Embed Size (px)
Citation preview
This presentation is the intellectual property of the author. Contact them at [email protected]
permission to reprint and/or distribute.
Skin Disease in AthletesThe War on Staph
John C. Browning, MD, FAAD, FAAP
Financial Disclosure
Dr. John C. Browning has disclosed that he is on the Advisory Board for TopMD, a Consultant to ViroXis, and a Speaker for Galderma.
War On Staph
• Background
• ‘Containment’ Maintenance Strategies
• Special Focus on Sodium Hypochlorite & AD
This presentation is the intellectual property of the author. Contact them at [email protected]
permission to reprint and/or distribute.
Human Microbiome
• The human skin microbiome refers to the entire collection of microbes – bacteria, archaea, fungi, viruses, and mites – that reside in and on human skin.
• The human body contains over 10 times more microbial cells than human cells
Skin Microbiome• The skin is colonized by a diverse milieu
of microorganisms, most of which are harmless or even beneficial to their host.
– Colonization is driven by the ecology of the skin surface, which is highly variable depending on topographical location, endogenous host factors and exogenous environmental factors.
– The cutaneous innate and adaptive immune responses can modulate the skin microbiota, but the microbiota also functions in educating the immune system (Grice and Segre)
• Heterogeneity and pattern of distribution of the skin microbiome for over 20 skin sites shown here using RNA sequencing in 10 healthy volunteers (Grice and Kong)
Grice EA, Segre JA. Nat Rev Microbiol. 2011 Apr;9(4):244-53.Kong HH. Trends Mol Med. 2011 Jun;17(6):320-8. Epub 2011 Mar 4.
Grice EA, et al. Science.2009; 324:1190–1192.
Bacterial Skin Populations Who’s Living On You?
• Transient---contaminant, non-reproducing
• Temporary resident ---not typically resident, yet can colonize
• Resident---growing, reproducing flora
• ‘Normal’ resident skin flora includes:– P. acnes– S. epidermis– S. aureus,– C. diphtheria, C.
jeikeium– P. aeruginosa
Kong HH. Trends Mol Med. 2011 Jun;17(6):320-8.
This presentation is the intellectual property of the author. Contact them at [email protected]
permission to reprint and/or distribute.
Know The Conditions
MRSA (vs MSSA)
• Resistant to beta-lactams and cephalosporins via mecA gene
• Community acquired (CA) cases emerged in the mid-late 1990’s
• Majority of cases are CA vs hospital acquired (HA)
• Majority of US cases are due to USA type 300
• Leading cause of boils and abscesses in US
• Increasingly common among atopics, athletes
Initial Episode vs Recurrence
• High frequency of recurrence among patients affected with both MRSA and MSSA– Especially common among family members
This presentation is the intellectual property of the author. Contact them at [email protected]
permission to reprint and/or distribute.
