Embed Size (px)
Citation preview
“2016 CMS Quality Audit-Gaps in Care”
November 2016
©2011 Proprietary and Confidential
ACO Announcements
• Reminders:
– ACO Notifications
– Requests for Tax ID information from PECOS
• 2016 ACO Patient lists
• Save the date: Annual Meeting January 25th 2017
2
©2011 Proprietary and Confidential
Agenda
• How quality is measured for the ACO by CMS
• 2016 ACO Gap in Care Measures
• CMP data collection
• Q&A section
3

©2011 Proprietary and Confidential
• 34 quality measures are separated into the following four key domains
1. Patient/Caregiver Experience
2. Care Coordination/Patient Safety
3. Preventive Health
4. Clinical Care for At Risk Population
Quality Measurement: Domains
4
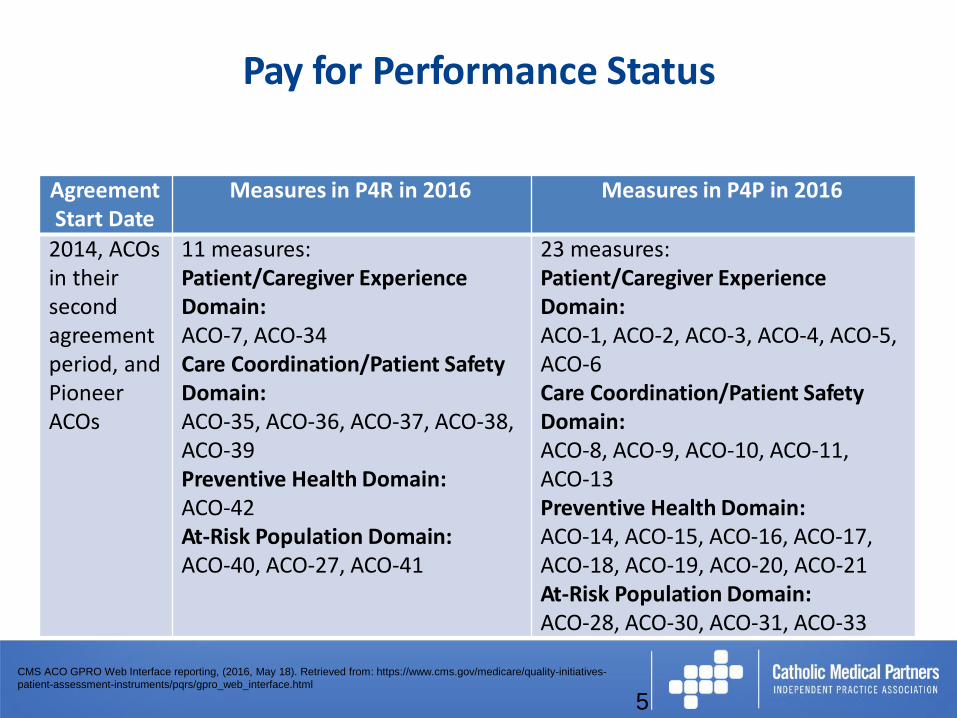
Pay for Performance Status
5
Agreement Start Date
Measures in P4R in 2016 Measures in P4P in 2016
2014, ACOsin their second agreement period, and Pioneer ACOs
11 measures: Patient/Caregiver Experience Domain:ACO-7, ACO-34Care Coordination/Patient Safety Domain:ACO-35, ACO-36, ACO-37, ACO-38, ACO-39Preventive Health Domain:ACO-42At-Risk Population Domain:ACO-40, ACO-27, ACO-41
