitamin D in
children causes rickets, a disease characterized by inadequate mineralization of bone, growth retardation, and
skeletal deformities such as bowed legs. The adult form of rickets, known as osteomalacia, results in weak
muscles as well as weak bones. Inadequate vitamin D may also contribute to the thinning of bones seen in
osteoporosis. Individuals with limited sun exposure (including women who completely cover their bodies for
religious reasons), elderly or homebound persons, and those with dark skin, particularly those who live in
northern latitudes, are at risk of vitamin D deficiency. Vitamin D is found in very few foods naturally; thus
fortification of milk and other foods (e.g., margarine, cereals, and breads) with the vitamin has helped protect
those populations in which sun exposure is inadequate. Supplemental vitamin D also may help protect against
bone fractures in the elderly, who make and activate vitamin D less efficiently even if exposed to sunlight.
Vitamin E
Vitamin Edeficiency is rare in humans, although it may develop in premature infants and in people with impaired
fat absorption or metabolism. In the former, fragility of red blood cells (hemolysis) is seen; in the latter, where
deficiency is more prolonged, neuromuscular dysfunction involving the spinal cord and retina may result in loss
of reflexes, impaired balance and coordination, muscle weakness, and visual disturbances. No specific metabolic
function has been established for vitamin E; however, it is an important part of the antioxidant system that
inhibits lipid peroxidation—i.e., it protects cells and their membranes against the damaging effects of free
radicals (reactive oxygen and nitrogen species) that are produced metabolically or enter the body from the
environment. The requirement for vitamin E is increased with increasing consumption of polyunsaturated fatty
acids. People who smoke or are subjected to air pollution may also need more of the vitamin to protect against
oxidative damage to the lungs.
Vitamin K
Vitamin K is necessary for the formation of prothrombin and other blood-clotting factors in the liver, and it also
plays a role in bone metabolism. A form of the vitamin is produced by bacteria in the colon and can be utilized to
some degree. Vitamin K deficiency causes impaired clotting of the blood and internal bleeding, even without
injury. Due to poor transport of vitamin K across the placenta, newborn infants in developed countries are
routinely given the vitamin intramuscularly or orally within six hours of birth to protect against a condition known
as hemorrhagic disease of the newborn. Vitamin K deficiency is rare in adults, except in syndromes with poor fat
absorption, in liver disease, or during treatment with certain anticoagulant drugs, which interfere with vitamin K
metabolism. Bleeding due to vitamin K deficiency may be seen in patients whose gut bacteria have been killed
by antibiotics.
Thiamin
Prolonged deficiency of thiamin (vitamin B ) results in beriberi, a disease that has been endemic in populations 1
where white rice has been the staple. Thiamin deficiency is still seen in areas where white rice or flour
constitutes the bulk of the diet and thiamin lost in milling is not replaced through enrichment. Symptoms of the
form known as dry beriberi include loss of appetite, confusion and other mental symptoms, muscle weakness,

Britannica LaunchPacks | The Treatment and Prevention of Disease
53 of 123© 2020 Encyclopædia Britannica, Inc.
painful calf muscles, poor coordination, tingling and paralysis. In wet beriberi there is edema and the possibility
of an enlarged heart and heart failure. Thiamin deficiency can also occur in populations eating large quantities of
raw fish harbouring intestinal microbes that contain the enzyme thiaminase. In the developed world, thiamin
deficiency is linked primarily to chronic alcoholism with poor diet, manifesting as Wernicke-Korsakoff syndrome,
a condition with rapid eye movements, loss of muscle coordination, mental confusion, and memory loss.
Riboflavin
Riboflavin (vitamin B ) deficiency, known as ariboflavinosis, is unlikely without the simultaneous deficiency of 2
other nutrients. After several months of riboflavin deprivation, symptoms include cracks in the skin at the
corners of the mouth, fissures of the lips, and an inflamed, magenta-coloured tongue. Because riboflavin is
readily destroyed by ultraviolet light, jaundiced infants who are treated with light therapy are administered the
vitamin. Milk, milk products, and cereals, major sources of riboflavin in the diet, are packaged to prevent
exposure to light.
Niacin
Symptoms of pellagra develop about two months after niacin is withdrawn from the diet. Pellagra is
characterized by the so-called three Ds—diarrhea, dermatitis, and dementia—and, if it is allowed to progress
untreated, death ensues. Pellagra was common in areas of the southern United States in the early 1900s and
still occurs in parts of India, China, and Africa, affecting people who subsist primarily on corn. The niacin in corn
and other cereal grains is largely in bound form, unable to be absorbed well. Soaking corn in lime water, as
practiced by Native American populations for centuries, frees bound niacin and thus protects against pellagra. In
addition, unlike other cereals, corn is low in the amino acidtryptophan, which can be converted in part to niacin.
Sufficient high-quality protein (containing tryptophan) in the diet can protect against niacin deficiency even if
intake of niacin itself is inadequate.
Vitamin B6
Vitamin B (pyridoxine and related compounds) is essential in protein metabolism, the synthesis of 6
neurotransmitters, and other critical functions in the body. Deficiency symptoms include dermatitis, microcytic
hypochromic anemia (small, pale red blood cells), impaired immune function, depression, confusion, and
convulsions. Although full-blown vitamin B deficiency is rare, marginal inadequacy is more widespread, 6
especially among the elderly, who may have a reduced ability to absorb the vitamin. People with alcoholism,
especially those with the liver diseases cirrhosis and hepatitis, are at risk of deficiency. A number of drugs,
including the tuberculosis drug isoniazid, interfere with vitamin B metabolism.6
Folic acid
Vitamin B and folic acid (folate) are two B vitamins with many closely related functions, notably participation in 12
DNA synthesis. As a result, people with deficiencies of either vitamin show many of the same symptoms, such as
weakness and fatigue due to megaloblastic anemia, a condition in which red blood cells, lacking sufficient DNA
for cell division, are large and immature. Deficiency of folic acid also causes disruption of cell division along the
gastrointestinal tract, which results in persistent diarrhea, and impaired synthesis of white blood cells and
platelets. Inadequate intake of the vitamin in early pregnancy may cause neural tube defects in the fetus. Thus,
women capable of becoming pregnant are advised to take 400 micrograms (μg) of folic acid daily from
supplements, fortified foods (such as fortified cereals), or both—in addition to consuming foods rich in folic acid

Britannica LaunchPacks | The Treatment and Prevention of Disease
54 of 123© 2020 Encyclopædia Britannica, Inc.
such as fresh fruits and vegetables (especially leafy greens) and legumes. The cancer drug methotrexate
interferes with folic acid metabolism, causing side effects such as hair loss and diarrhea. Folic acid deficiency
may also result from heavy use of alcohol, which interferes with absorption of the vitamin.
Vitamin B12
Deficiency of vitamin B (cobalamin), like folic acid, results in megaloblastic anemia (large, immature red blood 12
cells), due to interference with normal DNA synthesis. Additionally, vitamin B maintains the myelin sheath that 12
protects nerve fibres; therefore, an untreated deficiency of the vitamin can result in nerve degeneration and
eventually paralysis. Large amounts of folic acid (over 1,000 μg per day) may conceal, and possibly even
exacerbate, an underlying vitamin B deficiency. Symptoms of vitamin B deficiency can include weakness, 12 12
fatigue, pain, shortness of breath, numbness or tingling sensations, mental changes, and vision problems. Only
animal foods are reliable sources of vitamin B . Vegans, who eat no foods of animal origin, are at risk of vitamin 12
B deficiency and must obtain the vitamin through fortified food or a supplement. For people who regularly eat 12
animal products, deficiency of the vitamin is unlikely, unless there is a defect in absorption. In order to be
absorbed, vitamin B must be bound to intrinsic factor, a substance secreted by the stomach. If intrinsic factor 12
is absent (due to an autoimmune disorder known as pernicious anemia) or if there is insufficient production of
hydrochloric acid by the stomach, absorption of the vitamin will be limited. Pernicious anemia, which occurs
most often in the elderly, can be treated by injections or massive oral doses (1,000 μg) of vitamin B .12
Pantothenic acid
Pantothenic acid is so widespread in foods that deficiency is unlikely under normal circumstances. Deficiency has
been seen only in individuals fed semisynthetic diets deficient in the vitamin or in subjects given a pantothenic
acid antagonist. Symptoms of deficiency include fatigue, irritability, sleep disturbances, abdominal distress, and
neurological symptoms such as tingling in the hands. Deficiency of the vitamin was suspected during World War
II when prisoners of war in Asia who exhibited “burning feet” syndrome, characterized by numbness and tingling
in the toes and other neurological symptoms, responded only to the administration of pantothenic acid.
Biotin
Deficiency of biotin is rare, and this may be due in part to synthesis of the vitamin by bacteria in the colon,
although the importance of this source is unclear. Biotin deficiency has been observed in people who regularly
eat large quantities of raw egg white, which contains a glycoprotein (avidin) that binds biotin and prevents its
absorption. A rare genetic defect that renders some infants unable to absorb a form of biotin in food can be
treated with a supplement of the vitamin. Long-term use of certain anticonvulsant drugs may also impair biotin
absorption. Symptoms of deficiency include skin rash, hair loss, and eventually neurological abnormalities.
Vitamin C
Vitamin C, also known as ascorbic acid, functions as a water-soluble antioxidant and as a cofactor in various
enzyme systems, such as those involved in the synthesis of connective tissue components and
neurotransmitters. Symptoms of scurvy, a disease caused by vitamin C deficiency, include pinpoint hemorrhages
(petechiae) under the skin, bleeding gums, joint pain, and impaired wound healing. Although rare in developed
countries, scurvy is seen occasionally in people consuming restricted diets, particularly those containing few
fruits and vegetables, or in infants fed boiled cow’s milk and no source of vitamin C. Scurvy can be prevented
with relatively small quantities of vitamin C (10 milligrams [mg] per day), although recommended intakes, which

Britannica LaunchPacks | The Treatment and Prevention of Disease
55 of 123© 2020 Encyclopædia Britannica, Inc.
aim to provide sufficient antioxidant protection, are closer to 100 mg per day. Disease states, environmental
toxins, drugs, and other stresses can increase an individual’s vitamin C needs. Smokers, for example, may
require an additional 35 mg of the vitamin daily to maintain vitamin C levels comparable to nonsmokers.
Minerals
Iron
Iron deficiency is the most common of all nutritional deficiencies, with much of the world’s population being
deficient in the mineral to some degree. Young children and premenopausal women are the most vulnerable.
The main function of iron is in the formation of hemoglobin, the red pigment of the blood that carries oxygen
from the lungs to other tissues. Since each millilitre of blood contains 0.5 mg of iron (as a component of
hemoglobin), bleeding can drain the body’s iron reserves. When iron stores are depleted a condition arises
known as microcytic hypochromic anemia, characterized by small red blood cells that contain less hemoglobin
than normal. Symptoms of severe iron deficiency anemia include fatigue, weakness, apathy, pale skin, difficulty
breathing on exertion, and low resistance to cold temperatures. During childhood, iron deficiency can affect
behaviour and learning ability as well as growth and development. Severe anemia increases the risk of
pregnancy complications and maternal death. Iron deficiency anemia is most common during late infancy and
early childhood, when iron stores present from birth are exhausted and milk, which is poor in iron, is a primary
food; during the adolescent growth spurt; and in women during the childbearing years, because of blood loss
during menstruation and the additional iron needs of pregnancy. Intestinal blood loss and subsequent iron
deficiency anemia in adults may also stem from ulcers, hemorrhoids, tumours, or chronic use of certain drugs
such as aspirin. In developing countries, blood loss due to hookworm and other infections, coupled with
inadequate dietary iron intake, exacerbates iron deficiency in both children and adults.
Iodine
Iodine deficiency disorders are the most common cause of preventable brain damage, which affects an
estimated 50 million people worldwide. During pregnancy, severe iodine deficiency may impair fetal
development, resulting in cretinism (irreversible mental retardation with short stature and developmental
abnormalities) as well as in miscarriage and stillbirth. Other more pervasive consequences of chronic iodine
deficiency include lesser cognitive and neuromuscular deficits. The ocean is a dependable source of iodine, but
away from coastal areas iodine in food is variable and largely reflects the amount in the soil. In chronic iodine
deficiency the thyroid gland enlarges as it attempts to trap more iodide (the form in which iodine functions in the
body) from the blood for synthesis of thyroid hormones, and it eventually becomes a visible lump at the front of
the neck known as a goitre. Some foods, such as cassava, millet, sweet potato, certain beans, and members of
the cabbage family, contain substances known as goitrogens that interfere with thyroid hormone synthesis;
these substances, which are destroyed by cooking, can be a significant factor in persons with coexisting iodine
deficiency who rely on goitrogenic foods as staples. Since a strategy of universal iodization of salt was adopted
in 1993, there has been remarkable progress in improving iodine status worldwide. Nonetheless, millions of
people living in iodine-deficient areas, primarily in Central Africa, Southeast and Central Asia, and even in central
and eastern Europe, remain at risk.
Zinc
A constituent of numerous enzymes, zinc plays a structural role in proteins and regulates gene expression. Zinc
deficiency in humans was first reported in the 1960s in Egypt and Iran, where children and adolescent boys with
stunted growth and undeveloped genitalia responded to treatment with zinc. Deficiency of the mineral was
attributed to the regional diet, which was low in meat and high in legumes, unleavened breads, and whole-grain
foods that contain fibre, phytic acid, and other factors that inhibit zinc absorption. Also contributing to zinc
Britannica LaunchPacks | The Treatment and Prevention of Disease
56 of 123© 2020 Encyclopædia Britannica, Inc.
deficiency was the practice of clay eating, which interferes with the absorption of zinc, iron, and other minerals.
Severe zinc deficiency has also been described in patients fed intravenous solutions inadequate in zinc and in
the inherited zinc-responsive syndrome known as acrodermatitis enteropathica. Symptoms of zinc deficiency
may include skin lesions, diarrhea, increased susceptibility to infections, night blindness, reduced taste and
smell acuity, poor appetite, hair loss, slow wound healing, low sperm count, and impotence. Zinc is highest in
protein-rich foods, especially red meat and shellfish, and zinc status may be low in protein-energy malnutrition.
Even in developed countries, young children, pregnant women, the elderly, strict vegetarians, people with
alcoholism, and those with malabsorption syndromes are vulnerable to zinc deficiency.
Calcium
Almost all the calcium in the body is in the bones and teeth, the skeleton serving as a reservoir for calcium
needed in the blood and elsewhere. During childhood and adolescence, adequate calcium intake is critical for
bone growth and calcification. A low calcium intake during childhood, and especially during the adolescent
growth spurt, may predispose one to osteoporosis, a disease characterized by reduced bone mass, later in life.
As bones lose density, they become fragile and unable to withstand ordinary strains; the resulting fractures,
particularly of the hip, may cause incapacitation and even death. Osteoporosis is particularly common in
postmenopausal women in industrial societies. Not a calcium-deficiency disease per se, osteoporosis is strongly
influenced by heredity; risk of the disease can be lessened by ensuring adequate calcium intake throughout life
and engaging in regular weight-bearing exercise. Sufficient calcium intake in the immediate postmenopausal
years does appear to slow bone loss, although not to the same extent as do bone-conserving drugs.
Fluoride
Learn what causes bad breath and how to prevent it.
© American Chemical Society
Fluoride also contributes to the mineralization of bones and teeth and protects against tooth decay.
Epidemiological studies in the United States in the 1930s and 1940s revealed an inverse relationship between
the natural fluoride content of waters and the rate of dental caries. In areas where fluoride levels in the drinking
water are low, prescription fluoride supplements are recommended for children older than six months of age;
dentists also may apply fluoride rinses or gels periodically to their patients’ teeth. Fluoridated toothpastes are an
important source of fluoride for children and also for adults, who continue to benefit from fluoride intake.
Sodium
Sodium is usually provided in ample amounts by food, even without added table salt (sodium chloride).
Furthermore, the body’s sodium-conservation mechanisms are highly developed, and thus sodium deficiency is
rare, even for those on low-sodium diets. Sodium depletion may occur during prolonged heavy sweating,
vomiting, or diarrhea or in the case of kidney disease. Symptoms of hyponatremia, or low blood sodium, include
muscle cramps, nausea, dizziness, weakness, and eventually shock and coma. After prolonged high-intensity
Britannica LaunchPacks | The Treatment and Prevention of Disease
57 of 123© 2020 Encyclopædia Britannica, Inc.
exertion in the heat, sodium balance can be restored by drinking beverages containing sodium and glucose (so-
called sports drinks) and by eating salted food. Drinking a litre of water containing two millilitres (one-third
teaspoon) of table salt also should suffice.
Chloride is lost from the body under conditions that parallel those of sodium loss. Severe chloride depletion
results in a condition known as metabolic alkalosis (excess alkalinity in body fluids).
Potassium
Potassium is widely distributed in foods and is rarely deficient in the diet. However, some diuretics used in the
treatment of hypertension deplete potassium. The mineral is also lost during sustained vomiting or diarrhea or
with chronic use of laxatives. Symptoms of potassium deficiency include weakness, loss of appetite, muscle
cramps, and confusion. Severe hypokalemia (low blood potassium) may result in cardiac arrhythmias. Potassium-
rich foods, such as bananas or oranges, can help replace losses of the mineral, as can potassium chloride
supplements, which should be taken only under medical supervision.
Water deficiency (dehydration)
Water is the largest component of the body, accounting for more than half of body weight. To replace fluid
losses, adults generally need to consume 2 to 4 litres of fluid daily in cool climates, depending on degree of
activity, and from 8 to 16 litres a day in very hot climates. Dehydration may develop if water consumption fails
to satisfy thirst; if the thirst mechanism is not functioning properly, as during intense physical exercise; or if
there is excessive fluid loss, as with diarrhea or vomiting. By the time thirst is apparent, there is already some
degree of dehydration, which is defined as loss of fluid amounting to at least 1 to 2 percent of body weight.
Symptoms can progress quickly if not corrected: dry mouth, sunken eyes, poor skin turgor, cold hands and feet,
weak and rapid pulse, rapid and shallow breathing, confusion, exhaustion, and coma. Loss of fluid constituting
more than 10 percent of body weight may be fatal. The elderly (whose thirst sensation may be dulled), people
who are ill, and those flying in airplanes are especially vulnerable to dehydration. Infants and children with
chronic undernutrition who develop gastroenteritis may become severely dehydrated from diarrhea or vomiting.
Treatment is with an intravenous or oral solution of glucose and salts.
Nutrient toxicitiesThe need for each nutrient falls within a safe or desirable range, above which there is a risk of adverse effects.
Any nutrient, even water, can be toxic if taken in very large quantities. Overdoses of certain nutrients, such as
iron, can cause poisoning (acute toxicity) and even death. For most nutrients, habitual excess intake poses a risk
of adverse health effects (chronic toxicity). Sustained overconsumption of the calorie-yielding nutrients
(carbohydrate, fat, and protein) and alcohol increases the risk of obesity and specific chronic diseases ( seebelow), and use of isolated amino acids can lead to imbalances and toxicities. However, for most individuals, the
risk of harm due to excess intake of vitamins or minerals in food is low.
Tolerable upper intake level (UL) for selected nutrients for adultsIn 1997 the U.S. Institute of Medicine
established a reference value called the Tolerable Upper Intake Level (UL) for selected nutrients, which is also
being used as a model for other countries. The UL is the highest level of daily nutrient intake likely to pose no
risk of adverse health effects for almost all individuals in the general population and is not meant to apply to
people under medical supervision. Discussed below as “safe intakes” for adults, most ULs for infants, children,
and adolescents are considerably lower.
Britannica LaunchPacks | The Treatment and Prevention of Disease
58 of 123© 2020 Encyclopædia Britannica, Inc.
Vitamins
Because they can be stored in the liver and fatty tissue, fat-soluble vitamins, particularly vitamins A and D, have
more potential for toxicity than do water-soluble vitamins, which, with the exception of vitamin B , are readily 12
excreted in the urine if taken in excess. Nonetheless, water-soluble vitamins can be toxic if taken as
supplements or in fortified food.
Symptoms of acute vitamin A poisoning, which usually require a dose of at least 15,000 μg (50,000 IU) in adults,
include abdominal pain, nausea, vomiting, headache, dizziness, blurred vision, and lack of muscular
coordination. Chronic hypervitaminosis A, usually resulting from a sustained daily intake of 30,000 μg (100,000
IU) for months or years, may result in wide-ranging effects, including loss of bone density and liver damage.
Vitamin A toxicity in young infants may be seen in a swelling of the fontanelles (soft spots) due to increased
intracranial pressure. Large doses of vitamin A taken by a pregnant woman also can cause developmental
abnormalities in a fetus, especially if taken during the first trimester; the precise threshold for causing birth
defects is unknown, but less than 3,000 μg (10,000 IU) daily appears to be a safe intake. Although most vitamins
occurring naturally in food do not cause adverse effects, toxic levels of vitamin A may be found in the liver of
certain animals. For example, early Arctic explorers are reported to have been poisoned by eating polar bear
liver. High beta-carotene intake, from supplements or from carrots or other foods that are high in beta-carotene,
may after several weeks impart a yellowish cast to the skin but does not cause the same toxic effects as
preformed vitamin A.
High intake of vitamin D can lead to a variety of debilitating effects, notably calcification of soft tissues and
cardiovascular and renal damage. Although not a concern for most people, young children are especially
vulnerable to vitamin D toxicity. Individuals with high intakes of fortified milk or fish or those who take many
supplements may exceed the safe intake of 50 μg (2,000 IU) per day.
Because of its function as an antioxidant, supplementation with large doses (several hundred milligrams per
day) of vitamin E in hopes of protecting against heart disease and other chronic diseases has become
widespread. Such doses—many times the amount normally found in food—appear safe for most people, but their
effectiveness in preventing disease or slowing the aging process has not been demonstrated. Daily intakes
greater than 1,000 mg are not advised because they may interfere with blood clotting, causing hemorrhagic
effects.
Large doses of niacin (nicotinic acid), given for its cholesterol-lowering effect, may produce a reddening of the
skin, along with burning, tingling, and itching. Known as a “niacin flush,” this is the first indicator of niacin
excess, and this symptom is the basis for the safe daily intake of 35 mg. Liver toxicity and other adverse effects
have also been reported with several grams of niacin a day.
Large doses of vitamin B have been taken in hopes of treating conditions such as carpal tunnel syndrome and 6
premenstrual syndrome. The most critical adverse effect seen from such supplementation has been a severe
sensory neuropathy of the extremities, including inability to walk. A daily intake of up to 100 mg is considered
safe, although only 1 to 2 mg are required for good health.
Use of vitamin C supplements has been widespread since 1970, when chemist and Nobel laureate Linus Pauling
suggested that the vitamin was protective against the common cold. Some studies have found a moderate
benefit of vitamin C in reducing the duration and severity of common-cold episodes, but numerous studies have
failed to find a significant effect on incidence. The most common side effect of high vitamin C intake is diarrhea
and other gastrointestinal symptoms, likely due to the unabsorbed vitamin traversing the intestine. The safe

Britannica LaunchPacks | The Treatment and Prevention of Disease
59 of 123© 2020 Encyclopædia Britannica, Inc.
intake of 2,000 mg a day is based on the avoidance of these gastrointestinal symptoms. Although other possible
adverse effects of high vitamin C intake have been investigated, none has been demonstrated in healthy people.
Minerals
A desirable dietary intake of the minerals generally falls in a fairly narrow range. Because of interactions, a high
intake of one mineral may adversely affect the absorption or utilization of another. Excessive intake from food
alone is unlikely, but consumption of fortified foods or supplements increases the chance of toxicity.
Furthermore, environmental or occupational exposure to potentially toxic levels of minerals presents additional
risks for certain populations.
Widespread calcium supplementation, primarily by children who do not drink milk and by women hoping to
prevent osteoporosis, has raised concerns about possible adverse consequences of high calcium intake. A major
concern has been kidney stones (nephrolithiasis), the majority of which are composed of a calcium oxalate
compound. For years, a low-calcium diet was recommended for people at risk of developing kidney stones,
despite disappointing effectiveness and a fair amount of research challenging the approach. However, a recent
study has provided strong evidence that a diet relatively low in sodium and animal protein with normal amounts
of calcium (1,200 mg per day) is much more effective in preventing recurrent stone formation than was the
traditional low-calcium diet. In fact, dietary calcium may be protective against kidney stones because it helps
bind oxalate in the intestine. Constipation is a common side effect of high calcium intake, but daily consumption
of up to 2,500 mg is considered safe for adults and for children at least one year old.
The use of magnesium salts in medications, such as antacids and laxatives, may result in diarrhea, nausea, and
abdominal cramps. Impaired kidney function renders an individual more susceptible to magnesium toxicity.
Excess magnesium intake is unlikely from foods alone.
High-dose iron supplements, commonly used to treat iron deficiency anemia, may cause constipation and other
gastrointestinal effects. A daily iron intake of up to 45 mg presents a low risk of gastrointestinal distress. Acute
toxicity and death from ingestion of iron supplements is a major poisoning hazard for young children. In people
with the genetic disorder hereditary hemochromatosis, a disease characterized by the overabsorption of iron, or
in those who have repeated blood transfusions, iron can build up to dangerous levels, leading to severe organ
damage, particularly of the liver and heart. It is considered prudent for men and postmenopausal women to
avoid iron supplements and high iron intakes from fortified foods. Toxicity from dietary iron has been reported in
South Africa and Zimbabwe in people consuming a traditional beer with an extremely high iron content.
Excess zinc has been reported to cause gastrointestinal symptoms such as nausea and vomiting. Chronic intake
of large amounts of zinc may interfere with the body’s utilization of copper, impair immune response, and
reduce the level of high-density lipoprotein cholesterol (the so-called good cholesterol). A safe intake of 40 mg of
zinc daily is unlikely to be exceeded by food alone, although it may be exceeded by zinc lozenges or
supplements, which are widely used despite a lack of data about their safety or efficacy.
Selenium is toxic in large amounts. Selenosis (chronic selenium toxicity) results in symptoms such as
gastrointestinal and nervous system disturbances, brittleness and loss of hair and nails, a garliclike odour to the
breath, and skin rash. There also have been reports of acute toxicity and death from ingestion of gram quantities
of the mineral. Excess selenium can be harmful whether ingested as selenomethionine, the main form found in
food, or in the inorganic forms usually found in supplements. A daily intake of up to 400 μg from all sources most
likely poses no risk of selenium toxicity.
Impaired thyroid gland function, goitre, and other adverse effects may result from high intakes of iodine from
food, iodized salt, or pharmaceutical preparations intended to prevent or treat iodine deficiency or other
Britannica LaunchPacks | The Treatment and Prevention of Disease
60 of 123© 2020 Encyclopædia Britannica, Inc.
disorders. Although most people are unlikely to exceed safe levels, individuals with certain conditions, such as
autoimmune thyroid disease, are particularly sensitive to excess iodine intake.
While the teeth are developing and before they erupt, excess fluoride ingestion can cause mottled tooth enamel;
however, this is only a cosmetic effect. In adults, excess fluoride intake is associated with effects ranging from
increased bone mass to joint pain and stiffness and, in extreme cases, crippling skeletal fluorosis. Even in
communities where water supplies naturally provide fluoride levels several times higher than recommended,
skeletal fluorosis is extremely rare.
High intakes of phosphorus (as phosphate) may affect calcium metabolism adversely and interfere with the
absorption of trace elements such as iron, copper, and zinc. However, even with the consumption of phosphate
additives in a variety of foods and in cola beverages, exceeding safe levels is unlikely. Manganese toxicity, with
central nervous system damage and symptoms similar to Parkinson disease, is a well-known occupational
hazard of inhaling manganese dust, but again, it is not likely to come from the diet. Similarly, copper toxicity is
unlikely to result from excessive dietary intake, except in individuals with hereditary or acquired disorders of
copper metabolism.
Alcohol
The acute effects of a large intake of alcohol are well known. Mental impairment starts when the blood
concentration is about 0.05 percent. A concentration of alcohol in the blood of 0.40 percent usually causes
unconsciousness, and 0.50 percent can be fatal. Accidents and violence, which are often alcohol-related, are
major causes of death for young persons. Women who drink during pregnancy risk physical and mental damage
to their babies (fetal alcohol syndrome). Alcohol also can interact dangerously with a variety of medications,
such as tranquilizers, antidepressants, and pain relievers.
Although numerous studies have confirmed that light to moderate drinkers have less heart disease and tend to
live longer than either nondrinkers or heavy drinkers, increasing chronic alcohol consumption carries with it
significant risks as well: liver disease; pancreatitis; suicide; hemorrhagic stroke; mouth, esophageal, liver, and
colorectal cancers; and probably breast cancer. In alcoholics, nutritional impairment may result from the
displacement of nutrient-rich food as well as from complications of gastrointestinal dysfunction and widespread
metabolic alterations. Thiamin deficiency, as seen in the neurological condition known as Wernicke-Korsakoff
syndrome, is a hallmark of alcoholism and requires urgent treatment.
Diet and chronic diseaseThe relationship between diet and chronic disease (i.e., a disease that progresses over an extended period and
does not resolve spontaneously) is complicated, not only because many diseases take years to develop but also
because identifying a specific dietary cause is extremely difficult. Some prospective epidemiologic studies
attempt to overcome this difficulty by following subjects for a number of years. Even then, the sheer complexity
of the diet, as well as the multifactorial origins of chronic diseases, makes it difficult to prove causal links.
Furthermore, many substances in food appear to act in a synergistic fashion—in the context of the whole diet
rather than as individual agents—and single-agent studies may miss these interactive effects.
The concept of “risk factors” has been part of the public vocabulary for several decades, ever since the
landmark Framingham Heart Study, begun in 1948, first reported in the early 1960s that cigarette smoking,
elevated blood cholesterol, and high blood pressure were predictors of one’s likelihood of dying from heart
disease. Other studies confirmed and further elucidated these findings, and an extensive body of research has
since shown that particular conditions or behaviours are strongly associated with specific diseases. Not all
Britannica LaunchPacks | The Treatment and Prevention of Disease
61 of 123© 2020 Encyclopædia Britannica, Inc.
individuals with a risk factor eventually develop a particular disease; however, the chance of developing the
disease is greater when a known risk factor is present and increases further when several risk factors are
present. Certain risk factors—such as diet, physical activity, and use of tobacco, alcohol, and other drugs—are
modifiable, although it is often difficult to effect such change, even if one is facing possible disability or
premature death. Others, including heredity, age, and sex, are not. Some risk factors are modifiable to varying
degrees; these include exposure to sunlight and other forms of radiation, biological agents, and chemical agents
(e.g., air and water pollution) that may play a role in causing genetic mutations that have been associated with
increased risk of certain diseases, particularly cancer.
Cardiovascular disease
Cardiovascular disease, a general term that encompasses diseases of the heart and blood vessels, is the leading
cause of death in developed countries. Coronary heart disease (CHD), also known as coronary artery disease or
ischemic heart disease, is the most common—and the most deadly—form of cardiovascular disease. CHD occurs
when the arteries carrying blood to the heart, and thereby oxygen and nutrients, become narrow and
obstructed. This narrowing is usually the result of atherosclerosis, a condition in which fibrous plaques (deposits
of lipid and other material) build up on the inner walls of arteries, making them stiff and less responsive to
changes in blood pressure. If blood flow is interrupted in the coronary arteries surrounding the heart, a
myocardial infarction (heart attack) may occur. Restriction of blood flow to the brain due to a blood clot or
hemorrhage may lead to a cerebrovascular accident, or stroke, and narrowing in the abdominal aorta, its major
branches, or arteries of the legs may result in peripheral arterial disease. Most heart attacks and strokes are
caused not by total blockage of the arteries by plaque but by blood clots that form more readily where small
plaques are already partially blocking the arteries.
Although atherosclerosis typically takes decades to manifest in a heart attack or stroke, the disease may
actually begin in childhood, with the appearance of fatty streaks, precursors to plaque. The deposition of plaque
is, in essence, an inflammatory response directed at repairing injuries in the arterial wall. Smoking,
hypertension, diabetes, and high blood levels of low-density lipoprotein (LDL) cholesterol are among the many
factors associated with vessel injury. Infection by certain bacteria or viruses may also contribute to inflammation
and vessel damage. Particularly vulnerable to premature CHD are middle-aged men, especially those with a
family history of the disease, and individuals with hereditary conditions such as familial hypercholesterolemias.
Diet and weight loss are influential in modifying four major risk factors for CHD: high levels of LDL cholesterol,
low levels of high-density lipoprotein (HDL) cholesterol, hypertension, and diabetes. However, the role of diet in
influencing the established risk factors is not as clear as the role of the risk factors themselves in CHD.
Furthermore, dietary strategies are most useful when combined with other approaches, such as smoking
cessation and regular exercise. Drug therapy may include cholesterol-lowering drugs such as statins, bile acid
sequestrants, and niacin, as well as aspirin or anticoagulants to prevent formation of blood clots and
antihypertensive medication to lower blood pressure. Although endogenous estrogen (that produced by the
body) is thought to confer protection against CHD in premenopausal women, recent studies call into question the
value of hormone therapy in reducing CHD risk in women who have gone through menopause.
Blood lipoproteins
Because lipids such as cholesterol, triglycerides, and phospholipids are nonpolar and insoluble in water, they
must be bound to proteins, forming complex particles called lipoproteins, to be transported in the watery
medium of blood. Low-density lipoproteins, which are the main transporters of cholesterol in the blood, carry
cholesterol from the liver to body cells, including those in the arteries, where it can contribute to plaque. Multiple
lines of evidence point to high levels of LDL cholesterol as causal in the development of CHD, and LDL is the
Britannica LaunchPacks | The Treatment and Prevention of Disease
62 of 123© 2020 Encyclopædia Britannica, Inc.
main blood lipoprotein targeted by intervention efforts. Furthermore, clinical trials have demonstrated that LDL-
lowering therapy reduces heart attacks and strokes in people who already have CHD.
High-density lipoproteins, on the other hand, are thought to transport excess cholesterol to the liver for removal,
thereby helping to prevent plaque formation. HDL cholesterol is inversely correlated with CHD risk; therefore
intervention efforts aim to increase HDL cholesterol levels. Another blood lipoprotein form, the very-low-density
lipoprotein (VLDL), is also an independent CHD risk factor, but to a lesser extent than LDL and HDL. As the major
carrier of triglyceride (fat) in the blood, VLDL is particularly elevated in people who are overweight and in those
with diabetes and metabolic syndrome.
Although LDL cholesterol is popularly referred to as “bad” cholesterol and HDL cholesterol is often called “good”
cholesterol, it is actually the lipoprotein form—not the cholesterol being carried in the lipoprotein—that is related
to CHD risk. Total cholesterol levels, which are highly correlated with LDL cholesterol levels, are typically used
for initial screening purposes, although a complete lipoprotein evaluation is more revealing. A desirable blood
lipid profile is a total cholesterol level below 200 milligrams per decilitre (mg/dl), an HDL cholesterol level of at
least 40 mg/dl, a fasting triglyceride level of less than 150 mg/dl, and an LDL cholesterol level below 100, 130, or
160 mg/dl, depending on degree of heart attack risk.
Dietary fat
Learn about researchers using olive oil to create healthier hot dogs.
© American Chemical Society
It is widely accepted that a low-fat diet lowers blood cholesterol and is protective against heart disease. Also, a
high-fat intake is often, although not always, linked to obesity, which in turn can increase heart disease risk. Yet,
the situation is complicated by the fact that different fatty acids have differing effects on the various lipoproteins
that carry cholesterol. Furthermore, when certain fats are lowered in the diet, they may be replaced by other
components that carry risk. High-carbohydrate diets, for example, may actually increase cardiovascular risk for
some individuals, such as those prone to metabolic syndrome or type 2 diabetes. Heredity also plays a role in an
individual’s response to particular dietary manipulations.
Overview of saturated and polyunsaturated fats.

