-
7/28/2019 AL STRABISMUS Final- Dr Ahmad Lotfi
1/21
Ocular Motility and Strabismus
Introduction:
As the eyes can see only objects in front of them in their field
of vision, they
have to move or rotate so that they can see wider fields. So for
the function of
the eyes to see, they have to be able to rotate to follow the
moving objects and
to see different objects in different locations in the
environment. Visual
stimulation of the retina initiates ocular movements to follow
the movingtargets and to stop the movements or fixate the eyes when
the target objects
stop moving. The ocular motility is as essential as the function
of vision
(imagine what would have been the situation if the eyes were
fixed organs like
the nose and the ears). The eye rotates around three axes in
three meridians;
the eye rotates horizontally (adduction and abduction) around a
vertical axis
and rotates vertically (elevation and depression) around a
horizontal axis and
torsionally (incyclotorsion and excyclotorsion) around an
anteroposterior axis.
This ocular motility is the function of the extraocular muscles
and their higher
cortical and supranuclear control. Each eye has six extraocular
muscles, fourrectus muscles and two oblique ones. The twelve
extraocular muscles (of both
eyes) act in a marvelous harmony through the higher central
control moving
both eyes at one and the same time and for the same distance
through the same
velocity. This is essential for what is called single binocular
vision and that is
why nobody can move only one eye while fixating the other one
(one can move
only one arm, only one leg but cannot move only one eye!!!! Can
you??). So,
we can believe that we have only one seeing organ divided into
two halves; the
right eye and the left eye.
The optical axis and the visual axis
The optical axis is an anatomical axis passing through the
anterior pole of the
eye to the posterior pole. The visual axis on the other hand- is
a physiological
axis. It starts from the fovea centralis (the most sensitive
area of the retina) and
passes through the nodal point of the crystalline lens (the
functional centre of
the lens) to cut the optical axis nasally making an angle of 5
degrees with it
(angle kappa). The eye rotates so that the visual axis is
directed to the object of
regard. This small angle (angle kappa) solves the problem of
having the eyes
anatomically parallel (simply look parallel) while the eyes are
physiologically
-
7/28/2019 AL STRABISMUS Final- Dr Ahmad Lotfi
2/21
converging so that the visual axes can meet at the object of
regard (parallel
lines simply do not meet at all). That is the advantage of
having the fovea
centralis deviated in the temporal retina so that the two visual
axes are
converging while the eyes are anatomically parallel. If the
fovea centralis were
in the posterior pole, the eyes would have been ALWAYS
converging lookinglike having convergent strabismus.
Fig 1: Optic axis and visual axis
The normal position of the eyes (orthotropia)
The eyes are normally placed so that the two visual axes are
directed toward
the object of regard i.e. the two visual lines normally transect
or cross at the
object of regard. Most of the time, the eyes are not parallel
and that is normal
because the two eyes are directed to one object which means that
the eyes are
converging towards that object. The eyes are only parallel while
looking at a
distant object but not so when looking at a near one and both
are normalpositions of the eyes. The corner stone is that the two
visual axes are directed to
the object of regard and so they meet at that object.
Ocular motility; Herings law and Sherringtons law:
The eyes move freely in its place so that the cornea can be
directed towards the
object of interest. The eyes can move horizontally, vertically
and even
torsionally like the case of a ball and socket joint. That is
why the optic nerve
-
7/28/2019 AL STRABISMUS Final- Dr Ahmad Lotfi
3/21
has a tortuous course in the orbit so that it is not stretched
when the eyes
rotate.
Twelve extraocular muscles with their higher control are
responsible for that
accurate ocular motility. That is why the extraocular muscles
have very rich
nerve supply and sophisticated supranuclear and cortical
control.According to Herings law; the yoke muscles receive equal
and simultaneous
stimulation. The yoke muscles are one muscle from each eye that
are
responsible for rotating the eyes in one direction of gaze e.g.
the medial rectus
of the right eye and the lateral rectus of the left eye are
responsible for moving
both eyes to the left side (left gaze) and they are called yoke
muscles. It was
clearly stated for the first time by Alhacenin hisBook of
Optics. Because of
this law one cannot move only one eye while fixating the other
one. This is also
essential for the coordination of the movement of both eyes for
maintenance of
binocular single vision.For the eyes to rotate in its place,
contraction of one muscle should be
accompanied by relaxation of its antagonist e.g. to rotate the
eye inwards, the
medial rectus should be stimulated while lateral rectus should
relax.
