Embed Size (px)
Citation preview
ww.sciencedirect.com
p u b l i c h e a l t h 1 2 6 ( 2 0 1 2 ) 4 5 9e4 7 0
Available online at w
Public Health
journal homepage: www.elsevier .com/puhe
Original Research
Why the Scots die younger: Synthesizing the evidence
G. McCartney a,*, C. Collins b, D. Walsh c, G.D. Batty d,e
a Public Health Observatory, NHS Health Scotland, 4th Floor, Elphinstone House, 65 West Regent Street, Glasgow G2 2AF, UKb School of Social Sciences, University of the West of Scotland, Paisley, UKcGlasgow Centre for Population Health, Glasgow, UKdUCL Epidemiology and Public Health, London, UKeMedical Research Council Social and Public Health Sciences Unit, Glasgow, UK
a r t i c l e i n f o
Article history:
Received 24 January 2011
Received in revised form
5 December 2011
Accepted 15 March 2012
Available online 10 May 2012
Keywords:
Scotland
Glasgow
Mortality
Scottish effect
Glasgow effect
Causality
Synthesis
* Corresponding author. Tel.: þ44 0141 354 2E-mail address: [email protected] (G.
0033-3506/$ e see front matter ª 2012 The Rdoi:10.1016/j.puhe.2012.03.007
s u m m a r y
Objective: To identify explanations for the higher mortality in Scotland relative to other
European countries, and to synthesize those best supported by evidence into an overall
explanatory framework.
Study design: Review and dialectical synthesis.
Methods: Candidate hypotheses were identified based on a literature review and a series of
research dissemination events. Each hypothesis was described and critically evaluated in
relation to the Bradford-Hill criteria for causation in observational epidemiology. A synthesis
of themore convincing hypotheseswas then attempted using a broadly ‘dialectical’ approach.
Results: Seventeen hypotheses were identified including: artefactual explanations (depriva-
tion, migration); ‘downstream explanations’ (genetics, health behaviours, individual values);
‘midstream’ explanations (substancemisuse; culture of boundlessness and alienation; family,
gender relations and parenting differences; lower social capital; sectarianism; culture of
limited social mobility; health service supply or demand; deprivation concentration); and
‘upstream’ explanations (climate, inequalities, de-industrialization, political attack). There is
little evidence available to determine why mortality rates diverged between Scotland and
other European countries between 1950 and 1980, but the most plausible explanations at
present link to particular industrial, employment, housing and cultural patterns. From 1980
onwards, the higher mortality has been driven by unfavourable health behaviours, and it
seems quite likely that these are linked to an intensifying climate of conflict, injustice and
disempowerment. This is best explained by developing a synthesis beginning from the polit-
ical attack hypothesis, which suggests that the neoliberal policies implemented from 1979
onwards across the UK disproportionately affected the Scottish population.
Conclusions: The reasons for the high Scottish mortality between 1950 and 1980 are unclear,
but may be linked to particular industrial, employment, housing and cultural patterns.
From 1980 onwards, the higher mortality is most likely to be accounted for by a synthesis
which begins from the changed political context of the 1980s, and the consequent hope-
lessness and community disruption experienced. This may have relevance to faltering
health improvement in other countries, such as the USA.
ª 2012 The Royal Society for Public Health. Published by Elsevier Ltd. All rights reserved.
928.McCartney).oyal Society for Public Health. Published by Elsevier Ltd. All rights reserved.
p u b l i c h e a l t h 1 2 6 ( 2 0 1 2 ) 4 5 9e4 7 0460
Introduction
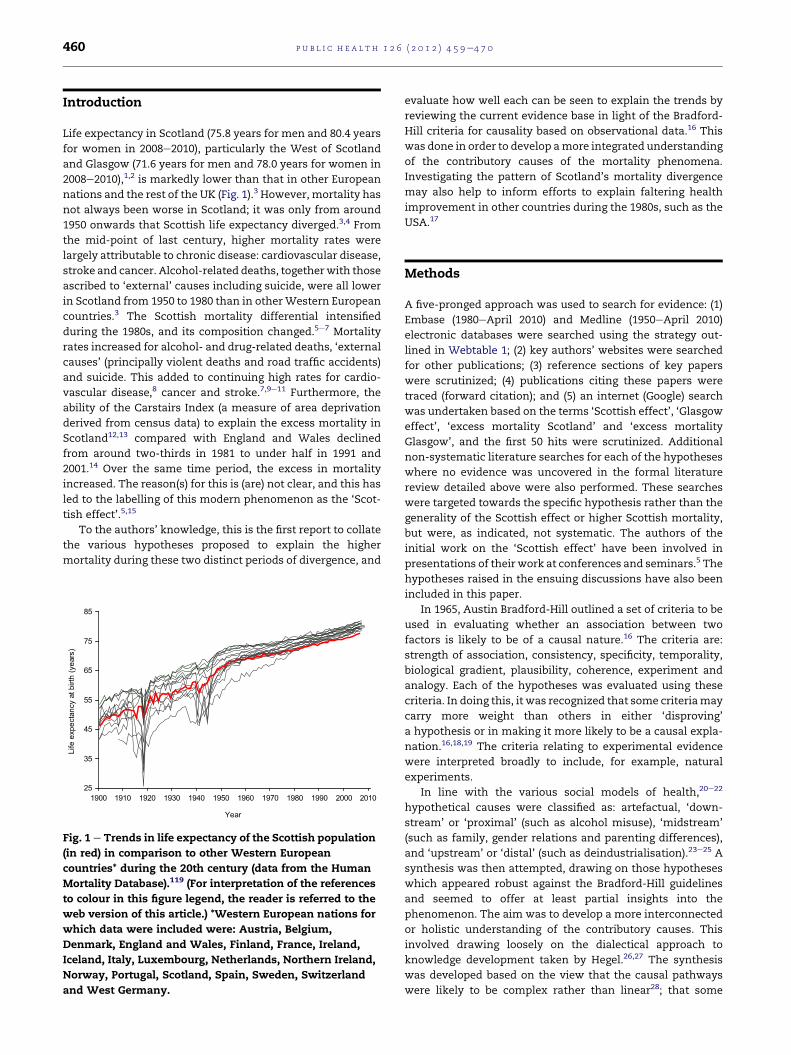
Life expectancy in Scotland (75.8 years for men and 80.4 years
for women in 2008e2010), particularly the West of Scotland
and Glasgow (71.6 years for men and 78.0 years for women in
2008e2010),1,2 is markedly lower than that in other European
nations and the rest of the UK (Fig. 1).3 However, mortality has
not always been worse in Scotland; it was only from around
1950 onwards that Scottish life expectancy diverged.3,4 From
the mid-point of last century, higher mortality rates were
largely attributable to chronic disease: cardiovascular disease,
stroke and cancer. Alcohol-related deaths, togetherwith those
ascribed to ‘external’ causes including suicide, were all lower
in Scotland from 1950 to 1980 than in otherWestern European
countries.3 The Scottish mortality differential intensified
during the 1980s, and its composition changed.5e7 Mortality
rates increased for alcohol- and drug-related deaths, ‘external
causes’ (principally violent deaths and road traffic accidents)
and suicide. This added to continuing high rates for cardio-
vascular disease,8 cancer and stroke.7,9e11 Furthermore, the
ability of the Carstairs Index (a measure of area deprivation
derived from census data) to explain the excess mortality in
Scotland12,13 compared with England and Wales declined
from around two-thirds in 1981 to under half in 1991 and
2001.14 Over the same time period, the excess in mortality
increased. The reason(s) for this is (are) not clear, and this has
led to the labelling of this modern phenomenon as the ‘Scot-
tish effect’.5,15
To the authors’ knowledge, this is the first report to collate
the various hypotheses proposed to explain the higher
mortality during these two distinct periods of divergence, and
25
35
45
55
65
75
85
1900 1910 1920 1930 1940 1950 1960 1970 1980 1990 2000 2010
Year
Life
exp
ecta
ncy
at b
irth
(yea
rs)
Fig. 1 e Trends in life expectancy of the Scottish population
(in red) in comparison to other Western European
countries* during the 20th century (data from the Human
Mortality Database).119 (For interpretation of the references
to colour in this figure legend, the reader is referred to the
web version of this article.) *Western European nations for
which data were included were: Austria, Belgium,
Denmark, England and Wales, Finland, France, Ireland,
Iceland, Italy, Luxembourg, Netherlands, Northern Ireland,
Norway, Portugal, Scotland, Spain, Sweden, Switzerland
and West Germany.
evaluate how well each can be seen to explain the trends by
reviewing the current evidence base in light of the Bradford-
Hill criteria for causality based on observational data.16 This
was done in order to develop amore integrated understanding
of the contributory causes of the mortality phenomena.
