Embed Size (px)
DESCRIPTION
A Practical Algorithmic Approach to the Diagnosis and Management of Solitary Pulmonary Nodules. 背景. 孤立性肺部结节( solitary pulmonary nodule , SPN )的定义:影像学显示的直径 ≤3cm 、边缘 2/3 以上被肺组织包绕的肺部高密度影,需除外淋巴结、肺不张及阻塞性肺炎。 胸片检查可发现 0.09%-7% 的 SPN 。胸部 CT 扫描则可发现 8%-51% 的 SPN 。 恶性肿瘤的比例为 1.1%-12% 。. 鉴别诊断. 感染性疾病. 新生物. - PowerPoint PPT Presentation
Citation preview


背景孤立性肺部结节( solitary pulmonary nodule , SPN)的定义:影像学显示的直径≤ 3cm、边缘 2/3以上被肺组织包绕的肺部高密度影,需除外淋巴结、肺不张及阻塞性肺炎。
胸片检查可发现 0.09%-7% 的 SPN。胸部 CT扫描则可发现 8%-51% 的 SPN。
恶性肿瘤的比例为 1.1%-12%。

鉴别诊断感染性疾病 新生物结核球圆形肺炎、机化性肺炎肺脓肿真菌:曲霉、酵母菌、隐球菌、组织胞浆菌、球孢子菌寄生虫:阿米巴病、包虫病、犬恶丝虫病麻疹奴卡菌非典型分枝杆菌耶氏肺孢子菌病脓毒症栓子
良性:错构瘤软骨瘤纤维瘤脂肪瘤神经瘤硬化性血管瘤浆细胞肉芽肿子宫内膜异位症
恶性:肺癌原发性肺类癌孤立性转移瘤畸胎瘤平滑肌瘤

鉴别诊断血管性疾病 先天性疾病动静脉畸形肺梗死肺动脉瘤肺静脉曲张血肿
支气管囊肿肺隔离症支气管闭锁 伴粘液嵌塞
免疫性疾病类风湿关节炎Wegener肉芽肿MPA结节病
淋巴性疾病肺内或胸膜下淋巴结淋巴瘤
肺外疾病皮下结节乳头影肋骨骨折胸膜肥厚、团块或积液
其他疾病盘状肺不张类脂性肺炎淀粉样变粘液嵌塞肺部瘢痕

评估内容临床评估CT扫描PET-CT
MRI

临床评估临床症状缺乏特异性临床危险因素可能有一定提示作用:高龄、吸烟、既往有恶性肿瘤病史……
注意询问居住地、接触史、当地流行病学可提示良性、感染性病变:球孢子菌、隐球菌或组织胞浆菌病
注意肺部原发疾病: IPF、石棉肺、硬皮病与肺癌风险增加有关

CT扫描生长速度结节大小部位边缘 /边界特点脂肪成分空洞磨玻璃结节

生长速度恶性、实性 SPN倍增时间 20-400天,大部分< 100天
• 倍增时间> 400天:肿瘤生长速度缓慢或为良性病变• 倍增时间< 20天:病变发生极为迅速,常见于感染性疾病。• 倍增时间> 730天:基本可考虑良性病变,但警惕生长缓慢的肺腺癌
实性结节的生长速度评估:• ≥直径 10mm:测量直径变化• 直径 8-10mm:测算三维体积• 直径< 8mm:困难
磨玻璃影或半实性结节的生长速度评估:更为困难,需同时考虑体积和密度


结节大小直径> 3cm,恶性可能性大直径< 3cm,不能排除恶性

部位在大多数恶性病变的病例中, SPN出现在上叶的几率较大,可能与吸入性的有害物质(如香烟烟雾)在上叶的浓度更大有关。

光滑 分叶 放射状
锯齿状 多角形 晕征
边缘或边界特点

边缘或边界特点

钙化及衰减
注: CT值> 200Hu提示结节内有钙化

弥漫性钙化(良性) 中心性钙化(良性)
同心圆钙化(良性) 爆米花样钙化(错构瘤)

