Embed Size (px)
Citation preview

© 2010 SECOIRSociedad Española de Cirugía Ocular Implanto-Refractiva
Anterior segment optical coherence tomography in corneal and conjunctival pathology
Victoria de Rojas, MD, PhD1; Antía Gestoso, MD1; Isabel López, MD1; Jose� na Pombo, MD1; María López, MD1; Alejandra Gómez, MD1; Margarita de la Fuente, MD1
PURPOSE: To analyse the usefulness of anterior segment spectral domain optical coherence tomography (AS-OCT) in the diagnosis and surgical planning ofcorneal-conjunctival disease.
METHODS: Retrospective study which included patients examined using AS-OCT (HD-Cirrus) between June and December 2011. � e following information was obtained: diagnosis, surgical procedure, AS-OCT image usefulness/quality, biomicroscopy photographs. Cases were classi� ed into the following groups: 1. � e AS-OCT provided a satisfactory image and provided additional information to that obtained by biomicroscopy that was useful for diagnosis/surgery 2. � e OCT provided a satisfactory image but did not provide useful additional information for the diagnosis/surgery 3. � e OCT did not provide a satisfactory image.
RESULTS: � e OCT examination was conducted in 63 eyes of 53 patients with the following diagnoses/procedures, which were classi� ed into (n=number of eyes): Group 1: Descemet’s membrane detachment (4), corneal leukomas (1), penetrating keratoplasty (6), deep anterior lamellar keratoplasty (4), endothelial keratoplasty (1), intracorneal rings (6), corneal thickness assessment (6), infectious keratitis (4), corneal / conjunctival squamous neoplasia (4), Salzmann’s degeneration (2), conjunctival nevus (1). Group 2: Limbal cysts (1), hydrops (1), uveitis (1), guttata (3), bullous keratopathy (4), conjunctivochalasis (2), tear meniscus measurement (6), pterygium (4). Group 3: histiocytosis (2).
CONCLUSION: AS-OCT examination has useful applications in diagnosis and surgical planning in corneal-conjunctival disease which make its inclusion recommended among the equipment of an ocular surface and cornea unit of a tertiary hospital.
J Emmetropia 2012; 3: 177-192
� e study of the anterior segment is an important part of any ophthalmologic examination. Among the imaging methods for evaluating the anterior segment, conventional biomicroscopy using a slit lamp represents the gold standard. Other methods include ultrasound biomicroscopy, Scheimp� ug imaging and optical coherence tomography (OCT).
Anterior segment OCT (AS-OCT) is a technology based on low optical coherence interferometry, which o� ers high resolution cross-sectional images of the tissues. � e technique has evolved considerably since the � rst corneal and anterior segment OCT images were published in 1994 by Izzat et al.1 and the � rst commercial instruments became available in 20012.
� e development of AS-OCT has provided a new diagnostic tool for evaluating corneal pathology, refractive surgery3, cataract surgery4, glaucoma5 and
Submitted: 12/06/2012Accepted: 12/13/20121 Departament of Ophthalmology, Complexo Hospitalario Universitario A Coruña (Spain).
Financial Disclosure: � e authors do not have any � nancial interest in any of the products mentioned.
Corresponding Author: Victoria de Rojas Silva Urbanización Aldea Nova, 68, 15220 Ames, A Coruña (Spain).E-mail: [email protected]
Acknowledgements: SECOIR has a program to promote the publication of research in Ophthalmology. � e authors were awarded a grant from the society to bene� t from editorial support for the publication of this study.
ARTICLE
ISSN: 2171-4703
EDITORIAL
JOURNAL OF EMMETROPIA - VOL 3, OCTOBER-DECEMBER
In this respect, the Spanish Society of Refractive Implant Ocular Surgery is keen to head up this optical system surgery project and also to achieve a fully consolidated concept of emmetropia by the year 2020. Our intention is to provide all the means required to accomplish this objective. To this e� ect, our tools will include congresses, Internet, Journal of Emmetropia and SECOmIR.
We believe that this idea will impact positively on Spanish ophthalmology and related industries, and particularly on the ocular health of our patients, which after all is the only reason which should prevail and justify such an initiative.
José F. AlfonsoChairman of SECOIR
177

OCT IN CORNEAL AND CONJUCTIVAL PATHOLOGY
JOURNAL OF EMMETROPIA - VOL 3, OCTOBER-DECEMBER
Figure 1. Descemet’s membrane detachment after cataract surgery. A. Biomicroscopic image of the detachment (x 25). B. Although visible in the slit lamp, the AS-OCT examination enabled its extent to be de� ned (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm). C. Biomicroscopic image after the injection of SF6 (x 16). D. AS-OCT image after injection of SF6 in which resolution of the detachment can be observed (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).
A
C
B
D
according to the usefulness of the AS-OCT examination in each case: Group 1: the image obtained by AS-OCT was satisfactory and provided additional information to that obtained by biomicroscopy that was useful for the diagnosis or surgery. Group 2: the AS-OCT provided a satisfactory image but did not add useful additional information for the diagnosis or surgery. Group 3: the AS-OCT did not provide a satisfactory image.
� e collection of data for the study complied with current Spanish legal requirements. Given the retrospective nature of the study design, informed consent was not required.
RESULTSA total of 63 eyes of 53 patients (32 men and 21
women) were included and classi� ed as follows: group 1 with a total of 39 eyes (61.9%) of 34 patients, group 2 with a total of 22 eyes (34.9%) of 18 patients and group 3 with a total of 2 eyes (3.1%) of 1 patient (Table 1).
Group 1- Descemet’s membrane detachment. Four cases in four patients. In two of the cases,
Descemet’s detachment was noted in the slit lamp, while in the other two, corneal oedema obscured visualisation of the tear. Even in the cases in which the tear was visualised in the slit lamp, the AS-OCT image
enabled its location and limits to be more accurately assessed (Figures 1 and 2).