23 measures: Patient/Caregiver Experience Domain:ACO-1, ACO-2, ACO-3, ACO-4, ACO-5, ACO-6Care Coordination/Patient Safety Domain:ACO-8, ACO-9, ACO-10, ACO-11, ACO-13Preventive Health Domain:ACO-14, ACO-15, ACO-16, ACO-17,ACO-18, ACO-19, ACO-20, ACO-21At-Risk Population Domain:ACO-28, ACO-30, ACO-31, ACO-33
CMS ACO GPRO Web Interface reporting, (2016, May 18). Retrieved from: https://www.cms.gov/medicare/quality-initiatives-
patient-assessment-instruments/pqrs/gpro_web_interface.html
©2011 Proprietary and Confidential
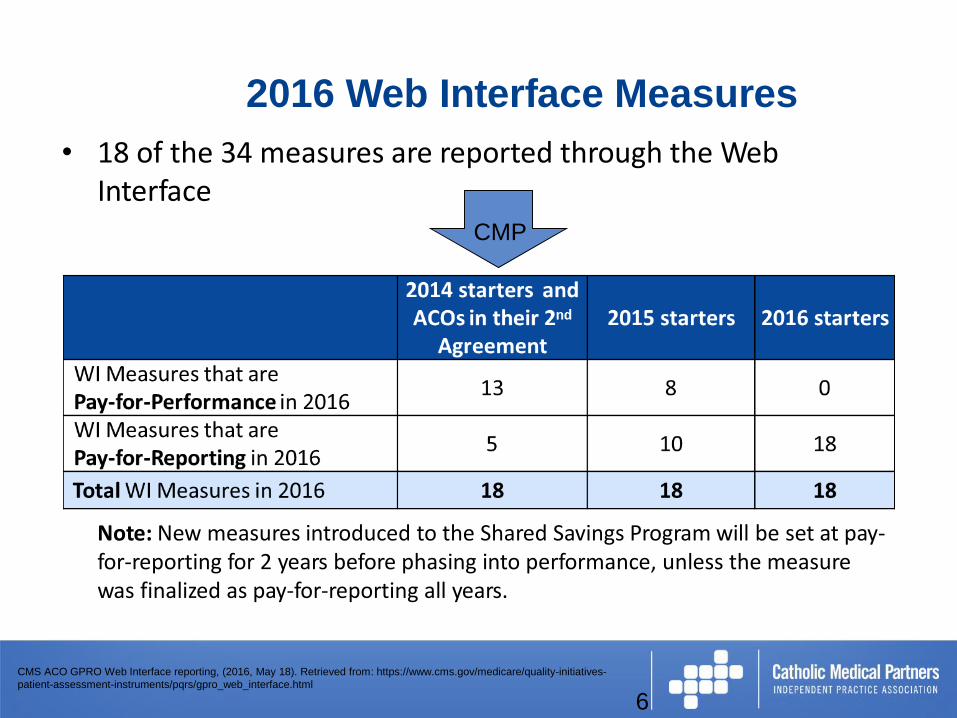
• 18 of the 34 measures are reported through the Web Interface
Note: New measures introduced to the Shared Savings Program will be set at pay-for-reporting for 2 years before phasing into performance, unless the measure was finalized as pay-for-reporting all years.
2016 Web Interface Measures
6
CMS ACO GPRO Web Interface reporting, (2016, May 18). Retrieved from: https://www.cms.gov/medicare/quality-initiatives-
patient-assessment-instruments/pqrs/gpro_web_interface.html
CMP
©2011 Proprietary and Confidential
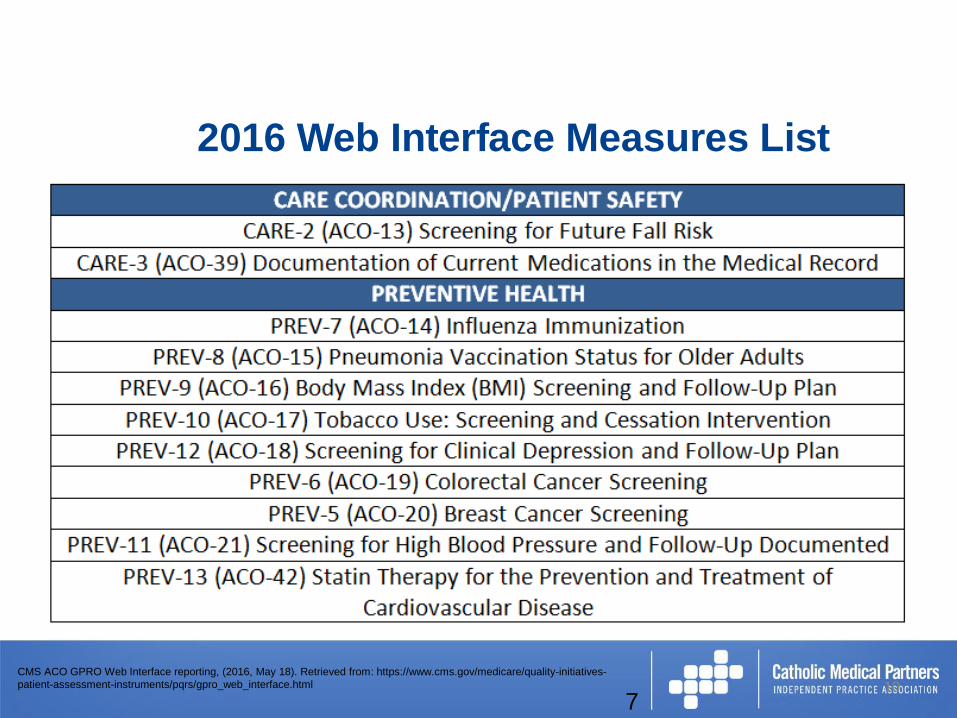
2016 Web Interface Measures List
10CMS ACO GPRO Web Interface reporting, (2016, May 18). Retrieved from: https://www.cms.gov/medicare/quality-initiatives-
patient-assessment-instruments/pqrs/gpro_web_interface.html
7
©2011 Proprietary and Confidential
