Embed Size (px)
Citation preview
The Laryngoscope Lippincott Williams & Willtins, Philadelphia 0 1998 The American Laryn ological Rhinological and Otological jociety, fnc.
Videostroboscopy of the Pharyngoesophageal Segment in Total Laryngectomees James Paul Dworkin, PhD; Robert J. Meleca, MD; Michelle M. Zormeier, MD; Mark L. Simpson, PhD; Ilene Garfield, MA; John R. Jacobs, MD; Robert H. Mathog, MD
Objectives: The reconstructed pharyngoesoph- ageal segment (PES) serves as the neoglottis following total laryngectomy, as it provides the source of vibra- tion for production of tracheoesophageal puncture (TEP) voice. To date, little information exists regard- ing the vibratory characteristics of the PES. The pur- pose of this investigation was to study the anatomy and physiology of the PES using videostroboscopy. Study Design: Prospective study investigating the anatomy and physiology of the PES in 34 laryngec- tomees who used TEP speech as their primary form of communication. Materials and Methods: Videostro- boscopy and voice recordings were graded by three trained, blinded judges using a seven-point scale. Re- sults: The patients demonstrated differences that al- lowed for separation of patients into two main groups: “poor“ and “effective” TEP speakers. The voice quality differences were explained by anatomic and physiologic characteristics of the PES. Redun- dant, thick, and dyssynchronous PES features were observed in patients with poor TEP speech skills; the effective speakers exhibited less redundant, thinner mucosa and more synchronous vibratory patterns. Moreover, the latter subgroup consistently demon- strated a greater degree of volitional PES control and less spasmodic activity than their poorly speaking counterparts. Length of the PES opening (measured in the horizontal plane) as well as amount and consis- tency of secretions did not appear to influence TEP speech or voice proficiency. Conclusion: Videostro- boscopy in laryngectomees is a noninvasive, inexpen- sive, easily performed procedure that may contribute valuable information regarding the anatomy and physiology of the PES, especially in patients who ex- perience difficulties achieving satisfactory TEP voice and speech production.
Laryngoscope, 1081773-1781,1998
Presented at the Meeting of the Middle Section of the American Laryngological, Rhinological and Otological Society, Inc., Minneapolis, Minnesota, January 23, 1998.
From the Department of Otolaryngology-Head and Neck Surgery, Wayne State University School of Medicine, Detroit, Michigan.
Send Reprint Requests to James P. Dworkin, PhD, 37000 Fox Glen, Farmington Hills, MI 48331, U.S.A.
INTRODUCTION The total laryngectomy procedure produces a defect
in the hypopharynx that must be reconstructed to form the pharyngoesophageal segment (PES1.1-5 This tubular- shaped region, composed largely of skeletal muscle tissue, serves as the neoglottis and enables production of esophageal voice. Early electromyographic studies of the PES demonstrated that proficient esophageal speakers generally exhibited greater volitional sphincteric muscle control than their counterparts with poor speech skills.6,’ Later analysis, however, suggested that there is no strong evidence that esophageal speakers can systematically reg- ulate PES muscle activity to pretune, control, or influence the vibratory behavior of this sphincter.8
The tracheoesophageal puncture (TEP) method of voice restoration following total laryngectomy was first described by Singer and Bl0m.9 This approach to rehabil- itation has received broad acceptance by numerous prac- titioners in the fields of otolaryngology and speech pathol- ogy. As the patient occludes the stoma with a finger or thumb during TEP speech efforts, the esophagus is dis- tended with air. This results in airflow-dependent reflex reactions of the PES, which induce a rise in sphincteric pressure.10 Transneoglottal airflow probably occurs as a consequence of both simultaneous volitional and passive relaxation responses of this striated muscular valve to such increase in sub(neo)glottal pressure. Vibrations of the closely approximated membranous surfaces of the PES occur as air columns are emitted with the aid of con- tinuous pulmonary effort to phonate. These processes op- erate in a manner similar to laryngeal phonation, with de- pendence on respiration subsystem forces and airflow to drive the vibratory source, and a closed tracheal airway to help sustain phonation.11 therefore tracheoesophageal voice production is considered to be mediated by both aerodynamic and myoelastic factors.1216
Despite the recent advances in videoendoscopic and stroboscopic technology, there is a paucity of objective data on the anatomy and physiology of the source of vi- bration underlying esophageal voice production. It is rea- sonable to assume that such information is vital to estab- lishing a more complete understanding of this important mechanism of alaryngeal communication. Fluoroscopy and roentgenography have been used to examine primar-
Laryngoscope 108: December 1998 Dworkin et al.: Videostroboscopy 1773
ily the anatomy of the pseudoglottis in laryngectomees. Results obtained from good esophageal speakers revealed constriction of a visible air column at the level of the fifth cervical vertebra immediately below the region of the cricopharyngeus muscle.16 When radiographs were em- ployed for comparative analyses of good versus poor esophageal speakers, the cricopharyngeus muscle was noted to determine the shape of the pseudoglottis.17
Several investigators used radiocinematography in the past to study the physiology of the PES.ls22 Summar- ily, these researchers discovered that during esophageal voice production the PES remains in a constant state of activity, and the tightness, length, and epicenter of vibra- tion of this sphincter vary with the modulations of speech and from patient to patient. Interestingly, there are no known published data on the vibratory characteristics or appearances of the PES in laryngectomees who use the TEP method of speech production. Therefore the present investigation was conducted to provide preliminary, heretofore unreported videostroboscopic information on this subject matter. Answers to the following questions were sought: 1) What are the general anatomic and phys- iologic features of the PES, both at rest and during vari- ous TEP voice activities? 2) Are there significant anatomic and physiologic variations from patient to patient? 3) Do these findings correlate with speech proficiency?
