Embed Size (px)
Citation preview
Transitional Cell Carcinoma in High-Grade High-Stage Ovarian Carcinoma
An Indicator of Favorable Response to Chemotherapy
SUSAN S. ROBEY, MD,*.t ELVlO G. SILVA, MD,' DAVID M. GERSHENSON, MD,$ DOIJIA MCLEMORE, HTL (ASCP),§ ADEL EL-NAGGAR, MD,' AND NELSON G. ORDONEZ, MD,*
'We reviewed 53 high-grade carcinomas of the ovary in order to define pathologic features that correlate with prognosis. All tumors were Stage 111 with comparable amounts of residual tumor left after the primary resection. Similar postoperative chemotherapeutic regimens were given to each patient, and there was a clinical followup of at least four years in each case. The tumors were classified according to their predominant (>SO%) histology as transitional cell carcinoma (TCC) (18 tumors), papillary serous (18), undifferentiated (8), or endometrioid (3). There were six mixed carcinomas without predominant histology. In 17 of 18 patients, TCC predominant tumors responded completely to chemotherapy and 15 of 18 ]patients (83%) are alive without disease 4 to 10 years after presentation (average 6.8 years). In comparison, itumor progression/recurrence developed in 31 of 35 non-TCC tumors (18 serous, eight undifferentiated, one endometrioid predominant, and four mixed carcinomas). Of these 35 patients, 27 (77%) died of disease ifrom 6 months to 7 years after presentation (average 2.5 yrs.). Flow cytometric determination of DNA icontent and immunoperoxidase studies did not allow discrimination between the histologic types of high- ;grade ovarian carcinomas. We conclude that TCC should be recognized as a distinct histologic type of ovarian carcinoma because of the favorable response to chemotherapy and improved patient survival.
Cancer 632339447, 1989.
F ALL MALIGNANCIES of the female genital tract, 0 ovarian carcinoma is the most common fatal tu- mor.' Prognostic factors for the survival of patients with ovarian carcinoma include tumor stage, histologic grade, patient perfclrmance status, and quantity of residual tumor left after primary resection..2-6 The histologic subtype is not considered to be of major prognostic imp~rtance.~
Ovarian carcinoma encompasses a variety of histologic patterns, including serous, endometnoid, and undiffer- entiated types.537 Carcinomas of the ovary which resemble transitional cell carcinoma (TCC) of the bladder have been
From the *Departments of Pathology, §Veterinary Medicine, and $Gynecology, The University of Texas M. D. Anderson Cancer Center, Houston, Texas.
t American 'Cancer Society Regular Clinical Fellow. Presented in part at the United States-Canadian Academy of Pathology
meeting, March 11, 1988, Washington, D. C. The authors thank Centocor, Malvern, Pennsylvania, for kindly sup-
plying the antibody, OC-125; Ms. Brenda Clayton for her preparation of the manuscript; Mr. Thomas Brooks for his technical assistance; and the Caduceus Foundation, New York, NY, for supporting this research.
Address for reprints: Susan S. Robey, MD, Department of Pathology- Box 85, M. D. Anderson Cancer Center, I5 15 Holcombe Blvd., Houston, Texas 77030.
Accepted for publication August 23, 1988.
described,* but are not generally considered as a distinct histologic subtype of common ovarian epithelial tumors.
We have observed that TCC is a histologic component of some high-grade ovarian carcinomas. We therefore un- dertook a study to determine the frequency with which TCC is present in such tumors. The prognosis of high- grade ovarian carcinomas composed predominantly of transitional cell carcinoma, their immunoreactivity for ovarian tumor antigens, and their DNA content as de- termined by flow cytometry are reported.
Materials and Methods
Case Selection
Fifty-three cases of high-grade ovarian carcinomas (Grade 3 in a three-grade system) were selected from the surgical pathology files of the M. D. Anderson Cancer Center dating from 1971 through 1985. All patients had Stage 111 disease with gross residual tumor left behind after primary surgical tumor debulking. Each patient received chemotherapy for a minimum of 6 months postopera- tively. Minimum clinical followup for patients who re- mained alive was 4 years (range: 4 to 10). Clinical infor- mation for patients in the study is given in Table 1.
839
840 CANCER March 1 1989 Vol. 63
TABLE 1 . Clinical Data Of 53 High-Grade Stage I11 Ovarian Carcinomas
TCC Non-TCC
Parameter (No. = 18) (No. = 35) predominant predominant
Average age (yrs)
Sites of tumor metastases Omentum Abdominal peritoneum Pelvic peritoneum Paraaortic lymph nodes
Amount of residual tumor 1 2 cm 2 2 cm Quantity unknown
HAC Melphalan, Cisplatin Cyclophosphamide,
Cisplatin Melphalan Hydroxymethylmelamine,
Cyclophosphamide Cisplatin, Doxorubicin,
Cyclophosphamide Other*
(Range)
Chemotherapy
50.9 (32-70)
12 7 4 1
9 6 3
10 1
1 3
0
0 3
55.8 (41-72)
32 10 5 1
12 20
3
9 7
5 3
3
2 6
TCC transitional cell carcinoma; HAC hydroxymethylmelamine,
* Combinations including Hydroxymethylmelamine, Melphalan, doxorubicin, cyclophosphamide.
Cisplatin and 5-Fluorouracil.
Histologic Review
Tumors were classified according to their predominant histology as TCC, serous, undifferentiated, or endome- trioid carcinoma. Predominant histology was defined as a single pattern that comprised over 50% of the tumor. Tumors with multiple histologic patterns but no predom- inant type were termed mixed carcinomas. An average of 8.3 sections were reviewed per case.