- Estimation of the depth of corneal leukomas.One case in one patient in which the examination
enabled the extent of the leukoma in depth to be accurately measured; at 140 µm, it was too thick to perform PTK, so this was discarded as a therapeutic option (Figure 3).
- Penetrating keratoplasty.OCT was performed in six eyes of � ve patients to
examine the graft-host junction. In all cases, visualisation was better than that obtained in the slit lamp, as the presence of steps could be noted. � e examination was performed in cases of post-keratoplasty astigmatism to assess intracorneal ring implantation (Figure 4).
- Deep anterior lamellar keratoplasty (DALK)OCT was carried out in four eyes of four patients
to analyse the graft-host junction, and to assess the residual stromal bed in cases of manual DALK.(Figure 5). In one case with a double chamber the day after surgery, the OCT showed a split between the two layers of Descemet’s membrane that was not observed in the slit lamp, and which explained the origin of the double chamber (Figure 6).
- Descemet’s stripping automated endothelial keratoplasty (DSAEK).
OCT IN CORNEAL AND CONJUCTIVAL PATHOLOGY
JOURNAL OF EMMETROPIA - VOL 3, OCTOBER-DECEMBER
Table 1. Group 1: the image obtained by AS-OCT was satisfactory and provided additional information to that obtained by biomicroscopy which was useful for the diagnosis or surgery. Group 2: the AS-OCT provided a satisfactory image but did not provide useful additional information for the diagnosis or surgery. Group 3: the AS-OCT did not provide a satisfactory image. DSAEK: Descemet’s stripping automated endothelial keratoplasty. No.: Number.
Table 1. Groups into which the cases examined using anterior segment optical coherence tomography were classifi ed.
Croup Pathology / Procedure No. Cases (%) No. PatientsGroup 1 39 (61.9%) 34
Descemet’s membrane detachment 4 4Corneal leukomas 1 1Penetrating keratoplasty 6 5Deep anterior lamellar keratoplasty 4 4DSAEK 1 1Intrastromal rings 6 6Assessment of corneal thickness 6 3Infectious keratitis 4 4Conjunctival / corneal intraepithelial squamous neoplasia 4 3Salzmann’s degeneration 2 2Conjunctival nevus 1 1
Group 2 22 (34.9%) 18Limbal cysts 1 1Hydrops in pellucid degeneration 1 1Uveitis 1 1Guttata 3 2Bullous keratopathy 4 4Conjunctivochalasis 2 2Tear meniscus height 6 3Pterygium 4 4
Group 3 2 (3.1%) 1Non-X histiocytosis 2 1
Total 63 53
corneal and conjunctival tumours6. � e technique does not require any contact, o� ers high resolution, the instruments are easy to use, it has rapid image acquisition and the examination is comfortable for the patient. All this has led to its becoming very popular in recent years.
Despite the aforementioned advantages, acquisition of these new technologies requires a � nancial investment that must be justi� ed on the basis of its clinical usefulness, more so in these times in which the high cost of technology and the limitations in healthcare resources make it necessary to prioritise and rationalise the incorporation of new equipment.
� e aim of this study was to analyse the usefulness of spectral domain AS-OCT (HD-Cirrus) in diagnosis and surgical planning in corneal-conjunctival disease in the ocular surface and cornea unit of a tertiary hospital.
PATIENTS AND METHODS� is is a retrospective case series study conducted
at the ophthalmology department of a tertiary hospital (Complexo Hospitalario Universitario A Coruña) with a catchment area of around 516,000 people. � eHD-Cirrus AS-OCT equipment database was reviewed and patients who had had an examination with the
anterior segment module between June 2010 and December 2011 were identi� ed. � eir medical records were then requested and the following data were collected: Diagnosis, surgical procedure, usefulness/quality of OCT images, slit lamp images. � e HD-Cirrus spectral domain OCT is a device that was originally designed for examination of the posterior segment, but version 4.0 of the instrument has an AS-OCT module for obtaining images of the anterior segment, with an axial resolution of 5 micrometres and transverse resolution of 15 micrometres, and a speed of 27,000 A-scans per second7. � is modality permits comfortable patient examination and is easy to use. � e mean acquisition time of the test is 4 minutes. � e instrument uses two tomography acquisition protocols and image analysis: anterior segment cube 512 x 128 and 5 line anterior segment raster7. � e slit lamp biomicroscopic images were obtained using the Topcon Slit Lamp SL-D7 equipped with the Topcon IMAGEneti-base (Topcon Corporation) to obtain photographs which were taken following the recommendations in the equipment guidelines (Topcon Photographic Guidelines).
� e study measure was the usefulness of the image obtained using AS-OCT. After the cases had been reviewed, and considering the slit lamp examination as the gold standard, they were classi� ed into three groups
178

OCT IN CORNEAL AND CONJUCTIVAL PATHOLOGY
JOURNAL OF EMMETROPIA - VOL 3, OCTOBER-DECEMBER
Figure 1. Descemet’s membrane detachment after cataract surgery. A. Biomicroscopic image of the detachment (x 25). B. Although visible in the slit lamp, the AS-OCT examination enabled its extent to be de� ned (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm). C. Biomicroscopic image after the injection of SF6 (x 16). D. AS-OCT image after injection of SF6 in which resolution of the detachment can be observed (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).
A
C
B
D
according to the usefulness of the AS-OCT examination in each case: Group 1: the image obtained by AS-OCT was satisfactory and provided additional information to that obtained by biomicroscopy that was useful for the diagnosis or surgery. Group 2: the AS-OCT provided a satisfactory image but did not add useful additional information for the diagnosis or surgery. Group 3: the AS-OCT did not provide a satisfactory image.
� e collection of data for the study complied with current Spanish legal requirements. Given the retrospective nature of the study design, informed consent was not required.
RESULTSA total of 63 eyes of 53 patients (32 men and 21
women) were included and classi� ed as follows: group 1 with a total of 39 eyes (61.9%) of 34 patients, group 2 with a total of 22 eyes (34.9%) of 18 patients and group 3 with a total of 2 eyes (3.1%) of 1 patient (Table 1).