MATERIALS AND METHODS
Patients Twenty-seven male and 7 female total laryngectomees, rang-
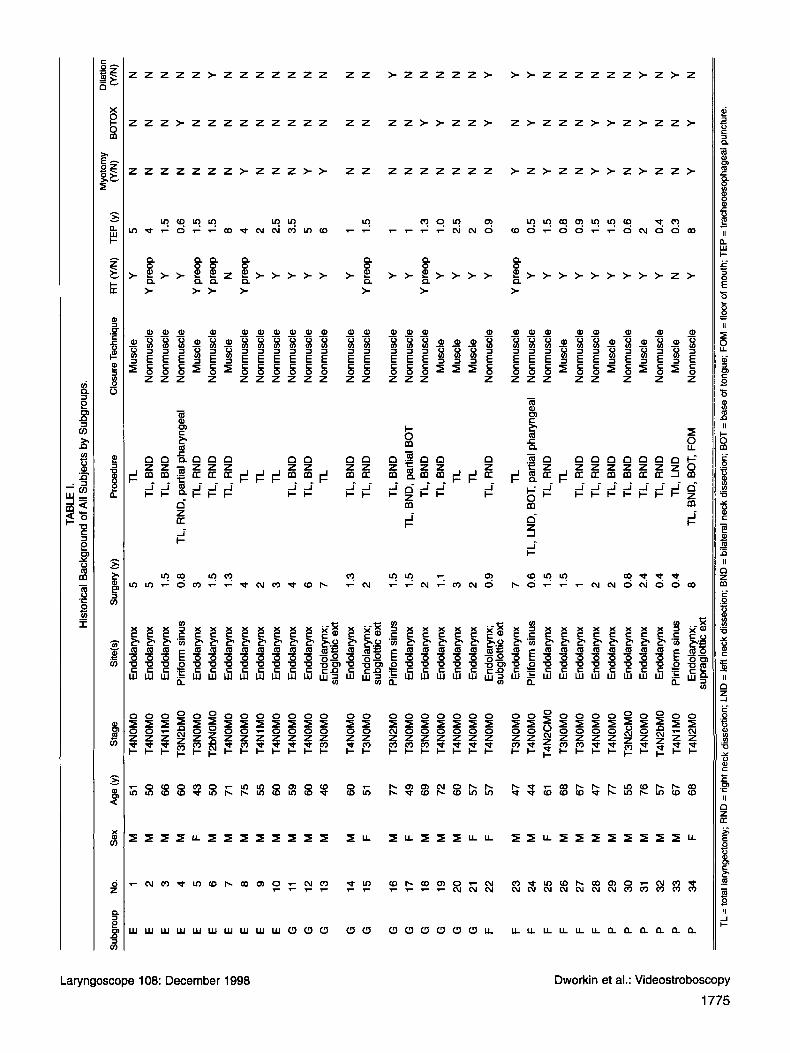
ing in age from 43 to 77 years, served as subjects for this investi- gation. To qualify for inclusion in the study, subjects were required to use exclusively the TEP method of speech production. Each of the 34 subjects used a low-pressure, Blom-Singer voice prosthesis. The disease was confined to the endolarynx in 28 subjects; 3 sub- jects presented endolaryngeal primary lesions with subglottic ex- tension. The piriform sinuses were involved in the remaining three individuals. Three of the subjects received their TEPs at the time of the laryngectomy procedure; 31 had puncture secondarily. Twenty-four patients underwent a non-muscle closure technique of the PES, and 10 patients had a muscle closure method. Table I offers a capsule historical summary of these subjects.
To segregate subjects into speech proficiency subgroups, three blinded judges on two separate occasions used a seven- point, equal-appearing interval rating scale to evaluate the speech proficiency of each subject. The overall mean ratings ob- tained from these skilled listeners permitted arbitrary subdivi- sion of the 34 subjects into the following TEP speaking groups for comparative analyses: 1) excellent (mean score between 1.0 and 1.5; n = lo), 2) good (mean score between 1.51 and 2.99; n = ll), 3) fair (mean score between 3.0 and 4.50; n = 7), and 4) poor (mean score exceeded 4.51; n = 6).
Analysis The anatomy and physiology of the PES were analyzed us-
ing the Kay Elemetrics’ (Lincoln Park, NJ) videolaryngostro- boscopy system (model 9100). A 70-degree rigid endoscope (Kay model 9105) was used to visualize the pseudoglottis. Each subject was requested to generate the following esophageal voice activi- ties: 1) vowel / i / prolongations at the most comfortable pitch and loudness levels; 2) pitch glides, using the same vowel; 3) loudness alterations, using the same vowel; and 4) rapid repetitions (di- adochokinesis) of the vowel.
Three judges were also used for this segment of the study, and they were blinded to the identity of the subjects. All ratings were performed independently and on two separate occasions. Table I1 illustrates the PES rating form used by the judges. They were instructed to rate each of the parameters listed using the seven-point bipolar scoring system.
RESULTS
Reliability Percentage agreement scores were computed to mea-
sure the degree to which judges agreed with each other and themselves on all ratings. The criterion for agreement was that no judge’s score could differ by more than one scale value from the mean rating for each parameter stud- ied. Judges were in full agreement with each other on 95% and 87% of the speech and stroboscopy ratings, respec- tively. They were in agreement with themselves more than 92% and 90% of the time for the speech proficiency and stroboscopy ratings, respectively. These data were in- terpreted as evidence of strong interjudge and intrajudge reliability.
Stroboscopy Characteristics Table I11 provides a composite breakdown of the
range, mean, and standard deviation stroboscopy data for all subgroups. For easy group comparisons, the mean data were extracted and displayed in Figure 1. The results of each measured parameter are discussed below to facili- tate interpretation of the overall group differences and similarities.
Morphology at Rest Length. Viewed endoscopically, this measurement is
taken in the horizontal plane and represents the maximal length of the PES opening achieved during phonatory tasks. Anatomically, the opening represents the most su- perior aspect of the PES. Note from Figure 1 that there was a narrow linear trend in the length of the PES across subgroups. The excellent TEP speakers were judged to possess the shortest (mean score = 3.79) visible vibratory segment, followed in increasing order by the good (mean score = 4.15), fair (mean score = 4 .38) and poor (mean score = 4.45) speaking subgroups. These differences were generally very small, and they would not support a hy- pothesis that length of the PES is a significant contribu- tor to TEP speech proficiency.
Thickness. Videostroboscopic visualization of the most superior aspect of the PES revealed what appeared to be a multilayered and/or mucosally redundant struc- ture in virtually all of the subjects studied. Ratings for the excellent, good, and fair subgroups were on average in the middle of the scale (mean score = 4.53, 4.25, and 4.57, re- spectively), evenly positioned between the very thin and very thick extremes. Subjects in the poor speaking sub- group were judged to exhibit mildly to moderately thicker, more redundant PES tissue characteristics than their counterparts in the other three subgroups. All judges com- mented that in comparison to the leaner mechanisms, subjects with thicker vibratory segments generally pro- duced more hoarse-harsh-strained vocal quality and
Laryngoscope 108: December 1998
1774 Dworkin et al.: Videostroboscopy
I;;
TAB
LE 1.
< 0 0 v
) 8 Su
bgro
up
No.
S
ex
Age
(y)
S
tage
S
ie(s
) S
urge
ry (Y
) P
roce
dure
C
losu
re T
echn
ique
R
T (Y
N)
TE
P (y
) (Y
/N)
BO
TOX
(Y
N)
His
toric
al B
ackg
roun
d of
All
Sub
ject
s by
Sub
grou
ps.
Myo
torn
y D
ilatio
n
-n
iij
E
1 M
51
T4
NOM
O
End
olar
ynx
5 T
L M
uscl
e Y
5 N
N
0
E
2 M
50
T4
NOM
O
End
olar
ynx
5 TL
, BN
D
Non
mus
cle
Ypr
eop
4 N
N
E
3
M
66
T4N
lMO
E
ndol
aryn
x 1.
5 TL
, B
ND
N
o n m
u sc I
e Y
1.
5 N
N
PP
0
8 E
4
M 60
T3
N2b
MO
P
irifo
rm s
inus
0.
8 TL
, R
ND
, par
tial p
hary
ngea
l N
onm
uscl
e Y
0.6
N
Y 3
E
5
F 43
T3
NOM
O
End
olar
ynx
3 TL
, R
ND
M
uscl
e Y
preo
p 1.
5 N
N
E
6
M 50
T2
bNO
MO
E
ndol
aryn
x 1.