Primary vs SecondarySkin & Soft Tissue Infections (SSTI)
Primary SSTI’sImpetigoCellulitisFolliculitis
Boils/Furunculosis
Secondary SSTI’sInfected Eczema (AD)Infected Dermatitis
BurnsWounds
Skin Barrier Intact Skin Barrier Impaired
Primary Staph Infections
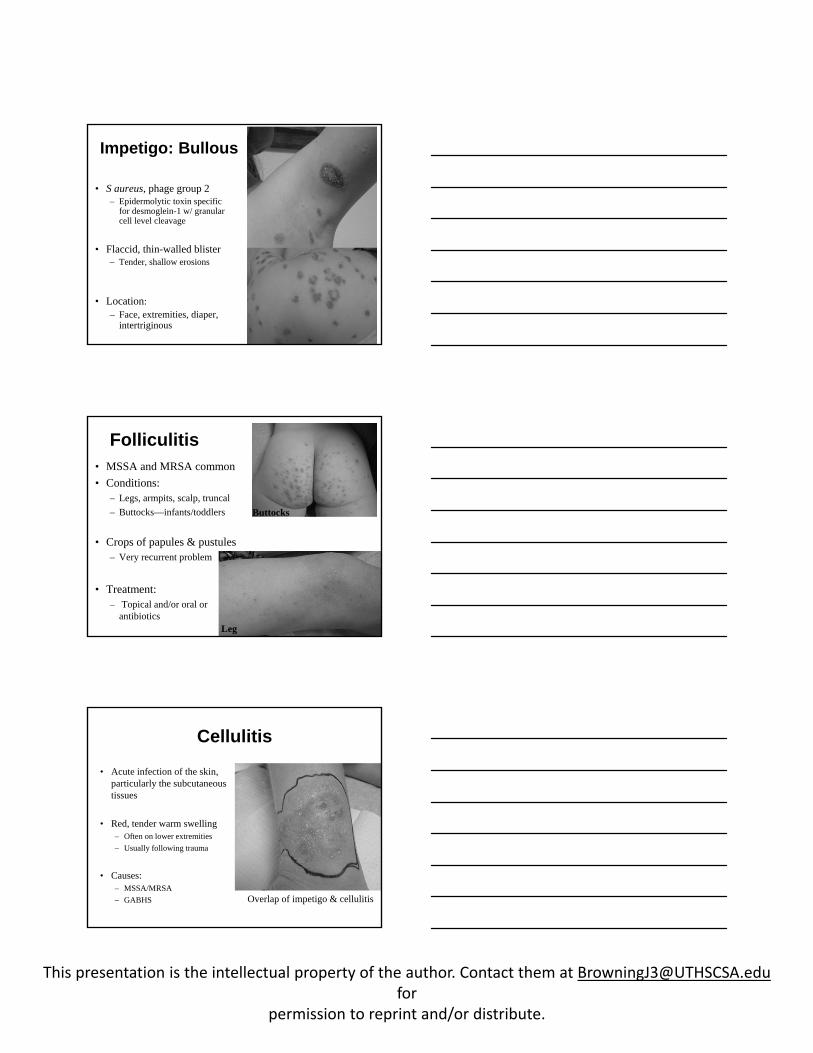
Impetigo• 70% of cases are due to S.
aureus– Remaining due to S. pyogenes
• 70% cases are non-bullous type
• Erythematous papules and thin-walled vesicles– Characteristic yellow crust.
• Face and extremities
• Carriage: Nasal; perineum
• No great study looking at incidence of impetigo from MRSA
This presentation is the intellectual property of the author. Contact them at [email protected]
permission to reprint and/or distribute.
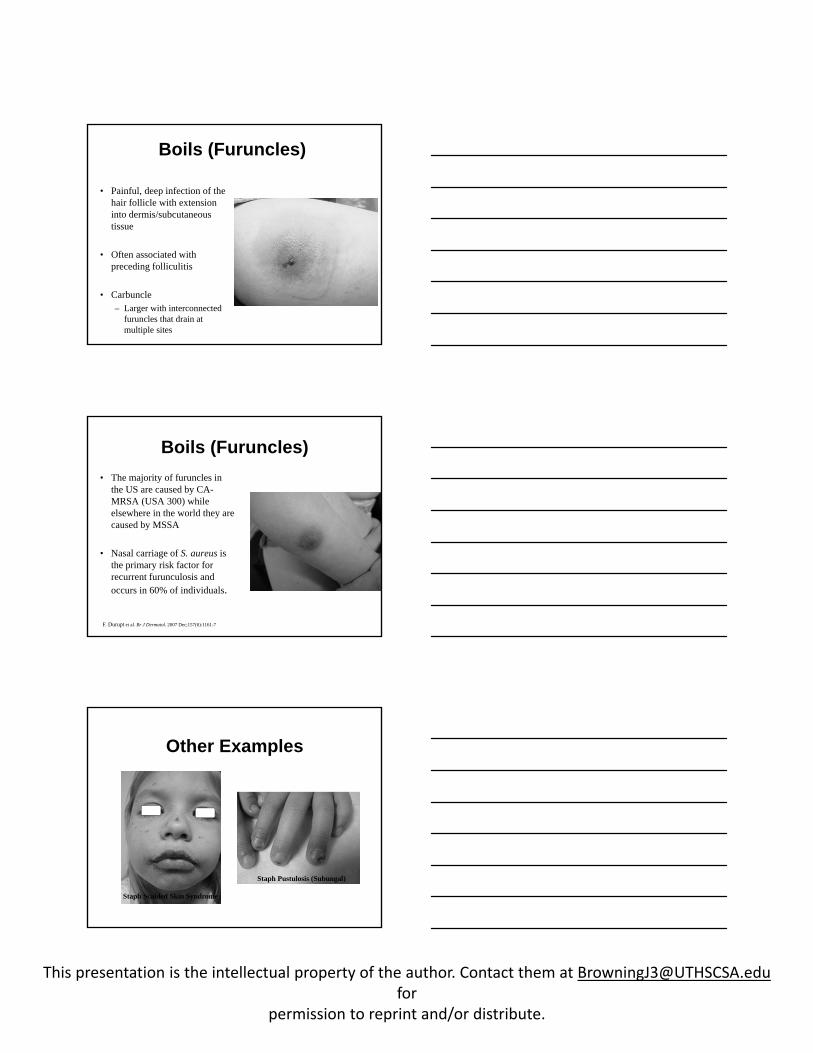
Impetigo: Bullous
• S aureus, phage group 2– Epidermolytic toxin specific
for desmoglein-1 w/ granular cell level cleavage
• Flaccid, thin-walled blister– Tender, shallow erosions
• Location:– Face, extremities, diaper,
intertriginous
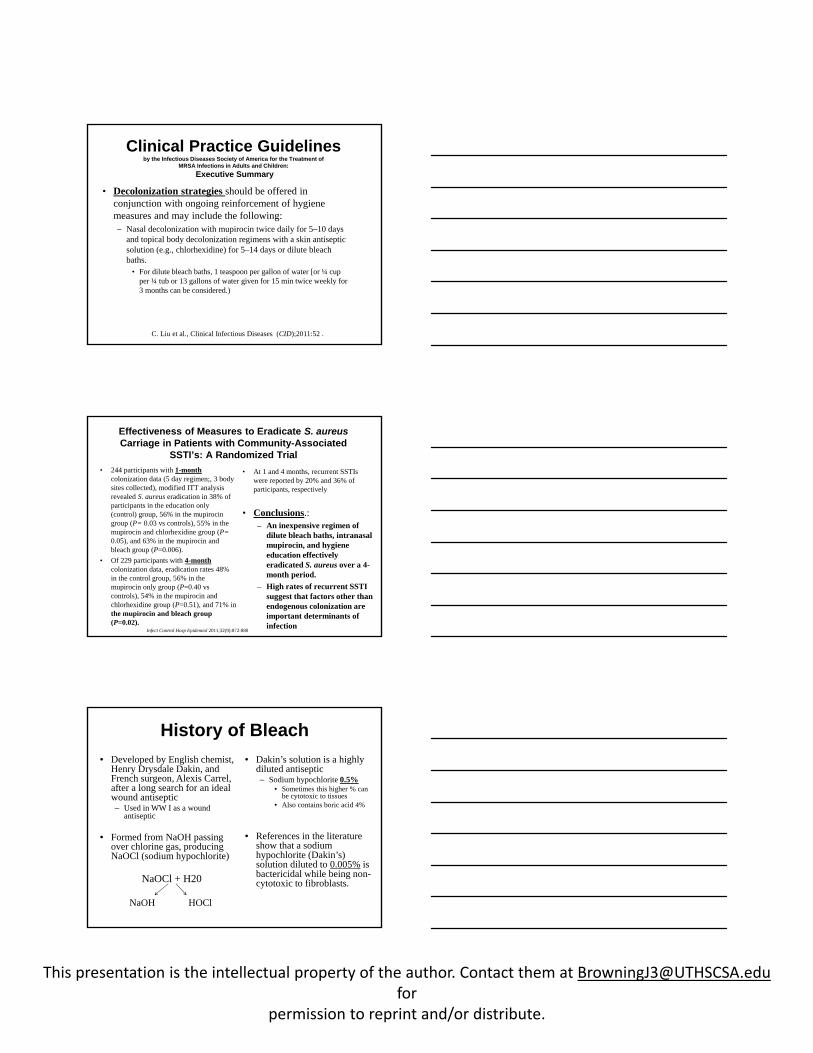
Folliculitis• MSSA and MRSA common• Conditions:
– Legs, armpits, scalp, truncal– Buttocks—infants/toddlers
• Crops of papules & pustules– Very recurrent problem
• Treatment:– Topical and/or oral or
antibiotics
Buttocks
Leg
Cellulitis
• Acute infection of the skin, particularly the subcutaneous tissues