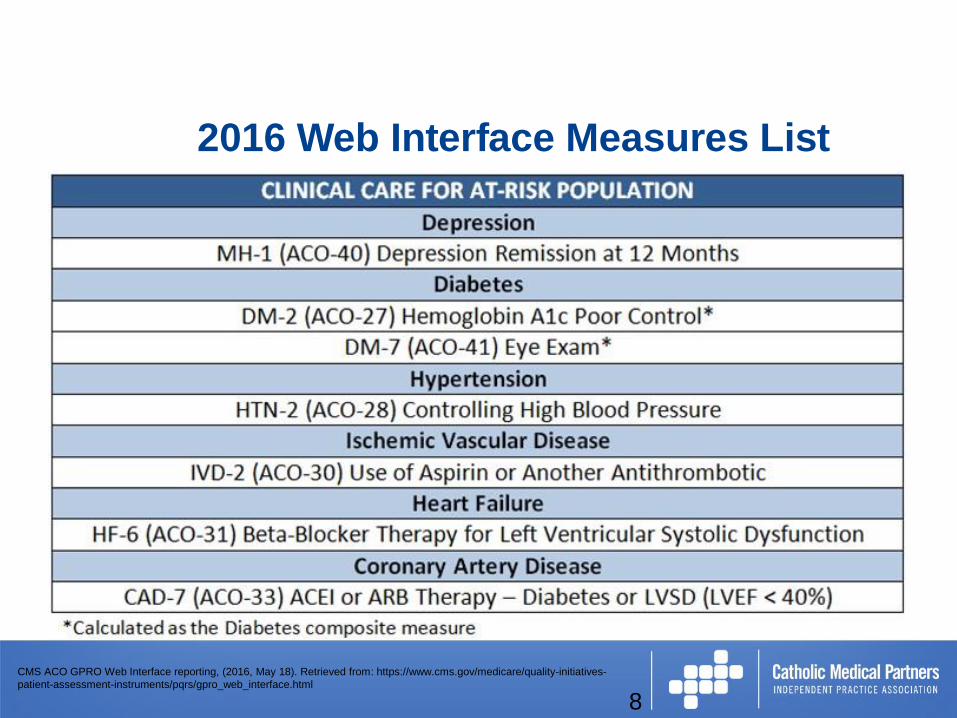
2016 Web Interface Measures List
8
CMS ACO GPRO Web Interface reporting, (2016, May 18). Retrieved from: https://www.cms.gov/medicare/quality-initiatives-
patient-assessment-instruments/pqrs/gpro_web_interface.html

©2011 Proprietary and Confidential
Audit Process
• ~4000 patients included in audit
• CMP team set up lists of patients via our website
• Letters/Email sent to all providers regarding audit
• Practices have approximately 3-4 weeks to complete
• Medical records may be requested to be faxed in
• Corrections may be necessary
• Outreach will include: phone calls and additional emails until the audit time period is complete
©2011 Proprietary and Confidential
Patient Confirmation
Status
• Data from Medicare claims are used to determine if a patient is eligible for quality reporting.
• ACO will remove a patient from all modules, measures and performance calculations based upon various CMS allowed circumstances.
• Example: Group practice 4 providers all using the same EMR is a participant in the ACO. Dr Jones receives review for Dr Smith. Who’s responsibility is it to complete the review? It is the practice responsibility! The review can be completed by either Dr Jones or Dr Smith.
