Embed Size (px)
Citation preview

Acta Scientiarum Lundensia (open access) Vol. 2012-010 2012-10-14
1
http://www2.msf.lu.se/b-persson/
Volym ASL 2012-010 Citation: (Acta Scientiarum Lundensia)
Persson B. R. R., Engström, P., Grafström, G., Bauréus Koch, C., Widegren, B., and Salford, L. G., (2012). Treatment of tumour cell with 5-aza-2-deoxycytidine (DAC) for immune tumour therapy of Glioma in Fischer 344 rats, Acta Scientiarum Lundensia, Vol. 2012-010, pp. 1-21 ISSN 1651-5013

Acta Scientiarum Lundensia (open access) Vol. 2012-010 2012-10-14
2
http://www2.msf.lu.se/b-persson/
Reseach article:
Treatment of tumour cell with 5-aza-2-deoxycytidine (DAC)
for immune tumour therapy of Glioma in Fischer 344 rats
Bertil R.R. Persson,1,4 Per Engström,1,4 Gustav Grafström,1,4
Catrin Bauréus Koch,1,4 Bengt Widegren3,4 and Leif G. Salford2,4
1Dept. Medical Radiation Physics, 2Dept of Neurosurgery, 3Dept of Tumor Immunology, 4Rausing Laboratory, Biomedical Centre, Lund University, 221 85 LUND, Sweden
Corresponding author: Bertil R.R. Persson, Lund University, Dept. of medical radiation physics, Barngatan 2, S-22185 Lund Sweden E-mail: [email protected]
Email addresses: [email protected];[email protected];[email protected]; [email protected];[email protected]

Acta Scientiarum Lundensia (open access) Vol. 2012-010 2012-10-14
3
http://www2.msf.lu.se/b-persson/
Abstract Fisher 344 rats with implanted N29 glioma tumours were treated with Pulsed Electric Fields (PEF) in combination with immunization using either IFN- gene-transfected syngeneic tumour cells or IFN- transfected N29 cells treated with 10 M 5-aza-2-deoxycytidine (DAC). Tumours (N29) were inoculated subcutaneously on both thighs of female F-344 syngeneic rats. The left tumour was treated once with 16 exponential pulses with an electric field strength of 1400 V/cm, and 1.0 ms duration (time constant). No anticancer drugs were given at any time. The following day and then once weekly for three weeks, the animals were given intra-peritoneal injections of irradiated, modified N29 tumour cells. The results were evaluated by daily measuring the size of tumour on both sides of the animals. Treatment with solely PEF in 32 animals resulted in a specific growth rate decrease of 20±6 % on the PEF exposed tumour. The effect at the non targeted tumour was negligible (0±4 %). Treatment with IFN- secreting tumour cells resulted in a significant decrease of tumour growth rate on the right tumour of 20± 2 % (p< 0.05 ) and no significant effect (3±0.3% ) was observed on the left tumour. Immunization with DAC treated IFN secreting cells in 12 animals showed no significant decreased growth rate, on neither the left nor the right tumours. By combining PEF+IFN no significant decrease in growth rate was achieved. But in the combination of PEF and IFN secreting cells grown in DAC medium the tumour growth rate decreased by about 50 % at the PEF treated tumour and there was a decrease of about 20% in tumour growth at the non-PEF treated tumour rate which is about the same as for PEF treatment alone.. Immune therapy of rats with intracranial N32 tumours by immunization with IFN- secreting syngeneic cells treated with DAC resulted in a slight (3%) but not significant increase in survival time. With a single RT fraction of 15 Gy there was, however, a significant increase of 32% in the length of survival time of the rats with N32 tumours (p<0.02). Radiation therapy with a single fraction of 15 Gy combined with immunization with IFN- secreting syngeneic cells treated with DAC resulted in significant (p<0.01) 34% increased length of survival time for the N32 tumours although there were no complete remissions.
Key words: Tumor growth rate, TGR, non-target, Abscopal, Fischer rat, glioma, radiation therapy, RT,
Immunization, syngeneic tumor cells, interferon-gamma, IFN.
Abbreviations: Control, ( Ctrl ); Immunization, (IMU); Interferon gamma, (IFN); Interlukine-18 (IL-18)
Intraperitoneally, (i.p.); Electroporation, (EP); Pulsed Electric Fields (PEF);
Tumor cell line induced by administration of ethyl-N-nitro urea to pregnant Fischer rats (N29);
Tumor growth rate %per day, (TGR); Tumor volume, (TV); Unexposed controls, (UC);
Unexposed tumours, (UE);

Acta Scientiarum Lundensia (open access) Vol. 2012-010 2012-10-14
4
http://www2.msf.lu.se/b-persson/
1. Introduction
The most malignant brain tumours, the malignant glioma (also named glioblastoma multiforme “GBM”- or astrocytoma grade IV) are among the most therapy-resistant human cancers. In a material of more than 1100 patients, operated for such tumours in the neurosurgical clinic at the Lund University Hospital during an 18-year period, only three adults (all specimens histo-pathologically re-evaluated) survived for more than 10 years. One of them had a recurrence after 12 years while two must be regarded as cured as they survive more than 30 years after their surgery (Salford et al., 1988). Despite substantial technical improvements in the current treatment modalities and new treatment modalities the survival rate for glioma patients is still very low (Barnholtz-Sloan et al., 2007 , Skold et al., 2010a, Skold et al., 2010b, Stupp et al., 2005).
In our search for more efficient therapeutic modalities against malignant glioma we have previously showed in an animal model, that electropermeabilization treatment in combination with chemotherapy using Bleomycin enhance the therapeutic effect (Salford et al., 1993). Sersa (1996) used Cisplatin instead of Bleomycin in combination with pulsed electric field treatment also found a stimulated immune response through increased activity of monocytes and T-lymphocytes (Sersa et al., 1996). A review of about the clinical use of bleomycin in the brain has recently been performed with the aim to use electroporation in combination with bleomycin “electrochemotherapy” (Linnert and Gehl, 2009). The conclusions of the reviewed studies were that chemotherapy treatment of brain tumors with bleomycin was fairly tolerable and much smaller amount of bleomycin would be used for “electrochemotherapy”.
Previous studies suggest that the host's immune system is activated after treatment of tumours exclusively with pulsed electric fields (PEF) (Mir et al., 1992, Mir et al., 1995, Roth et al., 1992a, Roth et al., 1992b). A combination of electro chemotherapy and immunotherapy by delivering histo-incompatible cells secreting interleukin-2 (IL-2) have studied (Mir et al., 1995, Orlowski et al., 1997, Orlowski et al., 1988, Ramirez et al., 1998). The tumours investigated were 3LL Lewis lung carcinoma in mice and VX2 tumours transplanted in rabbit liver. Histo-incompatible xenogeneic (interspecies genetic disparity) cells and allergenic (interspecies genetic disparity) cells were transfected to secrete IL-2. These IL-2-secreting cells were injected intra-tumour ally or in the peri-tumoural oedema after electro chemotherapy. The addition of immunotherapy to the electro chemotherapy treatment of rabbit liver tumours increased the cure rate from 30 to 40%. But more important it had a clear anti-metastatic effect on tumour spread in liver and lung. Injection of IL-2-producing cells in combination with electro chemotherapy, and only this treatment, performed on the 3LL tumours in mice, led to cures of also the untreated contra laterally implanted tumours. This systemic anti-tumour effect also resulted in immunity against the tumour and complete protection against further tumour cell inoculation. The same strain and tumour, showed a significant decrease in the number of lung metastases after electro chemotherapy and injection of IL-2-producing cells (Orlowski et al., 1997).
Engström et al. (2001) treated colorectal tumours in the liver with pulsed electric fields in combination with bleomycin (Engström et al. 2001a). Two weeks after this electro chemotherapy treatment, the tumours were excised, sectioned and stained for CD4, CD8

