Embed Size (px)
Citation preview

Postgrad MedJ7 1998;74:733-736 C The Fellowship of Postgraduate Medicine, 1998
Oesophageal subepithelial fibrosis: an extension oforal submucosal fibrosis
S P Misra, Vatsala Misra, Manisha Dwivedi, S C Gupta
MLN Medical College,Allahabad 211 01, IndiaDepartment ofGastroenterologyS P MisraM DwivediDepartment ofPathologyV MisraDepartment ofOtorhinolaryngologyS C Gupta
Accepted 30 June 1998
SummaryFifty-five patients with oral submucosalfibrosis and an equal number of patientswith no evidence of the disease were stud-ied. All patients underwent upper gastro-intestinal endoscopy and any abnormalitywas noted. Multiple oesophageal biopsieswere obtained from the upper end of theoesophagus and from any endoscopicallyobserved abnormality. The histologicalchanges in the two groups were assessedblindly by an experienced histopatholo-gist. Histological abnormalities werenoted in the oesophageal mucosa in 2% ofcontrols and 66% of patients with oralsubmucosal fibrosis (p < 0.0001). In thecontrol group, acanthosis was seen in onepatient, while in the patient group atrophyofthe squamous epithelium was evident in52%, hyperkeratosis in 52%, parakeratosisin 30%, dyskeratosis in 14%, acanthosis in14%, and papillomatosis and mild dyspla-sia in 2% patients. Subepithelial collageni-zation was seen in 32 (64%) patients. Theoesophageal abnormalities were seenmore frequently in patients who hadconsumed Pan masala, Gutka, betel nut,tobacco or a combination ofsome or all ofthese, with or without betel leaf, for > 5years compared to those consuming themfor a shorter period of time (91% vs 46%,p< 0.001). It is concluded that oral submu-cosal fibrosis is not a disease confined tothe oral cavity; the oesophagus may alsobe involved in about two-thirds of pa-tients.
Keywords: oral submucosal fibrosis; oesophagealsubepithelial fibrosis; betel; Indians; chewing tobacco
Oral submucosal fibrosis (OSMF) is a chronicirreversible disease of unknown aetiology. It ismainly found in Indians' 2 and affects about0.2-1.2% of the urban population attendingdental clinics in India.`5 It has also been seenamong Indians living in Kenya, Malaysia,Uganda, South Africa, Fiji and the UK,'10 andcases have been reported from ethnic groups inTaiwan, Nepal, Thailand, Vietnam and SriLanka.""`13 The disease leads to fibro-elastictransformation of the lamina propria andepithelial atrophy of the oral mucosa. Later, theoral mucous membrane becomes stiff, leadingto trismus. Although the aetiology is notknown, it has been postulated that the diseaseis caused by irritation of the oral submucosa by
irritants such as capsaicin in chillies andtannins in betel nuts.'" 14 Genetic and environ-mental factors have also been blamed for thedisease.'5 As the name denotes, the diseasemostly affects the oral mucosa and, althoughinvolvement of the oesophageal mucosa hasoccasionally been reported,' there is a paucityof reports describing oesophageal involvement.This study was set up to study the prevalence ofoesophageal disease in patients with OSMF.
Materials and methods
The study group consisted of 55 patients withOSMF and 55 other patients with no evidenceof OSMF who were undergoing upper gastro-intestinal endoscopy. Patients with oesophagealdisease (eg, gastro-oesophageal reflux disease,carcinoma of the oesophagus, oesophagealstricture or oesophageal varices) were ex-cluded. The diagnosis of OSMF was made onclinical grounds and buccal biopsy in 36patients and on clinical grounds alone in theremaining 19 patients. OSMF was clinicallyclassified as severe if the patient could not openhis mouth to accommodate a paediatricmouthguard with an outer diameter of 20 mm,during upper gastrointestinal endoscopy.A detailed clinical history was obtained,
including the duration of the disease andsymptoms, and information on any sub-stance(s) chewed and the duration of con-sumption. Thereafter, all subjects underwentupper gastrointestinal endoscopy with aforward-viewing endoscope (Olympus modelXQ 20 or XP 20, Olympus Optical Corpora-tion, Tokyo). A specially designed mouthguardwas used in patients who could not open theirmouth fully for even a paediatric mouthguardto be inserted.'6 A careful search was made forany abnormality during endoscopy, especiallyin the oesophagus. Multiple oesophageal biop-sies were obtained from any abnormalitynoticed during endoscopy, and in all cases fromthe upper end ofthe oesophagus, just below theupper oesophageal sphincter. All biopsies werefixed in 10% formalin and sent for histopatho-logical examination.