The degrees of nuclear anaplasia, vascular invasion, and tumor necrosis were evaluated for each case, and the average number of mitotic figures per 10 high power fields was counted. From the gross description, the percentages of solid and papillary components were determined.
Immunoperoxidase Studies
In 35 cases where paraffin blocks were available, im- munohistochemical studies were performed using the av- idin-biotin-peroxidase complex (ABC) method of Hsu and colleagues9 in the following manner: 3-4 micrometer- thick, formalin-fixed, paraffin-embedded sections were floated on 0.1% Elmer's glue-coated slides (Borden, Co- lumbus, OH) and dried overnight at 54°C. The tissue sections were then deparaffinized in xylene, and rehy- drated in descending grade (100%-70%) ethanol solutions. In order to enhance the immunostaining, the sections were
digested with 0.1 % protease (type XIV, Sigma Chemical, St. Louis, MO) in phosphate buffer, pH 7.6 for 30 minutes. Endogenous peroxidase activity was blocked with 3% hy- drogen peroxide in absolute methanol for 10 minutes. Sections were incubated with mouse monoclonal antibody (MoAb) OC-125 (Centocor, Inc., Malvern, PA, 1500 di- lution). This antibody is directed against the CA125 an- tigen. '' Tissue sections were also stained with a MoAb to carcinoembryonic antigen (CEA) (Hybritech, Indianap- olis, IN, 1:750 dilution), a MoAb directed against human milk fat globule related antigen (HMFG-2 MoAb)" (Seward Laboratories, London, 1: 100 dilution) and a polyclonal antibody raised in rabbits against human cho- rionic gonadotrophin (HCG) (Dako Corp., Santa Barbara, CA, 1:1,000 dilution). All the primary antibodies were incubated for 1 hour at room temperature. This was fol- lowed by immunoperoxidase staining using ABC kits (Vector Laboratories, Burlingame, CA). Preincubation with normal horse serum was used for monoclonal an- tibodies and normal goat serum for polyclonal antibodies ( 1 : 10 dilution) to minimize background. The immuno- staining was developed using 3-amino-9-ethylcarbazole as chromogen. The specificity of the immunoreaction was verified by staining known positive and negative control tissue sections.
Flow Cytometry
Flow cytometry determination of tumor cell DNA content was performed on paraffin-embedded tissue using the method of McLemore et al.'* Briefly, two 25 pm sec- tions of tumor were placed in a 13 mm X 100 mm test tube, deparaffinized, rehydrated, and washed in Dulbec- CO'S phosphate buffered saline (DPBS) (Gibco Laborato- ries, Grand Island, NY) with 30 mM magnesium chloride, pH 7.5.
The tissue was then incubated for 5 minutes in 0.5% pepsin in distilled water (Sigma Chemical Corp., St. Louis, MO), pH 1.5, prewarmed to 37°C. Disaggregation was accomplished by drawing the tissue and pepsin solution through a 20-gauge needle into a syringe and then forcing it back into the tube four or five times. The disaggregation reaction was stopped by adding 2 ml of cold (4°C) DPBS and placing the tube into a container of shaved ice. Sam- ples were centrifuged and washed twice with cold DPBS.
After the final wash, the buffer was removed and 60 pl of a 0.25 pg/ml solution of propridium iodide (Sigma Chemical Corp.) was added. RNA was hydrolyzed by adding 6 drops of 250 pg/ml ribonuclease A (Worthington Biochemical, Freehold, NJ) to each tube. Samples were then filtered through a 50-pm nylon mesh filter (Small Parts Inc., Miami, FL) and analyzed using a FACS flow cytometer (Becton-Dickinson, Sunnyvale, CA). 5000 cells were evaluated per specimen. Data were analyzed using
No. 5 TCC IN OVARIAN CARCINOMA Robey et al. 84 1
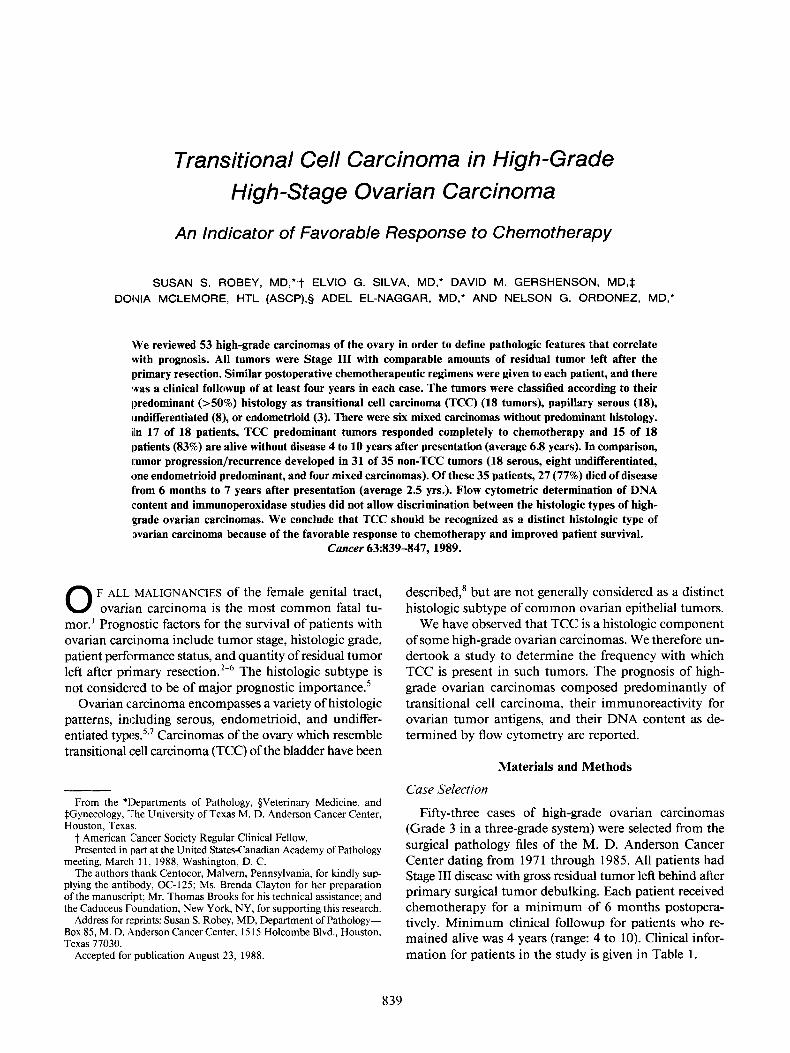
FIG. IA-C. Transitional cell carcinoma of ovary. (A) Cystic spaces lined by multilayered tumor epithelium resembling TCC of bladder (H & E, X176). (B) Papillary projection in a TCC (H 8t E, X880). (C) Cytologic detail of an ovarian TCC (H & E, X1760).