• Red, tender warm swelling– Often on lower extremities– Usually following trauma
• Causes:– MSSA/MRSA– GABHS Overlap of impetigo & cellulitis
This presentation is the intellectual property of the author. Contact them at [email protected]
permission to reprint and/or distribute.
Boils (Furuncles)
• Painful, deep infection of the hair follicle with extension into dermis/subcutaneous tissue
• Often associated with preceding folliculitis
• Carbuncle– Larger with interconnected
furuncles that drain at multiple sites
Boils (Furuncles)• The majority of furuncles in
the US are caused by CA-MRSA (USA 300) while elsewhere in the world they are caused by MSSA
• Nasal carriage of S. aureus is the primary risk factor for recurrent furunculosis and occurs in 60% of individuals.
F. Durupt et al. Br J Dermatol. 2007 Dec;157(6):1161-7
Other Examples
Staph Pustulosis (Subungal)
Staph Scalded Skin Syndrome
This presentation is the intellectual property of the author. Contact them at [email protected]
permission to reprint and/or distribute.
Clinical Practice Guidelines by the Infectious Diseases Society of America for the Treatment of
MRSA Infections in Adults and Children:Executive Summary
• Decolonization strategies should be offered in conjunction with ongoing reinforcement of hygiene measures and may include the following:– Nasal decolonization with mupirocin twice daily for 5–10 days