5 TL
, R
ND
N
onm
uscl
e Y
pre
op
1.5
N
N
z A
E
7 M
71
T4
NOM
O
End
olar
ynx
1.3
TL,
RN
D
Mus
cle
N
8 N
N
E
8
M
75
T3NO
MO
E
ndol
aryn
x 4
TL
Non
mus
cle
Ypr
eop
4 Y
N
E
9
M
55
T4N
lMO
E
ndol
aryn
x 2
TL
Non
mus
cle
Y 2
N
N
E
10
M
60
T4NO
MO
E
ndol
aryn
x 3
TL
Non
mus
cle
Y 2.
5 N
N
G
11
M
59
T4
NOM
O
End
olar
ynx
4 TL
, B
ND
N
onm
uscl
e Y
3.5
N
N
G
12
M
60
T4NO
MO
E
ndol
aryn
x 6
TL,
BN
D
Non
mus
cle
Y 5
Y
N
G
13
M
46
T3NO
MO
E
ndol
aryn
x;
7 T
L N
onm
uscl
e Y
6 Y
N
G
14
M
60
T4NO
MO
E
ndol
aryn
x 1.
3 TL
, B
ND
N
onm
uscl
e Y
1 N
N
G
15
F
51
T3NO
MO
E
ndol
aryn
x;
2 TL
, R
ND
N
onm
uscl
e Y
pre
op
1.5
N
N
G
16
M
77
T3N
2MO
P
irifo
rmsi
nus
1.5
TL,
BN
D
Non
mus
cle
Y 1
N
N
G
17
F 49
T3
NOM
O
End
olar
ynx
1.5
TL,
BN
D, p
artia
l BO
T N
onm
uscl
e Y
1
N
N
G
18
M
69
T3NO
MO
E
ndol
aryn
x 2
TL,
BN
D
Non
mus
cle
Y p
reop
1.
3 N
Y
G
19
M
72
T4
NOM
O
End
olar
ynx
1.1
TL,
BN
D
Mus
cle
Y
1 .o
N
Y G
20
M
60
T4
NOM
O
End
olar
ynx
3 T
L M
uscl
e Y
2.
5 N
N
G
21
F
57
T4NO
MO
E
ndol
aryn
x 2
TL
Mus
cle
Y
2 N
N
F
22
F 57
T4
NOM
O
End
olar
ynx;
0.
9 TL
, R
ND
N
onm
uscl
e Y
0.
9 N
Y
F 23
M
47
T3
NOM
O
End
olar
ynx
7 TL
N
onm
uscl
e Y
preo
p 6
Y
N
F 24
M
44
T4
NOM
O
Piri
form
sin
us
0.6
TL,
LND
, BO
T, p
artia
l pha
ryng
eal
Non
mus
cle
Y 0.
5 N
Y
F 25
F
61
T4N
2CM
O
End
olar
ynx
1.5
TL,
RN
D
Non
mus
cle
Y
1.5
Y
N
F
26
M
68
T3NO
MO
E
ndol
aryn
x 1.
5 T
L M
uscl
e Y
0.8
N
N
F 27
M
67
T3
NOM
O
End
olar
ynx
1 TL
, R
ND
N
onm
uscl
e Y
0.
9 N
N
B 4 3
F 28
M
47
T4
NOM
O
End
olar
ynx
2 TL
, R
ND
N
onm
uscl
e Y
1.5
Y
Y 9
P
29
M
77
T4NO
MO
E
ndol
aryn
x 2
TL,
BN
D
Mus
cle
Y 1.
5 Y
Y
P
30
M
55
T3N
2cM
O
End
olar
ynx
0.8
TL.
BN
D
Non
mus
cle
Y 0.
6 N
N
E
l 5
P
31
M
76
T4NO
MO
E
ndol
aryn
x 2.
4 TL
, R
ND
M
uscl
e Y
2 Y
Y
P 32
M
57
T4
N2b
MO
E
ndol
aryn
x 0.
4 TL
, R
ND
N
onm
uscl
e Y
0.
4 N
N
P
33
M
67
T4N
1 MO
Piri
form
sin
us
0.4
TL, L
ND
M
uscl
e N
0.
3 N
N
% a U
P
34
F 68
T4
N2M
O
End
olar
ynx;
8
TL,
BND
, BO
T, F
OM
N
onm
uscl
e Y
8
Y
Y
48
A
m U
(D
(0
OD
subg
lotti
c ex
t
subg
lotti
c ex
t
subg
lotti
c ex
t
x .. CL m
28
su
prag
lotti
c ex
t
25
TL =
tota
l lar
ynge
ctor
ny; R
ND
= ri
ght n
eck
diss
ectio
n; L
ND
= le
ft ne
ck d
isse
ctio
n; B
ND
= b
ilate
ral n
eck
diss
ectio
n; B
OT
= b
ase
of to
ngue
; FO
M =
floor
of m
outh
; TE
P =
trac
heoe
soph
agea
l pun
ctur
e.
N
N
N
N
N
Y N
N
N
N
N
N
N
N
N
Y Y N
N
N
N
N
N
Y N
Y N
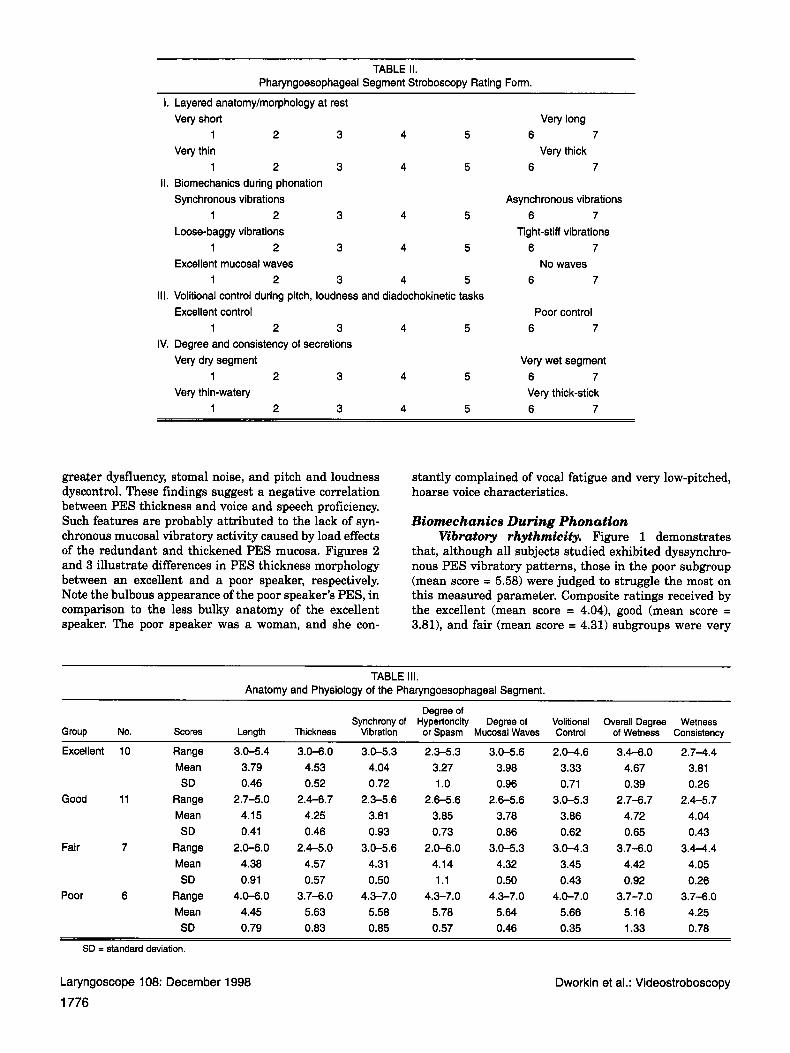
TABLE 11. Pharyngoesophageal Segment Stroboscopy Rating Form.