Investigating the pattern of Scotland’s mortality divergence
may also help to inform efforts to explain faltering health
improvement in other countries during the 1980s, such as the
USA.17
Methods
A five-pronged approach was used to search for evidence: (1)
Embase (1980eApril 2010) and Medline (1950eApril 2010)
electronic databases were searched using the strategy out-
lined in Webtable 1; (2) key authors’ websites were searched
for other publications; (3) reference sections of key papers
were scrutinized; (4) publications citing these papers were
traced (forward citation); and (5) an internet (Google) search
was undertaken based on the terms ‘Scottish effect’, ‘Glasgow
effect’, ‘excess mortality Scotland’ and ‘excess mortality
Glasgow’, and the first 50 hits were scrutinized. Additional
non-systematic literature searches for each of the hypotheses
where no evidence was uncovered in the formal literature
review detailed above were also performed. These searches
were targeted towards the specific hypothesis rather than the
generality of the Scottish effect or higher Scottish mortality,
but were, as indicated, not systematic. The authors of the
initial work on the ‘Scottish effect’ have been involved in
presentations of their work at conferences and seminars.5 The
hypotheses raised in the ensuing discussions have also been
included in this paper.
In 1965, Austin Bradford-Hill outlined a set of criteria to be
used in evaluating whether an association between two
factors is likely to be of a causal nature.16 The criteria are:
strength of association, consistency, specificity, temporality,
biological gradient, plausibility, coherence, experiment and
analogy. Each of the hypotheses was evaluated using these
criteria. In doing this, it was recognized that some criteriamay
carry more weight than others in either ‘disproving’
a hypothesis or in making it more likely to be a causal expla-
nation.16,18,19 The criteria relating to experimental evidence
were interpreted broadly to include, for example, natural
experiments.
In line with the various social models of health,20e22
hypothetical causes were classified as: artefactual, ‘down-
stream’ or ‘proximal’ (such as alcohol misuse), ‘midstream’
(such as family, gender relations and parenting differences),
and ‘upstream’ or ‘distal’ (such as deindustrialisation).23e25 A
synthesis was then attempted, drawing on those hypotheses
which appeared robust against the Bradford-Hill guidelines
and seemed to offer at least partial insights into the
phenomenon. The aim was to develop a more interconnected
or holistic understanding of the contributory causes. This
involved drawing loosely on the dialectical approach to
knowledge development taken by Hegel.26,27 The synthesis
was developed based on the view that the causal pathways
were likely to be complex rather than linear28; that some

p u b l i c h e a l t h 1 2 6 ( 2 0 1 2 ) 4 5 9e4 7 0 461
explanations were likely to be necessary but insufficient; and
that distinct hypotheses may reflect differing viewpoints on
the same phenomena, and may deal with different parts or
elements of a single causal pathway.
A fuller description of the methods, results and discussion
is given elsewhere.29
Results
The electronic database search yielded 309 potentially rele-
vant papers. From these, 76 were selected for detailed exam-
ination on the basis of the relevance of the title and abstract.
The notes from the discussions at various fora for the
dissemination of previous research5,9,10,12,13 identified further
hypotheses which were not reflected in the academic
literature.
In total, 17 hypotheses were identified which addressed
either: the higher mortality in Scotland, the higher mortality
in Glasgow (or the West of Scotland), the excess mortality in
Scotland after accounting for deprivation (Scottish effect), or
the excessmortality in Glasgow (or theWest of Scotland) after
accounting for deprivation (Glasgow effect). As indicated
above, some of the hypotheses are clearly closely related, and
others can also be linked. The hypotheses are dealt with below
in the following order: artefactual explanations (deprivation
and migration), ‘downstream’ explanations, ‘midstream’
explanations and ‘upstream’ explanations. The evidence
identified in each case is summarized and briefly appraised.
Where possible, evidence is given comparing Scotland with
England and Western Europe, and comparing Glasgow with
the rest of Scotland and other cities. For some of the hypoth-
eses, there has been little or no research. This does not
preclude the possibility that they will prove to be relevant in
the future, and a programme of research which will consider
a number of them is due to begin soon. Table 1 summarizes
how, in light of the currently available evidence, each of the
hypotheseswas found to fare against the Bradford-Hill criteria
for each of the time periods and population comparisons (i.e.
Glasgow compared with Scotland, Scotland compared with
England, Scotland compared with Western Europe) under
consideration. The links and relationships between the
hypotheses as regards the two periods are then dealt with
later in the paper.
Deprivation
HypothesisGreater deprivation in Scotland, particularly in the West of
Scotland and Glasgow, explains Scotland’s health trends.
EvidenceIn 1981, the majority of the excess mortality in Scotland,
compared with the rest of Britain, could be accounted for by
use of the Carstairs Index (a measure of area deprivation
derived from census data based on car ownership, over-
crowding, male unemployment and social class).14 The terms
‘Scottish effect’ or ‘Glasgow effect’ reflect the decline in the
proportion of the excess which could be so explained in 1991
and 2001, by reference to Carstairs or other available
measures of deprivation.5 One suggestion is that, in reality,
higher deprivation would account for a much higher propor-
tion of the excess, but that thesemeasures no longer ‘capture’
it effectively, either within Scotland or in comparison with
England (as differently sized urban populations were
compared between Scotland and England/Wales).30,31 Thus,
for the post-1980 period only, the suggestion is that the
‘effects’ are actually ‘artefacts’ created by inadequate depri-
vation measures. No evidence was identified that compared
deprivation levels between Scotland and other European
nations from 1950. The areas within the UK which show the
greatest deprivation have the greatest excess mortality.6,7
However, for the period 2003e2007, areas in Manchester and
Liverpool showed significantly lower mortality than areas of
similar size and income deprivation in Glasgow.12,13
Migration
HypothesisThere was a greater degree of emigration of healthy individ-
uals from Scotland than from other areas (the flip side of the
‘healthy migrant effect’).32e34
EvidenceAlthough there has been substantial emigration,6 recent
migrants display amortality pattern very similar to that of the
non-emigrating population and retain their higher mortality
rates.35e39 However, deprivation and localized migration does
explain much of the concentration of mortality within
Scotland.40e43
Genetic differences
HypothesisThe population is either predisposed to negative health
behaviours or is particularly vulnerable to the effects of such
behaviours due to genotype.
EvidenceThemigration studies are supportive of a genetic cause in that
the emigrant populations from Scotland and Glasgow carry
their mortality patterns with them as they move.35,39,40
However, a genetic cause is much less likely because the
mortality divergence between Scotland and the rest of the UK
seems to have occurred much too rapidly to be explained by
changes in the gene pool.