Sherrington describes this phenomenon in his law of reciprocal
innervation. He
stated that; stimulation of one muscle is accompanied by equal
and
simultaneous inhibition of its antagonist. So to look to the
right side, both the
right lateral rectus and the left medial rectus muscles should
have equal and
simultaneous stimulation (according to Herings law) and also
both the right
medial rectus and the left lateral rectus muscles should receive
equal and
simultaneous inhibition (according to Sherringtons law).
Binocular single vision
It is defined as the coordinated use of the two eyes in order to
produce a single
visual mental impression leading to a full three dimensional
vision or
stereopsis. This requires both sensory and motor coordination of
both eyes.
Motor coordination of the two sets of extraocular muscles is
essential so that
the eyes can be moved voluntarily or reflexly with great
precision and perfect
alignment in any desired direction. Sensory coordination between
the two
retinae is essential so that the corresponding retinal points
are simultaneously
used and stimulated by the same object.
Corresponding retinal points are one point in the right retina
and one point in
the left retina that have the same visual pathway and the same
cortical destiny.
Each point of the retina of the right eye has a corresponding
point in the retina
of the left eye. The most important two corresponding points are
the two foveae.
The object of regard is fixated by the two foveae. Any object to
the right side of
the object of regard stimulates a point nasal to the fovea of
the right eye and a
point temporal to the fovea of the left eye. Those two points
are correspondingretinal points. At the level of the optic chiasm,
the nasal fibers of both sides
http://en.wikipedia.org/wiki/Ibn_al-Haythamhttp://en.wikipedia.org/wiki/Book_of_Opticshttp://en.wikipedia.org/wiki/Ibn_al-Haythamhttp://en.wikipedia.org/wiki/Book_of_Optics
-
7/28/2019 AL STRABISMUS Final- Dr Ahmad Lotfi
4/21
cross to the opposite side so that they run with temporal fibers
of the other
retina in the optic tract. So the optic tract carries the fibers
of the
corresponding retinal points and this continues through the
visual pathway till
the occipital cortex where fusion of the two images takes place.
For the cortex
to be able to fuse the two retinal images of the same object,
the object muststimulate two corresponding points otherwise the
object will be seen double.
This is the case if one eye deviates because at that situation
the objects will not
simulate corresponding retinal points.
Grades of binocular visionGrade I, simultaneous perception is
the ability to see at one and the same time
two dissimilar images, one formed on each retina, but not
necessarily
superimposed.
Grade II, fusion is the mental ability to blend two similar
images falling oncorresponding retinal points, one image being
formed on each retina, and
perceive them as one.
Grade III, stereopsis is the appreciation of depth brought about
primarily by
the fusion of the two images received by slightly disparate
points on the two
retina.
Following reflex and fixation reflex
The most important source of reflex tonus to the extraocular
muscles comesfrom the visual impulses themselves. Changes in the
visual field, even when
of slight attention value, can be shown to produce marked
changes in the
extraocular muscle tone e.g. optokinetic nystagmus. So the
following reflex
simply makes the eyes move to track the moving object of regard
and keeps
it always fixated by the foveae of both retinae.
The fixation reflex comes into play after the object of regard
has been
captured by the foveae by means of the following reflex. This
reflex serves to
maintain the object on the fovea. The attention value of the
object of regard
determines to a great extent how active this reflex will be. The
stimulus of this
reflex is the sharp image of the object of regard when perceived
by the fovea
centralis and the response is the fixation of the eye at that
position. So, if a
child has a congenital disease affecting vision marked in both
eyes, this reflex
will not develop normally due to the absence of the its stimulus
which is the
sharp clear image. That is why cases with bilateral congenital
dense cataract
develop searching nystagmus.
Fusional reflexes
-
7/28/2019 AL STRABISMUS Final- Dr Ahmad Lotfi
5/21
For the visual cortex to be able to blend the two images, both
eyes should be
in a position so that objects are perceived by corresponding
retinal points
otherwise objects will be seen double. Doubling of the images is
the stimulus
for fusional reflexes. The response is reflex fine ocular
movements till the
objects are seen by corresponding retinal points to eliminate
diplopia. So, anydeviation of the eyes leads to capturing of
objects by non corresponding
retinal points and so the visual cortex cannot fuse the two
images with the
result of diplopia. This diplopia reflexly stimulates the
fusional reflexes to
realign the eyes so that objects stimulate corresponding retinal
points. Objects
are captured by corresponding retinal points only when the eyes
are in a
normal position where the two visual axes are directed to the
object of regard.
