Embed Size (px)
Citation preview

Hindawi Publishing CorporationCase Reports in Surgery Volume 983090983088983089983091 Article ID 983089983093983088983092983093983095 983091 pageshttpdxdoiorg983089983088983089983089983093983093983090983088983089983091983089983093983088983092983093983095
Case Report
Adrenal Cyst Presenting as Hepatic Hydatid Cyst
Abdulla Darwish1 Veena Nagaraj1 Mohmmed B Mustafa1 and Ahmed Al Ansari2
983089 Pathology Department Bahrain Defense Force Hospital PO Box 983090983096983091983092983095 Riffa Bahrain983090 Department of General Surgery Bahrain Defense Force Hospital PO Box 983090983096983091983092983095 Riffa Bahrain
Correspondence should be addressed to Ahmed Al Ansari drahmedalansarigmailcom
Received 983089983097 February 983090983088983089983091 Accepted 983089983096 March 983090983088983089983091
Academic Editors S H Ein H Imura and Y-B ang
Copyright copy 983090983088983089983091 Abdulla Darwish et al Tis is an open access article distributed under the Creative Commons AttributionLicense which permits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
Introduction Although adrenal cysts areuncommon theincidence rate is increasing with theadvancesin radiologicaltechnologiesTe incidental detection o adrenal cysts nowadays has become more requent as a result o the increase usage o high quality imaging modalities Adrenal cysts originate rom the adrenal gland and canbe classi1047297ed into either true or pseudocyst Presentationof Case In this report we describedan adrenal cyst oendothelialtypein a 983091983088-year-oldladywho wasmistakenly diagnosedto have ahydatidcyst both clinically and by imaging Discussion Although adrenal cysts are uncommonthe incidencerate is increasing withthe requent use o various high quality radiological technologies Adrenal cyst should be considered in the differential diagnosiswhen dealing with upper abdominal cysts Te size o the adrenal cyst can vary rom a ew millimeters up to 983093983088 cm in diameterMost o the adrenal cysts are unilateral while 983096ndash983089983093 o those cysts do present bilaterally Te majority o cases are diagnosedbetween the983091rd and983093th decades Conclusion Although most o the adrenal cysts are benign in nature surgical excision is advisableespecially when the cysts are greater than 983093 cm in diameter and in the case o suspecting malignancy
1 Introduction
Most o the adrenal cysts are asymptomatic and heteroge-neous in nature [983089 983090] Big cysts can present incidentallyor due to the mass effect compressing on adjacent struc-tures causing abdominal or 1047298ank pain [983091] oday with theimprovement in imaging modalities and increase in theirusage adrenal cysts are being detected more requently asincidental lesions [983091]
In 983089983097983096983097 Medeiros et al stated that around 983091983088983088 caseswere discovered to that date [983092] In a literature review in983089983097983097983097 Neri and Nance described that 983091983092 o all adrenal cystsare discovered incidentally and 983091983097 present with abdominalpain or due to mass compression effect [983093]
In 983090983088983089983088 Wedmid and Palese documented that more than983094983088983088 adrenal cystic lesions were reported in the literature[983091 983094] Adrenal cysts can present unilaterally or bilaterallyAlthough that the majority o the adrenal cysts are unilateral983096ndash983089983093 are bilateral without side predominance [983095] Wepresent a trueadrenal cyst o endothelial typeclosely attachedto the hilum o the liver which was misdiagnosed clinically and radiologically as a Hydatid cyst
2 Case Report
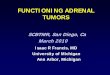
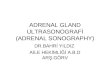
A 983091983088-year-old emale with a history o bronchial asthma andpregnant at 983089983092weeks o gestation presented with hyperemesisgravidarum to one o the private hospitals in the cityAbdominal ultrasound was perormed showing a large cystin the liver measuring 983089983090 times 983095 cm in size which was diagnosedas a hydatid liver cyst On general examination signs o dehydration were detected Abdominal examination revealedmild diffuse upper abdominal tenderness She was givensymptomatic treatment and reerred to the surgical clinicor ollowup which she ailed to attend Afer delivery andduring the routine ollow-up visit abdominal ultrasound wasdone showing evidence o a bilocular cyst with internal septameasuring 983089983093times 983095 cm situated in the right lobe o the liver withan extension to the undersurace C scan o the abdomenand pelvis revealed a septated cyst arising rom the right lobeo the liver (Figure 983089) A calci1047297ed septation within the cystand some degree o calci1047297cation o the superior aspect o thecyst were detected Te lef adrenal gland spleen and bothkidneys were all normal However the right adrenal glandcould not be delineated All other investigations including