842 CANCER March I 1989 Vol. 6 3
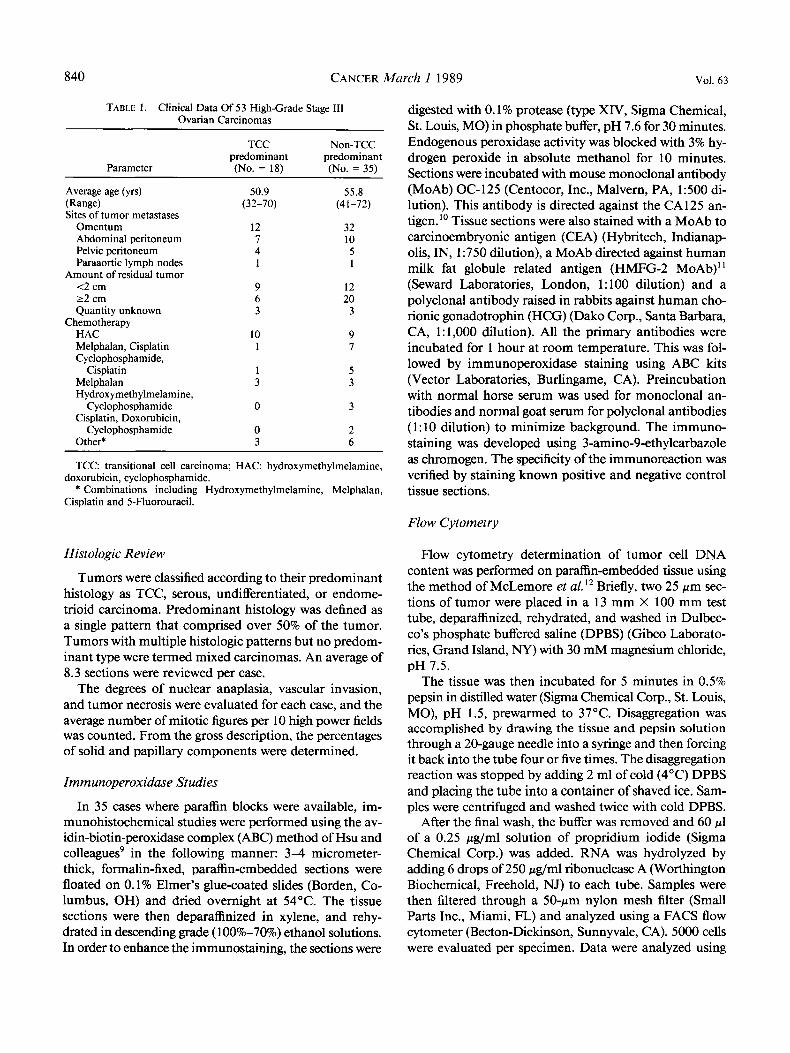
FIG. 2A-D. (A) TCC of ovary (H & E, X80). (B) TCC of ovary (H & E, X176). (C) TCC with solid nests of cells infiltrating a fibrous stroma (H & E, X80). (D) Mucin production in a TCC (arrow) (H & E, X176).