The extraocular muscles
Each eye has six extraocular muscles, four rectus and two
oblique muscles.
The four rectus muscles have common origins posteriorly from the
annulus
of Zinn and they insert anteriorly into the sclera some
millimeters from the
corneoscleral limbus. So when they contract they pull the
insertion point
backwards. The oblique muscles -on the other hand- originate
anteriorly (the
trochlea is the functional origin of the superior oblique and
the anteromedial
aspect of the floor of the orbit is the origin of the inferior
oblique) and insert
posteriorly. So when they contract they pull the insertion point
forwards. Thisis essential to keep the eye in its place when the
muscles contract as every
movement of the eye is caused by more than one muscle. If all
the extra
ocular muscles were originating posteriorly and inserting
anteriorly, any
ocular movement would have been associated with retraction of
the eyeball
and narrowing of the palpebral fissure.
The medial rectus muscle originates at the apex of the orbit
from theannulus of Zinn and inserts 5.5 mm from the limbus. It is
supplied by
oculomotor nerve and acts as an adductor of the globe.
The lateral rectus muscle originates also from the annulus of
Zinn andinserts 7.0 mm from the limbus. It is supplied by the
Abducent nerve and acts
as an abductor of the globe.
b
-
7/28/2019 AL STRABISMUS Final- Dr Ahmad Lotfi
6/21
Fig 2: Extra ocular muscles
Fig 3: Extra ocular muscle actions (left) and measurements
(right).
-
7/28/2019 AL STRABISMUS Final- Dr Ahmad Lotfi
7/21
Fig 4: Extra ocular muscles; from above and from below.The
superior rectus muscle has the same origin and inserts 8.0 mm
fromthe limbus. Its actions are; elevation, adduction and
intorsion. It is supplied
by the oculomotor nerve. It is supplied by the oculomotor
nerve.
The inferior rectus muscle also originates from the annulus of
Zinn andinserts 6.5 mm from the limbus. Its actions are depression,
adduction and
extorsion. It is supplied by the oculomotor nerve.
The superior oblique muscle originates above the annulus of Zinn
andtravels anteriorly till the trochlear and then turns backwards
and laterally to
be inserted in the upper lateral quadrant of the globe. Its
actions areintorsion, abduction and depression. It is supplied by
the trochlear nerve.
The inferior oblique muscle originates anteriorly from the bone
of thefloor of the orbit anteromedially and travels posteriorly and
laterally to be
inserted in the lower lateral quadrant of the globe. Its actions
are extorsion,
abduction and elevation. It is supplied by the oculomotor
nerve.
The extraocular muscles have special properties such as They
have very rich nerve supply e.g. the lateral rectus has
special cranial nerve that supplies the lateral rectus only.
They have very rich blood supply.
They have morel elastic fibers than the other striated
muscles so that muscle contractions and relaxations are
smooth.
They do not show signs of fatigue although they are
voluntary striated muscles. That is because only one tenth
of the muscle fibers is in action and the other nine tenths
are at rest.
-
7/28/2019 AL STRABISMUS Final- Dr Ahmad Lotfi
8/21
Strabismus or Heterotropia
DefinitionStrabismus is simply an ocular deviation. It can be
defined as an extraocular
muscle imbalance, dysfunction or disturbance (not necessarily
paralysis) so
that the two visual axes do not intersect at the object of
regard. Normally the
two visual axes are directed to the object of regard and so the
should meet at
the site of that object. If they do not meet there, strabismus
exists.
Etiology
This includes any of those obstacles that may impede the
development ormaintenance of the binocular perception and fusional
reflexes. Those
obstacles may be optical, sensory, motor or psychological.
1) Optical obstacles : these obstacles prevent the formation of
suitable
retinal images that can be successfully fused in the visual
cortex into a
single mental impression. Those obstacles include high
refractive
errors, anisometropia and aniseikonia. Opacities of the ocular
media
also cause optical obstacles that interfere with the correct
formation of
images on the retina leading, if bilateral to nystagmus, but if
unilateral
to concomitant strabismus.