Acta Scientiarum Lundensia (open access) Vol. 2012-010 2012-10-14
5
http://www2.msf.lu.se/b-persson/
positive lymphocytes and macrophages. The results showed overall presence of low levels of CD4 positive lymphocytes and ED2 positive macrophages. Large amounts of CD8 positive lymphocytes were found in viable tumour treated with electric pulses (EP) and bleomycin and the lowest amounts in tumours treated with bleomycin only. The largest amounts of ED1 positive macrophages were found in tumours treated with EP and EP+bleomycin. At 14 days after electro chemotherapy treatment, none out of 13 treated animals showed signs of tumour spread. These results strongly suggest that electro chemotherapy stimulates an activation of the host's immune system against the tumour and prevents tumour spreading (Engström et al. 2001a).
Studies, of rats with N32 glioma tumours immunized with tumour infiltrating leukocytes
from N32- IFN- have been shown to have significantly stronger infiltration by CD8+ T-cells; significantly more NK cells; and increased number of CD25 expressing T-cells compared to
the controls. Therapeutic immunization with IFN- transfected glioma cells was shown induce regression of pre-inoculated intra-cerebral wild type tumours of N32 and a newly developed ENU induced rat glioma cell line called N29 in an animal model (Visse et al., 2000, Visse et al., 1999).
The encouraging results from those animal experiments motivated the start of a human immune-gene therapy study including 20 patients with glioblastoma multiforme, where >80% of the tumour was surgically removed. The primary goal of the study was to ascertain whether
immunisation with autologous tumour cells expressing gene-sequences for human interferon- is safe for the patients. But is also indicated an immunological response that significantly prolonged survival (Salford et al., 2005, Salford et al., 2006, Salford et al., 2002, Salford et al., 2004, Salford et al., 2001, Salford et al., 2011, Visse et al., 2005, Persson et al., 2005).
The tumour, however, escape the host´s immune surveillance by down regulate gene expressions of tumour associated antigens and human Leukocyte antigens (HLA) as well as expression of co-stimulatory molecules (Ahmad et al., 2004, Poschke et al., 2011). One mechanism used by tumor cells to decrease the expression of several genes, including tumor suppressor genes, is epigenetic DNA methylation (Merlo et al., 1995, Razin and A.D., 1980). Among the post-translational processes, DNA methylation is one of the most extensively characterized epigenetic modifications which biological role is to maintain DNA transcriptional quiescent, resulting in gene silencing (Bestor, 2000, Bird, 2002, Jones and Baylin, 2002). This process is dependent upon the action of DNA methyl-transferases (DNMTs), enzymes that catalyze the addition of methyl groups to the 5’ carbon of the cytosine residues (Bird, 2002).
5-Azacytidine (5aza-CR) is a nucleoside analog that binds to RNA and interrupts mRNA translation and when incorporated into DNA inhibits methylation by trapping the enzymes DNA-methyl-transferases (DNMTs) (Gravina et al., 2010). It can selectively activate eukaryotic gene expression, and in some cases, even alter the differentiated state of cells (Jones, 1985). Low-dose schedule of 5-azacytidine followed by donor lymphocyte an infusion (DLIs) has been used for treatment of patients with relapse of acute myeloid leukemia (AML) or chronic myelomonocytic leukemia (CMMoL) after allografting. Overall, 66% of the patients benefited from this treatment, with continued CRs achieved in 4 (16%) patients (Luebbert et al., 2010).

Acta Scientiarum Lundensia (open access) Vol. 2012-010 2012-10-14
6
http://www2.msf.lu.se/b-persson/
The nucleoside analog 5-aza-2-deoxycytidine (5-aza-CdR, decitabine, DAC) is a potent inhibitor of DNA methylation which act as a de-methylating agent which have been used in the treatment of several types of neoplasms (Lubbert, 2000, Almstedt et al., 2010, Luebbert et al., 2009, Luebbert et al., 2010, Cashen et al., 2010, Garcia-Manero and Gore, 2005, Yang et al., 2005, Goffin and Eisenhauer, 2002). This agent can also selectively activate eukaryotic gene expression, and in some cases, even alter the differentiated state of cells by inhibiting enzymes that methylation of cytosine residues in eukaryotic DNA (Jones, 1985). In melanoma cells treated with DAC, up regulation of HLA class I antigens and of HLA-A1 and -A2 alleles and de novo expression of NY-ESO-1 protein have been identified (Coral et al., 2002, Coral et al., 1999). It is now registered pharmaceutical for treatment of malignant melanoma.
In poorly immunogenic gliomas it has been shown that treatment with low concentrations of DAC re-activates the expression of silenced tumor antigens in the glioma cells which might enhance the response of immunotherapy (Natsume et al., 2008, Natsume et al., 2009).
Chemotherapy of neuroblastoma with DAC combined with interferon-gamma IFN- has shown to increase the expression of tumor antigens and MHC molecules on neuroblastoma cells which makes these tumor cell lines more susceptible to CTL-mediated killing (Bao et al.,
2011). Exposure to interferon-gamma (IFN-) or DAC can also be associated with re-activation of down-regulated expression of MHC class I/II antigens in glioma tumours (Adair and Hogan, 2009, Esparza et al., 2001, Natsume et al., 2009, Natsume et al., 2008, Schrump et al., 2006).
The findings mentioned above provide the basis to use of 5-aza-2-deoxycytidine (DAC)
treatment of IFN- transfected tumour cells aimed for immune therapy in the present study. We used Fischer 344 rats with N29 glioma tumours subcutaneously implanted on both flanks to study the immunoreactions.
In two groups of Fischer-344 syngeneic rats N32 tumours were inoculated intracerebrally. After one week a single radiotherapy session (RT) was given with 15 Gy of 60Co-gamma radiation the animals combined with immune therapy (IT). This was given within 2 hours
before irradiation by intraperitoneally injections of IFN- transfected N32 tumour cells treated with DAC and then repeated once weekly at most for three weeks
2 Material and methods (L14: 24,14)
2.1 Animals
We use inbred Fischer-344 rats of both sexes, females weighing around 190 g and males 370 g respectively. The strain was maintained by continuous, single-line brother/sister mating in our laboratory. During the experiment the rats were housed in a climate controlled cabinet and all other time they were kept in Macralon cages provided with food pellets and water ad libitum. All experimental animal procedures were approved by the Animal Ethical Committee in Malmö/Lund (Lunds tingsrätt, Box 75, 22100 Lund Sweden). The animals were observed daily for symptoms of the growing tumours, such as losing weight, unwillingness to move, shaggy fur and reddening of the eyes and nose. When an animal developed such symptoms or the

Acta Scientiarum Lundensia (open access) Vol. 2012-010 2012-10-14
7
http://www2.msf.lu.se/b-persson/
largest tumour exceeded 9 cm3, it was euthanized.
2.2 Cell lines and culture
The rat glioma N29 and N32 cell line was induced by administration of ethyl-N-nitro urea to 17 - 18-days pregnant Fischer rats. At 205 days after administration 80-90% of the offspring developed tumours in the central or peripheral nervous system. The cell-lines have been successfully propagated both in vitro and in vivo. (Siesjö et al., 1996). All cells were cultured in antibiotic-free RPMI-1640 medium supplemented with 5-10% foetal calf serum, 2 mM L-glutamine, 10 mM HEPES, 0.5 mM pyruvate and 0.096% NaHCO3. Cell-cultures were regularly checked for contaminating microbes by staining with the fluorescent dye Hoechst 32 258, examined with fluorescent microscopy. Cultures with suspected Mycoplasma infection were eliminated or treated with Mycoplasma Removal Agent (Hoechst, Germany) twice with 7 days interval, and repeatedly confirmed free of infection. As above cell cultures were maintained in culture flasks (Nunc, Denmark) and harvested by treatment with trypsin / EDTA.
2.3 Transfection of cells for immunization
Cells used for immunization were N29 or N32 tumour cells which were IFN gene transfected
to enhance secretion of interferon-gamma. The IFN gene (The GenBank accession number for
the genes is: IFN, no. AF010466) was inserted into the cloning site (either the BamHI or the EcoRI sites) of the retroviral vector pLXSN (GenBank accession no. M28248n). The gene
constructs were sequenced, and 5 g of plasmid DNA was subsequently used to transfect the retroviral packaging cell line GP1E86. Transfectam (Promega, Madison, Wis.) was used for transfect ion, according to the protocol of the manufacturer. The cell colonies which produced the highest number of retroviral particles were selected. Supernatants of these cells were used to infect the tumour cells. The infected tumour cells were cultured on selective media (Geneticin), and several single-cell clones were selected by limiting dilutions. The clones were checked for expression by either Northern blot analysis or semi quantitative polymerase chain reaction, and
verified by studying the expression of the protein. After cell cloning, IFN production was evaluated by ELISA in supernatants that were harvested from tumour cells plated in 48-well plates, incubated for 48 hours at 37°C, and confirmed as 70 ng/106 cells. For immunizations, cells were cultured for 1 week, washed twice, and suspended in medium (Visse et al., 1999). The cells were transferred from the culture flasks to 15 ml centrifuge test tubes (Nanclon) and
stored in a melting ice bath before irradiation with 134Cs -rays using a Gammacell 2000 (Mølsgaard Medical, Risø, Denmark) source. The dose rate was 4.0 Gy/min with a cell density
of 2104 cells/ml in serum free medium (IMDM-0) that does not allow the cells to grow during the procedure. During the irradiation the cells were kept at room temperature. Before and directly after the irradiation they were placed on melting ice. The sterilized cells are not
proliferating but are secreting IFN for some time after administration to the rat.