No. 5 TCC IN OVARIAN CARCINOMA - Robey et al. 843
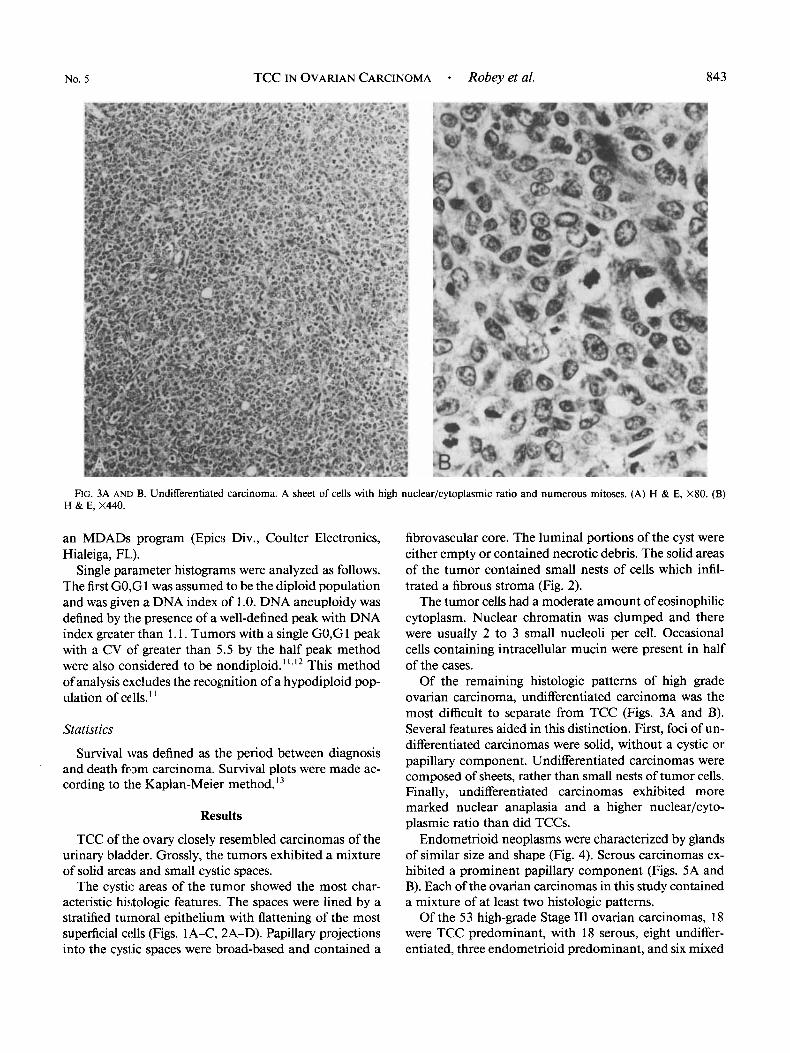
FIG. 3A AND B. Undifferentiated carcinoma. A sheet of cells with high nuclear/cytoplasmic ratio and numerous mitoses. (A) H & E, X80. (B) H & E, X440.
an MDADs program (Epic!; Div., Coulter Electronics, Hialeiga, FL).
Single parameter histograms were analyzed as follows. The first GO,G 1 was assumed. to be the diploid population and was given a DNA index of 1 .O. DNA aneuploidy was defined by the presence of a well-defined peak with DNA index greater than 1.1. Tumors with a single GO,G 1 peak with a CV of greater than 5.5 by the half peak method were also considered to be nondiploid. ' ' , I 2 This method of analysis excludes the recognition of a hypodiploid pop- ulation of cells."
Statistics
Survival was defined as the period between diagnosis and death from carcinoma. Survival plots were made ac- cording to the Kaplan-Meier method.I3
Results
TCC of the ovary closely resembled carcinomas of the urinary bladder. Grossly, the tumors exhibited a mixture of solid areas and small cystic spaces.
The cystic areas of the tumor showed the most char- acteristic histologic features. The spaces were lined by a stratified tumoral epithelium with flattening of the most superficial cells (Figs. 1 A-C, 2A-D). Papillary projections into the cysi.ic spaces were broad-based and contained a
fibrovascular core. The luminal portions of the cyst were either empty or contained necrotic debris. The solid areas of the tumor contained small nests of cells which infil- trated a fibrous stroma (Fig. 2).
The tumor cells had a moderate amount of eosinophilic cytoplasm. Nuclear chromatin was clumped and there were usually 2 to 3 small nucleoli per cell. Occasional cells containing intracellular mucin were present in half of the cases.
Of the remaining histologic patterns of high grade ovarian carcinoma, undifferentiated carcinoma was the most difficult to separate from TCC (Figs. 3A and B). Several features aided in this distinction. First, foci of un- differentiated carcinomas were solid, without a cystic or papillary component. Undifferentiated carcinomas were composed of sheets, rather than small nests of tumor cells. Finally, undifferentiated carcinomas exhibited more marked nuclear anaplasia and a higher nuclear/cyto- plasmic ratio than did TCCs.