2) Sensory obstacles : they include all causes of uniocular
defective vision
especially in infants and young children. These include failure
of
development or disease of the macula or other parts of the
visual
pathway. Prolonged uniocular activity as in occupations such as
watch
makers or microscopists may also lead to development of
strabismus.
Care should be taken in cases of unilateral congenital severe
ptosis and
also in cases of corneal ulcers in infants as prolonged
occlusion of one
eye may develop strabismus.
3) Motor obstacles : these prevent the adequate coordination of
the two
eyes. These include any disease of the muscles, myoneural
junctions,motor nerves or the supranuclear or cortical control
4) Psychological obstacles : any severe mental or physical
trauma is liable
to convert pre-existing latent strabismus into a manifest
one.
Classification of StrabismusStrabismus may be
1) True or
2) Apparent. Apparent strabismus is simply a false or pseudo
strabismus.
Pseudo strabismus may be due to epicanthus, wide
interpupillarydistance or high errors of refraction.
-
7/28/2019 AL STRABISMUS Final- Dr Ahmad Lotfi
9/21
True strabismus may be1) Manifest or
2) Latent.
Manifest strabismus may be1) Concomitant (where the angle of
deviation is equal in all directions of
gaze) or
2) Incomitant (where the angle of deviation is not equal in all
directions
of gaze) as in cases of paretic or restrictive strabismus.
Concomitant strabismus may be1) Accommodative,
2) Nonaccommodative or
3) Partially accommodative.
Accommodative strabismus may be1) Refractive,2) Non refractive
or
3) Mixed.
I. Heterophoria (latent strabismus)
Heterophoria or latent strabismus is defined as tendency of one
or both eyes
to deviate but this tendency is controlled by the fusional
reflexes to maintainbinocular single vision and to avoid diplopia.
When one eye deviates, the
images of the object of regard are not formed on corresponding
retinal points.
At this situation the visual cortex will not be able to fuse or
blend the two
images and so the object is seen double. This diplopia
stimulates the fusional
reflexes to readjust the extraocular muscle tone to keep the
visual axes
directed to the object of regard to maintain binocular single
vision and
eliminate diplopia. If one eye is covered, diplopia will not be
perceived if the
covered eye deviates. To summarize, there is tendency of one or
both eyes to
deviate but this deviation leads to diplopia. Diplopia
stimulates fusionalreflexes to realign the eyes and correct the
deviation.
So if the controlling reflexes are inhibited by any means, the
latent deviation
will be manifest. Covering one eye eliminates the binocular
diplopia and so
the controlling fusional reflexes will not act. In such a case
the deviation of
one eye will be manifest.
Types of heterophoria Esophoria; a latent tendency of visual
axis to deviate inwards i.e.
toward the nose.
Exophoria; a latent tendency of the visual axis to deviate
outwards i.e.away from the midline.
-
7/28/2019 AL STRABISMUS Final- Dr Ahmad Lotfi
10/21
Hyperphoria; a latent vertical deviation in which the visual
axis of one
eye tends to deviate upwards as compared with that of the other
eye.
Hypophoria; a latent tendency of the visual axis of one eye to
deviate
downwards as compared with that of the other eye.
Cyclophoria; a latent tendency of the vertical meridian of one
eye towheel-rotate inwards (incyclophoria) or outwards
(excyclophoria) from
the vertical position. Cyclophoria is usually associated with
hyper and
hypophoria.
Symptoms and signs of heterophoriaHeterophoria may be
symptomless but symptoms may arise when the effort,
required to maintain the eyes in orthotropia, becomes a
conscious effort.
Symptoms of heterophoria include;
Headaches or eye aches
Intermittent diplopia
Intermittent strabismus usually noticed by the relatives
Blurring of vision or running of the words into one another
while
reading
Nausea and giddiness
Feeling of heavy lids, redness of the conjunctiva
Etiology of heterophoria High errors of refraction where myopia
leads to exophoria while
hyperopia leads to esophoria
Wide orbits
Minor weakness of one or more of the extraocular muscles
Diagnosis of heterophoria
1. Cover- uncover test; by covering one eye, the binocular
diplopia will
not be seen and so controlling reflexes will not be initiated.