Britannica LaunchPacks | The Treatment and Prevention of Disease
63 of 123© 2020 Encyclopædia Britannica, Inc.
Contunico © ZDF Enterprises GmbH, Mainz
In general, saturated fatty acids, which are found primarily in animal foods, tend to elevate LDL and total blood
cholesterol. However, the most cholesterol-raising saturated fatty acids (lauric, myristic, and palmitic acids) can
come from both plant and animal sources, while stearic acid, derived from animal fat as well as from cocoa
butter, is considered neutral, neither raising nor lowering blood cholesterol levels.
When saturated fatty acids are replaced by unsaturated fatty acids—either monounsaturated or
polyunsaturated—LDL and total blood cholesterol are usually lowered, an effect largely attributed to the
reduction in saturated fat. However, polyunsaturated fatty acids tend to lower HDL cholesterol levels, while
monounsaturated fatty acids tend to maintain them. The major monounsaturated fatty acid in animals and
plants is oleic acid; good dietary sources are olive, canola, and high-oleic safflower oils, as well as avocados,
nuts, and seeds. Historically, the low mortality from CHD in populations eating a traditional Mediterranean diet
has been linked to the high consumption of olive oil in the region, although the plentiful supply of fruits and
vegetables could also be a factor. Olive oil consumption is also associated with decreased levels of amyloid-beta
plaque formation and a reduction of inflammation in the brain; such plaques and inflammation are indicative of
Alzheimer disease. Studies in animals suggest that a diet rich in olive oil helps preserve memory and learning
ability.
The two types of polyunsaturated fatty acids found in foods are omega-3 fatty acids and omega-6 fatty acids.
Linoleic acid, the primary omega-6 fatty acid in most diets, is widespread in foods; the major source is vegetable
oils such as sunflower, safflower, and corn oils. Low cardiovascular disease rates in Eskimo populations eating
traditional diets high in omega-3 fatty acids initially provoked the speculation that these fatty acids may be
protective against CHD. The primary lipid-altering effect of omega-3 fatty acids is the reduction of blood
triglycerides. Omega-3 fatty acids may also protect the heart and blood vessels by lowering blood pressure,
reducing blood clotting, preventing irregular heart rhythms, and acting as anti-inflammatory agents. The long-
chain omega-3 fatty acids eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) are derived from alpha-
linolenic acid, a shorter-chain member of the same family. Fatty fish such as salmon, herring, sardines,
mackerel, and tuna are high in both EPA and DHA. Flaxseed is an excellent source of alpha-linolenic acid, which
the body can convert to the long-chain omega-3 fatty acids. Other sources of omega-3 fatty acids include
walnuts, hazelnuts, almonds, canola oil, soybean oil, dark green leafy vegetables such as spinach, and egg yolk.
A diet high in polyunsaturated fatty acids may increase LDL lipid oxidation and thereby accelerate
atherosclerosis; therefore, it should be accompanied by increased intakes of vitamin E, an antioxidant. Fish oil
supplements are not advised without medical supervision because of possible adverse effects, such as bleeding.
The safety of (as opposed to naturally occurring ) unsaturated fatty acids has been called into question trans cisbecause -fatty acids in the diet raise LDL cholesterol to about the same extent as do saturated fatty acids, transand they can also lower HDL cholesterol. -fatty acids are found naturally in some animal fats, such as beef, Transbutter, and milk, but they are also produced during the hydrogenation process, in which unsaturated oils are
made harder and more stable. Certain margarines, snack foods, baked goods, and deep-fried products are major
food sources of -fatty acids.trans
Dietary cholesterol
Cholesterol in food and cholesterol in the blood are distinct entities, and they are often confused. Dietary
cholesterol is found only in foods of animal origin, and it is particularly high in egg yolk and organ meats.
Cholesterol in the diet raises LDL cholesterol but not as much as saturated fatty acids do. If dietary cholesterol is
already high, consuming even more cholesterol may not increase blood cholesterol levels further because of
feedback control mechanisms. Also, there is great individual variation in response to dietary cholesterol. For
Britannica LaunchPacks | The Treatment and Prevention of Disease
64 of 123© 2020 Encyclopædia Britannica, Inc.
healthy people, a cholesterol intake averaging less than 300 mg daily is recommended; however, because
cholesterol is synthesized by the body, none is required in the diet.
Other dietary factors
Ingestion of soluble fibre, a component of dietary fibre (indigestible plant material), lowers LDL and total blood
cholesterol levels and has been linked to decreased mortality from cardiovascular disease. Sources of soluble
fibre include whole oats, barley, legumes, some vegetables, and fruits, particularly apples, plums, apricots,
blueberries, strawberries, and citrus fruits; psyllium and other fibre supplements may also be recommended. The
mechanism whereby soluble fibre lowers cholesterol levels is unclear, although it is probably related to its ability
to bind with cholesterol and bile acids in the gut, thereby removing them from circulation. Other factors may
contribute as well, such as fermentation of fibre by bacteria in the colon, resulting in compounds that inhibit
cholesterol synthesis.
Light to moderate alcohol intake (up to two drinks per day for men and one drink per day for women) is
associated with reduced CHD risk, primarily because of its ability to raise HDL cholesterol levels and possibly
because it helps prevent blood clot formation. Alcohol intake may help explain the so-called French paradox:
heart disease rates in France are low despite a CHD risk profile comparable to that in the United States, where
rates are relatively high. Wine also contains antioxidant compounds, such as resveratrol from grape skins, that
may inhibit LDL oxidation, but the beneficial effect of these substances is likely far less than that of alcohol itself.
Mortality from stroke and heart disease is significantly associated with dietary sodium (salt) intake, but only in
overweight individuals, who may have an increased sensitivity to dietary sodium. Sodium intake also appears to
have a direct effect on risk of stroke beyond its effect on blood pressure, which itself influences stroke risk. On
the other hand, diets rich in potassium are linked to reduced risk of stroke.
Soy foods are associated with decreased LDL and total blood cholesterol levels, as well as other vascular effects
associated with reduced CHD risk. Tofu, tempeh, miso, soy flour, soy milk, and soy nuts are among the soy foods
that contain isoflavones, estrogen-like compounds that are thought to be responsible for these beneficial
cardiovascular effects.
Antioxidant substances found in food and taken as dietary supplements include vitamin C, vitamin E, and beta-
carotene (a plant precursor to vitamin A). Dietary antioxidants may lower CHD risk, although clinical trials have
not yet supported this notion.
Other factors
For blood pressure that is equal to or greater than the “prehypertension” level of 120/80 millimetres of mercury
(mm Hg), the more elevated the blood pressure, the greater the risk of heart disease. Hypertension (140/90 mm
Hg and above) and atherosclerosis are mutually reinforcing: hypertension injures artery walls, thereby
encouraging plaque formation; and once plaque has formed and arteries are less elastic, hypertension is
aggravated. If hypertension is treated, the incidence of CHD, stroke, and congestive heart failure decreases.
Diabetes—often accompanied by hypertension, high blood triglyceride levels, and obesity—is an important risk
factor for heart disease and also warrants aggressive intervention. Furthermore, for people with diabetes who
have a heart attack, there is an unusually high death rate, immediately or in the ensuing years. If blood glucose
levels are strictly controlled, vascular complications will be decreased.
Obesity is also an important factor in cardiovascular disease, primarily through its influence on other
simultaneously present risk factors. Obese individuals often have an abnormal glucose tolerance and diabetes,
hypertension, and blood lipoprotein abnormalities, including higher triglyceride levels and lower HDL cholesterol
Britannica LaunchPacks | The Treatment and Prevention of Disease
65 of 123© 2020 Encyclopædia Britannica, Inc.
levels. Fat accumulation around the waist (the so-called apple shape) puts one at greater risk for premature
heart disease than does fat accumulation around the hips (pear shape). A waist circumference greater than 102
cm (40 inches) for men or 88 cm (35 inches) for women is considered a high risk. Besides helping to control
weight, regular exercise is thought to decrease CHD risk in several ways: slowing the progression of
atherosclerosis, increasing the blood supply to the heart muscle, increasing HDL cholesterol, reducing VLDL
levels, improving glucose tolerance, and reducing blood pressure. At a minimum, 30 minutes of moderate
aerobic activity, such as brisk walking, on most days is recommended.
A newly described constellation of CHD risk factors called metabolic syndrome is marked by abdominal obesity,
low HDL cholesterol, elevated blood triglycerides, high blood pressure, and insulin resistance. First named
Syndrome X in 1988 by American endocrinologist Gerald Reaven, this condition is exacerbated when susceptible
people eat high-carbohydrate diets. Individuals with metabolic syndrome benefit from regular physical activity
and weight reduction, along with a diet lower in carbohydrates and saturated fat and higher in unsaturated fat.
Individuals with the genetic disease hereditary hemochromatosis excessively absorb iron, which can build up to
dangerously high levels and damage the heart, liver, and other organs. Approximately 1 in 9 people of European
descent are carriers (i.e., have one of two possible genes) for the disease and have an increased risk of heart
disease. However, studies examining the possible role of dietary iron in heart disease risk for those who lack the
gene for hemochromatosis have been inconclusive.
The amino acid homocysteine, when present in elevated amounts in blood, may damage arteries and promote
atherosclerosis. Inadequate intake of vitamin B , vitamin B , or folic acid can increase blood homocysteine 6 12
levels, although folic acid deficiency is the most common cause. While elevated homocysteine is not yet an
established risk factor for CHD, it is prudent to ensure adequate intake of folic acid.
Dietary recommendations
Although plaque formation starts in childhood, infants or children under two years of age should not have any
dietary restriction placed on cholesterol and fat. After age two, dietary recommendations to reduce CHD risk
generally focus on controlling intake of total fat, saturated and -fatty acids, and dietary cholesterol, transcombined with physical activity and weight management. Since atherosclerosis is so common, such diets are
considered useful not only for the general public but also for people with high LDL cholesterol or other CHD risk
factors. A preventive diet for adults might include 20 to 35 percent of kilocalories as dietary fat, with low intake
of saturated and -fatty acids (no more than 10 percent of kilocalories), and cholesterol intake below 300 mg transdaily. A therapeutic diet, which should be managed by a registered dietitian or other qualified nutrition
professional, is even more restrictive. Practical suggestions include reducing intake of fatty spreads, organ
meats, fatty meats, egg yolks, full-fat dairy products, baked goods and fried foods; removing skin from poultry;
and carefully reading food labels to reduce hidden fats in processed foods. An emphasis on oats and other whole
grains, vegetables, and fruits—with the inclusion of nonfat or low-fat dairy products, fish, legumes, poultry, and
lean meats—is likely to benefit not only cardiovascular health but also overall health.
Hypertension
Hypertension, or high blood pressure, is one of the most common health problems in developed countries. It is
an important risk factor for other diseases, such as coronary heart disease, congestive heart failure, stroke,
aneurysm, and kidney disease. Most people with high blood pressure have essential, or primary, hypertension,
for which no specific cause can be determined. Heredity plays a role in the development of the disease, but so
do modifiable factors such as excess weight, physical inactivity, high alcohol intake, and diets high in salt. For
reasons that are not entirely clear, African Americans have among the highest rates of hypertension in the world.
Britannica LaunchPacks | The Treatment and Prevention of Disease
66 of 123© 2020 Encyclopædia Britannica, Inc.
Hypertension is usually defined as a blood pressure equal to or greater than 140/90 mm Hg, i.e., equivalent to
the pressure exerted by a column of mercury 140 mm high during contraction of the heart (systole) and 90 mm
high during relaxation (diastole); either systolic or diastolic blood pressure, or both, may be elevated in
hypertension. Individuals with hypertension can be asymptomatic for years and then suddenly experience a fatal
stroke or heart attack. Prevention and management of hypertension can significantly decrease the chance of
complications. Early identification of hypertension is important so that lifestyle modification can begin as early
as possible.
Overweight people, especially those with excess abdominal fat, have a much greater risk of developing
hypertension than do lean people. Weight loss alone, sometimes as little as 4.5 kg (10 pounds), can be
extremely effective in reducing high blood pressure. Increasing physical activity can, of course, help with weight
control, but it also appears to lower blood pressure independently.
Large studies examining salt intake and blood pressure in communities around the world have clearly
established that blood pressure is positively related to dietary intake of sodium (salt). Primitive societies in which
sodium intake is low have very little hypertension, and the increase in blood pressure that typically occurs with
age in industrialized societies fails to occur. On the other hand, in countries with extremely high salt
consumption, hypertension is common and stroke is a leading cause of death. Furthermore, experimental
studies indicate that decreasing sodium intake can reduce blood pressure.
Some people appear to be genetically sensitive to salt. Although salt restriction may only help lower blood
pressure in those who are salt sensitive, many individuals consume more salt than is needed. Dietary
recommendations typically encourage the general population to limit sodium intake to no more than 2,400 mg
daily, which amounts to a little more than a teaspoon of salt. This level can be achieved by restricting salt used
in cooking, not adding salt at the table, and limiting highly salted foods, processed foods (many of which have
hidden sodium), and so-called fast foods. Canned vegetables, breakfast cereals, and luncheon meats are
particularly high in sodium.
Heavy alcohol consumption (more than two drinks a day) is associated with hypertension. Vegetarians, and
particularly vegans (who consume no foods of animal origin, including milk and eggs) tend to have lower blood
pressure than do meat eaters. The diet recommended for reducing blood pressure, which will also benefit
cardiovascular health, emphasizes fruits, vegetables, and low-fat dairy products; includes whole grains, poultry,
fish, and nuts; and contains only small amounts of red meat and sugary foods and beverages. Reducing salt
intake should further increase the effectiveness of the diet.
A variety of drugs is used to treat hypertension, some of which have nutritional repercussions. Thiazide diuretics,
for example, increase potassium loss from the body, usually necessitating the intake of additional potassium,
which is particularly plentiful in foods such as bananas, citrus fruits, vegetables, and potatoes. Use of potassium-
based salt substitutes is not advised without medical supervision.
Cancer
Second only to cardiovascular disease as a cause of death in much of the world, cancer is a major killer of adults
ages 45 and older. The various types of cancer differ not only in location in the body and affected cell type but
also in the course of the disease, treatments, and suspected causal or contributory factors.
Studies of identical twins reveal that, even for those with an identical genetic makeup, the risk for most cancers
is still largely related to environmental factors. Another line of evidence supporting the limited role of heredity in
most cancers is studies of migrant populations, in which cancer rates tend to grow more like a group’s adopted
country with each passing generation. For example, rates of breast and colorectal cancers in individuals who
Britannica LaunchPacks | The Treatment and Prevention of Disease
67 of 123© 2020 Encyclopædia Britannica, Inc.
migrate from rural Asia to the United States gradually increase to match the higher cancer rates of the United
States. On the other hand, risk of stomach cancer gradually decreases after Japanese migrants move to the
United States. Nutrition is among the critical environmental and lifestyle factors investigated in migration
studies, although identifying specific dietary components that affect the changing disease rates has been more
elusive. A number of cancer organizations around the world have estimated that 30 to 40 percent of all cases of
cancer could be prevented by appropriate dietary means.
Most cancer-causing substances (carcinogens) probably enter the body through the alimentary canal in food and
beverages. Although some foodborne toxins, pesticides, and food additives may be carcinogenic if taken in
sufficient quantity, it is primarily the foodstuffs themselves that are associated with cancer. Some dietary
patterns or components may promote cancer, while others may inhibit it.
Substances in the diet, or other environmental factors, can act anywhere along the multistage process of cancer
development (carcinogenesis): initiation, in which DNA, the genetic material in a cell, is altered; promotion, in
which cells with altered DNA multiply; and progression, in which cancer cells spread to surrounding tissue and
distant sites (metastasis).
Studies attempting to relate total fat or specific types of fat to various cancers have been inconsistent. High
intake of dietary fat may promote cancer, but this could be due at least in part to the extra energy (calories) that
fat provides. Obesity is associated with several types of cancer, including colorectal, prostate, uterine,
pancreatic, and breast cancers. A possible mechanism for this effect is the higher circulating levels of estrogen,
insulin, and other hormones that accompany increased body fat. Furthermore, regular exercise has been shown
in a number of studies to reduce the risk of breast and colon cancers. In laboratory animals, restricting energy
intake is the most effective method for reducing cancer risk; chronic underfeeding inhibits the growth of many
spontaneous tumours and most experimentally induced tumours.
High alcohol consumption is another factor that has been implicated in the development of various cancers,
especially of the mouth, throat, liver, and esophagus (where it acts synergistically with tobacco) and probably of
the breast, colon, and rectum. The fact that moderate use of alcohol has a beneficial effect on cardiovascular
disease underscores how complex and potentially confusing is the connection between food and health.
Foods also contain substances that offer some protection against cancer. For example, fresh fruits and
vegetables, and specifically vitamins C and E, eaten at the same time as nitrate-containing foods (such as ham,
bacon, sausages, frankfurters, and luncheon meats), inhibit nitrosamine production and thus help protect
against stomach cancer. Several hundred studies have found a strong association between diets high in
vegetables and fruits and lower risk for various cancers, although identifying specific protective factors in such
diets has been more difficult. Vitamin C, vitamin E, carotenoids such as beta-carotene (a plant precursor of
vitamin A), and the trace mineral selenium act in the body’s antioxidant systems to help prevent DNA damage
by reactive molecules known as free radicals. Specific vegetables, notably the cruciferous vegetables (broccoli,
cauliflower, Brussels sprouts, kale, and other members of the cabbage family), contain sulforaphane and other
compounds known as isothiocyanates, which induce enzymes that detoxify carcinogens and have been
demonstrated to protect against cancer in animal studies. Dietary fibre in plant foods may also be protective: it
dilutes potential carcinogens, binds to them, and speeds up transit time through the gut, thereby limiting
exposure. Fruits and vegetables are rich in phytochemicals (biologically active plant substances), which are
currently being investigated for potential anticarcinogenic activity. Animal studies suggest that antioxidant
compounds known as polyphenols, which are found in both black and green tea, may be protective against the
growth of cancer. Regular consumption of tea, especially in Japan and China, where green tea is the preferred
type, has been associated with a decreased risk of various cancers, especially stomach cancer, but the evidence
has been conflicting.

Britannica LaunchPacks | The Treatment and Prevention of Disease
68 of 123© 2020 Encyclopædia Britannica, Inc.
The dietary approach most likely to reduce cancer risk is one that is rich in foods from plant sources, such as
fruits, vegetables (especially cruciferous ones), whole grains, beans, and nuts; has a limited intake of fat,
especially animal fat; includes a balance of energy intake and physical activity to maintain a healthy body
weight; and includes alcohol in moderation, if at all. Intake of carcinogenic compounds can also be reduced by
trimming fat and removing burned portions from meat before eating.
Colorectal cancer
Consumption of meat, particularly red meat and processed meat, is associated with a modest increase in risk of
colorectal cancer. However, it is unclear whether this effect is related to a specific component of meat; to the
fact that other nutrients, such as fibre, may be in short supply in a high-meat diet; or to carcinogenic
substances, such as heterocyclic amines and polycyclic aromatic hydrocarbons, which are produced during high-
temperature grilling and broiling, particularly of fatty muscle meats. High alcohol consumption and low intakes
of calcium and folic acid have also been linked to an increased rate of colorectal cancer.
Although fibre-rich foods also appear to be protective against colorectal cancer in many studies, attempts to
demonstrate a specific protective effect of dietary fibre, distinct from the nonfibre constituents of vegetables
and fruits, have been inconclusive. Obesity is an important risk factor for colorectal cancer in men and
premenopausal women, and mild or moderate physical activity is strongly associated with a decreased risk of
colon cancer.
Prostate cancer
There is a growing body of evidence that a diet low in fat and animal products and rich in fruits and vegetables,
including the cruciferous type, is protective against prostate cancer. This protection may be partially explained
by a fibre found in fruits and vegetables called pectin, which has been shown to possess anticancer properties.
Lower prostate cancer risk has been associated with the consumption of tomatoes and tomato products, which
are rich sources of the carotenoid antioxidant lycopene. Prostate cancer rates are low in countries such as Japan
where soy foods are consumed regularly, but there is no direct evidence that soy protects against the disease.
The possible protective effect against prostate cancer of vitamin E and the mineral selenium is under
investigation.
Breast cancer
The relationship between diet and breast cancer is unclear. High-fat diets have been suspected of contributing to
breast cancer, based on international correlations between fat intake and breast cancer rates, as well as animal
studies. However, large prospective studies have not confirmed this connection, even though a diet high in fat
may be inadvisable for other reasons. Similarly, a diet high in fruits and vegetables is certainly healthful but
provides no known protection against breast cancer. Alcohol intake is associated with breast cancer, but the
increased risk appears related only to heavy drinking. Lifelong regular exercise may be protective against breast
cancer, possibly because it helps to control weight, and obesity is associated with increased risk of
postmenopausal breast cancer. Heredity and levels of estrogen over the course of a lifetime are the primary
established influences on breast cancer risk.
Enthusiasm for soy foods and soy products as protection against breast cancer has been growing in recent years
in the industrialized world. Although Japanese women, who have low breast cancer rates, have a lifelong
exposure to high dietary soy, their situation is not necessarily comparable to midlife supplementation with soy
isoflavones (estrogen-like compounds) in Western women. Isoflavones appear to compete with estrogen (e.g., in
premenopausal women), and thereby blunt its effect; when in a low-estrogen environment (e.g., in
postmenopausal women) they exert weak estrogenic effects. There is as yet no consistent evidence that soy in