Group 1- Descemet’s membrane detachment. Four cases in four patients. In two of the cases,
Descemet’s detachment was noted in the slit lamp, while in the other two, corneal oedema obscured visualisation of the tear. Even in the cases in which the tear was visualised in the slit lamp, the AS-OCT image
enabled its location and limits to be more accurately assessed (Figures 1 and 2).
- Estimation of the depth of corneal leukomas.One case in one patient in which the examination
enabled the extent of the leukoma in depth to be accurately measured; at 140 µm, it was too thick to perform PTK, so this was discarded as a therapeutic option (Figure 3).
- Penetrating keratoplasty.OCT was performed in six eyes of � ve patients to
examine the graft-host junction. In all cases, visualisation was better than that obtained in the slit lamp, as the presence of steps could be noted. � e examination was performed in cases of post-keratoplasty astigmatism to assess intracorneal ring implantation (Figure 4).
- Deep anterior lamellar keratoplasty (DALK)OCT was carried out in four eyes of four patients
to analyse the graft-host junction, and to assess the residual stromal bed in cases of manual DALK.(Figure 5). In one case with a double chamber the day after surgery, the OCT showed a split between the two layers of Descemet’s membrane that was not observed in the slit lamp, and which explained the origin of the double chamber (Figure 6).
- Descemet’s stripping automated endothelial keratoplasty (DSAEK).
OCT IN CORNEAL AND CONJUCTIVAL PATHOLOGY
JOURNAL OF EMMETROPIA - VOL 3, OCTOBER-DECEMBER
Table 1. Group 1: the image obtained by AS-OCT was satisfactory and provided additional information to that obtained by biomicroscopy which was useful for the diagnosis or surgery. Group 2: the AS-OCT provided a satisfactory image but did not provide useful additional information for the diagnosis or surgery. Group 3: the AS-OCT did not provide a satisfactory image. DSAEK: Descemet’s stripping automated endothelial keratoplasty. No.: Number.
Table 1. Groups into which the cases examined using anterior segment optical coherence tomography were classifi ed.
Croup Pathology / Procedure No. Cases (%) No. PatientsGroup 1 39 (61.9%) 34
Descemet’s membrane detachment 4 4Corneal leukomas 1 1Penetrating keratoplasty 6 5Deep anterior lamellar keratoplasty 4 4DSAEK 1 1Intrastromal rings 6 6Assessment of corneal thickness 6 3Infectious keratitis 4 4Conjunctival / corneal intraepithelial squamous neoplasia 4 3Salzmann’s degeneration 2 2Conjunctival nevus 1 1
Group 2 22 (34.9%) 18Limbal cysts 1 1Hydrops in pellucid degeneration 1 1Uveitis 1 1Guttata 3 2Bullous keratopathy 4 4Conjunctivochalasis 2 2Tear meniscus height 6 3Pterygium 4 4
Group 3 2 (3.1%) 1Non-X histiocytosis 2 1
Total 63 53
corneal and conjunctival tumours6. � e technique does not require any contact, o� ers high resolution, the instruments are easy to use, it has rapid image acquisition and the examination is comfortable for the patient. All this has led to its becoming very popular in recent years.
Despite the aforementioned advantages, acquisition of these new technologies requires a � nancial investment that must be justi� ed on the basis of its clinical usefulness, more so in these times in which the high cost of technology and the limitations in healthcare resources make it necessary to prioritise and rationalise the incorporation of new equipment.
� e aim of this study was to analyse the usefulness of spectral domain AS-OCT (HD-Cirrus) in diagnosis and surgical planning in corneal-conjunctival disease in the ocular surface and cornea unit of a tertiary hospital.
PATIENTS AND METHODS� is is a retrospective case series study conducted
at the ophthalmology department of a tertiary hospital (Complexo Hospitalario Universitario A Coruña) with a catchment area of around 516,000 people. � eHD-Cirrus AS-OCT equipment database was reviewed and patients who had had an examination with the
anterior segment module between June 2010 and December 2011 were identi� ed. � eir medical records were then requested and the following data were collected: Diagnosis, surgical procedure, usefulness/quality of OCT images, slit lamp images. � e HD-Cirrus spectral domain OCT is a device that was originally designed for examination of the posterior segment, but version 4.0 of the instrument has an AS-OCT module for obtaining images of the anterior segment, with an axial resolution of 5 micrometres and transverse resolution of 15 micrometres, and a speed of 27,000 A-scans per second7. � is modality permits comfortable patient examination and is easy to use. � e mean acquisition time of the test is 4 minutes. � e instrument uses two tomography acquisition protocols and image analysis: anterior segment cube 512 x 128 and 5 line anterior segment raster7. � e slit lamp biomicroscopic images were obtained using the Topcon Slit Lamp SL-D7 equipped with the Topcon IMAGEneti-base (Topcon Corporation) to obtain photographs which were taken following the recommendations in the equipment guidelines (Topcon Photographic Guidelines).
� e study measure was the usefulness of the image obtained using AS-OCT. After the cases had been reviewed, and considering the slit lamp examination as the gold standard, they were classi� ed into three groups
179

OCT IN CORNEAL AND CONJUCTIVAL PATHOLOGY
JOURNAL OF EMMETROPIA - VOL 3, OCTOBER-DECEMBER
Figure 4. A. Patient referred for intracorneal ring implantationpost-keratoplasty. � e graft-host junction shows good apposition with no steps (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm). B. Another case of penetrating keratoplasty in which a step can be seen at the graft-host junction (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).
Figure 5. A. Deep anterior lamellar keratoplasty (DALK) which was completed manually, reaching the level of Descemet’s membrane(x 16). B. � e AS-OCT did not show a residual host bed.C. Graft-host junction. D. Another case of manual DALK with a residual bed of 108 µm. (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).