and topical body decolonization regimens with a skin antiseptic solution (e.g., chlorhexidine) for 5–14 days or dilute bleach baths.
• For dilute bleach baths, 1 teaspoon per gallon of water [or ¼ cup per ¼ tub or 13 gallons of water given for 15 min twice weekly for 3 months can be considered.)
C. Liu et al., Clinical Infectious Diseases (CID);2011:52 .
Effectiveness of Measures to Eradicate S. aureus Carriage in Patients with Community-Associated
SSTI’s: A Randomized Trial• 244 participants with 1-month
colonization data (5 day regimen;, 3 body sites collected), modified ITT analysis revealed S. aureus eradication in 38% of participants in the education only (control) group, 56% in the mupirocin group (P= 0.03 vs controls), 55% in the mupirocin and chlorhexidine group (P= 0.05), and 63% in the mupirocin and bleach group (P=0.006).
• Of 229 participants with 4-monthcolonization data, eradication rates 48% in the control group, 56% in the mupirocin only group (P=0.40 vs controls), 54% in the mupirocin and chlorhexidine group (P=0.51), and 71% in the mupirocin and bleach group (P=0.02).
• At 1 and 4 months, recurrent SSTIs were reported by 20% and 36% of participants, respectively
• Conclusions.:– An inexpensive regimen of
dilute bleach baths, intranasal mupirocin, and hygiene education effectively eradicated S. aureus over a 4-month period.