Britannica LaunchPacks | The Treatment and Prevention of Disease
69 of 123© 2020 Encyclopædia Britannica, Inc.
the diet offers protection against breast cancer or any other cancer; and the effects of dietary soy once cancer
has been initiated are unknown (estrogen itself is a cancer promoter). Ongoing research on the benefits of soy is
promising, and consumption of soy foods such as tofu is encouraged, but consumption of isolated soy
constituents such as isoflavones, which have unknown risks, is not warranted.
Diabetes mellitus and metabolic disorders
Diabetes mellitus is a group of metabolic disorders of carbohydrate metabolism characterized by high blood
glucose levels (hyperglycemia) and usually resulting from insufficient production of the hormone insulin (type 1
diabetes) or an ineffective response of cells to insulin (type 2 diabetes). Secreted by the pancreas, insulin is
required to transport blood glucose (sugar) into cells. Diabetes is an important risk factor for cardiovascular
disease, as well as a leading cause of adult blindness. Other long-term complications include kidney failure,
nerve damage, and lower limb amputation due to impaired circulation.
Type 1 diabetes (formerly known as juvenile-onset or insulin-dependent diabetes) can occur at any age but often
begins in late childhood with the pancreas failing to secrete adequate amounts of insulin. Type 1 diabetes has a
strong genetic link, but most cases are the result of an autoimmune disorder, possibly set off by a viral infection,
foreign protein, or environmental toxin. Although elevated blood sugar is an important feature of diabetes, sugar
or carbohydrate in the diet is not the cause of the disease. Type 1 diabetes is managed by injections of insulin,
along with small, regularly spaced meals and snacks that spread glucose intake throughout the day and
minimize fluctuations in blood glucose.
Type 2 diabetes (formerly known as adult-onset or non-insulin-dependent diabetes) is the more common type of
diabetes, constituting 90 to 95 percent of cases. With this condition, insulin resistance renders cells unable to
admit glucose, which then accumulates in the blood. Although type 2 diabetes generally starts in middle age, it
is increasingly reported in childhood, especially in obese children. Genetic susceptibility to this form of diabetes
may not be expressed unless a person has excess body fat, especially abdominal obesity. Weight loss often
helps to normalize blood glucose regulation, and oral antidiabetic agents may also be used. Lifestyle
intervention (e.g., diet and exercise) is highly effective in delaying or preventing type 2 diabetes in high-risk
individuals.
Migration studies have shown that urbanization and adoption of a Western diet and habits can dramatically
increase the rate of type 2 diabetes. For example, a high prevalence of the disorder is seen in the Pima Indians
of Arizona, who are sedentary and eat a high-fat diet, whereas prevalence is low in a closely related group of
Pimas living a traditional lifestyle—physically active, with lower body weight and a diet that is lower in fat—in a
remote, mountainous region of Mexico. Type 2 diabetes is a serious health problem among Native Americans
and other ethnic minorities in the United States. Worldwide, the prevalence of type 2 diabetes has increased
sharply, along with the rise in obesity.
Specific treatment plans for diabetics are designed after individual medical assessment and consultation with a
registered dietitian or qualified nutrition professional. The therapeutic diet, which has changed considerably over
the years, focuses on complex carbohydrates, dietary fibre (particularly the soluble type), and regulated
proportions of carbohydrate, protein, and fat. Because heart disease is the leading cause of death among
diabetics, saturated fatty acids and -fatty acids are also restricted, and physical activity and weight control transare strongly encouraged. Older dietary recommendations restricted sugar in the diabetic diet, but recent
guidelines allow a moderate intake of sugars, so long as other carbohydrates are reduced in the same meal. Diet
and exercise are also used to manage a condition known as gestational diabetes, which develops in a small
percentage of pregnant women and usually resolves itself after delivery, though such women are subsequently
at increased risk of developing type 2 diabetes.
Britannica LaunchPacks | The Treatment and Prevention of Disease
70 of 123© 2020 Encyclopædia Britannica, Inc.
Research in the 1990s led to the development of a new tool, the glycemic index, which reflects the finding that
different carbohydrate foods have effects on blood glucose levels that cannot be predicted on the basis of their
chemical structure. For example, the simple sugars formed from digestion of some starchy foods, such as bread
or potatoes, are absorbed more quickly and cause a faster rise in blood glucose than does table sugar (sucrose),
fruit, or milk. In practical terms, however, if a carbohydrate food is eaten as part of a mixed meal, its so-called
glycemic effect is less consequential. The glycemic index may prove to be a useful option for planning diabetic
diets, but it in no way obviates the need for other established therapeutic practices, such as limiting total
carbohydrate intake and managing body weight.
The trace element chromium is a cofactor for insulin and is important for glucose tolerance. Malnourished infants
with impaired glucose tolerance have been shown to benefit from additional chromium, but there is no evidence
that most people with diabetes are deficient in chromium or in need of chromium supplementation.
If a diabetic injects too much insulin, blood glucose may drop to dangerously low levels; the irritability,
shakiness, sweating, headache, and confusion that ensue are indicative of low blood sugar, known as
hypoglycemia. Severe hypoglycemia, if untreated, can lead to seizures, coma, and even death. Reactive
hypoglycemia of nondiabetic origin is a distinct disorder of carbohydrate metabolism in which blood glucose falls
unduly (below 50 mg/dl) after an overproduction of the body’s own insulin in response to a meal high in simple
sugars; symptoms of hypoglycemia occur simultaneously. However, this condition is uncommon.
Numerous inherited metabolic disorders, also known as inborn errors of metabolism, respond to dietary
treatment. Most of these relatively rare disorders are inherited as autosomal recessive traits (i.e., both parents
must be carriers) and result in a specific enzyme or cofactor that has reduced activity or is absent altogether.
Biochemical pathways of amino acid, carbohydrate, or fatty acid metabolism may be affected, each having a
number of possible enzyme defects. In some cases, newborn screening programs, and even prenatal diagnosis,
allow for early identification and successful intervention. Without prompt and aggressive treatment, most of
these disorders have a poor prognosis, resulting in severe intellectual disability and other forms of illness.
Phenylketonuria (PKU), a condition in which the amino acid phenylalanine is not properly metabolized to the
amino acid tyrosine, is the most recognized of these disorders. Treatment involves lifelong restriction of
phenylalanine in the diet and supplementation with tyrosine. With early detection and meticulous management,
normal growth and intellectual functioning are possible.
Obesity and weight control
The discovery of the leptin protein in mice and its connection to diabetes and obesity.
HudsonAlpha Institute for Biotechnology
The World Health Organization (WHO) has recognized obesity as a worldwide epidemic affecting more than 500
million adults and paradoxically coexisting with undernutrition in both developing and industrialized countries.
There also have been reports of an alarming increase in childhood obesity worldwide. Obesity (excess body fat
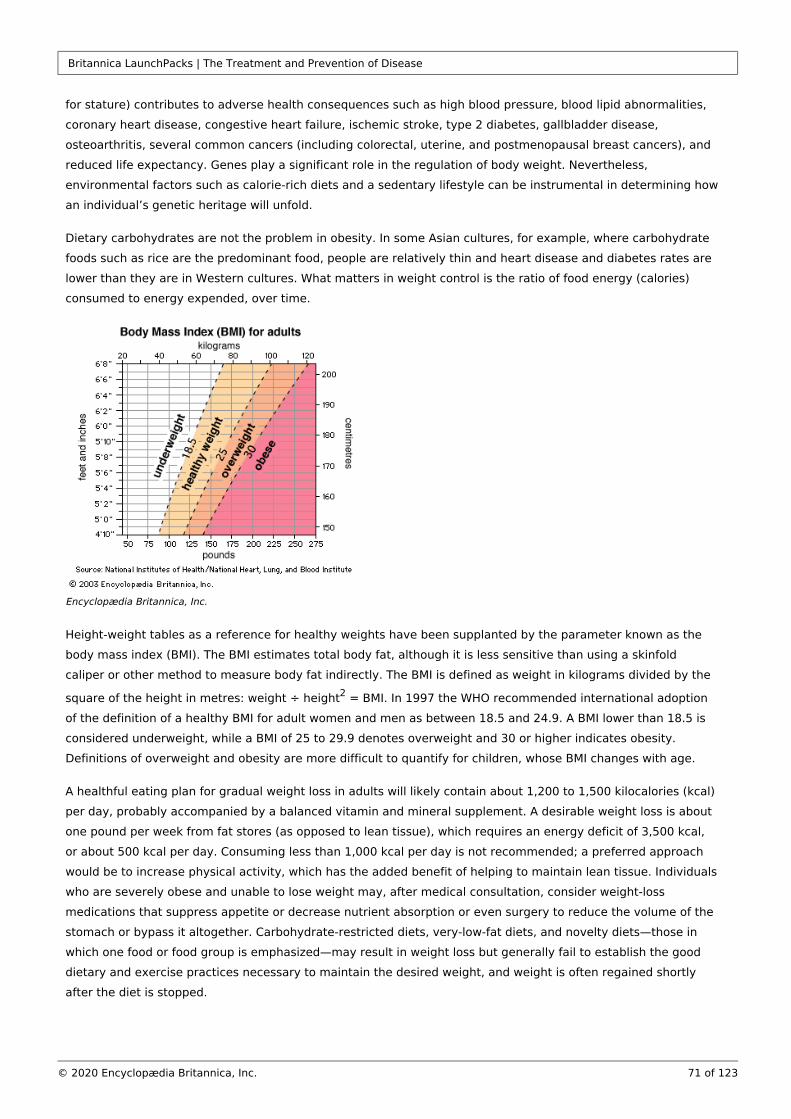
Britannica LaunchPacks | The Treatment and Prevention of Disease
71 of 123© 2020 Encyclopædia Britannica, Inc.
for stature) contributes to adverse health consequences such as high blood pressure, blood lipid abnormalities,
coronary heart disease, congestive heart failure, ischemic stroke, type 2 diabetes, gallbladder disease,
osteoarthritis, several common cancers (including colorectal, uterine, and postmenopausal breast cancers), and
reduced life expectancy. Genes play a significant role in the regulation of body weight. Nevertheless,
environmental factors such as calorie-rich diets and a sedentary lifestyle can be instrumental in determining how
an individual’s genetic heritage will unfold.
Dietary carbohydrates are not the problem in obesity. In some Asian cultures, for example, where carbohydrate
foods such as rice are the predominant food, people are relatively thin and heart disease and diabetes rates are
lower than they are in Western cultures. What matters in weight control is the ratio of food energy (calories)
consumed to energy expended, over time.
Encyclopædia Britannica, Inc.
Height-weight tables as a reference for healthy weights have been supplanted by the parameter known as the
body mass index (BMI). The BMI estimates total body fat, although it is less sensitive than using a skinfold
caliper or other method to measure body fat indirectly. The BMI is defined as weight in kilograms divided by the
square of the height in metres: weight ÷ height = BMI. In 1997 the WHO recommended international adoption 2
of the definition of a healthy BMI for adult women and men as between 18.5 and 24.9. A BMI lower than 18.5 is
considered underweight, while a BMI of 25 to 29.9 denotes overweight and 30 or higher indicates obesity.
Definitions of overweight and obesity are more difficult to quantify for children, whose BMI changes with age.
A healthful eating plan for gradual weight loss in adults will likely contain about 1,200 to 1,500 kilocalories (kcal)
per day, probably accompanied by a balanced vitamin and mineral supplement. A desirable weight loss is about
one pound per week from fat stores (as opposed to lean tissue), which requires an energy deficit of 3,500 kcal,
or about 500 kcal per day. Consuming less than 1,000 kcal per day is not recommended; a preferred approach
would be to increase physical activity, which has the added benefit of helping to maintain lean tissue. Individuals
who are severely obese and unable to lose weight may, after medical consultation, consider weight-loss
medications that suppress appetite or decrease nutrient absorption or even surgery to reduce the volume of the
stomach or bypass it altogether. Carbohydrate-restricted diets, very-low-fat diets, and novelty diets—those in
which one food or food group is emphasized—may result in weight loss but generally fail to establish the good
dietary and exercise practices necessary to maintain the desired weight, and weight is often regained shortly
after the diet is stopped.
Britannica LaunchPacks | The Treatment and Prevention of Disease
72 of 123© 2020 Encyclopædia Britannica, Inc.
A successful approach to long-term weight management requires establishing new patterns: eating healthfully,
but eating less; engaging in regular physical activity; and changing behaviour patterns that are
counterproductive, such as eating while watching television. Limiting intake of fatty foods, which are more
energy-rich, is also helpful, as is eating smaller portions and drinking water instead of calorie-containing drinks.
Low-fat foods are not always low in total calories, as the fat may be replaced by sugars, which themselves
provide calories. Individuals who use artificial or nonnutritive sweeteners do not necessarily reduce their total
calorie intake.
Research with genetically obese laboratory animals led to the discovery of the gene in mice and humans. obUnder the direction of this gene, adipose (fat) tissue cells secrete leptin, a protein hormone. When fat stores
increase, leptin sends a signal to the hypothalamus (a regulatory centre in the brain) that stimulates one to eat
less and expend more energy. Certain genetic mutations result in insufficient production of functional leptin or in
a failure to respond to the leptin signal. Treatment with leptin may prove useful for the small percentage of
obese persons who have a defect in the gene, although it is not yet known whether leptin therapy will induce obweight loss in those who are leptin-resistant or who do not have mutations in the gene.ob
Eating disorders
Eating disorders such as anorexia nervosa and bulimia nervosa are serious health problems reflecting an undue
concern with body weight. Girls and young women are most vulnerable to the pressures of society to be thin,
although boys and men can also fall prey to these disorders, which have lifelong consequences and can even be
fatal. The incidence of eating disorders has risen during the last 50 years, particularly in the United States and
western Europe.
Anorexia nervosa is characterized by low body weight, propensity for drastic undereating, intense fear of gaining
weight or becoming fat (despite being underweight), and a distorted body image. Consequences include
impaired immunity, anemia, and diminished digestive function. Without intervention, a state of semi-starvation
similar to marasmus may occur, requiring hospitalization and even force-feeding to prevent death. Treatment
usually requires a coordinated approach, with the participation of a physician, psychiatrist, dietitian, and possibly
other health professionals.
Bulimia nervosa is thought to be more prevalent than anorexia nervosa, and both disorders may even occur in
the same person. In bulimia nervosa recurrent episodes of “binge eating” are followed by a form of purging,
such as self-induced vomiting, fasting, excessive exercise, or the use of laxatives, enemas, or diuretics.
Treatment usually involves a structured eating plan.
Young athletes often restrict energy intakes to meet weight guidelines and body-image expectations of their
sport. Females are most affected, but male athletes, such as gymnasts, wrestlers, boxers, and jockeys, are also
vulnerable. Intense training among young female athletes, coupled with food energy restriction, often results in
amenorrhea (failure to menstruate for at least three consecutive months) and bone loss similar to that at
menopause. Calcium supplementation may be required.
Tooth decay
Dental caries (tooth decay) is an oral infectious disease in which bacteria, primarily , in the Streptococcus mutansdental plaque metabolize simple sugars and other fermentable carbohydrates into acids that dissolve tooth
enamel. Dental plaque (not to be confused with the lipid-containing plaque found in arteries) is a mass of
bacteria and sticky polymers that shield the tooth from saliva and the tongue, thereby facilitating decay. All
dietary forms of sugar, including honey, molasses, brown sugar, and corn syrup, can cause tooth decay;
Britannica LaunchPacks | The Treatment and Prevention of Disease
73 of 123© 2020 Encyclopædia Britannica, Inc.
fermentable carbohydrates in crackers, breads, cereals, and other grain products, as well as milk, fruits, and fruit
juices, also have cariogenic (decay-causing) potential. Eating sugary or starchy foods between meals, especially
sticky foods that stay on the teeth longer, increases the time that teeth are exposed to destructive acids.
Artificial sweeteners are not cariogenic, and xylitol, a sugar alcohol used in some chewing gums, is even
cariostatic, i.e., it reduces new tooth decay by inhibiting plaque and suppressing decay-causing bacteria. Putting
an infant to sleep with a bottle, especially one containing juice or other sweetened beverages, milk, or infant
formula can lead to a condition called “baby bottle tooth decay.”
Fluoride is extremely effective at protecting tooth enamel from decay, especially while enamel is being formed
in the jaws before the permanent teeth erupt. Fluoridation of water in communities where fluoride is not
naturally high is a safe and effective public health measure. Water with approximately one part per million of
fluoride protects against dental caries without causing the mottling of teeth that can occur at higher levels. In
areas without fluoridated water, fluoride supplements are recommended for children. Brewed tea, marine fish
consumed with bones, and seaweed are significant food sources of fluoride.
Regular brushing and flossing of the teeth and gums, as well as rinsing the mouth after meals and snacks, are
important measures that protect against periodontal (gum) disease as well as dental caries. Gum health also
depends on a properly functioning immune system and good overall nutrition. Key nutrients include vitamin C,
which helps protect against gingivitis (inflamed gums), and calcium and vitamin D, which help ensure a strong
jawbone and teeth.
Heartburn and peptic ulcer
When gastric contents, containing hydrochloric acid, flow backward from the stomach, the lining of the
esophagus becomes inflamed, leading to the burning sensation known as heartburn. Occasional heartburn (also
known as acid indigestion) is a common occurrence, typically precipitated by eating certain foods. However,
some people experience heartburn regularly, a condition known as gastroesophageal reflux disease (GERD).
Individuals with GERD are advised to limit their intake of alcohol and caffeine, which relax the lower esophageal
sphincter and actually promote reflux, as well as their intake of fat, which delays gastric emptying. Chocolate,
citrus fruit and juices, tomatoes and tomato products, spearmint and peppermint oils, and certain spices may
aggravate heartburn, but these foods do not appear to cause the condition.
For overweight or obese individuals with GERD, weight loss may have a beneficial effect on symptoms. Eating
smaller meals, chewing food thoroughly, eating more slowly, avoiding tight-fitting clothes, not smoking, and not
lying down before about three hours after eating are among the factors that may improve the condition. Without
medical supervision, drugs such as antacids and acid controllers should be used only infrequently.
It is now known that a peptic ulcer (a sore on the lining of the stomach or duodenum) is not caused by stress or
eating spicy foods, as was once thought; rather, most peptic ulcers are caused by the infectious bacterial agent
and can be treated by a simple course of antibiotics. However, stress and dietary factors—Helicobacter pylorisuch as coffee, other caffeinated beverages, and alcohol—can aggravate an existing ulcer.
Bowel conditions and diseases
Constipation, a condition characterized by the difficult passage of relatively dry, hardened feces, may arise from
insufficient dietary fibre (roughage) or other dietary factors, such as taking calcium or iron supplements, in
addition to daily routines that preclude relaxation. Straining during defecation can also contribute to
diverticulosis, small outpouchings in the colonic wall, which may become inflamed (diverticulitis) and present
serious complications. Another possible consequence of straining is hemorrhoids, swollen veins of the rectum
and anus that typically lead to pain, itching, and bleeding. Constipation can usually be treated by eating high-
Britannica LaunchPacks | The Treatment and Prevention of Disease
74 of 123© 2020 Encyclopædia Britannica, Inc.
fibre foods such as whole-grain breads and cereals, drinking sufficient amounts of water, and engaging in regular
exercise. By drawing water into the large intestine (colon), fibre—especially the insoluble type—helps form a
soft, bulky stool. Eating dried fruits such as prunes, which contain a natural laxative substance (dihydroxyphenyl
isatin) as well as being high in fibre, also helps stimulate the bowels. Although laxatives or enemas may be
helpful, frequent use may upset fluid, mineral, and electrolyte (salt) balances and interfere with vitamin
absorption. Any persistent change in bowel habits should be evaluated by a physician.
In contrast to constipation, diarrhea—loose, watery stools, and possibly an increased frequency of bowel
movements—can be a cause for immediate concern. Acute diarrhea of bacterial origin is relatively common and
often self-limiting. Other common causes of acute diarrhea include viral infections, parasites, food intolerances
or allergies, medications, medical or surgical treatments, and even stress. Regardless of cause, drinking fluids is
important for treating a temporary bout of diarrhea. However, if severe and persisting, diarrhea can lead to
potentially dangerous dehydration and electrolyte imbalances and requires urgent medical attention, especially
in infants and children. Prolonged vomiting presents similar risks.
Inflammatory bowel disease (IBD), such as Crohn disease (regional ileitis) or ulcerative colitis, results in impaired
absorption of many nutrients, depending upon which portion of the gastrointestinal tract is affected. Children
with IBD may fail to grow properly. Treatment generally includes a diet low in fat and fibre, high in protein and
easily digestible carbohydrate, and free of lactose (milk sugar). Increased intakes of certain nutrients, such as
iron, calcium, and magnesium, and supplementation with fat-soluble vitamins may also be recommended, along
with additional fluid and electrolytes to replace losses due to diarrhea.
Irritable bowel syndrome (IBS) is a common gastrointestinal disorder characterized by a disturbance in intestinal
peristalsis. Symptoms include excessive gas, abdominal discomfort, and cramps, as well as alternating diarrhea
and constipation. Although it can be extremely uncomfortable, IBS does not cause intestinal damage. Dietary
treatment involves identifying and avoiding “problem” foods, notably legumes and other gas-producing
vegetables and dairy products, and possibly reducing caffeine consumption. For most people with IBS, a low-fat
diet, smaller meals, and a gradual increase in fibre intake are helpful.
Food-drug interactionsDrugs may interfere with or enhance the utilization of nutrients, sometimes leading to imbalances. A common
example is the increased loss of potassium that results from the use of certain diuretics to treat high blood
pressure. Nutrient absorption can also be affected by drugs that change the acidity of the gastrointestinal tract,
alter digestive function, or actually bind to nutrients. For example, regular use of laxatives, antacids, or mineral
oil can reduce nutrient absorption and over time may lead to deficiency. Elderly individuals who take multiple
medicines are particularly at risk of impaired nutritional status.
On the other hand, foods can alter drug absorption or interact with drugs in undesirable ways, resulting in drug
ineffectiveness or toxicity. For example, protein and vitamin B interfere with the effectiveness of levodopa, 6
used to treat Parkinson disease. Tyramine, an amino-acid derivative found in certain aged cheeses and red
wines, may cause hypertension in individuals being treated for depression with monoamine oxidase (MAO)
inhibitors. Grapefruit juice contains unique substances that can block the breakdown of some drugs, thereby
affecting their absorption and effectiveness. These drugs include certain cholesterol-lowering statins, calcium
channel blockers, anticonvulsant agents, estrogen, antihistamines, protease inhibitors, immunosuppressants,
antifungal drugs, and psychiatric medications. Eating grapefruit or drinking grapefruit juice within a few hours or
even a few days of taking these medications could result in unintended consequences.
Britannica LaunchPacks | The Treatment and Prevention of Disease
75 of 123© 2020 Encyclopædia Britannica, Inc.
Vitamin and mineral supplements and herbal products can also interact with medicines. For example, one or
more of the supplemental antioxidants studied—vitamin C, vitamin E, beta-carotene, and selenium—may blunt
the effectiveness of certain drugs (e.g., high-dose niacin, when used in combination with statins) in raising HDL
cholesterol levels and improving cardiovascular health. Also, the herbal supplement St. John’s wort can alter the
metabolism of drugs such as protease inhibitors, anticlotting drugs, and antidepressants, and it can reduce the
effectiveness of oral contraceptives.
Food allergies and intolerances
Research suggests that oral desensitization therapy, in which escalating doses of peanuts are…
Science in Seconds (www.scienceinseconds.com)
A true food allergy involves an abnormal immunologic response to an otherwise harmless food component,
usually a protein. In the case of antibody-mediated (immediate hypersensitivity) food allergies, within minutes or
hours of exposure to the allergen, the body produces specific immunoglobulin E antibodies and releases
chemical mediators such as histamine, resulting in gastrointestinal, skin, or respiratory symptoms ranging from
mild to life-threatening. Much less common are cell-mediated (delayed hypersensitivity) food allergies, in which
a localized inflammatory process and other symptoms may not start for up to a day. Adverse food reactions that
do not involve the immune system, aside from foodborne infection or poisoning, are called food intolerances or
sensitivities. Most common of these is lactose intolerance, which is a genetically determined deficiency of the
enzyme lactase that is needed to digest the milk sugar, lactose.
Milk allergy and lactose intolerance are distinct conditions that are often confused. Only about 1 percent of the
population has a true allergy to the protein in cow’s milk. Milk allergy is found most often in infants, whose
immune and digestive systems are immature. On the other hand, much of the world’s population, except those
of northern European descent, is to some degree lactose intolerant after early childhood. Undigested lactose
reaching the large intestine can cause abdominal discomfort, flatulence, and diarrhea. Lactose-intolerant
individuals can often handle with little or no discomfort small quantities of dairy products, especially yogurt or
other milk products containing the bacterium ; alternatives are the use of lactose-Lactobacillus acidophilushydrolyzed milk products or lactase tablets or drops, which convert lactose to simple, digestible sugars.
Celiac disease (also known as celiac sprue, nontropical sprue, or gluten-sensitive enteropathy) is a hereditary
disorder in which consumption of wheat gluten and related proteins from rye and barley is not tolerated. Recent
studies indicate that oats may be safe if not contaminated with wheat. Celiac disease, which may be a type of
cell-mediated food allergy, affects primarily individuals of European descent and rarely those of African or Asian
descent. It is characterized by inflammatory damage to the mucosal cells lining the small intestine, leading to
malabsorption of nutrients and such symptoms as diarrhea, fatigue, weight loss, bone pain, and neurological
disturbances. Multiple nutritional deficiencies may ensue and, in children, growth is impaired. The disorder is
often associated with autoimmune conditions, particularly autoimmune thyroid disease and type 1 diabetes.
Britannica LaunchPacks | The Treatment and Prevention of Disease
76 of 123© 2020 Encyclopædia Britannica, Inc.
Although celiac disease can be life-threatening if untreated, patients can recover if gluten is eliminated from the
diet.
Other adverse reactions to foods or beverages may be drug effects, such as those caused by caffeine or alcohol.
Certain foods, such as ripened cheese, chocolate, red wine, and even ice cream, trigger headaches in some
individuals. Food additives that can cause reactions in susceptible people include sulfite preservatives, used in
some wines, dried fruits, and dried potato products; nitrate and nitritepreservatives, used in processed meats;
certain food colorants, particularly tartrazine (also known as FD&C Yellow #5); and the flavour enhancer
monosodium glutamate (MSG). Some adverse reactions to food are purely psychological and do not occur when
the food is served in a disguised form.
Learn about parental guidelines introduced in 2017 to combat peanut allergies in children.
Encyclopædia Britannica, Inc.
Nearly any food has allergenic potential, but foods that most commonly cause antibody-mediated allergic
reactions are cow’s milk, eggs, wheat, fish, shellfish, soybeans, peanuts, and tree nuts (such as almonds,
walnuts, and cashews). Depending on processing methods, edible oils and other products derived from these
foods may still contain allergenic protein residues. Severely allergic people may react to extremely small
amounts of an offending food, even inhaled vapours.
Studies differ significantly as to the percentage of adults and children who have true food allergies. However,
most seem to agree that few adults (about 2 to 5 percent) and slightly more children (roughly 3 to 8 percent) are
affected. Most children outgrow food allergies, particularly if the offending food is avoided for a year or two.
However, food allergies can develop at any time, and some allergies, such as those to peanuts, tree nuts, and
shellfish, may be lifelong. Common symptoms of antibody-mediated food allergy include tightening of the throat,
swelling of the lips or tongue, itchy lips, wheezing, difficulty breathing, headache, nasal congestion, skin rash
(eczema), hives, nausea, vomiting, stomach cramps, diarrhea and, in severe cases, life-threatening anaphylactic
shock. People susceptible to anaphylaxis are advised to carry a syringe loaded with epinephrine at all times and
to seek emergency medical care if an allergic reaction begins.
Food allergies are often hard to document, even by physicians trained in allergy and immunology. Blood tests for
antibodies to specific allergens, skin tests, and even an elimination diet, in which suspect foods are eliminated
from the diet and then added back one at a time, may not be definitive. The most conclusive diagnostic test is a
so-called double-blind food challenge, in which neither doctor nor patient knows whether a suspect food or a
harmless placebo is being given; however, these controlled clinical tests are expensive and time-consuming.
Labels are important for identifying hidden ingredients in packaged foods, although they are often imprecise and
cannot be relied on naively. For example, even if a product is labeled as nondairy, a listing of casein, caseinate,
or whey indicates the presence of milk protein. Peanuts may be found in unlikely foods, such as chili, stew,
processed meats, oils, flours, cream substitutes, and desserts.
Britannica LaunchPacks | The Treatment and Prevention of Disease
77 of 123© 2020 Encyclopædia Britannica, Inc.
Research has indicated that, at least in some instances, the severity of an allergy may be reduced through
desensitization, in which a person is exposed over time to increasing amounts of the antigen to which he or she
is allergic. Methods of desensitization differ; for example, allergy shots involve the injection of antigens, whereas
sublingual immunotherapy involves small doses of antigen given as drops under the tongue. Sublingual
immunotherapy in particular is considered a safe and effective means of building tolerance to food allergens.
Toxins in foodsEdible skins of fruits and vegetables are rich in vitamins, minerals, and fibre; however, pesticide residues and
other environmental contaminants are typically more plentiful in the outer layers of these foods. Pesticides also
tend to accumulate in the fat and skin of animals. Intake of toxic substances is reduced by consuming a wide
variety of foods; washing fruits and vegetables carefully; and trimming fat from meat and poultry and removing
skin from poultry and fish. Even organic produce requires thorough washing: it may not have synthetic
chemicals, but mold, rot, fecal matter or other natural substances can contaminate it at any point from field to
market. Peeling helps reduce these unwanted chemicals and microbes, although valuable nutrients will be lost
as well.
A greenish tinge on potatoes, although merely the harmless substance chlorophyll, indicates that the natural
toxicant solanine may be present. Solanine builds up when a potato is handled roughly, exposed to light or
extremes of temperature, or is old. Symptoms of solanine poisoning include diarrhea, cramps, and headache,
although many damaged potatoes would have to be eaten to cause serious illness. Peeling away green areas or
removing sprouts or the entire skin (despite its high nutrient content) reduces solanine intake.
Swordfish and shark, as well as tuna steaks, may contain high levels of methylmercury (which remains after
cooking) and should be avoided by pregnant women. Nonbacterial toxins in seafood include scombrotoxin
(histamine) in spoiled fish, which can result in a severe allergic reaction when eaten; dinoflagellates (microscopic
algae), associated with the so-called red tide, which can cause paralytic shellfish poisoning when consumed; and
ciguatera, found in certain warm-water reef fish.( fish poisoning; shellfish poisoning.)See also
Natural toxins in some species of mushrooms cause symptoms ranging from gastrointestinal upset to
neurological effects, even hallucinations. Most mushroom fatalities are due to consumption of amatoxins in
, the mushroom species known as the death cap, which, if not lethal, can cause lasting liver Amanita phalloidesand kidney damage. As there are no antidotes for mushroom poisoning, and identification of mushroom species
by inexperienced mushroom pickers is often imprecise, consumption of wild mushrooms is not advised.
Foodborne illnessesContamination of foods or beverages with disease-causing organisms—bacteria, viruses, fungi, and parasites—
can result in symptoms ranging from mild stomach upset, headache, muscle aches, and fever to abdominal
cramps, vomiting, and diarrhea. Severe cases can result in dangerous dehydration, nerve damage, paralysis,
kidney failure, and death. Symptoms may develop within hours or days after eating contaminated food, and they
are not always easy to distinguish from influenza or other illnesses. Drinking clear liquids (such as chicken broth,
juices, and water) helps replace fluids and electrolytes lost during a mild infection, but immediate medical
attention is required when symptoms are severe. Most susceptible are infants and young children, pregnant
women, the elderly, and people with weakened immune systems or certain chronic diseases. Particularly risky
foods include raw or undercooked meat, poultry, eggs, seafood, and unpasteurized (raw) milk products and
juices.
Britannica LaunchPacks | The Treatment and Prevention of Disease
78 of 123© 2020 Encyclopædia Britannica, Inc.
Common food-borne illnessesSome common foodborne illnesses are listed in the table.
Most cases of foodborne illness are caused by bacteria and the toxins they produce. , found Campylobacter jejuniin raw or undercooked foods of animal origin, especially poultry, is responsible for more diarrheal illness
throughout the world than any other bacterium. Travelers’ diarrhea is often caused by specific types of
bacteria, while other types cause much of the diarrhea in infants, particularly during Escherichia coli E. coliweaning, in developing countries. Other common foodborne infections are caused by various strains of
bacteria and the Norwalk family of viruses.Salmonella
Smoking, drying, fermenting, and the adding of sugar or salt are traditional methods used to preserve food and
keep it safe. During the 20th century public health advances such as disinfection of water supplies,
pasteurization of milk, safe canning, widespread use of refrigeration, and improved food-safety practices
eliminated typhoid fever, tuberculosis, and cholera, for example, as common foodborne diseases. However,
others have taken their place. New causes of foodborne illness continue to be discovered or described. A
recently characterized microscopic parasite, , was the cause of outbreaks of diarrheal Cyclospora cayetanensisillness in the United States and Canada starting in 1996. Guatemalan raspberries, contaminated with Cyclosporavia the water supply, were the suspected source of infection. Another recently described parasite,
, contaminates water supplies and foods and is an important cause of diarrhea Cryptosporidium parvumthroughout the world, particularly in children and in persons with HIV.
In 1993, undercooked hamburgers emerged in the United States as a potential source of O157:H7, a E. colideadly strain of a normally harmless bacterium found in the human digestive tract. Subsequently, this microbe
has also been found in unpasteurized fruit juice, such as fresh-pressed apple cider, and other foods possibly
contaminated with animal feces. The bacterium produces a potent toxin that may result in bloody diarrhea;
hemolytic uremic syndrome, a possible complication, is a major cause of acute kidney failure in children. E. coliO157:H7 infection, which can be spread by persons who unknowingly incubate the bacterium in their intestines
and transmit it through poor toilet hygiene, appears to be on the rise worldwide, particularly in North America
and western Europe.
Certain other bacteria also produce a toxin, which then causes a poisoning or intoxication rather than a bacterial
infection per se. For example, , found in improperly canned foods, produces the lethal Clostridium botulinumneurotoxin that causes botulism. The toxin responsible for staphylococcal food poisoning is produced by
typically after contamination from nasal passages or cuts on the skin.Staphylococcus aureus
Many molds (fungi) on food are harmless and, in fact, are flavour enhancing, such as those used to ripen certain
cheeses. However, some molds—particularly those on grains, nuts, fruits, and seeds—produce poisons known as
mycotoxins. The mycotoxins of greatest concern are aflatoxins, which can infect nuts, peanuts, corn, and wheat.
Prolonged low-level exposure to aflatoxins, as seen in regions of Asia and Africa, is suspected of contributing to
liver cancer. Discarding nuts that are discoloured, shriveled, or moldy helps reduce the risk.
Eating raw shellfish, sushi, or undercooked fish puts one at risk for parasites, such as tapeworms, as well as for
bacteria and viruses, all of which are killed by proper cooking. The great majority of seafood-related illness is
caused by the consumption of raw bivalve mollusks. Clams, mussels, and scallops, which are usually served
cooked, are of less public health concern than oysters, which are often eaten raw.
Bovine spongiform encephalopathy (BSE), commonly known as mad cow disease, was first seen in British cattle
in the 1980s. However, it was not linked to human disease until 1996, when 10 young adults in the United
Kingdom died of variant Creutzfeldt-Jakob disease, a fatal brain-wasting disease thought to have been
transmitted by consumption of meat containing brain or spinal tissue from BSE-infected cattle. It is suspected
Britannica LaunchPacks | The Treatment and Prevention of Disease
79 of 123© 2020 Encyclopædia Britannica, Inc.
that the diseased cattle had been infected by eating the ground remains of sheep with the neurodegenerative
disease scrapie. BSE appears to be caused by infectious protein particles called prions, which kill brain cells and
leave holes in the brain. Details of disease transmission are still unclear, as is the potential risk from cosmetics,
dietary supplements, gelatin, or vaccines containing bovine ingredients, or from blood transfusions. Ground beef,
sausages, and frankfurters are more likely to be contaminated with nervous-system tissue than are whole cuts of
beef. Dairy products are considered safe, even if they come from BSE-infected cows.
Good personal hygiene and food safety practices are important in protecting against foodborne illness. The main
source of contamination is fecal matter, which is reduced by frequently washing hands with soap and hot water,
especially before preparing food. Thorough washing also decontaminates towels, surfaces, cutting boards,
utensils, and other equipment that has touched uncooked meat. Other food safety guidelines include keeping
cold foods cold, keeping hot foods hot, and refrigerating leftovers quickly.
Growth of microorganisms, parasites, and insects on certain foods (such as meat, poultry, spices, fruits, and
vegetables) can be controlled by low-dose irradiation, which has been approved for specific uses in a number of
countries, such as Japan, France, Italy, Mexico, and the United States. Food irradiation technology—which does
not make foods radioactive—is considered safe by the World Health Organization and various health agencies,
but it has yet to receive wide consumer acceptance.
Botanicals and functional foodsMany herbal products show sufficient promise in preventing or treating disease that they are being tested in
rigorous scientific studies, including clinical trials. However, the “botanicals” currently on the market in many
countries are untested with regard to safety and efficacy, and consumers should approach their use in an
informed and cautious way. Just as with pharmaceuticals, herbal products can have mild to severe side effects,
and “natural” does not mean “safe.” Furthermore, the amounts of active ingredients in supplements can vary
widely and, according to laboratory analyses, the potency specified on labels is often inaccurate. Some
preparations even contain none of the active ingredients listed on the label or may have unwanted contaminants.
Potentially dangerous herbal products include comfrey and kava, which can cause liver damage, and ephedra
(ma huang), which has caused fatal reactions in some people, especially those with high blood pressure or heart
disease. Because of possible complications, patients scheduled to undergo surgery or other medical procedures
may be advised to discontinue certain supplements for days or even weeks before surgery. Safety and efficacy
concerns also need to be addressed, as “designer foods” fortified with herbs and bioactive substances continue
to proliferate.
The distinction between foods, dietary supplements, and drugs is already being blurred by the burgeoning
market in so-called functional foods (such as cholesterol-lowering margarine), which aim to provide health
benefits beyond mere nutrient value. Moreover, recent advances in molecular biology offer the possibility of
using genetic profiles to determine unique nutrient requirements, thereby providing customized dietary
recommendations to more effectively delay or prevent disease.
Jean Weininger
Additional ReadingComprehensive treatments of nutrition in health and disease are found in et al. (eds.), MAURICE E. SHILS Modern
, 10th ed. (2006); and (eds.), Nutrition in Health and Disease BARBARA A. BOWMAN ROBERT M. RUSSELL Present
, 9th ed. (2006); , , and , Knowledge in Nutrition JAMES L. GROFF SAREEN S. GROPPER JACK L. SMITH Advanced Nutrition
Britannica LaunchPacks | The Treatment and Prevention of Disease
80 of 123© 2020 Encyclopædia Britannica, Inc.
, 5th ed. (2009); and , and Human Metabolism GORDON M. WARDLAW CAROL BYRD-BREDBENNER Wardlaw’s Perspectives
, 9th ed. (2012); and , , 12th ed. in Nutrition ELEANOR NOSS WHITNEY SHARON RADY ROLFES Understanding Nutrition
(2011); and and (eds.), , 12th ed. (2008).L. KATHLEEN MAHAN SYLVIA ESCOTT-STUMP Krause’s Food & Nutrition Therapy
World hunger and malnutrition
Useful guides for understanding malnutrition include (ed.), THOMAS J. MARCHIONE Scaling Up; Scaling Down:
(1999); and and , Overcoming Malnutrition in Developing Countries FRANCES MOORE LAPPÉ ANNA LAPPÉ Hope’s
(2002); and (eds.), Edge: The Next Diet for a Small Planet RICHARD D. SEMBA MARTIN W. BLOEM Nutrition and
(2001); and , Health in Developing Countries MICHAEL C. LATHAM Human Nutrition in the Developing World
(1997).
Diet and chronic disease
Comprehensive sources on diet and chronic disease are NATIONAL RESEARCH COUNCIL (U.S.) COMMITTEE ON DIET
, (1989); and AND HEALTH Diet and Health: Implications for Reducing Chronic Disease Risk INSTITUTE OF
, , a series of reports published periodically starting in 1997. MEDICINE (U.S.) Dietary Reference Intakes
Dietary recommendations for cardiovascular disease are discussed in EXPERT PANEL ON DETECTION,
, “Executive Summary of the Third Report EVALUATION, AND TREATMENT OF HIGH BLOOD CHOLESTEROL IN ADULTS
of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and
Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III),” Journal of the American , vol. 285 (May 16, 2001); and , Medical Association NUTRITION COMMITTEE OF THE AMERICAN HEART ASSOCIATION
“AHA Dietary Guidelines,” , vol. 102, p. 2284 (2000).Circulation
A major international report on diet and cancer prevention is WORLD CANCER RESEARCH FUND/AMERICAN
, (1997). INSTITUTE FOR CANCER RESEARCH Food, Nutrition, and the Prevention of Cancer: A Global Perspective
A classic article on the value of nutrition in cancer prevention is and , “The Causes of R. DOLL R. PETO
Cancer: Quantitative Estimates of Avoidable Risks of Cancer in the United States Today,” Journal of the , vol. 66, pp. 1191–1308 (1981). An evaluation of claims for the use of diet, National Cancer Institute
herbs, and supplements in cancer prevention and treatment is , AMERICAN CANCER SOCIETY American Cancer
, 2nd ed. (2009).Society Complete Guide to Complementary & Alternative Cancer Methods
Practical information for controlling diabetes with proper nutrition is detailed in AMERICAN DIABETES
, (1999).ASSOCIATION Guide to Medical Nutrition Therapy
Obesity and eating disorders
The causes and consequences of obesity and a comprehensive framework for treatment are considered in
and (eds.), (2002). The relationship THOMAS A. WADDEN ALBERT J. STUNKARD Handbook of Obesity Treatment
between body image and eating disorders and approaches to treatment are examined in and IRA M. SACKER
, MARC A. ZIMMER Dying to Be Thin: Understanding and Defeating Anorexia Nervosa and Bulimia—A Practical
(1987, rev. ed. 2001); and and (eds.), Lifesaving Guide J. KEVIN THOMPSON LINDA SMOLAK Body Image, Eating
, 2nd ed. (2009).Disorders, and Obesity in Youth: Assessment, Prevention, and Treatment
Food allergies and intolerances
Information about food allergies is presented in and , JONATHAN BROSTOFF LINDA GAMLIN Food Allergies and
(2000); and Food Intolerance: The Complete Guide to Their Identification and Treatment CELIDE BARNES
and , (1998).KOERNER ANNE MUNOZ-FURLONG Food Allergies: How to Eat Safely and Enjoyably
Britannica LaunchPacks | The Treatment and Prevention of Disease
81 of 123© 2020 Encyclopædia Britannica, Inc.
Citation (MLA style):
"Nutritional disease." , Encyclopædia Britannica LaunchPacks: The Treatment and Prevention of DiseaseBritannica, 11 Nov. 2020. packs-ngl.eb.com. Accessed 6 Apr. 2022.
While every effort has been made to follow citation style rules, there may be some discrepancies. Please refer to the appropriate style manual or other sources if you have any questions.
therapeuticsBritannica Note:
The treatment and care of someone to combat disease, injury, or mental disorder is known as therapy, or therapeutics.
treatment and care of a patient for the purpose of both preventing and combating disease or alleviating pain or
injury. The term comes from the Greek , which means “inclined to serve.”therapeutikos
Prozac pills.
Tom Varco
In a broad sense, therapeutics means serving and caring for the patient in a comprehensive manner, preventing
disease as well as managing specific problems. Exercise, diet, and mental factors are therefore integral to the
prevention, as well as the management, of disease processes. More specific measures that are employed to
treat specific symptoms include the use of drugs to relieve pain or treat infection, surgery to remove diseased
tissue or replace poorly functioning or nonfunctioning organs with fully operating ones, and counseling or
psychotherapy to relieve emotional distress. Confidence in the physician and in the method selected enhances
effectiveness.
Preventive medicineThe rationale for preventive medicine is to identify risk factors in each individual and reduce or eliminate those
risks in an attempt to prevent disease. Primary prevention is the preemptive behavior that seeks to avert
Britannica LaunchPacks | The Treatment and Prevention of Disease
82 of 123© 2020 Encyclopædia Britannica, Inc.
disease before it develops—for example, vaccinating children against diseases. Secondary prevention is the
early detection of disease or its precursors before symptoms appear, with the aim of preventing or curing it.
Examples include regular cervical Papanicolaou test (Pap smear) screening and mammography. Tertiary
prevention is an attempt to stop or limit the spread of disease that is already present. Clearly, primary
prevention is the most cost-effective method of controlling disease.
Leading causes of death worldwide include cardiovascular disease, cancer, cerebrovascular disease, accidental
injuries, and chronic lung disease. A major preventable cause of death is cigarettesmoking, which is linked to
increased risk of cardiovascular disease (e.g., heart attack), cancer, stroke, and chronic lung diseases such as
emphysema and chronic bronchitis.
Multiple organizations worldwide have established recommendations and guidelines for disease prevention. For
example, in the United States, following earlier work by the Canadian Task Force on the Periodic Health
Examination, the U.S. Preventive Services Task Force was established to evaluate the effectiveness of various
screening tests, immunizations, and prophylactic regimens based on a critical review of the scientific literature.
Its report, , lists the recommendations for a variety of conditions evaluated Guide to Clinical Preventive Servicesby the panel.
A nurse administering a vaccine via intramuscular injection into the left shoulder muscle of a…
James Gathany/Centers for Disease Control and Prevention (CDC)
Immunization is the best method for preventing infectious diseases. Standard immunizations of infants and
children include those for diphtheria, tetanus, and pertussis, or whooping cough (DTP); polio (OPV); measles,
mumps, and rubella (MMR); type b (HbCV); and hepatitis B (HBV). A yearly vaccine Haemophilus influenzaeagainst the influenza virus should be administered to infants and young children, to adults who are over age 65,
to those at risk because of chronic cardiopulmonary disease, and to those in chronic care facilities. Adults at age
65 should also be immunized against pneumococcal pneumonia with a vaccine containing 23 of the most
common strains of .Streptococcus pneumoniae
Acquired immunodeficiency syndrome (AIDS), caused by human immunodeficiency virus (HIV), is a major
infectious disease problem. Although a vaccine is expected, obstacles to its development are great. Primary
preventive measures include abstaining from sexual contact, using condoms, and, among intravenous drug
users, avoiding the sharing of needles.
The risk factors for coronary artery disease that can be modified to prevent heart attack are cigarette smoking,
hypertension, an elevated serum cholesterol level, a sedentary lifestyle, obesity, stress, and excessive alcohol
consumption. In addition to an elevated total serum cholesterol level, an elevated low-density lipoprotein (LDL)
level and a decreased high-density lipoprotein (HDL) level are significant risk factors. The total cholesterol level
and elevated LDL level can be reduced by appropriate diet, whereas a low HDL can be raised by stopping