A
A
B
B
C
D
neoplasia or pterygium. In the slit lamp, we were unable to di� erentiate the contribution of the stroma or the epithelium to the thickening (Figure 15).
- Conjunctival nevus: one case in one patient with a conjunctival nevus in which the OCT examination showed cysts; this was indicative of the benign nature of the lesion but was not detected with the slit lamp (Figure 16).
- Infectious keratitis. Four eyes of four patients. AS-OCT enabled the
depth of the in� ltrate and the residual leukoma to be assessed, which is important for monitoring the evolution; this is not possible with the slit lamp. � e thickness of an endothelial plaque and the corneal thickness can also be measured precisely in the area of infection (Figures 12 and 13).
- Corneal-conjunctival squamous neoplasia. Four eyes of three patients. On the AS-OCT, a pattern typical of epithelial thickening was observed, which disappeared abruptly at the junction with the normal epithelium, with no thickening of the underlying stroma (Figure 14).
- Salzmann’s degeneration. In two cases in two patients, the AS-OCT showed the same pattern of thinning epithelium above the underlying stromal nodule, which was unlike the pattern observed in other lesions such as corneal-conjunctival squamous
OCT IN CORNEAL AND CONJUCTIVAL PATHOLOGY
JOURNAL OF EMMETROPIA - VOL 3, OCTOBER-DECEMBER
Figure 2. Descemet’s membrane detachment after cataract surgery in an eye with previous penetrating keratoplasty.A. � e corneal oedema did not allow the detachment to be seen in the slit lamp and the diagnosis was made through the AS-OCT examination, in which epithelial bullae were also observed (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm). B. After the injection of SF6, the resolution of the detachment and decrease in the corneal thickness can be noted after the oedema is reduced (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm). C. Biomicroscopy image after resolution of the detachment (x 16).
Figure 3. A. Patient with leukoma referred to assess treatment by phototherapeutic keratectomy (PTK) (x 16). B. � e AS-OCT examination enables the depth of the leukoma to be measured; it reached 140 µm, too thick for PTK treatment (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).
A
A
B
B
C
� e OCT examination in DSAEK enabled the graft thickness to be measured (100 µm), and to assess its apposition and edges (Figure 7).
- Intrastromal rings.In six cases in six patients, AS-OCT was used to
accurately measure the depth of the intracorneal ring implant, which could only be estimated approximately with the slit lamp (Figure 8).
- Assessment of corneal thickness. Assessment was performed in six eyes of three patients.
� e typical ectasia pro� le was observed above the thinned area, characteristic of a pellucid cornea, which may be di� cult to observe in the slit lamp in an incipient case (Figure 9) In both eyes of one patient, the AS-OCT examination provided relevant information for making the di� erential diagnosis in a case of lipid degeneration which had been referred as Terrien’s marginal degeneration, after higher than average corneal thickness was observed in the area of the degeneration (Figure 10).
In the other case, the thinning due to infectious keratitis of a previous transplant was measured (Figure 11).
180

OCT IN CORNEAL AND CONJUCTIVAL PATHOLOGY
JOURNAL OF EMMETROPIA - VOL 3, OCTOBER-DECEMBER
Figure 4. A. Patient referred for intracorneal ring implantationpost-keratoplasty. � e graft-host junction shows good apposition with no steps (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm). B. Another case of penetrating keratoplasty in which a step can be seen at the graft-host junction (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).
Figure 5. A. Deep anterior lamellar keratoplasty (DALK) which was completed manually, reaching the level of Descemet’s membrane(x 16). B. � e AS-OCT did not show a residual host bed.C. Graft-host junction. D. Another case of manual DALK with a residual bed of 108 µm. (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).
A
A
B
B
C
D
neoplasia or pterygium. In the slit lamp, we were unable to di� erentiate the contribution of the stroma or the epithelium to the thickening (Figure 15).
- Conjunctival nevus: one case in one patient with a conjunctival nevus in which the OCT examination showed cysts; this was indicative of the benign nature of the lesion but was not detected with the slit lamp (Figure 16).
- Infectious keratitis. Four eyes of four patients. AS-OCT enabled the
depth of the in� ltrate and the residual leukoma to be assessed, which is important for monitoring the evolution; this is not possible with the slit lamp. � e thickness of an endothelial plaque and the corneal thickness can also be measured precisely in the area of infection (Figures 12 and 13).
- Corneal-conjunctival squamous neoplasia. Four eyes of three patients. On the AS-OCT, a pattern typical of epithelial thickening was observed, which disappeared abruptly at the junction with the normal epithelium, with no thickening of the underlying stroma (Figure 14).
- Salzmann’s degeneration. In two cases in two patients, the AS-OCT showed the same pattern of thinning epithelium above the underlying stromal nodule, which was unlike the pattern observed in other lesions such as corneal-conjunctival squamous
OCT IN CORNEAL AND CONJUCTIVAL PATHOLOGY
JOURNAL OF EMMETROPIA - VOL 3, OCTOBER-DECEMBER
Figure 2. Descemet’s membrane detachment after cataract surgery in an eye with previous penetrating keratoplasty.A. � e corneal oedema did not allow the detachment to be seen in the slit lamp and the diagnosis was made through the AS-OCT examination, in which epithelial bullae were also observed (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm). B. After the injection of SF6, the resolution of the detachment and decrease in the corneal thickness can be noted after the oedema is reduced (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm). C. Biomicroscopy image after resolution of the detachment (x 16).
Figure 3. A. Patient with leukoma referred to assess treatment by phototherapeutic keratectomy (PTK) (x 16). B. � e AS-OCT examination enables the depth of the leukoma to be measured; it reached 140 µm, too thick for PTK treatment (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).
A
A
B
B
C
� e OCT examination in DSAEK enabled the graft thickness to be measured (100 µm), and to assess its apposition and edges (Figure 7).
- Intrastromal rings.In six cases in six patients, AS-OCT was used to
accurately measure the depth of the intracorneal ring implant, which could only be estimated approximately with the slit lamp (Figure 8).