Health behaviours
HypothesisA higher prevalence of unfavourable health behaviours
(relating to alcohol, tobacco, illicit drugs, physical activity and
diet) is responsible for the mortality patterns.
EvidenceThere is a higher prevalence of problem drug use in Scotland44
and there was a rapid rise in illicit drug-related deaths during
the 1980s.45 Alcohol-related deaths are elevated and have
risen rapidly from around 1990.6 Alcohol consumption in
Glasgow is higher than in the rest of Scotland, even after
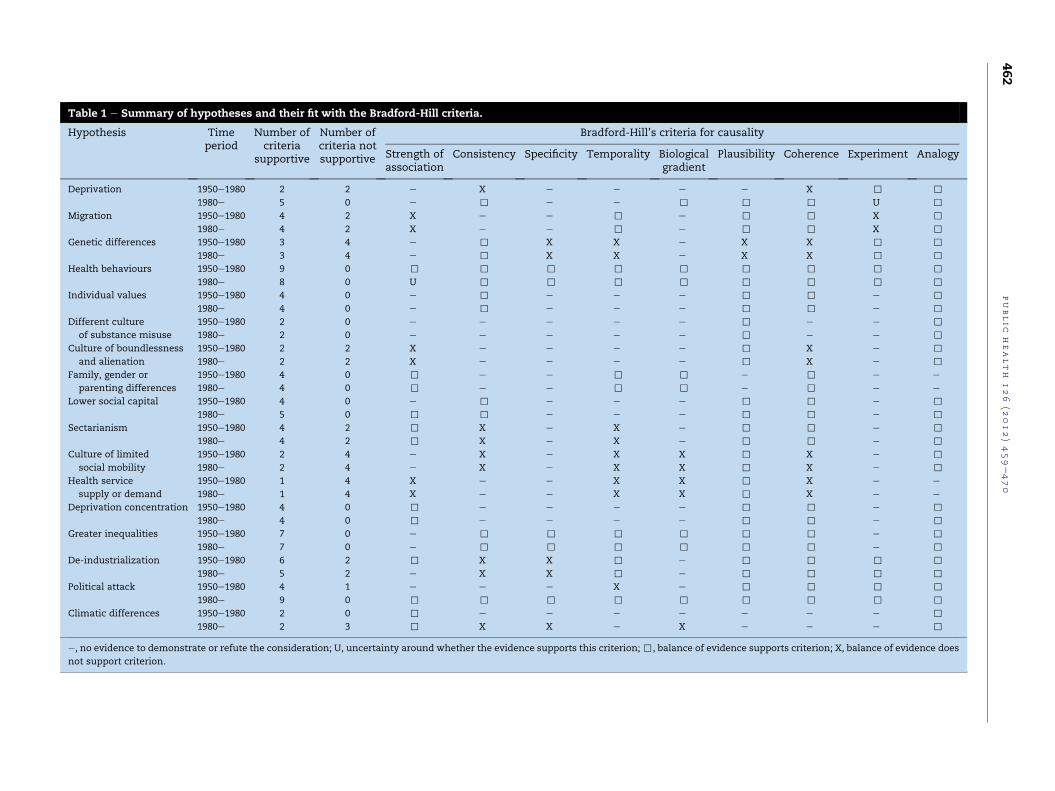
Table 1 e Summary of hypotheses and their fit with the Bradford-Hill criteria.
Hypothesis Timeperiod
Number ofcriteria
supportive
Number ofcriteria notsupportive
Bradford-Hill’s criteria for causality
Strength ofassociation
Consistency Specificity Temporality Biologicalgradient
Plausibility Coherence Experiment Analogy
Deprivation 1950e1980 2 2 e X e e e e X , ,
1980e 5 0 e , e e , , , U ,
Migration 1950e1980 4 2 X e e , e , , X ,
1980e 4 2 X e e , e , , X ,
Genetic differences 1950e1980 3 4 e , X X e X X , ,
1980e 3 4 e , X X e X X , ,
Health behaviours 1950e1980 9 0 , , , , , , , , ,
1980e 8 0 U , , , , , , , ,
Individual values 1950e1980 4 0 e , e e e , , e ,
1980e 4 0 e , e e e , , e ,
Different culture
of substance misuse
1950e1980 2 0 e e e e e , e e ,
1980e 2 0 e e e e e , e e ,
Culture of boundlessness
and alienation
1950e1980 2 2 X e e e e , X e ,
1980e 2 2 X e e e e , X e ,
Family, gender or
parenting differences
1950e1980 4 0 , e e , , e , e e
1980e 4 0 , e e , , e , e e
Lower social capital 1950e1980 4 0 e , e e e , , e ,
1980e 5 0 , , e e e , , e ,
Sectarianism 1950e1980 4 2 , X e X e , , e ,
1980e 4 2 , X e X e , , e ,
Culture of limited
social mobility
1950e1980 2 4 e X e X X , X e ,
1980e 2 4 e X e X X , X e ,
Health service
supply or demand
1950e1980 1 4 X e e X X , X e e
1980e 1 4 X e e X X , X e e
Deprivation concentration 1950e1980 4 0 , e e e e , , e ,
1980e 4 0 , e e e e , , e ,
Greater inequalities 1950e1980 7 0 e , , , , , , e ,
1980e 7 0 e , , , , , , e ,
De-industrialization 1950e1980 6 2 , X X , e , , , ,
1980e 5 2 e X X , e , , , ,
Political attack 1950e1980 4 1 e e e X e , , , ,
1980e 9 0 , , , , , , , , ,
Climatic differences 1950e1980 2 0 , e e e e e e e ,
1980e 2 3 , X X e X e e e ,
e, no evidence to demonstrate or refute the consideration; U, uncertainty around whether the evidence supports this criterion;,, balance of evidence supports criterion; X, balance of evidence does
not support criterion.
public
health
126
(2012)459e470
462

p u b l i c h e a l t h 1 2 6 ( 2 0 1 2 ) 4 5 9e4 7 0 463
adjustment for deprivation.46 Similarly, smoking-related
deaths (including cardiovascular disease, respiratory disease
and cancer)6 and smoking prevalence are higher in Greater
Glasgow than Scotland.47e52 Health Survey data relating to
diet, smoking and obesity comparing Scotland with England
do not explain overall excess mortality after adjustment for
deprivation,53,54 but this could reflect incomplete ascertain-
ment of these behaviours whichmay have a cumulative effect
across the life course on mortality experience.
Individual values
HypothesisThere is a higher prevalence of individuals who are more
hedonistic than elsewhere, or have lower aspirations, and
this, in turn, leads to a higher prevalence of adverse health
behaviours and higher mortality.
EvidenceNo evidence was identified relating to this hypothesis,
although it is related to some of the culturally orientated
hypotheses (see below).
Different culture of substance misuse
HypothesisThe way in which substances (illicit drugs, tobacco and
alcohol) are consumed in Scotland/Glasgow differs from
elsewhere, and/or there is a unique culture surrounding their
use which exacerbates their effects (as opposed to the
consumption rates per capita).
EvidenceVery little evidence comparing such cultures was identified,
although a review comparing alcohol cultures reported that
Scotland was not different from England, and not distinctive
in relation to other comparison nations.55
Culture of boundlessness and alienation
HypothesisA culture of boundlessness, hopelessness and alienation
(similar to some cultural patterns observed during the 19th
Century)56e58 is a cause of the higher mortality.
EvidenceThere is conflicting evidence around whether or not
a distinctive subculture exists, or whether differences simply
reflect greater privation and sharpening inequality.59e62
However, it is plausible that such a culture might be associ-
ated with the rise in alcohol-related, drug-related, violent and
suicide deaths.