I. Layered anatomy/morphology at rest Very short Very long
Very thin Very thick 1 2 3 4 5 6 7
1 2 3 4 5 6 7 11. Biomechanics during phonation
Synchronous vibrations Asynchronous vibrations
Loose-baggy vibrations Tight-stiff vibrations
Excellent mucosal waves No waves
1 2 3 4 5 6 7
1 2 3 4 5 6 7
1 2 3 4 5 6 7 111. Volitional control during pitch, loudness and diadochokinetic tasks
Excellent control Poor control 1 2 3 4 5 6 7
IV. Degree and consistency of secretions Very dry segment
1 2 3 4 5 6 7 Very thin-watery Very thick-stick
1 2 3 4 5 6 7
Very wet segment
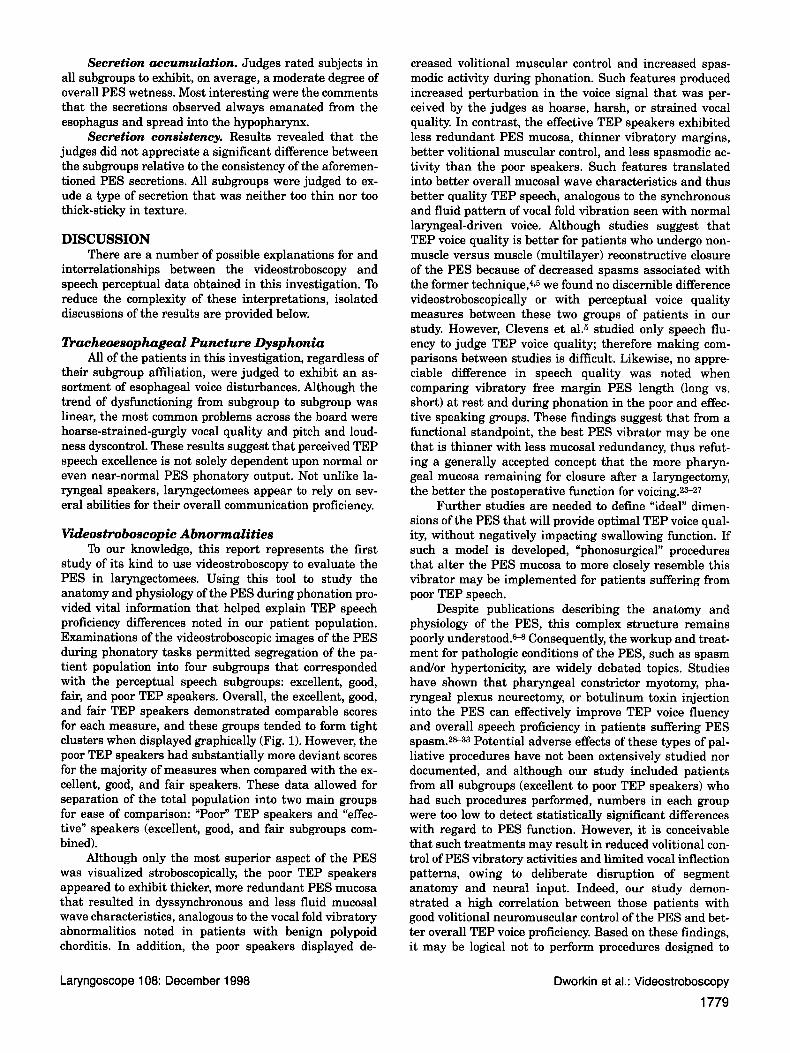
greater dysfluency, stoma1 noise, and pitch and loudness dyscontrol. These findings suggest a negative correlation between PES thickness and voice and speech proficiency. Such features are probably attributed to the lack of syn- chronous mucosal vibratory activity caused by load effects of the redundant and thickened PES mucosa. Figures 2 and 3 illustrate differences in PES thickness morphology between an excellent and a poor speaker, respectively. Note the bulbous appearance of the poor speaker’s PES, in comparison to the less bulky anatomy of the excellent speaker. The poor speaker was a woman, and she con-
stantly complained of vocal fatigue and very low-pitched, hoarse voice characteristics.
Biomechanics During Phonation Vibratory rhythmicity. Figure 1 demonstrates
that, although all subjects studied exhibited dyssynchro- nous PES vibratory patterns, those in the poor subgroup (mean score = 5.58) were judged to struggle the most on this measured parameter. Composite ratings received by the excellent (mean score = 4.041, good (mean score = 3.811, and fair (mean score = 4.31) subgroups were very
TABLE 111. Anatomy and Physiology of the Pharyngoesophageal Segment.
Degree of Synchrony of Hypertoncity Degree of Volitional Overall Degree Wetness
Group No. Scores Length Thickness Vibration or Spasm Mucosal Waves Control of Wetness Consistency
Excellent 10 Range 3.0-5.4 3.0-6.0 3.0-5.3 2.3-5.3 3.0-5.6 2.0-4.6 3.4-6.0 2.7-4.4 Mean 3.79 4.53 4.04 3.27 3.98 3.33 4.67 3.81 SD 0.46 0.52 0.72 1 .o 0.96 0.71 0.39 0.26
Good 11 Range 2.7-5.0 2.4-6.7 2.3-5.6 2.6-5.6 2.6-5.6 3.0-5.3 2.7-6.7 2.4-5.7 Mean 4.15 4.25 3.81 3.85 3.78 3.86 4.72 4.04 SD 0.41 0.46 0.93 0.73 0.86 0.62 0.65 0.43
Fair 7 Range 2.0-6.0 2.4-5.0 3.0-5.6 2.0-6.0 3.0-5.3 3.0-4.3 3.7-6.0 3.4-4.4 Mean 4.38 4.57 4.31 4.14 4.32 3.45 4.42 4.05 SD 0.91 0.57 0.50 1.1 0.50 0.43 0.92 0.26
Mean 4.45 5.63 5.58 5.78 5.64 5.66 5.16 4.25 SD 0.79 0.83 0.85 0.57 0.46 0.35 1.33 0.78
Poor 6 Range 4.0-6.0 3.7-6.0 4.3-7.0 4.3-7.0 4.3-7.0 4.0-7.0 3.7-7.0 3.7-6.0
SD = standard deviation.
