Embed Size (px)
Citation preview

Hemophagocytic Syndromes
Brant Ward, MD, PhDAllergy & Immunology

Goals Recognize the diagnostic criteria for HLH
Become familiar with the genetic and mechanistic causes of HLH
Describe the differences between genetic and acquired forms of HLH
Formulate an effective treatment plan

Hemophagocytosis
Pathologic finding of phagocytosis of red blood cells, leukocytes, and thrombocytes by macrophages
Thought to occur after over-activation of macrophages due to dysregulated immune responses

Hemophagocytosis In 1939, Scott & Robb-Smith described patients
with “atypical Hodgkin’s disease” – proliferation of histiocytes affecting all lympho-reticular tissues
Farquhar & Claireaux described a familial syndrome with similar features in 1952
Hallmark clinical features include fever, splenomegaly, and cytopenias; hepatitis, altered mental status, and neurological involvement seen as well
Syndromes characterized by hemophagocytosis are termed ‘hemophagocytic lymphohistiocytsis’ (HLH)

Diagnosis of HLH Diagnostic criteria for HLH were proposed by the
Histiocyte Society in 1991
Five of the eight following criteria must be present to make the diagnosis:
Alternatively, identification of one of the known genetic defects associated with the disease
Ferritin is the most sensitive at discerning HLH from other disorderso Ferritin >10,000 ng/ml is >90% specific for HLH in
children
o Ferritin >50,000 ng/ml is less specific in adults, but still very sensitive
• Fever• Cytopenias in 2 of 3 lineages• Splenomegaly• Hypertriglyceridemia and/or
hypofibrinogenemia• Hemophagocytosis• Low or absent NK cell activity• Hyperferritinemia• Elevated plasma levels of soluble CD25

Causes of HLH
HLH
Perforin deficiency
Munc 13-4 deficiency
Syntaxin 11 deficiency
Munc 18-2 deficiency
Unknown gene
mutations
Immune deficiencies Malignancy
Autoimmune diseases
Viral infections
Bacterial infections
Fungal infections
Helminthic infections
Medications

Subtypes of HLH Genetic HLH
o Disorders characterized by elevated risk for HLH
o Includes Familial Hemophagocytic Lymphohistiocytosis (FHL) as well as certain immunodeficiencies
o Caused by defects in the cell-mediated cytotoxicity pathways
Acquired HLH o A.k.a., Reactive Hemophagocytic Lymphohistiocytosis
(RHL)
o Varied group of disorders that result in hemophagocytic symptoms
o Caused by dysregulated immune responses leading to lymphocyte and macrophage activation

Primary HLH FHL can be divided into 5 subtypes:
o FHL1 – caused by unknown defect on chromosome 9
o FHL2 – caused by deficiency of Perforino FHL3 – caused by deficiency of Munc 13-4o FHL4 – caused by deficiency of Syntaxin 11o FHL5 – caused by deficiency of Munc 18-2
Chediak-Higashi & Griscelli II syndromes are characterized by partial albinism and immune deficiency
XLP is characterized by massive lymphoproliferation and immune deficiency

FHL Sometimes referred to as Farquhar’s disease after
its describer (1952)
Autosomal recessive inheritance with estimated incidence of 1:50,000 live births (male > female)
Symptoms are usually evident by 1 year (70-80% of case) and can even present at birth or in utero
Some forms can present in later childhood or even as adults
Overwhelming HLH is the primary symptom, and deficient NK cell-mediated cytotoxicity is characteristic

FHL1 Identified from four consanginous families of
Pakistani descent using homozygosity mapping
First defined susceptibility locus for FHL, located at 9q21.3-22
This locus contains hundreds of candidate genes, though none have been identified as the culprit

FHL2 Perforin (PRF1) was the first
identified gene causing FHL
>70 different mutations have been identified
Trp374 stop has high incidence in Turkish families
L364 frame-shift is found in Japanese families
L17 frameshift found in families of African origin
Stepp, et al. Science. 1999 Dec 3;286(5446):1957-9.

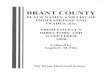
Perforin Protein found in lytic granules of NK cells and
cytotoxic T lymphocytes
Contains MACPF domain that shares a high degree of homology with complement proteins C6-9
Oligomerizes within the membrane of target cell, forming a channel in the membrane
Perforin alone is sufficient to lyse target cells at high (i.e., non-physiologic) concentrations
Perforin channels allow entry of granzymes from the immune synapse into the target cell cytoplasm

MACPF Structure & Function
Kondos, et al. Tissue Antigens. 2010 Nov;76(5):341-51.