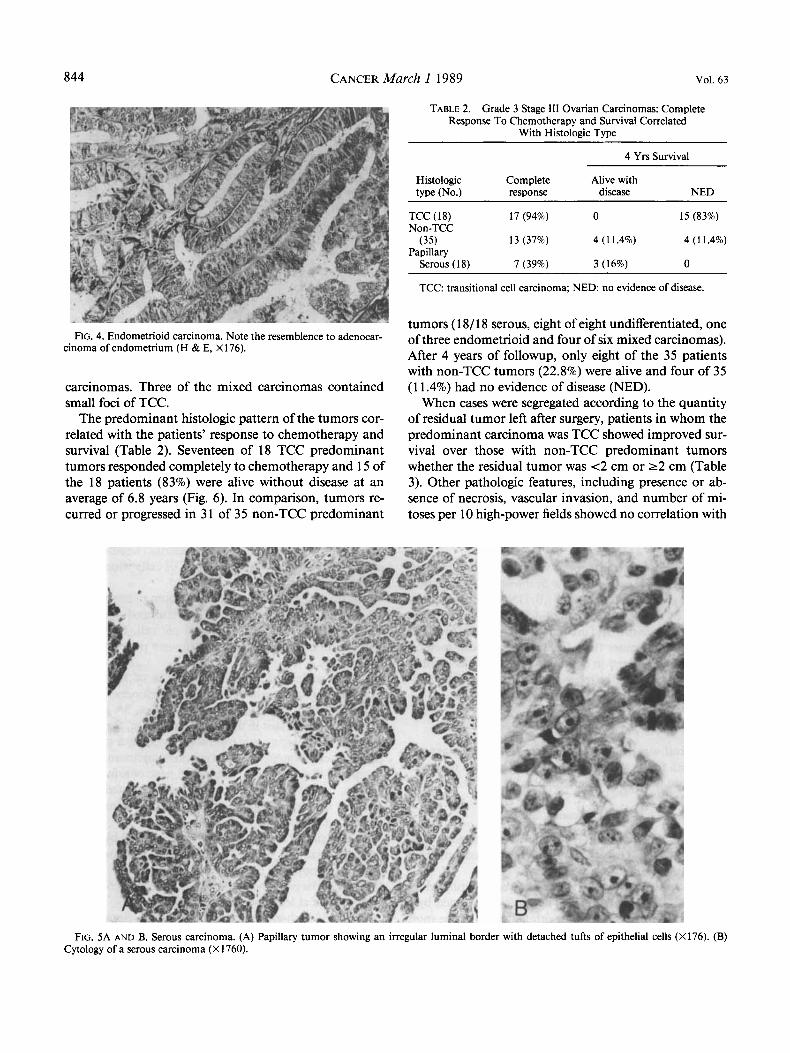
Endometrioid neoplasms were characterized by glands of similar size and shape (Fig. 4). Serous carcinomas ex- hibited a prominent papillary component (Figs. 5A and B). Each of the ovarian carcinomas in this study contained a mixture of at least two histologic patterns.
Of the 53 high-grade Stage I11 ovarian carcinomas, 18 were TCC predominant, with 18 serous, eight undiffer- entiated, three endometrioid predominant, and six mixed
844 CANCER March I 1989 Vol. 63
FIG. 4. Endometrioid carcinoma. Note the resemblence to adenocar- cinoma of endometrium (H & E, X 176).
carcinomas. Three of the mixed carcinomas contained small foci of TCC.
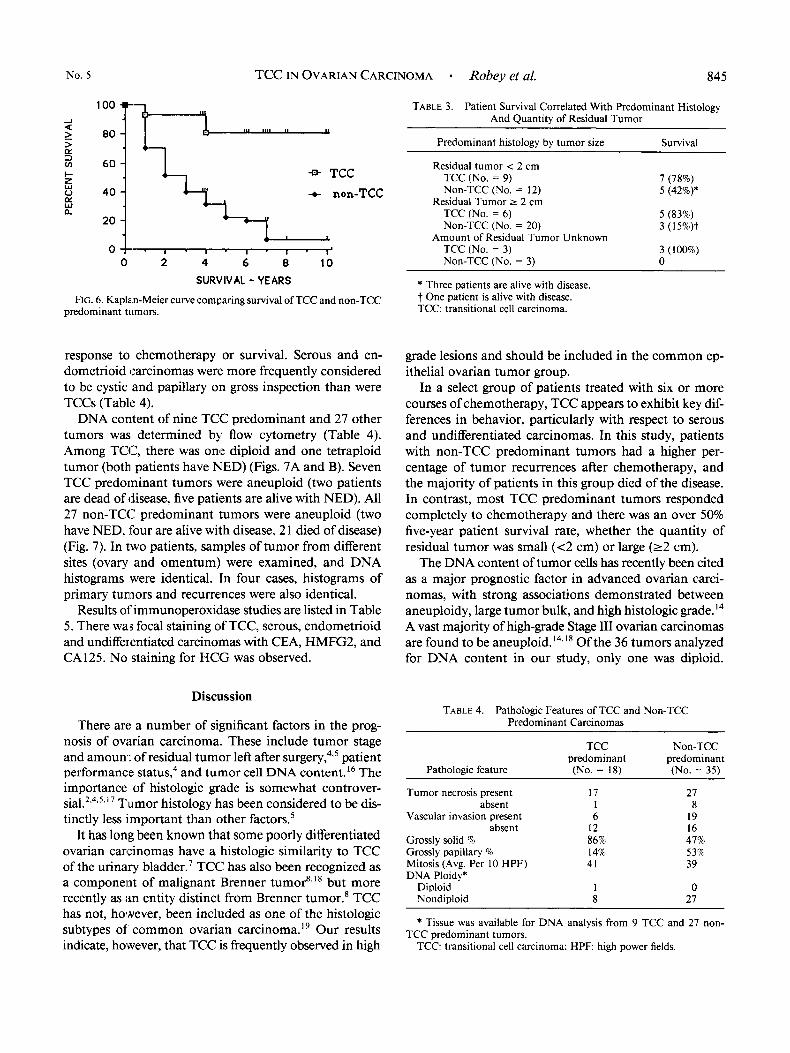
The predominant histologic pattern of the tumors cor- related with the patients’ response to chemotherapy and survival (Table 2). Seventeen of 18 TCC predominant tumors responded completely to chemotherapy and 15 of the 18 patients (83%) were alive without disease at an average of 6.8 years (Fig. 6). In comparison, tumors re- curred or progressed in 3 1 of 35 non-TCC predominant
TABLE 2. Grade 3 Stage 111 Ovarian Carcinomas: Complete Response To Chemotherapy and Survival Correlated
With Histologic Type
4 Yrs Survival
Histologic Complete Alive with type (No.) response disease NED
TCC ( 18) 17 (94%) 0 15 (83%) Non-TCC
Papillary (35) 13 (37%) 4 (11.4%) 4 (1 1.4%)
Serous ( 18) 7 (39%) 3 (16%) 0
TCC transitional cell carcinoma; NED. no evidence of disease.
tumors ( 18/ 18 serous, eight of eight undifferentiated, one of three endometrioid and four of six mixed carcinomas). After 4 years of followup, only eight of the 35 patients with non-TCC tumors (22.8%) were alive and four of 35 ( 1 1.4%) had no evidence of disease (NED).