So, if thereis a tendency for deviation, it will show itself in the
form of deviation
of the eye under cover. When the cover is removed, binocular
diplopia
is perceived and in no time the fusional reflexes will correct
the
alignment of the eyes and so, the uncovered eye will be seen
moving
from the deviating position to the normal one. If the covered
eye is
deviating under cover and then corrects its position when
uncovered,
there is heterophoria.
2. Ocular movement testing; they are found to be normal.
3. Worths four dot test; five dots are seen, namely two red and
threegreen in cases of heterophoria.
-
7/28/2019 AL STRABISMUS Final- Dr Ahmad Lotfi
11/21
4. Maddox rod and tangent scale test; the Maddox rod is placed
in trial
frame before one eye with its cylinders horizontally aligned,
the other
eye remaining uncovered. The patient then looks at a spot white
light
in the tangent scale. If the patient is normal, a red light
appears to go
vertically through the spotlight. In the event of exophoria
oresophoria, the red line appears to be at one side of the
spotlight. Then,
the Maddox rod is rotated so that its cylinders become vertical.
Here
the red light appears horizontal. In orthophoria, the red light
appears
horizontally through the spotlight. In cases of Hyperphoria
or
hypophoria, the red line appears to be below or above the
spotlight
respectively. The amount of latent deviation is measured on a
tangent
scale.
Fig 5: Maddox rod test (right) and tangent scale (left)
5. The Maddox wing test; this is a test to measure the latent
deviation for
near fixation.
Fig 6: The Maddox wing test
-
7/28/2019 AL STRABISMUS Final- Dr Ahmad Lotfi
12/21
6. Assessment of binocular functions using Titmus fly stereotest
is found
to be normal in most cases. In a minority of cases it is found
to be
subnormal.
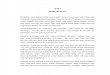
Fig 7: Titmus fly stereotest
Treatment of heterophoria:
1. Cases without symptoms; sometimes heterophoria is
discovered
accidentally during routine examination where it is not noticed
by the
patient or his relatives. In such a case, no treatment is needed
even it is
wise not to mention it to the patient.
2. Cases with symptoms;
Accurate correction of any refractive error may alleviate the
symptoms.
Orthoptic training for horizontal phorias may be tried before
prisms.
The use of prisms. A prism of an appropriate strength may
beincorporated with the glasses of the patient. The power of
prism
diopters needed is divided between the two eyes. Prisms are
more
beneficial for vertical phorias.
Surgical correction is indicated when the other modalities fail
to
correct the latent deviation.
II. Manifest StrabismusII.1. Paralytic strabismus
-
7/28/2019 AL STRABISMUS Final- Dr Ahmad Lotfi
13/21
If the ocular deviation is due to paralysis (complete loss of
movement) or
paresis (partial loss of movement) of one or more of the
extraocular muscles,
it is called paralytic or incomitant strabismus. Incomitance
means that the
angle of deviation is not the same in all directions of gaze. In
such a case the
eyes may be orthotropic in one direction of gaze and
heterotropic of differentdegrees in the other directions. The
deviation increases in the direction of
action of the affected muscle and decreases in the direction of
action of its
antagonist.
Etiology
It is due a lesion anywhere the nuclei of the third, fourth and
sixth cranial
nerves and the muscles themselves. The lesions may be due any of
the
following causes;
1. Congenital absence of the nerve nucleus or absence of the
muscle orits malinsertion.
2. Traumatic, either affecting the muscle or its nerve
supply.
3. Inflammatory, encephalitis, neuritis or DS.
4. Vascular, cerebral hemorrhage or thrombosis.
5. Toxic, alcohol, lead poisoning or diphtheria toxins.
6. Neoplastic, a tumor pressing on the nerve supply of the
muscle.
7. Myogenic, myasthenia gravis, thyrotoxic myopathy or
ocular
myopathy.
Symptoms1. Binocular diplopia; the patient sees everything
double when using both
eyes and sees normal when closing one eye. In cases of
horizontal
deviations, diplopia is crossed (heteronymous) in cases of
exotropia and
uncrossed (homonymous) in cases of esotropia.
2. Deviation of one eye and the deviation increases in certain
direction.
3. Vertigo, nausea and uncertain gait. These symptoms disappear
when
the patient closes one eye to avoid diplopia, so these symptoms
are due
to diplopia.