After routine processing, 3-5 ,um sectionswere cut from paraffin wax embedded sections,stained with haematoxylin and eosin, andevaluated by a histopathologist who wasunaware of the clinical diagnosis or endoscopicfindings. The sections were examined forhistological changes. In the epithelium, evi-dence of atrophy of the lining squamousepithelium, hyperkeratosis, parakeratosis,
on April 23, 2020 by guest. P
rotected by copyright.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.74.878.733 on 1 Decem
ber 1998. Dow
nloaded from
734 Misra, Misra, Dwivedi, et al
dyskeratosis, acanthosis, papillomatosis anddysplasia was sought. In the subepithelialtissue, evidence of collagenization was sought,which was subjectively graded as mild or severeby the histopathologist. Oesophageal biopsieswhich were superficial and did not containsubepithelial tissue were not evaluated.
STATISTICSThe two groups were compared by theStudent's t-test, X'-test with or without Yates'correction and the Fischer's exact test.
Results
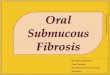
CONTROLSThe mean age of the controls was 31.2 ± 11.8years; 45/55 were males. None ofthese subjectsshowed any oesophageal abnormality on en-doscopy. Oesophageal biopsies were too super-ficial for proper interpretation in six subjectsand were discarded. Of the other 49 subjects,oesophageal biopsy from one subject showedevidence of acanthosis in the epithelial tissue.There was, however, no evidence of collageni-zation of the lamina propria. No histologicabnormality was seen in the oesophageal biop-sies from the other 48 subjects (figure 1).
PATIENTSThe mean age of this group was 29.4 ± 10.6years; 47/55 were males. The age and sex ratiowere not significantly different from the controlgroup. One patient was asymptomatic and wasfound to have OSMF accidentally when hecould not open his mouth fully duringendoscopic examination to detect the cause ofmelaena. All patients except one chewed eitherPan masala, Gutka, betel nut, tobacco or acombination of some or all of these, with orwithout betel leaf. All 54 of these patients con-sumed betel nut in one form or another. Onlytwo patients smoked cigarettes. The offendingsubstance had been chewed for a mean ± SD of6.2 ± 6.4 years (range 0.5-25). One 25-year-old man with a history of inability to open hismouth fully for the last year denied the use ofany offending agent. This was corroborated byhis parents and siblings. The mean ± SD dura-tion of symptoms in the patients was 18 ± 32.8months (range 0.5-168).
All patients had difficulty in opening theirmouths. It was clinically severe in 23 (42%)patients in whom a specially designed mouth-guard had to be used for upper gastrointestinalendoscopy. Thirty-nine (71%) complained ofburning sensations in the mouth while eatinghighly seasoned food and 21(38%) patientshad ulcers in their mouth. Oesophageal symp-toms were noted in seven (13%) patients. Dys-phagia was reported by four (7%) patients andodynophagia by two patients. One patient hadboth dysphagia and odynophagia. Loss of tastesensation was noticed by two patients andoccasional bleeding from the cheek by onepatient.None of the patients showed any abnormal-
ity during upper gastrointestinal endoscopy.Oesophageal biopsies were too superficial forproper interpretation in five (9%) patients. Of
R-:
zI
-. F.
- ~~~~~~s |!:::,.. ..: ...a
Figure 1 Oesophageal biopsy from a control subject.Note the normal lamina propria (H&E, orig x 80)
.... ...S, ....... ...s..s'[email protected]*. 4t ..i.w iii- ^ :. s. ..^
.........
