Embed Size (px)
Citation preview
Need of medical care due to hyperemesis gravidarum in different pregnancy outcomes
Miina Nurmi, 10.10.2019
Results from a nation-wide register study, 2005–2017
We aimed at evaluating the ”burden of illness” caused by HG
1. In terms of the number of hospitalizations and outpatient visits
2. And in different pregnancy outcomes
• Deliveries (live births and stillbirths)
• Gestational trophoblastic disease (molar pregnancies)
• Ectopic pregnancies
• Spontaneous abortions
• Pregnancy terminations
Objective
Miina Nurmi, 10.10.2019
• Data of women with HG diagnosis (N=9,315) between 2005 and
2017 were retrieved from Finnish health care registers
• Finnish Hospital Discharge Register: diagnoses (HG, spontaneous
abortion, gestational trophoblastic disease, ectopic pregnancy)
• N.B. the name of the register – officially Care Register for Health Care
• Inpatient and outpatient data from hospitals, specialized health care
clinics and emergency wards administratively associated with specialized
clinics
• Finnish Medical Birth Register: deliveries
• Finnish Register of Induced Abortions: pregnancy terminations
Methods/Registers
Miina Nurmi, 10.10.2019
• Hyperemesis gravidarum, HG
• All O21 diagnoses in the ICD-10 classification (WHO 2004)
• O21 Excessive vomiting in pregnancy
• O21.0 Mild hyperemesis gravidarum (starting before the end of the 22nd week of gestation)
• O21.1 Hyperemesis gravidarum with metabolic disturbance (starting before the end of the 22nd week of
gestation)
• O21.2 Late vomiting of pregnancy (starting after 22 completed weeks of gestation)
• O21.8 Other vomiting complicating pregnancy
• O21.9 Vomiting of pregnancy, unspecified
• Diagnoses given by physicians in the health care services
