-
7/29/2019 Angiolymphoid Hyperplasia With Eosinophilia, F 55,
Lower Lip, PPT
1/21
Angiolymphoid Hyperplasia with
Eosinophilia
Spencer Rusin M4, CUMC
Deba P Sarma, MDOmaha
-
7/29/2019 Angiolymphoid Hyperplasia With Eosinophilia, F 55,
Lower Lip, PPT
2/21
Patient Presentation
F 55, presents with a 10-month history of :
Non-ulcerated, painless nodule (0.5 cm)on her lower lip
No history of trauma or ear-nose-throatdisease.
-
7/29/2019 Angiolymphoid Hyperplasia With Eosinophilia, F 55,
Lower Lip, PPT
3/21
Differential Diagnosis
Mucocele
Lymphocytoma cutis
Granuloma faciale Benign and malignant tumors of skin and
adnexae
Kimura disease
Others
-
7/29/2019 Angiolymphoid Hyperplasia With Eosinophilia, F 55,
Lower Lip, PPT
4/21
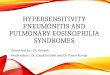
A well circumscribed
dermal nodule
composed of central
angiomatous vascular
proliferation with
stromal and peripheral
infiltrates of
lymphocytes andeosinophils.
H&E: low power
-
7/29/2019 Angiolymphoid Hyperplasia With Eosinophilia, F 55,
Lower Lip, PPT
5/21
Proliferation of small blood vessels, lined by
enlargedendothelial cells (epitheliod in appearance) with uniform
ovoid
nuclei and intracytoplasmic vacuoles.
-
7/29/2019 Angiolymphoid Hyperplasia With Eosinophilia, F 55,
Lower Lip, PPT
6/21
Prominent eosinophilic and lymphocytic infiltration
-
7/29/2019 Angiolymphoid Hyperplasia With Eosinophilia, F 55,
Lower Lip, PPT
7/21
Lymphoid aggregate with follicle formation amongst the
vascular proliferative cells.
-
7/29/2019 Angiolymphoid Hyperplasia With Eosinophilia, F 55,
Lower Lip, PPT
8/21
Immunostains
CD 3Peripheral lymphocytes: Positive
CD 20 - Peripheral lymphocytes: Positive
CD31Vascular epitheliod endothelial cells:Positive
CK AE1/3 - Negative
S-100 - Negative
-
7/29/2019 Angiolymphoid Hyperplasia With Eosinophilia, F 55,
Lower Lip, PPT
9/21
CD 31 stain highlights the endothelial cells demonstrating a
strong angiogenesis component to the nodule.
-
7/29/2019 Angiolymphoid Hyperplasia With Eosinophilia, F 55,
Lower Lip, PPT
10/21
Diagnosis
Angiolymphoid hyperplasia with eosinophilia
(ALHE)
-
7/29/2019 Angiolymphoid Hyperplasia With Eosinophilia, F 55,
Lower Lip, PPT
11/21
Differential Diagnosis
ALHE
Primarily a localizedhyperplasia
Infrequentlymphadenopathy
20%
Rare blood eosinophlia
Histology:
Vascularproliferation>inflammatory cells
Epitheliod endothelialcells lining bloodvessels
Eosinophils present
Kimura Disease
Systemic involvement: Lymphadenopathy
Blood eosinophlia Nephrotic syndrome as
a result of glomerularIgE deposition.
Histological presentation ofKimura disease differs fromALHE in
two factors.
Vascular proliferation
-
7/29/2019 Angiolymphoid Hyperplasia With Eosinophilia, F 55,
Lower Lip, PPT
12/21
ALHE
General presentation:
Range from asymptomatic to itchy orpainful erythematous nodules,
2-3cm indiameter.
The nodules may pulsate or bleed.
-
7/29/2019 Angiolymphoid Hyperplasia With Eosinophilia, F 55,
Lower Lip, PPT
13/21
Pre-auricular lesions of ALHE.