NOTE: Failure to mark the specific reason for removing the patient during Patient Confirmation will result in the patient record remaining incomplete
15CMS ACO GPRO Web Interface reporting, (2016, May 18). Retrieved from: https://www.cms.gov/medicare/quality-initiatives-
patient-assessment-instruments/pqrs/gpro_web_interface.html
9
©2011 Proprietary and Confidential
Gaps in Care Measures
• IVD Use of Aspirin or another Antithrombotic
• Heart Failure- Beta Blocker Therapy for LVSD
• CAD/Diabetes or LVEF<40%- ACE Inhibitor/ARB Therapy for CAD
• Breast Cancer Screening
• Depression Screening
• Falls Risk Screening
©2011 Proprietary and Confidential
IVD-2: Use of Aspirin or Another
Antithrombotic
12
Description:
Percentage of patients 18 years of age and older who were discharged alive for acute myocardial infarction (AMI), coronary artery bypass graft (CABG) or percutaneous coronary interventions (PCI) in the 12 months prior to the measurement period, or who had an active diagnosis of ischemic vascular disease (IVD) during the measurement period, and who had documentation of use of aspirin or another antithrombotic during the measurement period.
Denominator Exclusions: None
What is the Quality Action?
Prescription of aspirin or another antithrombotic.
CMS ACO GPRO Web Interface reporting, (2016, May 18). Retrieved from: https://www.cms.gov/medicare/quality-initiatives-
patient-assessment-instruments/pqrs/gpro_web_interface.html

©2011 Proprietary and Confidential
IVD-2: Use of Aspirin or Another
Antithrombotic
13
Who may perform the Quality Action?
Any eligible professional with prescribing authority may prescribe the use of aspirin or another antithrombotic. In addition to aspirin, antithrombotic medications may include: clopidogrel, a combination of aspirin and extended release dipyridamole, Prasugrel, Ticagrelor, or Ticlopidine.
When must the Quality Action be performed?
The prescription for aspirin or another antithrombotic must be either initiated or continued during the measurement period.
CMS ACO GPRO Web Interface reporting, (2016, May 18). Retrieved from: https://www.cms.gov/medicare/quality-initiatives-
patient-assessment-instruments/pqrs/gpro_web_interface.html

©2011 Proprietary and Confidential
IVD-2: Use of Aspirin or Another
Antithrombotic
14
What are the documentation requirements relative to the Quality Action?
The patient’s medical record must contain:
• An active diagnosis of ischemic vascular disease or discharged alive for AMI, CABG or PCI;
and
• An active prescription for aspirin or another antithrombotic anytime during the measurement period.
CMS ACO GPRO Web Interface reporting, (2016, May 18). Retrieved from: https://www.cms.gov/medicare/quality-initiatives-
patient-assessment-instruments/pqrs/gpro_web_interface.html
©2011 Proprietary and Confidential
HF-6: Beta-Blocker Therapy for LVSD
(LVEF < 40%)
15
Description:
Percentage of patients aged 18 years and older with a diagnosis of heart failure (HF) with a current or prior left ventricular ejection fraction (LVEF)< 40% who were prescribed beta-blocker therapy either within a 12 month period when seen in the outpatient setting OR at each hospital discharge.
Denominator Exclusions: None
What is the Quality Action?
Prescription of beta-blocker therapy. Beta-blocker therapy is limited to the prescription of bisoprolol, carvedilol, or sustained release metoprolol succinate.
CMS ACO GPRO Web Interface reporting, (2016, May 18). Retrieved from: https://www.cms.gov/medicare/quality-initiatives-
patient-assessment-instruments/pqrs/gpro_web_interface.html

©2011 Proprietary and Confidential
HF-6: Beta-Blocker Therapy for LVSD
(LVEF < 40%)
16
Who may perform the Quality Action?
Any eligible professional with prescribing authority may prescribe the beta-blocker therapy.
When must the Quality Action be performed?
The prescription for beta-blocker therapy must be either initiated or continued during the measurement period.
CMS ACO GPRO Web Interface reporting, (2016, May 18). Retrieved from: https://www.cms.gov/medicare/quality-initiatives-
patient-assessment-instruments/pqrs/gpro_web_interface.html
©2011 Proprietary and Confidential
HF-6: Beta-Blocker Therapy for LVSD
(LVEF < 40%)
17
What are the documentation requirements relative to the Quality Action?
