Embed Size (px)
Citation preview
Journal of Aesthetic & Reconstructive Surgery ISSN 2472-1905
2017Vol. 3 No.2: 7
iMedPub Journals www.imedpub.com
Case Report
DOI: 10.4172/2472-1905.100030
1© Under License of Creative Commons Attribution 3.0 License | This article is available in: http://aesthetic-reconstructive-surgery.imedpub.com/archive.php
Mehmet Emin Cem Yıldırım1, Sidika Findik2 andZeynep Altuntas1
1 DepartmentofPlastic,ReconstructiveandAestheticSurgery,SchooloftheMedicine,NecmettinErbakanUniversity,Konya,Turkey
2 DepartmentofPathology,SchooloftheMedicine,NecmettinErbakanUniversity,Konya,Turkey
*Corresponding author: ZeynepAltuntas
Tel: +90 332 223 60 00-7033Fax: +90 332 323 61 81
DepartmentofPlasticandReconstructiveandAestheticSurgery,SchooloftheMedicine,NecmettinErbakanUniversity,42080Meram,Konya,Turkey.
Citation: YıldırımMEC,FindikS,AltuntasZ(2017)ARareCaseofJuvenilGiantFibroadenoma.JAesthetReconstrSurg.Vol.3No.2:7.
IntroductionThemostcommoncauseofbreastmassesseeninyoungwomenis fibroadenomas. It is characterized as benign. Etiologically,increasedestrogenandreceptorsusceptibilityhavebeenaccused[1].Massgrowthusuallystopswhenitreaches2cminsize.Thosewithasizegreaterthan5cmarecalledgiantfibroadenomes[2].Juvenilegiantfibroadenomasareveryrarecasesandconstitute0.5%ofallfibroadenomas.Inthisstudy,wepresenta12-year-oldfemalepatientofgiantjuvenilefibroadenoma.
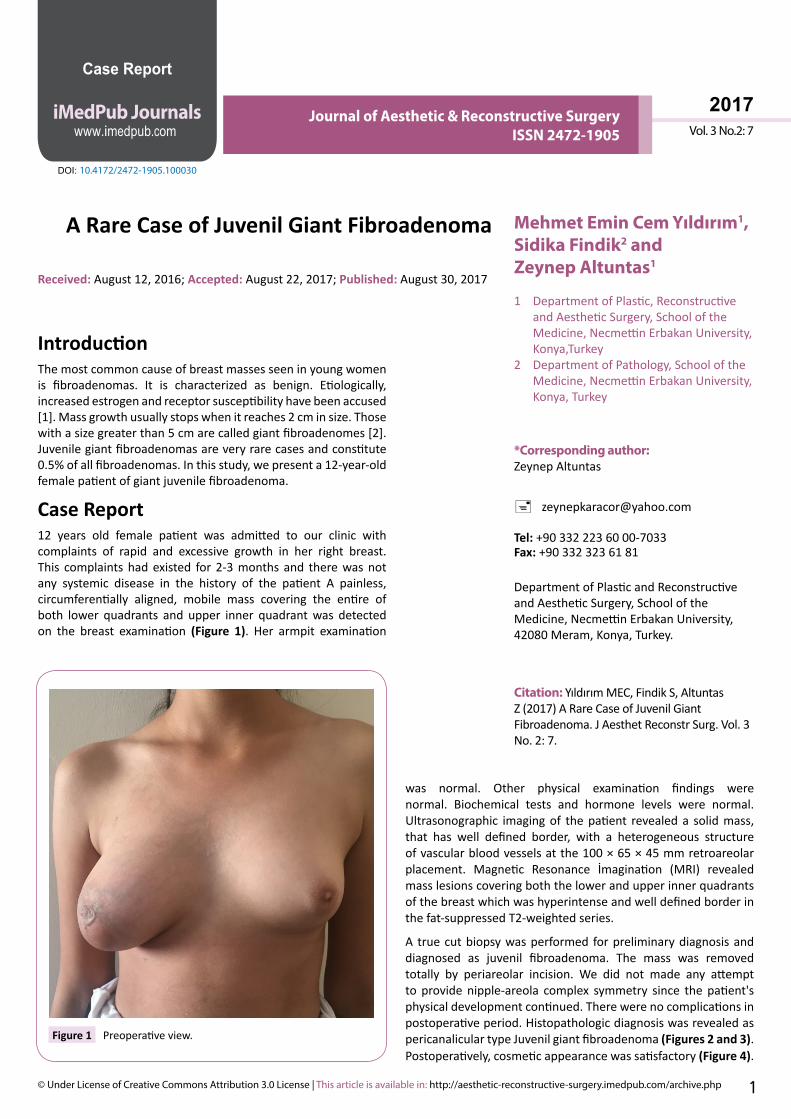