Britannica LaunchPacks | The Treatment and Prevention of Disease
83 of 123© 2020 Encyclopædia Britannica, Inc.
smoking and increasing physical activity. If those measures do not provide adequate control, a variety of drugs
capable of lowering the cholesterol level are available.
The major risk factor for stroke is hypertension, with cigarette smoking and type 2 diabetes mellitus significantly
increasing the risk. Transient ischemic attacks (TIAs) occur before stroke in 20 percent of patients and consist of
sudden onset of one or more of the following symptoms: temporary loss of vision in one eye, unilateral
numbness, temporary loss of speech or slurred speech, and localized weakness of an arm or leg. Attacks last
less than 24 hours and resolve without permanent damage until the stroke occurs.
The most important preventive behaviour in averting cancer is the avoidance of cigarette smoke. Smoking
accounts for 30 percent of all cancer deaths, and there is increasing recognition of the danger of environmental
or secondhand smoke to the nonsmoker. Primary prevention of skin cancer includes restricting exposure to
ultraviolet light by using sunscreens or protective clothing. For other cancers, secondary preventive measures
include mammography, clinical breast examinations, and breast self-examinations for breast cancer; pelvic
examinations and Pap tests for cervical cancer and ovarian cancer; and sigmoidoscopy, digital rectal
examinations, and stool tests for occult blood for colorectal cancer.
Demineralization of bone and a reduction in bone mass (osteoporosis) occur most often in men and women age
70 or older and may result in fractures, low back pain, and loss of stature. Osteoporosis in postmenopausal
women that is caused by estrogen deficiency is the most common manifestation. The most effective method for
preventing loss of bone mass after menopause is estrogen replacement therapy and increased calcium intake.
Primary preventive measures include increasing physical activity and avoiding cigarettes and heavy alcohol
consumption.
Alcohol abuse is the primary reason that accidents are a major cause of death in the United States. Other factors
are failure to wear seat belts or motorcycle helmets, sleep deprivation, and guns in the home. Taking reasonable
precautions and being aware of the potential dangers of alcohol and firearms can help reduce the number of
deaths due to accidents.
Treatment of symptomsPain
Pain is the most common of all symptoms and often requires treatment before its specific cause is known. Pain is
both an emotional and a physical experience and is difficult to compare from one person to another. One patient
may have a high pain threshold and complain only after the disease process has progressed beyond its early
stage, while another with a low pain threshold may complain about pain that would be ignored or tolerated by
most people. Pain from any cause can be increased by anxiety, fear, depression, loneliness, and frustration or
anger.
Acute pain serves a useful function as a protective mechanism that leads to the removal of the source of the
pain, whether it be localized injury or infection. Chronic pain serves a less useful function and is often more
difficult to treat. Although acute pain requires immediate attention, its cause is usually easily found, whereas
chronic pain complaints may be more vague and difficult to isolate.
The ideal method for treating pain is to eliminate the cause, such as to surgically remove an inflamed structure,
to apply hot compresses to a muscle spasm, or to set a fractured bone in a cast. Alternatives to drug therapy,
such as physical therapy, are relied on whenever possible. Analgesic drugs (pain relievers) most often used to
alleviate mild and moderate pain are the nonsteroidal anti-inflammatory drugs (NSAIDs) such as aspirin,
Britannica LaunchPacks | The Treatment and Prevention of Disease
84 of 123© 2020 Encyclopædia Britannica, Inc.
ibuprofen, acetaminophen, or indomethacin. If these are ineffective, a weak opiate such as codeine,
hydrocodone, or oxycodone may be prescribed. Severe pain not controlled by these agents requires a strong
opiate such as morphine or meperidine. Because opiates are addictive, their use is controlled. In the United
States, for example, opiate use is regulated by the Controlled Substances Act, and individuals prescribing or
dispensing these drugs must register annually with the Drug Enforcement Administration. Each drug is assigned
to one of five groups, from schedule I, which includes drugs that have the highest potential for abuse, to
schedule V, which includes drugs with a limited dependence-causing potential.
Nausea and vomiting
Nausea and vomiting are common symptoms that may arise from diseases of the gastrointestinal tract
(including gastroenteritis or bowel obstruction), from medications such as analgesics or digoxin, or from nervous
system disturbances such as migraines or motion sickness. Vomiting is controlled by a vomiting centre located
in the medulla oblongata of the brainstem.
Identifying and treating the cause is important, especially if the condition responds well to treatment and is
serious if not addressed. A bowel obstruction can occur as a result of adhesions from previous abdominal
surgery. Obstruction or decreased bowel motility also can occur with constipation and fecal impaction. Such
important and treatable causes must be ruled out before resorting to antiemetic (serving to prevent or cure
vomiting) drugs. The most frequently used antiemetic agents are the phenothiazines, the most popular being
prochlorperazine (Compazine). Antihistamines may be useful in motion sickness. Newer and more powerful
drugs are needed to control the vomiting associated with cancer chemotherapy. Ondansetron is given to
patients undergoing cancer chemotherapy, surgery, or radiation therapy with agents that cause severe nausea
and vomiting. This drug is very effective in these patients.
Learn what causes morning sickness, or nausea, in pregnant women.
© American Chemical Society
Nausea and vomiting are experienced by more than 50 percent of pregnant women during the first trimester.
These symptoms are referred to as morning sickness, although they can occur at any time of the day. They may
be distressing, but they cause no adverse effect on the fetus. Drug therapy not only is unnecessary but should
be avoided unless proved safe for the fetus. Treatment involves rest and intake of frequent small meals and
pyridoxine (vitamin B ).6
Diarrhea
Acute diarrhea can result from food poisoning, laxatives, alcohol, and some antacids. Usually it is caused by an
acute infection with bacteria such as , , and . These agents can Escherichia coli Salmonella Staphylococcus aureusenter the body on food, in water, or when contaminated objects (e.g., a teething ring) are put into the mouth. In
infants, acute diarrhea is usually self-limiting, and treatment consists primarily of preventing dehydration.
Traveler’s diarrhea affects up to half of those traveling to developing areas of the world. Preventive measures
Britannica LaunchPacks | The Treatment and Prevention of Disease
85 of 123© 2020 Encyclopædia Britannica, Inc.
include chewing two tablets of bismuth subsalicylate (Pepto-Bismol) four times a day, drinking only bottled water
or other bottled or canned beverages, and eating only fruits that may be peeled, canned products, and
restaurant food that is thoroughly cooked. Avoiding dairy products, raw seafood and vegetables, and food served
at room temperature also limits exposure. Severe cases require antibiotic therapy.
Cough
Coughing is a normal reflex that helps clear the respiratory tract of secretions and foreign material. It also can
result from irritation of the airway or from stimulation of receptors in the lung, diaphragm, ear (tympanic
membrane), and stomach. The most common cause of acute cough is the common cold. Chronic cough is most
often caused by irritation and excessive mucus production that results from cigarette smoking or from postnasal
drainage associated with an allergic reaction.
Treatment includes humidification of the air to loosen secretions and to counteract the drying effect of coughing
and inflammation. Moist air from a vaporizer or a hot shower helps, as do hot drinks and soups. Antihistamines
are often used to treat acute cough, but their value is questionable if an allergy is not present. They may also
cause additional drying of the respiratory mucosa. Guaifenesin is widely used in cough preparations to help
liquefy secretions and aid expectoration. Decongestants reduce secretions by causing vasoconstriction of the
nasopharyngeal mucosa. The most common decongestants found in many cough preparations are
pseudoephedrine, phenylephrine, and phenylpropanolamine. They may cause high blood pressure, restlessness,
and urinary retention and should be used with caution in anyone being treated for hypertension. Narcotics are
powerful cough suppressants, codeine being one of the most frequently used. Several safer nonnarcotic
antitussive (cough-preventing) agents are available, such as dextromethorphan, which has almost equal
effectiveness but fewer side effects. Most cough preparations containing dextromethorphan also contain a
decongestant and an expectorant. Because coughing is an important defense mechanism in clearing secretions
from blocked airways, a productive cough (one that produces secretions) should not be suppressed.
Insomnia
Insomnia is a difficulty in falling asleep or staying asleep or the feeling that sleep is not refreshing. Transient
insomnia can occur following stressful life events or schedule changes, as shift workers or those who travel
across multiple time zones experience. Disturbed sleep can also be related to the intake of stimulating drugs or
to the presence of anxiety, depression, or medical conditions associated with pain. The elderly spend less time
sleeping, and their sleep is lighter and marked by more frequent awakenings. This situation may be exacerbated
by afternoon napping.
The treatment of insomnia involves establishing good sleep hygiene: maintaining a consistent schedule of when
to retire and awaken, setting a comfortable room temperature, and minimizing disruptive stimuli such as noise
and light. Daily exercise is beneficial but should be avoided immediately before bedtime. Stimulants should be
avoided, including nicotine and caffeine. Alcohol disrupts the normal sleep pattern and should also be avoided.
Drinkers sleep more lightly and frequently awaken unknowingly, which leaves them feeling unrefreshed the next
day.
When medication is required, physicians usually prescribe one of the sleep-inducing benzodiazepines. They may
have long-, intermediate-, or ultrashort-acting effects. None should be used regularly for long periods. Various
nonbenzodiazepine hypnotics and sedatives are also available, and their usefulness varies according to
individual preference.

Britannica LaunchPacks | The Treatment and Prevention of Disease
86 of 123© 2020 Encyclopædia Britannica, Inc.
Designing a therapeutic regimenOnce the physician makes a diagnosis or identifies the most likely cause of the symptoms and decides on the
appropriate treatment, an entirely new set of conditions becomes operative. One of the first conditions to be
considered is the patient’s reason for seeking medical advice and the patient’s expectations. The patient’s visit
may have been precipitated by the feeling that a minor symptom may be something serious. If tests can rule out
this possibility, reassurance may serve as a therapeutic action. When possible, physicians work to cure a disease
and thereby relieve the symptoms, but many times the disease is unknown or chronic and incurable. In either
case, relief from or improvement of symptoms or restoration of normal functioning is the goal. When neither a
cure nor complete relief of symptoms is possible, an explanation of the disease and knowledge of the cause and
what to expect may provide significant relief. Patients often want to know the name of the disease, what caused
it, how long it will last, what additional symptoms may occur, and what they can do to assist the physician’s
treatment to hasten recovery. Providing information about the disease can help to alleviate anxiety and fears
that could otherwise impede the patient’s progress.
An essential ingredient of any successful therapeutic regimen is the positive attitude of the patient toward the
physician. A relationship of trust and respect for the physician based on reputation or years of supportive care is
one of the physician’s most powerful therapeutic tools.
When selecting a management plan, the physician usually has several options, and the outcomes or
consequences of each will vary. Often, the best choice is one made together with the patient, who may have
definite preferences for a trial of therapy over further testing or for oral medication rather than an injection,
even if the latter would provide more rapid relief. The possible side effects of the medicine or treatment may
well influence therapeutic choice, such as if a person would prefer dizziness to nausea. Once a course of therapy
is selected, a new decision tree arises that leads to new options, depending on the response. Further testing,
increasing the dose of medication, or changing to a new drug may be required. Almost every treatment has
some degree of risk, from either unwanted side effects or unexpected complications. The physician describes
these risks in terms of probability, expecting the patient to accept or reject the treatment based on these odds
and his or her willingness to suffer the side effects or to risk the complications to achieve relief.
Another factor affecting therapeutic success is patient compliance—the degree to which patients adhere to the
regimen recommended by their physician. Therapeutic regimens that require significant changes in lifestyle,
such as recommendations to follow a special diet, begin an exercise program, or discontinue harmful habits such
as smoking cigarettes, are likely to result in poor compliance. Also, the greater the number of drugs prescribed
and the more complicated the regimen, the poorer is the compliance. A patient is much more likely to
successfully follow a regimen of taking a single dose of medication daily than one prescribed four times daily.
Patients also may not fully realize the need to continue taking the medication after their symptoms have
subsided, despite a physician’s instruction to finish the medicine. Patient compliance may be most difficult to
achieve in chronic but generally asymptomatic illnesses such as hypertension. Patients who experience no
symptoms may need to be convinced of the necessity of taking their medication daily to prevent the occurrence
of an untoward event (e.g., in hypertension, a stroke or other cardiovascular problems). Similarly, patients with
depression or anxiety may want to discontinue medication once their symptoms abate. Until a relapse occurs,
they may not recognize the need to continue taking the medication until instructed to taper the dosage slowly.
In deciding which therapeutic regimen is likely to be most effective, the physician must depend on scientific
studies that compare one drug or treatment regimen with others that have been proved effective. The most
dependable study is one that is truly objective and removes the possibility of bias on the part of the patient who