Acta Scientiarum Lundensia (open access) Vol. 2012-010 2012-10-14
8
http://www2.msf.lu.se/b-persson/
2.4 DAC -treatment of IFN transfected cells
As mentioned above the DNA de-methylating agent 5-aza-2-deoxycytidine (DAC) is a cytosine analogue that covalently binds to DNA methyl-transferase and inhibits its activity which is causing de-methylation. The gene expressions which may be silenced by hyper-methylation of their promoters are re-activated by DAC. Expressions of HLA class I is significantly increased in DAC -treated glioma cells when compared to that in untreated cells, which makes DAC to a potent immune stimulator.
IFN transfected N29 cells was transferred to culture medium containing 10 M 5-aza-2-deoxycytidine (DAC, Sigma-Aldrich) and treated during 3 days in a CO2-incubator. The medium was then replaced with fresh medium without DAC, and the cells were irradiated as above and used for immunization.
2.5 Inoculation and treatment of subcutaneous tumours
The rat glioma N29 was induced in our laboratory by subcutaneous administration in the hind legs. Two hundred thousand (200 000) cells were inoculated into the right leg, whilst 50 000 cells were inoculated into the left leg in order to simulate a secondary smaller tumour. Tumour volume is estimated as an ellipsoid by length, width and thickness measured with a calliper. Tumours were treated about 4 weeks after inoculation when a solid tumour had developed with a diameter of 1-1.5 cm. Before treatment of the tumours, animals were anesthetized with 5% chloral hydrate given intraperitoneally (i.p.).
2.6 Immunization with IFN gene modified N29 tumour cells.
The first immunization with sterilized cells was given five days before the radiation treatment and then two more times with 14-day intervals. Immunization was performed with a number of
3106 IFN gene modified N29 tumour cells (with or without DAC treatment) injected intraperitoneally.
2.7 Pulsed Electric Field (PEF) treatment (EP).
Two rectangular flat electrodes were mounted on a slide calliper and connected to an exponential pulse generator (Figure 1). In the first series of experiment we used a BTX600 ( Genetronics, San Diego, USA) and since year 2000 a CytorExp 2000 (Aditus Medical AB, Lund Sweden) was used.
The pulsed delivered was monitored by an oscilloscope and the load was adjusted so that the time constant of the exponential pulse was 1 ms.
The hair over the tumour was shaved off and the skin was carefully covered with electrocardial paste to ensure good electrical contact between electrodes and skin. The paste also moistened the skin, reducing the transdermal impedance and limited the risk of skin

Acta Scientiarum Lundensia (open access) Vol. 2012-010 2012-10-14
9
http://www2.msf.lu.se/b-persson/
necrosis from the pulse treatment. The tumours were gently fixed in position between the two electrodes, and the voltage was adjusted to the distance between the electrodes to deliver pulses of identical field strength to all tumours. Sixteen pulses of approximately 1400 V/cm with a time constant of 1 ms were delivered transdermally to the whole tumour during approx. 20 seconds. This treatment was repeated daily for four days.
Figure 1 Experimental set-up for electric impulse treatment
2.8 Inoculation and radiation treatment of intra-cerebral tumours
Inoculation was performed by injection of 5000 N32 cells, in 5 l nutrient solution into the head of the right caudate nucleus of Fischer 344 rats. A stereotaxic technique with a Hamilton syringe was used and to avoid extra-cranial tumour growth, the injection site was cleaned with 70% ethanol after injection and the borehole was sealed with wax.
Treatment was performed with the animals arranged into groups of controls, radiation therapy with 15 Gy, immunization and the combinations of radiation therapy with immune therapy.
Acta Scientiarum Lundensia (open access) Vol. 2012-010 2012-10-14
10
http://www2.msf.lu.se/b-persson/
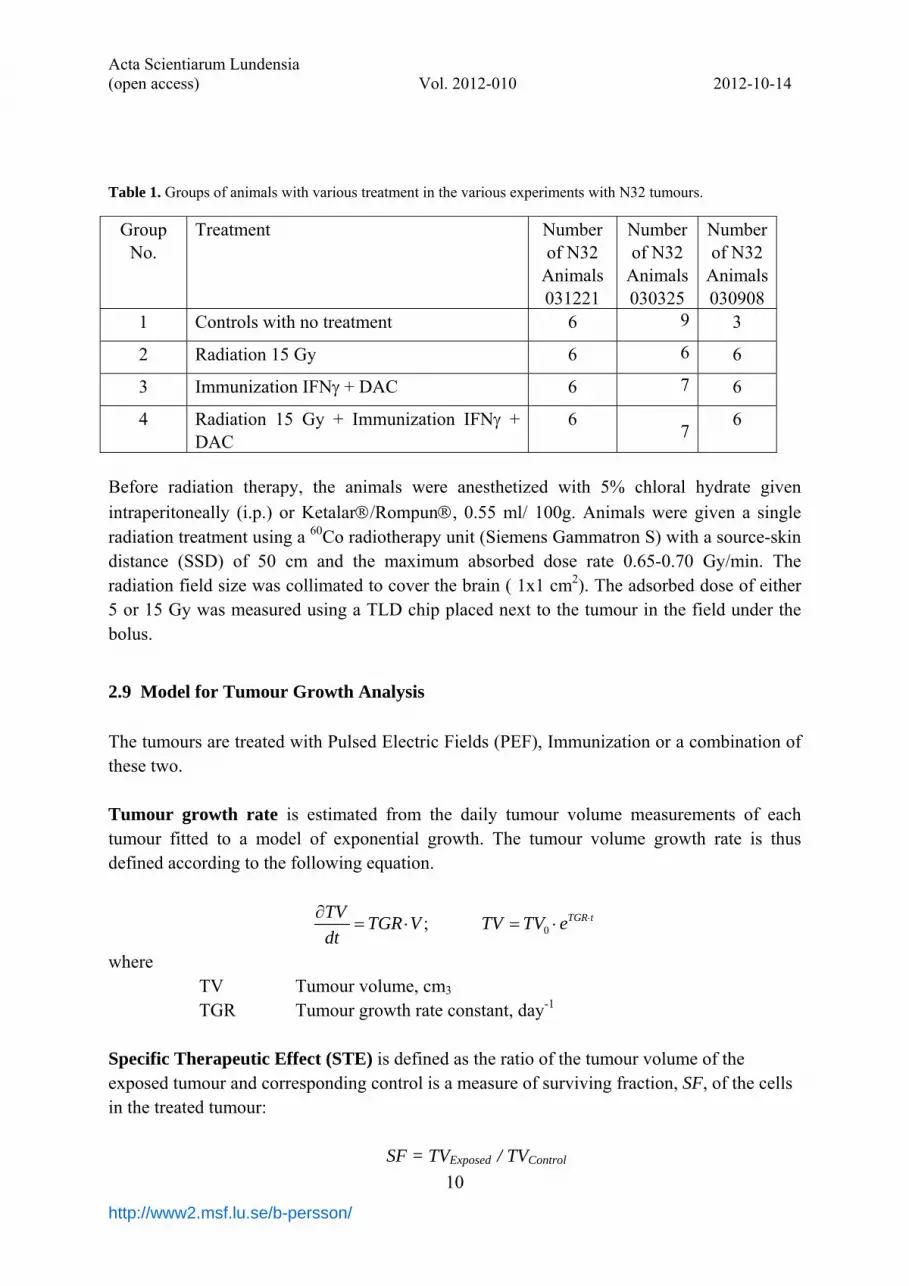
Table 1. Groups of animals with various treatment in the various experiments with N32 tumours.
Group No.
Treatment Number of N32
Animals 031221
Number of N32
Animals 030325
Number of N32
Animals030908
1 Controls with no treatment 6 9 3
2 Radiation 15 Gy 6 6 6
3 Immunization IFN + DAC 6 7 6
4 Radiation 15 Gy + Immunization IFN + DAC
6 7
6
Before radiation therapy, the animals were anesthetized with 5% chloral hydrate given
intraperitoneally (i.p.) or Ketalar/Rompun, 0.55 ml/ 100g. Animals were given a single radiation treatment using a 60Co radiotherapy unit (Siemens Gammatron S) with a source-skin distance (SSD) of 50 cm and the maximum absorbed dose rate 0.65-0.70 Gy/min. The radiation field size was collimated to cover the brain ( 1x1 cm2). The adsorbed dose of either 5 or 15 Gy was measured using a TLD chip placed next to the tumour in the field under the bolus.
2.9 Model for Tumour Growth Analysis
The tumours are treated with Pulsed Electric Fields (PEF), Immunization or a combination of these two. Tumour growth rate is estimated from the daily tumour volume measurements of each tumour fitted to a model of exponential growth. The tumour volume growth rate is thus defined according to the following equation.
0; TGR tTVTGR V TV TV e
dt
where TV Tumour volume, cm3 TGR Tumour growth rate constant, day-1
Specific Therapeutic Effect (STE) is defined as the ratio of the tumour volume of the exposed tumour and corresponding control is a measure of surviving fraction, SF, of the cells in the treated tumour:
SF = TVExposed / TVControl