Case Report12 years old female patient was admitted to our clinic withcomplaints of rapid and excessive growth in her right breast.This complaintshadexisted for2-3months and therewasnotany systemic disease in the history of the patient A painless,circumferentially aligned, mobile mass covering the entire ofboth lower quadrants and upper inner quadrantwas detectedon the breast examination (Figure 1). Her armpit examination
was normal. Other physical examination findings werenormal. Biochemical tests and hormone levels were normal.Ultrasonographic imagingof thepatient revealeda solidmass,that has well defined border, with a heterogeneous structureofvascularbloodvesselsatthe100×65×45mmretroareolarplacement. Magnetic Resonance İmagination (MRI) revealedmasslesionscoveringboththelowerandupperinnerquadrantsofthebreastwhichwashyperintenseandwelldefinedborderinthefat-suppressedT2-weightedseries.
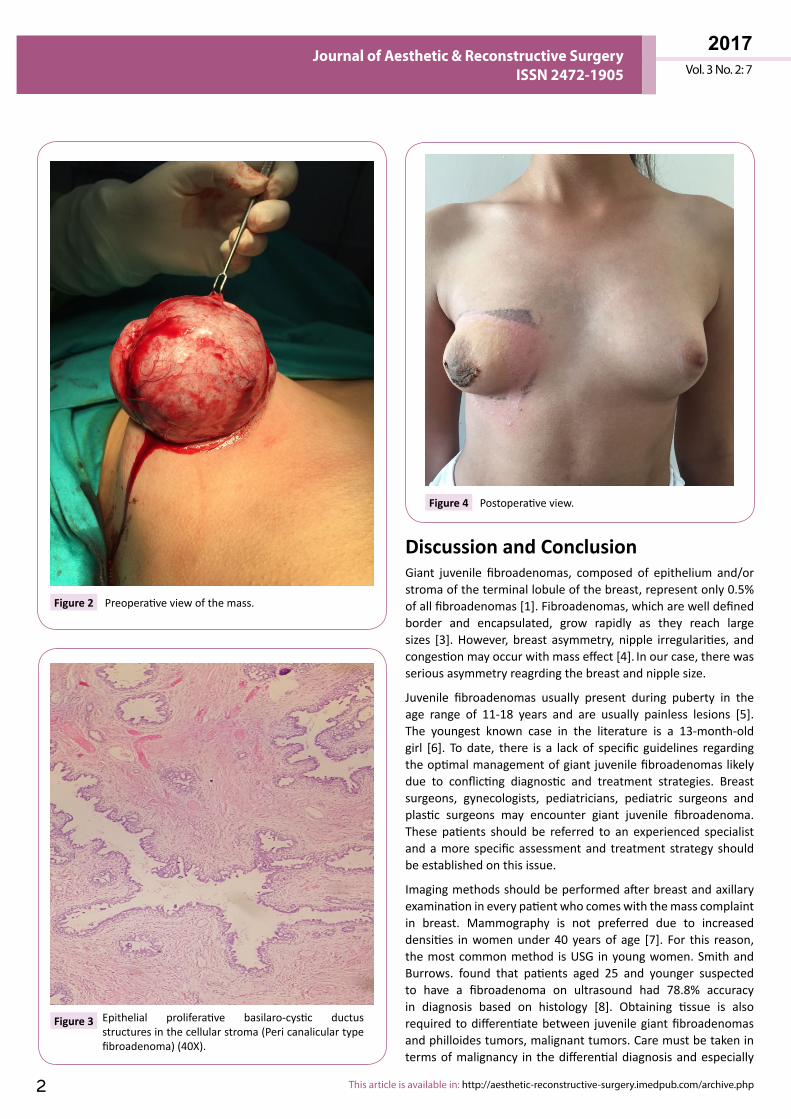
A truecutbiopsywasperformed forpreliminarydiagnosisanddiagnosed as juvenil fibroadenoma. The mass was removedtotally by periareolar incision. We did not made any attemptto providenipple-areola complex symmetry since thepatient'sphysicaldevelopmentcontinued.Therewerenocomplicationsinpostoperativeperiod.HistopathologicdiagnosiswasrevealedaspericanaliculartypeJuvenilgiantfibroadenoma(Figures 2 and 3).Postoperatively,cosmeticappearancewassatisfactory(Figure 4).