- Assessment of corneal thickness. Assessment was performed in six eyes of three patients.
� e typical ectasia pro� le was observed above the thinned area, characteristic of a pellucid cornea, which may be di� cult to observe in the slit lamp in an incipient case (Figure 9) In both eyes of one patient, the AS-OCT examination provided relevant information for making the di� erential diagnosis in a case of lipid degeneration which had been referred as Terrien’s marginal degeneration, after higher than average corneal thickness was observed in the area of the degeneration (Figure 10).
In the other case, the thinning due to infectious keratitis of a previous transplant was measured (Figure 11).
181
OCT IN CORNEAL AND CONJUCTIVAL PATHOLOGY
JOURNAL OF EMMETROPIA - VOL 3, OCTOBER-DECEMBER
Figure 8. A. Intrastromal segments, biomicroscopic image (x 16). B. AS-OCT in which the depth of the implant is measured (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).
Figure 7. A. DSAEK for bullous keratopathy (x 16). B. OCT image in which the graft thickness is measured (100 µm) and good adhesion of the donor button can be observed. C. Edges of the graft (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).
A
A
B
B
C
DISCUSSION� is study shows that AS-OCT examination performs
well in the diagnosis and treatment of a wide range of corneal and conjunctival pathologies. It is a quick, non-invasive examination which is easy for the doctor to
perform and comfortable for the patient. As it does not require contact, it can be used in the immediate post-operative period following corneal surgery.
� e most relevant aspects for the diagnosis or treatment of the cases studied using AS-OCT are discussed below.
OCT IN CORNEAL AND CONJUCTIVAL PATHOLOGY
JOURNAL OF EMMETROPIA - VOL 3, OCTOBER-DECEMBER
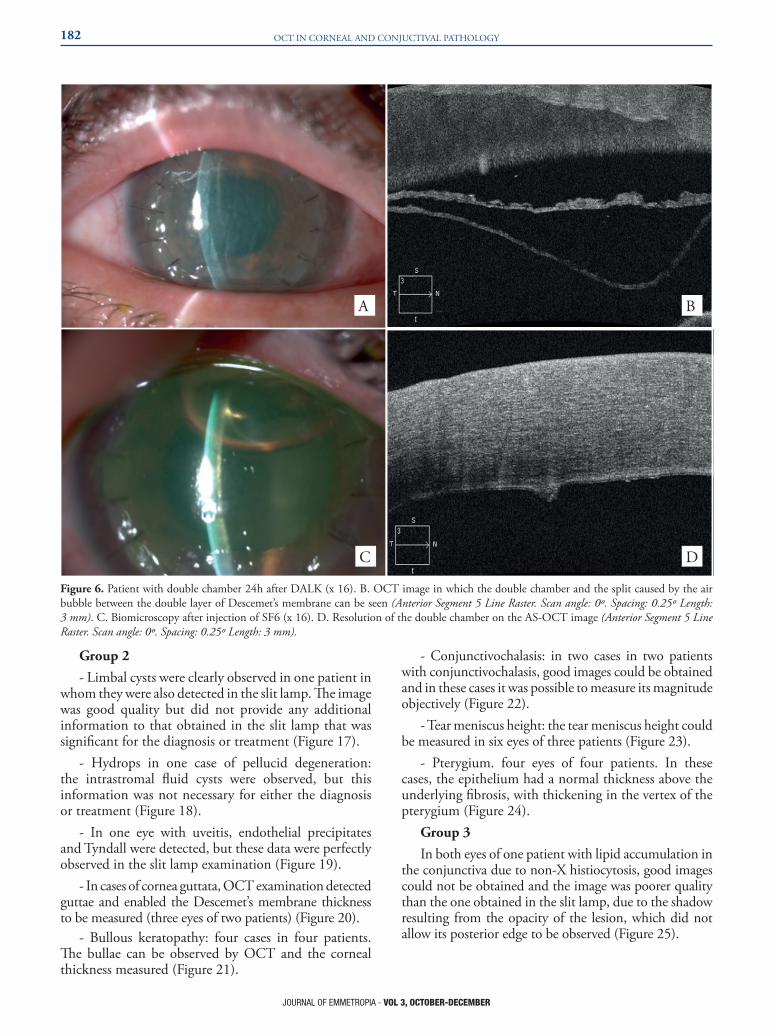
Figure 6. Patient with double chamber 24h after DALK (x 16). B. OCT image in which the double chamber and the split caused by the air bubble between the double layer of Descemet’s membrane can be seen (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length:3 mm). C. Biomicroscopy after injection of SF6 (x 16). D. Resolution of the double chamber on the AS-OCT image (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).
A B
C D
Group 2- Limbal cysts were clearly observed in one patient in
whom they were also detected in the slit lamp. � e image was good quality but did not provide any additional information to that obtained in the slit lamp that was signi� cant for the diagnosis or treatment (Figure 17).
- Hydrops in one case of pellucid degeneration: the intrastromal � uid cysts were observed, but this information was not necessary for either the diagnosis or treatment (Figure 18).
- In one eye with uveitis, endothelial precipitates and Tyndall were detected, but these data were perfectly observed in the slit lamp examination (Figure 19).
- In cases of cornea guttata, OCT examination detected guttae and enabled the Descemet’s membrane thickness to be measured (three eyes of two patients) (Figure 20).
- Bullous keratopathy: four cases in four patients. � e bullae can be observed by OCT and the corneal thickness measured (Figure 21).
- Conjunctivochalasis: in two cases in two patients with conjunctivochalasis, good images could be obtained and in these cases it was possible to measure its magnitude objectively (Figure 22).
- Tear meniscus height: the tear meniscus height could be measured in six eyes of three patients (Figure 23).
- Pterygium. four eyes of four patients. In these cases, the epithelium had a normal thickness above the underlying � brosis, with thickening in the vertex of the pterygium (Figure 24).