When cases were segregated according to the quantity of residual tumor left after surgery, patients in whom the predominant carcinoma was TCC showed improved sur- vival over those with non-TCC predominant tumors whether the residual tumor was <2 cm or 2 2 cm (Table 3). Other pathologic features, including presence or ab- sence of necrosis, vascular invasion, and number of mi- toses per 10 high-power fields showed no correlation with
FIG. 5A AND B. Serous carcinoma. (A) Papillary tumor showing an irregular luminal border with detached tufts of epithelial cells (X176). (B) Cytology of a serous carcinoma (X 1760).
No. 5 TCC IN OVARIAN CARCINOMA - Robey et al. 845
-1 Q
response to chemotherapy or survival. Serous and en- dometrioid carcinomas were more frequently considered to be cystic and papillary on gross inspection than were TCCs (Table 4).
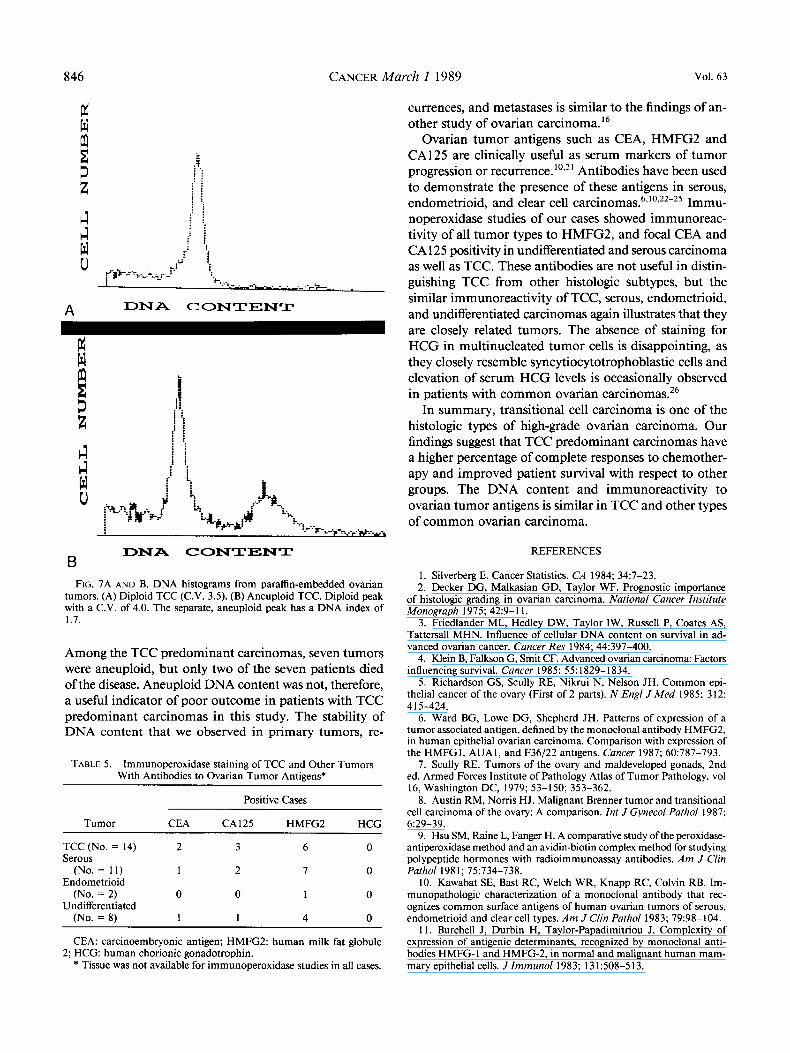
DNA content of nine TCC predominant and 27 other tumors was determined by flow cytometry (Table 4). Among TCC, there was one diploid and one tetraploid tumor (both patients have NED) (Figs. 7A and B). Seven TCC predominant tumors were aneuploid (two patients are dead of disease, five patients are alive with NED). All 27 non-TCC predominant tumors were aneuploid (two have NED, four are alive with disease, 2 1 died of disease) (Fig. 7). In two patients, samples of tumor from different sites (ovary and omentum) were examined, and DNA histograms were identical. In four cases, histograms of primary tumors and recurrences were also identical.
Results of'immunoperoxidase studies are listed in Table 5. There was focal staining of TCC, serous, endometrioid and undifferentiated carcinomas with CEA, HMFG2, and CA125. No staining for HCG was observed.
