Embed Size (px)
Citation preview
Journal of Dermatology and Clinical Research
Cite this article: Kurtovic A, Sklar LR, Mehregan DA, Moiin A (2015) An Unusual Presentation of Facial Porokeratosis Presenting in a Child. J Dermatolog Clin Res 3(5): 1058.
Central
*Corresponding authorAli Moiin, Department of Dermatology, Wayne State University. 18100 Oakwood Boulevard, Suite 300, Dearborn, MI 48124, USA, Tel: 313-429-7845; E-mail:
Submitted: 31 August 2015
Accepted: 09 September 2015
Published: 11 September 2015
Copyright© 2015 Moiin et al.
OPEN ACCESS
Keywords•Porokeratosis•Facial•Child
Case Report
An Unusual Presentation of Facial Porokeratosis Presenting in a ChildAdnan Kurtovic, Lindsay R Sklar, David A Mehregan and Ali Moiin*Department of Dermatology, Wayne State University, USA
Abstract
We report the case of a 14-year-old African American male who presented with a four-month history of a slowly growing asymptomatic plaque on his face. Physical exam revealed a solitary hyper pigmented plaque that extended from the glabella to the right nasal ala in a linear and confluent manner down the right nasal sidewall. The plaque was lichenified and well demarcated with a distinctive hyperkeratosis ridge like border. Initial biopsy was non-specific. After failing the therapy, a repeated biopsy was done which revealed porokeratosis.
ABBREVIATIONSPM: Porokeratosis of Mibelli; DSAP: Disseminated
Superficial Actinic Porokeratosis; DSP: Disseminated Superficial Porokeratosis; PEODDN: Porokeratotic Eccrine Ostial and Dermal Duct Nevus
INTRODUCTIONPorokeratosis is a disorder of keratinization with the rare
potential of malignant transformation. At least five clinical variants of porokeratosis have been described which include disseminated superficial actinic porokeratosis (DSAP), disseminated superficial porokeratosis (DSP), porokeratosis of Mibelli (PM), linear porokeratosis, porokeratosis plantaris Palmaris et disseminata, and punctate porokeratosis. These variants are unified by a characteristic thin hyperkeratotic rim surrounding a slightly atrophic macule or patch which may spread centrifugally [1]. This distinctive border is known histologically as the “cornoid lamella”. The cornoid lamella is a thin column of parakeratosis overlying an interrupted granular layer and dyskeratotic keratinocytes [2]. The center of the lesion may reveal an atrophic, normal, or acanthotic epidermis. Porokeratosis presenting exclusively on the face is extremely rare and exclusive facial presentation in a child is exceptionally rare. We herein report the third case of exclusive facial porokeratosis presenting in a child.
CASE PRESENTATIONA 14-year-old African American male with no past medical
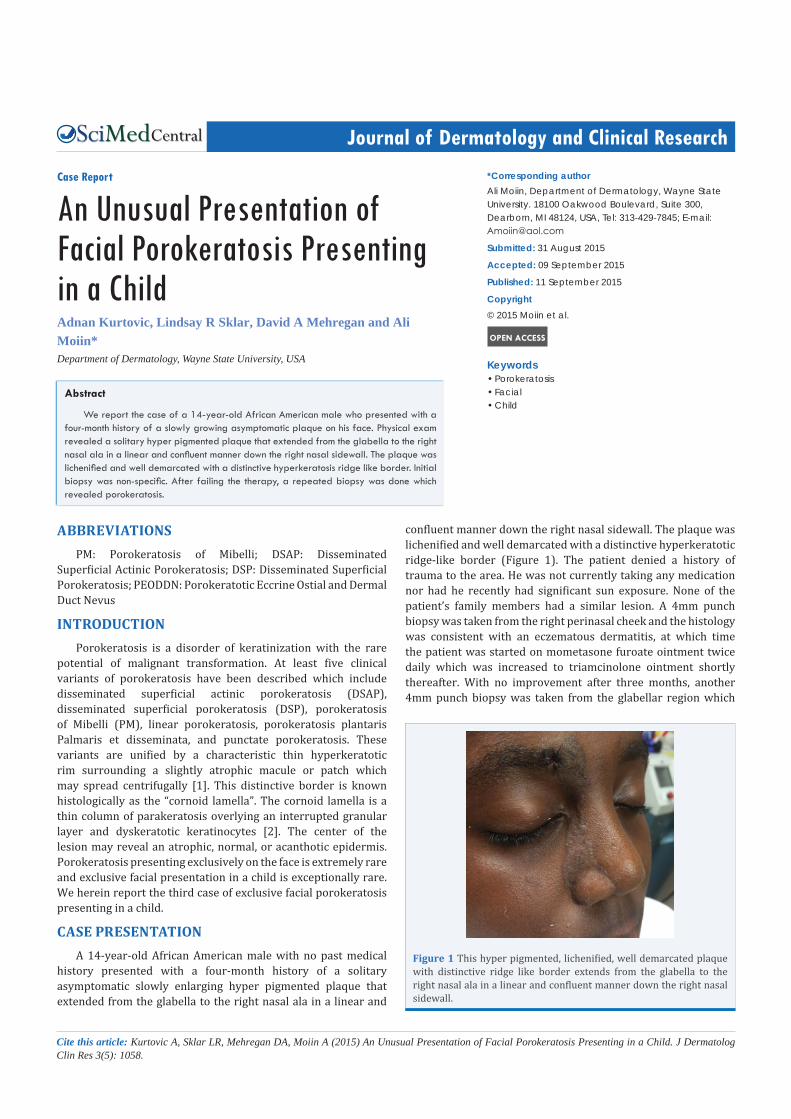
history presented with a four-month history of a solitary asymptomatic slowly enlarging hyper pigmented plaque that extended from the glabella to the right nasal ala in a linear and
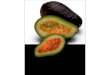
confluent manner down the right nasal sidewall. The plaque was lichenified and well demarcated with a distinctive hyperkeratotic ridge-like border (Figure 1). The patient denied a history of trauma to the area. He was not currently taking any medication nor had he recently had significant sun exposure. None of the patient’s family members had a similar lesion. A 4mm punch biopsy was taken from the right perinasal cheek and the histology was consistent with an eczematous dermatitis, at which time the patient was started on mometasone furoate ointment twice daily which was increased to triamcinolone ointment shortly thereafter. With no improvement after three months, another 4mm punch biopsy was taken from the glabellar region which