The patient’s medical record must contain:
• An active diagnosis of heart failure;
and
• LVEF of < 40% (or documented as moderate or severe) at anytime in the
patient’s history, up through the last day of the measurement period;
and
• An active prescription for beta-blocker therapy anytime during the measurement period
CMS ACO GPRO Web Interface reporting, (2016, May 18). Retrieved from: https://www.cms.gov/medicare/quality-initiatives-
patient-assessment-instruments/pqrs/gpro_web_interface.html
©2011 Proprietary and Confidential
CAD-7: ACE Inhibitor or ARB Therapy –
Diabetes or LVSD (LVEF < 40%)
18
Description:
Percentage of patients aged 18 years and older with a diagnosis of coronary artery disease seen within a 12 month period who also have diabetes OR a current or prior Left Ventricular Ejection Fraction (LVEF) < 40% who were prescribed ACE inhibitor or ARB therapy.
Denominator Exclusions: None
What is the Quality Action?
Prescription of either an ACE inhibitor or ARB therapy.
CMS ACO GPRO Web Interface reporting, (2016, May 18). Retrieved from: https://www.cms.gov/medicare/quality-initiatives-
patient-assessment-instruments/pqrs/gpro_web_interface.html
©2011 Proprietary and Confidential
CAD-7: ACE Inhibitor or ARB Therapy –
Diabetes or LVSD (LVEF <40%)
19
Who may perform the Quality Action?
Any eligible professional with prescribing authority may prescribe ACE inhibitor or ARB therapy.
When must the Quality Action be performed?
The prescription of an ACE inhibitor or ARB therapy must be documented as either initiated or continuing during the measurement period.
CMS ACO GPRO Web Interface reporting, (2016, May 18). Retrieved from: https://www.cms.gov/medicare/quality-initiatives-
patient-assessment-instruments/pqrs/gpro_web_interface.html

©2011 Proprietary and Confidential
CAD-7: ACE Inhibitor or ARB Therapy –
Diabetes or LVSD (LVEF <40%)
What are the documentation requirements relative to the Quality Action?
The patient’s medical record must contain:
• An active diagnosis of coronary artery disease or history of cardiac surgery;
and
• An active diagnosis of diabetes and/or LVEF < 40% (or documentation ofmoderate or severe LVSD) at anytime in their history, up through the lastday of the measurement period;
and
• An active prescription for an ACE inhibitor or ARB therapy anytime during the measurement period.
29CMS ACO GPRO Web Interface reporting, (2016, May 18). Retrieved from: https://www.cms.gov/medicare/quality-initiatives-
patient-assessment-instruments/pqrs/gpro_web_interface.html
19
©2011 Proprietary and Confidential
PREV 5: Breast Cancer Screening
21
Description:
Percentage of women 50 through 74 years of age who had a mammogram to screen for breast cancer within 27 months.
Exclusions: A bilateral mastectomy or two unilateral mastectomies
Exceptions: None
What is the Quality Action?
A mammogram to screen for breast cancer.
Note: 3D mammography, MRI, and ultrasound are not considered breast cancer screening for this measure.
Who may perform the Quality Action?
Any qualified healthcare professional may perform the mammogram.
CMS ACO GPRO Web Interface reporting, (2016, May 18). Retrieved from: https://www.cms.gov/medicare/quality-initiatives-
patient-assessment-instruments/pqrs/gpro_web_interface.html
©2011 Proprietary and Confidential
PREV 5: Breast Cancer Screening
9
When must the Quality Action be performed?
The mammogram must be performed during the measurement period, or 27 months prior to the end of the measurement period (i.e., between October 1, 2014 –December 31, 2016); however, it may not precede the patient’s 50th birthday.
What are the documentation requirements relative to the Quality Action?
The patient’s medical record must contain:
• Date the mammogram was performed and the results
CMS ACO GPRO Web Interface reporting, (2016, May 18). Retrieved from: https://www.cms.gov/medicare/quality-initiatives-
patient-assessment-instruments/pqrs/gpro_web_interface.html
22
1
©2011 Proprietary and Confidential
PREV 12: Depression Screening and
Follow-up Plan
Description:
Percentage of patients aged 12 years and older screened for clinical depression onthe date of the encounter using an age appropriate standardized depression screening tool (that is normalized and validated) AND if positive, a follow-up plan is documented on the date of the positive screen.