Group 3In both eyes of one patient with lipid accumulation in
the conjunctiva due to non-X histiocytosis, good images could not be obtained and the image was poorer quality than the one obtained in the slit lamp, due to the shadow resulting from the opacity of the lesion, which did not allow its posterior edge to be observed (Figure 25).
182

OCT IN CORNEAL AND CONJUCTIVAL PATHOLOGY
JOURNAL OF EMMETROPIA - VOL 3, OCTOBER-DECEMBER
Figure 8. A. Intrastromal segments, biomicroscopic image (x 16). B. AS-OCT in which the depth of the implant is measured (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).
Figure 7. A. DSAEK for bullous keratopathy (x 16). B. OCT image in which the graft thickness is measured (100 µm) and good adhesion of the donor button can be observed. C. Edges of the graft (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).
A
A
B
B
C
DISCUSSION� is study shows that AS-OCT examination performs
well in the diagnosis and treatment of a wide range of corneal and conjunctival pathologies. It is a quick, non-invasive examination which is easy for the doctor to
perform and comfortable for the patient. As it does not require contact, it can be used in the immediate post-operative period following corneal surgery.
� e most relevant aspects for the diagnosis or treatment of the cases studied using AS-OCT are discussed below.
OCT IN CORNEAL AND CONJUCTIVAL PATHOLOGY
JOURNAL OF EMMETROPIA - VOL 3, OCTOBER-DECEMBER
Figure 6. Patient with double chamber 24h after DALK (x 16). B. OCT image in which the double chamber and the split caused by the air bubble between the double layer of Descemet’s membrane can be seen (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length:3 mm). C. Biomicroscopy after injection of SF6 (x 16). D. Resolution of the double chamber on the AS-OCT image (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).
A B
C D
Group 2- Limbal cysts were clearly observed in one patient in
whom they were also detected in the slit lamp. � e image was good quality but did not provide any additional information to that obtained in the slit lamp that was signi� cant for the diagnosis or treatment (Figure 17).
- Hydrops in one case of pellucid degeneration: the intrastromal � uid cysts were observed, but this information was not necessary for either the diagnosis or treatment (Figure 18).
- In one eye with uveitis, endothelial precipitates and Tyndall were detected, but these data were perfectly observed in the slit lamp examination (Figure 19).
- In cases of cornea guttata, OCT examination detected guttae and enabled the Descemet’s membrane thickness to be measured (three eyes of two patients) (Figure 20).
- Bullous keratopathy: four cases in four patients. � e bullae can be observed by OCT and the corneal thickness measured (Figure 21).
- Conjunctivochalasis: in two cases in two patients with conjunctivochalasis, good images could be obtained and in these cases it was possible to measure its magnitude objectively (Figure 22).
- Tear meniscus height: the tear meniscus height could be measured in six eyes of three patients (Figure 23).
- Pterygium. four eyes of four patients. In these cases, the epithelium had a normal thickness above the underlying � brosis, with thickening in the vertex of the pterygium (Figure 24).
Group 3In both eyes of one patient with lipid accumulation in
the conjunctiva due to non-X histiocytosis, good images could not be obtained and the image was poorer quality than the one obtained in the slit lamp, due to the shadow resulting from the opacity of the lesion, which did not allow its posterior edge to be observed (Figure 25).
183

OCT IN CORNEAL AND CONJUCTIVAL PATHOLOGY
JOURNAL OF EMMETROPIA - VOL 3, OCTOBER-DECEMBER
Figure 12. A. Bacterial keratitis. B. AS-OCT image of the area of the in� ltrate that enables its thickness to be measured. C. AS-OCT image of the same case after resolution of the keratitis showing the appearance and depth of the residual leukoma (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).
Figure 13. A. Fungal keratitis (x 10). B. AS-OCT image in which the in� ltrate, thinning and thickness of the endothelial plaque can be observed and measured (Anterior Segment 5 Line Raster. Scan angle: 89º. Spacing: 0.25º Length: 3 mm).
Figure 14. A. Corneal-conjunctival intraepithelial squamous neoplasia (x 25). B. A typical epithelial thickening pattern can be observed on the AS-OCT which disappears abruptly at the junction with the normal epithelium, without any thickening of the underlying stroma (Anterior Segment Analysis: Anterior Segment Cube 512 x 128).
A
A A
B
B B
OCT IN CORNEAL AND CONJUCTIVAL PATHOLOGY
JOURNAL OF EMMETROPIA - VOL 3, OCTOBER-DECEMBER
Figure 11. A. Keratoplasty in which bacterial keratitis occurred in the graft (x 10). B. AS-OCT image in the thinned area, with a thickness of 104 µm which the ultrasound pachymeter did not measure, as it was below its lower measurement limit (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).
Figure 10. A. Biomicroscopy of a case referred to our unit with a diagnosis of Terrien’s marginal degeneration (x 16). B. � e AS-OCT examination showed the absence of peripheral thinning typical of this entity, and a diagnosis of primary lipid degeneration was established (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).
A B
Figure 9. A. Pellucid degeneration with a suspicious appearance on biomicroscopy (x 16). B. AS-OCT cross-sectional pro� le in the lower region of the cornea showing the protrusion above the thinned area (Anterior Segment 5 Line Raster. Scan angle: 90º. Spacing: 0.25º Length: 3 mm).
A B
A B
184

OCT IN CORNEAL AND CONJUCTIVAL PATHOLOGY
JOURNAL OF EMMETROPIA - VOL 3, OCTOBER-DECEMBER
Figure 12. A. Bacterial keratitis. B. AS-OCT image of the area of the in� ltrate that enables its thickness to be measured. C. AS-OCT image of the same case after resolution of the keratitis showing the appearance and depth of the residual leukoma (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).
Figure 13. A. Fungal keratitis (x 10). B. AS-OCT image in which the in� ltrate, thinning and thickness of the endothelial plaque can be observed and measured (Anterior Segment 5 Line Raster. Scan angle: 89º. Spacing: 0.25º Length: 3 mm).