983090 Case Reports in Surgery
F983145983143983157983154983141 983089 C abdomen and pelvis showing the cyst
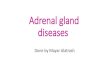
F983145983143983157983154983141 983090 Macroscopic appearance o the specimen showing tenseglistening grey brown cyst 1047297lled with clear 1047298uid Note the residualadrenal tissue attached to the external surace
chest X-ray renal unction tests liver unction tests otherbiochemical tests electrolytes hematocrit and thyroid unc-tion tests were normal Urine culture and sensitivity and viralserology were all normal Antibodies or a hydatid cyst werenegative (983089983094983088 reerence range lt 983091983094983088) Due to the large sizeo the cyst surgical intervention was considered laparotomy was perormed and the cyst was excised
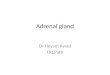
Macroscopic examination o the specimen showed a 983089983090times 983097 times 983095 cm partially collapsed multilocular brownish glis-tening cyst weighing 983090983089983088 grams and containing serous 1047298uid(Figure 983090) Te outer surace showed a 983092 times 983090 times 983088983093 cm yellow-ish atty adrenal tissue attached to the cyst Te average wallthickness o the cyst was 983088983090 cm the inner lining was largely smooth with ocal roughened papilloid areas Microscopi-cally the multilocular cyst showed a ocally calci1047297ed 1047297broticcyst wall lined by low cuboidal to 1047298attened epithelium whichshowed strong positivity or actor-983096 immunohistochemistry (Figures 983091 983092 and 983093) Congested blood vessels and clusters o lipidized adrenal cortical cells were also seen in the stromaTe included adrenal gland was within normal limits Nopleomorphism or mitosis was seen Te overall appearancewas consistent with a benign adrenal cyst o endothelial type
3 Discussion
Since 983089983094983095983088s when the 1047297rst adrenal cyst was described therehas been an evolution in the various radiological modalitieswhich has contributed to the incidental diagnosis o adrenalcysts [983091] Although adrenal cysts are uncommon the inci-dence rate is increasing with the requent use o high quality
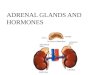
F983145983143983157983154983141 983091 low power view o the adrenal cyst composed o multi-locular spaces1047297lled with eosinophilic material Note the presence o calci1047297cation at the lower lef side o the photo (HampE stained slide)
F983145983143983157983154983141 983092 Tis photo shows a 1047297brocollagenous cyst wall withattached adrenal tissue (HampE stained slides)
F983145983143983157983154983141983093 showing cystic cell lining positive or actor VIII con1047297rm-ing endothelial cell origin (immunohistochemistry stained slide)
radiological imaging techniques Te most common type o adrenal cysts reported in the literature is the nonunctionalcyst However adrenal cysts can present in different ormsthey can be small or large unctional or nonunctionaltrue or pseudocysts and benign or malignant [983090 983096] Onpathological examination the majority o adrenal cysts arecategorized as either pseudocysts or true cysts Te incidencerate o adrenal cysts varies rom one type to another In theliterature pseudocysts account or 983094983088 o the cases and canbe classi1047297ed into hemorrhagic cysts neoplastic and parasiticcysts Noepithelial lining is ound in this type o adrenal cysts
Case Reports in Surgery 983091
[983090 983091 983096] rue adrenal cysts account or 983092983088 o the cases andcan present as endothelial cysts and epithelial cysts and rarely as vascular cysts or cystic lymphangiomas [ 983091 983096]