Figure 1 This hyper pigmented, lichenified, well demarcated plaque with distinctive ridge like border extends from the glabella to the right nasal ala in a linear and confluent manner down the right nasal sidewall.

Moiin et al. (2015)Email:
J Dermatolog Clin Res 3(5): 1058 (2015) 2/3
Central
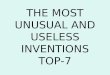
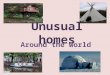
revealed a column of parakeratotic cells within a keratin filled epidermal invagination overlying an absent granular layer and dyskeratotic keratinocytes (Figure 2 A,B). With the diagnosis of porokeratosis, the patient was started on clobetasol ointment twice daily .At three months follow up; the lesion had decreased in both size and extent of hyperpigmentation (Figure 3). The clinical improvement may be explained by the increased strength of the topical steroid from triamcinolone ointment to clobetasol ointment.
DISCUSSION Porokeratosis of Mibelli (PM) is the second most common type
of porokeratosis, following DSAP. There is a 2:1 male to female predominance. PM most frequently appears during childhood as a small asymptomatic, painful, or pruritic papule that slowly expands over years to reach a size of a few centimeters but may expand up to 20 centimeters in diameter. The typical presentation is that of a hypo pigmented or hyper pigmented slightly atrophic plaque surrounded by a distinctive hyperkeratotic ridge. Lesions of PM are usually located unilaterally on an extremity however other locations have been less commonly reported. Malignant
transformation, most commonly squamous cell carcinoma, is estimated to occur in 7.5 to 11 percent of patients with porokeratosis [3]. Thus, patients with porokeratosis should be followed closely for signs of malignancy.
There are several features that make this case of porokeratosis unique, most notably, the exclusive facial presentation. While 15% of patients with DSAP may have facial lesions, exclusive facial presentation of porokeratosis is exceptionally rare. In the first reported case of facial porokeratosis, Nabai and Mehregan described atrophic facial lesions presenting similarly to chronic discoid lupus erythematosus, however, this case was not exclusive to the face, as the patient also had porokeratosis on the hand [4]. In 1980, Mehregan et al., reported six cases of porokeratosis exclusively on the face [5].The case series of Mehregan et al., included the case of a 14-year-old male with porokeratosis extending from the left upper cutaneous lip to the nasal bridge; this was the first reported case of exclusive facial porokeratosis presenting in a patient under the age of 18 [5].A second case has since been documented by Chowdhury et al., in their description of a 15-year-old male with porokeratosis on the nasal bridge [6]. A total of 31 cases of exclusive facial porokeratosis have been reported since Mehregan’s initial case series, all but one of which presented in adulthood [6,7].
The lesion in the patient we report appeared blaschkolinear and for this reason, porokeratotic eccrine ostial and dermal duct nevus (PEODDN) should be considered in the differential diagnosis. PEODDN is a very rare disorder of keratinization with clinical and histological overlap with several porokeratotic dermatoses. PEODDN favors locations where pilosebaceous units are absent, such as the palms and soles. It has a propensity to present in a blaschko linear configuration. The cornoid lamella in PEODDN is limited to the acrosyringia which distinguishes it from other forms of porokeratosis which may or may not involve the acrosyringia [8]. Our patient’s facial presentation and lack of acrosyringial involvement on histopathology makes PEODDN an unlikely diagnosis.