FHL3 Due to mutations in Munc
13-4
Identified from 7 affected families (6 consanguinous)
Munc 13-4 defiency accounts for 30-35% of cases
Together with perforin gene mutations, cause up to 70% of FHL cases
Feldmann, et al. Cell. 2003 Nov 14;115(4):461-73.

Munc 13-4 Member of the Munc 13-UNC 13 family of proteins
Many expressed at the neurological synapse, acting as priming factors for synaptic vesicle secretion
Deficiency causes impaired release of cytotoxic granules from cells, but no affect on interferon- secretion
Munc 13-4 is required for priming of lytic granules that are docked at the plasma membrane
Goblet cells in lung epithelium express high levels of Munc 13-4, but deficiency causes no observable lung pathology

FHL4 Mutations in syntaxin
11 characterize FHL4
Identified in a large consanguineous Kurdish family
All identified mutations in are null mutations
Syntaxin mutations account for ~20% of FHL cases in Turkish and Kurdish populations
zur Stadt, et al. Hum Mol Genet. 2005 Mar 15;14(6):827-34.

Syntaxin 11 Soluble N-ethylmaleimide sensitive factor
attachment protein receptor (SNARE) family member
Phylogenetically related to the target membrane SNARE (t-SNARE) proteins syntaxin 1-4
Selective pairing of t-SNARE, v-SNARE, and adaptor proteins form a stable parallel four helical bundle
Deficiencies cause defects in NK cell, but not CTL, cytotoxic activity, which is partially rescued by IL-2
FHL4 phenotype does not differ from that of FHL 2 or 3

FHL5 Results from deficiency
of Munc 18-2
Identified in patients of African, Arabian, Turkish, and European descent
Phenotype appears to correlate with genotype based on age of onset and severity of disease
Cote, et al. J Clin Invest. 2009 Dec;119(12):3765-73.

Munc 18-2 Also called syntaxin-binding-protein-2 (STXBP2)
Member of SM family of fusion accessory proteins —complimentary role with SNAREs in membrane fusion
Syntaxin 11 expression is impaired in Munc 18-2 deficient cells , suggesting a requirement for Munc18-2
From data on Munc 18-1, Munc 18-2/syntaxin 11 complex regulates docking and initiation of SNARE complex formation

Chediak-Higashi Syndrome
Pigmentary dilution, HLH, defective NK, T cell, & neutrophil function
HLH typically occurs later than in FHL (2-10 years)
Light complexion, silvery hair, and characteristic peripheral nerve disease
Infections are common, due to inability to kill organisms after phagocytosis
Reddy, et al. Int J Trichology. 2011 Jul;3(2):107-11.

LYST Caused by mutation in CHSI/LYST, a ubiquitously-
expressed protein
Function of LYST has been inferred from studies of other BEACH family proteins
May regulate sorting of endosomal proteins into lysosomes or regulate fusion or fission events of lysosomes
Striking feature is the occurrence of giant intra-cytoplasmic lysosomal structures in all granulated cells, with lack of degranulation upon stimulus

Griscelli Syndrome Type 2
Pigmentary dilution, HLH, and pyogenic infections
Onset of HLH is later than in FHL (median age 3 years)
Patients have silvery hair and light skin
NK cells and CTLs show impaired degranulation

Rab27a Caused by mutations in the gene encoding
Rab27a, a ubiquitously expressed small GTPase
Enriched on endosomal structures that fuse with cytotoxic granules before release of their contents
Deficiency renders cytotoxic granules unable to reach the immune synapse to dock with the plasma membrane
Interacts with Munc 13-4 to coordinate the final step of the exocytic process, between docking and priming of the granule

XLP X-linked lymphoproliferative disorder—
characterized by hypogammaglobulinemia or lymphoproliferation
Caused by mutations in SLAM-associated protein (SAP) or X-linked inhibitor of apoptosis (XIAP)
Epstein-Barr virus infection results in fulminant and fatal mononucleosis
HLH is almost always associated with EBV infection
SAP deficiency results in a partial cytotoxic defect; no observable cytotoxic defect in XIAP deficiency

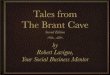
Granule Formation and Function
Vesicle Maturation
(LYST)
Vesicle Docking(Rab27a)
Vesicle Priming(Munc 13-4)
Vesicle Fusion(Syntaxin 11/Munc
18-2)
Effector Function(Perforin)

Models of Pathogenesis
APC
Virus-infected Cells
CTL
IFN-

Models of Pathogenesis
APC
Virus-infected Cells
CTL
IFN-
CTL

Impaired DC Deletion Perforin deficient mice with HLH have normal
total amount of dendritic cells, but…
Terrell & Jordan. Blood. 2013 Jun 27;121(26):5184-91.