– High rates of recurrent SSTI suggest that factors other than endogenous colonization are important determinants of infection
Infect Control Hosp Epidemiol 2011;32(9):872-880
History of Bleach • Developed by English chemist,
Henry Drysdale Dakin, and French surgeon, Alexis Carrel, after a long search for an ideal wound antiseptic– Used in WW I as a wound
antiseptic
• Formed from NaOH passing over chlorine gas, producing NaOCl (sodium hypochlorite)
NaOCl + H20
NaOH HOCl
• Dakin’s solution is a highly diluted antiseptic– Sodium hypochlorite 0.5%
• Sometimes this higher % can be cytotoxic to tissues
• Also contains boric acid 4%
• References in the literature show that a sodium hypochlorite (Dakin’s) solution diluted to 0.005% is bactericidal while being non-cytotoxic to fibroblasts.
This presentation is the intellectual property of the author. Contact them at [email protected]
permission to reprint and/or distribute.
Mechanisms of BleachTraditional Theories:• Potent oxider
– Forms reactive oxygen species (ROS) which damage DNA, RNA, and lipids, and proteins
• Membrane disruption– Due to increased pH
• Organic and fat solvent– Reacts with NaOH
• Recent : – 1) Neutralizing of amino
acids1 (NaOH)– 2) Chloramination reaction
with amino acids, leading to degradation1,3 (HOCl)
– 3) Oxidative unfolding and aggregation of proteins (heat shock protein 33)2
(HOCl)– 4) May affect bacterial
biofilm3 (endodontics literature)
1) Estrela et al, Braz Dent J, 2002:13: 113‐1172) Winter et al., Cell, 2008; 135:691‐701.3) ZahedM. Int Dent J, 2008; 58:329‐41.
Sodium hypochlorite Concentration
• Household bleach: Laundry– 3-6% solution of sodium hypochlorite
• Endodontics: Root Canals– 0.5-6% sodium hypochlorite used to help dissolve
necrotic tissue (began in the early 1920’s)
• Skin: Cleansing/Wound Care– Most topical products contain less than 0.1% sodium
hypochlorite
Sodium Hypochlorite• Burns/Wounds:
– NaOCl 0.025% was found to be bactericidal against gram-positive and gram-negative bacteria 1
– In another study2, the optimal concentration of 0.006% would be suitable for the treatment of burn wound infections without causing tissue toxicity.
• Killing MRSA strains:– Fisher et al3 found that,
after 5 minutes in a bath of sodium hypochlorite at 2.5 microL⁄milliL of tap water (equivalent to approximately ½ cup of bleach in 13 gallons of water, or a ¼ filled bathtub) was most effective at killing multiple community‐acquired MRSA strains
1) Heggers JP, Sazy JA, Stenberg BD et al. J Burn Care Rehabil, 1991;12:420–424.2) Coetzee E, Whitelaw A, Kahn D et al. Burns 20113) Fisher RG, Chain RL, Hair PS et al .Pediatr Infect Dis J, 2008;27:934–935.
This presentation is the intellectual property of the author. Contact them at [email protected]
permission to reprint and/or distribute.
Bleach Dilutions(6%)
Sodium Cups Bathtub (40-60 gallon)Hypochlorite (%)
0.009% (90 ppm) ¼ cup ¼ tub0.019% (190 ppm) ½ cup ¼ tub0.005% (50 ppm) ¼ cup ½ tub0.009% (90 ppm) ½ cup ½ tub 0.005% (50 ppm) ½ cup Full tub
References:Bathtub: 40-60 gallons; 1 gallon = 128 oz, 40 gallons = 5120 oz; 1 cup = 8 ozSwimming pool reference: 3 parts per million (available chlorine)
8-10 minutes, 2-3 times/wk Infant tub: 1-2 tsp/gallonRinse after
OTC Topical Antibiotics
• Double Antibiotic Ointment (Polysporin®)– Bacitracin– Polymyxin B
• Triple Antibiotic Ointment (Neosporin®)– Bacitracin– Polymyxin B– Neomycin
• Both products are indicated for prevention of SSTI’s, including wound management for skin abrasion and minor burns
• Polymyxin B binds to the cell membrane and act as a surfactant that destroys bacterial cell membranes.