Britannica LaunchPacks | The Treatment and Prevention of Disease
87 of 123© 2020 Encyclopædia Britannica, Inc.
wants the drug to work and the bias of the physician who may expect a certain outcome and subtly influence the
interpretation. Such a study is “double-blind”: it controls for both possible tendencies by comparing an active
drug with an inactive placebo (an inert drug). Neither the patient nor the physician knows which drug the patient
is taking, so that neither one’s bias can influence the result. Although this is the best way to demonstrate the
effectiveness of a drug, it is sometimes very difficult to control for all the variables that could influence the
outcome, such as varying degrees of stress one group or another may be under. Physicians will use the results
of a wide variety of clinical studies to decide whether a regimen or drug is likely to work in a given patient;
however, they will depend most heavily on their past experience with drugs or other techniques that have
worked under similar circumstances. It is knowledge based on experience and on understanding of the patient
that leads to the greatest therapeutic success.
DietProphylactic measures of nutrition
General requirements
Adequate nutritional intake is required to maintain health and prevent disease. Certain nutrients are essential;
without them a deficiency disease will result. Required nutrients that cannot be synthesized by the body and
therefore must be taken regularly include essential amino acids, water-soluble and fat-soluble vitamins,
minerals, and essential fatty acids. The U.S. Recommended Dietary Allowances (RDAs), one of many sets of
recommendations put out by various countries and organizations, have been established for these essential
nutrients by the Food and Nutrition Board of the National Academy of Sciences. The RDAs are guidelines and not
absolute minimums. Intake of less than the RDA for a given nutrient increases the risk of inadequate intake and
a deficiency disorder. Nutritional requirements are greater during the periods of rapid growth (infancy,
childhood, and adolescence) and during pregnancy and lactation. Requirements vary with physical activity,
aging, infections, medications, metabolic disorders (e.g., hyperthyroidism), and other medical situations. RDAs
do not address all circumstances and are designed only for the average healthy person.
Protein, needed to maintain body function and structure, consists of nine essential amino acids that must be
provided from different foods in a mixed diet. Ten to 15 percent of calories should come from protein. The
oxidation of 1 gram (0.036 ounce) of protein provides 4 kilocalories of energy. The same is true for
carbohydrate. Fat yields 9 kilocalories.
According to the U.S. RDAs, carbohydrate should provide about 45 to 65 percent of calories in the diet, in the
form of sugars, starches (complex carbohydrates), and dietary fibre (indigestible carbohydrates). Fibre is not
digestible but increases the bulk of the stool and facilitates faster intestinal transit. A high-fibre diet is associated
with a reduced risk of colorectal cancer, owing in part to the diminished time that cancer-producing substances
in the diet remain in contact with the bowel wall; increasing bulk also decreases the concentration of these
substances. Dietary fibre can be insoluble (wheatbran) or soluble (oat bran and psyllium). Only the soluble fibres
found in oats, fruit, and legumes lower blood cholesterol and benefit individuals with diabetes by delaying the
absorption of glucose.
The most concentrated source of energy is fat, the source of fat-soluble vitamins and essential fatty acids. More
than one-third of calories in the American diet come from fat, though the ideal is slightly less than that amount.
Most Americans also consume excess cholesterol; 200 milligrams is recommended daily.
Britannica LaunchPacks | The Treatment and Prevention of Disease
88 of 123© 2020 Encyclopædia Britannica, Inc.
Requirements in infancy
Nutritional needs are greatest during the first year of life. Meeting the energy demands during this period of
rapid growth requires 100 to 120 kilocalories per kilogram per day. Breast milk, the ideal food, is not only readily
available at the proper temperature, it also contains antibodies from the mother that help protect against
disease. Infant formulas closely approximate the contents of breast milk, and both contain about 50 percent of
calories from carbohydrate, 40 percent from fat, and 10 percent from protein.
Breast milk or commercial formula is recommended for the first six months of life and may be continued through
the first year. Solid foods are introduced at four to six months of age, starting with rice cereal and then
introducing a new vegetable, fruit, or meat each week. Cow’s milk generally is not given to infants younger than
six months of age, and low-fat milk is avoided throughout infancy, since it does not contain adequate calories
and polyunsaturated fats required for development. Additional iron and vitamins may be given, especially to
infants at high risk of iron deficiency, such as those with a low birth weight.
Toddlers are usually picky eaters, but attempts should be made to include the following four basic food groups in
their diet: meat, fish, poultry, or eggs; dairy products such as milk or cheese; fruits and vegetables; and cereals,
rice, or potatoes. Mealtime presents an opportunity for social interaction and strengthening of the family unit.
This starts with the bonding between mother and child during breast-feeding and continues as a source of family
interaction throughout childhood.
Requirements in adolescence
Nutritional needs during adolescence vary according to activity levels, with some athletes requiring an
extremely high-calorie diet. Other adolescents, however, who are relatively sedentary consume calories in
excess of their energy needs and become obese. Peer pressure and the desire for social acceptance can
profoundly affect the quality of nutrition of the adolescent as food intake may shift from the home to fast-food
establishments.
Pregnancy during adolescence can present special hazards if the pregnancy occurs before the adolescent has
finished growing and if she has established poor eating habits. Pregnancy increases the already high
requirements for calcium, iron, and vitamins in these teenagers.
Eating disorders such as anorexia nervosa and bulimia arise predominantly in young individuals as a result of
biological, psychological, and social factors. An excessive concern with body image and a fear of becoming fat
are hallmarks of these conditions. The patient with anorexia nervosa has a distorted body image and an
inordinate fear of gaining weight; consequently, he or she reduces nutritional intake below the amount needed
to maintain a normal minimal weight. Severe electrolyte disturbances and death can result. Bulimia is a
behavioral disorder marked by binge eating followed by acts of purging (e.g., self-induced vomiting, ingestion of
laxatives or diuretics, or vigorous exercising) to avoid weight gain.
Requirements of the elderly
The elderly often have decreased intestinal motility and decreased gastric acid secretion that can lead to
nutritional deficiencies. The problem can be accentuated by poorly fitting dentures, poor appetite, and a
decreased sense of taste and smell. Although lower levels of activity reduce the need for calories, older persons
may feel something is wrong if they do not have the appetite of their younger years, even if caloric intake is
adequate to maintain weight. The reduction in gastric acid secretion can lead to decreased absorption of
vitamins and other nutrients. Nutritional deficiencies can reduce the level of cognitive functioning. Vitamin
supplementation, especially with cobalamin (vitamin B ), may be particularly valuable in the elderly.12

Britannica LaunchPacks | The Treatment and Prevention of Disease
89 of 123© 2020 Encyclopædia Britannica, Inc.
The diet of the geriatric population is often deficient in calcium and iron, with the average woman ingesting only
half the amount of calcium needed daily. Decreased intake of vegetables can also contribute to various
nutritional deficiencies.
Constipation, which is common in the elderly, results from decreased intestinal motility and immobility and is
worsened by reduced fluid and fibre intake. The multiple medications that the elderly are likely to be taking may
contribute to constipation and prevent the absorption of certain nutrients. Some drugs, such as the
phenothiazines, may interfere with temperature regulation and lead to problems during hot weather, especially
if fluid intake is inadequate.
Requirements in pregnancy
The growing fetus depends on the mother for all nutrition and increases the mother’s usual demand for certain
substances such as iron, folic acid, and calcium, which should be added as supplements to a balanced diet that
contains most of the other required nutrients. The diet of adolescent girls, however, is often deficient in calcium,
iron, and vitamins. If poor nutritional habits have been established previously and are maintained during
pregnancy, the pregnant adolescent and her fetus are at increased risk.
In addition to avoiding non-nutritious foods, the pregnant woman should abstain from alcohol, smoking, and
illicit drugs, which all have a detrimental effect on the fetus. Caution should be used in taking over-the-counter
medicines during pregnancy, including vitamin and mineral supplements. Although the average recommended
weight gain during pregnancy is approximately 11.3 kilograms (25 pounds), the pregnant woman should be less
concerned with a maximum weight gain than she is with meeting the nutritional requirements of pregnancy. Low
weight gain (less than 9.1 kilograms) has been associated with intrauterine growth retardation and prematurity.
Women who are breast-feeding should continue taking vitamin supplements and increasing their intake of
calcium and protein to provide adequate breast milk. This regimen will not interfere with the mother’s ability to
slowly lose the weight gained during pregnancy.
Therapeutic measures of nutrition
Changes in diet can have a therapeutic effect on obesity, diabetes mellitus, hypertension, peptic ulcer, and
osteoporosis.
Obesity
A significant number of persons in developed countries meet the definition of obesity (20 percent above ideal
body weight). Obesity occurs when the number of calories consumed exceeds the number that is metabolized,
the remainder being stored as adipose (fat) tissue. Many theories address the causes of obesity, but no single
cause is apparent. Multiple factors influence weight, including genetic factors, hormone levels, activity levels,
metabolic rates, eating patterns, and stress.
The treatment of obesity requires reducing calorie intake while increasing calorie expenditure (exercise).
Because obesity is a chronic illness, it requires long-term lifestyle changes unless surgery is performed to effect
permanent changes in the digestion of food. Thus fad diets, no matter how effective they are in the short term,
remain inadequate for long-term weight control. A reduction in calorie intake of 500 kilocalories per day should
lead to a loss of 0.45 kilogram (1 pound) per week. This reduction can be increased by greater calorie reduction
or an accompanying exercise program. With exercise, the weight loss will be primarily fat, whereas without it,
muscle is lost as well. Exercise also leads to a “positive” addiction that makes it easier to sustain regular
exercising for long periods. It reduces the risk of heart disease and can improve self-esteem.
Britannica LaunchPacks | The Treatment and Prevention of Disease
90 of 123© 2020 Encyclopædia Britannica, Inc.
Weight-reduction diets for the obese individual should be similar to those used by nonobese persons but with
fewer calories—namely, a low-fat diet that avoids high-calorie foods. One of the most popular and successful of
these diets is the very-low-calorie diet (VLCD) that results in rapid fat loss while minimizing the loss of lean
muscle tissue. These diets require supplementation with potassium and a vitamin-mineral complex. Fad diets
that eliminate one foodstuff, such as carbohydrate or protein, may give short-term results but fail in the long
term to maintain weight loss. Furthermore, these diets can lead to medically significant problems, such as
ketosis (a buildup of ketones in the body). Fad diets promoting high protein intake, particularly those
emphasizing high meat consumption and excluding key food groups such as grains and dairy, can increase a
person’s risk of heart disease.
Appetite-suppressing drugs have limited short-term and no long-term effectiveness. Surgery can provide long-
term benefits but may not be an option for some individuals. The most frequently performed procedures are
vertical banded gastroplasty and gastric bypass, both of which reduce the size of the stomach. Gastric bypass is
effective in teenagers as well as adults, with potentially lifelong benefits in young persons, especially when
combined with behavioral changes to improve eating habits and physical activity.
Diabetes mellitus
Diet is the cornerstone of diabetic treatment whether or not insulin is prescribed. The goal is to regulate the
patient’s blood glucose level to as close to normal as possible and for the patient to achieve and maintain an
ideal weight. Refined and simple sugars are avoided, and saturated fat is reduced by focusing the diet on poultry
and fish rather than meat as a major source of protein. Soluble fibre such as that found in beans and oatmeal is
recommended in contrast to the insoluble fibre found in wheat and bran. Artificial sweeteners may be used as
low-calorie replacements for simple sugar. In order to minimize the risk of long-term consequences, diabetic
patients generally must adhere to a balanced diet with restricted saturated fat intake while maintaining normal
weight. Meals of equal caloric content may be spaced throughout the day, especially when supplemental insulin
is needed.
Hypertension
Many patients with hypertension benefit from a low-sodium diet (reduced sodium chloride [table salt] intake)
and physicians often recommend this as part of the initial therapy for hypertension. If alterations in diet fail to
counteract the hypertension, drugs such as diuretics may be prescribed along with potassium supplements
(because most diuretics may deplete potassium). Other dietary measures are directed toward achieving an ideal
body weight because obesity contributes to hypertension and increases the risk of cardiovascular disease. An
adequate low-sodium diet can be achieved with a no-added-salt diet—that is, no salt is added to food after
preparation, and foods with a high-sodium content such as cured meats are avoided. Low-sodium diets should
be combined with increased potassium, which can be obtained by eating fruits, especially bananas, and
vegetables, or using salt substitutes.
Peptic ulcer
In the past a bland diet and frequent ingestion of milk and cream were the mainstays of ulcer treatment. Today
the only dietary regimen is the avoidance of irritating foods, such as spicy and highly seasoned foods, and
coffee. Certain drug therapies can decrease gastric acidity much more than antacids and other dietary
measures. Infection of the stomach by the bacterium is recognized as a major factor in Helicobacter pylorichronic gastritis and recurrent peptic ulcer in many patients. The bacterial infection requires a treatment
regimen consisting of antibiotics and a bismuth-containing compound, which is different from the treatment of
an ulcer that is not caused by .H. pylori
Osteoporosis
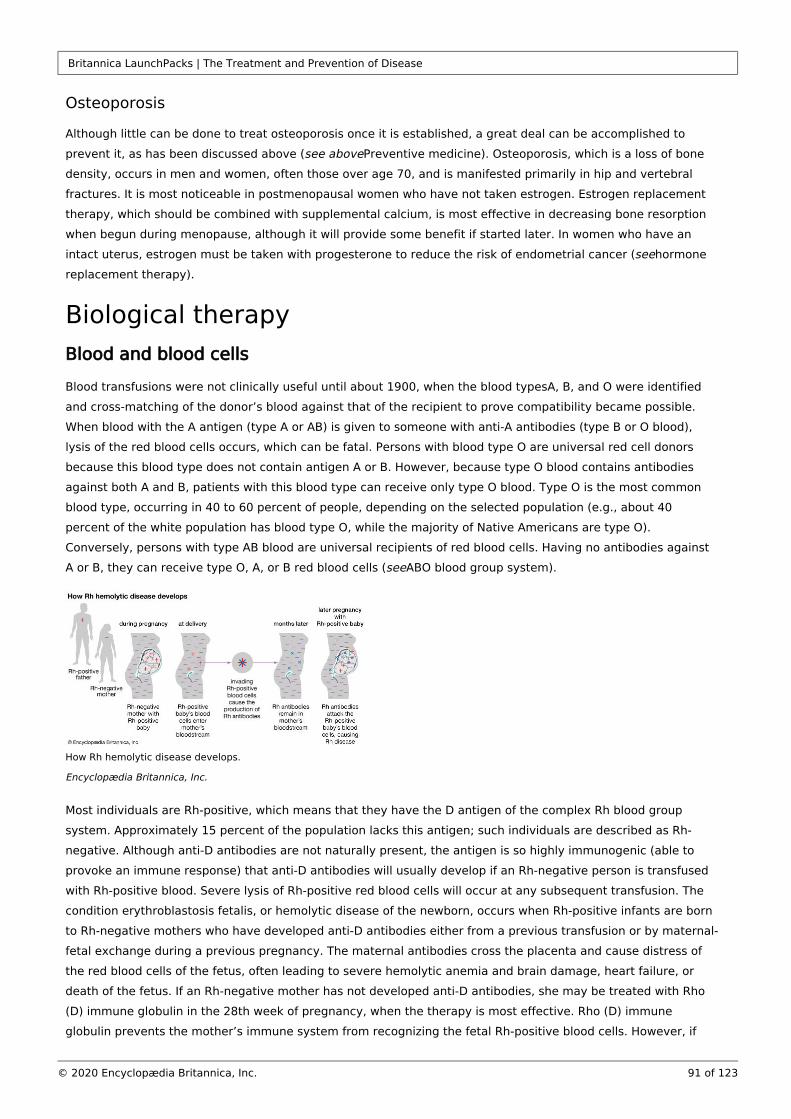
Britannica LaunchPacks | The Treatment and Prevention of Disease
91 of 123© 2020 Encyclopædia Britannica, Inc.
Osteoporosis
Although little can be done to treat osteoporosis once it is established, a great deal can be accomplished to
prevent it, as has been discussed above ( Preventive medicine). Osteoporosis, which is a loss of bone see abovedensity, occurs in men and women, often those over age 70, and is manifested primarily in hip and vertebral
fractures. It is most noticeable in postmenopausal women who have not taken estrogen. Estrogen replacement
therapy, which should be combined with supplemental calcium, is most effective in decreasing bone resorption
when begun during menopause, although it will provide some benefit if started later. In women who have an
intact uterus, estrogen must be taken with progesterone to reduce the risk of endometrial cancer ( hormone seereplacement therapy).
Biological therapyBlood and blood cells
Blood transfusions were not clinically useful until about 1900, when the blood typesA, B, and O were identified
and cross-matching of the donor’s blood against that of the recipient to prove compatibility became possible.
When blood with the A antigen (type A or AB) is given to someone with anti-A antibodies (type B or O blood),
lysis of the red blood cells occurs, which can be fatal. Persons with blood type O are universal red cell donors
because this blood type does not contain antigen A or B. However, because type O blood contains antibodies
against both A and B, patients with this blood type can receive only type O blood. Type O is the most common
blood type, occurring in 40 to 60 percent of people, depending on the selected population (e.g., about 40
percent of the white population has blood type O, while the majority of Native Americans are type O).
Conversely, persons with type AB blood are universal recipients of red blood cells. Having no antibodies against
A or B, they can receive type O, A, or B red blood cells ( ABO blood group system).see
How Rh hemolytic disease develops.
Encyclopædia Britannica, Inc.
Most individuals are Rh-positive, which means that they have the D antigen of the complex Rh blood group
system. Approximately 15 percent of the population lacks this antigen; such individuals are described as Rh-
negative. Although anti-D antibodies are not naturally present, the antigen is so highly immunogenic (able to
provoke an immune response) that anti-D antibodies will usually develop if an Rh-negative person is transfused
with Rh-positive blood. Severe lysis of Rh-positive red blood cells will occur at any subsequent transfusion. The
condition erythroblastosis fetalis, or hemolytic disease of the newborn, occurs when Rh-positive infants are born
to Rh-negative mothers who have developed anti-D antibodies either from a previous transfusion or by maternal-
fetal exchange during a previous pregnancy. The maternal antibodies cross the placenta and cause distress of
the red blood cells of the fetus, often leading to severe hemolytic anemia and brain damage, heart failure, or
death of the fetus. If an Rh-negative mother has not developed anti-D antibodies, she may be treated with Rho
(D) immune globulin in the 28th week of pregnancy, when the therapy is most effective. Rho (D) immune
globulin prevents the mother’s immune system from recognizing the fetal Rh-positive blood cells. However, if
Britannica LaunchPacks | The Treatment and Prevention of Disease
92 of 123© 2020 Encyclopædia Britannica, Inc.
the mother develops antibodies, the fetus and the mother must be closely monitored. If delivery occurs at the
normal time following a full-length pregnancy, the infant may receive a blood transfusion to replace damaged or
diseased red blood cells with healthy blood cells. Early delivery, however, is often necessary, and in severe
cases, blood transfusion in the womb is performed.
Whole blood, which contains red blood cells, plasma, platelets, and coagulation factors, is almost never used for
transfusions because most transfusions only require specific blood components. It can be used only up to 35
days after it has been drawn and is not always available, because most units of collected blood are used for
obtaining components.
Packed red blood cells are what remains of whole blood after the plasma and platelets have been removed. A
450-millilitre unit of whole blood is reduced to a 220-millilitre volume. Packed red blood cells are used most often
to raise a low hemoglobin or hematocrit level in patients with chronic anemia or mild hemorrhage.
Leukocyte-poor red blood cells are obtained by employing a filter to remove white blood cells (leukocytes) from
a unit of packed red blood cells. This type of transfusion is used to prevent febrile (fever) reactions in patients
who have had multiple febrile transfusion reactions in the past, presumably to white blood cell antigens.
Removal of leukocytes from blood components is referred to as leukocyte reduction, or leukoreduction. In
addition to lowering the risk of febrile transfusion reactions, leukoreduced blood components may have a
decreased chance of transmitting cytomegalovirus, a member of the herpesvirus family, as well as other strictly
cell-associated viruses. Transfusion using leukoreduced blood components also reduces the risk of immunization
to white cells and to platelet antigens and perhaps reduces the risk of the immunosuppressive effects of
transfusion.
A micrograph of a round aggregation of platelets (magnified 1,000×).
Dr. F. Gilbert/Centers for Disease Control and Prevention (CDC) (Image Number: 6645)
Platelet transfusions are used to prevent bleeding in patients with very low platelet counts, usually less than
20,000 cells per microlitre, and in those undergoing surgery or other invasive procedures whose counts are less
than 50,000 cells per microlitre.
Autologous transfusion is the reinfusion of one’s own blood. The blood is obtained before surgery and its use
avoids transfusion reactions and transfusion-transmitted diseases. Donation can begin one month before surgery
and be repeated weekly, depending on the number of units likely to be needed. Intraoperative blood salvage is
another form of autologous transfusion. The intraoperative blood salvage device recovers the shed blood, which
is then anticoagulated, centrifuged to concentrate the red blood cells, and washed in a sterile centrifuge bowl.
The salvaged blood (primarily washed red cells) can be rapidly infused into the patient during surgical
procedures.
Plasma
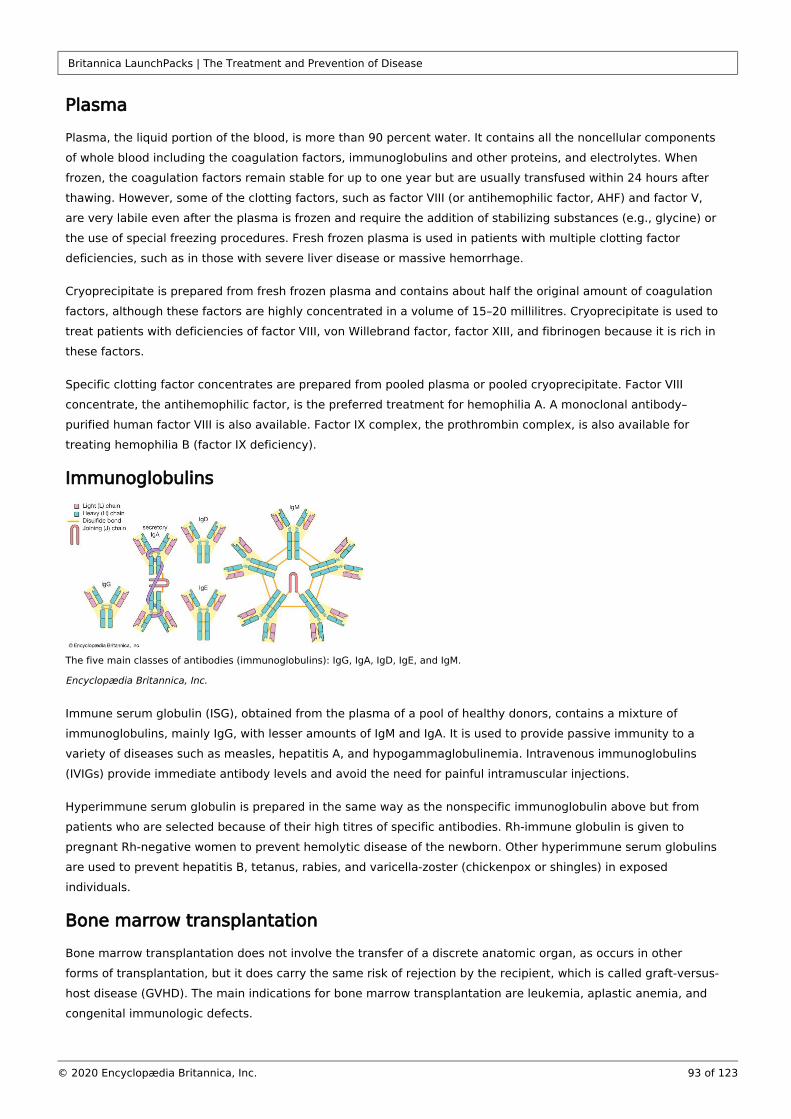
Britannica LaunchPacks | The Treatment and Prevention of Disease
93 of 123© 2020 Encyclopædia Britannica, Inc.
Plasma
Plasma, the liquid portion of the blood, is more than 90 percent water. It contains all the noncellular components
of whole blood including the coagulation factors, immunoglobulins and other proteins, and electrolytes. When
frozen, the coagulation factors remain stable for up to one year but are usually transfused within 24 hours after
thawing. However, some of the clotting factors, such as factor VIII (or antihemophilic factor, AHF) and factor V,
are very labile even after the plasma is frozen and require the addition of stabilizing substances (e.g., glycine) or
the use of special freezing procedures. Fresh frozen plasma is used in patients with multiple clotting factor
deficiencies, such as in those with severe liver disease or massive hemorrhage.
Cryoprecipitate is prepared from fresh frozen plasma and contains about half the original amount of coagulation
factors, although these factors are highly concentrated in a volume of 15–20 millilitres. Cryoprecipitate is used to
treat patients with deficiencies of factor VIII, von Willebrand factor, factor XIII, and fibrinogen because it is rich in
these factors.
Specific clotting factor concentrates are prepared from pooled plasma or pooled cryoprecipitate. Factor VIII
concentrate, the antihemophilic factor, is the preferred treatment for hemophilia A. A monoclonal antibody–
purified human factor VIII is also available. Factor IX complex, the prothrombin complex, is also available for
treating hemophilia B (factor IX deficiency).
Immunoglobulins
The five main classes of antibodies (immunoglobulins): IgG, IgA, IgD, IgE, and IgM.
Encyclopædia Britannica, Inc.
Immune serum globulin (ISG), obtained from the plasma of a pool of healthy donors, contains a mixture of
immunoglobulins, mainly IgG, with lesser amounts of IgM and IgA. It is used to provide passive immunity to a
variety of diseases such as measles, hepatitis A, and hypogammaglobulinemia. Intravenous immunoglobulins
(IVIGs) provide immediate antibody levels and avoid the need for painful intramuscular injections.
Hyperimmune serum globulin is prepared in the same way as the nonspecific immunoglobulin above but from
patients who are selected because of their high titres of specific antibodies. Rh-immune globulin is given to
pregnant Rh-negative women to prevent hemolytic disease of the newborn. Other hyperimmune serum globulins
are used to prevent hepatitis B, tetanus, rabies, and varicella-zoster (chickenpox or shingles) in exposed
individuals.
Bone marrow transplantation
Bone marrow transplantation does not involve the transfer of a discrete anatomic organ, as occurs in other
forms of transplantation, but it does carry the same risk of rejection by the recipient, which is called graft-versus-
host disease (GVHD). The main indications for bone marrow transplantation are leukemia, aplastic anemia, and
congenital immunologic defects.
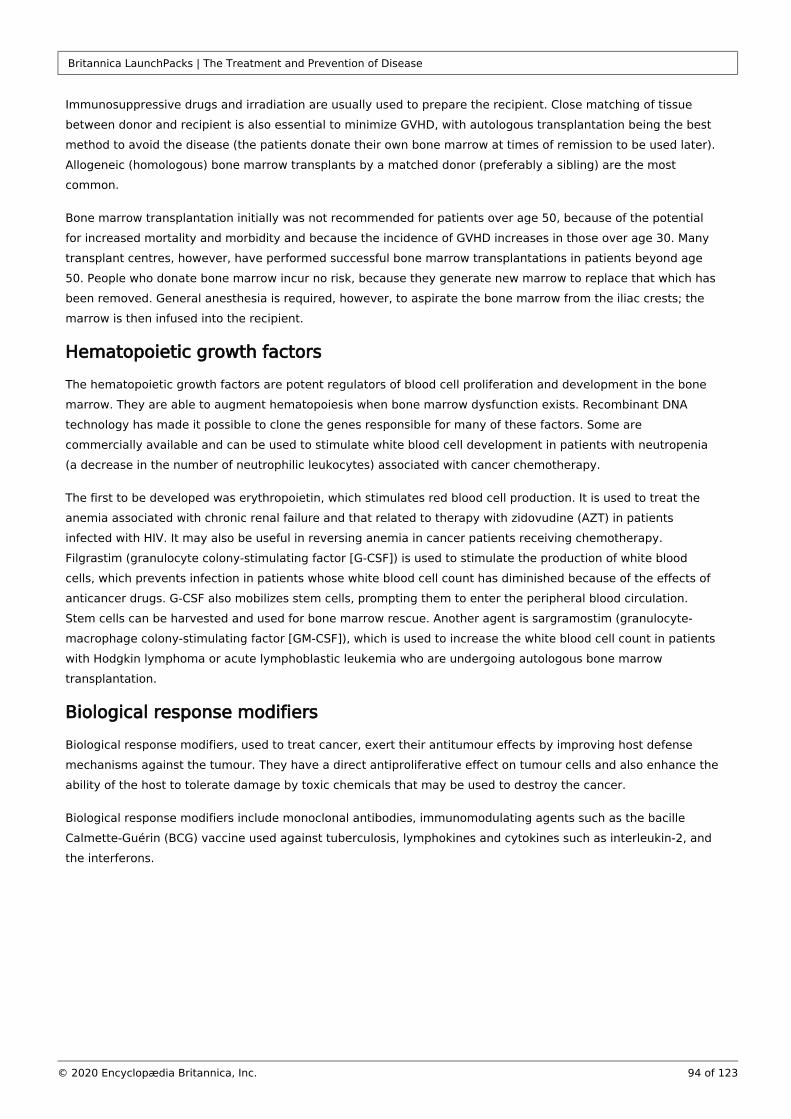
Britannica LaunchPacks | The Treatment and Prevention of Disease
94 of 123© 2020 Encyclopædia Britannica, Inc.
Immunosuppressive drugs and irradiation are usually used to prepare the recipient. Close matching of tissue
between donor and recipient is also essential to minimize GVHD, with autologous transplantation being the best
method to avoid the disease (the patients donate their own bone marrow at times of remission to be used later).
Allogeneic (homologous) bone marrow transplants by a matched donor (preferably a sibling) are the most
common.
Bone marrow transplantation initially was not recommended for patients over age 50, because of the potential
for increased mortality and morbidity and because the incidence of GVHD increases in those over age 30. Many
transplant centres, however, have performed successful bone marrow transplantations in patients beyond age
50. People who donate bone marrow incur no risk, because they generate new marrow to replace that which has
been removed. General anesthesia is required, however, to aspirate the bone marrow from the iliac crests; the
marrow is then infused into the recipient.
Hematopoietic growth factors
The hematopoietic growth factors are potent regulators of blood cell proliferation and development in the bone
marrow. They are able to augment hematopoiesis when bone marrow dysfunction exists. Recombinant DNA
technology has made it possible to clone the genes responsible for many of these factors. Some are
commercially available and can be used to stimulate white blood cell development in patients with neutropenia
(a decrease in the number of neutrophilic leukocytes) associated with cancer chemotherapy.
The first to be developed was erythropoietin, which stimulates red blood cell production. It is used to treat the
anemia associated with chronic renal failure and that related to therapy with zidovudine (AZT) in patients
infected with HIV. It may also be useful in reversing anemia in cancer patients receiving chemotherapy.
Filgrastim (granulocyte colony-stimulating factor [G-CSF]) is used to stimulate the production of white blood
cells, which prevents infection in patients whose white blood cell count has diminished because of the effects of
anticancer drugs. G-CSF also mobilizes stem cells, prompting them to enter the peripheral blood circulation.
Stem cells can be harvested and used for bone marrow rescue. Another agent is sargramostim (granulocyte-
macrophage colony-stimulating factor [GM-CSF]), which is used to increase the white blood cell count in patients
with Hodgkin lymphoma or acute lymphoblastic leukemia who are undergoing autologous bone marrow
transplantation.
Biological response modifiers
Biological response modifiers, used to treat cancer, exert their antitumour effects by improving host defense
mechanisms against the tumour. They have a direct antiproliferative effect on tumour cells and also enhance the
ability of the host to tolerate damage by toxic chemicals that may be used to destroy the cancer.
Biological response modifiers include monoclonal antibodies, immunomodulating agents such as the bacille
Calmette-Guérin (BCG) vaccine used against tuberculosis, lymphokines and cytokines such as interleukin-2, and
the interferons.
Britannica LaunchPacks | The Treatment and Prevention of Disease
95 of 123© 2020 Encyclopædia Britannica, Inc.
Three vials filled with human leukocyte interferon.
National Institutes of Health
The three major classes of interferons are interferon-α, produced by white blood cells; interferon-β, produced by
fibroblasts; and interferon-γ, produced by lymphocytes. The interferons are proteins produced by these cells in
response to viral infections or other stimuli; they have antiviral, antiproliferative, and immunomodulatory
properties that make them useful in treating some viral infections and cancers. They do not act directly on the
viruses but rather indirectly, increasing the resistance of cells to viral infections. This can be particularly useful in
patients who have an impaired immune system and a diminished ability to fight viral infections, especially those
with AIDS.
Interferon-α is produced by a recombinant DNA process using genetically engineered . Escherichia coliRecombinant interferon-α appears to be most effective against hairy-cell leukemia and chronic myelogenous
leukemia, lymphoma, multiple myeloma, AIDS-associated Kaposi sarcoma, and chronic hepatitis C. It is
moderately effective in treating melanoma, renal cell carcinoma, and carcinoid. It also can enhance the
effectiveness of chemotherapy in some cancers. Unfortunately, treatment with this drug can be quite toxic.
Interferon-γ may prove useful in treating a different set of diseases—for example, chronic conditions such as
rheumatoid arthritis.
Hormones
The term is derived from the Greek , meaning “to set in motion.” It refers to a chemical hormone hormaeinsubstance that has a regulatory effect on a certain organ or organs. There are sex hormones such as estrogen
and progesterone, thyroid hormones, insulin, adrenal cortical and pituitary hormones, and growth hormones.
Estrogens (estradiol, estone, and estriol) promote the growth and development of the female reproductive
system—the vagina, uterus, and fallopian tubes—and the breasts. They are responsible for the development of
secondary sex characteristics—growth of pubic and axillary hair and pigmentation of the nipples and genitals—
and contribute to bone formation. The decrease in estrogen after menopause contributes to bone
demineralization and osteoporosis, and hormone replacement therapy is often recommended to counteract this
occurrence. Postmenopausal estrogen also prevents atrophic vaginitis, in which the vaginal mucosa becomes
thin and friable. Estrogens can be administered orally, transdermally (through the skin), vaginally, or
intramuscularly.
Progestins combined with estrogens constitute the oral contraceptives that inhibit ovulation by affecting the
hypothalamus and pituitary. Progestin-only pills and injections are also effective contraceptives; they work by
forming a thick cervical mucus that is relatively impenetrable to sperm. The mortality associated with all forms