• Admission: Diagnosis date
• Readmission: More than diagnosis date during the same pregnancy
Methods/Definitions
Miina Nurmi, 10.10.2019
We should
include all of
these ladies!
Miina Nurmi, 10.10.2019
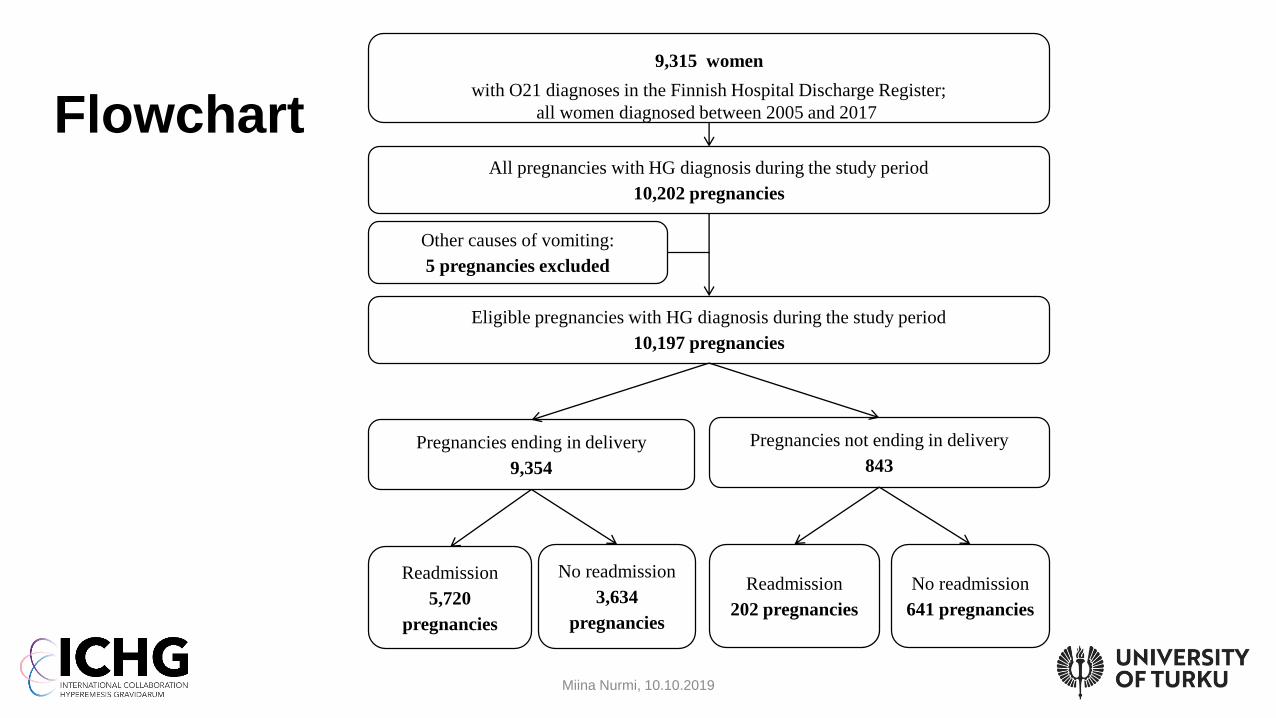
Flowchart
9,315 women
with O21 diagnoses in the Finnish Hospital Discharge Register;
all women diagnosed between 2005 and 2017
Other causes of vomiting:
5 pregnancies excluded
Readmission
5,720
pregnancies
Pregnancies ending in delivery
9,354
No readmission
3,634
pregnancies
Pregnancies not ending in delivery
843
Readmission
202 pregnancies
No readmission
641 pregnancies
Eligible pregnancies with HG diagnosis during the study period
10,197 pregnancies
All pregnancies with HG diagnosis during the study period
10,202 pregnancies
• Primary outcome measure: total number of outpatient visits and
hospitalizations
• Dates calculated from the health care system’s point of view: one woman’s
one outpatient visit + hospitalization on the same day are calculated as two
• Secondary outcome measures
• Readmissions due to HG in live births, stillbirths, gestational trophoblastic
disease, ectopic pregnancies, spontaneous abortions and pregnancy
terminations
• Pregnancy-specific
• Dates calculated from the women’s point of view: one woman’s one
outpatient visit + hospitalization on the same day are calculated as one
Outcome measures
Miina Nurmi, 10.10.2019
One outpatient
resource plus one
hospital resource
have been used.
”I’m ill today,
please just
help me,
anywhere!”
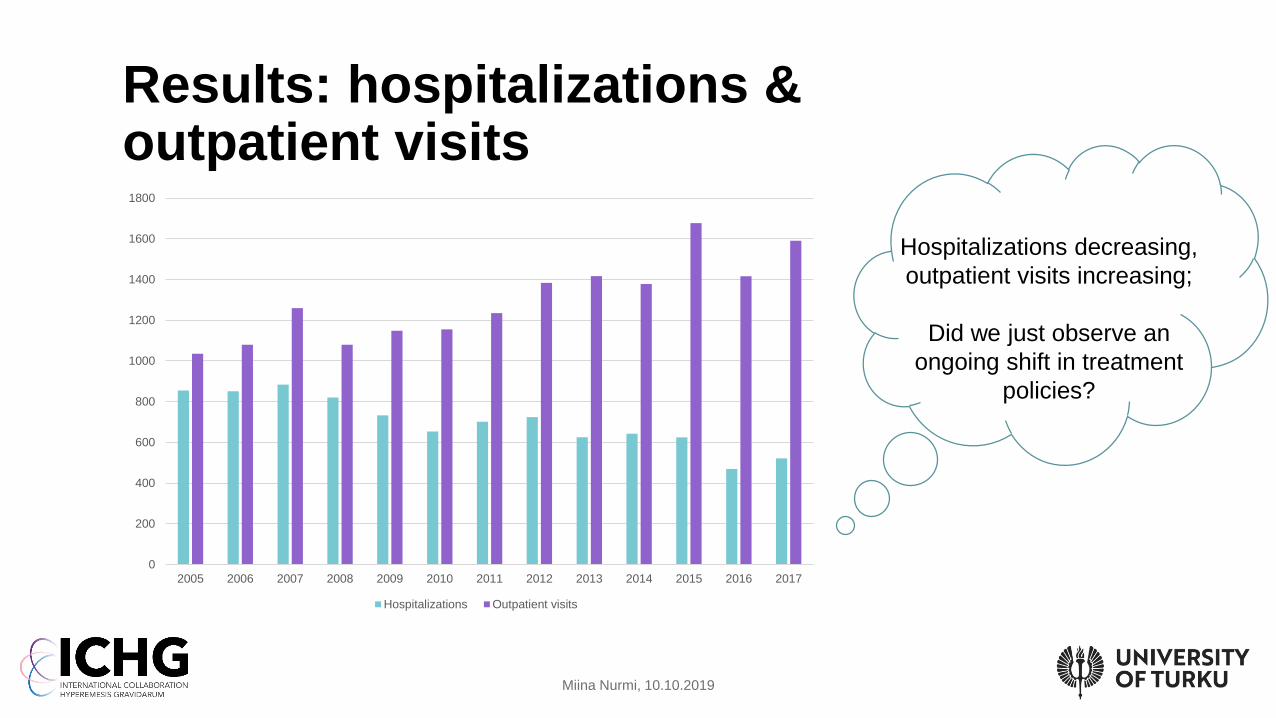
Results: hospitalizations & outpatient visits
Miina Nurmi, 10.10.2019
Hospitalizations decreasing,
outpatient visits increasing;
Did we just observe an
ongoing shift in treatment
policies?