Family, gender relations and parenting differences
HypothesisFamily breakdown, acrimony between partners or dysfunc-
tional parenting are more prevalent, and have a negative
influence on health.33,63e65
EvidenceNo comparative evidence was identified for this hypothesis,
other than the higher rates of reported domestic violence in
Glasgow than in Scotland overall.6 Some reports suggest that
alcohol misuse and gambling have maintained male identity
in the early 20th Century,66,67 which makes it unlikely to be
the causal exposure since the divergent mortality was not
seen until around 1950. Family disruption is closely associated
with a range of negative social and health outcomes,68,69 and
its prevalence rose rapidly from the early 1970s.70 However,
there is little difference in either lone parenthood or teenage
pregnancies between Glasgow, Liverpool or Manchester (or
between Scotland and England).12
Lower ‘social capital’
HypothesisLower ‘social capital’ is responsible for the mortality patterns.
EvidenceVery few comparative data are available for this hypothesis,
and further work is required to clarify whether there is
a difference between populations. However, some limited
comparisons (including volunteering and electoral attitudes)
suggest that Glasgow does less well than Scotland as a whole
on this indicator, but that Scotland is comparable to England
and Wales,71 and Glasgow is similar to Liverpool and Man-
chester.6 The only exception is the lower religious identifica-
tion in Scotland and Glasgow, although individual-level data
for older groups do not suggest that this has a protective
effect.6,12,72 Fear of crime may be lower in Glasgow than
elsewhere in Scotland, but somemeasures of ‘bonding capital’
may be higher in Scotland.71 The hypothesis is consistent with
the findings of Stuckler et al. in relation to the protective effect
of ‘social capital’ in Eastern Europe in the face of
neoliberalism.73
Sectarianism
HypothesisThe commonly recognized sectarian divide between Catholics
and Protestants in Scotland (and Glasgow and the West of
Scotland in particular) has contributed causally to the
mortality phenomenon.
EvidenceNo evidencewas identified that examinedwhether Scotland is
more affected by such divisions.33,74 However, Northern
Ireland (which undoubtedly has a greater sectarian problem
than Scotland) has reduced its mortality more rapidly than
Scotland since the middle of the 20th Century, and there is no
consistent association between peaks in sectarianism and
mortality in Scotland.34
Culture of limited social mobility
HypothesisA culture of limited aspiration and social immobility, linked to
a lack of confidence (fostered by Calvinism e a particular
Christian teaching which stresses the absolute power of God)

p u b l i c h e a l t h 1 2 6 ( 2 0 1 2 ) 4 5 9e4 7 0464
and other inhibiting social norms, is a cause of the higher
mortality.33,75
EvidenceThis hypothesis focuses on the emergence of cultural patterns
in the first decades of the 20th Century,33 giving a problematic
temporal relation with both mortality divergences. No
comparative evidence was identified for confidence (except
more recently in adolescents).76 Association with Calvinism
(using Presbyterianism as a proxy) is weak since it has always
been more dominant in the North of Scotland,77 and no
evidence was identified to suggest that a ‘cultural Calvinism’
extends to other groups. There is mixed evidence relating to
those associated with the Irish Catholic community in the
West of Scotland, whose younger members suffer greater
deprivation but have similar health outcomes,78 whose adults
are exposed to a worse diet,79 and whose working men have
higher mortality after adjusting for smoking and deprivation
(particularly from cardiovascular disease).80
Health service supply or demand
HypothesisThe quality, accessibility or demand for health services is
a cause of the higher mortality.
EvidenceThere is evidence that the variation in health service use
between Scotland and the rest of the UK is minimal compared
with the variation in the provision of services within regions
and cities,81 but there is an absence of evidence examining the
distribution of the inverse care law (whereby services are
provided in inverse proportion to the need for services).82e84
Scotland has higher health spending than other parts of the
UK,85 although it is unclear if this is related to greater need,
rurality, higher quality or lower productivity.86 No evidence
was identified which compares how National Health Service
resources are deployed (e.g. proportion spent on primary care
in different areas). The quality of primary care is higher in
Scotland (as measured by the Quality and Outcomes Frame-
work), as are vaccination rates, the care of patients with acute
heart attacks and waiting times,85 although making valid
comparisons presents methodological difficulties.87 Most of
the specific causes of mortality which have diverged since
1980 are not normally considered to be amenable to health
care.
Deprivation concentration (‘area effects’)
HypothesisThe deprived areas in Scotland and Glasgow form large,
concentrated, monocultural communities to a greater extent
than elsewhere, and this has a negative causal impact on
health.
EvidenceVariation in Scottishmortality in 2001 was better explained by
including a measure of the deprivation in surrounding
geographical areas, in addition to the deprivation of the
specific area of residence.88
Greater inequalities
HypothesisGreater income inequality is a cause of the phenomenon.
EvidenceThis fits with a growing evidence base which suggests that
health and social outcomes are better in more equitable
nations.89,90 Some studies have found an association between
higher regional income inequality and worse self-rated health
in Britain,89e91 whilst others have found no relation.92 Income
inequality is lower in Scotland than in England,93,94 although
inequality effects may be most profound at a UK level.95,96
De-industrialization
HypothesisA particularly profound de-industrialization was suffered in
Scotland and this is a cause of the phenomenon.
EvidenceScotland (and Glasgow along with the West of Scotland) was
recently found to have higher mortality than comparable de-
industrialized areas across Northern Europe, despite lower
poverty levels and lower unemployment.9,10 The West of
Scotland lost the greatest number of industrial jobs as
a proportion of total employmentwhen comparedwith 10 such
de-industrialized areas across the UK and mainland
Europe,9,10,97 and experienced greater de-industrialization than
elsewhere in the UK (Merseyside being the next worst affected
region).98 There is a close temporal relationship between de-
industrialization and the emergence of the Scottish effect.9,10
Political attack
HypothesisThe UK was exposed to a form of neoliberalism after 1979 e
not seen in other European countries e which amounted to
a political attack on the organized working class. Scotland,
and particularly Glasgow, was more vulnerable than other
parts of the UK (indicated by the relative scale of de-
industrialization and the extent of reliance on council
housing compared with other UK regions). This political
attack provoked a distinctive reaction in sociopolitical culture
encapsulated in the idea of a nation being under ‘attack’ by
a government without a political mandate, creating a ‘demo-
cratic deficit’, which was, in turn, compounded by the relative
acquiescence of local government.99,100
EvidenceDeprivation explains a larger proportion of the excessmortality
betweenScotlandandEngland/Walesuntil the implementation
of neoliberalism by the Thatcher Government in the
1980s.5,6,12,13 Indeed, themortality rates in theWest of Scotland
comparewell with other European de-industrialized areas until
this time.9,10 A mortality pattern similar, if more profound, to
Scotlandappeared in the formerUSSRafter 1989as it undertook
a rapid transition from state communism to free market capi-
talism (including similar cause-specific mortality
patterns).73,101,102 Neoliberalism was implemented most

p u b l i c h e a l t h 1 2 6 ( 2 0 1 2 ) 4 5 9e4 7 0 465
vigorously in the UK comparedwith other European nations.103
TheWestofScotlandhadahigherproportionofcouncilhousing
and industrial employment than other UK regions, and the
specific opposition from the region to the neoliberal politics of
an earlier Conservative administration (that of Edward Heath)
may have made the region a particular target for the
attack.100,104 The electoral trends and historical accounts of the
period after 1979 show a particular reaction, in terms of socio-
political culture, against neoliberalism, indicative of a strongly
intensifying sense of disempowerment.100 Finally, Glasgow is
noted as having had a particular emphasis on accommodating
andpromoting neoliberalismduring the 1980s,whichmayalso,
in part, help explain the greater vulnerability of the city.105,106
Climatic differences
HypothesisA lack of sunlight leads to a deficit in vitaminD,107 and harsher
winters increase mortality through the effects of the cold.