4. Abnormal head posture. This posture is adopted to avoid
diplopia andits distressing effects and in the interest of
maintaining binocular single
vision. Abnormal head posture is simply moving the head instead
of the
eye. When the right lateral rectus is paralyzed, the right eye
cannot
move to the right, so the head is turned to the right. Abnormal
head
posture may be horizontal (in the form of face turn to the right
or to the
left), vertical (in the form of chin elevation or depression) or
torsional
(in the form of head tilt to the right shoulder or to the left
one).
5. Past pointing; the patient does not see objects in their
correct locations
and so he cannot point to them correctly e.g. the patient
complains thathe cannot catch a pen on the desk, he might put his
hand in front,
-
7/28/2019 AL STRABISMUS Final- Dr Ahmad Lotfi
14/21
behind or beside the pen.
Signs1. Deviation of one eye; misalignment is obvious in one
direction and
less obvious in another direction. Deviation may disappear
incertain direction (the direction of action of the antagonistic
muscle).
This is called incomitant strabismus.
2. Limitation of ocular movement; limitation is seen in the
direction of
action of the affected muscle i.e. limitation of abduction in
cases of
lateral rectus palsy.
3. The secondary angle of deviation is greater than the primary
angle
of deviation. The primary angle is the deviation elicited when
the
patient fixes with the sound normal eye and the secondary angle
is
the deviation elicited when the patient fixes with the affected
eye.Considering Herings law explains this fact.
4. Compensatory head posture; in the form of face turn, chin
elevation
or depression or in the form of head tilt to one shoulder.
5. False projection; the paralysed eye does not see objects in
their
correct location due to increased innervation conveyed by the
nerve
supplying the paralysed muscle in an effort to force it to act.
False
projection can be demonstrated by asking the patient to close
his
sound eye and telling him to point quickly to an object in front
of
him. The finger will be directed to one side of the object
depending
on the direction of the main action of the affected muscle.
Pathological sequelae of paralysis of individual extraocular
muscles Contracture of the direct antagonist; this takes place
because
the contraction of the direct antagonist becomes unopposed.
Overaction of the contralateral synergist; this is due to
overstimulation of the affected muscle to force it to
contract.
According to Herings law, the contralateral synergist
receives also overstimulation leading to its overaction.
Inhibitional palsy of the contralateral antagonist; accordingto
Sherringtons law when the contralateral synergist receives
overstimulation its antagonist receives over-inhibition.
Paralysis of individual ocular muscles
Clinical picture of lateral rectus palsy (Abducent nerve
palsy)
Esotropia in the primary position
Limitation of abduction
-
7/28/2019 AL STRABISMUS Final- Dr Ahmad Lotfi
15/21
Esotropia increases on looking to the affected
side
Secondary angle of deviation is greater than the
primary angle
Uncrossed diplopia Face turn to the side of the affected
muscle
Fig.8: Right Abducent nerve palsy. There is esotropia of the
right eye in
the primary position (A) and limitation of abduction of the
right eye onright gaze (B)
2. Clinical picture of third nerve palsy Ptosis is present and
may mask diplopia if the lid covers the
pupillary area.
Limitation of elevation, depression and adduction
Large angle exotropia
Pupil may be dilated and fixed
Paralysis of accommodation with difficult near work
Crossed diplopia
-
7/28/2019 AL STRABISMUS Final- Dr Ahmad Lotfi
16/21
Fig.9: Third nerve palsy of the right eye (the ptosed upper lid
is elevated by
the examiner to show exotropia)
3. Clinical picture of trochlear nerve palsy Head tilt to the
opposite shoulder
Limitation of downward and inward movement
Hypertropia if the head is forced to tilt to the same side
shoulder
Hypertropia when looking to the opposite side
Fig. 10: Trochlear nerve palsy of the right eye where there is
Hypertropia in the primary
position (A) that increases when looking to the left (B) and
decreases when looking to the
right(C). Hypertropia increases when tilting the head to the
left (D) and decreases when
tilting the head to the left shoulder (E).
-
7/28/2019 AL STRABISMUS Final- Dr Ahmad Lotfi
17/21
Treatment of paralytic strabismusThe aim of treatment is as
follows:
To restore comfortable binocular single vision over as a large
an area
as possible.
To make the ocular movement as symmetrical and equal as
possible.