Discussion
There are a number of significant factors in the prog- nosis of ovarian carcinoma. These include tumor stage and amouni; of residual tumor left after ~ u r g e r y , ~ , ~ patient performance tatu us,^ and tumor cell DNA content.16 The importance of histologic grade is somewhat controver- sia1.2-4-531 ' Tumor histology has been considered to be dis- tinctly less important than other factor^.^
It has long been known that some poorly differentiated ovarian carcinomas have a histologic similarity to TCC of the urinary bladder.7 TCC has also been recognized as a component of malignant Brenner tumor'.'' but more recently as ;in entity distinct from Brenner tumor.' TCC has not, however, been included as one of the histologic subtypes of common ovarian carcinoma.l' Our results indicate, however, that TCC is frequently observed in high
TABLE 3. Patient Survival Correlated With Predominant Histology And Quantity of Residual Tumor
Predominant histology by tumor size Survival
Residual tumor < 2 cm TCC (No. = 9) Non-TCC (No. = 12)
Residual Tumor 2 2 cm TCC (No. = 6 ) Non-TCC (No. = 20)
TCC (No. = 3) Non-TCC (No. = 3) 0
7 (78%) 5 (42%)*
5 (83%) 3 ( 1 5%)t
3 (100%) Amount of Residual Tumor Unknown
* Three patients are alive with disease. t One patient is alive with disease. TCC: transitional cell carcinoma.
grade lesions and should be included in the common ep- ithelial ovarian tumor group.
In a select group of patients treated with six or more courses of chemotherapy, TCC appears to exhibit key dif- ferences in behavior, particularly with respect to serous and undifferentiated carcinomas. In this study, patients with non-TCC predominant tumors had a higher per- centage of tumor recurrences after chemotherapy, and the majority of patients in this group died of the disease. In contrast, most TCC predominant tumors responded completely to chemotherapy and there was an over 50% five-year patient survival rate, whether the quantity of residual tumor was small (<2 cm) or large (22 cm).
The DNA content of tumor cells has recently been cited as a major prognostic factor in advanced ovarian carci- nomas, with strong associations demonstrated between aneuploidy, large tumor bulk, and high histologic grade.I4 A vast majority of high-grade Stage I11 ovarian carcinomas are found to be aneuploid.'4,'8 Of the 36 tumors analyzed for DNA content in our study, only one was diploid.
TABLE 4. Pathologic Features of TCC and Non-TCC Predominant Carcinomas
Pathologic feature
Tumor necrosis present absent
Vascular invasion present
Grossly solid % Grossly papillary 9% Mitosis (Avg. Per 10 HPF) DNA Ploidy*
Diploid Nondiploid
absent
TCC predominant (No. = 18)
17 1 6
12 86% 14% 41
1 8
Non-TCC predominant (No. = 35)
27 8
19 16 47% 53% 39
0 27
* Tissue was available for DNA analysis from 9 TCC and 27 non-
TCC: transitional cell carcinoma; H P F high power fields. TCC predominant tumors.
846 CANCER March 1 1989 Vol. 63
lz w
3 z A A w 0
B
A DNA CONTENT
. . 1 i i
i t
P ! i . . . .
DNA CONTENT B
FIG. 7A AND B. DNA histograms from paraffin-embedded ovarian tumors. (A) Diploid TCC (C.V. 3.5). (B) Aneuploid TCC. Diploid peak with a C.V. of 4.0. The separate, aneuploid peak has a DNA index of 1.7.
Among the TCC predominant carcinomas, seven tumors were aneuploid, but only two of the seven patients died of the disease. Aneuploid DNA content was not, therefore, a useful indicator of poor outcome in patients with TCC predominant carcinomas in this study. The stability of DNA content that we observed in primary tumors, re-
TABLE 5. Immunoperoxidase staining of TCC and Other Tumors With Antibodies to Ovarian Tumor Antigens*
Positive Cases
Tumor CEA CAI25 HMFG2 HCCI
TCC (No. = 14) 2 3 6 0 Serous
(No. = 11) 1 2 I 0 Endometrioid
(No. = 2) 0 0 1 0 Undifferentiated
(No. = 8) 1 1 4 0
CEA: carcinoembryonic antigen; HMFG2: human milk fat globule
* Tissue was not available for immunoperoxidase studies in all cases. 2; HCG: human chorionic gonadotrophin.
currences, and metastases is similar to the findings of an- other study of ovarian carcinoma. l 6
Ovarian tumor antigens such as CEA, HMFG2 and CA125 are clinically useful as serum markers of tumor progression or recurrence. Antibodies have been used to demonstrate the presence of these antigens in serous, endometrioid, and clear cell Immu- noperoxidase studies of our cases showed immunoreac- tivity of all tumor types to HMFG2, and focal CEA and CA 125 positivity in undifferentiated and serous carcinoma as well as TCC. These antibodies are not useful in distin- guishing TCC from other histologic subtypes, but the similar immunoreactivity of TCC, serous, endometrioid, and undifferentiated carcinomas again illustrates that they are closely related tumors. The absence of staining for HCG in multinucleated tumor cells is disappointing, as they closely resemble syncytiocytotrophoblastic cells and elevation of serum HCG levels is occasionally observed in patients with common ovarian carcinomas.26
In summary, transitional cell carcinoma is one of the histologic types of high-grade ovarian carcinoma. Our findings suggest that TCC predominant carcinomas have a higher percentage of complete responses to chemother- apy and improved patient survival with respect to other groups. The DNA content and immunoreactivity to ovarian tumor antigens is similar in TCC and other types of common ovarian carcinoma.
REFERENCES
1. Silverberg E. Cancer Statistics. CA 1984; 34:7-23. 2. Decker DG, Malkasian GD, Taylor WF. Prognostic importance
of histologic grading in ovarian carcinoma. National Cancer Institute Monograph 1975; 42:9-11.