Britannica LaunchPacks | The Treatment and Prevention of Disease
96 of 123© 2020 Encyclopædia Britannica, Inc.
of birth control is less than that associated with childbirth, except for women older than age 35 who smoke
cigarettes. Their risk of stroke, heart attacks, and other cardiovascular problems is greatly increased, so their
use of oral contraceptives is contraindicated. Levonorgestrel is a form of synthetic progestin that provides birth
control.
Androgens consist of testosterone and its derivatives, the anabolic steroids. Testosterone is produced in the
testes in males, and small amounts are produced by the ovary and adrenal cortex in females. Testosterone is
used to stimulate sexual organ development in androgen-deficient males and to initiate puberty in selected boys
with delayed growth. The anabolic steroids are testosterone derivatives that provide anabolic activity with less
stimulation of growth of the sexual organs. Anabolic steroids have been used to increase muscle strength and
endurance. However, this practice can have serious long-term consequences, such as the development of
atherosclerotic disease because of the steroids’ effects on the blood lipids, especially the lowering of high-
density lipoproteins. Their use in juvenile athletes can cause premature epiphyseal closure (early ossification of
the growth zone of bones), compromising the attainment of their full adult height, and can have an impact on
sexual development.
Human chorionic gonadotropin (HCG), a hormone produced by cells of the placenta, can be extracted from the
urine of pregnant women days after fertilization and thus is used in the early detection of pregnancy. It is also
used to stimulate descent of the testicles in boys with prepubertal cryptorchidism and to treat infertility in men
with underdeveloped testicles.
Growth hormone, produced by the pituitary gland, stimulates linear growth and regulates metabolic functions.
Inadequate secretion of this hormone by the pituitary will impair growth in children, which is evidenced by their
poor rate of growth and delayed bone age (i.e., slowed bone development). A synthetic preparation of the
hormone is used to treat children who have a congenital deficiency of growth hormone.
Adrenal corticosteroids are any of the steroid hormones produced by the adrenal cortex except for the sex
hormones. These include the mineralocorticoids (aldosterone) and glucocorticoids (cortisol), the secretion of
which is regulated by the adrenocorticotrophic hormone (ACTH) produced in the anterior pituitary.
Overproduction of ACTH by the pituitary gland leads to excessive secretion of glucocorticoids from the adrenal
gland, resulting in Cushing syndrome. This syndrome also can result from an increased concentration of
corticosteroids secreted by benign and malignant tumours of the adrenal gland. Conversely, the production of an
insufficient amount of adrenal corticosteroids results in primary adrenocortical insufficiency (Addison disease).
The glucocorticoids are used primarily for their potent anti-inflammatory effects in rheumatic disorders, collagen
diseases, dermatologic diseases, allergic disorders, and respiratory diseases and for the palliative management
of leukemia and lymphoma. Cortisone and hydrocortisone are less potent than prednisone and triamcinolone,
whereas dexamethasone and betamethasone have the greatest anti-inflammatory potency. Disadvantages of
corticosteroid use include the masking of signs of infection, an increase in the risk of peptic ulcer, the
development of edema and muscle weakness, the loss of bone substance (osteoporosis), and glucose
intolerance resembling diabetes mellitus.
Insulin, secreted by the pancreas, is the principal hormone governing glucose metabolism. Insulin preparations
were extracted from beef or pork pancreas until recombinant DNA technology made it possible to manufacture
human insulin. Other antidiabetic agents are also available for treating type 2 diabetes. The sulfonylureas are
oral hypoglycemic agents used as adjuncts to diet and exercise in the treatment of type 2 diabetes.
Thyroid hormones include thyroxine and triiodothyronine, which regulate tissue metabolism. Natural desiccated
thyroid produced from beef and pork and the synthetic derivatives levothyroxine and liothyronine are used in
replacement therapy to treat hypothyroidism that results from any cause.
Britannica LaunchPacks | The Treatment and Prevention of Disease
97 of 123© 2020 Encyclopædia Britannica, Inc.
Drug therapyGeneral features
Principles of druguptake and distribution
Study of the factors that influence the movement of drugs throughout the body is called pharmacokinetics,
which includes the absorption, distribution, localization in tissues, biotransformation, and excretion of drugs. The
study of the actions of the drugs and their effects is called pharmacodynamics. Before a drug can be effective, it
must be absorbed and distributed throughout the body. Drugs taken orally may be absorbed by the intestines at
different rates, some being absorbed rapidly, some more slowly. Even rapidly absorbed drugs can be prepared in
ways that slow the degree of absorption and permit them to remain effective for 12 hours or longer. Drugs
administered either intravenously or intramuscularly bypass problems of absorption, but dosage calculation is
more critical.
Individuals respond differently to the same drug. Elderly persons, because of reduced kidney and liver function,
may metabolize and excrete drugs more slowly. Because of this and other factors, the elderly usually require
lower doses of medication than do younger people.
Other factors that affect the individual’s response to drugs are the presence of disease, degree of nutrition or
malnutrition, genetics, and the presence of other drugs in the system. Furthermore, just as the pain threshold
varies among individuals, so does the response to drugs. Some people need higher-than-average doses; some,
being very sensitive to drugs, cannot tolerate even average doses, and they experience side effects when others
do not.
Infants and children may have different rates of absorption than adults because bowel motility is irregular or
gastric acidity is decreased. Drug distribution may be different in some people, such as premature infants who
have little fatty tissue and a greater proportion of body water. Metabolic rates, which affect pharmacokinetics,
are much higher during childhood. The dosages of drugs for children are usually calculated on the basis of
weight (milligrams per kilogram) or on the basis of body surface area (milligrams per square metre). If a drug
has a wide margin of safety, it may be given as a fraction of the adult dose based on age, but the great variation
in size among children of the same age complicates this computation. Children are not small adults, and drug
dosages may be quite different than they are for adults.
The elderly are particularly susceptible to adverse drug effects because they often have multiple illnesses that
require their taking various medications, some of which may be incompatible with others. In addition to
decreased renal and hepatic function, gastric acid secretion decreases with age, and arteriosclerosis narrows the
arteries, decreasing blood flow to the intestines and other organs. The precautions followed in prescribing
medication for the elderly are an excellent example of the principle that should govern all drug therapy—drugs
should be used in the lowest effective dose, especially because side effects increase with concentration.
Because of illness or frailty, elderly people often have less reserve and may not be able to tolerate minor side
effects that younger adults might not even notice.
When drugs are given in repeated doses, a steady state is achieved: the amount being administered equals the
amount being excreted or metabolized. With some drugs, however, it may be difficult to determine the proper
dose because of individual variations. In these cases, determining the plasma level of the drug may be useful,
especially if the therapeutic window (i.e., the concentration above which the drug is toxic and below which it is
ineffective) is relatively small. Plasma levels of phenytoin, used to control epilepsy; digitalis, prescribed to
combat heart failure; and lithium, used to moderate bipolar disorder, are often monitored to ensure safety.
Britannica LaunchPacks | The Treatment and Prevention of Disease
98 of 123© 2020 Encyclopædia Britannica, Inc.
Indications for use
The purpose of using drugs is to relieve symptoms, treat infection, reduce the risk of future disease, and destroy
selected cells such as in the chemotherapeutic treatment of cancer. The best treatment, however, may not
require a drug at all. Recognizing that no effective medication exists is just as important as knowing which one
to select. When more than one drug is useful, physicians select the one that is most effective and least
hazardous. A recently developed drug may promise better results, yet it will be less predictable and possibly
more expensive.
Every drug has multiple actions: it will affect organs and systems beyond those to which it is specifically
targeted. Some patients may also experience idiosyncratic effects (abnormal reactions peculiar to that
individual) as well as allergic reactions to certain drugs—additional reasons to select drugs carefully and avoid
their use altogether when simpler measures will work. A case in point is the belief that penicillin or other
antibiotics will cure viral infections—they will not. While new antiviral drugs are under development, using
antibiotics unnecessarily is unwise and potentially dangerous. The number of drug-resistant organisms is
growing and must be counteracted by the judicious prescribing of these chemicals.
Unnecessary drug use also increases the possibility of drug interactions that may interfere with drug
effectiveness. Interaction can occur in the stomach or intestinal tract where the presence of one drug may
interfere with the absorption of another. Antacids, for example, reduce the absorption of the antibiotic
tetracycline by forming insoluble complexes. Of greater importance is the interference of one drug with another.
Some drugs can inhibit the metabolism of another drug, which allows the amount of the drug to accumulate in
the system, leading to potential toxicity if the dose is not decreased. Cimetidine, a drug used to treat peptic
ulcers, causes few side effects by itself, but it does inhibit drug-metabolizing microsomal enzymes in the liver,
increasing concentrations of many drugs that depend on these enzymes to be metabolized. This inhibition can
be serious if the other drug is the anticoagulant warfarin. Bleeding can result if the dose is not reduced. Many
other drugs are affected, such as antihypertensives (e.g., calcium channel blockers), antiarrhythmics (e.g.,
quinidine), and anticonvulsants (e.g., phenytoin). One drug can also decrease the renal excretion of another.
Sometimes this effect is used to advantage, as, for example, when probenecid is given with penicillin to
decrease its removal and thereby increase its concentration in the blood. But this type of interaction can be
deadly: quinidine, for instance, can reduce the clearance of digoxin, a drug used to treat heart failure, potentially
increasing its concentration to dangerous levels. Two drugs can also have additive effects, leading to toxicity,
though either one alone would be therapeutic.
Problems with drug interactions can occur when a patient is being treated by different physicians and one
physician is not aware of the drug(s) that another has prescribed. Sometimes a physician may prescribe a drug
to treat a symptom that actually is a side effect of another drug. Discontinuing the first drug is preferable to
adding another that may have side effects of its own. When a new symptom occurs, a recently initiated drug
usually is suspected before other causes are investigated. Patients are advised to inform their physicians of any
new drugs they are taking, as well as consult with the pharmacist about possible interactions that a
nonprescription drug might have with a prescription drug already being taken. Having a personal physician who
monitors all the drugs, both prescription and nonprescription, that the patient is taking is a wise course to follow.
In the United States, responsibility for assuring the safety and efficacy of prescription drugs is delegated to the
Food and Drug Administration (FDA). This includes the approval of new drugs, identification of new indications,
official labeling (to prevent unwarranted claims), surveillance of adverse drug reactions, and approval of
methods of manufacture. Before an investigational new drug (IND) can be tested in humans, it must be
submitted to and approved by the FDA. If clinical trials are successful, a new drug application (NDA) must be

Britannica LaunchPacks | The Treatment and Prevention of Disease
99 of 123© 2020 Encyclopædia Britannica, Inc.
approved before it can be licensed and sold. This process usually takes years, but if the drug provides benefit to
patients with life-threatening illnesses when existing treatments do not, then accelerated approval is possible.
Physicians can receive permission to use an unapproved drug for a single patient. This consent, called
emergency use and sometimes referred to as single-patient compassionate use, is granted if the situation is
desperate and no other treatment is available. The FDA also sometimes grants approval to acquire drugs from
other countries that are not available in the United States if a life-threatening situation seems to warrant this
action. Another way to gain access to an investigational drug is to participate in a clinical trial. If it is a well-
controlled, randomized, double-blind trial rather than an “open trial”—in which the investigator is not “blinded”
and knows who is the subject and who is the control—the patient runs the risk of being given a placebo rather
than the active drug. The Federal Trade Commission (FTC) has responsibility for “truth in advertising” to assure
that false or misleading claims are not made about foods, over-the-counter drugs, or cosmetics.
Similar drug regulatory agencies exist in other countries and governing bodies as well. For example, China has
its own Food and Drug Administration, which regulates drugs, medical devices, and cosmetics. In Europe the
European Medicines Agency approves drugs, while also overseeing the scientific evaluation of medicines and
monitoring the safety and effectiveness of drugs marketed within countries in the European Union.
A rare disease presents a unique problem in treatment because the number of patients with the disease is so
small that it is not worthwhile for companies to go through the lengthy and expensive process required for
approval and marketing. In the United States, drugs produced for such cases are made available under the
Orphan Drug Act of 1983, which was intended to stimulate the development of drugs for rare diseases.
Controlled substances are drugs that foster dependence and have the potential for abuse. In the United States,
the Drug Enforcement Administration (DEA) regulates their manufacture, prescribing, and dispensing. Controlled
substances are divided into five classes, or schedules, based on their potential for abuse or physical and
psychological dependence. Schedule I encompasses heroin and other drugs with a high potential for abuse and
no accepted medical use in the United States. Schedule II drugs, including narcotics such as opium and cocaine
and stimulants such as amphetamines, have a high potential for abuse and dependence. Schedule III includes
those drugs such as certain stimulants, depressants, barbiturates, and preparations containing limited amounts
of codeine that cause moderate dependence. Schedule IV contains drugs that have limited potential for abuse or
dependence, and includes some sedatives, antianxiety agents, and nonnarcotic analgesics. Schedule V drugs
have an even lower potential for abuse than do schedule IV substances. Some, such as cough medicines and
antidiarrheal agents containing limited amounts of codeine, can be purchased without a prescription. Physicians
must have a DEA registration number to prescribe any controlled substance. Special triplicate prescription forms
are required in certain states for schedule II drugs, and a patient’s supply of these drugs cannot be replenished
without a new prescription. Similar drug enforcement agencies exist in other countries and international regions
as well, including the European Union, where illicit drug use and drug trafficking are policed by the European
Drug Enforcement Agency.
Systemic drug therapy
Systemic drug therapy involves treatment that affects the body as a whole or that acts specifically on systems
that involve the entire body, such as the cardiovascular, respiratory, gastrointestinal, or nervous systems.
Mental disorders also are treated systemically.
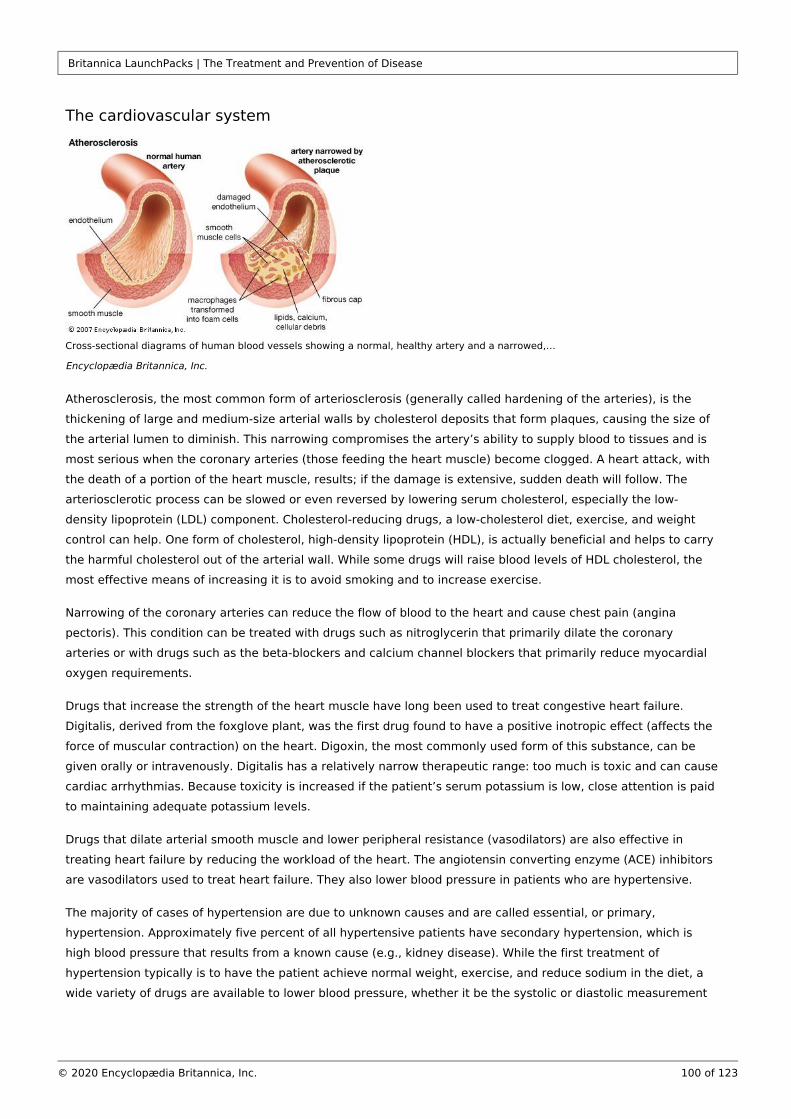
Britannica LaunchPacks | The Treatment and Prevention of Disease
100 of 123© 2020 Encyclopædia Britannica, Inc.
The cardiovascular system
Cross-sectional diagrams of human blood vessels showing a normal, healthy artery and a narrowed,…
Encyclopædia Britannica, Inc.
Atherosclerosis, the most common form of arteriosclerosis (generally called hardening of the arteries), is the
thickening of large and medium-size arterial walls by cholesterol deposits that form plaques, causing the size of
the arterial lumen to diminish. This narrowing compromises the artery’s ability to supply blood to tissues and is
most serious when the coronary arteries (those feeding the heart muscle) become clogged. A heart attack, with
the death of a portion of the heart muscle, results; if the damage is extensive, sudden death will follow. The
arteriosclerotic process can be slowed or even reversed by lowering serum cholesterol, especially the low-
density lipoprotein (LDL) component. Cholesterol-reducing drugs, a low-cholesterol diet, exercise, and weight
control can help. One form of cholesterol, high-density lipoprotein (HDL), is actually beneficial and helps to carry
the harmful cholesterol out of the arterial wall. While some drugs will raise blood levels of HDL cholesterol, the
most effective means of increasing it is to avoid smoking and to increase exercise.
Narrowing of the coronary arteries can reduce the flow of blood to the heart and cause chest pain (angina
pectoris). This condition can be treated with drugs such as nitroglycerin that primarily dilate the coronary
arteries or with drugs such as the beta-blockers and calcium channel blockers that primarily reduce myocardial
oxygen requirements.
Drugs that increase the strength of the heart muscle have long been used to treat congestive heart failure.
Digitalis, derived from the foxglove plant, was the first drug found to have a positive inotropic effect (affects the
force of muscular contraction) on the heart. Digoxin, the most commonly used form of this substance, can be
given orally or intravenously. Digitalis has a relatively narrow therapeutic range: too much is toxic and can cause
cardiac arrhythmias. Because toxicity is increased if the patient’s serum potassium is low, close attention is paid
to maintaining adequate potassium levels.
Drugs that dilate arterial smooth muscle and lower peripheral resistance (vasodilators) are also effective in
treating heart failure by reducing the workload of the heart. The angiotensin converting enzyme (ACE) inhibitors
are vasodilators used to treat heart failure. They also lower blood pressure in patients who are hypertensive.
The majority of cases of hypertension are due to unknown causes and are called essential, or primary,
hypertension. Approximately five percent of all hypertensive patients have secondary hypertension, which is
high blood pressure that results from a known cause (e.g., kidney disease). While the first treatment of
hypertension typically is to have the patient achieve normal weight, exercise, and reduce sodium in the diet, a
wide variety of drugs are available to lower blood pressure, whether it be the systolic or diastolic measurement