• Bactericidal activity against some gram-negative organisms• Rarely cause allergic contact dermatitis
• Bacitracin and Neomycin have gram-positive coverage, but they are less effective and do not treat MRSA.
Rx Topical Antibiotics
• Fusidic acid– Inhibitor of bacterial
protein synthesis – Effective against
gram-positive species, such as Staphylococcus and Corynebacterium.
– Not available in US
• Mupirocin Cream (Bactroban®; Centany®)
• Mupirocin Ointment (generic)
• Retapumulin (Altabax®)
This presentation is the intellectual property of the author. Contact them at [email protected]
permission to reprint and/or distribute.
Mupirocin
• Inhibitor of bacterial isoleucyl t-RNA synthetase and protein synthesis
• Bactericidal vs. gram positive bacteria
• Ointment also used to help decrease S. aureus nasal colonization
• Cream:– Indicated for secondarily
infected traumatic skin lesions caused by S. aureus and S. pyogenes
• Ointment:– Indicated for impetigo,
superf infected dermatoses, and weeping lesions due to S. aureus, B-hemolyticstrep, and S. pyogenes.
Retapamulin 1% Ointment (Altabax™)
• Class of pleuromutilins which selectively inhibit the elongation phase of bacterial protein synthesis at a unique (50s subunit) site on ribosome.
• Retapamulin is FDA-approved for the topical treatment of impetigo caused by S. aureus (MSSA) and S. pyogenes in both adults and children.
• Retapamulin shows in vitro activity against S. aureus and S. pyogenes, including isolates resistant to b-lactams, macrolides, quinolones, and mupirocin
Bangert, Levy, Hebert. Pediatr Dermatol, Vol. 29 (3), 243–248, 2012Jones RN, et al. Antimicrob Agents Chemother 2006;50:2583–2586.Woodford N et al. J Antimicrob Chemother 2008;62:766–768.
Trends In Resistance
Biocides & Topicals
This presentation is the intellectual property of the author. Contact them at [email protected]
permission to reprint and/or distribute.
Bleach-Derived Products
Diluted Dakin’s Solution(Century Pharmaceuticals)
• Indication:– OTC--mechanical cleansing of dirt and debris
from skin, abrasions, cuts, and minor irritations.– Professional--mechanical cleansing and
debriding acute and chronic wounds; such as stage I-IV pressure ulcers, diabetic foot ulcers, pre and post surgical wounds, first and second degree bums, grafted and donor sites.
• Key Ingredient: – Sodium hypochlorite concentration 0.0125%
• Considered to be a ‘preservative’ – Other concentrations listed on their website
Aurstat® Hydrogel(Onset Dermatologics)
• Indication: – Minor skin abrasions,
lacerations, minor irritations, and intact skin
– Applied 1-2 times daily
• Microcyn®-based technology• Sodium hypochlorite 0.002%• Hypochlorous acid 0.008%
• Non-irritating• Can be used on the face
• Kill Times:– In laboratory testing,
Aurstat™ killed 99.99% of S. aureus within 30 seconds
• Rx required– Available as a kit
(Aurstat™ or Hylatopic™)
• 1 small study used in combo with Hylatopic™
Source: Onset Pharmceuticals
This presentation is the intellectual property of the author. Contact them at [email protected]
permission to reprint and/or distribute.
CLn® Body Wash(TopMD, Inc.)