Acta Scientiarum Lundensia (open access) Vol. 2012-010 2012-10-14
11
http://www2.msf.lu.se/b-persson/
The therapeutic effect, TE, is a measure of the number of lethal events that has occurred
in the cells of the treated tumour volume and thus defined as:
TE = – ln(SF) = [TGRControl – TGRExposed ]·t In order to get a therapeutic effect measure independent of time a quantity named
“specific therapeutic effect” STE is defined. That is the tumour growth rate difference between the control and exposed tumour divided by tumour growth rate of the controls.
For an individual rat; expSTE Control osed ControlTGR TGR TGR
For a group of N exposed rats 1
1STE = ;
N
C ENi
Ci
TGR TGR
TGR
where E
iTGR
The average of the individual Tumour growth rate constant (day-1) in the group
CTGR
The average of the individual Tumour growth rate constant (day-1) in the group of unexposed control rats.
The STE is equal to 0 when the average of tumour growth rate constant of the exposed
group, is equal to the average of the tumour growth rate constant of the control. The STE is equal to 1 when the average tumour growth rate constant of the exposed
group, is equal to 0, which means arrested tumour growth. The STE is larger than 1 when the average tumour growth rate constant of the exposed
group, is negative (< 0), which means a declining tumour volume.
2.10 Statistics
Since the experimental data represent a relatively small sample we apply the Fisher Exact Probability Test for the analysis of the survival rate. For analyzing the significance of survival time we apply both t-test and Mann-Whitney test for comparison.
3. Results
The tumours are treated with Pulsed Electric Fields (PEF), Immunization or a combination of these two. Tumour growth rate (TGR) is estimated after the first treatment from the volume of each tumour fitted to a model of exponential growth.

Acta Scientiarum Lundensia (open access) Vol. 2012-010 2012-10-14
12
http://www2.msf.lu.se/b-persson/
The general immunological effect was evaluated by comparing the growth rate of the untreated contra lateral tumours.
3.1 Experiments
Experiment 1: Rats (3 animals in each group) with N29 glioma tumours implanted on both
flanks were treated with Pulsed Electric Fields (PEF) followed by injections of IL-18 or IFN- secreting cells. The left tumour was treated once with 16 pulses at an electric field strength of 1400 V/cm, and 1.0 ms duration (time constant).
The tumour growth rate of tumours animals treated with either IFN or IL18 syngeneic tumour cells with and without PEF treatment showed no difference in contra lateral tumour growth compared to animals given no treatment. But a significantly (p<0.05) inhibited growth
rate was observed, in animals given Pulsed Electric Fields (PEF) in combination with IFN- secreting cells.
The combined treatment also resulted in a prolonged survival (the time for the contra lateral tumour to reach the predetermined limit volume), by 50%. These preliminary results indicated that a systemic response of the host's immune system can been achieved against the tumour. It encouraged to more studies of Pulsed Electric Fields combined with
immunotherapy using syngeneic IFN- secreting tumour cells. Experiment 2: Rats (6 rats in each group) with N29 glioma tumours implanted on both flanks were treated with either Square or Exponential Pulsed Electric Fields (PEF) followed by
injections IFN- secreting cells. Tumours (N29) were inoculated subcutaneously on both thighs of female Fischer-344 syngeneic rats. The left tumour was treated four days with 16 pulses at electric field strength of 1400 V/cm, and 1.0 ms duration (time constant of exponential pulses and pulse length of square pulses). A significant (p<0.05) decrease in growth-rate was just found in the tumours treated with exponential pulses 33 ± 13 % and in
combination with syngeneic IFN- secreting tumour cells 18 ± 7 %. For the left tumours in the same groups the corresponding decrease in growth-rate were 17± 9 % and 6 ± 10 % which might indicate a general immune response. Experiment 3: Rats (8 rats in each group) with N29 glioma tumours implanted on both flanks
were treated with exponential Pulsed Electric Fields (PEF) followed by injections IFN- secreting cells. Tumours (N29) were inoculated subcutaneously on both thighs of female Fischer-344 syngeneic rats. The left tumour was treated four days with 16 pulses at electric field strength of 1400 V/cm, and 1.0 ms duration (time constant of exponential pulses and pulse length of square pulses).
The decrease in tumour growth rate was about the same in the PEF treated tumour either
without (26 ± 6 %) or with (22 ± 6 %) immunization with syngeneic IFN- secreting tumour
cells. For the left tumours in the same IFN- group the corresponding decrease was 14± 1 % while no general response was recorded in the other groups.
Acta Scientiarum Lundensia (open access) Vol. 2012-010 2012-10-14
13
http://www2.msf.lu.se/b-persson/
Experiment 4: Rats (8 rats in each group) with N29 glioma tumours implanted on both flanks
were treated with exponential Pulsed Electric Fields (PEF) followed by injections IFN- secreting cells or DEC treated IFN- secreting cells. Tumours (N29) were inoculated subcutaneously on both thighs of female Fischer-344 syngeneic rats. The left tumour was treated four days with 16 pulses at electric field strength of 1400 V/cm, and 1.0 ms duration (time constant of exponential pulses and pulse length of square pulses).
The PEF treatment caused a decrease in growth-rate on the right tumour of 33 ± 9 % and
27 ± 5 % in combination with syngeneic IFN- secreting tumour cells. In these groups no effect was observed on the opposite untreated tumour. But in combination with DAC treated
syngeneic IFN- secreting tumour cells the decrease in tumour growth rate was 51 ± 16 % for the PEF treated tumour and 37 ± 9 % for the opposite untreated tumour. This might indicate a strong immunological response of the DEC treated cells.
Experiment 5: Rats (7- 9 rats in each group) with N29 glioma tumours implanted on both flanks were treated with exponential Pulsed Electric Fields (PEF) followed by injections IFN-
secreting cells or DAC treated IFN- secreting cells. Tumours (N29) were inoculated subcutaneously on both thighs of female Fischer-344 syngeneic rats. The left tumour was treated four days with 16 pulses at electric field strength of 1400 V/cm, and 1.0 ms time constant of the exponential pulses.
The PEF treatment on the right tumour caused a decrease in growth-rate of 26 ± 6 % and
22 ± 6 % in combination with syngenic IFN- secreting tumour cells. No effect was observed
on the opposite untreated tumour. But in combination with DAC treated syngeneic IFN- recreating tumour cells the decrease in growth-rate was 40 ± 5 % for the PEF treated tumour and 5 ± 0.5 % .for the opposite untreated tumour.
3.2 Summary of experiments 1-5 including PEF and/or immunization
Rats with N29 glioma tumours implanted on both flanks were treated either independently
with exponential pulsed electric fields (PEF) or i.p. injections with IFN secreting cells (with or without DAC treatment) and in their combinations. The right tumour was treated with PEF (one. two or four days with 16 pulses at electric field strength of 1400 V/cm. and 1.0 ms time
constant) and / or immunisation with syngeneic IFN secreting cells (with or without DAC treatment) and their combinations. The contra-lateral left tumour received no treatment with
pulsed electric fields PEF but was affected by the immunisation with IFN secreting cells.
Acta Scientiarum Lundensia (open access) Vol. 2012-010 2012-10-14
14
http://www2.msf.lu.se/b-persson/
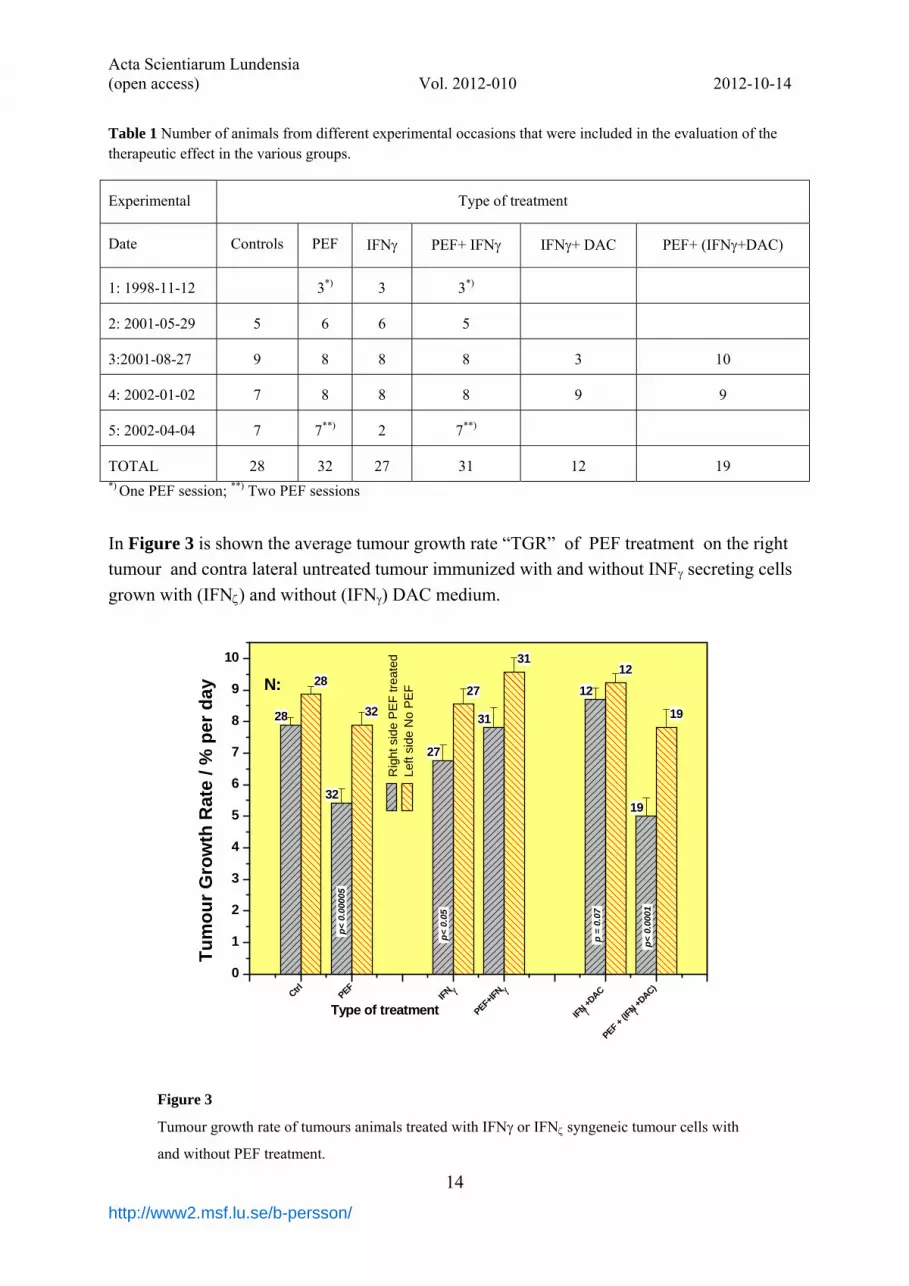
Table 1 Number of animals from different experimental occasions that were included in the evaluation of the therapeutic effect in the various groups.
Experimental Type of treatment
Date Controls PEF IFN PEF+ IFN IFN+ DAC PEF+ (IFN+DAC)
1: 1998-11-12 3*) 3 3*)
2: 2001-05-29 5 6 6 5
3:2001-08-27 9 8 8 8 3 10
4: 2002-01-02 7 8 8 8 9 9
5: 2002-04-04 7 7**) 2 7**)
TOTAL 28 32 27 31 12 19 *) One PEF session; **) Two PEF sessions
In Figure 3 is shown the average tumour growth rate “TGR” of PEF treatment on the right
tumour and contra lateral untreated tumour immunized with and without INF secreting cells
grown with (IFN) and without (IFN) DAC medium.
28
32
27
31
12
19
28
32
27
3112
19
Ctrl
PEF IF
N
PEF+IF
N
IFN +
DAC
PEF +
(IFN +
DAC) 0
1
2
3
4
5
6
7
8
9
10
p<
0.0
001
p =
0.0
7
p<
0.0
5
Tu
mo
ur
Gro
wth
Rat
e /
% p
er d
ay
Type of treatment
Rig
ht s
ide
PE
F tr
eate
d L
eft s
ide
No
PE
FN:
p<
0.0
0005
Figure 3
Tumour growth rate of tumours animals treated with IFN or IFN syngeneic tumour cells with
and without PEF treatment.