EvidenceThere is evidence of a gradient in vitamin D levels in pop-
ulation blood samples between Scotland and the rest of the
UK (but not between areas in Scotland),108 but there is no
coherence with the problematic cause-specific mortalities nor
clear evidence of temporal changes (although changes in diet
or housing are plausible drivers of such change).108 There
were 51,600 Scottish excess winter deaths between 1989 and
2001, almost all of which occurred in those aged over 65 years,
andmostly in deprived areas such as Glasgow.109,110 Although
important, this could not easily explain the divergence from
1980, which affected younger age groups, nor explain the
cause-specific mortality patterns.7
As indicated earlier, Table 1 summarizes how each of the
above hypotheses was found to fare against the Bradford-Hill
criteria for each of the time periods under consideration.
Synthesis for the mortality divergence 1950e1980
The divergence of Scottishmortality from that of its European
neighbours from 1950 onwards was largely due to a less rapid
Substance misuse
Key determining
factors
Low wage and unstable industrial
employment
Increased stress
Gender disharmony
Possible
Poverty and inequality
Migration patterns
Erosion osocial capit
Overcrowding and poor housing conditions
Lack of vitamin D
Lack of coservices &
Fig. 2 e Simplified representation of the synthesis of the cause of
from 1950 onwards.
reduction in deaths from cardiovascular disease, stroke,
respiratory disease and cancer. There has been less research
into this earlier divergence, and the precise nature of the
causal pathways is therefore far from certain. On balance, it is
likely that a greater exposure to negative health behaviours
such as smoking, alcohol, poor diet and low levels of physical
activity goes some way to explaining the divergence. Cultural
factors (including family, gender relations and parenting
differences, a culture of limited social mobility, and a negative
alcohol culture) may have been operant, but it is less likely
that they are the cause of the divergent pattern (e.g. Scotland
had lower alcohol-related deaths than the rest of Europe until
around 1990).11 It is unclear whether Scotland suffered from
greater poverty than other European nations around 1950, but
it is possible, and in terms of historical accounts plau-
sible,111,112 that unemployment, more precarious industrial
employment, inequality, overcrowded housing conditions
and the large-scale reconstruction which resulted in the
peripheral council housing estates around Glasgow, Edin-
burgh and other large Scottish conurbations could be impor-
tant in providing a causal explanation (Fig. 2). However,
significant new work would be required to investigate this.
More work is also required to determine whether or not
climatic influences (including the role of vitamin D) are
important in explaining the higher mortality in Scotland
during this time. It does not seem likely that genetic factors or
health service quality, supply or demand are important
explanations for the mortality divergence, although there is
little evidence available to examine such suggestions.
Synthesis for the mortality divergence from 1980
It is likely that a proportion of the excessmortality in Scotland
and Glasgow not explained by the Carstairs Index is, in fact,
due to deprivation, and that the Index has become a less
sensitive measure. However, the comparisons of Glasgow,
Liverpool and Manchester provide strong evidence that there
is amortality excess in Glasgow in addition to that attributable
to deprivation.12,13 Migration is unlikely to have played a key
role in generating the higher mortality pattern. It does not
Multiple deprivation
('area effects')
mechanisms Outcomes
f al Cardiovascular
disease
Respiratory disease
Stroke
Cancer
Inequalities
Social isolation
Excess winter deathsmmunity
facilities
Construction of peripheral
council housing
the divergence of Scottishmortality from the rest of Europe

p u b l i c h e a l t h 1 2 6 ( 2 0 1 2 ) 4 5 9e4 7 0466
seem likely that genetic factors, climatic influences or health
service quality, supply or demand are important explanations
for the higher mortality from 1980, the Scottish effect or
Glasgow effect.
A hypothesis showing a strong fit with the Bradford-Hill
criteria concerns the prevalence of various health behav-
iours (particularly alcohol and drug use). Although these
exposures are causal, the synthesis requires an explanation
for the higher prevalence of these negative health behaviours,
or why their effects aremore profound in the Scottish context.
The culturally orientated hypotheses (including individual
values; lower social capital; family, gender relations and
parenting differences; substance abuse; culture of alienation
and boundlessness; and culture of limited social mobility) are
plausible and have some evidence, but require further
comparative research and are challenged in terms of
explainingwhy the Scottish and Glaswegian populations were
worse affected than other areas from the early 1980s (rather
than at an earlier time). These cultural hypotheses, and the
hypothesis relating to negative health behaviours, are there-
fore necessary and important explanations in describing the
causes of the Scottish effect and the Glasgow effect, but are
not sufficient. Structural explanations (including inequalities
and de-industrialization) fit well with the Bradford-Hill
criteria and are likely to have played an important causal
role, but on the basis of the available evidence and the appli-
cation of the Bradford-Hill criteria, the political attack
hypothesis seems to be the strongest upstream candidate,
best placed to bring together the most likely behavioural,
cultural and structural determinants of health into a coherent
narrative which can explain the post-1980 mortality
phenomenon (Fig. 3). However, other posited explanations, for
which there is currently little or no research evidence, may
prove important in developing e or altering e this view. It is
important, therefore, that further research relevant to these
hypotheses is undertaken.
Discussion
Clearly, further work is required on the higher mortality in
Scotland between 1950 and 1980. The most plausible causal
Key
determining
factors
Stress
Possibl
Alienation and boundlessness
Deindustrialisation
Rise in inequality and poverty
Breakdownwork
Poverty and inequality
Industrial dependence
Scottish culture
Trigger
Political attack
Fig. 3 e Simplified representation of the synthesis of the cause
effect.
explanation on the basis of current thinking and available
evidence is that higher poverty, deprivation and inequality
were associated with particular industrial employment
patterns, housing and urban environments, particular
community and family dynamics, and negative health
behaviour cultures. From 1980 onwards, the higher mortality
is driven by negative health behaviours, and it is likely that
these were linked to an intensifying climate of conflict,
injustice and disempowerment. This seems best explained by
the political attack hypothesis which suggests that the
neoliberal policies implemented from 1979 onwards dispro-
portionately affected the Scottish and Glaswegian pop-
ulations. In each case, it is important to bear in mind, as
highlighted previously, that causal pathways are likely to be
complex, and that underlying causes may be compounded or
alleviated by a range of other factors.
Strengths and weaknesses of the study
It is unlikely that there are important hypotheses for the
mortality phenomenon in Scotland (and Glasgow) that were
missed by the search strategy. However, the study has not yet
reached saturation point, and each key publication tends to
generate further speculation. For example, a reviewer of this
paper suggested that the Barker hypothesis113 might provide
some explanation (which it may do, but not without some
exploration of the key differences in pre-birth exposurese not
captured by the measures of deprivation e between the pop-
ulations of interest). The appraisal process using the Bradford-
Hill criteria was robust and is likely to have minimized bias in
the synthesis process. It is, however, possible that some
deductive hypotheses arising from outside the health
research field may have been missed. Furthermore, it may be
that some evidence relating to a particular hypothesis has
been overlooked since the search strategy for each hypoth-
esis, once identified, was not systematic (as performing 17
systematic reviews was not practical). This could have
significantly underestimated the quantity and quality of the
evidence available for a particular explanation, and could
have biased the results of the synthesis. Finally, for some of
the hypotheses, there has been, as indicated previously, little
or no research. Such hypotheses might yet prove to be
Disempowerment and hopelessness
Democratic deficit
Substance misuse
e mechanisms Outcomes
Drugs-related
Alcohol-related
Suicide
Road traffic accidents
Decreased social capital
Violence
in confidence of ing classes
of the higher Scottish mortality from 1980 and the Scottish

p u b l i c h e a l t h 1 2 6 ( 2 0 1 2 ) 4 5 9e4 7 0 467
relevant, and the application of the Bradford-Hill criteria in
this paper should not be seen in any way to preclude that
possibility. A further programme of research which will
investigate a number of them is due to begin soon.