VM
ii .i8
WS:H'S' rt;; .Yls
',, OFt
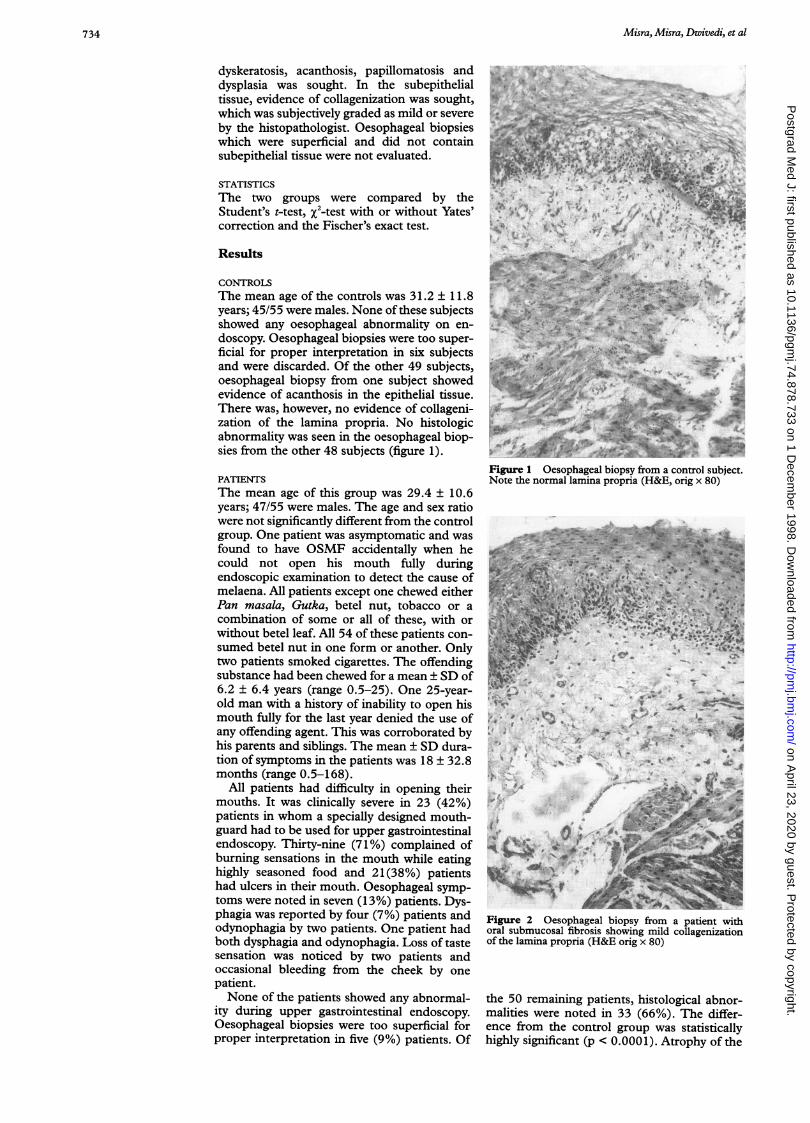
Figure 2 Oesophageal biopsy from a patient withoral submucosal fibrosis showing mild collagenizationof the lamina propria (H&E orig x 80)
the 50 remaining patients, histological abnor-malities were noted in 33 (66%). The differ-ence from the control group was statisticallyhighly significant (p < 0.0001). Atrophy of the
on April 23, 2020 by guest. P
rotected by copyright.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.74.878.733 on 1 Decem
ber 1998. Dow
nloaded from

Oesophageal subepithelialfibrosis 735
Figure 3 Severe collagenization of the laminapropria in a patient with oral submucosal fibrosis(H&E orig x 80)
squamous epithelium was evident in 26 (52%),hyperkeratosis in 26 (52%), parakeratosis in 15(30%), dyskeratosis in 7(14%) and acanthosisin seven (14%) patients. Papillomatosis andmild dysplasia were evident in one (2%) patienteach. Subepithelial collagenization was seen in32 (64%) patients; it was mild in 15 (30%)(figure 2) and severe in 17 (34%) patients (fig-ure 3).