Britannica LaunchPacks | The Treatment and Prevention of Disease
101 of 123© 2020 Encyclopædia Britannica, Inc.
that is too high. A stepped-care approach has traditionally been used, starting with a single, well-tolerated drug,
such as a diuretic. If it proves inadequate, a second drug is added and the combination manipulated until the
most effective regimen with the fewest side effects is found. Occasionally, a third drug may be necessary.
The respiratory system
The drugs most frequently used for respiratory treatment are those that relieve cough in acute bronchitis.
Antibiotics are effective only if the cause is bacterial. Most often, however, a virus is responsible, and the
symptoms rather than the cause of the disease are treated, primarily with drugs that loosen or liquefy thick
mucus (expectorants) and humidification (steam) that soothes the irritated mucous lining. While these
treatments are widely prescribed, they have not been proven effective clinically. Likewise, although cough
suppressants are used to reduce unnecessary coughing, they subvert the cough’s natural protective mechanism
of ridding the airway of secretions and foreign substances. A commonly used non-opioid cough suppressant is
dextromethorphan, which is nearly as effective as codeine and is available in over-the-counter preparations. If
nasal congestion and postnasal drainage are present, an antihistamine and decongestant may be useful.
Asthma is a narrowing of the airways characterized by episodic wheezing. Bronchodilators are effective in a mild
to moderate attack. Frequent attacks require long-term treatment with anti-inflammatory drugs such as
cromolyn sodium, nedocromil sodium, or a corticosteroid.
Chronic obstructive pulmonary disease (COPD) manifests late in life with chronic cough and shortness of breath.
Although most of the damage has already occurred, some benefit can still be obtained by stopping smoking,
using bronchodilators, and administering antibiotics early when superimposed infection occurs. Supplemental
oxygen therapy is used in severe cases.
The gastrointestinal system
Drugs are frequently used to reduce lower bowel activity when diarrhea occurs or to increase activity if
constipation is the problem. Laxatives in the form of stimulants (e.g., cascara sagrada), bulk-forming agents (e.
g., psyllium seed), osmotics (e.g., milk of magnesia), or lubricants (e.g., mineral oil) are commonly used.
Diarrhea must be treated with appropriate antibiotics if the cause is bacterial, as in traveler’s diarrhea, or with
an antiparasitic agent if a parasite is to blame. Antidiarrheal agents include narcotics (codeine, paregoric),
nonnarcotic analogs (loperamide hydrochloride), and bismuth subsalicylate (Pepto-Bismol).
Chronic gastritis and recurrent peptic ulcer often result from infection with and are treated Helicobacter pyloriwith antibiotics and bismuth. Ulcers not caused by are treated with drugs that reduce the secretion of H. pylorigastric acid, such as the H -receptor antagonists (e.g., cimetidine), or agents that form a barrier protecting the 2
stomach against the acid (e.g., sucralfate). Antacids are used for additional symptomatic relief.
Nausea and vomiting are protective reflexes that should not be totally suppressed without the underlying cause
being known. They may be psychogenic or caused by gastrointestinal or central nervous system disorders,
medications, or systemic conditions (pregnancy or diabetic acidosis). Among the most widely used antiemetics
are the phenothiazines (e.g., Compazine), but new drugs continue to be developed that help control the
vomiting related to cancer chemotherapy.
The nervous system
Alzheimer disease is the most prevalent form of dementia (loss of intellectual function), and treatment had been
primarily supportive until drugs that showed modest promise for improving cognition (e.g., tacrine) were
Britannica LaunchPacks | The Treatment and Prevention of Disease
102 of 123© 2020 Encyclopædia Britannica, Inc.
developed. Evidence that the continual use of cognitive faculties slows memory loss in the elderly has been
supported by research showing that older persons who are stimulated regularly with memory exercises retain
information better than those who are not.
Parkinsonism, named after English surgeon James Parkinson, who described the condition in 1817 as “the
shaking palsy,” is a chronic neurological disorder involving progressive loss of motor function. Although no
treatment is known to halt the advance of the disease, levodopa and certain other drugs can significantly relieve
the symptoms of tremor, muscular rigidity, and postural instability.
Migraine, a condition thought to arise in part from abnormal neurophysiological responses, can be alleviated by
one of the many forms of ergotamine and nonsteroidal anti-inflammatory drugs (NSAIDs). Sumatriptan is a drug
that has significantly improved the treatment of severe migraine attacks, causing fewer side effects than
ergotamine or dihydroergotamine.
Mental disorders
Some of the greatest recent advances in pharmacotherapy have been in the treatment of anxiety disorders and
depression. The benzodiazepines were the mainstay of treatment for anxiety disorders beginning in the 1960s,
although their prolonged use incurs the risk of mild dependence. The azapirones (e.g., buspirone) have little
potential for producing dependency and are not affected by alcohol intake. Newer and safer medications are also
available for treating panic disorder and obsessive-compulsive disorder.
Depression is among the most common life-threatening diseases, and considerable advances have been made in
managing this disorder. The selective serotonin reuptake inhibitors (SSRIs), such as Prozac, match previous
antidepressants in effectiveness and have fewer unpleasant side effects. They also are safer if an overdose is
taken, which is a significant threat in the case of severely depressed patients.
Local drug therapy
Local anesthetics produce loss of sensation and make it possible for many surgical procedures to be performed
without a general anesthetic. Barring any complications, the need for the patient to remain overnight in the
hospital is obviated. Local anesthetics are also used to anesthetize specific peripheral nerves or larger nerve
trunks. These nerve blocks can provide relief in painful conditions like rib fractures, but they are most frequently
used to anesthetize an extremity during hand or foot surgery. Spinal anesthesia and epidural anesthesia, in
which a local anesthetic is injected into the subarachnoid or epidural space of the lumbar (lower back) area of
the spinal canal, provide pain relief during childbirth or surgery that involves the pelvic area yet lack the
problems associated with a general anesthetic. Topical anesthetics, a type of local anesthetic, are also used on
the skin, in the eye’s conjunctiva and cornea, and in the mucous membranes of the nose, mouth, larynx, vagina,
or urethra.
Medications prescribed for dermatologic disorders account for a large amount of local drug therapy, whether it
be a substance to stimulate hair growth or to soothe a burning and itching rash. Many different corticosteroid
preparations are available to treat eczema, allergic reactions to substances like poison ivy, or seborrheic
dermatitis. Sunblocks are used to protect the skin against ultraviolet rays and prevent skin cancer that can result
from exposure to such radiation. Acne is controlled with skin cleansers, keratolytics to promote peeling, and
topical antibiotics to prevent or treat infection. Physicians use various wet dressings, lotions, gels, creams, and
ointments to treat acutely inflamed weeping and crusting sores and to moisturize and protect dry, cracked, and
scaling skin. Burns heal more rapidly and with less scarring when treated appropriately with topical preparations
like silver sulfadiazine. infections of the mucous lining of the mouth (i.e., thrush) or the vagina respond Candidato nystatin or one of the imidazole drugs. The traditional treatment of genital warts has been the topical
Britannica LaunchPacks | The Treatment and Prevention of Disease
103 of 123© 2020 Encyclopædia Britannica, Inc.
application of podophyllin, a crude resin. The emergence of new technologies in the latter part of the 20th
century, however, made possible the development of interferon-α, which is effective in the majority of patients
when injected into the lesion itself or subcutaneously below it.
Most ophthalmic drugs are local—eye drops to treat glaucoma, steroid-antibacterial mixtures to treat infection,
artificial tears for dry-eye syndromes, or mydriatics (drugs causing dilation of the pupil), like atropine, that
facilitate refraction and internal examination of the eye.
Chemotherapy
Chemotherapy is the treatment of disease using chemical agents that are intended to eliminate the causative
organism without harming the patient. In the strict sense, this applies to the use of antibiotics to treat such
invading organisms as bacteria, viruses, fungi, or parasites. The term is commonly used, however, to describe
the use of drugs to treat cancer, in which case the target is not a causative organism but abnormally multiplying
cells. The purpose of the therapy is to selectively kill tumour cells and to leave normal cells unharmed—a very
difficult task because most drugs have a narrow therapeutic zone beyond which they harm normal cells as well
as cancer cells.
Watch the subtle disruptive effect that the widely used anticancer drug Taxol has inside a cell.
Displayed by permission of The Regents of the University of California. All rights reserved.
Anticancer drugs are only relatively selective for cancer cells, and the toughest task for the physician is to select
a drug that will destroy the most cancer cells, leave normal cells unharmed, and cause the fewest unpleasant
and undesirable side effects. The therapeutic goal is to favourably balance the risk-benefit ratio in which the
morbidity of the treatment is weighed against its potential benefits. If a treatment causes patients to be
miserable and has only a slight chance of prolonging life, many patients will forego further treatment. However,
if the potential for significantly prolonging survival by aggressive therapy exists, the patient may decide to
continue with the therapy.
The effectiveness of chemotherapy depends on the highest possible concentration of the drug being at the
tumour site sufficiently long to kill the tumour cells. The maximal opportunity for a cure exists in the early stage
of the disease, when the tumour is small and localized. The larger and more disseminated the tumour, the more
difficult it is to eradicate. The stage the tumour is in will also determine the route of administration, which can be
oral, intravenous, intra-abdominal, intrathecal (into the subarachnoid space of the spinal cord), or intra-arterial—
specifically, into the artery feeding the tumour.
Suppression of bone marrow activity, which results in a decrease in blood cell production, represents the most
limiting factor in chemotherapy. Because chemotherapy is most effective when used at the highest nontoxic
dose, the interval between treatments may need to be prolonged to prevent complete bone marrow
Britannica LaunchPacks | The Treatment and Prevention of Disease
104 of 123© 2020 Encyclopædia Britannica, Inc.
suppression. Supportive measures undertaken when bone marrow suppression occurs include repeated platelet
transfusions (to combat bleeding caused by diminished platelet production) and white blood cell transfusions (to
control infection).
Adjuvant chemotherapy is the use of drugs to eradicate or suppress residual disease after surgery or irradiation
has been used to treat the tumour. This is necessary because distant micrometastases often occur beyond the
primary tumour site. Adjuvant chemotherapy reduces the rate of recurrence of some cancers, especially ovarian
cancer, osteogenic sarcoma, colorectal cancer, and nephroblastoma. The antiestrogen drug tamoxifen has been
effective in selected patients with breast cancer.
Surgical therapyMajor categories of surgery
Wound treatment
Wounds, whether caused by accidental injury or a surgical scalpel, heal in three ways: (1) primary intention
(wound edges are brought together, as in a clean surgical wound), (2) secondary intention (the wound is left
open and heals by epithelization), or (3) third intention, or delayed closure (the wound is identified as potentially
infected, is left open until contamination is minimized, and is then closed).
Choosing which method is best depends on whether excessive bacterial contamination is present, whether all
necrotic material and foreign bodies can be identified and removed, and whether bleeding can be adequately
controlled. Normal healing can occur only if the wound edges are clean and can be closely opposed without
undue stress on the tissue. An adequate blood supply to the wound is essential. If the tissue is tight and the
edges cannot be closed without tension, the blood supply will be compromised. Cutting under the skin to free it
from the underlying subcutaneous tissue may allow the edges to be brought together without tension. If direct
approximation is still not possible, then skin grafts or flaps are used for closure.
Wound closure begins with a thorough cleansing of the wound and the installation of a local anesthetic, usually
lidocaine, which takes effect quickly and lasts for one to two hours. If the wound is contaminated, further
cleansing is performed after instilling the local anesthetic, especially if foreign material is present. If the injury
resulted from a fall on gravel or asphalt as in some motorcycle accidents, then aggressive scrubbing is needed
to remove the many small pieces imbedded beneath the skin. High-pressure irrigation with saline solution will
remove most foreign material and reduce the risk of subsequent infection. Contaminated wounds must be
considered to be prone to infection with , which causes tetanus, and appropriate immunization Clostridium tetaniis given to prevent the condition.
Sutures are the most commonly used means of wound closure, although staples and adhesive tissue tape may
be more appropriate in certain circumstances. Silk sutures were originally used to close skin wounds, but nylon
is stronger and causes less tissue reaction. Ideally, sutures are of the smallest possible diameter that will still
maintain approximation of the wound edges. Absorbable sutures made of catgut (made not from cat but from
sheep intestines) or a synthetic material such as polyglycolic acid are used to approximate the deeper layers of
tissue beneath the skin so that tissue reaction will be lessened. The objective is to eliminate any unfilled space
that could delay healing or allow fluid to accumulate. Drains connected to closed suction are used to prevent the
collection of fluid when it is likely to accumulate, but drains serve as a source of contamination and are used
infrequently. Staples permit faster closure of the skin but are less precise than sutures. When the edges can be
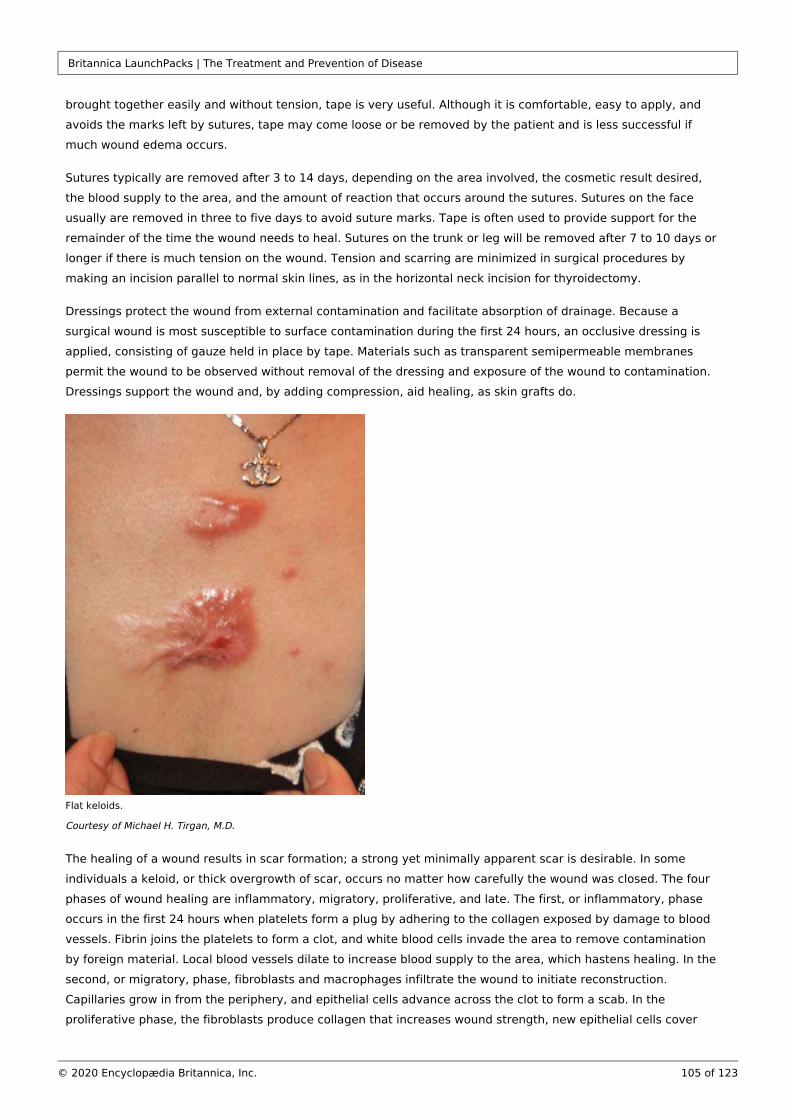
Britannica LaunchPacks | The Treatment and Prevention of Disease
105 of 123© 2020 Encyclopædia Britannica, Inc.
brought together easily and without tension, tape is very useful. Although it is comfortable, easy to apply, and
avoids the marks left by sutures, tape may come loose or be removed by the patient and is less successful if
much wound edema occurs.
Sutures typically are removed after 3 to 14 days, depending on the area involved, the cosmetic result desired,
the blood supply to the area, and the amount of reaction that occurs around the sutures. Sutures on the face
usually are removed in three to five days to avoid suture marks. Tape is often used to provide support for the
remainder of the time the wound needs to heal. Sutures on the trunk or leg will be removed after 7 to 10 days or
longer if there is much tension on the wound. Tension and scarring are minimized in surgical procedures by
making an incision parallel to normal skin lines, as in the horizontal neck incision for thyroidectomy.
Dressings protect the wound from external contamination and facilitate absorption of drainage. Because a
surgical wound is most susceptible to surface contamination during the first 24 hours, an occlusive dressing is
applied, consisting of gauze held in place by tape. Materials such as transparent semipermeable membranes
permit the wound to be observed without removal of the dressing and exposure of the wound to contamination.
Dressings support the wound and, by adding compression, aid healing, as skin grafts do.
Flat keloids.
Courtesy of Michael H. Tirgan, M.D.
The healing of a wound results in scar formation; a strong yet minimally apparent scar is desirable. In some
individuals a keloid, or thick overgrowth of scar, occurs no matter how carefully the wound was closed. The four
phases of wound healing are inflammatory, migratory, proliferative, and late. The first, or inflammatory, phase
occurs in the first 24 hours when platelets form a plug by adhering to the collagen exposed by damage to blood
vessels. Fibrin joins the platelets to form a clot, and white blood cells invade the area to remove contamination
by foreign material. Local blood vessels dilate to increase blood supply to the area, which hastens healing. In the
second, or migratory, phase, fibroblasts and macrophages infiltrate the wound to initiate reconstruction.
Capillaries grow in from the periphery, and epithelial cells advance across the clot to form a scab. In the
proliferative phase, the fibroblasts produce collagen that increases wound strength, new epithelial cells cover

Britannica LaunchPacks | The Treatment and Prevention of Disease
106 of 123© 2020 Encyclopædia Britannica, Inc.
the wound area, and capillaries join to form new blood vessels. In the late phase, the production of new and
stronger collagen remodels the scar, blood vessels enlarge, and the epithelium at the surface heals.
Many factors, including diabetes mellitus or medications, can affect wound healing. In a patient whose diabetes
is well controlled, wound healing is essentially normal, but, if the blood glucose level is elevated, it can impair
healing and predispose the wound to infection. Kidney failure or liver failure and malnutrition also will delay
wound healing, as will poor circulation caused by arteriosclerosis. Having steroids or anticancer or other drugs in
the system can adversely affect the normal healing process.
Surgical extirpation
Medical team performing surgery.
© Brasiliao/Shutterstock.com
Extirpation is the complete removal or eradication of an organ or tissue and is a term usually used in cancer
treatment or in the treatment of otherwise diseased or infected organs. The aim is to completely remove all
cancerous tissue, which usually involves removing the visible tumour plus adjacent tissue that may contain
microscopic extensions of the tumour. Excising a rim of adjacent, seemingly normal tissue ensures a complete
cure unless there has been extension through the lymphatic system, which is the primary route for cancer to
spread. For this reason, local lymph nodes are often removed with the tumour. Pathological examination of the
nodes will show whether the cancer has metastasized (spread). This indicates the likelihood of cure and whether
additional treatment such as radiation therapy or chemotherapy is needed. If complete removal of a tumour is
not possible, palliative surgery, which provides relief but is not a cure, may be useful to relieve pain or pressure
on adjacent structures. Radical surgery may not always be best, as in the early stages of breast cancer. Removal
of the entire breast and surrounding structures, including the axillary lymph nodes, has been shown to provide
no greater benefit than a lumpectomy (removal of the tumour only) followed by radiation to the area in early
stages of breast cancer, while it often causes the patient increased psychological distress. However, because of
improvements in breast reconstruction techniques, the trauma of a radical mastectomy is becoming less severe.
Britannica LaunchPacks | The Treatment and Prevention of Disease
107 of 123© 2020 Encyclopædia Britannica, Inc.
Reconstructive surgery
Reconstructive surgery is employed when a significant amount of tissue is missing as a result of trauma or
surgical removal. A skin graft may be required if the wound cannot be closed directly. If a large surface area is
involved, a thin split-thickness skin graft, consisting of epidermis only, is used. Unfortunately, although these
grafts survive transplantation more successfully and heal more rapidly than other types of grafts, they are
aesthetically displeasing because their appearance differs markedly from that of normal skin. In a small defect,
especially one involving the face or hand, a full-thickness skin graft, consisting of epidermis and dermis, is used,
and skin is generally donated from the ear, neck, or groin. Exposure of bone, nerve, or tendon requires a skin
flap. This can be a local flap, in which tissue is freed and rotated from an adjacent area to cover the defect, or a
free flap, in which tissue from another area of the body is used. An example of a local flap is the rotation of
adjacent tissue (skin and subcutaneous tissue) to cover the defect left from removing a skin cancer. A free flap is
used when the amount of tissue needed is not available locally, as in an injury to the lower leg from an
automobile bumper. The amount and type of tissue needed and the blood supply available determine the type of
flap to be used. The blood supply must be adequate to supply the separated flap and wound edge with
nourishment.
Tissue expanders are another way of creating extra tissue that can be used to cover a defect. Inflatable plastic
reservoirs are implanted under the normal skin of an adjacent area. For several weeks the reservoir is expanded
with saline to stretch the overlying skin, which is then used to cover the defect.
Reconstructive surgery is performed for a variety of surgical conditions. It may require the fashioning of a new
“organ,” as in an artificial bladder, or may involve insertion of prosthetic devices such as artificial heart valves,
pacemakers, joints, blood vessels, or bones.
U.S. soldier with two prostheses playing table football.
Walter Reed/U.S. Army
Prosthetic devices can be used to replace diseased tissue. They usually perform better than donated tissue
because they are made of material that does not stimulate rejection. The first prosthetic limbs were developed
in the early 16th century. In cardiovascular medicine, one of the first prosthetic devices to be used was the
Dacron aortic graft, which was introduced by American surgeon Michael DeBakey and colleagues in 1954 to
replace aortic aneurysms (dilated vessels that risk rupture and death) or vessels obstructed by arteriosclerotic
plaques. Grafts made of similar materials were later employed to replace diseased arteries throughout the body.
Other prosthetic devices include heart valves and metal joints (e.g., hip, knee, or shoulder).