Received: August12,2016; Accepted: August22,2017;Published: August30,2017
A Rare Case of Juvenil Giant Fibroadenoma
Figure 1 Preoperativeview.
2017Journal of Aesthetic & Reconstructive Surgery
ISSN 2472-1905 Vol. 3 No. 2: 7
This article is available in: http://aesthetic-reconstructive-surgery.imedpub.com/archive.php2
Discussion and ConclusionGiant juvenile fibroadenomas, composed of epithelium and/orstromaoftheterminallobuleofthebreast,representonly0.5%ofallfibroadenomas[1].Fibroadenomas,whicharewelldefinedborder and encapsulated, grow rapidly as they reach largesizes [3].However, breast asymmetry, nipple irregularities, andcongestionmayoccurwithmasseffect[4]. Inourcase,therewasseriousasymmetryreagrdingthebreastandnipplesize.
Juvenile fibroadenomas usually present during puberty in theage range of 11-18 years and are usually painless lesions [5].The youngest known case in the literature is a 13-month-oldgirl [6]. Todate, there is a lackof specific guidelines regardingtheoptimalmanagementofgiantjuvenilefibroadenomaslikelydue to conflicting diagnostic and treatment strategies. Breastsurgeons, gynecologists, pediatricians, pediatric surgeons andplastic surgeons may encounter giant juvenile fibroadenoma.These patients should be referred to an experienced specialistandamore specificassessmentand treatment strategy shouldbeestablishedonthisissue.
Imagingmethodsshouldbeperformedafterbreastandaxillaryexaminationineverypatientwhocomeswiththemasscomplaintin breast. Mammography is not preferred due to increaseddensities inwomenunder40yearsof age [7]. For this reason,themostcommonmethod isUSG inyoungwomen.SmithandBurrows. found that patients aged 25 and younger suspectedto have a fibroadenoma on ultrasound had 78.8% accuracyin diagnosis based on histology [8]. Obtaining tissue is alsorequiredtodifferentiatebetween juvenilegiantfibroadenomasandphilloidestumors,malignanttumors.Caremustbetakenintermsofmalignancy in thedifferentialdiagnosisandespecially
Figure 2 Preoperativeviewofthemass.
Figure 3 Epithelial proliferative basilaro-cystic ductusstructuresinthecellularstroma(Pericanaliculartypefibroadenoma)(40X).
Figure 4 Postoperativeview.

Vol. 3 No. 2: 7
2017Journal of Aesthetic & Reconstructive Surgery
ISSN 2472-1905
3© Under License of Creative Commons Attribution 3.0 License
phylloides tumors should be considered. Philloides tumor is ararefibroepithelialbreasttumorthataccountsforlessthan1%ofallprimarybreastneoplasms,2-3%ofallfibroepithelial tumors[9,10].Theyaresimilarbenignfibroadenomabutdistinguishedfrom benign fibroadenomas, histologically increased cellularityandclinicallylocalrecurrenceandmetastaticspread.Therefore,the patient who is diagnosed with breast mass should beevaluatedintermsofphysicalexamination,imagingandbiopsy.TherearestudiesintheliteraturethatsuggestthatFineNeedleAspiration (FNA) biopsies are not reliable. one of the largestseriesofover1,400FNAsof adolescentbreastmasses,Kapinaet al. concluded FNA is not required [11]. However, sensitivityof the true-cut biopsy in the literature is reported to be 88-98%,specificity94-100%,andaccuracy93-99%[12,13]. Thus,inourcase,true-cutbiopsywasperformedinsteadoffineneedlebiopsy for tissue obtaining after imaging and histopathologicalpreliminarydiagnosiscameasjuvenilefibroadenoma.