Acta Scientiarum Lundensia (open access) Vol. 2012-010 2012-10-14
15
http://www2.msf.lu.se/b-persson/
In Figure 4 is shown the Specific Theraåeutc effect “STE” of PEF treatment on the right
tumour and contra lateral untreated tumour immunized with and without INF secreting cells
grown with (IFN) and without (IFN) DAC medium.
27
12
32
31
19
27
12
32
31
19
IFN
IFN +DAC
PEF
-
PEF+IFN
PEF+(IFN + DAC)
-0,3 -0,2 -0,1 0,0 0,1 0,2 0,3 0,4 0,5
Specific Therapeutic Effect "STE"
Left No PEF treatment Right PEF treatment
Type of treatment
Figure 4 Specific Theapeutic effect (STE) of tumours animals treated with
IFN or IFN syngeneic tumour cells with and without PEF treatment.
The PEF treatment on the right tumour caused a decrease in growth-rate of 30±3 % (p< 0.00005). But no significant effect (10±1%) was observed on the opposite untreated tumour.
Treatment with IFN- secreting tumour cells resulted in a significant decrease of tumour growth rate on the right tumour of 20± 2 % (p< 0.05 ) and no significant effect (3±0.3 % ) was observed on the left tumour.
PEF in combination with syngeneic IFN- secreting tumour cells resulted in no significant decrease in tumour growth-rate on neither right (1±0.0%) nor left (zero) tumour.
Treatment with DAC treated IFN- secreting tumour cells resulted in no decrease of tumour growth rate on neither the right tumour nor the left tumour.
But PEF in combination with DAC treated syngeneic IFN- secreting tumour cells resulted in significant decrease in growth-rate of 40 ± 5 % ( p< 0.0001 ) for the PEF treated tumour and a slight decrease 10 ± 0.1 % .for the left, not PEF treated tumour.

Acta Scientiarum Lundensia (open access) Vol. 2012-010 2012-10-14
16
http://www2.msf.lu.se/b-persson/
3.3 Survival of Fischer 344 rats with intracerebrally implanted N32 glioma tumours after radiation therapy combined with immunization by syngeneic IFN- secreting tumour cells treated with DAC.
The pooled results of the experiments 030325 and 031908 in terms of the mean survival time
in each group animals with intra cerebral N32 tumours treated with IFN transfected cells treated with DAC immunization, radiation therapy and their combination are given in Figure 5
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 320
2
4
6
median survival (d): 19 3
Time after inoculation / days
Con
trol
s
Number of living rats (Exp 030325 + 030908)
0
2
4
6
median survival (d): 19.5 1.4t test vs ctrl: NS
Imm
uniz
edIF
N+
DA
C
0
2
4
6
median survival (d): 25 3.1t test vs ctrl: p< 0.02
RT
15 G
y
0
2
4
6
t.test vs ctrl: p<0.01t-test vs rad: p<0,02t-test vs imu: p<0.01
RT
15 G
y +
Imu
median survival (d) 25.5 3.8
Figure 5
Survival plot of intra cerebral implanted N32 tumours Controls (Lower panel). Immunization with syngeneic N32 tumour cells (2nd panel); radiation therapy (3rd panel) and a combination of radiation therapy and immunization (upper panel). (Exp. 030325 + 030908).
In experiment 6 two groups of Fischer-344 syngeneic rats get N32 tumours inoculated intracerebrally. Within one hour after a single radiotherapy session (RT) was given with 15 Gy of 60Co-gamma radiation the animals. Immune therapy (IT) was given by intraperitoneally injections of modified N32 tumour cells secreting interferon-gamma cells treated with DAC before irradiation. The immunization was repeated once weekly at most for three weeks.
Immune therapy (IT) by immunization with IFN- secreting syngeneic cells treated with DAC resulted in a slight (3%) but not significant increase in survival time. A single RT fraction of 15 Gy there was a significant increase of 32% in the length of survival time of the rats with N32 tumours (p<0.02). Radiation therapy with a single fraction of 15 Gy combined
with immunization with IFN- secreting syngeneic cells treated with DAC resulted in