0
200
400
600
800
1000
1200
1400
1600
1800
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
Hospitalizations Outpatient visits
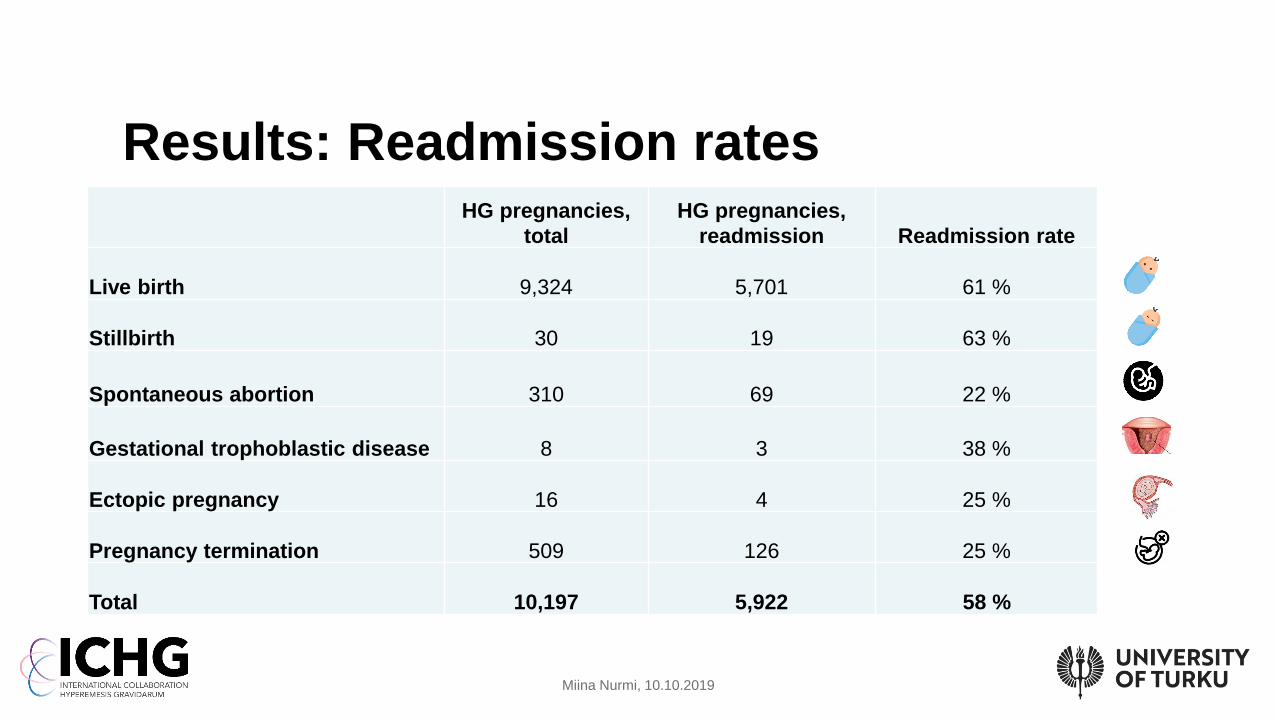
Results: Readmission rates
Miina Nurmi, 10.10.2019
HG pregnancies,
total
HG pregnancies,
readmission Readmission rate
Live birth 9,324 5,701 61 %
Stillbirth 30 19 63 %
Spontaneous abortion 310 69 22 %
Gestational trophoblastic disease 8 3 38 %
Ectopic pregnancy 16 4 25 %
Pregnancy termination 509 126 25 %
Total 10,197 5,922 58 %
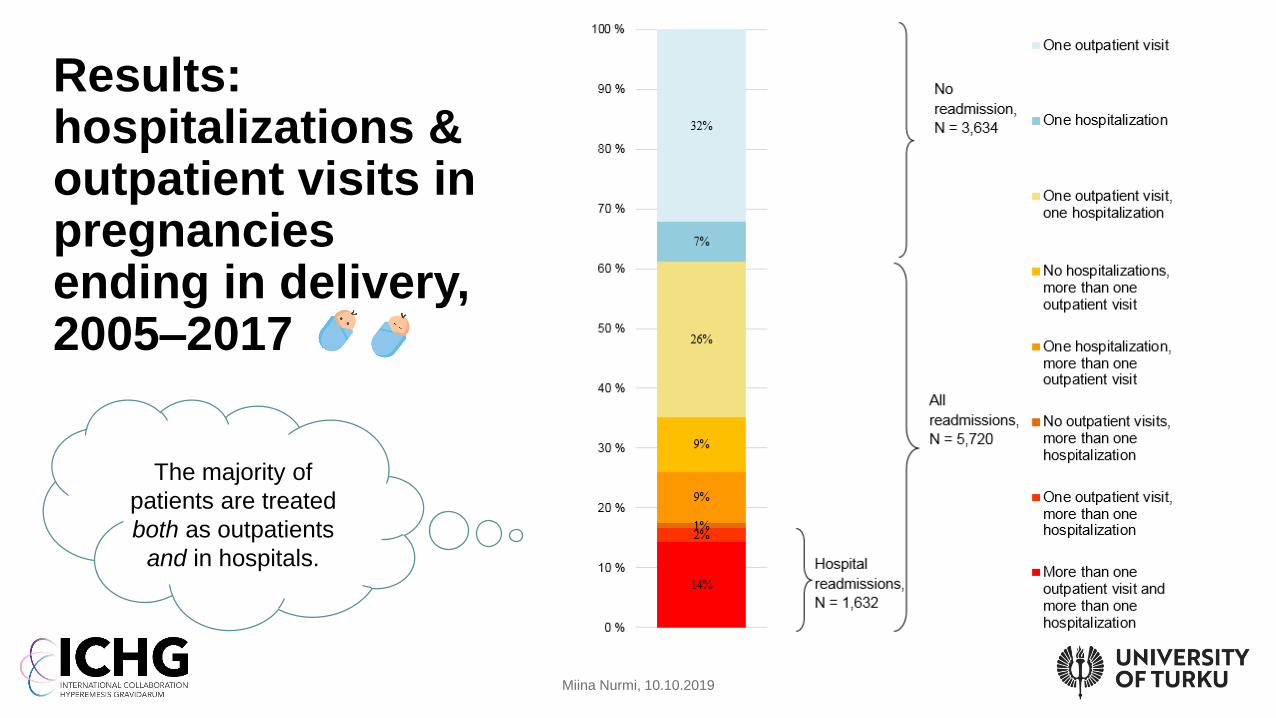
Results: hospitalizations & outpatient visits in pregnanciesending in delivery, 2005–2017
Miina Nurmi, 10.10.2019
The majority of
patients are treated
both as outpatients
and in hospitals.
• Always to be remembered with registers: you can only find cases which have
been entered in the register
• Interpretation!
• Example 1, one woman in our data
• HG pregnancy terminated in 2005, in pregnancy week 14
• HG pregnancy ending in delivery in 2008
• Pregnancy terminated in 2014, in pregnancy week 5 (with no HG diagnosis)
• Without a diagnosis it is not possible to know whether the third pregnancy was or wasn't an HG
pregnancy (or would have been at later weeks)
• Example 2, readmission rate in pregnancy terminations
• In the first analysis, pregnancy termination appeared to be associated with very high readmission
rate, but corrected analysis showed a lower rate
• Double checking & manual checking!
• Cases with HG diagnosis and pregnancy termination on the same date
• Time limits between diagnoses; date formats; pregnancy week at termination