Histological abnormalities in the oesopha-geal biopsies were seen in 13 of 28 (46%)patients with a history of consuming one ormore of the offending agents listed above for <5 years compared to 20 of 22 (91%) consum-ing them for > 5 years. The difference betweenthe two groups was statistically highly signifi-cant (p < 0.001). Histological abnormalitieswere seen in 14 of 20 (70%) patients withclinically severe OSMF compared to 19 of 30(63%) patients with clinically milder disease.The difference between these two groups wasnot statistically significant. Of the sevenpatients with oesophageal symptoms, six hadhistologically severe collagenization (figure 3),and five had been consuming the offendingagent(s) for ¢ 5 years. The other two had con-sumed the offending agents for 2 and 3 years,respectively. The patient with idiopathicOSMF did not have any histologic abnormalityin his oesophageal biopsy.
Discussion
Oral submucosal fibrosis is not an uncommoncondition in Indian subjects consuming betelnut, tobacco, Pan masala and Gutka, with orwithout betel leaf. The disease is also commonin expatriates from the Indian subcontinent inthe developed countries, especially in the UKwhere it has been reported from London andother cities.6'0 It has been estimated that in thecity of Leicester one may find as many as 3000cases of OSMF. In a study from Durban, witha large (46%) Indian population, a prevalenceof 3.4% has been reported.'7 The importanceof the disease lies in the fact that it is a prevent-able precancerous condition of the oral cavitywhich leads to substantial morbidity especiallyin the younger population.While OSMF is predominantly a disease of
the oral cavity, fibrosis is also known to extendinto the pharynx via the pillars and down to the
pyriform fossa. It appears logical that theoesophagus should also be involved because atleast some of the material which is chewed orkept in the mouth will go down the oesoph-agus, leading to irritation of the oesophagealmucosa, which is similar to that of the oral cav-ity. However, although involvement of theoesophagus has been reported,' there are noconfirmatory reports to substantiate this. AMEDLINE search revealed only one article onthe subject.'8 In this study by Maher et al, onlythe endoscopic appearance of the oesophagealmucosa was evaluated because the oesophagealbiopsies obtained were too superficial in natureto be of any value. The authors noted that themucosa was whitish pale in two of the 30patients studied, stiff and fibrotic in 19,leathery in four, and firm or gritty in anothertwo cases.
In the present study, we were unable to findany endoscopic abnormality in our OSMFpatients. However, histologically, oesophagealinvolvement could be demonstrated in abouttwo-thirds of patients with OSMF. In themajority of cases the disease in the oesophaguswas clinically not apparent and oesophagealsymptoms were seen in only seven of the 50(14%) patients. Of interest was the finding thatsix out of these seven patients had severe col-lagenization of the lamina propria of theoesophagus.
Oesophageal subepithelial fibrosis was morecommon in patients who had consumed betelnut, tobacco, Pan masala or Gutka, with orwithout betel leaf, for a longer period.However, 46% of patients had developed thedisease after consuming the offending agent(s)for less than 5 years. It therefore appears that,although the chances of developing oesopha-geal subepithelial fibrosis are high if one of theoffending agents are chewed on a long-termbasis, even a period of usage as short as a yearmay be sufficient to cause this condition. Thiswas also evident in a small group of sevenpatients who had symptoms of dysphagia andodynophagia along with oesophageal subepi-thelial fibrosis.One of the patients with OSMF denied
consuming any of the known offending agents,which was confirmed by his parents and siblings.There was however, no oesophageal involve-ment in this patient. Such idiopathic cases ofOSMF are known to occur rarely, but themajority of cases occur in people who consumethe above-mentioned offending agents.The implications of oesophageal involve-
ment in patients with OSMF may havefar-reaching implications. It is possible that, inat least some of these patients, the lesion willdevelop into frank carcinoma of the upperoesophagus, as it is well known that OSMF is apremalignant disease.'"Although oesophageal subepithelial fibrosis
has not been reported earlier in patients withOSMF, ultrastructural abnormalities such asdiscontinuous, fragmented basement mem-brane, with reduction of hemidesmosomes,and widened intracellular spaces, have beennoted in the oesophageal mucosa of chronictobacco chewers.20 With the changes seen on
on April 23, 2020 by guest. P
rotected by copyright.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.74.878.733 on 1 Decem
ber 1998. Dow
nloaded from

736 Misra, Misra, Dwivedi, et al
light microscopy in about two-thirds ofpatientswith OSMF, the definition ofOSMF should bemodified to include the involvement of theoesophagus.While banning tobacco, betel nut, betel,
Panmasala and Gutka is the key to preventionof the disease, this may not be possible in the
developing countries because of the lack ofpolitical will. However, in the UK, where alarge number of immigrants from the Indiansubcontinent reside, a blanket ban on import ofsuch articles would go a long way in preventingthis precancerous but potentially preventabledisease.