Figure 14. A. Corneal-conjunctival intraepithelial squamous neoplasia (x 25). B. A typical epithelial thickening pattern can be observed on the AS-OCT which disappears abruptly at the junction with the normal epithelium, without any thickening of the underlying stroma (Anterior Segment Analysis: Anterior Segment Cube 512 x 128).
A
A A
B
B B
OCT IN CORNEAL AND CONJUCTIVAL PATHOLOGY
JOURNAL OF EMMETROPIA - VOL 3, OCTOBER-DECEMBER
Figure 11. A. Keratoplasty in which bacterial keratitis occurred in the graft (x 10). B. AS-OCT image in the thinned area, with a thickness of 104 µm which the ultrasound pachymeter did not measure, as it was below its lower measurement limit (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).
Figure 10. A. Biomicroscopy of a case referred to our unit with a diagnosis of Terrien’s marginal degeneration (x 16). B. � e AS-OCT examination showed the absence of peripheral thinning typical of this entity, and a diagnosis of primary lipid degeneration was established (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).
A B
Figure 9. A. Pellucid degeneration with a suspicious appearance on biomicroscopy (x 16). B. AS-OCT cross-sectional pro� le in the lower region of the cornea showing the protrusion above the thinned area (Anterior Segment 5 Line Raster. Scan angle: 90º. Spacing: 0.25º Length: 3 mm).
A B
A B
185

OCT IN CORNEAL AND CONJUCTIVAL PATHOLOGY
JOURNAL OF EMMETROPIA - VOL 3, OCTOBER-DECEMBER
Figure 17. A. Limbal cysts, biomicroscopy (x 40). B. AS-OCT image of limbal cysts (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).
Figure 18. A. Hydrops in pellucid degeneration (x 16).B. AS-OCT image of the intrastromal cysts in hydrops (Anterior Segment Analysis: Anterior Segment Cube 512 x 128).
Figure 19. Endothelial precipitates in uveitis, AS-OCT. B. Tyndall in the same case obtained by AS-OCT (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).
A A
A
B B
B
post-operative visual acuity, with thinner grafts associated with better visual acuities, although this has not been found in all studies12. Moreover, thicker grafts are related with a higher likelihood of graft failure13. Using data from the OCT examination, the hypermetropic change that occurs after DSAEK surgery was explained14. It was also used to detect � uid at the interface, and to assess the good adhesion of the graft15.
- Intracorneal rings.� e depth at which intracorneal rings are implanted
is an important factor in the outcome of the surgery, and can be measured with OCT while it can only be estimated approximately with the slit lamp16.
- Assessment of corneal thickness.� e assessment of central and peripheral corneal
thickness is a very important parameter in the diagnosis and follow-up of numerous corneal pathologies. In relation to this parameter, we understand that the gold standard examination with which OCT should be compared is ultrasound pachymetry. Nevertheless, we believe that the comparison with biomicroscopy remains valid with respect to comparison with a technique capable of providing cross-sectional images. One of the main advantages of AS-OCT is that it allows us to perform the measurement at the exact point in the image that we wish to evaluate, unlike ultrasound pachymetry.
OCT IN CORNEAL AND CONJUCTIVAL PATHOLOGY
JOURNAL OF EMMETROPIA - VOL 3, OCTOBER-DECEMBER
Figure 15. Salzmann’s corneal degeneration showing epithelial thinning over the underlying stromal nodule (*) (Anterior Segment Analysis: Anterior Segment Cube 512 x 128).
Figure 16. A. Conjunctival nevus. No microcysts were observed in the slit lamp examination (x 16). AS-OCT examination in which the cysts and the well-de� ned posterior limit of the lesion can be clearly seen, both signs of its benign nature (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm). C. Histological image of the cysts.
A
B
C
Group 1 AS-OCT provided important information for
diagnosis and/or surgical treatment in 61.9% of the cases analysed retrospectively.
- Descemet’s membrane detachment. � e contribution of OCT images in the diagnosis,
classi� cation and treatment of Descemet’s membrane detachment has been demonstrated in recent publications4,8,9. � e oedema that accompanies the detachment can hinder its diagnosis, as in the second case in this paper, or not allow its extent to be de� ned, as in the � rst.
- Estimation of the depth of corneal leukomas.In the slit lamp, the depth of a leukoma can only
be estimated approximately. AS-OCT allows it to be measured objectively, and helps to decide the most appropriate treatment in each case.
- Penetrating keratoplasty.We used OCT examination in certain patients to assess
the graft-host junction before implanting intracorneal rings for high post-keratoplasty astigmatism. � e OCT showed the graft-host junction and its characteristics, such as the presence or not of steps, in greater detail than the slit lamp. � e presence of steps is related with higher astigmatisms, and is also important in planning endothelial grafts after previous penetrating keratoplasty10.
- Deep anterior lamellar keratoplasty (DALK). We consider the information from OCT to be particularly important in the evaluation of DALK. Several publications have shown the relationship between the residual bed after manual DALK and visual acuity11. � e residual bed can be measured very accurately with OCT. As in the case of Descemet’s detachment, OCT is also useful in the treatment of double chamber, and as shown in our case, to
identify its cause: splitting of Descemet’s membrane into its two layers was not observed in the slit lamp.
- Descemet’s stripping automated endothelial keratoplasty (DSAEK).
Using OCT, the apposition of the graft to the host bed can be assessed, as well as the graft thickness, as our case shows3. Graft thickness has been related with the
186

OCT IN CORNEAL AND CONJUCTIVAL PATHOLOGY
JOURNAL OF EMMETROPIA - VOL 3, OCTOBER-DECEMBER
Figure 17. A. Limbal cysts, biomicroscopy (x 40). B. AS-OCT image of limbal cysts (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).
Figure 18. A. Hydrops in pellucid degeneration (x 16).B. AS-OCT image of the intrastromal cysts in hydrops (Anterior Segment Analysis: Anterior Segment Cube 512 x 128).