Acta Scientiarum Lundensia (open access) Vol. 2012-010 2012-10-14
17
http://www2.msf.lu.se/b-persson/
significant (p<0.01) 34% increased length of survival time for the rats with N32 tumours although there were no complete remissions.
4. Discussions and Conclusion
In the first experiment rats with N29 glioma tumours implanted on both flanks were
treated with Pulsed Electric Fields (PEF) followed by injections of either IL-18 or IFN- gene transfected syngeneic tumour cells. A significantly inhibited tumour growth rate was
observed, in animals given Pulsed Electric Fields (PEF) combined with IFN- secreting cells and in animals given PEF combined with IL-18 secreting cells. The tumour growth-rate
decreased mostly in the combination PEF+IFN and the in following experiments therefore
only IFN transfected cells were used. In a following experiment rats with N29 glioma tumours implanted on both flanks were
treated with either square or exponential Pulsed Electric Fields (PEF) followed by injections
of IFN- secreting cells. Tumours (N29) were inoculated subcutaneously on both thighs of female Fischer-344 syngeneic rats. The left tumour was treated four days with 16 pulses at electric field strength of 1400 V/cm, and 1.0 ms time constant of exponential pulses or 1.0 ms pulse length of square pulses. We found that the treatment with exponential pulses were more efficient than square wave pulsed both alone and in combination with immune therapy. Thus in the following experiments we used just exponential pulses PEF treatment.
In total five experimental sessions were performed embodying in total 149 animals of which 28 were controls. PEF treatment alone was performed in 32 animals which caused a decrease in growth-rate of 30± 3 % (p< 0.00005) for the treated tumour. But no significant decrease in tumour growth rate was observed on the opposite untreated tumour, which indicates that no general immune response was achieved by PEF treatment alone.
Treatment with i.p. injection of IFN- secreting syngeneic tumour cells was performed in 27 animals. This treatment resulted in a significant decrease of tumour growth rate on the larger right tumour of 20±2 % (p< 0.05). But no significant effect (3±0.3%) was observed on the smaller left tumour that indicates a larger immune-suppression of the smaller tumour.
PEF treatment in combination with syngeneic IFN- secreting tumour cells was performed in 31 animals. This combined treatment did not resulted in any significant decrease in tumour growth-rate on neither the right (1±0.0%) nor the left (zero) tumours. Thus the PEF
treatment seems to extinguish the immune response recorded with immunization with IFN- secreting tumour cells alone.
By using i.p. injection of DAC treated IFN- secreting tumour cells in 12 animals no decrease of tumour growth rate was achieved neither on the right tumours nor the left
tumours. Thus the DAC treatment IFN- secreting tumour cells seems to extinguish its immune stimulating effect. But PEF treatment of 19 animals in combination with i.p. injection
of DAC treated syngeneic IFN- secreting tumour cells resulted in significant decrease in growth-rate of 40 ± 5 % ( p< 0.0001 ) for the PEF treated tumour and a slight decrease 10 ± 0.1 % for the left, not PEF treated tumour. These results are slightly but not significantly better than treatment with PEF alone (right p=0.7; left p=0.2). In conclusion PEF treatment of

Acta Scientiarum Lundensia (open access) Vol. 2012-010 2012-10-14
18
http://www2.msf.lu.se/b-persson/
tumours in combination with IFN- secreting tumour cells does not decrease the growth rate of the N29 glioma tumours.
In animals, with intra-cerebral brain N32 tumours inoculated in the brain of Fischer-344
syngeneic rats, immune therapy (IT) by immunization with IFN- secreting syngeneic cells treated with DAC resulted in a slight (3%) but not significant increase in survival time. With a single 15 Gy fraction radio-therapy there was a significant (p<0.02) increase of 32% in the length of survival time of the rats with N32 tumours. Radiation therapy with a single 15 Gy
fraction combined by immunization with IFN- secreting syngeneic cells treated with DAC resulted in significant (p<0.01) 34% increased length of survival time compared to the controls rats. No complete remission, however, was observed in any group. The mean survival time of 25.5 days in the group with combined treatment using DAC treated cells is somewhat longer but not significant different from the 23 days recorded for combined
treatment with immunization using IFN- secreting syngeneic cells (Persson et al., 2010). A recent study has confirmed our previous results that in an animal model PEF treatment
in combination with i.v. chemotherapy using 1 mg Bleomycin (Lundbeck AB, Sweden) per kg body weight enhance the survival of rats with implanted brain tumours (Salford et al., 1993, Agerholm-Larsen et al., 2011). Agerholm-Larsen et al. (2011) used the same N32 brain tumour model as used by us in the present study (but only 3,000 N32 cells were inoculated in the brain), and injected 42 IU Bleomycin (Baxter A/S) intra-cranially before the application of square pulsed electrical field (32 pulses, 100 V, 0.1 ms, and 1 Hz). They confirmed the tumour volume by magnetic resonance imaging (MRI) before and after the treatment, and found complete remissions in 9 out of 13 rats (69%) receiving the combination of intra-tumoural administration of bleomycin and subsequent PEF (Agerholm-Larsen et al., 2011). Unfortunately, however, they did not examined the immunological response of the treatment, and the short life span of <30 days of the treated rats does not guarantee further non-survivals (cf. Figure 4) and subsequently recurrence of the tumour. The combination of bleomycin and a single radiation therapy session combined with immune therapy might be a more interesting alternative for treatment of human glioma (Persson, 2011, Persson et al., 2010).
References
ADAIR, S. J. & HOGAN, K. T. 2009. Treatment of ovarian cancer cell lines with 5-aza-2′-deoxycytidine upregulates the expression of cancer-testis antigens and class I major histocompatibility complex-encoded molecules. Cancer immunology and immunotherapy., 58, 589-601.
AGERHOLM-LARSEN, B., IVERSEN, H. K., IBSEN, P., MOLLER, J. M., MAHMOOD, F., JENSEN, K. S. & GEHL, J. 2011. Preclinical Validation of Electrochemotherapy as an Effective Treatment for Brain Tumors. Cancer Research, 71, 3753-3762.
AHMAD, M., REES, R. C. & ALI, S. A. 2004. Escape from immunotherapy: possible mechanisms that influence tumor regression/progression. Cancer Immunology, Immunotherapy, 53, 844-854.
ALMSTEDT, M., BLAGITKO-DORFS, N., DUQUE-AFONSO, J., KARBACH, J., PFEIFER, D., JAEGER, E. & LUEBBERT, M. 2010. The DNA demethylating agent 5-aza-2 '-deoxycytidine induces expression of NY-ESO-1 and other cancer/testis antigens in myeloid leukemia cells. Leukemia Research, 34, 899-905.
BAO, L., DUNHAM, K. & LUCAS, K. 2011. MAGE-A1, MAGE-A3, and NY-ESO-1 can be upregulated on neuroblastoma cells to facilitate cytotoxic T lymphocyte-mediated tumor cell killing. Cancer Immunology Immunotherapy, 60, 1299-1307.