1 Jayanthi V, Probert CSJ, Sher KS, Mayberry JF. Oralsubmucosal fibrosis - a preventable disease. Gut 1992;33:4-6.
2 Pathak AG. Oral submucous fibrosis. Natl Med J India1993;3:249-50.
3 Pindborg JJ, Mehta FS, Gupta PC, Dattary DK. Prevalenceof oral submucous fibrosis among 50915 Indian villagers. BrJf Cancer 1968;22:646-54.
4 Pindborg JJ, Kalapessi HK, Kale S, Singh B, TalyerkhanBN. Frequency of oral leukoplakia and related conditionsamong 10,000 Bombayites: preliminary report. Jf All IndiaDent Assoc 1965;37:228-9.
5 Zachariah J, Mathew B, Varma NAR, Iqbal AM, PindborgJJ. Frequency of oral mucosal lesions among 5000 individu-als in Trivandrum, South India. Jf All India Dental Assoc1966;38:290-6.
6 Kennedy TF, MacDonald DG. Oral submucous fibrosis. Acase report. Br DentJ 1968;124:121-4.
7 Moos KF, Madan DK. Submucous fibrosis. BrDentj 1968;125:313-7.
8 McGurk M, Craig GT. Oral submucous fibrosis: two casesof malignant transformation in Asian immigrants to theUnited Kingdom. BrJ Oral Max Surg 1984;22:56-64.
9 Foster BA. Oral submucous fibrosis: a cause for concern. BrDentJ 1986;160:378.
10 CaniffJP, Harvey W, Harris M. Oral submucous fibrosis: itspathogenesis and management. Br DentJ 1986;160:429-34.
11 Su JP. Idiopathic scleroderma of the mouth. Report of threecases. Arch Otolaryngol 1954;59:331-2.
12 Pindborg JJ, Sirsat MS. Oral submucous fibrosis. Oral Surg1966;22:764-79.
13 Shiaw YY, Kwan HW. Submucous fibrosis in Taiwan. OralSurg 1979;47:453-7.
14 Seedat HA, Van Wyk CW. Betel nut chewing and dietaryhabits of chewers with and without submucous fibrosis andwith concomitant oral cancer. S Aft Med J 1988;74:572-5.
15 Lemmer J, Shear M. Oral submucosal fibrosis: A possiblecase in a person of Caucasian descent. Br Dent Surg1967;122:343-6.
16 Misra SP, Dwivedi M. A mouthguard for endoscopic exam-ination of patients with oral submucus fibrosis and ankylosisof the temporomandibular joint. Endoscopy 1998;30:S37.
17 Seedat HA, Van Wyk CW Betel nut chewing andsubmucous fibrosis in Durban. S Aft Med Jf 1988;74:568-71.
18 Maher R, Ahmed W, Qureshi H, Zuberi SJ, Syed S.Oesophageal changes in oral submucous fibrosis usingfibreoptic endoscopy - a pilot study. J Pakistan Med Assoc1991;41:312-3.
19 Pindborg JJ, Murthy PR, Bhonsle RB, Gupta PC, DaftaryDK, Mehta FS. Oral submucous fibrosis as a precancerouscondition. ScandJ3 Dent Res 1984;92:224-9.
20 Shankaran K, Kandarkar SV, Contractor QQ, Kalro RH,Desai HG. Ultrastructural changes in oesophageal mucosaof chronic tobacco chewers. Indian J Med Res 1993; 98:15-9.
on April 23, 2020 by guest. P
rotected by copyright.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.74.878.733 on 1 Decem
ber 1998. Dow
nloaded from