Role of Interferon
Jordan, et al. Blood. 2004 Aug 1;104(3):735-43.

Role of CTLs in HLH
Jordan, et al. Blood. 2004 Aug 1;104(3):735-43.

Cytokine Storm The cytokines production and immune activation
triggered by these cells is thought to cause the observed symptomso Fever is induced by overproduction of IL-1o Pancytopenia is a consequence of TNF and IFNo Activated macrophages actively secrete ferritino Macrophages also secrete plasminogen activator,
leading to consumption of plasma fibrinogeno Activated lymphocytes secrete soluble CD25 and
infiltrate the liver and central nervous systemo Proliferation of macrophages expressing CD163 in
marrow and lymphoid tissue leads to hemophagocytosis

Cytokine Storm
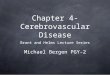
Spectrum of Cytokine-Induced Disease
Normal respons
e to infxn
SIRS
Severe
sepsis
Macrophage
activation syndrome
Acquired HLH
Genetic HLH

Role of Macrophages in HLH
Schaer, et al. Eur J Haematol. 2006 Nov;77(5):432-6.

Macrophage Activation Syndrome
First description of the disorder may have been as early as 1970s
‘Macrophage activation syndrome’ (MAS) first used in 1992 by Albert, et al.
MAS occurs in both children and adults with autoimmune syndromes
Characterized by cytopenias, organ dysfunction, coagulopathy, and inappropriate activation of macrophages in a proinflammatory milieu

MAS and Autoimmunity
MAS can be associated with a wide variety of autoimmune diseases
Strongest associations is with systemic juvenile idiopathic arthritis (sJIA), with estimated clinically apparent MAS in 7-13% of subjects
Subclinical bone marrow evidence of MAS in >50% of sJIA patients
However, MAS also occurs with SLE and adult-onset Still’s disease, along with multiple other diseases

MAS and AutoimmunityAutoimmune Diseases Associated with
MAS
Adult-onset Still’s disease
Ankylosing spondylitis
Dermatomyositis
Enthesitis-related arthritis
Inflammatory bowel disease
Kawasaki disease
Polyarticular JIA
Sarcoidosis
Systemic JIA
Systemic lupus erythematosus
Unidentified autoimmune disease

Diagnosis of MAS sJIA and other autoimmune conditions are
associated with fevers, anemia, hepatosplenomegaly, lymphadenopathy, and elevated serum ferritin
Ravelli, et al., defined a set of criteria for the diagnosis of MAS in patients with sJIA
A number of characteristic findings on routine studies were also identified
Subsequent investigation demonstrated that the criteria do not always apply to MAS in other autoimmune conditions

Diagnosis of MASLaboratory Criteria Value
Thrombocytopenia ≤ 262 x 106/l
Elevation in AST > 59 U/L
Leukocytosis ≤ 4.0 x 106/l
Hypofibrinogenemia ≤ 250 mg/dL
Clinical Criteria Manifestation
CNS dysfunction
IrritabilityHeadacheLethargy
DisorientationSeizures
Coma
HemorrhagesEcchymoses
PurpuraMucosal bleeding
Hepatomegaly≥ 3 cm below costal
margin
Diagnosis requires:
>2 Laboratory criteria>2 Lab + Clinical criteria
Addition of ferritin >500 ng/ml may better discriminate MAS vs systemic infection.
Adapted from: Davi, et al. Arthritis Rheumatol. 2014 Oct;66(10):2871-80.

Infection and HLH In 1979, Risdall, et al., described 19 patients with
evidence of HLH and viral infection after transplantation
Later, it was shown that most patients had no evidence of immune system dysfunction before developing RHL
‘Virus associated hemophagocytic syndrome’ was used to denote any case of HLH without a genetic cause
Eventually, bacteria, fungi, and even protozoa were shown to trigger RHL, leading to the term ‘infection associated hemophagocytic syndrome’ (IAHS)

Infection and HLH
Infections Associated with HLHEpstein-Barr virus Escherichia coli
Cytomegalovirus Salmonella sp.
Varicella virus Enterococcus sp.
HHV6 Mycoplasma sp.
Parvovirus B19 Tick-born bacteria
Hepatitis A Tuberculosis
HIV Visceral leishmaniasis
Adenovirus Plasmodium sp.
Influenza Toxoplasma sp.
Coxsackievirus Pneumocystis jiroveci
Torovirus Candida sp.