Most o the adrenal cysts are asymptomatic and canbe diagnosed incidentally more commonly situated in theright side and can be detected more requently in emalepatients [983091 983096] Te size o the adrenal cysts can vary rom ew millimeters up to 983093983088 cm in diameter [983097] Most o the adrenalcysts are unilateral with 983096ndash983089983093 that can present bilaterally [983095] Te majority o cases are diagnosed between the 983091rd and983093th decades [983089983088 983089983089] An adrenal cyst located in the lef side canbe conused or a pancreatic pseudocyst while a right-sidedadrenal cyst can be conused or a liver cyst [983089983090] as presentedin this case
Investigations can range rom hormonal workup to radi-ological modalities C scan is the investigation o choice orthe diagnosis o adrenal cysts It can show the location o thecyst reveal the density and de1047297ne the wall borders MRI issuperior in the differential diagnosis and in distinguishingbetween an adrenal lesion and a renal lesion [ 983089983091] Hormonalworkup in the orm o a 983090983092-hour urinary metanephrineserum potassium or three consecutive days a low-dosedexamethasone suppression test and aldosterone renin ratiois necessary in all cases o adrenal cysts in order to diagnoseunctional disease that is not clinically detected [ 983096]
Adrenal cysts can be managed either conservatively or by surgical excision Management is dependent on theunctional status o the cyst the probability o malignancyand complications such as hemorrhage or inection o thecyst [983089 983091 983092] Excision or aspiration o the adrenal cyst isrecommended i the patient is symptomatic and presentingwith endocrine abnormalities or with rapid expansion o the cyst and when malignancy cannot be ruled out [983089983092]In addition Bellantone et al have recommended surgicalresection o cysts that are greater than 983093 cm due to therisk o hemorrhage and inection [983095] Surgical resection willdecrease the incidence o uture complications in the orm o hemorrhage into the cyst local pressure effect and inectiono the cyst and to exclude the possibility o malignancy [ 983089]
4 Conclusion
Adrenal cysts should be considered in the differential diag-nosis when dealing with upper abdominal cysts Althoughmost adrenal Cysts are benign in nature surgical excision isadvisable especially when the cysts are larger than 983093 cm indiameter and there is a suspicion o malignancy
Consent
Written inormed consent was obtained rom the patient orpublication o this case report and accompanying images Acopy o the written consent is available or review on request
Conflict of Interests
All authors have no con1047298ict o interests
References
[983089] M R Khan S Ajmal and Saleem ldquoGiant adrenal endothelialcyst associated with acute and chronic morbidity in a youngemale a case reportrdquo Cases Journal vol 983090 no 983097 article 983096983096983092983089983090983088983088983097
[983090] J Sell M R Williamson R D Boutin and B J IgelldquoC demonstration o a giant adrenal endothelial cyst o the angiomatous subtyperdquo Computerized Medical Imaging and Graphics vol 983089983096 no 983094 pp 983092983094983097ndash983092983095983089 983089983097983097983092
[983091] A Wedmid and M Palese ldquoDiagnosis and treatment o theadrenal cystrdquo Current Urology Reports vol 983089983089 no 983089 pp 983092983092ndash983093983088983090983088983089983088
[983092] L J Medeiros K B Lewandrowski and A L Vickery ldquoAdrenalpseudocyst a clinical and pathologic study o eight casesrdquoHuman Pathology vol 983090983088 no 983095 pp 983094983094983088ndash983094983094983093 983089983097983096983097
[983093] L M Neri and F C Nance ldquoManagement o adrenal cystsrdquo American Surgeon vol 983094983093 no 983090 pp 983089983093983089ndash983089983094983091 983089983097983097983097
[983094] H P Chien Y S Chang P S Hsu et al ldquoAdrenal cysticlesions a clinicopathological analysis o 983090983093 cases with proposedhistogenesis and review o the literaturerdquo Endocrine Pathology vol 983089983097 no 983092 pp 983090983095983092ndash983090983096983089 983090983088983088983096
[983095] R Bellantone A Ferrante M Raffaelli M Boscherini C PLombardi and F Crucitti ldquoAdrenal cystic lesions report o 983089983090surgically treated cases and review o the literaturerdquo Journal of Endocrinological Investigation vol 983090983089 no 983090 pp 983089983088983097ndash983089983089983092 983089983097983097983096
[983096] P V Pradeep A K Mishra V Aggarwal P R K BhargavS K Gupta and A Agarwal ldquoAdrenal cysts an institutionalexperiencerdquo World Journal of Surgery vol 983091983088 no 983089983088 pp 983089983096983089983095ndash983089983096983090983088 983090983088983088983094