• Indication:– Clean and relieve
dryness/flaking of skin
• Available as cosmetic product– In-office dispensing– Web site (www.clnwash.com)
• Passed All Basic Testing:– Epiocular™; Repeat insult
patch test; US/Euro Antimicrobial Effectiveness Test
• Kill Rates S. aureus:• 98% kill rate at 2 min• 99.9 at 3 and 5 min
• Studies:– Completed Pilot Study
• 18 moderate-severe atopics(submitted for publication)
– Planned:• 50 patient multi-center study
in moderate-severe atopics• 20 patient single-center
comparative study for hand eczema (investigator-initiated)
• 30 patient acne pilot study
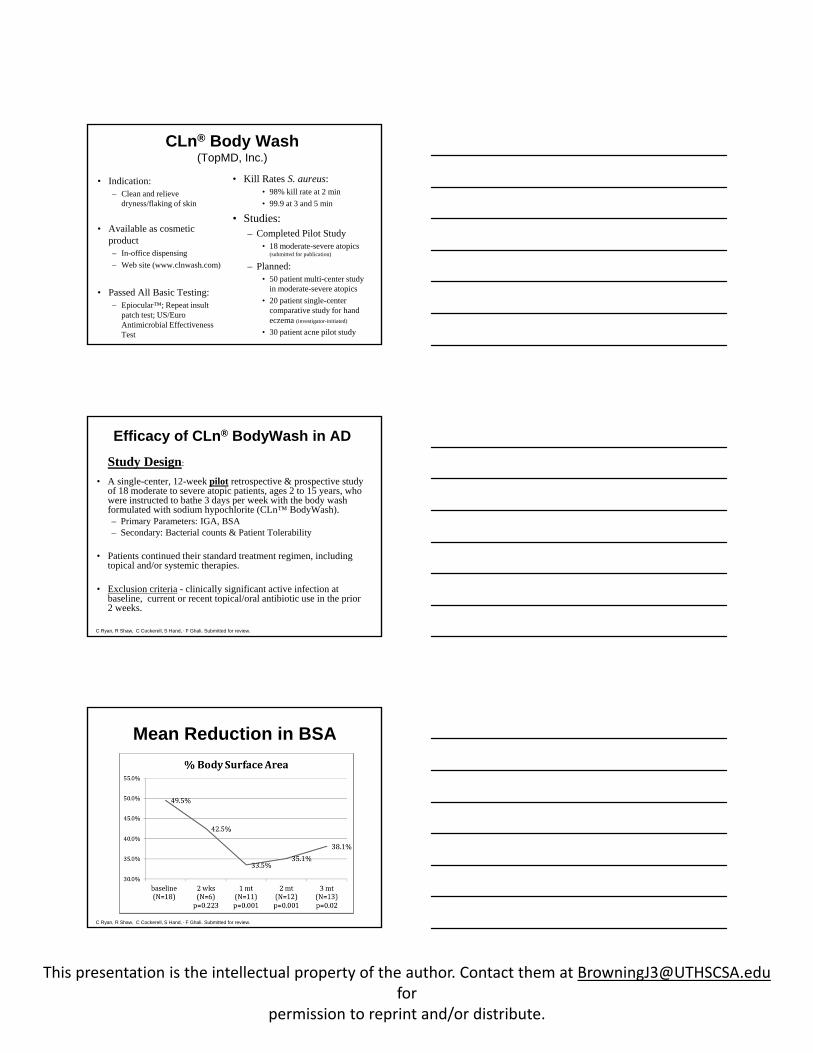
Efficacy of CLn® BodyWash in ADStudy Design:
• A single-center, 12-week pilot retrospective & prospective study of 18 moderate to severe atopic patients, ages 2 to 15 years, who were instructed to bathe 3 days per week with the body wash formulated with sodium hypochlorite (CLn™ BodyWash).– Primary Parameters: IGA, BSA– Secondary: Bacterial counts & Patient Tolerability
• Patients continued their standard treatment regimen, including topical and/or systemic therapies.
• Exclusion criteria - clinically significant active infection at baseline, current or recent topical/oral antibiotic use in the prior 2 weeks.
C Ryan, R Shaw, C Cockerell, S Hand, , F Ghali. Submitted for review.
Mean Reduction in BSA
C Ryan, R Shaw, C Cockerell, S Hand, , F Ghali. Submitted for review.
This presentation is the intellectual property of the author. Contact them at [email protected]
permission to reprint and/or distribute.