Acta Scientiarum Lundensia (open access) Vol. 2012-010 2012-10-14
19
http://www2.msf.lu.se/b-persson/
BARNHOLTZ-SLOAN, J. S., SLOAN, A. E. & SCHWARTZ, A. G. 2007 Cancer of the Brain and Other Central Nervous System. In: GLOECKLER RIES, L. A., YOUNG, J., J. L., KEEL, G. E., EISNER, M. P., D, L. Y. & D, H. M.-J. (eds.) SEER Survival Monograph: Cancer Survival Among Adults: U.S. SEER Program, 1988-2001. Patient and Tumor Characteristics. . Bethesda, MD,: National Cancer Institute, SEER Program, .
BESTOR, T., H. 2000. The DNA methyltransferases of mammals. Human molecular genetics, 9, 2395. BIRD, A. 2002. DNA methylation patterns and epigenetic memory. Genes & Development, 16, 6-21. CASHEN, A. F., SCHILLER, G., J.,, O´DONNELL M. R. & F., D. J. 2010. Multicenter, Phase II Study of
Decitabine for the First-Line Treatment of Older Patients With Acute Myeloid Leukemia. JOURNAL OF CLINICAL ONCOLOGY, 28, 556-561.
CORAL, S., SIGALOTTI, L., ALTOMONTE, M., ENGELSBERG, A., COLIZZI, F., CATTAROSSI, I., MARASKOVSKY, E., JAGER, E., SELIGER, B. & MAIO, M. 2002. 5-aza-2 '-deoxycytidine-induced expression of functional cancer testis antigens in human renal cell carcinoma: Immunotherapeutic implications. Clinical Cancer Research, 8, 2690-2695.
CORAL, S., SIGALOTTI, L., GASPAROLLO, A., CATTAROSSI, I., VISINTIN, A., CATTELAN, A., ALTOMONTE, M. & MAIO, M. 1999. Prolonged upregulation of the expression of HLA class I antigens and costimulatory molecules on melanoma cells treated with 5-aza-2 '-deoxycytidine (5-AZA-CdR). Journal of Immunotherapy, 22, 16-24.
ESPARZA, C., MENDEZ, R., JURADO, J. M., SERRANO, A., MARTINEZ, J., HERNANDEZ, V., RUIZ-CABELLO, F. & GARRIDO, F. 2001. Re-expression of HLA class I antigens and restoration of antigen-specific cytotoxic T lymphocytes in melanoma cells following 5-AZA-2'deoxycytidine treatment. European Journal of Cancer, 37, S417-S418.
GARCIA-MANERO, G. & GORE, S. D. 2005. Future Directions for the Use of Hypomethylating Agents. Seminars in Hematology, 42, S50-S59.
GOFFIN, J. & EISENHAUER, E. 2002. DNA methyltransferase inhibitors-state of the art. Annals of Oncology, 13, 1699-1716.
GRAVINA, G., FESTUCCIA, C., MARAMPON, F., POPOV, V., PESTELL, R., ZANI, B. & TOMBOLINI, V. 2010. Biological rationale for the use of DNA methyltransferase inhibitors as new strategy for modulation of tumor response to chemotherapy and radiation. Molecular Cancer, 9, 305-305.
JONES, P. A. 1985. ALTERING GENE-EXPRESSION WITH 5-AZACYTIDINE. Cell, 40, 485-486. JONES, P. A. & BAYLIN, S. B. 2002. The fundamental role of epigenetic events in cancer. Nature reviews.
Genetics, 3, 415-428. LINNERT, M. & GEHL, J. 2009. Bleomycin treatment of brain tumors: an evaluation. Anti-Cancer Drugs,
20, 157-164. LUBBERT, M. 2000. DNA methylation inhibitors in the treatment of leukemias, myelodysplastic syndromes
and hemoglobinopathies: Clinical results and possible mechanisms of action. DNA Methylation and Cancer, 249, 135-164.
LUEBBERT, M., BERTZ, H., RUETER, B., MARKS, R., CLAUS, R., WAESCH, R. & FINKE, J. 2009. Non-intensive treatment with low-dose 5-aza-2 '-deoxycytidine (DAC) prior to allogeneic blood SCT of older MDS/AML patients. Bone Marrow Transplantation, 44, 585-588.
LUEBBERT, M., BERTZ, H., WAESCH, R., MARKS, R., RUETER, B., CLAUS, R. & FINKE, J. 2010. Efficacy of a 3-day, low-dose treatment with 5-azacytidine followed by donor lymphocyte infusions in older patients with acute myeloid leukemia or chronic myelomonocytic leukemia relapsed after allografting. Bone Marrow Transplantation, 45, 627-632.
MERLO, A., HERMAN, J. G., MAO, L., LEE, D. J., GABRIELSON, E., BURGER, P. C., BAYLIN, S. B. & SIDRANSKY, D. 1995. 5′ CpG island methylation is associated with transcriptional silencing of the tumour suppressor p16/CDKN2/MTS1 in human cancers. Nat Med, 1, 686-692.
MIR, L. M., ROTH, C., ORLOWSKI, S., BELEHRADEK, J., FRADELIZI, D., PAOLETTI, C. & KOURILSKY, P. 1992. POTENTIATION OF THE ANTITUMORAL EFFECT OF ELECTROCHEMOTHERAPY BY AN IMMUNOTHERAPY WITH ALLOGENEIC CELLS PRODUCING INTERLEUKIN-2. Comptes Rendus De L Academie Des Sciences Serie Iii-Sciences De La Vie-Life Sciences, 314, 539-544.
MIR, L. M., ROTH, C., ORLOWSKI, S., QUINTINCOLONNA, F., FRADELIZI, D., BELEHRADEK, J. & KOURILSKY, P. 1995. SYSTEMIC ANTITUMOR EFFECTS OF ELECTROCHEMOTHERAPY COMBINED WITH HISTOINCOMPATIBLE CELLS SECRETING INTERLEUKIN-2. Journal of Immunotherapy, 17, 30-38.