Implications
It is clear that there is a difference between how the Scottish
mortality problem is commonly viewed and the findings of
this preliminary synthesis. Usually, the higher mortality is
attributed to higher rates of smoking, greater alcohol
consumption and poorer diet, which is, of course, truee as far
as it goes. However, such an explanation is not sufficient to
understand why the mortality picture in Scotland is so very
different from that of other, seemingly comparable, areas.
This is a common theme in public health, and exemplifies the
need to consider the ‘upstream causes of the causes’.114e116
The policies of the recently elected UK Conservative-Liberal
coalition include radical cuts to public spending (focused, in
particular, although by no means exclusively, on welfare
benefits), privatizing and residualizing public services, and
massive reliance on private sector growth and entrepreneur-
ialism to provide employment, wealth and welfare. These
policies quite closely resemble the Thatcherite neoliberal
agenda of the 1980s, which this study suggests was closely
connected to processes of community disruption and dis-
empowerment in that decade. This study also suggests that
agenda, theorized as ‘political attack’, is likely to be important
as a point of departure in providing a broad and synthetic
causal explanation for both the Scottish mortality crisis and
for the sharp rise in health inequalities over the last 30
years.117 These policies also closely resemble those which
have had a detrimental impact on aggregate mortality across
Europe.118
Further comparative work to identify which factors played
an important role in the divergence of Scottish mortality from
1950 is merited, as are further systematic reviews of the
literature for each of the identified hypotheses.
Conclusion
For over half a century, Scotland has suffered from higher
mortality than comparably wealthy countries, and for the last
30 years has suffered from a new and troubling mortality
pattern. It is unlikely that any single cause is entirely
responsible, and there is uncertainty around why Scotland
started to diverge from elsewhere in Europe around 1950. It is
clearer that the health and social patterns that emerged from
the 1980s are more closely linked to negative health behav-
iours (e.g. alcohol consumption), but these behaviours are, in
turn, heavily influenced and shaped by the social, cultural and
economic disruption which occurred as the political and
economic policies of the UK changed from the late 1970s. Any
understanding of the Scottish mortality patterning requires,
as well as a clear focus on behaviours, an understanding of the
most ‘upstream’ determinants of health, including those to be
confronted in economic, social and political history. Any
analysis which only refers to tobacco use or alcohol, or even to
‘early years’, massively significant as these factors
undoubtedly are, will inevitably fail to identify the overall
causality of this profoundly troubling phenomenon, and will
be liable to generate, at best, partial policy interventions,
which are, in turn, most liable to prove disappointing in their
outcomes.
Acknowledgements
Ethical approval
None sought.
Funding
None declared.
Competing interests
GM is a member of the Scottish Socialist Party. DW, GDB and
CC have no competing interests.
r e f e r e n c e s
1. Life expectancy for areas in Scotland. Edinburgh: NationalRecords of Scotland. Available at: http://www.gro-scotland.gov.uk/statistics/theme/life-expectancy/scottish-areas/2008-2010/index.html; 2011. 2008e2010, [last accessed 15November 2011]..
2. Norman P, Boyle P, Exeter D, Feng Z, Popham F. Risingpremature mortality in the UK’s persistently deprived areas:only a Scottish phenomenon? Soc Sci Med 2011;73:1e10.
3. Leon D, Morton S, Cannegieter S, McKee M. Understanding thehealth of Scotland’s population in an international context:a review of current approaches, knowledge and recommendationsfor new research directions. London: London School of Hygieneand Tropical Medicine & Public Health Institute for Scotland.Available at: http://www.scotpho.org.uk/home/Comparativehealth/InternationalComparisons/int_mortality_comparisons.asp; 2003 [last accessed 20 April2010].
4. McCartney G, Walsh D, Whyte B, Collins C. Has Scotlandalways been the ‘sick man’ of Europe?. Eur J Public Health.doi:10.1093/eurpub/ckr136.
5. Hanlon P, Lawder R, Buchanan D, Redpath A, Walsh D,Wood R. Why is mortality higher in Scotland than in England& Wales? Decreasing influence of socioeconomicdeprivation between 1981 and 2001 supports the existence ofa ‘Scottish effect’. J Public Health 2005;27:199e204.
6. Hanlon P, Walsh D, Whyte B. Let Glasgow flourish. Glasgow:Glasgow Centre for Population Health; 2006.
7. Leyland A, Dundas R, McLoone P, Boddy F. Cause-specificinequalities in mortality in Scotland: two decades of change.A population-based study. BMC Public Health; 2007::7.
8. Davies C, Dundas R, Leyland A. Increasing socioeconomicinequalities in first acute myocardial infarction in Scotland,1990e92 and 2000e02. BMC Public Health; 2009::9.
9. Walsh D, Taulbut M, Hanlon P. The aftershock ofdeindustrialization e trends in mortality in Scotland andother parts of post-industrial Europe. Eur J Public Health2010;20:58e64.
10. Walsh D, Taulbut M, Hanlon P. The aftershock ofdeindustrialisation e trends in mortality in Scotland and otherparts of post-industrial Europe. Glasgow: Glasgow Centre forPopulation Health; 2008.
p u b l i c h e a l t h 1 2 6 ( 2 0 1 2 ) 4 5 9e4 7 0468
11. Whyte B. Scottish mortality in a European context 1950e2000: ananalysis of comparative mortality trends. Edinburgh: ScottishPublic Health Observatory. Available at: http://www.scotpho.org.uk/nmsruntime/saveasdialog.asp?lID¼3591&sID¼3079; 2007 [last accessed 20 April 2010].
12. Walsh D, Bendel N, Jones R, Hanlon P. Investigating a ‘Glasgoweffect’: why do equally deprived UK cities experience differenthealth outcomes. Glasgow: Glasgow Centre for PopulationHealth; 2010.
13. Walsh D, Bendel N, Jones R, Hanlon P. It’s not ‘justdeprivation’: why do equally deprived UK citiesexperience different health outcomes? Public Health2010;124:487e95.
14. Carstairs V, Morris R. Deprivation: explaining differences inmortality between Scotland and England and Wales. BMJ1989;299:886e9.
15. The Scottish effect? Edinburgh: Scottish Council FoundationHealthy Public Policy Network; 1998.
16. Hill A. The environment and disease: association orcausation? Proc R Soc Med 1965;58:295e300.
17. Navarro V, Muntaner C, Borrell C, Benach J, Quiroga A,Rodrıguez-Sanz M, et al. Politics and health outcomes.Lancet; 2006::1033e7.
18. Identifying the environmental causes of disease. how shouldwe decide what to believe and when to take action?. London:Academy of Medical Sciences; 2007.
19. Weiss NS. Can the ‘specificity’ of an association berehabilitated as a basis for supporting a causal hypothesis?Epidemiology 2001;13:6e8.
20. Dahlgren G, Whitehead M. Policies and strategies to promotesocial equity in health. Stockholm: Institute of Futures Studies;1991.
21. Evans R, Stoddart G. Producing health, consuming healthcare. Soc Sci Med 1990;31:1347e63.
22. Lynch J. Socio-epidemiology: some observations the past,present and future. Australas Epidemiol 2000;7:7e15.
23. Link B, Phelan J. McKeown and the idea that socialconditions are fundamental causes of disease. Am J PublicHealth 2002;92:730e2.