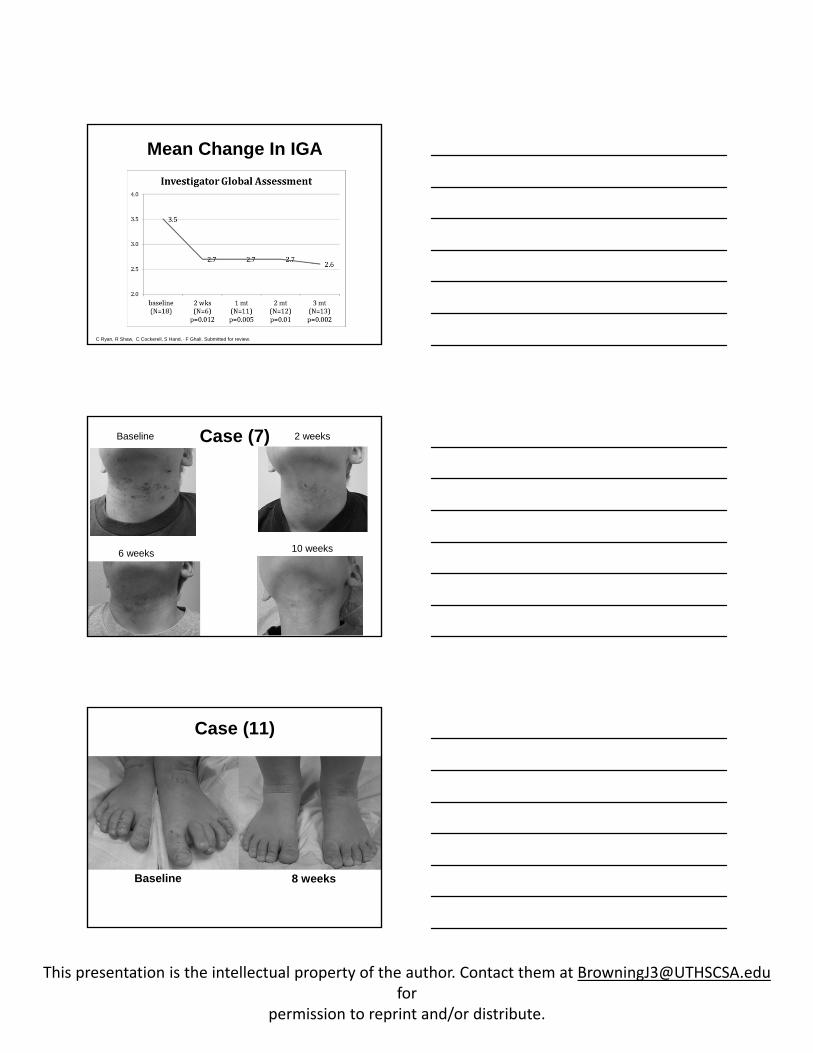
Mean Change In IGA
C Ryan, R Shaw, C Cockerell, S Hand, , F Ghali. Submitted for review.
Case (7)Baseline
6 weeks
2 weeks
10 weeks
Case (11)
Baseline 8 weeks
This presentation is the intellectual property of the author. Contact them at [email protected]
permission to reprint and/or distribute.
Results: CLn® BodyWash
• Changes in BSA and IGA showed statistically significant results.
• Adverse Events:– 3 reported burning/stinging
• Tolerability:– CLn Body Wash™ was well-
tolerated and overall patient preference was statistically significant over the traditional bleach baths.
• Bacteriology:– Decreasing trend in
quantitative S. aureus counts; statistically significant at 1 month
• MRSA colonization rate 44% (moderate-severe AD), higher than other studies
• Conclusions:– Similar to traditional bleach
baths, this study supports the adjunctive use of sodium hypochlorite wash in the treatment of AD
C Ryan, R Shaw, C Cockerell, S Hand, , F Ghali. Submitted for review.
The End