Acta Scientiarum Lundensia (open access) Vol. 2012-010 2012-10-14
20
http://www2.msf.lu.se/b-persson/
NATSUME, A., WAKABAYASHI, T., SHIMATO, S., TSUJIMURA, K., KUZUSHIMA, K. & YOSHIDA, J. 2009. The DNA demethylating agent 5-aza-2-deoxycytidine induces the expression of cancer-testis antigens in human gliomas: Epigenetic target for tumor immunotherapy. Neuro-Oncology, 11, 225-225.
NATSUME, A., WAKABAYASHI, T., TSUJIMURA, K., SHIMATO, S., ITO, M., KUZUSHIMA, K., KONDO, Y., SEKIDO, Y., KAWATSURA, H., NARITA, Y. & YOSHIDA, J. 2008. The DNA demethylating agent 5-aza-2'-deoxycytidine activates NY-ESO-1 antigenicity in orthotopic human glioma. International Journal of Cancer, 122, 2542-2553.
ORLOWSKI, S., AN, D. J., BELEHRADEK, J., JR. & MIR, L. M. 1997. Antimetastatic effects of electrochemotherapy (ECT) and of histoincompatible interleukin-2 (IL-2) secreting cells in the murine Lewis lung tumor (3LL). Proceedings of the American Association for Cancer Research Annual Meeting, 38, 33.
ORLOWSKI, S., BELEHRADEK, J., PAOLETTI, C. & MIR, L. M. 1988. TRANSIENT ELECTROPERMEABILIZATION OF CELLS IN CULTURE - INCREASE OF THE CYTO-TOXICITY OF ANTICANCER DRUGS. Biochemical Pharmacology, 37, 4727-4733.
PERSSON, A., SKAGERBERG, G., SALFORD, L. G., ENGLUND, E. & BRAIN IMMUNO GENE TUMOUR, T. 2005. Immunotreatment in patients with glioblastoma multiforme - a histopathological evaluation of reactive and inflammatory changes. Clinical Neuropathology, 24, 201-208.
PERSSON, B. R. R. 2011. Radiation Immune Modulation Therapy of Glioma, Advances in the Biology, Imaging and Therapies for Glioblastoma. In: CHEN, C. C. (ed.) http://www.intechopen.com/articles/show/title/radiation-immune-modulation-therapy-of-glioma. InTech.
PERSSON, B. R. R., KOCH, C. B., GRAFSTRÖM, G., CEBERG, C., AF ROSENSCHÖLD, P. M., NITTBY, H., WIDEGREN, B. & SALFORD, L. G. 2010. Radiation Immunomodulatory Gene Tumor Therapy of Rats with Intracerebral Glioma Tumors. Radiation Research, 173, 433-440.
POSCHKE, I., MOUGIAKAKOS, D. & KIESSLING, R. 2011. Camouflage and sabotage: tumor escape from the immune system. Cancer Immunology, Immunotherapy, 60, 1161-1171.
RAMIREZ, L. H., ORLOWSKI, S., AN, D., BINDOULA, G., DZODIC, R., ARDOUIN, P., BOGNEL, C., BELEHRADEK, J., MUNCK, J. N. & MIR, L. M. 1998. Electrochemotherapy on liver tumours in rabbits. British Journal of Cancer, 77, 2104-2111.
RAZIN, A. & A.D., R. 1980. DNA Methylation and Gene Function. Science, 210, 604-610. ROTH, C., MIR, L., CRESSENT, M., QUINTINCOLONNA, F., LEY, V., FRADELIZI, D. &
KOURILSKY, P. 1992a. IL-2 GENE TRANSDUCTION IN MALIGNANT-CELLS - APPLICATIONS IN CANCER CONTAINMENT. Bone Marrow Transplantation, 9, 174-176.
ROTH, C., MIR, L. M., CRESSENT, M., QUINTINCOLONNA, F., LEY, V., FRADELIZI, D. & KOURILSKY, P. 1992b. INHIBITION OF TUMOR-GROWTH BY HISTOINCOMPATIBLE CELLS EXPRESSING INTERLEUKIN-2. International Immunology, 4, 1429-1436.
SALFORD, L. G., ASK, E., SIESJÖ, P., SKAGERBERG, G., BAUREUS-KOCH, C., BLENNOW, C., DARABI, A., ELFGREN, C., ENGLUND, E., JANELIDZE, S., LARSSON, E. M., LILJA, A., PERSSON, B. R. R., RYDELIUS, A., STROMBLAD, S., VISSE, E. & WIDEGREN, B. 2005. Immunization with autologous glioma cells transfected with IFN-g gene significantly prolongs survival in GBM-patients older than 50 years. Neuro-Oncology, 7, 370-370.
SALFORD, L. G., BRUN, A. & NIRFALK, S. 1988. 10-YEAR SURVIVAL AMONG PATIENTS WITH SUPRATENTORIAL ASTROCYTOMAS GRADE-III AND GRADE-IV. Journal of Neurosurgery, 69, 506-509.
SALFORD, L. G., PERSSON, B. R. R., BRUN, A., CEBERG, C. P., KONGSTAD, P. C. & MIR, L. M. 1993. A NEW BRAIN-TUMOR THERAPY COMBINING BLEOMYCIN WITH IN-VIVO ELECTROPERMEABILIZATION. Biochemical and Biophysical Research Communications, 194, 938-943.
SALFORD, L. G., RYDELIUS, A., SKAGERBERG, G., SIESJO, P., DARABI, A., PERSSON, B., VISSE, E. & WIDEGREN, B. 2006. Immune therapy significantly prolongs survival of GBM patients. Neuro-Oncology, 8, 351-351.
SALFORD, L. G., SIESJO, P., SKAGERBERG, G., PERSSON, B. R. R., LARSSON, E. M., LINDVALL, M., VISSE, E. & WIDEGREN, B. 2002. Search for effective therapy against glioblastoma multiforme - Clinical immunisation with autologous glioma cells transduced with the human interferon-gamma gene. Developments in Neuroscience, Proceedings, 1247, 211-220.
SALFORD, L. G., SIESJO, P., SKAGERBERG, G., VISSE, E., DARABI, A., LILJA, A., BLENNOW, C., STROMBLAD, S., ASK, E., RYDELIUS, A., PERSSON, B. R. R., KOCH, C. B., ENGLUND, E., LARSSON, E. M., MANDAHL, N. & WIDEGREN, B. 2004. Brain immuno gene tumour therapy (BRIGTT). Neuro-Oncology, 6, 344-344.
Acta Scientiarum Lundensia (open access) Vol. 2012-010 2012-10-14
21
http://www2.msf.lu.se/b-persson/
SALFORD, L. G., SIESJÖ, P., SKAGERBERG, G., PERSSON, B. R. R., LARSSON, E. M., LINDVALL, M., VISSE, E. & WIDEGREN, B. Year. Search for effective therapy against glioblastoma multiforme - clinical immunisation with autologous glioma cells transduced with the human Interferon-g gene In: The 2nd International Mt. BANDAI Symposium for Neuroscience 2001, 2001 Yatsuyamada Koriyama-City, Fukushima 936-8563 Japan. Southern Yohoku Research Institute for Neurosciences, 143-149.
SALFORD, L. G., SIESJÖ, P., SKAGERBERG, G., RYDELIUS, A., BLENNOW, C., LILJA, Å., PERSSON, B. R. R., STRÖMBLAD, S., VISSE, E. & WIDEGREN, B. 2011. Immunization with autologous IFN-g secreting glioma cells in patients with Glioblastoma Multiforme - a phase 1-2 clinical trial. To be published.
SCHRUMP, D. S., FISCHETTE, M., R., NGUYEN, D., M., ZHAO, M., LI, X., KUNST, T. F., HANCOX, A., HONG J., A., CHEN, G. A., PISHCHIK, V., FIGG, W. D., MURGO, A. J. & STEINBERG, S. M. 2006. Phase I Study of Decitabine-Mediated Gene Expression in Patients with Cancers Involving the Lungs, Esophagus, or Pleura. Clinical Cancer Research, 12, 5777-5785.
SERSA, G., KOTNIK, V., CEMAZAR, M., MIKLAVCIC, D. & KOTNIK, A. 1996. Electrochemotherapy with bleomycin in SA-1 tumor-bearing mice - Natural resistance and immune responsiveness. Anti-Cancer Drugs, 7, 785-791.
SIESJÖ, P., VISSE, E. & SJÖGREN, H. O. 1996. Cure of established, intracerebral rat gliomas induced by therapeutic immunizations with tumor cells and purified APC or adjuvant IFN-gamma treatment. Journal of Immunotherapy, 19, 334-345.
SKOLD, K., GORLIA, T., PELLETTIERI, L., GIUSTI, V., H-STENSTAM, B. & HOPEWELL, J. W. 2010a. Boron neutron capture therapy for newly diagnosed glioblastoma multiforme: an assessment of clinical potential. British Journal of Radiology, 83, 596-603.
SKOLD, K., H-STENSTAM, B., DIAZ, A. Z., GIUSTI, V., PELLETTIERI, L. & HOPEWELL, J. W. 2010b. Boron Neutron Capture Therapy for glioblastoma multiforme: advantage of prolonged infusion of BPA-f. Acta Neurologica Scandinavica, 122, 58-62.
STUPP, R., MASON, W. P., VAN DEN BENT, M. J., WELLER, M., FISHER, B., TAPHOORN, M. J. B., BELANGER, K., BRANDES, A. A., MAROSI, C., BOGDAHN, U., CURSCHMANN, J., JANZER, R. C., LUDWIN, S. K., GORLIA, T., ALLGEIER, A., LACOMBE, D., CAIRNCROSS, J. G., EISENHAUER, E., MIRIMANOFF, R. O., VAN DEN WEYNGAERT, D., KAENDLER, S., KRAUSENECK, P., VINOLAS, N., VILLA, S., WURM, R. E., MAILLOT, M. H. B., SPAGNOLLI, F., KANTOR, G., MALHAIRE, J. P., RENARD, L., DE WITTE, O., SCANDOLARO, L., VECHT, C. J., MAINGON, P., LUTTERBACH, J., KOBIERSKA, A., BOLLA, M., SOUCHON, R., MITINE, C., TZUK-SHINA, T., KUTEN, A., HAFERKAMP, G., DE GREVE, J., PRIOU, F., MENTEN, J., RUTTEN, I., CLAVERE, P., MALMSTROM, A., JANCAR, B., NEWLANDS, E., PIGOTT, K., TWIJNSTRA, A., CHINOT, O., RENI, M., BOIARDI, A., FABBRO, M., CAMPONE, M., BOZZINO, J., FRENAY, M., GIJTENBEEK, J., BRANDES, A. A., DELATTRE, J. Y., BOGDAHN, U., DE PAULA, U., VAN DEN BENT, M. J., HANZEN, C., PAVANATO, G., SCHRAUB, S., PFEFFER, R., SOFFIETTI, R., WELLER, M., KORTMANN, R. D., TAPHOORN, M., TORRECILLA, J. L., MAROSI, C., GRISOLD, W., HUGET, P., FORSYTH, P., FULTON, D., KIRBY, S., WONG, R., FENTON, D., FISHER, B., CAIRNCROSS, G., WHITLOCK, P., BELANGER, K., BURDETTE-RADOUX, S., GERTLER, S., SAUNDERS, S., LAING, K., SIDDIQUI, J., MARTIN, L. A., GULAVITA, S., PERRY, J., MASON, W., THIESSEN, B., PAI, H., ALAM, Z. Y., EISENSTAT, D., MINGRONE, W., et al. 2005. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. New England Journal of Medicine, 352, 987-996.
VISSE, E., DARABI, A., ENELL, K., JANELIDZE, S., LARSSON, M., WIDEGREN, B., SKAGERBERG, G., SIESJO, P. & SALFORD, L. 2005. Increased number of leukocytes secreting IFN-gamma in patients immunized with autologous IFN-gamma secreting glioma cells correlate with prolonged survival. Neuro-Oncology, 7, 372-372.
VISSE, E., JOHANSSON, A. C. M., WIDEGREN, B., SJOGREN, H. O. & SIESJO, P. 2000. Immunohistochemical analysis of glioma-infiltrating leucocytes after peripheral therapeutic immunization with interferon-gamma-transfected glioma cells. Cancer Immunology Immunotherapy, 49, 142-151.
VISSE, E., SIESJÖ, P., WIDEGREN, B. & SJÖGREN, H. O. 1999. Regression of intracerebral rat glioma isografts by therapeutic subcutaneous immunization with interferon-gamma, interleukin-7, or B7-1-transfected tumor cells. Cancer Gene Therapy, 6, 37-44.
YANG, H., HOSHINO, K., SANCHEZ-GONZALEZ, B., KANTARJIAN, H. & GARCIA-MANERO, G. 2005. Antileukemia activity of the combination of 5-aza-2'-deoxycytidine with valproic acid. Leukemia Research, 29, 739-748.





