[983097] H Sanal M Kocaoglu D Yildirim et al ldquoImaging eatureso benign adrenal cystsrdquo European Journal of Radiology vol 983094983088no 983091 pp 983092983094983093ndash983092983094983097 983090983088983088983094
[983089983088] D G Foster ldquoAdrenal cysts Review o literature and report o caserdquo Archives of Surgery vol 983097983090 no 983089 pp 983089983091983089ndash983089983092983091 983089983097983094983094
[983089983089] G A Abeshouse R B Goldstein and B S Abeshouse ldquoAdrenalcysts Review o the literature and report o three casesrdquo Journal of Urology vol 983096983089 pp 983095983089983089ndash983095983089983097 983089983097983093983097
[983089983090] N Singh R K George S K Gupta A Gupta and A AgarwalldquoGiant adrenal cyst presenting as a diagnostic dilemma a casereportrdquo International Surgery vol 983097983088 no 983090 pp 983095983096ndash983096983088 983090983088983088983093
[983089983091] Y K Guo Z G Yang Y Li et al ldquoUncommon adrenalmasses C and MRI eatures with histopathologic correlationrdquoEuropean Journal of Radiology vol 983094983090 no 983091 pp 983091983093983097ndash983091983095983088 983090983088983088983095
[983089983092] G De oma R Gabriele M Plocco and P Sapienza ldquoAdrenalcysts therapeutical indicationsrdquo Minerva Chirurgica vol 983093983088no 983089983088 pp 983097983090983093ndash983097983090983096 983089983097983097983093
Submit your manuscripts at
httpwwwhindawicom

983090 Case Reports in Surgery
F983145983143983157983154983141 983089 C abdomen and pelvis showing the cyst
F983145983143983157983154983141 983090 Macroscopic appearance o the specimen showing tenseglistening grey brown cyst 1047297lled with clear 1047298uid Note the residualadrenal tissue attached to the external surace
chest X-ray renal unction tests liver unction tests otherbiochemical tests electrolytes hematocrit and thyroid unc-tion tests were normal Urine culture and sensitivity and viralserology were all normal Antibodies or a hydatid cyst werenegative (983089983094983088 reerence range lt 983091983094983088) Due to the large sizeo the cyst surgical intervention was considered laparotomy was perormed and the cyst was excised
Macroscopic examination o the specimen showed a 983089983090times 983097 times 983095 cm partially collapsed multilocular brownish glis-tening cyst weighing 983090983089983088 grams and containing serous 1047298uid(Figure 983090) Te outer surace showed a 983092 times 983090 times 983088983093 cm yellow-ish atty adrenal tissue attached to the cyst Te average wallthickness o the cyst was 983088983090 cm the inner lining was largely smooth with ocal roughened papilloid areas Microscopi-cally the multilocular cyst showed a ocally calci1047297ed 1047297broticcyst wall lined by low cuboidal to 1047298attened epithelium whichshowed strong positivity or actor-983096 immunohistochemistry (Figures 983091 983092 and 983093) Congested blood vessels and clusters o lipidized adrenal cortical cells were also seen in the stromaTe included adrenal gland was within normal limits Nopleomorphism or mitosis was seen Te overall appearancewas consistent with a benign adrenal cyst o endothelial type
3 Discussion
Since 983089983094983095983088s when the 1047297rst adrenal cyst was described therehas been an evolution in the various radiological modalitieswhich has contributed to the incidental diagnosis o adrenalcysts [983091] Although adrenal cysts are uncommon the inci-dence rate is increasing with the requent use o high quality
F983145983143983157983154983141 983091 low power view o the adrenal cyst composed o multi-locular spaces1047297lled with eosinophilic material Note the presence o calci1047297cation at the lower lef side o the photo (HampE stained slide)
F983145983143983157983154983141 983092 Tis photo shows a 1047297brocollagenous cyst wall withattached adrenal tissue (HampE stained slides)
F983145983143983157983154983141983093 showing cystic cell lining positive or actor VIII con1047297rm-ing endothelial cell origin (immunohistochemistry stained slide)