-
7/29/2019 Angiolymphoid Hyperplasia With Eosinophilia, F 55,
Lower Lip, PPT
14/21
ALHE Hypotheses regarding ALHEs origin:
Reactive process to insect bites
Hyperestrogen states
Immunologic mechanisms
Reactive vascular proliferation subsequent toinflammation
associated with traumatized blood
vessels One study reported a history of trauma in only 9%
of 116 patients with ALHE
-
7/29/2019 Angiolymphoid Hyperplasia With Eosinophilia, F 55,
Lower Lip, PPT
15/21
ALHE
Age: 20-50 years, M = F
Locations affected by ALHE:
Head and neck:
Specifically the forehead, scalp, and skin aroundears.
Trunk and genitalia
Three documented cases of ALHE affecting the lip.
-
7/29/2019 Angiolymphoid Hyperplasia With Eosinophilia, F 55,
Lower Lip, PPT
16/21
ALHE
Progression of ALHE:
Most common course: ALHE remains stable
Infrequent outcome: ALHE spontaneously
regresses Chronic nature of ALHE necessitates treatment.
Recurrence rate ranges from 33-50%
-
7/29/2019 Angiolymphoid Hyperplasia With Eosinophilia, F 55,
Lower Lip, PPT
17/21
Treatment
Medical:
Isoretinoin
Corticosteroids
interferon alfa-2b Benefits:
Improved cosmetic outcomes
Limitations:
Relies on patient compliance Not a permanent cure
-
7/29/2019 Angiolymphoid Hyperplasia With Eosinophilia, F 55,
Lower Lip, PPT
18/21
Treatment
Surgical:
Laser therapy
Carbon dioxide laser
Ultralong pulsed dye laser Nd:YAG laser
Benefits:
Improved cosmetic outcome
Limitations: Multiple treatments
Adversely affected by the depth of invasion orsize of
vessels
-
7/29/2019 Angiolymphoid Hyperplasia With Eosinophilia, F 55,
Lower Lip, PPT
19/21
Treatment
Surgical:
Excisional
Simple surgical excision
Mohs surgery Benefits:
Excision of the arterial and venous segments atthe base decrease
recurrence
Limitations:
Scarring
-
7/29/2019 Angiolymphoid Hyperplasia With Eosinophilia, F 55,
Lower Lip, PPT
20/21
References
S. Seregard, Angiolymphoid hyperplasia with eosinophilia should
not be confused withKimura's disease, Acta Ophthalmologica
Scandinavica, vol. 79, issue 1, pps. 9193, 2001.
S.W. Weiss, J.R. Goldblum, "Enzinger and Weiss's Soft Tissue
Tumors, 4th edition," St.Louis: Mosby, 2001. 863-864.
G.C. Wells, I.W. Whimster, "Subcutaneous angiolymphoid
hyperplasia with eosinophilia,British Journal of Dermatology, vol.
81, pp 1-15, 1969.
R.L. Moy, D.B. Luftman, Q.H. Nguyen, J.S. Amenta,"Estrogen
receptors and the response to
sex hormones in angiolymphoid hyperplasia with
eosinophilia,"Archives of Dermatology,vol 128, pp. 825-828, 1992.
R. Grimwood, J.M. Swinehart, J.L Aeling, "Angiolymphoid hyperplasia
with eosinophilia,"
Archives of Dermatology, vol. 115, pp. 205-207, 1979. P. Von den
Driesch, M. Gruschwitz, H. Schell, W. Sterry, Distribution of
adhesion
molecules, IgE, and CD23 in a case of angiolymphoid hyperplasia
with eosinophilia,Journal of the American Academy of Dermatology,
vol. 26, issue 5, part 2, pp. 799-804,1992.
T.G. Olsen, E.B. Helwig, "Angiolymphoid hyperplasia with
eosinophilia," Journal ofAmerican Academy of Dermatology, vol 12,
pp. 781-796, 1985.
P.G. Henry, J.W. Burnett, Angiolymphoid hyperplasia with
eosinophilia,Archives ofDermatology, vol. 114, no. 8, pp.
1168-1172, 1978. J.F. Fetsch, S.W. Weiss, Observations concerning
the pathogenesis of epithelioid
hemangioma (angiolymphoid hyperplasia), Modern Pathology, vol.