Laryngoscope 108: December 1998
1776 Dworkin et al.: Videostroboscopy
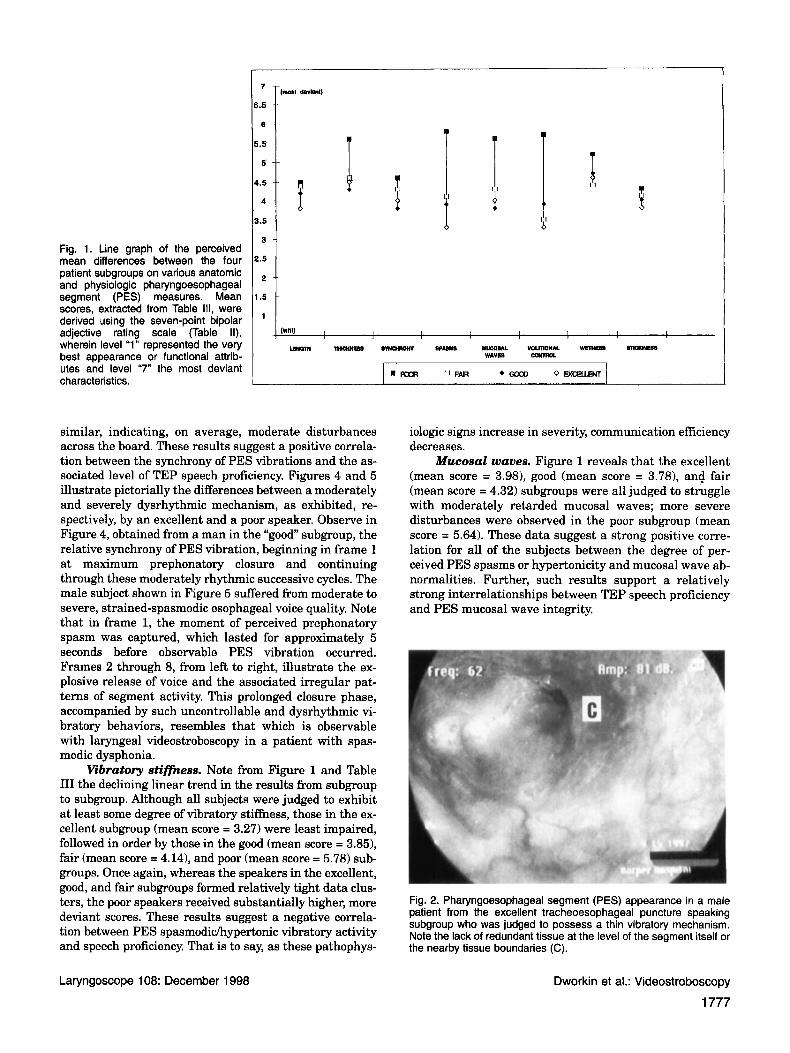
Fig. 1. Line graph of the perceived mean differences between the four patient subgroups on various anatomic and physiologic pharyngoesophageal segment (PES) measures. Mean scores, extracted from Table 111, were derived using the seven-point bipolar adjective rating scale (Table II), wherein level “1” represented the very best appearance or functional attrib- utes and level “7” the most deviant characteristics.
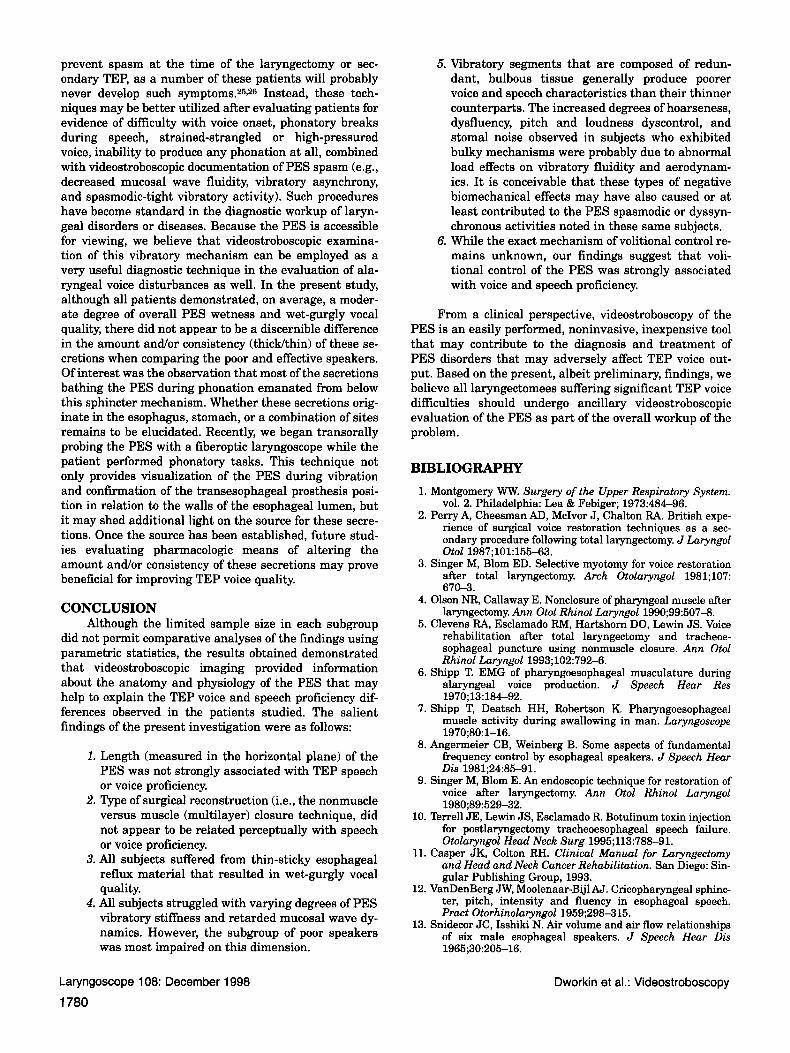
similar, indicating, on average, moderate disturbances across the board. These results suggest a positive correla- tion between the synchrony of PES vibrations and the as- sociated level of TEP speech proficiency. Figures 4 and 5 illustrate pictorially the differences between a moderately and severely dysrhythmic mechanism, as exhibited, re- spectively, by an excellent and a poor speaker. Observe in Figure 4, obtained from a man in the “good” subgroup, the relative synchrony of PES vibration, beginning in frame 1 at maximum prephonatory closure and continuing through these moderately rhythmic successive cycles. The male subject shown in Figure 5 suffered from moderate to severe, strained-spasmodic esophageal voice quality. Note that in frame 1, the moment of perceived prephonatory spasm was captured, which lasted for approximately 5 seconds before observable PES vibration occurred. Frames 2 through 8, from left to right, illustrate the ex- plosive release of voice and the associated irregular pat- terns of segment activity. This prolonged closure phase, accompanied by such uncontrollable and dysrhythmic vi- bratory behaviors, resembles that which is observable with laryngeal videostroboscopy in a patient with spas- modic dysphonia.
Vibratory stifficess. Note from Figure 1 and Table I11 the declining linear trend in the results from subgroup to subgroup. Although all subjects were judged to exhibit a t least some degree of vibratory stiffness, those in the ex- cellent subgroup (mean score = 3.27) were least impaired, followed in order by those in the good (mean score = 3.85), fair (mean score = 4.14), and poor (mean score = 5.78) sub- groups. Once again, whereas the speakers in the excellent, good, and fair subgroups formed relatively tight data clus- ters, the poor speakers received substantially higher, more deviant scores. These results suggest a negative correla- tion between PES spasmodichypertonic vibratory activity and speech proficiency. That is to say, as these pathophys-
H s 6
iologic signs increase in severity, communication efficiency decreases.