The patient reported herein was an African American adolescent who presented with a hyperkeratotic plaque on the face. Historically, dark-skinned people are rarely affected by porokeratosisand very few cases of porokeratosis presenting as hyperkeratotic and verrucous thick plaques have been reported which further promotes the uniqueness of this case [3,9,10].It is important to note that the initial biopsy did not reveal the cornoid lamella of porokeratosis, which resulted in a misdiagnosis of a dermatitis. This was likely due to the fact that the border of the plaque was not adequately sampled. When a presumed diagnosis of dermatitis does not respond to topical steroids, it is crucial to consider other diagnoses and a repeat biopsy.
While the patient’s lesion did improve with a stronger topical steroid, it must be noted that the clinical improvement seen with topical steroids often only temporary. There is also some concern that topical corticosteroids may induce proliferation of porokeratosis via immunosuppressive effects [11]. While treatment is generally not required, many patients desire treatment for either symptomatic or cosmetic concerns. For patients with small lesions, physical modalities such as cryotherapy, electrodessication and curettage, or excision are
Figure 3 At 3 months follow up, the lesion has decreased in size, thickness, and extent of hyperpigmentation.
A) B)
Figure 2 A 4mm punch biopsy revealing a column of parakeratotic cells within a keratin filled epidermal invagination overlying an absent granular layer and dykeratotic keratinocytes (A). A higher power view of the cornoid lamella (B).

Moiin et al. (2015)Email:
J Dermatolog Clin Res 3(5): 1058 (2015) 3/3
Central
Kurtovic A, Sklar LR, Mehregan DA, Moiin A (2015) An Unusual Presentation of Facial Porokeratosis Presenting in a Child. J Dermatolog Clin Res 3(5): 1058.
Cite this article
recommended, however there is a risk of pigment changes and scarring. For patients with larger lesions, topical 5-FU or imiquimod are treatment options.
This case report should serve as a reminder to physicians to keep porokeratosis in their differential diagnosis if a distinctive hyperkeratotic ridge is seen at the border of a plaque despite potential unusual presenting features such as a lichenified plaque instead of an atrophic plaque or an uncommon exclusive facial presentation in a child. If porokeratosis is in the differential, the border of the lesion must be biopsied to detect the cornoid lamella. It is important not to miss a diagnosis of porokeratosis, as these patients do require long term follow up to monitor for development of malignancy.
REFERENCES1. Kanitakis J, Euvrard S, Faure M, Claudy A. Porokeratosis and
immunosuppression. Eur J Dermatol. 1998; 8: 459-465.
2. Wade TR, Ackerman AB. Cornoid lamellation. A histologic reaction pattern. Am J Dermatopathol. 1980; 2: 5-15.
3. Sertznig P, von Felbert V, Megahed M. Porokeratosis: present concepts. J Eur Acad Dermatol Venereol. 2012; 26: 404-412.
4. Nabai H, Mehregan AH. Porokeratosis of Mibelli. A report of two unusual cases. Dermatologica. 1979; 159: 325-331.
5. Mehregan AH, Khalili H, Fazel Z. Mibelli’s porokeratosis of the face. A report of seven cases. J Am Acad Dermatol. 1980; 3: 394-396.
6. Chowdhury MM, Inaloz HS, Holt PJ. A scaly macule on the bridge of the nose of a 15-year-old boy. Pediatr Dermatol. 2000; 17: 149-150.
7. Gutierrez EL, Galarza C, Ramos W, Tello M, De Paz PC, Bobbio L, et al. Facial porokeratosis: A series of six patients. Australas J Dermatol. 2010; 51: 191-194.
8. Wang NS, Meola T, Orlow SJ, Kamino H. Porokeratotic eccrine ostial and dermal duct nevus: a report of 2 cases and review of the literature. Am J Dermatopathol. 2009; 31: 582-586.
9. Koley S, Sarkar J, Choudhary S, Dhara S, Choudhury M, Bhattacharya S. Different morphological variants of hypertrophic porokeratosis and disseminated lesions of porokeratosis of Mibelli: a rare co-existence. Indian J Dermatol Venereol Leprol. 2011; 77: 199-202.
10. Thomas C, Ogboli MI, Carr RA, Charles-Holmes R. Hypertrophic perianal porokeratosis in association with superficial actinic porokeratosis of the leg. Clin Exp Dermatol. 2003; 28: 676-677.
11. Sertznig P, von Felbert V, Megahed M. Porokeratosis: present concepts. J Eur Acad Dermatol Venereol. 2012; 26: 404-412.