General principles in management of paralytic strabismus:
Treatment of the cause should be tried at first. It is wise to
allow enough time
for spontaneous recovery. It is advised to wait for 6 months
before deciding to
correct the deviation surgically. Surgical treatment is
indicated when there is
no hope of recovery (after 6 months of stability of the
condition) and before
development of the secondary changes as direct antagonist
contracture.
Surgical treatment is in the form of weakening of the direct
antagonist and
contralateral synergist. The contralateral antagonist might be
strengthened.
For example, in cases with lateral rectus paralysis, the direct
antagonist that
is the medial rectus should be recessed and the contra lateral
synergist that is
the medial rectus of the other eye should be also recessed.
Resection of the
affected muscle may be of help if the paralysis is not complete.
In cases with
complete paralysis, resection of the affected muscle might not
be of help and
in such cases muscle transposition is indicated.
II.2. Concomitant strabismus
It is a type of strabismus where the angle of deviation is
constant in all
directions of gaze. Concomitant strabismus may be accommodative,
non-
accommodative or partially accommodative.
II.2.a. Accommodative strabismus
It is a type of concomitant strabismus that is caused by
accommodation.
Accommodation is the ability of the eye (mainly the crystalline
lens) to
change its diopteric power to focus objects at different
distances from the eye.
As the object of regard approaches the eyes, the eyes have to do
two things;
first, the eyes have to converge to direct the visual axis to
the object and
second the eyes have to accommodate to focus the near object on
the retina.
There is a relationship between accommodation and its
accompanying
convergence where the eyes converge for 3-5 prism diopters for
each diopterof accommodation.
-
7/28/2019 AL STRABISMUS Final- Dr Ahmad Lotfi
18/21
Accommodative strabismus has the following criteria:
1. It has a late onset (around the age of 2-5 years). The late
onset is due to
the late development of accommodation reflex.
2. There is a high error of refraction (in the refractive and
mixed types)3. It starts as an intermittent esotropia then becomes
manifest
4. It is corrected by glasses
Fig 11: Accommodative esotropia (above) corrected with glasses
(below).
There are three types of accommodative esotropia:
1. Refractive type; where the deviation is due to the high
refractive error.
In such cases, when the error of refraction is corrected by
glasses, the
deviation is corrected both for distant and for near
fixation.
2. Non-refractive type; where the deviation is due to high AC/A
ratio. The
AC/A ratio is the ratio between accommodative convergence (AC)
and
accommodation (A). Normally there is equilibrium
betweenaccommodation and its convergence to keep the eyes directed
at the
object of regard (convergence) and at the same time to keep the
object
sharply focused on the retina (accommodation). If this
equilibrium is
disturbed with over convergence, the eyes will deviate with
normal
accommodation. In such cases there is minor error of refraction
and
the eyes are orthotropic in distant fixation and esotropia
appears only
in near fixation. Such cases are treated by bifocal glasses
where there
are two lenses in front of each eye, one upper lens and one
lower lens.
The lower segment lens has a power of 3 diopters more than the
upper
-
7/28/2019 AL STRABISMUS Final- Dr Ahmad Lotfi
19/21
segment lens. The lower segment functions to stop accommodation
at
near fixation which is the cause of overconvergence.
3. Mixed type; where there is an error of refraction causing
refractive
accommodative esotropia and also there is high AC/A ratio. In
such
cases, there is a small esotropia for distant fixation
(refractiveaccommodative esotropia) that increases markedly with
near fixation
(non refractive accommodative esotropia). In such cases,
bifocal
glasses are prescribed where the upper segment corrects the
error of
refraction (corrects the refractive element) and the lower
segment has a
power of extra 3 diopters (to stop accommodation for near that
is
responsible for the marked increase in the esotropia for near
fixation
due to the high AC/A ratio).
II.2.b. Non accommodative concomitant strabismus
It is a type of concomitant strabismus not related to
accommodation and so
not corrected by glasses. It may start congenitally or at early
infancy where it
is called essential infantile esotropia. It may start later in
life where it is
usually due to decompensated latent strabismus or due to marked
loss of
vision in one eye .
Essential infantile esotropia
Essential infantile esotropia is the convergent strabismus that
dates since
birth or since early infancy. It is characterized by
Large angle of esotropia
Cross fixation where the infant fixates objects in the right
side of its field of vision by the left eye and objects in
the
left side of the field by the right eye.
Small usual error of refraction
Oblique muscle dysfunction A- and V- pattern deviation
Dissociated vertical deviation.