Mucosal waves. Figure 1 reveals that the excellent (mean score = 3.98), good (mean score = 3.781, and fair (mean score = 4.32) subgroups were all judged to struggle with moderately retarded mucosal waves; more severe disturbances were observed in the poor subgroup (mean score = 5.64). These data suggest a strong positive corre- lation for all of the subjects between the degree of per- ceived PES spasms or hypertonicity and mucosal wave ab- normalities. Further, such results support a relatively strong interrelationships between TEP speech proficiency and PES mucosal wave integrity.
Fig. 2. Pharyngoesophageal segment (PES) appearance in a male patient from the excellent tracheoesophageal puncture speaking subgroup who was judged to possess a thin vibratory mechanism. Note the lack of redundant tissue at the level of the segment itself or the nearby tissue boundaries (C).
Laryngoscope 108: December 1 998 Dworkin et al.: Videostroboscopy
1777
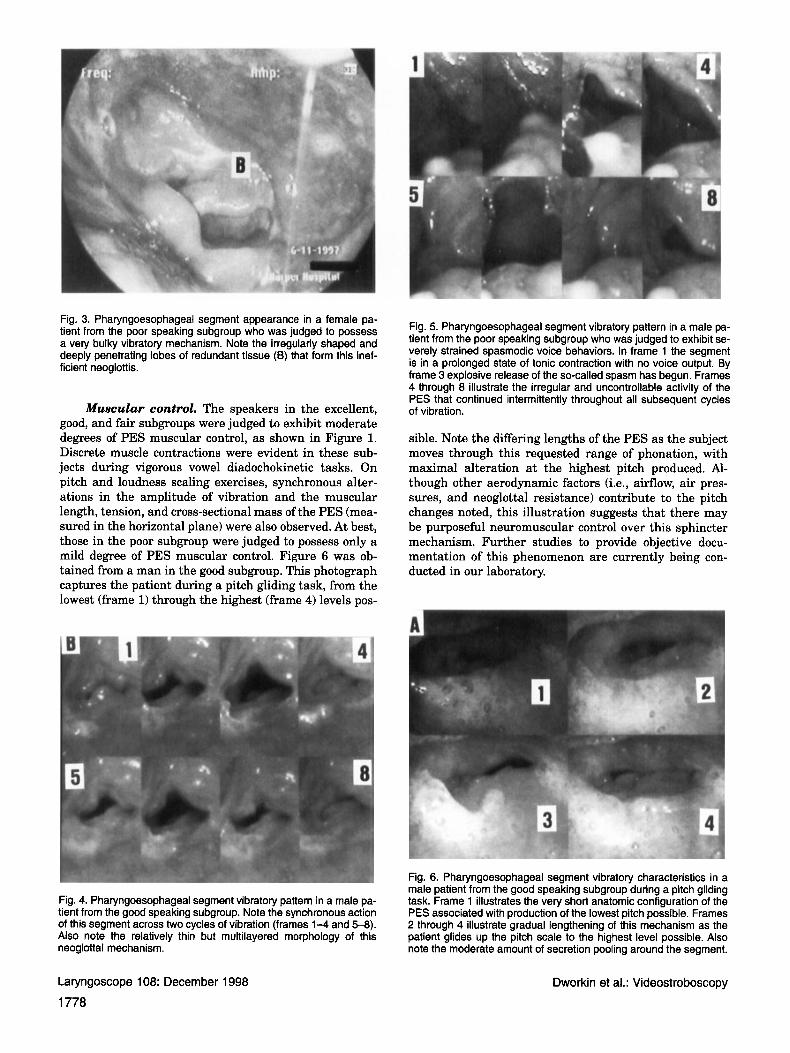
Fig. 3. Pharyngoesophageal segment appearance in a female pa- tient from the poor speaking subgroup who was judged to possess a very bulky vibratory mechanism. Note the irregularly shaped and deeply penetrating lobes of redundant tissue (6) that form this inef- ficient neoglottis.
Muscular control. The speakers in the excellent, good, and fair subgroups were judged to exhibit moderate degrees o f PES muscular control, as shown in Figure 1. Discrete muscle contractions were evident in these sub- jects during vigorous vowel diadochokinetic tasks. O n pi tch and loudness scaling exercises, synchronous alter- ations in the amplitude o f vibrat ion and the muscular length, tension, and cross-sectional mass of the PES (mea- sured in the horizontal plane) were also observed. At best, those in the poor subgroup were judged to possess only a mild degree o f PES muscular control. Figure 6 was ob- tained f rom a man in the good subgroup. This photograph captures the patient during a p i tch gliding task, f rom the lowest (frame 1) through the highest (frame 4) levels pos-
Fig. 5. Pharyngoesophageal segment vibratory pattern in a male pa- tient from the poor speaking subgroup who was judged to exhibit se- verely strained spasmodic voice behaviors. In frame 1 the segment is in a prolonged state of tonic contraction with no voice output. By frame 3 explosive release of the so-called spasm has begun. Frames 4 through 8 illustrate the irregular and uncontrollable activity of the PES that continued intermittently throughout all subsequent cycles of vibration.
sible. Note the dif fering lengths o f the PES as the subject moves through this requested range o f phonation, w i t h maximal alterat ion at the highest p i tch produced. Al- though other aerodynamic factors (i.e., airflow, air pres- sures, and neoglottal resistance) contribute to the pitch changes noted, th is i l lustrat ion suggests that there may be purposeful neuromuscular control over th is sphincter mechanism. Fur ther studies to provide objective docu- mentation of th is phenomenon are currently being con- ducted in our laboratory.
Fig. 6. Pharyngoesophageal segment vibratory characteristics in a male patient from the good speaking subgroup during a pitch gliding task. Frame 1 illustrates the very short anatomic configuration of the PES associated with production of the lowest pitch possible. Frames 2 through 4 illustrate gradual lengthening of this mechanism as the patient glides up the pitch scale to the highest level possible. Also note the moderate amount of secretion pooling around the segment.
Fig. 4. Pharyngoesophageal segment vibratory pattern in a male pa- tient from the good speaking subgroup. Note the synchronous action of this segment across two cycles of vibration (frames 1-4 and 5-8). Also note the relatively thin but multilayered morphology of this neoglottal mechanism.
Laryngoscope 108: December 1998
1778 Dworkin et al.: Videostroboscopy
Secretion accumulation. Judges rated subjects in all subgroups to exhibit, on average, a moderate degree of overall PES wetness. Most interesting were the comments that the secretions observed always emanated from the esophagus and spread into the hypopharynx.
Secretion consistency. Results revealed that the judges did not appreciate a significant difference between the subgroups relative to the consistency of the aforemen- tioned PES secretions. All subgroups were judged to ex- ude a type of secretion that was neither too thin nor too thick-sticky in texture.
DISCUSSION There are a number of possible explanations for and
interrelationships between the videostroboscopy and speech perceptual data obtained in this investigation. To reduce the complexity of these interpretations, isolated discussions of the results are provided below.
Dacheoesophageal Puncture Dysphonia All of the patients in this investigation, regardless of
their subgroup affiliation, were judged to exhibit an as- sortment of esophageal voice disturbances. Although the trend of dysfunctioning from subgroup to subgroup was linear, the most common problems across the board were hoarse-strained-gurgly vocal quality and pitch and loud- ness dyscontrol. These results suggest that perceived TEP speech excellence is not solely dependent upon normal or even near-normal PES phonatory output. Not unlike la- ryngeal speakers, laryngectomees appear to rely on sev- eral abilities for their overall communication proficiency.