radiological imaging techniques Te most common type o adrenal cysts reported in the literature is the nonunctionalcyst However adrenal cysts can present in different ormsthey can be small or large unctional or nonunctionaltrue or pseudocysts and benign or malignant [983090 983096] Onpathological examination the majority o adrenal cysts arecategorized as either pseudocysts or true cysts Te incidencerate o adrenal cysts varies rom one type to another In theliterature pseudocysts account or 983094983088 o the cases and canbe classi1047297ed into hemorrhagic cysts neoplastic and parasiticcysts Noepithelial lining is ound in this type o adrenal cysts
Case Reports in Surgery 983091
[983090 983091 983096] rue adrenal cysts account or 983092983088 o the cases andcan present as endothelial cysts and epithelial cysts and rarely as vascular cysts or cystic lymphangiomas [ 983091 983096]
Most o the adrenal cysts are asymptomatic and canbe diagnosed incidentally more commonly situated in theright side and can be detected more requently in emalepatients [983091 983096] Te size o the adrenal cysts can vary rom ew millimeters up to 983093983088 cm in diameter [983097] Most o the adrenalcysts are unilateral with 983096ndash983089983093 that can present bilaterally [983095] Te majority o cases are diagnosed between the 983091rd and983093th decades [983089983088 983089983089] An adrenal cyst located in the lef side canbe conused or a pancreatic pseudocyst while a right-sidedadrenal cyst can be conused or a liver cyst [983089983090] as presentedin this case
Investigations can range rom hormonal workup to radi-ological modalities C scan is the investigation o choice orthe diagnosis o adrenal cysts It can show the location o thecyst reveal the density and de1047297ne the wall borders MRI issuperior in the differential diagnosis and in distinguishingbetween an adrenal lesion and a renal lesion [ 983089983091] Hormonalworkup in the orm o a 983090983092-hour urinary metanephrineserum potassium or three consecutive days a low-dosedexamethasone suppression test and aldosterone renin ratiois necessary in all cases o adrenal cysts in order to diagnoseunctional disease that is not clinically detected [ 983096]
Adrenal cysts can be managed either conservatively or by surgical excision Management is dependent on theunctional status o the cyst the probability o malignancyand complications such as hemorrhage or inection o thecyst [983089 983091 983092] Excision or aspiration o the adrenal cyst isrecommended i the patient is symptomatic and presentingwith endocrine abnormalities or with rapid expansion o the cyst and when malignancy cannot be ruled out [983089983092]In addition Bellantone et al have recommended surgicalresection o cysts that are greater than 983093 cm due to therisk o hemorrhage and inection [983095] Surgical resection willdecrease the incidence o uture complications in the orm o hemorrhage into the cyst local pressure effect and inectiono the cyst and to exclude the possibility o malignancy [ 983089]
4 Conclusion
Adrenal cysts should be considered in the differential diag-nosis when dealing with upper abdominal cysts Althoughmost adrenal Cysts are benign in nature surgical excision isadvisable especially when the cysts are larger than 983093 cm indiameter and there is a suspicion o malignancy
Consent
Written inormed consent was obtained rom the patient orpublication o this case report and accompanying images Acopy o the written consent is available or review on request
Conflict of Interests
All authors have no con1047298ict o interests
References
[983089] M R Khan S Ajmal and Saleem ldquoGiant adrenal endothelialcyst associated with acute and chronic morbidity in a youngemale a case reportrdquo Cases Journal vol 983090 no 983097 article 983096983096983092983089983090983088983088983097
[983090] J Sell M R Williamson R D Boutin and B J IgelldquoC demonstration o a giant adrenal endothelial cyst o the angiomatous subtyperdquo Computerized Medical Imaging and Graphics vol 983089983096 no 983094 pp 983092983094983097ndash983092983095983089 983089983097983097983092
[983091] A Wedmid and M Palese ldquoDiagnosis and treatment o theadrenal cystrdquo Current Urology Reports vol 983089983089 no 983089 pp 983092983092ndash983093983088983090983088983089983088
[983092] L J Medeiros K B Lewandrowski and A L Vickery ldquoAdrenalpseudocyst a clinical and pathologic study o eight casesrdquoHuman Pathology vol 983090983088 no 983095 pp 983094983094983088ndash983094983094983093 983089983097983096983097
[983093] L M Neri and F C Nance ldquoManagement o adrenal cystsrdquo American Surgeon vol 983094983093 no 983090 pp 983089983093983089ndash983089983094983091 983089983097983097983097