Denominator Exclusions: Active diagnosis of depression or bipolar disorder
What is the Quality Action?
Completion of a depression screening using an age appropriate standardized depression screening tool. If the screening is positive, a follow-up plan is also required.
23CMS ACO GPRO Web Interface reporting, (2016, May 18). Retrieved from: https://www.cms.gov/medicare/quality-initiatives-
patient-assessment-instruments/pqrs/gpro_web_interface.html
©2011 Proprietary and Confidential
PREV 12: Depression Screening and
Follow-up Plan
24
A follow-up plan for a positive screen must contain one or more of the following:
• Additional evaluation for depression
• Suicide risk assessment
• Referral to a practitioner who is qualified to diagnose and treat depression
• Pharmacological interventions
• Other interventions or follow-up for the diagnosis or treatment of depression
Who may perform the Quality Action?
A qualified healthcare professional must administer the screening tool.
CMS ACO GPRO Web Interface reporting, (2016, May 18). Retrieved from: https://www.cms.gov/medicare/quality-initiatives-
patient-assessment-instruments/pqrs/gpro_web_interface.html
©2011 Proprietary and Confidential
PREV 12: Depression Screening
and Follow-up Plan
25
When must the Quality Action be performed?
The depression screening must be performed during the measurement period. If a follow-up plan is required, it must be documented on the date of the positive screen.
What are the documentation requirements relative to the Quality Action?
The patient’s medical record must contain:
• The date and results of an age appropriate standardized depression screening tool;
• If a follow-up plan is required, documentation of discussion of the plan. The follow-up plan must be specified as an intervention that pertains to depression;
or
• Documentation of exclusion criteria.
CMS ACO GPRO Web Interface reporting, (2016, May 18). Retrieved from: https://www.cms.gov/medicare/quality-initiatives-
patient-assessment-instruments/pqrs/gpro_web_interface.html
©2011 Proprietary and Confidential
CARE-2: Screening for Future Fall Risk
26
Description:Percentage of patients 65 years of age and older who were screened for future fall risk during the measurement period.
Denominator Exclusions: None
What is the Quality Action?Completion of a fall risk screening. The screening may be done with a formal screening tool as long as it fulfills the fall history documentation requirements.
Who may perform the Quality Action?
Eligible professionals reporting this measure may document measure information received from the patient, authorized representative(s), caregiver(s) or other available healthcare resources .
CMS ACO GPRO Web Interface reporting, (2016, May 18). Retrieved from: https://www.cms.gov/medicare/quality-initiatives-
patient-assessment-instruments/pqrs/gpro_web_interface.html

©2011 Proprietary and Confidential
CARE-2: Screening for Future Fall Risk
27
When must the Quality Action be performed?
The screening must take place within the measurement period.
What are the documentation requirements relative to the Quality Action?
The patient’s medical record must contain:
• Documentation of whether the patient has been assessed for a history of falls or any fall with injury. Documentation of no falls is sufficient.
NOTE: Screening may be done with any formal screening tool as long as it fulfills thefall history documentation requirements.
CMS ACO GPRO Web Interface reporting, (2016, May 18). Retrieved from: https://www.cms.gov/medicare/quality-initiatives-
patient-assessment-instruments/pqrs/gpro_web_interface.html

©2011 Proprietary and Confidential
Gaps in Care- Action Plan
• Use EMR to review reports
– Analyze Gaps in Care
– Assign practice employee to the gaps in care
– Fill in gaps by December 31, 2016

WHY IMPORTANT?
©2011 Proprietary and Confidential
Why is reporting important?
• As an ACO, we must report all measures within each domain.
• Incomplete reporting, failure to meet minimum attainment, and poor performance on the audit may result in a Corrective Action Plan (CAP) or termination
• Dual sided risk contract!
64
QUESTIONS
©2011 Proprietary and Confidential
Announcements
• Next Lunch & Learn: 12/21/2016
• Reminders:
– ACO Notifications
– Requests for Tax ID information from PECOS
• 2016 ACO Patient lists
• Save the date: Annual Meeting January 25th 2017
Sheree M Arnold
ACO Clinical Transformation Specialist
(716)862-2453