Discussion/methodological issues
Miina Nurmi, 10.10.2019
At least
so many!
”Thus, these results
should be considered
as the lower limit of the
real number of cases.”
• Analyzing background factors to find out if or how
pregnancies involving repeated admissions due to
HG differ from pregnancies involving only one
admission due to HG
• Unfortunately this can only be done with pregnancies
ending in delivery, so the other pregnancy outcomes
still remain less well characterized
Next steps
Miina Nurmi, 10.10.2019
But at least
we’ve tried
our best!
Acknowledgements
Working on the register data:
Miina Nurmi, MSc, PhD student/University of Turku
Päivi Polo, MD, PhD, Professor (Obstetrics and Gynaecology)/University of Turku
Päivi Rautava, MD, PhD, Professor (Public Health)/University of Turku
Mika Gissler, PhD, Research Professor/THL National Institute of Health and Welfare
Tero Vahlberg, MSc, biostatistician/University of Turku
Working on our other datasets:
Linda Laitinen, MD, PhD student/University of Turku
Nina Kulovuori, MD, PhD student/University of Turku
Data extraction, anonymization and data provision:
Jouni Meriläinen, Senior Planning Officer/THL National Institute of Health and Welfare
Jouni Rasilainen, Senior Planning Officer/THL National Institute of Health and Welfare
Backup support:
Friends and families
Thank you for your attention
Miina Nurmi, 10.10.2019
























![[ PowerPoint Template ]](https://img.pdfslide.net/doc/110x75/631afe995d5809cabd0fa04b/-powerpoint-template-.jpg)