EBV and HLH EBV is the most common infectious trigger of
RHL, accounting for 74% of viral triggers in one study
EBV carries the worst prognosis among viral triggers, with 73% mortality in one case series (before HLH ’04)
Incidence is highest in east Asians countries, possibly due to more-virulent endemic strain
Rarely detected in B-cell lymphoma-associated RHL; present in 80% with T/NK cell lymphoma-triggered RHL
Mortality was found to be 14x higher in EBV-associated RHL patients who did not receive etoposide

Medication-Induced HLH
Medications Associated with HLH
Aspirin Morniflumate
NSAIDs Methotrexate
Sulfasalazine Infliximab
Etanercept Penicillamine
Anakinra Vancomycin
Gold salts Parenteral lipids
Autologous stem cell transplantation

HScore for Diagnosing RHL
Included Parameters
Known underlying immunosuppression
Temperature
Organomegaly
No. of cytopenias
Ferritin
Triglycerides
Fibrinogen
AST
Hemophagocytosis on BM biopsy
Freely available at:http://saintantoine.aphp.fr/score/
Fardet, et al. Arthritis Rheumatol. 2014 Sep;66(9):2613-20.

FHL/RHL Overlap Adult-onset HLH has been associated with
homozygous and heterzygous mutations in multiple FHL genes
Striking number variants of FHL-associated genes have been identified in MAS patients
Current recommendation is to perform genetic analyses on ALL patients suspected or confirmed to have HLH
Kaufman, et al. Arthritis Rheumatol. 2014 Dec;66(12):3486-95.

Treatment of HLHFinally!

Treatment of HLH Immediate aim is to suppress over-whelming
inflammation and immune activation; many different agents have been tried
In 1991, the Histiocyte Society developed the HLH 94 treatment protocol, improving survival in pediatric populations from ~25% to 51-55%
In 2002, Henter, et al., showed an overall survival rate of 80% in patients that underwent HSCT
Histiocyte Society updated the treatment protocol in 2004, including new treatments such as HSCT

Stratified Treatment Guidelines

HLH 2004 Protocol
Systemic Therapy
Dexamethasone
Etoposide Cyclosporine
Week 1 10 mg/m2 daily 150 mg/m2 IV biw
3 mg/kg bid
Week 2 10 mg/m2 daily 150 mg/m2 IV biw
To Trough 200 g/L
Week 3 5 mg/m2 daily 150 mg/m2 IV qwk
To Trough 200 g/L
Week 4 5 mg/m2 daily 150 mg/m2 IV qwk
To Trough 200 g/L
Week 5 2.5 mg/m2 daily 150 mg/m2 IV qwk
To Trough 200 g/L
Week 6 2.5 mg/m2 daily 150 mg/m2 IV qwk
To Trough 200 g/L
Week 7 1.25 mg/m2 daily 150 mg/m2 IV qwk
To Trough 200 g/L
Week 8 Taper and d/c 150 mg/m2 IV qwk
To Trough 200 g/L

RHL/MAS Treatment Applicability of HLH 04 protocol to RHL syndromes
(e.g., MAS) and to adult populations is not been established
Mutliple groups support a graded-approach, with corticosteroids alone as initial treatment
Initial Therapy
High-dose corticosteroids (prednisolone 30 mg/kg x3 days)
Elimination of suspected triggers, infection control
Aggressive supportive measures
Secondary Therapy
Intravenous immunoglobulin (1-3 g/kg)
Cyclosporine A, etoposide

MAS Treatment Options
Proposed Treatments for Autoimmune-Associated HLH
Cyclosporine A Plasmaphoresis
Etanercept Abatacept
Anakinra Antithymocyte globulin
Intravenous immunoglobulin Corticosteroids
Etoposide Naproxen
Splenectomy

Treatment Notes Several series suggest outcomes are poor in RHL if
infection control measures are used alone
RHL triggered by leishmaniasis may be treated solely with amphotericin
Etoposide is crucial for EBV-associated RHL — inhibits activated T cells, plus EBV NA in infected cells
Multiple groups agree that HLH 2004 should be initiated for relapses of RHL, despite etiology
HSCT has best overall outcome among all single treatment modalities across all patient populations

Summary HLH is a clinical syndrome of overwhelming
immune activation and cytokine production
Cytokine storm in HLH occurs due to failure to clear antigen presenting cells and/or activated T cells
Genetic variants may predispose patients to HLH at any age
Treatment is aimed at controlling the inflammatory cytokine cascade, and may require BMT in severe cases