[983094] H P Chien Y S Chang P S Hsu et al ldquoAdrenal cysticlesions a clinicopathological analysis o 983090983093 cases with proposedhistogenesis and review o the literaturerdquo Endocrine Pathology vol 983089983097 no 983092 pp 983090983095983092ndash983090983096983089 983090983088983088983096
[983095] R Bellantone A Ferrante M Raffaelli M Boscherini C PLombardi and F Crucitti ldquoAdrenal cystic lesions report o 983089983090surgically treated cases and review o the literaturerdquo Journal of Endocrinological Investigation vol 983090983089 no 983090 pp 983089983088983097ndash983089983089983092 983089983097983097983096
[983096] P V Pradeep A K Mishra V Aggarwal P R K BhargavS K Gupta and A Agarwal ldquoAdrenal cysts an institutionalexperiencerdquo World Journal of Surgery vol 983091983088 no 983089983088 pp 983089983096983089983095ndash983089983096983090983088 983090983088983088983094
[983097] H Sanal M Kocaoglu D Yildirim et al ldquoImaging eatureso benign adrenal cystsrdquo European Journal of Radiology vol 983094983088no 983091 pp 983092983094983093ndash983092983094983097 983090983088983088983094
[983089983088] D G Foster ldquoAdrenal cysts Review o literature and report o caserdquo Archives of Surgery vol 983097983090 no 983089 pp 983089983091983089ndash983089983092983091 983089983097983094983094
[983089983089] G A Abeshouse R B Goldstein and B S Abeshouse ldquoAdrenalcysts Review o the literature and report o three casesrdquo Journal of Urology vol 983096983089 pp 983095983089983089ndash983095983089983097 983089983097983093983097
[983089983090] N Singh R K George S K Gupta A Gupta and A AgarwalldquoGiant adrenal cyst presenting as a diagnostic dilemma a casereportrdquo International Surgery vol 983097983088 no 983090 pp 983095983096ndash983096983088 983090983088983088983093
[983089983091] Y K Guo Z G Yang Y Li et al ldquoUncommon adrenalmasses C and MRI eatures with histopathologic correlationrdquoEuropean Journal of Radiology vol 983094983090 no 983091 pp 983091983093983097ndash983091983095983088 983090983088983088983095
[983089983092] G De oma R Gabriele M Plocco and P Sapienza ldquoAdrenalcysts therapeutical indicationsrdquo Minerva Chirurgica vol 983093983088no 983089983088 pp 983097983090983093ndash983097983090983096 983089983097983097983093
Submit your manuscripts at
httpwwwhindawicom

Case Reports in Surgery 983091
[983090 983091 983096] rue adrenal cysts account or 983092983088 o the cases andcan present as endothelial cysts and epithelial cysts and rarely as vascular cysts or cystic lymphangiomas [ 983091 983096]
Most o the adrenal cysts are asymptomatic and canbe diagnosed incidentally more commonly situated in theright side and can be detected more requently in emalepatients [983091 983096] Te size o the adrenal cysts can vary rom ew millimeters up to 983093983088 cm in diameter [983097] Most o the adrenalcysts are unilateral with 983096ndash983089983093 that can present bilaterally [983095] Te majority o cases are diagnosed between the 983091rd and983093th decades [983089983088 983089983089] An adrenal cyst located in the lef side canbe conused or a pancreatic pseudocyst while a right-sidedadrenal cyst can be conused or a liver cyst [983089983090] as presentedin this case
Investigations can range rom hormonal workup to radi-ological modalities C scan is the investigation o choice orthe diagnosis o adrenal cysts It can show the location o thecyst reveal the density and de1047297ne the wall borders MRI issuperior in the differential diagnosis and in distinguishingbetween an adrenal lesion and a renal lesion [ 983089983091] Hormonalworkup in the orm o a 983090983092-hour urinary metanephrineserum potassium or three consecutive days a low-dosedexamethasone suppression test and aldosterone renin ratiois necessary in all cases o adrenal cysts in order to diagnoseunctional disease that is not clinically detected [ 983096]
Adrenal cysts can be managed either conservatively or by surgical excision Management is dependent on theunctional status o the cyst the probability o malignancyand complications such as hemorrhage or inection o thecyst [983089 983091 983092] Excision or aspiration o the adrenal cyst isrecommended i the patient is symptomatic and presentingwith endocrine abnormalities or with rapid expansion o the cyst and when malignancy cannot be ruled out [983089983092]In addition Bellantone et al have recommended surgicalresection o cysts that are greater than 983093 cm due to therisk o hemorrhage and inection [983095] Surgical resection willdecrease the incidence o uture complications in the orm o hemorrhage into the cyst local pressure effect and inectiono the cyst and to exclude the possibility o malignancy [ 983089]