Videostroboscopic Abnormalities To our knowledge, this report represents the first
study of its kind to use videostroboscopy to evaluate the PES in laryngectomees. Using this tool to study the anatomy and physiology of the PES during phonation pro- vided vital information that helped explain TEP speech proficiency differences noted in our patient population. Examinations of the videostroboscopic images of the PES during phonatory tasks permitted segregation of the pa- tient population into four subgroups that corresponded with the perceptual speech subgroups: excellent, good, fair, and poor TEP speakers. Overall, the excellent, good, and fair TEP speakers demonstrated comparable scores for each measure, and these groups tended to form tight clusters when displayed graphically (Fig. 1). However, the poor TEP speakers had substantially more deviant scores for the majority of measures when compared with the ex- cellent, good, and fair speakers. These data allowed for separation of the total population into two main groups for ease of comparison: “Poor” TEP speakers and “effec- tive” speakers (excellent, good, and fair subgroups com- bined).
Although only the most superior aspect of the PES was visualized stroboscopically, the poor TEP speakers appeared to exhibit thicker, more redundant PES mucosa that resulted in dyssynchronous and less fluid mucosal wave characteristics, analogous to the vocal fold vibratory abnormalities noted in patients with benign polypoid chorditis. In addition, the poor speakers displayed de-
creased volitional muscular control and increased spas- modic activity during phonation. Such features produced increased perturbation in the voice signal that was per- ceived by the judges as hoarse, harsh, or strained vocal quality. In contrast, the effective TEP speakers exhibited less redundant PES mucosa, thinner vibratory margins, better volitional muscular control, and less spasmodic ac- tivity than the poor speakers. Such features translated into better overall mucosal wave characteristics and thus better quality TEP speech, analogous to the synchronous and fluid pattern of vocal fold vibration seen with normal laryngeal-driven voice. Although studies suggest that TEP voice quality is better for patients who undergo non- muscle versus muscle (multilayer) reconstructive closure of the PES because of decreased spasms associated with the former technique,4,5 we found no discernible difference videostroboscopically or with perceptual voice quality measures between these two groups of patients in our study. However, Clevens et al.5 studied only speech flu- ency to judge TEP voice quality; therefore making com- parisons between studies is difficult. Likewise, no appre- ciable difference in speech quality was noted when comparing vibratory free margin PES length (long vs. short) a t rest and during phonation in the poor and effec- tive speaking groups. These findings suggest that from a functional standpoint, the best PES vibrator may be one that is thinner with less mucosal redundancy, thus refut- ing a generally accepted concept that the more pharyn- geal mucosa remaining for closure after a laryngectomy, the better the postoperative function for voicing.2S27
Further studies are needed to define “ideal” dimen- sions of the PES that will provide optimal TEP voice qual- ity, without negatively impacting swallowing function. If such a model is developed, “phonosurgical” procedures that alter the PES mucosa to more closely resemble this vibrator may be implemented for patients suffering from poor TEP speech.
Despite publications describing the anatomy and physiology of the PES, this complex structure remains poorly understood.- Consequently, the workup and treat- ment for pathologic conditions of the PES, such as spasm andor hypertonicity, are widely debated topics. Studies have shown that pharyngeal constrictor myotomy, pha- ryngeal plexus neurectomy, or botulinum toxin injection into the PES can effectively improve TEP voice fluency and overall speech proficiency in patients suffering PES spasm.2g-33 Potential adverse effects of these types of pal- liative procedures have not been extensively studied nor documented, and although our study included patients from all subgroups (excellent to poor TEP speakers) who had such procedures performed, numbers in each group were too low to detect statistically significant differences with regard to PES function. However, it is conceivable that such treatments may result in reduced volitional con- trol of PES vibratory activities and limited vocal inflection patterns, owing to deliberate disruption of segment anatomy and neural input. Indeed, our study demon- strated a high correlation between those patients with good volitional neuromuscular control of the PES and bet- ter overall TEP voice proficiency. Based on these findings, it may be logical not to perform procedures designed to
Laryngoscope 108: December 1998 Dworkin et al.: Videostroboscopy
1779
prevent spasm at the time of the laryngectomy or sec- ondary TEP, as a number of these patients will probably never develop such symptoms.26926 Instead, these tech- niques may be better utilized after evaluating patients for evidence of difficulty with voice onset, phonatory breaks during speech, strained-strangled or high-pressured voice, inability to produce any phonation at all, combined with videostroboscopic documentation of PES spasm (e.g., decreased mucosal wave fluidity, vibratory asynchrony, and spasmodic-tight vibratory activity). Such procedures have become standard in the diagnostic workup of laryn- geal disorders or diseases. Because the PES is accessible for viewing, we believe that videostroboscopic examina- tion of this vibratory mechanism can be employed as a very useful diagnostic technique in the evaluation of ala- ryngeal voice disturbances as well. In the present study, although all patients demonstrated, on average, a moder- ate degree of overall PES wetness and wet-gurgly vocal quality, there did not appear to be a discernible difference in the amount andor consistency (thicWthin) of these se- cretions when comparing the poor and effective speakers. Of interest was the observation that most of the secretions bathing the PES during phonation emanated from below this sphincter mechanism. Whether these secretions orig- inate in the esophagus, stomach, or a combination of sites remains to be elucidated. Recently, we began transorally probing the PES with a fiberoptic laryngoscope while the patient performed phonatory tasks. This technique not only provides visualization of the PES during vibration and confirmation of the transesophageal prosthesis posi- tion in relation to the walls of the esophageal lumen, but it may shed additional light on the source for these secre- tions. Once the source has been established, future stud- ies evaluating pharmacologic means of altering the amount and/or consistency of these secretions may prove beneficial for improving TEP voice quality.
CONCLUSION Although the limited sample size in each subgroup
did not permit comparative analyses of the findings using parametric statistics, the results obtained demonstrated that videostroboscopic imaging provided information about the anatomy and physiology of the PES that may help to explain the TEP voice and speech proficiency dif- ferences observed in the patients studied. The salient findings of the present investigation were as follows:
1. Length (measured in the horizontal plane) of the PES was not strongly associated with TEP speech or voice proficiency.
2. Type of surgical reconstruction (i.e., the nonmuscle versus muscle (multilayer) closure technique, did not appear to be related perceptually with speech or voice proficiency.
3. All subjects suffered from thin-sticky esophageal reflux material that resulted in wet-gurgly vocal quality.
4. All subjects struggled with varying degrees of PES vibratory stiffness and retarded mucosal wave dy- namics. However, the subgroup of poor speakers was most impaired on this dimension.
5. Vibratory segments that are composed of redun- dant, bulbous tissue generally produce poorer voice and speech characteristics than their thinner counterparts. The increased degrees of hoarseness, dysfluency, pitch and loudness dyscontrol, and stoma1 noise observed in subjects who exhibited bulky mechanisms were probably due to abnormal load effects on vibratory fluidity and aerodynam- ics. It is conceivable that these types of negative biomechanical effects may have also caused or at least contributed to the PES spasmodic or dyssyn- chronous activities noted in these same subjects.