脂肪成分脂肪组织的 CT值在 -40~-120Hu之间,在错构瘤中出现的比例可达 60%,少见于类脂质肺炎恶性肿瘤罕见:脂肪肉瘤肺转移(大部分为实性病变)、肾细胞癌

空洞良性 恶性肺脓肿感染性肉芽肿血管炎早期郎格罕细胞增生症肺梗死空洞壁厚度< 5mm
鳞癌空洞壁不规律且厚度> 15mm

空洞泡沫样透亮区:结节内出现小的透亮区可见于:
原位腺癌或支气管肺泡癌肺淋巴瘤结节病圆形肺炎机化性肺炎
支气管肺泡癌

半实性(部分磨玻璃)结节半实性结节大部分为腺癌可能,包括不典型腺瘤样增生、原位腺癌、低浸润性腺癌、肺泡癌。
CT扫描中半实性结节内实性成分越多,侵袭程度越高。单纯通过影像学特点区别半实性结节的良恶性很困难,要诊断良性半实性结节应慎重,因为有些恶性病变可以生长速度很慢。
临床上,即使此类病变在 2年以上无进展或 PET检查未见异常,仍倾向于考虑恶性病变可能

PET-CT扫描生长速度结节大小SUV ( Standardized uptake value)

生长速度与单纯 CT扫描类似,对直径在 8mm以上的结节可根据三维体积计算法准确评估生长速度

结节大小PET对直径 8-10mm以上的结节敏感性较好直径< 10mm的结节或磨玻璃结节敏感性较差

SUV值高 SUV值提示 FDG摄取量增加,与代谢活跃有关,多提示为恶性病变
以平均 SUV > 2.5作为界值有较好的敏感性和特异性在诊断有困难的病例中,可以通过延迟扫描来观察结节的代谢程度以帮助作鉴别诊断,如果延迟 2小时以上,结节仍具有较高的摄取值,则提示为恶性,但目前尚存在争议

PET-CT的缺点对直径< 8-10mm 的 SPN敏感性低,结节体积太小而难以被发现
对代谢不活跃的病灶常出现假阴性,如原位腺癌、类癌对恶性可能性较高的结节,即使 PET检查阴性,也应该考虑外科活检或手术切除
PET检查阴性的 SPN仍应密切随访至少 2年以上假阳性结果常见于感染或炎性病变,如结核、真菌、结节病
组织病理活检仍作为 SPN诊断的金标准

MRI动态MRI可以反映 SPN内部的微血管结构并进行定量在动态MRI检查中,增强比斜率( slope of enhancement
ratio)以 0.04/s为界值,敏感度、特异度、阳性预测值、阴性预测值及准确度分别达到 96.3%, 82.1%, 95.7%, 84.2%, 93.6%,优于 CT 及 PET-CT
动态MRI今后有望成为 SPN的理想诊断方法

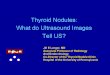
预测恶性几率( Pretest Probability)的计算整合患者的临床症状、危险因素及影像学资料,相对客观、定量地计算 SPN的恶性几率
Age is the patient's age in years, smoke = 1 if the patient is a current or former smoker (otherwise, smoke = 0), diameter is the diameter of the nodule in millimeters, spiculation = 1 if the edge of the nodule has spicules (otherwise, spiculation = 0), and location = 1 if the nodule is located in an upper lobe (otherwise, location = 0).

Practical Algorithmic Approach to the SPN



总结推荐使用预测恶性几率的计算方法帮助评估 SPN,更有利于临床医师对患者进行危险分层。
实性 SPN 直径< 8mm 或 8mm以上但恶性可能性小的病变,推荐定期复查 CT。 对直径 8mm以上且恶性可能性大的病变,推荐手术切除或活检,但同时应考虑患者的意愿及临床状况。
对中危病变,应考虑 PET-CT,如果 PET-CT提示代谢活性高,应考虑手术切除。磨玻璃样结节
≤直径 5mm的单纯磨玻璃样结节无需进一步处理, 5mm以上需要定期复查 CT并随访 2年以上。
半实性结节且直径> 5mm,如果病变在 3月以上持续存在,应行 PET-CT或外科手术切除。