3. Friedlander ML, Hedley DW, Taylor IW, Russell P, Coates AS, Tattersall MHN. Influence of cellular DNA content on survival in ad- vanced ovarian cancer. Cancer Res 1984; 44:397-400.
4. Klein B, Falkson G, Smit CF. Advanced ovarian carcinoma: Factors influencing survival. Cancer 1985; 55: 1829- 1834.
5. Richardson GS, Scully RE, Nikrui N, Nelson JH. Common epi- thelial cancer of the ovary (First of 2 parts). N Engl JMed 1985; 312:
6. Ward BG, Lowe DG, Shepherd JH. Patterns of expression of a tumor associated antigen, defined by the monoclonal antibody HMFGZ, in human epithelial ovarian carcinoma. Comparison with expression of the HMFGI, AUAI, and F36f22 antigens. Cancer 1987; 60:787-793.
7. Scully RE. Tumors of the ovary and maldeveloped gonads, 2nd ed. Armed Forces Institute of Pathology Atlas of Tumor Pathology, vol 16, Washington DC, 1979; 53-150; 353-362.
8. Austin RM, Noms HJ. Malignant Brenner tumor and transitional cell carcinoma of the ovary: A comparison. Int J Gynecol Pathol 1987;
9. Hsu SM, Raine L, Fanger H. A comparative study ofthe peroxidase- antiperoxidase method and an avidin-biotin complex method for studying polypeptide hormones with radioimmunoassay antibodies. Am J Clin Pathol 1981; 75:734-738.
10. Kawabat SE, Bast RC, Welch WR, Knapp RC, Colvin RB. Im- munopathologic characterization of a monoclonal antibody that rec- ognizes common surface antigens of human ovarian tumors of serous, endometrioid and clear cell types. Am J Clin Pathol 1983; 79:98-104.
1 1. Burchell J, Durbin H, Taylor-Papadimitriou J. Complexity of expression of antigenic determinants, recognized by monoclonal anti- bodies HMFG-1 and HMFG-2, in normal and malignant human mam- mary epithelial cells. J Imrnunol 1983; 131:508-5 13.
41 5-424.
6129-39.

No. 5 TCC IN OVARIAN CARCINOMA - Robey et al. 847
12. McLemore DD, Wall TJ, Stephens LC, Jardine JH. Processing of paraffin embedded tissues for flow cytometry. J Histotechnol 1987; 10:109-113.
13. Hedley IDW, Friedlander ML, Taylor IW. Application of DNA flow cytometry to paraffin-embedded archival material for the study of aneuploidy and its clinical significance. Cytometry 1985; 6:327-333.
14. Hedley :DW, Friedlander ML, Taylor IW, R u g CA, Musgrove EA. Method for analysis of cellular DNA content of paraffin-embedded pathological material using flow cytometry. J Histochem Cylochem 1983; 3 1:1333-1335.
15. Kaplan :EL, Meier P. Nonparametric estimation from incomplete observations. J Am Stat Assoc 1958; 53:457-481.
16. Rodenburg CJ, Cornelisse CJ, Heintz PAM, Hermans J, Fleuren GJ. Tumor ploidy as a major prognostic factor in advanced ovarian cancer. Cancer 1987; 59:3 17-323.
17. Sorbe B, Frankendal B, Veress B. Importance of histologic grading in the prognosis of epithelial ovarian carcinoma. Obstet Gynecol 1982; 59:576-582.
18. Ryback BJ, Ober WB, Bernacki EG. Malignant Brenner tumor of the ovary: Report of three cases. Diagn Gynecol Obstet 198 I ; 3:61- 74.
19. Serov S’F, Scully RE, Sobin LH. International histological clas- sification ofturnors, No. 9. Histological typing of ovarian tumors, World Health Organixation, Geneva, 1973; 17-18.
20. Feichter GE, Kiihn W, Czernobilsky B et al. DNA flow cytometry of ovarian tumors with correlation to histopathology. Znt J Gynecol Pathol
2 I . Bergmann J-F, Bidart J-M, George M, Beaugrand M, Levy VG, Bohuon C. Elevation of CA 125 in patients with benign and malignant ascites. Cancer 1987; 59:213-217.
22. Baker VV, Haskill S, Fowler WC, Walton LA, Cume JL. Cellular DNA content and CA-125 antigen expression in ovarian carcinomas. Oncology 1987; 44:283-286.
23. Kawabat SE, Bast RC, Bhan AK, Welch WR, Knapp RC, Colvin RB. Tissue distribution of a coelomic-epithelium-related antigen rec- ognized by the monoclonal antibody OC125. Znt JGynecol Patholl983; 2:275-285.
24. Nouwen EJ, Hendrix PG, Dauwe S, Eerdekens MW, DeBroe ME. Tumor markers in the human ovary and its neoplasms: A comparative immunohistochernical study. Am J Pathol 1987; 126:230-242.
25. Shishi J, Ghazizadeh M, Oguro T, Aihara K, Araki T. Immu- nohistochemical localization of CA 125 antigen in formalin-fixed paraffin sections of ovarian tumors with the use of Pronase. Am J Clin Pathol
26. Samaan NA, Smith JP, Rutledge FN, Schultz PN. The significance of measurement of human placental lactogen, human chorionic gonad- otropin, and carcinoembryonic antigen in patients with ovarian carci- noma. Am J Obstet Gynecol 1976; 126:186-189.
1985; 4:336-345.
1986; 85:595-598.





