6. While the exact mechanism of volitional control re- mains unknown, our findings suggest that voli- tional control of the PES was strongly associated with voice and speech proficiency.
From a clinical perspective, videostroboscopy of the PES is an easily performed, noninvasive, inexpensive tool that may contribute to the diagnosis and treatment of PES disorders that may adversely affect TEP voice out- put. Based on the present, albeit preliminary, findings, we believe all laryngectomees suffering significant TEP voice difficulties should undergo ancillary videostroboscopic evaluation of the PES as part of the overall workup of the problem.
BIBLIOGRAPHY 1. Montgomery WW. Surgery of the Upper Respiratory System.
vol. 2. Philadelphia: Lea & Febiger; 1973:484-96. 2. Perry A, Cheesman AD, McIvor J, Chalton RA. British expe-
rience of surgical voice restoration techniques as a sec- ondary procedure following total laryngectomy. J Laryngol Otol 1987;101:155-63.
3. Singer M, Blom ED. Selective myotomy for voice restoration after total laryngectomy. Arch Otolaryngol 1981;107: 670-3.
4. Olson NR, Callaway E. Nonclosure of pharyngeal muscle after laryngectomy. Ann Otol Rhinol Laryngol 1990;99:507-8.
5. Clevens RA, Esclamado RM, Hartshorn DO, Lewin JS. Voice rehabilitation after total laryngectomy and tracheoe- sophageal puncture using nonmuscle closure. Ann Otol Rhinol Laryngol 1993;102:792-6.
6. Shipp T. EMG of pharyngoesophageal musculature during alaryngeal voice production. ~ J Speech Hear Res 1970;13:184-92.
7. Shipp T, Deatsch HH, Robertson K. Pharyngoesophageal muscle activity during swallowing in man. Laryngoscope
8. Angermeier CB, Weinberg B. Some aspects of fundamental frequency control by esophageal speakers. J Speech Hear Dis 1981;24:85-91.
9. Singer M, Blom E. An endoscopic technique for restoration of voice aRer laryngectomy. Ann Otol Rhinol Laryngol
10. Terrell JE, Lewin JS, Esclamado R. Botulinum toxin injection for postlaryngectomy tracheoesophageal speech failure. Otolaryngol Head Neck Surg 1995;113:788-91.
11. Casper JK, Colton RH. Clinical Manual for Laryngectomy and Head and Neck Cancer Rehabilitation. San Diego: Sin- gular Publishing Group, 1993.
12. VanDenBerg JW, Moolenaar-Bijl AJ. Cricopharyngeal sphinc- ter, pitch, intensity and fluency in esophageal speech. Pract Otorhinolaryngol 1959;298-3 15.
13. Snidecor JC, Isshiki N. Air volume and air flow relationships of six male esophageal speakers. J Speech Hear Dis
1970;80:1-16.
1980;89:529-32.
1965;30:205-16.
Laryngoscope 108: December 1998
1780 Dworkin et at.: Videostroboscopy
14. Snidecor JC, Isshiki N. Vocal and air use characteristics of a superior male esophageal speaker. Folia Phoniatr Logop 1965;17:217-32.
15. Moon JB, Weinberg B. Aerodynamic and myoelastic contri- butions to tracheoesophageal voice production. J Speech Hear Res 1987;30:387-95.
16. Robe EY, Moore P, h d r e w s AH, Holinger PH. A study of the role of certain factors in the development of speech aRer laryngec- tomy, I type of operation. Laryngoscope 195Q66173-86.
17. Damste PH. Oesophageal. Hoitsema: Groningen, 1958. 18. Damste PH, VanDenBerg J , Moolenaar-Bijl AJ. Intake of air
in oesophageal speech. Acta Physiol Pharmacol Need
19. Dicarlo LM, Amster W, Herrer G. Speech After Laryngectomy. Syracuse, Ny: Syracuse University Press, 1955.
20. Diedrich WM, Youngstrom K. A cineradiographic study of pseudoglottis in laryngectomized patients. Rockville Pike, MD: American Speech and Hearing Association Conven- tion Report; 1960.
21. Schlosshauer B, Mockel G. Roentgenkinematografische Darstellung der pseudoprache nach laryngektomie. Arch Ohr Nus UK Ehik Heilk USW 1954;165:581-638.
22. Hodson CJ, Oswald MV. Speech Recovery After lbtal Laryn- gectomy. London: Livingstone, 1958.
23. Guttman MR. "racheopharyngeal fistulization: a new proce- dure in the laryngectomized patient. k n s Am Laryngol Rhino1 Otol Soc 1935;41:219-26.
24. Mason M. The rehabilitation of patients following surgical removal of the larynx. J Laryngol 1950;64:759-70.
1956;5:238-9.
25. Horowitz JB, Sasaki CT. Effect of cricopharyngeus myotomy on postlaryngectomy pharyngeal contraction pressures. Laryngoscope 1993;103:138-9.
26. Simpson IC, Smith JC, Gorden MT. Laryngectomy: the influ- ence of muscle reconstruction on the mechanism of esophageal voice production. J Laryngol Otol 1972;86:
27. Winans CS, Reinbach EJ, Waldrop WF'. Esophageal determi- nants of alaryngeal speech. Arch Otol 1974;99:10-4.
28. Baugh RF, Lewin JS, Baker SR. Preoperative assessment of tracheoesophageal speech. Laryngoscope 1987;97:461-6.
29. Zormeier MM, Meleca RJ, Dworkin JP, Simpson ML. Botu- linum toxin injection to improve tracheoesophageal speech after total laryngectomy. Paper presented at the meeting of the Academy of Otolaryngology, Head and Neck Surgery, San Francisco, CA, 1997.
30. Mahieu HF, Annyas AA, Schutte HK, VanDerJagt EJ. Pharyngoesophageal myotomy for vocal rehabilitation of laryngectomees. Laryngoscope 1987;97:451-7.
31. Scott PM, Bleach NR, Perry AR, Cheesman AD. Complica- tions of pharyngeal myotomy for alaryngeal voice rehabil- itation of laryngectomees. J Laryngol Otol 1993;107: 430-3.
32. Terrell JE, Lewin JS, Esclamado R. Botulinum toxin injec- tion for postlaryngectomy tracheoesophageal speech fail- ure. Otolaryngol Head Neck Surg 1995;113:788-91.
33. Crary MA, Glowasky AL. Using botulinum toxin A to improve speech and swallowing function following total laryngec- tomy. Arch Otolaryngol Head Neck Surg 1996;122:760-3.
961-90.
VISIT The Laryngoscope Interactive Caee Studies
on the World Wide Web http:l I www.laryngoscope.com
Review current case studies, written by an expert on the topic, and discover useful techniques and procedures. Our interactive site allows you to share your own experiences and interact with colleagues to examine the advantages and disadvantages of various approaches. A new and exciting case study will be posted every month. Past case studies will always be available to view at the site. Current Case Study: November 16-December 15: Management of substernal goiter.
Laryngoscope 108: December 1998 Dworkin et al.: Videostroboscopy
1781





