Thetreatmentofjuvenilefibroadenomaisexcisionorobservation.Incasesofsimplefibroadenoma,conservativetreatmentmaybepreferredas10%ofthelesionsspontaneouslyresolve.However,in cases of giant fibroadenomas, surgical treatment should beperformed and additional reconstructive procedures might benecessary.Intheageofpuberty,tumorexcisionandsimultaneousbreast reconstruction principles can be performed to protectthebreastparenchyma,providesymmetryof thenipple-areolacomplexandavoidiatrogenicamastia[11,14].Revisionsurgeriesmaybeneededinordertoprovideacosmeticappearanceaftertheexcisionofthemass. Inourcase,weremovedthemassbyperiareolarincisionandtheremainingbreasttissueintheupperquadrantwassufficienttoprovidethesymmetrywhencomparedtothecounter-breast.However,sincethepatientwasintheageof growth, the possible revision operations for nipple–areolarcomplexsymmetrywerepostponedafterpuberty.
References1 SosinM, PulcranozM, Feldman ED, Patel KM,NahabedianMY, et
al. (2015) Giant juvenile fibroadenoma: A systemic review withdiagnosticandtreatmentrecommendation.GlandSurg4:312-321.
2 Marchant DJ (2002) Benign breast disease. Obstet Gynecol ClinNorthAm29:1-20.
3 ÇalışkanM, Acar A, ErdemH, KurtMD, Subaşı İE, et al. (2011)Juvenile giant fibroadenoma: case report. Medical Journal ofUmraniye3:17-19.
4 Thuruthiyath N, Das PC, Avabratha KS, Mascarenhas V, Marla N(2012) Giant fibroadenoma of breast in anadolescent girl. OmanMedJ27:314-315.
5 Wechselberger G, Schoeller T, Piza-Katzer H (2002) Juvenilefibroadenomaofthebreast.Surgery132:106-107.
6 JungYS,LeeKJ,YoonTI(2005)Juvenilefibroadenomain13-month-oldfemalechild.JPaediatrChildHealth41:78-79.
7 TemplemanC,HertweckSP(2000)Breastdisordersinthepediatricandadolescentpatient.ObstetGynecolClinNorthAm27:19-34.
8 SmithGE,BurrowsP(2008)Ultrasounddiagnosisoffibroadenoma-isbiopsyalwaysnecessary?ClinRadiol63:511-515.
9 ObuigboW(2003)Breastfibroadenomainteenagefemales.TurkishJPediatr45:326-328.
10 ParkerSJ,HarriesSA(2001)Phyllodestumours.PostgradMedJ77:428-435.
11 Kapila K, Pathan SK, Al-Mosawy FA (2008) Fine needle aspirationcytologyofbreastmasses in childrenandadolescents:experiencewith1404aspirates.ActaCytol52:681-686.
12 BrunnerAH,SagmeisterT,KremerJ,RissP,BrustmannH(2009)Theaccuracyoffrozensectionanalysisinultrasound-guidedcoreneedlebiopsyofbreastlesions.BMCCancer24:341.
13 HomeshNA,IssaMA,El-SofianiHA(2005)Thediagnosticaccuracyof fine needle aspiration cytology versus core needle biopsy forpalpablebreastlump(s).SaudiMedJ26:42-46.
14 ChangD,McGrathM(2007)Managementofbenigntumoursoftheadolescentbreast.PlastReconstrSurg120:13e-19e.

























![Fibroadenoma mammae [Autosaved]](https://img.pdfslide.net/doc/110x75/557201784979599169a1a911/fibroadenoma-mammae-autosaved.jpg)