Latent or manifest-latent nystagmus
It is treated surgically by weakening of the two medial rectus
muscles with
-sometimes- strengthening of one or both lateral rectus
muscles.
II.2.c. Partially accommodative strabismus
It is a type of concomitant strabismus. It is due in part- to
accommodation
and so can be partially corrected by glasses both for distant
and near fixation.
-
7/28/2019 AL STRABISMUS Final- Dr Ahmad Lotfi
20/21
For example, if the patient has an angle of 30 degrees without
glasses and an
angle of 20 degrees (both for distant and near fixation) with
glasses, the
patient has partially accommodative strabismus. Such cases need
both optical
(glasses) and surgical treatments.
Surgical treatment of concomitant strabismus
To correct a concomitant deviation, one should weaken the muscle
pulling
the eye in the direction of deviation and strengthen its
antagonist e.g. in
esotropia the medial rectus should be weakened and the lateral
rectus should
be strengthened. Weakening of a muscle can be achieved through
recession
of its insertion. Strengthening can be achieved through
resection of some
millimeters of the muscle tendon. Resection of a muscle leads to
its stretching
and so increases its contractility according to Starlings law.
On the other
hand, recession of a muscle decreases its stretching and so
decreases its
power of contraction. Weakening can be achieved also through
partial
tenotomy or in some rare cases complete tenotomy. Strengthening
can also be
performed via tucking or folding of the muscle tendon and also
via
advancement of the tendon (the opposite to recession). The
amount of
resection and recession is determined according to the degree of
deviation;
the higher the degree of deviation in prism diopters the more
the amount of
resection and recession in millimeters.
Strabismic AmblyopiaAmblyopia (lazy eye) denotes diminished
visual acuity due to
impairment of foveal vision without demonstrable clinical or
structural
anomaly of the eye or the visual pathway. Strabismic
amblyopia
denotes reduced foveal vision as a result of manifest deviation
in one
eye. Amblyopia develops easier in younger children and also can
be
corrected easily in the younger ages. As the child is getting
older,
amblyopia develops with difficulty and at the same time is
corrected
with difficulty. That is why early development of strabismus (in
infants)
leads to deeper amblyopia than that which develops as a result
of
deviations starting in older children.
Strabismic amblyopia can be corrected by means of what is
called
occlusion therapy. Occlusion of the sound non amblyopic eye
forces
the brain to perceive images coming from the amblyopic eye.
By
repetition of occlusion for a long time the relationship between
the
amblyopic eye and the visual cortex is getting better and the
functional
loss of vision is corrected either completely or partially.
-
7/28/2019 AL STRABISMUS Final- Dr Ahmad Lotfi
21/21
Nystagmus
It is an involuntary rhythmic oscillatory movements of the eyes.
It is usually
bilateral; however it might be unilateral in an amblyopic
squinting eye whenthe sound eye is occluded.
Clinical types:1. Jerking nystagmus; oscillations consist of two
phases, a slow movement
in one direction followed be a quick correcting jerk in the
opposite
direction. Nystagmus is described as right, left, up or down
according to
the direction of the quick correcting phase.
2. Pendular nystagmus ; both phases are of equal speed i.e. to
and- fro
movements like a pendulum. This is usually of ocular origin due
to
defective central vision and is called searching nystagmus.3.
Rotatory nystagmus ; here the oscillatory movements occur around
the
optic axis (intortions and extortions).
Etiology of nystagmus:Nystagmus may be due to causes in the eyes
(ocular nystagmus), in the
labyrinth or due to central causes.
1. Ocular nystagmus ; it may be physiological (as end-gaze
nystagmus,
optokinetic nystagmus and latent nystagmus) or pathological
(as
searching nystagmus, congenital idiopathic nystagmus and
spasmus
nutans).
2. Vestibular or labyrinthine nystagmus; may be physiological in
cases of
caloric stimulation or Galvanic stimulation or with rotation of
the
head. It may be pathological in cases with labyrinthitis or
Meniere
disease. It is usually of the jerking type.
3. Central nystagmus; this is typically jerking nystagmus. It
may be due
to disturbance of the complex mechanism coordinating the
sensations
coming from the labyrinth and the eyes and controlling the
orientation
of the eye movements. It may be due to lesions of the brain
stem, the
cerebellum or the spinocerebellar tract.