Embed Size (px)
Citation preview

HCA Healthcare HCA Healthcare
Scholarly Commons Scholarly Commons
Internal Medicine Research & Publications
1-25-2020
An Atypical Presentation of IVC Thrombosis An Atypical Presentation of IVC Thrombosis
Samantha Gelman MD HCA Healthcare, [email protected]
Gregory Shimizu MD
Rajesh Gulati MD HCA Healthcare, [email protected]
Follow this and additional works at: https://scholarlycommons.hcahealthcare.com/internal-medicine
Part of the Cardiovascular Diseases Commons, Diagnosis Commons, and the Therapeutics Commons
Recommended Citation Recommended Citation Gelman S, Shimizu G, Kubomoto S. An atypical presentation of IVC thrombosis. Poster presented at: SGIM California-Hawaii Regional Meeting; January 25, 2020; Irvine, CA.
This Poster is brought to you for free and open access by the Research & Publications at Scholarly Commons. It has been accepted for inclusion in Internal Medicine by an authorized administrator of Scholarly Commons.

An Atypical Presentation of IVC ThrombosisSamantha Gelman, MD; Gregory Shimizu, MD; Scott Kubomoto, MD; Rajesh Gulati, MD
Internal Medicine Residency – Riverside Community Hospital / UC Riverside School of Medicine
Inferior vena cava (IVC) thrombosis is commonly caused byeither a congenital anomaly or an IVC filter that was notpreviously removed. Other causes include an inheritedthrombophilia or acquired. It is found in 2.6%-4% of patientswith lower extremity deep vein thrombosis (DVT). The mortalityrate of IVC thrombosis is twice as high as that of DVT.Morbidities include post-thrombotic syndrome (PTS), disablingvenous claudication, pulmonary embolism, and venousulceration. In one study the rate of recurrent DVT in iliocavalthrombosis was 73% in those with untreated residual outflowstenosis versus 13% in those who had stenting of residualstenosis. Here we present an atypical case of IVC thrombosis ina young male without any inherited or acquired risk factors.
Introduction
A 28-year-old male with no past medical history presents with persistent abdominal pain for two weeks. The pain has been gradually worsening with radiation to the back with associated symptoms of heaviness in bilateral lower extremities without any calf or leg tenderness. CT imaging demonstrated IVC thrombosis with extension into femoral and renal veins with retroperitoneal inflammation.
On admission, patient was found to have an elevated PTT 102.2, PT 16.8, fibrinogen of 885, D-dimer 1492, and a normocytic anemia. Patient was started on a heparin drip. Echocardiogram showed normal left ventricular function with an ejection fraction of 55-60%.
The patient underwent ultrasound guided venogram which demonstrated a thrombus extending from the left common iliac vein into the inferior vena cava. Reconstitution of the IVC was not seen and catheter directed thrombolysis was performed. Patient then had a percutaneous mechanical thrombectomy of the left common iliac vein and IVC followed by placement of a new thrombolysis catheter. He subsequently underwent balloon angioplasty of the IVC and left common iliac vein with success at opening peri-aortic venous collaterals draining the left common iliac vein.
Case description
The hypercoagulable work up for this patient was negative forFactor V Leiden, APCR, JAK 2 mutation, Protein C & S, AT-IIIdeficiency, Prothrombin Gene, SPEP, UPEP, and homocysteine.Patient was found to have a positive anti-cardiolipin antibodyhowever, was lost to follow up. The most likely etiology of histhrombotic event is anatomical secondary to ileocavalthrombosis. The patient was to be on indefinite anti-coagulation (Apixaban) despite this being his known firstthrombotic event.
This case presentation is unusual as it shows evidence of ayoung adult presenting with IVC thrombosis without anypredisposing factors. Most anatomical anomalies that areassociated with this condition are involved in one of threecategories infrarenal (i.e.: duplicate IVC), renal (accessory leftrenal vein) and suprarenal (congenital caval stenosis oratresia). It is important to include this diagnosis in yourdifferential even in younger age groups as it is associated withsignificant morbidity and mortality.
Discussion
Kenneth A Bauer, MD, Gregory YH Lip, MD (2019). Overview ofthe causes of venous thrombosis. UpToDate.
Mohamad Alkhouli, Mohammad Morad, Craig R. Narins, FarhanRaza and Riyaz Bashir (2016). Inferior Vena Cava Thrombosis.JACC. Vol 9, Issue 7.
Courtney M. Hollingsworth, Therese Mead (2019). InferiorVena Caval Thrombosis. StatPearls.
References
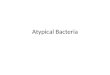
CT findings consistent with IVC thrombosis, note the extension in to the femoral and renal
veins
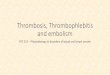
An example of the multimodal approach: A) Acute left ilio-femoral DVT. B)
Thrombolysis reveals pancaking of the left common iliac vein. C) Venoplasty and
stenting of the left common/external iliac vein.
Disclaimer: This activity was supported (in whole or in part) by HCA and/or an HCA affiliated entity. The views expressed in this publication represent those of the authors and do not necessarily represent the official views of HCA or any of its affiliated entities.