Britannica LaunchPacks | The Treatment and Prevention of Disease
108 of 123© 2020 Encyclopædia Britannica, Inc.
Transplantation surgery
The success of organtransplantation was greatly improved following the discovery in the early 1970s of the
immunosuppressive substance cyclosporine. Other immunosuppressive drugs have since been developed,
including certain glucocorticoids (e.g., prednisone), macrolide lactones (e.g., sirolimus), and antibodies (e.g.,
muromonab-CD3 and basiliximab).
Surgeon Andrew Ready flushing a donated kidney during a transplant at Queen Elizabeth Hospital,…
Christopher Furlong/Getty Images
Kidney transplants are among the most commonly performed types of transplant surgery. Kidneys often are
donated from living relatives to ensure the greatest prospects of long-term survival. The best survival rates are
between identical twins. Cadaver transplants are also used. The one-year graft survival rate is 90 percent or
higher. Approximately 50 percent of grafts cease to function after 8 to 11 years; others, however, last 20 years
or more. Kidneys removed from living donors can be preserved for up to 72 hours before they must be
implanted; most are implanted within 24 hours because successful transplantation decreases with time.
Heart and heart-lung organs can be preserved for four to six hours, and the success rate with this procedure
continues to improve. Extensive matching of blood groups and tissue types is performed to minimize the risk of
rejection. The size of the donor and donated organ should match the size of the recipient and the recipient’s
organ, and the time between pronouncement of death and procurement of the organ should be kept as short as
possible.
In selected patients, liver transplantation has become an accepted treatment for end-stage liver disease.
Mortality following surgery is about 10 to 20 percent, depending on recipient age and health. Survivors require
long-term immunosuppressive therapy.
Surgical techniques
Laser surgery
A laser is a device that produces an extremely intense monochromatic, nondivergent beam of light capable of
generating intense heat when focused at close range. Its applications in the medical field include the surgical
welding of a detached retina and the stanching of bleeding (called laser photocoagulation) in the gastrointestinal
tract that can result from a peptic ulcer. Because a laser beam is absorbed by pigmented lesions, it can be used
to treat pigmented tumours, remove tattoos, or coagulate a hemangioma (a benign but disfiguring tumour of
blood vessels). Laser surgery has also been found to be effective in treating superficial bladder cancer and can
Britannica LaunchPacks | The Treatment and Prevention of Disease
109 of 123© 2020 Encyclopædia Britannica, Inc.
be combined with ultrasonography for transurethral ultrasound-guided laser-induced prostatectomy (TULIP).
More recent uses include the treatment of glaucoma and lesions of the cervix and vulva, including carcinoma in
situ and genital warts.
Cryosurgery
Cryosurgery is the destruction of tissue using extreme cold. Warts, precancerous skin lesions (actinic keratoses),
and small cancerous skin lesions can be treated using liquid nitrogen. Other applications include removing
cataracts, extirpating central nervous system lesions (including hard-to-reach brain tumours), and treating some
heart conduction disorders.
Stereotactic surgery
Stereotactic surgery is a valuable neurosurgical technique that enables lesions deep in the brain that cannot be
reached otherwise to be located and treated using cold (as in cryosurgery), heat, or chemicals. In this procedure,
the head is held motionless in a head ring (halo frame), and the lesion or area to be treated is located using
three-dimensional coordinates based on information from X rays and electrodes.
Stereotactic techniques are also used to focus high-intensity radiation on localized areas of the brain to treat
tumours or to obliterate arteriovenous malformations. This technique is also employed to guide fine-needle
aspiration biopsies of brain lesions; it requires that only one burr hole be made in the skull with the patient
under local anesthesia. Stereotactic fine-needle biopsy also is used to evaluate breast lesions that are not
palpable but are detected by mammography.
Minimally invasive surgery
Endoscopic image of the duodenum.
Samir
Traditional open surgical techniques are being replaced by new technology in which a small incision is made and
a rigid or flexible endoscope is inserted, enabling internal video imaging. Endoscopic procedures (endoscopy)
are commonly performed on nasal sinuses, intervertebral disks, fallopian tubes, shoulders, and knee joints, as
well as on the gallbladder, appendix, and uterus. Although it has many advantages over traditional surgery,
endosurgery may be more expensive and have higher complication rates than traditional approaches.
Trauma surgery
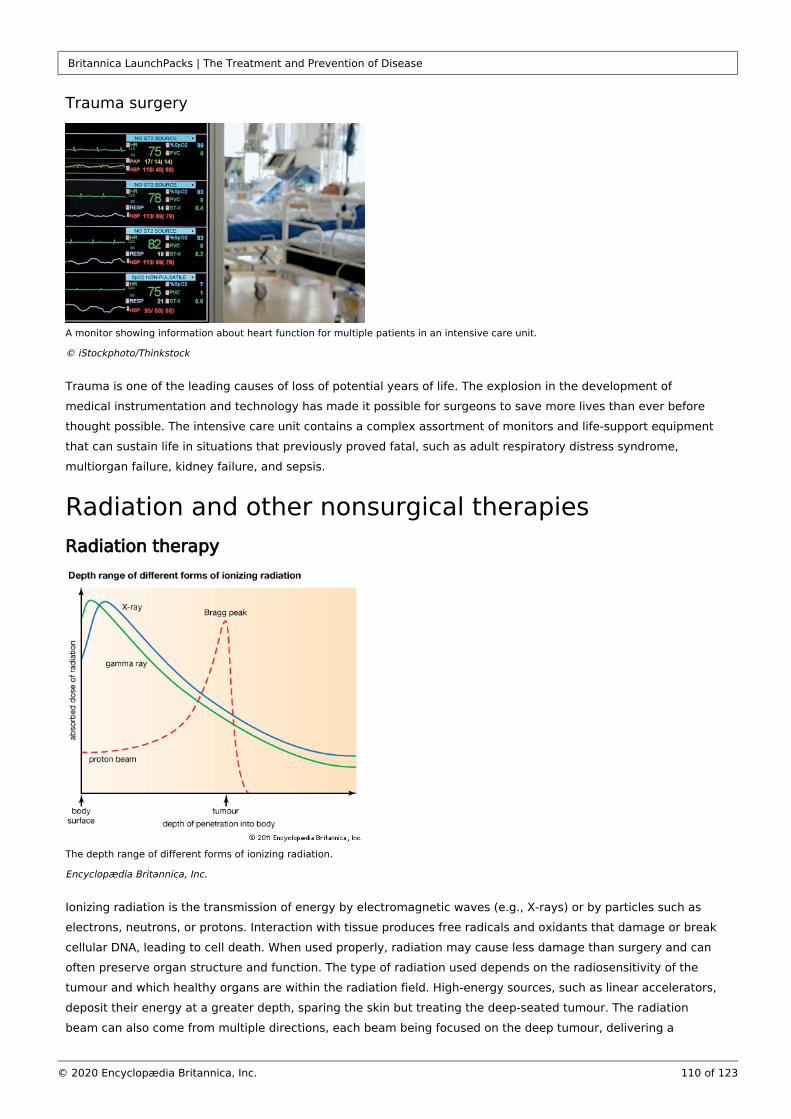
Britannica LaunchPacks | The Treatment and Prevention of Disease
110 of 123© 2020 Encyclopædia Britannica, Inc.
Trauma surgery
A monitor showing information about heart function for multiple patients in an intensive care unit.
© iStockphoto/Thinkstock
Trauma is one of the leading causes of loss of potential years of life. The explosion in the development of
medical instrumentation and technology has made it possible for surgeons to save more lives than ever before
thought possible. The intensive care unit contains a complex assortment of monitors and life-support equipment
that can sustain life in situations that previously proved fatal, such as adult respiratory distress syndrome,
multiorgan failure, kidney failure, and sepsis.
Radiation and other nonsurgical therapiesRadiation therapy
The depth range of different forms of ionizing radiation.
Encyclopædia Britannica, Inc.
Ionizing radiation is the transmission of energy by electromagnetic waves (e.g., X-rays) or by particles such as
electrons, neutrons, or protons. Interaction with tissue produces free radicals and oxidants that damage or break
cellular DNA, leading to cell death. When used properly, radiation may cause less damage than surgery and can
often preserve organ structure and function. The type of radiation used depends on the radiosensitivity of the
tumour and which healthy organs are within the radiation field. High-energy sources, such as linear accelerators,
deposit their energy at a greater depth, sparing the skin but treating the deep-seated tumour. The radiation
beam can also come from multiple directions, each beam being focused on the deep tumour, delivering a
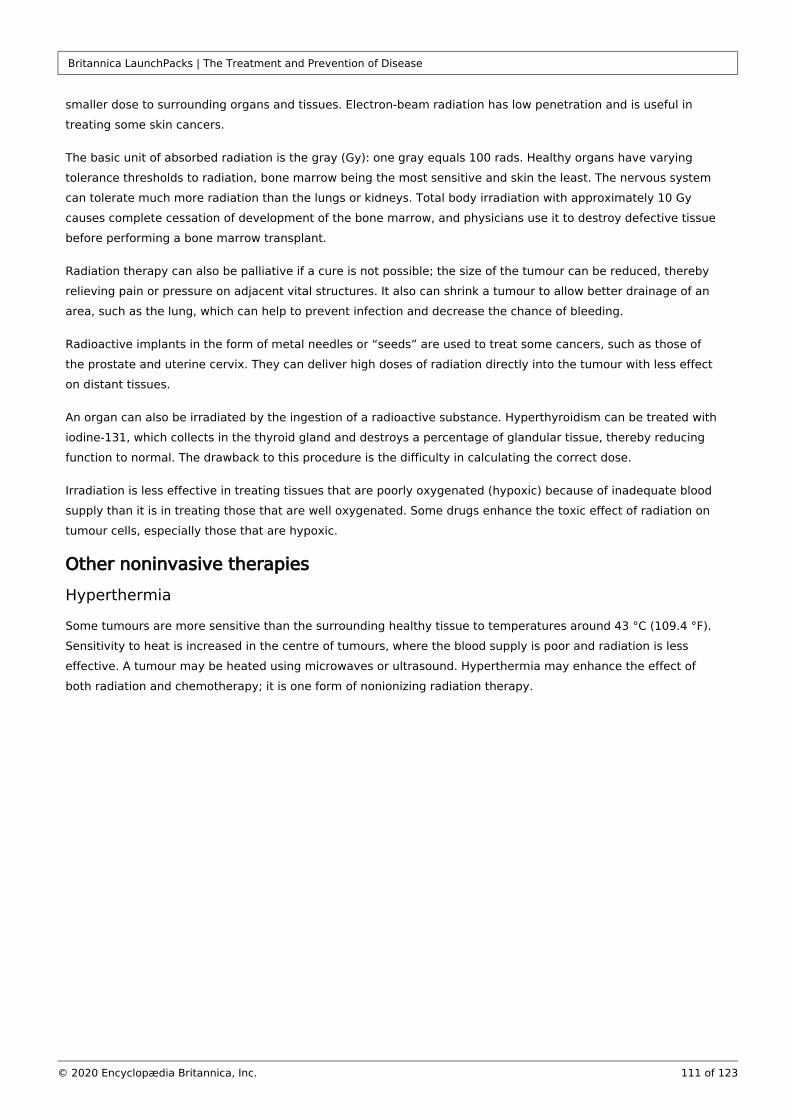
Britannica LaunchPacks | The Treatment and Prevention of Disease
111 of 123© 2020 Encyclopædia Britannica, Inc.
smaller dose to surrounding organs and tissues. Electron-beam radiation has low penetration and is useful in
treating some skin cancers.
The basic unit of absorbed radiation is the gray (Gy): one gray equals 100 rads. Healthy organs have varying
tolerance thresholds to radiation, bone marrow being the most sensitive and skin the least. The nervous system
can tolerate much more radiation than the lungs or kidneys. Total body irradiation with approximately 10 Gy
causes complete cessation of development of the bone marrow, and physicians use it to destroy defective tissue
before performing a bone marrow transplant.
Radiation therapy can also be palliative if a cure is not possible; the size of the tumour can be reduced, thereby
relieving pain or pressure on adjacent vital structures. It also can shrink a tumour to allow better drainage of an
area, such as the lung, which can help to prevent infection and decrease the chance of bleeding.
Radioactive implants in the form of metal needles or “seeds” are used to treat some cancers, such as those of
the prostate and uterine cervix. They can deliver high doses of radiation directly into the tumour with less effect
on distant tissues.
An organ can also be irradiated by the ingestion of a radioactive substance. Hyperthyroidism can be treated with
iodine-131, which collects in the thyroid gland and destroys a percentage of glandular tissue, thereby reducing
function to normal. The drawback to this procedure is the difficulty in calculating the correct dose.
Irradiation is less effective in treating tissues that are poorly oxygenated (hypoxic) because of inadequate blood
supply than it is in treating those that are well oxygenated. Some drugs enhance the toxic effect of radiation on
tumour cells, especially those that are hypoxic.
Other noninvasive therapies
Hyperthermia
Some tumours are more sensitive than the surrounding healthy tissue to temperatures around 43 °C (109.4 °F).
Sensitivity to heat is increased in the centre of tumours, where the blood supply is poor and radiation is less
effective. A tumour may be heated using microwaves or ultrasound. Hyperthermia may enhance the effect of
both radiation and chemotherapy; it is one form of nonionizing radiation therapy.
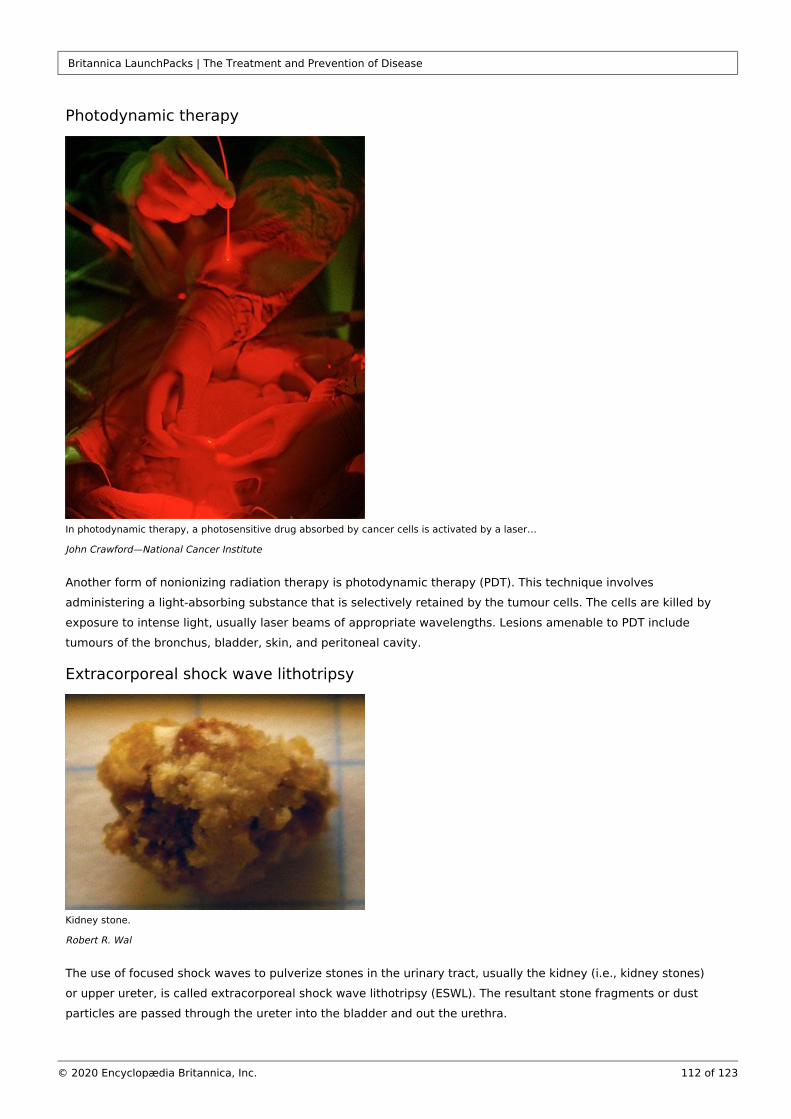
Britannica LaunchPacks | The Treatment and Prevention of Disease
112 of 123© 2020 Encyclopædia Britannica, Inc.
Photodynamic therapy
In photodynamic therapy, a photosensitive drug absorbed by cancer cells is activated by a laser…
John Crawford—National Cancer Institute
Another form of nonionizing radiation therapy is photodynamic therapy (PDT). This technique involves
administering a light-absorbing substance that is selectively retained by the tumour cells. The cells are killed by
exposure to intense light, usually laser beams of appropriate wavelengths. Lesions amenable to PDT include
tumours of the bronchus, bladder, skin, and peritoneal cavity.
Extracorporeal shock wave lithotripsy
Kidney stone.
Robert R. Wal
The use of focused shock waves to pulverize stones in the urinary tract, usually the kidney (i.e., kidney stones)
or upper ureter, is called extracorporeal shock wave lithotripsy (ESWL). The resultant stone fragments or dust
particles are passed through the ureter into the bladder and out the urethra.
Britannica LaunchPacks | The Treatment and Prevention of Disease
113 of 123© 2020 Encyclopædia Britannica, Inc.
A woman during an extracorporeal shock wave lithotripsy (ESWL) procedure. Ultrasound waves are…
© John Harvey Perez
The patient is given a general, regional, or sometimes even local anesthetic and is immersed in water, and the
shock wave is applied to the flank over the kidney. If the stone is small, submersion in a water bath is not
necessary; shock waves are transmitted through the skin via a water-filled rubber bulb positioned over the stone
site. Stones that are too large to be treated in this manner are removed by passing an endoscope into the ureter.
PsychotherapyDrug therapy
The use of drugs to treat mental disorders has expanded dramatically with the development of new and more
effective medications for a variety of disorders that formerly were not treatable. Drugs that affect the mind are
called psychotropic and can be divided into three categories: antipsychotic drugs, antianxiety agents, and
antidepressant drugs.
Antipsychotic agents
The advent of antipsychotic, or neuroleptic, drugs such as chlorpromazine enabled many patients to leave
mental hospitals and function in society. The primary indication for the use of antipsychotics is schizophrenia, a
severe mental disorder characterized by delusions, hallucinations, and sometimes unusual behaviour. One form,
paranoid schizophrenia, is marked by delusions that are centred around a single theme, often accompanied by
hallucinations. The most effective drug to use may depend on an individual patient’s metabolism of the drug or
the severity and nature of the side effects.
Antianxiety agents
Drugs that combat anxiety, also known as anxiolytics or minor tranquilizers, enable otherwise dysfunctional
patients to cope more effectively with the environmental or personal factors that trigger symptoms. This class of
drugs includes the barbiturates, benzodiazepines, nonbenzodiazepine-nonbarbiturates, and hypnotics. The
barbiturates phenobarbital, amobarbital, pentobarbital, and secobarbital have been around the longest and are
used primarily as sedatives or for seizure disorders (phenobarbital).
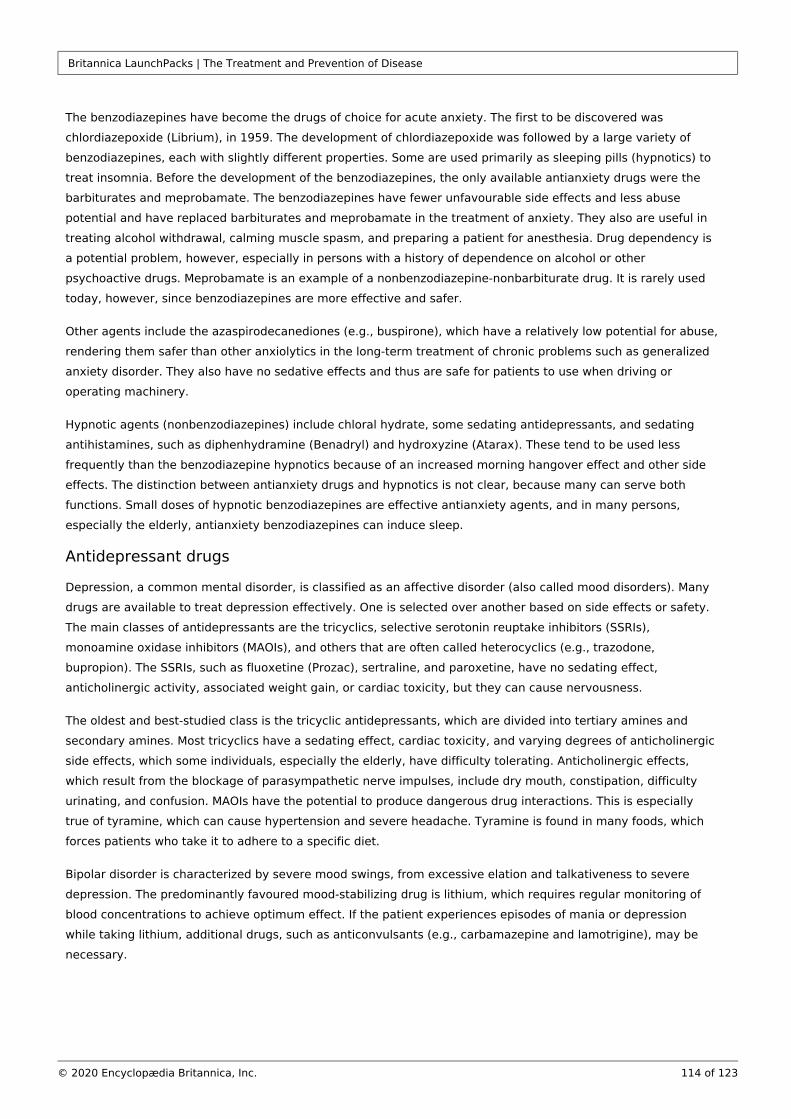
Britannica LaunchPacks | The Treatment and Prevention of Disease
114 of 123© 2020 Encyclopædia Britannica, Inc.
The benzodiazepines have become the drugs of choice for acute anxiety. The first to be discovered was
chlordiazepoxide (Librium), in 1959. The development of chlordiazepoxide was followed by a large variety of
benzodiazepines, each with slightly different properties. Some are used primarily as sleeping pills (hypnotics) to
treat insomnia. Before the development of the benzodiazepines, the only available antianxiety drugs were the
barbiturates and meprobamate. The benzodiazepines have fewer unfavourable side effects and less abuse
potential and have replaced barbiturates and meprobamate in the treatment of anxiety. They also are useful in
treating alcohol withdrawal, calming muscle spasm, and preparing a patient for anesthesia. Drug dependency is
a potential problem, however, especially in persons with a history of dependence on alcohol or other
psychoactive drugs. Meprobamate is an example of a nonbenzodiazepine-nonbarbiturate drug. It is rarely used
today, however, since benzodiazepines are more effective and safer.
Other agents include the azaspirodecanediones (e.g., buspirone), which have a relatively low potential for abuse,
rendering them safer than other anxiolytics in the long-term treatment of chronic problems such as generalized
anxiety disorder. They also have no sedative effects and thus are safe for patients to use when driving or
operating machinery.
Hypnotic agents (nonbenzodiazepines) include chloral hydrate, some sedating antidepressants, and sedating
antihistamines, such as diphenhydramine (Benadryl) and hydroxyzine (Atarax). These tend to be used less
frequently than the benzodiazepine hypnotics because of an increased morning hangover effect and other side
effects. The distinction between antianxiety drugs and hypnotics is not clear, because many can serve both
functions. Small doses of hypnotic benzodiazepines are effective antianxiety agents, and in many persons,
especially the elderly, antianxiety benzodiazepines can induce sleep.
Antidepressant drugs
Depression, a common mental disorder, is classified as an affective disorder (also called mood disorders). Many
drugs are available to treat depression effectively. One is selected over another based on side effects or safety.
The main classes of antidepressants are the tricyclics, selective serotonin reuptake inhibitors (SSRIs),
monoamine oxidase inhibitors (MAOIs), and others that are often called heterocyclics (e.g., trazodone,
bupropion). The SSRIs, such as fluoxetine (Prozac), sertraline, and paroxetine, have no sedating effect,
anticholinergic activity, associated weight gain, or cardiac toxicity, but they can cause nervousness.
The oldest and best-studied class is the tricyclic antidepressants, which are divided into tertiary amines and
secondary amines. Most tricyclics have a sedating effect, cardiac toxicity, and varying degrees of anticholinergic
side effects, which some individuals, especially the elderly, have difficulty tolerating. Anticholinergic effects,
which result from the blockage of parasympathetic nerve impulses, include dry mouth, constipation, difficulty
urinating, and confusion. MAOIs have the potential to produce dangerous drug interactions. This is especially
true of tyramine, which can cause hypertension and severe headache. Tyramine is found in many foods, which
forces patients who take it to adhere to a specific diet.
Bipolar disorder is characterized by severe mood swings, from excessive elation and talkativeness to severe
depression. The predominantly favoured mood-stabilizing drug is lithium, which requires regular monitoring of
blood concentrations to achieve optimum effect. If the patient experiences episodes of mania or depression
while taking lithium, additional drugs, such as anticonvulsants (e.g., carbamazepine and lamotrigine), may be
necessary.
Britannica LaunchPacks | The Treatment and Prevention of Disease
115 of 123© 2020 Encyclopædia Britannica, Inc.
Behavioral therapy
Behavioral therapy, also called behavioral modification, uses psychological counseling to change activity that is
undesirable or potentially harmful. Treatment most often is directed toward changing harmful habits, such as
discontinuing cigarette smoking, dieting to lose weight, controlling alcohol abuse, or managing stress more
effectively.
Several types of behavioral therapy are used. Rational emotive therapy aims at altering inaccurate or irrational
thoughts that lead to negative emotions or maladaptive behaviour. Other behavioral approaches attempt to
modify physical responses. Neurofeedback, for example, uses sensitive electronic devices and the principles of
reinforcement to provide continuous visual or auditory “feedback,” which helps patients learn to control subtle
physical processes. Relaxation training, including deep muscle relaxation exercises, is a stress-reducing
technique that can be used conveniently any time of the day. These cognitive behavioral techniques have been
used to treat insomnia, hypertension, headaches, chronic pain, and phobias.
Behavioral therapies have been developed for common problems of both childhood (e.g., academic
performance, enuresis, and stuttering) and adulthood (e.g., marital discord).
Group therapy
Psychotherapy in which an experienced therapist—a psychiatrist, psychologist, social worker, or member of the
clergy—works with a group of patients or relatives is called group therapy. The process uses the interaction of
group members to benefit each member of the group. Behavioral modification through group interaction and
support can be used to change eating behaviours, which can lead to a reduction in weight. Support groups are
available to assist patients and families in dealing with cancer, alcoholism, abuse, bereavement, and other crises.
Family and systemic therapy
General systems theories emerged in the biological and social sciences following World War II. This led to the
conceptualization of the individual as an interdependent part of larger social systems. In psychotherapy,
systemic therapy does not focus on how problems start, but rather on how the dynamics of relationships
influence the problem. The therapist’s goal is to alter the dynamics of the relationships rather than to focus only
on the behaviour or internal dynamics of individuals. For example, if a child is having temper tantrums, attention
would be given to the stage of family development, the quality of communication between its members, and the
clarity and flexibility of family roles.
Family counseling brings the entire family together to discuss specific problems of one or more family members,
including adolescent discipline problems, marital discord, drug abuse, or relationship problems in families that
can arise from remarriage.
Psychodynamic therapies
Austrian neurologist Sigmund Freud held that all behaviour is influenced by unconscious motivations and
conflicts. Personality characteristics are thought to be shaped from the earliest childhood experiences.
Psychological defenses are seen mainly as unconscious coping responses, the purpose of which is to resolve the
conflicts that arise between basic desires and the constraints of external reality. Emotional problems are seen as
maladaptive responses to these unconscious conflicts.
Psychodynamic therapies emphasize that insight is essential to lasting change. Insight means understanding
how a problem emerged and what defensive purpose it serves. A classic form of psychodynamic therapy is
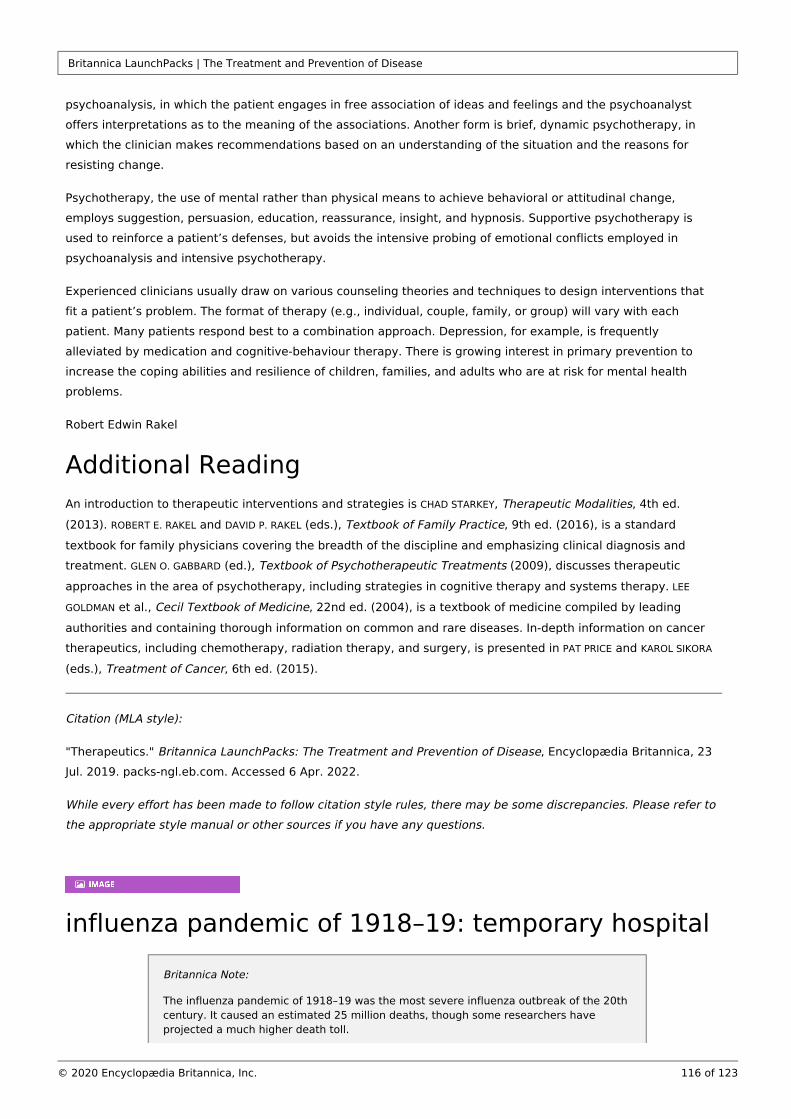
Britannica LaunchPacks | The Treatment and Prevention of Disease
116 of 123© 2020 Encyclopædia Britannica, Inc.
psychoanalysis, in which the patient engages in free association of ideas and feelings and the psychoanalyst
offers interpretations as to the meaning of the associations. Another form is brief, dynamic psychotherapy, in
which the clinician makes recommendations based on an understanding of the situation and the reasons for
resisting change.
Psychotherapy, the use of mental rather than physical means to achieve behavioral or attitudinal change,
employs suggestion, persuasion, education, reassurance, insight, and hypnosis. Supportive psychotherapy is
used to reinforce a patient’s defenses, but avoids the intensive probing of emotional conflicts employed in
psychoanalysis and intensive psychotherapy.
Experienced clinicians usually draw on various counseling theories and techniques to design interventions that
fit a patient’s problem. The format of therapy (e.g., individual, couple, family, or group) will vary with each
patient. Many patients respond best to a combination approach. Depression, for example, is frequently
alleviated by medication and cognitive-behaviour therapy. There is growing interest in primary prevention to
increase the coping abilities and resilience of children, families, and adults who are at risk for mental health
problems.
Robert Edwin Rakel
Additional ReadingAn introduction to therapeutic interventions and strategies is , , 4th ed. CHAD STARKEY Therapeutic Modalities
(2013). and (eds.), , 9th ed. (2016), is a standard ROBERT E. RAKEL DAVID P. RAKEL Textbook of Family Practice
textbook for family physicians covering the breadth of the discipline and emphasizing clinical diagnosis and
treatment. (ed.), (2009), discusses therapeutic GLEN O. GABBARD Textbook of Psychotherapeutic Treatments
approaches in the area of psychotherapy, including strategies in cognitive therapy and systems therapy. LEE
et al., , 22nd ed. (2004), is a textbook of medicine compiled by leading GOLDMAN Cecil Textbook of Medicine
authorities and containing thorough information on common and rare diseases. In-depth information on cancer
therapeutics, including chemotherapy, radiation therapy, and surgery, is presented in and PAT PRICE KAROL SIKORA
(eds.), , 6th ed. (2015).Treatment of Cancer
Citation (MLA style):
"Therapeutics." , Encyclopædia Britannica, 23 Britannica LaunchPacks: The Treatment and Prevention of DiseaseJul. 2019. packs-ngl.eb.com. Accessed 6 Apr. 2022.
While every effort has been made to follow citation style rules, there may be some discrepancies. Please refer to the appropriate style manual or other sources if you have any questions.
influenza pandemic of 1918–19: temporary hospital
Britannica Note:
The influenza pandemic of 1918–19 was the most severe influenza outbreak of the 20th century. It caused an estimated 25 million deaths, though some researchers have projected a much higher death toll.
Britannica LaunchPacks | The Treatment and Prevention of Disease
117 of 123© 2020 Encyclopædia Britannica, Inc.
A temporary hospital in Camp Funston, Kansas, during the 1918–19 influenza pandemic.
Courtesy of the National Museum of Health and Medicine, Armed Forces Institute of Pathology, Washington, D.C
Citation (MLA style):
Influenza pandemic of 1918–19: temporary hospital. Image. Britannica LaunchPacks: The Treatment and , Encyclopædia Britannica, 4 Mar. 2022. packs-ngl.eb.com. Accessed 6 Apr. 2022.Prevention of Disease
While every effort has been made to follow citation style rules, there may be some discrepancies. Please refer to the appropriate style manual or other sources if you have any questions.
Watch archival footage of children with polio and Jonas Salk administering immunization injections
Britannica Note:
At its peak incidence in the United States, in 1952, approximately 21,000 cases of paralytic polio (a rate of 13.6 cases per 100,000 population) were recorded.
Britannica LaunchPacks | The Treatment and Prevention of Disease
118 of 123© 2020 Encyclopædia Britannica, Inc.
Video Transcript
NARRATOR: The polio virus attacks certain kinds of nerve cells, and for hundreds of years it killed and crippled,
especially children. By 1952 Dr. Jonas Salk and his research team at the University of Pittsburgh had developed a
killed-virus vaccine against polio. The effort to eradicate the disease started small, with Dr. Salk and his team
immunizing a few thousand students in the Pittsburgh area. But soon it became a nationwide mobilization to
protect every child against the polio threat. Salk's vaccine and the live polio vaccine developed later by Albert
Sabin, were effective in controlling the viral disease.
Archival footage showing children with polio, Jonas Edward Salk giving injections, an immunization centre, and
vials of vaccine being produced.
Encyclopædia Britannica, Inc.
Citation (MLA style):
Watch archival footage of children with polio and Jonas Salk administering immunization injections. Video.
, Encyclopædia Britannica, 4 Mar. 2022. packs-Britannica LaunchPacks: The Treatment and Prevention of Diseasengl.eb.com. Accessed 6 Apr. 2022.
While every effort has been made to follow citation style rules, there may be some discrepancies. Please refer to the appropriate style manual or other sources if you have any questions.
Britannica LaunchPacks | The Treatment and Prevention of Disease
119 of 123© 2020 Encyclopædia Britannica, Inc.
Learn how vaccines enhance the human immune system to fight against harmful pathogens
Video Transcript
Vaccines save more than 9 million lives each year, even though they contain ingredients that can be pretty
dangerous. But that's precisely the point-- those nasty ingredients are the only reason that vaccines work at all.
On their own, our bodies are already pretty good at fighting off illness. When an unfamiliar pathogen invades our
body, patrolling immune cells engulf a few of these foes to gather intel. The cells then churn out a chemical
alarm, transmitting the enemy's information along the chains of command and triggering the production of
specially targeted antibodies and assassin cells to fend off the rest of the invaders. After the battle, some of
these specialized troops stick around so that if the pathogen returns, they can help mount a quicker response.
However, some pathogens are so powerful that they can overwhelm the immune system before it's able to
mount a defense. Vaccination lets us stage a practice version of this battle in advance of the real one so that the
immune system can develop and stockpile weapons specifically targeted at the enemy. That does require
introducing a bit of the enemy into our bodies, but it's an enemy that we've already disarmed, either by killing it,
breeding a super weak strain, or dismembering it to get at recognizable, but not dangerous, parts. Enter
formaldehyde. It's a critical ingredient in some common vaccines, like those for tetanus and influenza, because it
alters the structure of those pathogens just enough to render them harmless. This reactivity also makes
formaldehyde dangerous to us in large doses, but vaccines contain only a tiny fraction of the formaldehyde we
consume in food and naturally produce in our bodies on a daily basis. In fact, the biggest risk with formaldehyde
is that it can leave pathogens so crippled that they won't trigger the proper immune response. So some vaccines
contain substances called adjuvants, which put the immune system on higher alert. Aluminum, for example,
causes a minor irritation at the injection site, summoning immune cells to the scene so they'll encounter the
weekend enemy. And although too much aluminum can be toxic, our bodies are super efficient at eliminating it,
keeping levels low even after lots of shots. So while boatloads of aluminum, buckets of formaldehyde, and an up-
lose meet and greet with a full-strength pathogen are all definitely bad ideas, a controlled concoction from a
doctor is designed to be just nasty enough to keep us safe. There's always a chance of an adverse reaction to
vaccine's ingredients, but the much scarier scenario would be to let polio, measles, and other deadly diseases
call the shots.
Britannica LaunchPacks | The Treatment and Prevention of Disease
120 of 123© 2020 Encyclopædia Britannica, Inc.
The basic strategies behind the use of vaccines to prepare the human immune system to deal with harmful
pathogens. Adjuvants, such as aluminum, are incorporated into vaccines to hasten the body's immune response.
© MinuteEarth
Citation (MLA style):
Learn how vaccines enhance the human immune system to fight against harmful pathogens. Video. Britannica , Encyclopædia Britannica, 4 Mar. 2022. packs-ngl.eb.LaunchPacks: The Treatment and Prevention of Disease
com. Accessed 6 Apr. 2022.
While every effort has been made to follow citation style rules, there may be some discrepancies. Please refer to the appropriate style manual or other sources if you have any questions.
Discover how gene therapy can treat diseases caused by genetic mutations such as cystic fibrosis
Video Transcript
NARRATOR: Genes carry the hereditary information responsible for the distinct characteristics of every
individual. They are composed of DNA, and it is the sequence of bases along a strand of DNA that determines
the genetic code. Disruptions of the number or order of bases in a gene are known as mutations. If severe
enough, these mutations can cause death or diseases such as cancer and cystic fibrosis. Gene therapy seeks to
treat or prevent genetic disease by introducing a normal, working gene into an individual's genome. This new
gene may serve to replace the mutated gene. The transformed cells then reproduce and generate normal gene
product, thereby reducing the symptoms of disease or eliminating the disease altogether. If, however, the new
gene replaces a working gene instead of the defective one, a new mutation may arise. Another approach to
gene therapy involves the introduction of a new gene that does not replace the mutation but rather aids the
body in fighting the disease. This new gene targets the damaged cells while leaving the healthy ones unharmed.
Gene therapy seeks to repair genetic mutations through the introduction of healthy, working genes.
Britannica LaunchPacks | The Treatment and Prevention of Disease
121 of 123© 2020 Encyclopædia Britannica, Inc.
Encyclopædia Britannica, Inc.
Citation (MLA style):
Discover how gene therapy can treat diseases caused by genetic mutations such as cystic fibrosis. Video.
, Encyclopædia Britannica, 4 Mar. 2022. packs-Britannica LaunchPacks: The Treatment and Prevention of Diseasengl.eb.com. Accessed 6 Apr. 2022.
While every effort has been made to follow citation style rules, there may be some discrepancies. Please refer to the appropriate style manual or other sources if you have any questions.
Discover how constantly mutating viruses are a challenge to a universal flu vaccine
Video Transcript
SOPHIA CAI: It seems like every year doctors and worried mothers want us to get a flu shot so we can avoid the
fever, aches, and pains of the dreaded influenza virus. And it's true, we should. But why do we need one every
year? And hey, why don't they always work? Stick around for answers to find out about an even better option,
the ever-elusive universal flu shot we've all been waiting for. Yeah, I have been waiting for it. Haven't you? Hey,
everybody. Sophia here. There are dozens of types of influenza viruses that cause flu symptoms. Remember, the
swine flu? That's the H1N1 virus. The avian flu? That's H5N1. These letters and numbers identify variations in
two different proteins on the surface of an influenza virus-- H for hemagglutinin, which has 18 subtypes, and N
for neuraminidase, which comes in 11 varieties. Every year, experts from the CDC and flu research centers
worldwide pick the strains they think will be most prevalent. Private companies then create flu shots containing
antigens from those specific strains. Antigens are essentially little biochemical flags that wave on the surface of
viruses to signal which strain they are. These antigen flags also signal to your body that it's time to create
antibodies. Antibodies circulate in your bloodstream, looking for antigens. And once they find them, they tell
your body to launch a full-blown immune response and protect itself against these invaders. So a flu shot is like
an inverse guest list for the party that is your body. A vaccine tells your immune system who to bounce when
they show up. The trouble is flu viruses are constantly mutating, which causes their antigens to change all the
time-- from year to year or even over one flu season. Scientists call this annoying behavior antigenic drift. Flu
Britannica LaunchPacks | The Treatment and Prevention of Disease
122 of 123© 2020 Encyclopædia Britannica, Inc.
experts have to pick out which strains of viruses to include in a vaccine months before flu season kicks off so
companies can produce and distribute the vaccine in time. If experts guess wrong, your antibodies won't
recognize the invading flu viruses. And they won't stop you from getting sick, even though you went through all
the trouble of going to the pharmacy and getting your flu shot to make your mom happy. I got mine, mom. So
wouldn't it be great if scientists could create a vaccine that would work on any flu strain, no matter what antigen
flag it's flying? A universal flu vaccine, if you will. Well, research from this year suggests that scientists are
getting closer to coming up with one. Scientists have focused their efforts on understanding hemagglutinin
stems, called HA stems. These HA stems are basically standardized flagpoles that various viruses use to fly their
antigen flags. Two different research groups have created HA stems for a single vaccine to protect against
multiple flu strains. Even better, that might mean you wouldn't have to get a flu shot every year, maybe just
every 5 or 10, depending on how good your body is at remembering the antigens. So far they've tested these
new vaccines in mice, ferrets, and non-human primates, many of which have been protected from the flu. But
humans have a unique immune system, so clinical trials in people will really be the definitive next step. So
here's to hoping that researchers can take the guesswork out of flu shots and that they guessed right this year.
Searching for a universal flu vaccine.
© American Chemical Society
Citation (MLA style):
Discover how constantly mutating viruses are a challenge to a universal flu vaccine. Video. Britannica , Encyclopædia Britannica, 4 Mar. 2022. packs-ngl.eb.LaunchPacks: The Treatment and Prevention of Disease
com. Accessed 6 Apr. 2022.
While every effort has been made to follow citation style rules, there may be some discrepancies. Please refer to the appropriate style manual or other sources if you have any questions.
Know why tuberculosis still poses a threat to humans and why the fight against this disease is far from over
Video Transcript

Britannica LaunchPacks | The Treatment and Prevention of Disease
123 of 123© 2020 Encyclopædia Britannica, Inc.
Video Transcript
NARRATOR: It's a deadly disease that only affects humans, and it's been around for a long time. CLIFTON BARRY:
This bug has been with humans since the paleolithic. NARRATOR: The fight against tuberculosis has been going
on for decades, even centuries. So why is this particular disease so hard to fight, and how close are we to
knocking it out? Though largely under control in the West, there are still about 9 million tuberculosis cases
reported worldwide each year, and more than a million deaths. Dr. Cliff Barry heads up the tuberculosis unit at
the National Institutes of Health. He recently published new findings on TB treatments in ACS Infectious
Diseases. Barry and his team are waging a fight against a resilient, constantly evolving, bacteria. BARRY: Drugs
and vaccines have been a huge failure recently. NARRATOR: There are treatments, but they are costly and
lengthy. BARRY: You take four drugs for two months, and then you continue on two of those for another four
months. So it's six months of treatment with a huge pill burden. NARRATOR: Those treatments have also been
around for decades, giving the disease time to adapt and leading to tougher drug resistant forms of the bacteria.
BARRY: It's a nightmare to deal with, because there is not really good options therapeutically. NARRATOR: Part
of the difficulty is that researchers still know very little about the bacteria itself. What is known is that the
bacteria's structure makes it even harder to fight. BARRY: They have an incredibly thick outer cell envelope
that's unlike anything else in the bacterial world. NARRATOR: It's hard to penetrate. And it has a unique way of
making itself at home in the lungs of a patient. TB uses the body's immune system to build a sort of castle inside
a lung called a granuloma. The immune system walls off the TB inside this castle of dead cells, but it doesn't kill
it off. Researchers have recently discovered that cholesterol in the bloodstream helps keep TB alive inside that
wall of cells. When the immune system can no longer keep TB walled off the disease strikes, killing at least half
the people infected with the active bacteria. Despite gains, Barry says the fight against tuberculosis is far from
over. BARRY: We have so much to learn. We have so far to go with this. NARRATOR: But he's buoyed by the
recent flood of research. BARRY: You got some good people focused on a hard problem now. And I think that's
probably why you see a lot more publishing in this area and a lot more-- and we will see a lot more publishing in
this area.
Learn why tuberculosis is still a threat to the human population.
© American Chemical Society
Citation (MLA style):
Know why tuberculosis still poses a threat to humans and why the fight against this disease is far from over. Video. , Encyclopædia Britannica, 4 Mar. 2022. Britannica LaunchPacks: The Treatment and Prevention of Diseasepacks-ngl.eb.com. Accessed 6 Apr. 2022.
While every effort has been made to follow citation style rules, there may be some discrepancies. Please refer to the appropriate style manual or other sources if you have any questions.















![[Cellulite – causes, prevention, treatment]](https://img.pdfslide.net/doc/110x75/634bd129913672970c0940e9/cellulite-causes-prevention-treatment.jpg)