24. Rose G. Sick individuals and sick populations. Int J Epidemiol1985;14:32e8.
25. McLaren L, McIntyre L, Kirkpatrick S. Rose’s populationstrategy of prevention need not increase social inequalitiesin health. Int J Epidemiol 2010;39:372e7.
26. Williams H. Hegel, Heraclitus, and Marx’s dialectic. HarvesterWheatsheaf; 1989.
27. Hegel G. Hegel’s science of logic. London: Allen & Unwin; 1812.28. Hunter DJ. Leading for health and wellbeing: the need for
a new paradigm. J Public Health 2009;31:202e4.29. McCartney G, Collins C, Walsh D, Batty GD. Accounting for
Scotland’s excess mortality: towards a synthesis. Glasgow:Glasgow Centre for Population Health. Available at: http://www.gcph.co.uk/assets/0000/1080/GLA147851_Hypothesis_Report__2_.pdf; 2011 [last accessed 15 November 2011].
30. George S. It’s not just deprivation e or is it? Public Health2010;124:196e7.
31. Reid J. Excess mortality in the Glasgow conurbation: exploring theexistence of a Glasgow effect. Glasgow: University of Glasgow;2008.
32. Boffeta P, Brennan P, Saracci R. Neoplasms. In: Detels R,McEwan J, Beaglehole R, Tanaka H, editors. Oxford textbookof public health. Oxford: Oxford University Press; 2004.p. 1156.
33. Craig C. The tears that made the Clyde e well-being in Glasgow.Glendaruel: Argyll Publishing; 2010.
34. Devine TM. The Scottish nation. London: Penguin; 1999.35. Popham F, Boyle PJ, Norman P. The Scottish excess in
mortality compared to the English and Welsh. Is it a country
of residence or country of birth excess? Health Place; 2010.doi:10.1016/j.healthplace.2010.03.007.
36. Wild S, McKeigue P. Cross sectional analysis of mortality bycountry of birth in England and Wales, 1970e92. BMJ1997;314:705e10.
37. Bhala N, Bhopal R, Brock A, Griffiths C, Wild S. Alcohol-related and hepatocellular cancer deaths by country of birthin England andWales: analysis of mortality and census data.J Public Health 2009;31:250e7.
38. Wannamethee S, Shaper A, Whincup P, Walker M. Migrationwithin Great Britain and cardiovascular disease: early lifeand adult environmental factors. Int J Epidemiol2002;31:1054e60.
39. Popham F, Boyle P, O’Reilly D, Leyland A. Selective internalmigration. Does it explain Glasgow’s worsening mortality record?Scottish Longitudinal study (SLS) research working paper series.Edinburgh: GRO Scotland; 2009.
40. Exeter D, Boyle P, Feng Z, Boyle M. Shrinking areas andmortality: an artefact of deprivation effects in the West ofScotland? Health Place 2009;15:399e401.
41. Exeter D, Feng Z, Flowerdew R, Boyle P. Shrinking areas andmortality: an artefact of deprivation effects? J EpidemiolCommun Health 2005;59:924e6.
42. Brimblecombe N, Dorling D, Shaw M. Migration andgeographical inequalities in health in Britain. Soc Sci Med2000;50:861e78.
43. Brimblecombe N, Dorling D, Shaw M. Mortality andmigration in Britain, first results from the British householdPanel survey. Soc Sci Med 1999;49:981e8.
44. World drug report 2010. New York: United Nations Office onDrugs and Crime; 2010.
45. Bloor M, Gannon M, Hay G, Jackson G, Leyland A.Contribution of problem drug users’ deaths to excessmortality in Scotland: secondary analysis of cohort study.BMJ 2008;337:a478.
46. Gray L. Comparisons of health-related behaviours and healthmeasures between Glasgow and the rest of Scotland. Glasgow:Glasgow Centre for Population Health; 2007.
47. Gray L. Is the ‘Glasgow effect’ of cigarette smoking explainedby socio-economic status? A multilevel analysis. BMC PublicHealth; 2009::9.
48. Hart C, Hole D, Gillis C, Smith G, Watt G, Hawthorne V. Socialclass differences in lung cancer mortality: risk factorexplanations using two Scottish cohort studies. Int JEpidemiol 2001;30:268e74.
49. Gruer L, Hart CL, Gordon DS, Watt GC. Effect of tobaccosmoking on survival of men and women by social position:a 28 year cohort study. BMJ 2009;338:b480.
50. Gillis C, Hole D, Boyle P. Cigarette smoking and male lungcancer in an area of very high incidence. I Report ofa caseecontrol study in the West of Scotland. J EpidemiolCommun Health 1988;42:38e43.
51. Gillis C, Hole D, Hawthorne V. Cigarette smoking and malelung cancer in an area of very high incidence. II Report ofa general population cohort study in the West of Scotland. JEpidemiol Commun Health 1988;42:44e8.
52. Mitchell R, Fowkes G, Blane D, Bartley M. High rates ofischaemic heart disease in Scotland are not explained byconventional risk factors. J Epidemiol Commun Health2005;59:565e7.
53. Shelton N. Regional risk factors for health inequalities inScotland and England and the ‘Scottish effect’. Soc Sci Med2009;69:761e7.
54. Gray L, Leyland A. A multilevel analysis of diet and socio-economic status in Scotland: investigating the ’Glasgoweffect’. Public Health Nutr 2008;12:1351e8.
55. Gordon R, Heim D, MacAskill S, Angus K, Dooley J, Merlot R,et al. Snapshots of drinking: a rapid review of drinking cultures
p u b l i c h e a l t h 1 2 6 ( 2 0 1 2 ) 4 5 9e4 7 0 469
and influencing factors: australia, Canada, France, Germany,Spain, Sweden and the United Kingdom and Scotland. Edinburgh:NHS Health Scotland; 2008.
56. Durkheim E. The division of labour in society. New York: TheFree Press; 1984.
57. Durkheim E. Suicide. New York: The Free Press; 1951.58. Marx K. Estranged labour. Economic and philosophic manuscripts
of 1844. New York: Dover Publications; 2007.59. Buckingham A. Is there an underclass in Britain? Br J Sociol
1999;50:49e75.60. MacDonald R, Marsh J. Employment, unemployment and
social polarization. In: CromptonR,Devine F, SavageM, Scott J,editors. Renewing class analysis. Oxford: Blackwell; 2000.
61. Marshall G, Roberts S, Burgoyne C. Social class andunderclass in Britain and the USA. Br J Sociol 1996;47:22e44.
62. Dean M. Christmas, The poor, and the development of a UKunderclass. Lancet 1989;334:1536e7.
63. Breakthrough Glasgow. ending the costs of social breakdown.London: Centre for Social Justice; 2008.
64. Craig C. Women and children last. Scott Rev Books 2010;6:4e6.65. Donnelly P. Explaining the Glasgow effect: could adverse
childhood experiences play a role? Public Health2010;124:498e9.
66. Hughes A. Working class culture, family fife and domesticviolence on Clydeside, c1918e1939: a view from below. ScottTrad; 2002.
67. Hughes A. Representation and counter-representations ofdomestic violence on Clydeside between the two WorldWars. Labour Hist Rev 2004;69:169e84.
68. O’Neill R. Experiments in living: the fatherless family. London:Civitas; 2002.
69. Britain Breakdown. Interim report on the state of the nation.London: Social Justice Policy Group; 2006.
70. Rowthorn R, Webster D. Male worklessness and the rise oflone parenthood in Great Britain. Camb J Regions Econ Soc2008;1:69e88.
71. Bell D, Blanchflower DG. The Scots may be brave but they areneither healthy nor happy. Bonn: Institute for the Study ofLabor; 2005.