4, issue 4, pp. 449-455,1991.
T.G. Olsen, E.B. Helwig, Angiolymphoid hyperplasia with
eosinophilia. A clinicopathologicstudy of 118 patients, Journal of
the American Academy of Dermatology, vol. 12, issue 5,pp. 781-796,
1985.
J. Scurry, G. Dennerstein, J. Brenan, Angiolymphoid hyperplasia
with eosinophilia of thevulva,Australian and New Zealand Journal of
Obstetrics and Gynaecology, vol. 35, issue 3,
pp. 347-348, 1995.
f i d
-
7/29/2019 Angiolymphoid Hyperplasia With Eosinophilia, F 55,
Lower Lip, PPT
21/21
References continued
J.R. Srigley, A.G. Ayala, N.G. Ordonez, A.W. van Nostrand,
Epithelioid hemangioma of thepenis. A rare and distinctive vascular
lesion,Archives of Pathology and LaboratoryMedicine, vol. 109, pp.
51-54, 1985.
J.I. Lopez, S.B. Battaglino, Angiolymphoid hyperplasia with
eosinophilia of the lower lip,International Journal of Dermatology,
vol. 32, issue 5, pp. 361-362, 1993.
H. Suzuki, A. Hatamochi, M. Horie, T. Suzuki, S. Yamazaki, A
case of angiolymphoidhyperplasia with eosinophilia (ALHE) of the
upper lip, Journal of Dermatology, vol. 32, no.
12, pp. 991-995, 2005. O.F. Salinas, Y.S. Corredoira, G.A.
Rojas, Angiolymphoid hyperplasia of the lip with
eosinophilia. Report of one case, Revista Medica de Chile, vol.
135, no.5, pp. 636-639,2007. (in Spanish)
A. Satpathy, C. Moss, F. Raafat, R. Slator, Spontaneous
regression of a rare tumour in achild: angiolymphoid hyperplasia
with eosinophilia of the hand: case report and review ofthe
literature, British Journal of Plastic Surgery, vol. 58, issue 6,
pps. 865-868, 2005.
B.V. Diaz, M.C. Lenoir, A. Ladoux, C. Frelin, M. Demarchez, S.
Michel, Regulation ofvascular endothelial growth factor expression
in human keratinocytes by retinoids,Journal of Biological
Chemistry, vol. 275, no. 1, pps. 642-650, 2000.
F. El Sayed, R. Dhaybi, A. Ammoury, M. Chababi, Angiolymphoid
hyperplasia witheosinophilia: efficacy of isotretinoin?, Head &
Face Medicine, vol. 2, p. 32-36, 2006. T. Kaur, K. Sandhu, S.
Gupta, A.J. Kanwar, B. Kumar, Treatment of angiolymphoid
hyperplasia with eosinophilia with the carbon dioxide laser,
Journal of DermatologicalTreatment, vol. 15, issue 5, pps. 328-330,
2004.
C. Angel, A. Lewis, T. Griffin, E. Levy, A. Benedetto,
Angiolymphoid hyperplasiasuccessfully treated with an ultralong
pulsed dye laser, Dermatologic Surgery, vol. 31, pps.713-716,
2005.
C.J. Miller, M.D. Ioffreda, C.T. Ammirati, Mohs micrographic
surgery for angiolymphoidhyperplasia with eosinophilia,
Dermatological Surgery, vol 30,issue 8, pps. 1169-1173,2004.
T. Rohrer, A.Allan, ANgiolymphoid hyperplasia with eosinophilia
successfully treated witha long pulsed tunable dye laser
Dermatologic Surgery vol 26 issue 3 pps 211 214












![Endometrium presentation - Dr Wright[1] · Endometrial Hyperplasia Simple hyperplasia Complex hyperplasia (adenomatous) Simple atypical hyperplasia ... Progression of Hyperplasia](https://img.pdfslide.net/doc/110x75/5b8a421e7f8b9a50388bc13d/endometrium-presentation-dr-wright1-endometrial-hyperplasia-simple-hyperplasia.jpg)