4 Conclusion
Adrenal cysts should be considered in the differential diag-nosis when dealing with upper abdominal cysts Althoughmost adrenal Cysts are benign in nature surgical excision isadvisable especially when the cysts are larger than 983093 cm indiameter and there is a suspicion o malignancy
Consent
Written inormed consent was obtained rom the patient orpublication o this case report and accompanying images Acopy o the written consent is available or review on request
Conflict of Interests
All authors have no con1047298ict o interests
References
[983089] M R Khan S Ajmal and Saleem ldquoGiant adrenal endothelialcyst associated with acute and chronic morbidity in a youngemale a case reportrdquo Cases Journal vol 983090 no 983097 article 983096983096983092983089983090983088983088983097
[983090] J Sell M R Williamson R D Boutin and B J IgelldquoC demonstration o a giant adrenal endothelial cyst o the angiomatous subtyperdquo Computerized Medical Imaging and Graphics vol 983089983096 no 983094 pp 983092983094983097ndash983092983095983089 983089983097983097983092
[983091] A Wedmid and M Palese ldquoDiagnosis and treatment o theadrenal cystrdquo Current Urology Reports vol 983089983089 no 983089 pp 983092983092ndash983093983088983090983088983089983088
[983092] L J Medeiros K B Lewandrowski and A L Vickery ldquoAdrenalpseudocyst a clinical and pathologic study o eight casesrdquoHuman Pathology vol 983090983088 no 983095 pp 983094983094983088ndash983094983094983093 983089983097983096983097
[983093] L M Neri and F C Nance ldquoManagement o adrenal cystsrdquo American Surgeon vol 983094983093 no 983090 pp 983089983093983089ndash983089983094983091 983089983097983097983097
[983094] H P Chien Y S Chang P S Hsu et al ldquoAdrenal cysticlesions a clinicopathological analysis o 983090983093 cases with proposedhistogenesis and review o the literaturerdquo Endocrine Pathology vol 983089983097 no 983092 pp 983090983095983092ndash983090983096983089 983090983088983088983096
[983095] R Bellantone A Ferrante M Raffaelli M Boscherini C PLombardi and F Crucitti ldquoAdrenal cystic lesions report o 983089983090surgically treated cases and review o the literaturerdquo Journal of Endocrinological Investigation vol 983090983089 no 983090 pp 983089983088983097ndash983089983089983092 983089983097983097983096
[983096] P V Pradeep A K Mishra V Aggarwal P R K BhargavS K Gupta and A Agarwal ldquoAdrenal cysts an institutionalexperiencerdquo World Journal of Surgery vol 983091983088 no 983089983088 pp 983089983096983089983095ndash983089983096983090983088 983090983088983088983094
[983097] H Sanal M Kocaoglu D Yildirim et al ldquoImaging eatureso benign adrenal cystsrdquo European Journal of Radiology vol 983094983088no 983091 pp 983092983094983093ndash983092983094983097 983090983088983088983094
[983089983088] D G Foster ldquoAdrenal cysts Review o literature and report o caserdquo Archives of Surgery vol 983097983090 no 983089 pp 983089983091983089ndash983089983092983091 983089983097983094983094
[983089983089] G A Abeshouse R B Goldstein and B S Abeshouse ldquoAdrenalcysts Review o the literature and report o three casesrdquo Journal of Urology vol 983096983089 pp 983095983089983089ndash983095983089983097 983089983097983093983097
[983089983090] N Singh R K George S K Gupta A Gupta and A AgarwalldquoGiant adrenal cyst presenting as a diagnostic dilemma a casereportrdquo International Surgery vol 983097983088 no 983090 pp 983095983096ndash983096983088 983090983088983088983093
[983089983091] Y K Guo Z G Yang Y Li et al ldquoUncommon adrenalmasses C and MRI eatures with histopathologic correlationrdquoEuropean Journal of Radiology vol 983094983090 no 983091 pp 983091983093983097ndash983091983095983088 983090983088983088983095
[983089983092] G De oma R Gabriele M Plocco and P Sapienza ldquoAdrenalcysts therapeutical indicationsrdquo Minerva Chirurgica vol 983093983088no 983089983088 pp 983097983090983093ndash983097983090983096 983089983097983097983093
Submit your manuscripts at
httpwwwhindawicom

Submit your manuscripts at
httpwwwhindawicom