72. Gilhooly M, Hanlon P, Cullen B, Macdonald S, Whyte B.Successful ageing in an area of deprivation: part 2 e
a quantitative exploration of the role of personality andbeliefs in good health in old age. Public Health2007;121:814e21.
73. Stuckler D, King L, McKee M. Mass privatisation and thepost-communist mortality crisis: a cross-national analysis.Lancet 2009;373:399e407.
74. Sectarianism in Glasgow e final report. Edinburgh: NFO SocialResearch; 2003.
75. Craig C. The Scots’ crisis of confidence. Glasgow: Big Thinking;2005.
76. Currie C, Todd J. Mental well-being among schoolchildren inScotland: age and gender patterns, trends and cross-nationalcomparisons. Edinburgh: Child & Adolescent Health ResearchUnit, University of Edinburgh; 2003.
77. Williams R. Britain’s regional mortality: a legacy fromdisaster in the Celtic periphery? Soc Sci Med 1994;39:189e99.
78. Abbots J, Williams R, Sweeting H, West P. Poor but healthy?The youngest generation of Irish catholics in west Scotland.Health Bull 2001;59:373e80.
79. Mullen K, Williams R, Hunt K. Irish descent, religion andfood consumption in the West of Scotland. Appetite2000;34:47e54.
80. Abbots J, Williams R, Smith G. Association of medical,physiological, behavioural and socio-economioc factors withelevated mortality in men of Irish heritage in West Scotland.J Public Health 1999;21:46e54.
81. Haynes R. Inequalities in health and health service use:evidence from the general household survey. Soc Sci Med1991;33:361e8.
82. Mercer S, Watt G. The inverse care law: clinical primary careencounters in deprived and affluent areas of Scotland. AnnFam Med 2007;5:503e10.
83. McLean G, Sutton M, Guthrie B. Deprivation and quality ofprimary care services: evidence for persistence of theinverse care law from the UK Quality and OutcomesFramework. J Epidemiol Commun Health 2006;60:917e22.
84. Smith C. Equity in the distribution of health and welfareservices: can we rely on the state to reverse the ’inverse carelaw’? Soc Sci Med 1986;23:1067e78.
85. Sutherland K, Coyle N. Quality in healthcare in England, Wales,Scotland, Northern Ireland: an intra-UK chartbook. London:Health Foundation; 2009.
86. Connolly S, Bevan G, Mays N. Funding and performance ofhealthcare systems in the four countries of the UK before and afterdevolution. London: Nuffield Trust; 2010.
87. McLaren J, Armstrong J, Harris R. Spending on health. ScottishGovernment budget options. Glasgow: Centre for Public Policyfor Regions in Association with KPMG; 2010.
88. Sridharan S, Tunstall H, Lawder R, Mitchell R. An exploratoryspatial data analysis approach to understanding therelationship between deprivation and mortality in Scotland.Soc Sci Med 2007;65:1942e52.
89. Wilkinson R. The impact of inequality: how to make sick societieshealthier. Abingdon: Routledge; 2005.
90. Wilkinson R, Pickett K. The spirit level: why more equal societiesalmost always do better. London: Penguin; 2009.
91. Weich S, Lewis G, Jenkins S. Income inequality and selfrated health in Britain. J Epidemiol Commun Health 2002;56:436e41.
92. Gravelle H, Sutton M. Income, relative income and self-ratedhealth in Britain 1979e2000. York: Centre for HealthEconomics; 2006.
93. Households below average income (HBAI) 1994/95e2007/08.London: Department for Work and Pensions; 2009.
94. Grainger S, Stewart S. Income distribution in Scotland. Scottisheconomic statistics. Edinburgh: Scottish Executive; 2007.
95. McLoone P, Boddy F. Deprivation and mortality in Scotland,1981 and 1991. BMJ 1994;309:1465e70.
96. Hills J, Brewer M, Jenkins S, Lister R, Lupton R, Machin S,et al. Anatomy of economic inequality in the UK: report of theNational Equality Panel. London; 2010.
97. Turok I, Edge N. The jobs gap in Britain’s cities: employment lossand labour market consequences. Bristol: Policy Press; 1999.
98. Owen D, Gillespie A, Coombes M. ’Job shortfalls’ in Britishlocal labour market areas: a classification of labour supplyand demand trends, 1971e1981. Region Stud 1984;18:469e88.
99. McCormack C. The wee yellow butterfly. Glasgow: ArgyllPublishing; 2009.
100. Collins C, McCartney G. Is a ‘political attack’ an explanationfor the ‘Scottish effect’ in health outcomes? Int J Health Serv;2011::41.
101. Leon D, Chenet L, Shkolnikov V, Zakharov S, Shapiro J,RakhmanovaG, et al. Huge variation inRussianmortality rates1984e1994: artefact, alcohol, or what? Lancet 1997;350:383e8.
102. Shkolnikov V, McKee M, Leon D. Changes in life expectancyin Russia in the mid-1990s. Lancet 2001;357:917e21.
103. Birch K, Mykhnenko V. Varieties of neoliberalism?Restructuring in large industrially dependent regionsacross Western and Eastern Europe. J Econ Geog 2009;9:355e80.
104. Phillips J.The industrial politics of devolution: Scotland in the 1960sand 1970s. Manchester: Manchester University Press;; 2008.
105. Gray N. The tyranny of rent. Variant 2010;37:37e43.

Appendix A. Supplementary material
Supplementary material associated with this article can be
found, in the online version, at doi:10.1016/j.puhe.2012.03.007.
p u b l i c h e a l t h 1 2 6 ( 2 0 1 2 ) 4 5 9e4 7 0470
106. Boyle M, McWilliams C, Rice G. The spatialities of actuallyexisting neoliberalism in Glasgow, 1977 to present.Geografiska Annaler Ser B Hum Geog 2008;90:313e25.
107. Gillie O. Scotland’s health deficit: an explanation and a plan.London: Health Research Forum Publishing; 2008.
108. Hypponen E, Power C. Hypovitaminosis D in British adults atage 45y: nationwide cohort study of dietary and lifestylepredictors. Am J Clin Nutr 2007;85:860e8.
109. Howieson S, Hogan M. Multiple deprivation and excesswinter deaths in Scotland. J R Soc Promot Health2005;125:18e22.
110. Bowie N, Jackson G. The raised incidence of winter deaths.Occasional paper no. 7. Edinburgh: General Registrar’s Officefor Scotland; 2002.
111. Foster J. The economic restructuring of the west of Scotland:1945e2000. In: Blazyca G, editor. Restructuring regional andglobal economics: towards a comparative study of Scotland andupper Silesia. Aldershot: Ashgate; 2003.
112. Foster J. TheTwentieth century. In:HoustonR,KnoxW, editors.The new Penguin history of Scotland. London: Penguin; 2001.
113. Barker D, Eriksson J, Forsen T. Fetal origins of adult disease:strength of effects and biological basis. Int J Epidemiol2002;31:1235e9.
114. McDowell I. From risk factors to explanation in publichealth. J Public Health 2008;30:219e23.
115. Coggon D, Martyn C. Time and chance: the stochastic natureof disease causation. Lancet 2005;365:1434e7.
116. McPherson K. Wider ‘causal thinking in the health sciences’.J Epidemiol Commun Health 1998;52:612e8.
117. Thomas B, Dorling D, Smith GD. Inequalities in prematuremortality in Britain: observational study from 1921 to 2007.BMJ 2010;341:c3639.
118. Stuckler D, Basu S, McKee M. Budget crises, health, andsocial welfare programmes. BMJ 2010;340:c3311.
119. Human mortality database: University of California,Berkeley & Max Planck Institute for DemographicResearch. Available at: www.mortality.org [last accessed 4June 2010].





