Figure 19. Endothelial precipitates in uveitis, AS-OCT. B. Tyndall in the same case obtained by AS-OCT (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).
A A
A
B B
B
post-operative visual acuity, with thinner grafts associated with better visual acuities, although this has not been found in all studies12. Moreover, thicker grafts are related with a higher likelihood of graft failure13. Using data from the OCT examination, the hypermetropic change that occurs after DSAEK surgery was explained14. It was also used to detect � uid at the interface, and to assess the good adhesion of the graft15.
- Intracorneal rings.� e depth at which intracorneal rings are implanted
is an important factor in the outcome of the surgery, and can be measured with OCT while it can only be estimated approximately with the slit lamp16.
- Assessment of corneal thickness.� e assessment of central and peripheral corneal
thickness is a very important parameter in the diagnosis and follow-up of numerous corneal pathologies. In relation to this parameter, we understand that the gold standard examination with which OCT should be compared is ultrasound pachymetry. Nevertheless, we believe that the comparison with biomicroscopy remains valid with respect to comparison with a technique capable of providing cross-sectional images. One of the main advantages of AS-OCT is that it allows us to perform the measurement at the exact point in the image that we wish to evaluate, unlike ultrasound pachymetry.
OCT IN CORNEAL AND CONJUCTIVAL PATHOLOGY
JOURNAL OF EMMETROPIA - VOL 3, OCTOBER-DECEMBER
Figure 15. Salzmann’s corneal degeneration showing epithelial thinning over the underlying stromal nodule (*) (Anterior Segment Analysis: Anterior Segment Cube 512 x 128).
Figure 16. A. Conjunctival nevus. No microcysts were observed in the slit lamp examination (x 16). AS-OCT examination in which the cysts and the well-de� ned posterior limit of the lesion can be clearly seen, both signs of its benign nature (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm). C. Histological image of the cysts.
A
B
C
Group 1 AS-OCT provided important information for
diagnosis and/or surgical treatment in 61.9% of the cases analysed retrospectively.
- Descemet’s membrane detachment. � e contribution of OCT images in the diagnosis,
classi� cation and treatment of Descemet’s membrane detachment has been demonstrated in recent publications4,8,9. � e oedema that accompanies the detachment can hinder its diagnosis, as in the second case in this paper, or not allow its extent to be de� ned, as in the � rst.
- Estimation of the depth of corneal leukomas.In the slit lamp, the depth of a leukoma can only
be estimated approximately. AS-OCT allows it to be measured objectively, and helps to decide the most appropriate treatment in each case.
- Penetrating keratoplasty.We used OCT examination in certain patients to assess
the graft-host junction before implanting intracorneal rings for high post-keratoplasty astigmatism. � e OCT showed the graft-host junction and its characteristics, such as the presence or not of steps, in greater detail than the slit lamp. � e presence of steps is related with higher astigmatisms, and is also important in planning endothelial grafts after previous penetrating keratoplasty10.
- Deep anterior lamellar keratoplasty (DALK). We consider the information from OCT to be particularly important in the evaluation of DALK. Several publications have shown the relationship between the residual bed after manual DALK and visual acuity11. � e residual bed can be measured very accurately with OCT. As in the case of Descemet’s detachment, OCT is also useful in the treatment of double chamber, and as shown in our case, to
identify its cause: splitting of Descemet’s membrane into its two layers was not observed in the slit lamp.
- Descemet’s stripping automated endothelial keratoplasty (DSAEK).
Using OCT, the apposition of the graft to the host bed can be assessed, as well as the graft thickness, as our case shows3. Graft thickness has been related with the
187

OCT IN CORNEAL AND CONJUCTIVAL PATHOLOGY
JOURNAL OF EMMETROPIA - VOL 3, OCTOBER-DECEMBER
Figure 22. A. Conjunctivochalasis, biomicroscopy (x 25).B. AS-OCT image in which the fold of the conjunctiva can be observed. C. � e AS-OCT image enables the cross-sectional area of the conjunctivochalasis to be measured, 487.500 mm2 (Anterior Segment 5 Line Raster. Scan angle: 90º. Spacing: 0.25º Length: 3 mm).24
Figure 23. � e AS-OCT enables the tear meniscus height to be measured, 700 µm in the case of the image, after instillation of arti� cial tears (Anterior Segment 5 Line Raster. Scan angle: 90º. Spacing: 0.25º Length: 3 mm).
A
B
C
- Corneal and conjunctival intraepithelial squamous neoplasia, Salzmann’s degeneration.
� e high resolution of the OCT images enable the epithelial thickness and variations in it to be assessed, as well as its spatial relationship with changes in the stromal thickness. � is has enabled typical patterns to be identi� ed in certain pathologies which help us to di� erentiate them from others. Corneal and conjunctival intraepithelial squamous neoplasia is characterised by thickening of the epithelium which ends abruptly at the limit with the normal epithelium6,
while in pterygium20 and Salzmann’s degeneration21, the epithelium is normal or thins over a stromal nodule, with the origin of the alteration found in the stroma.
- Conjunctival nevus.Shields et al. have recently shown the high sensitivity
of OCT examination in the assessment of conjunctival nevi22. � e presence of cysts is a sign that the lesion is benign and therefore their detection is important. In the case shown in this paper, the cysts were not observed in the slit lamp examination, but were observed in the OCT images.
Group 2� e information provided by OCT in the cases
classi� ed into group 2 was not relevant for either the diagnosis or treatment (34.9% of the cases studied). When it comes to assessing the usefulness of the technique, we must take into account that in the classi� cation that we used in this paper, we have adhered to information which is relevant for the diagnosis or treatment. Nevertheless, in some of the cases classi� ed into group 2, the high resolution of the images obtained enables measurements to be taken that cannot be obtained by biomicroscopy; although not relevant in clinical practice, these could be important for research. For example, the technique enables the tear meniscus height23, magnitude of conjunctivochalasis24, and Descemet’s membrane thickness25 to be measured, as has been observed in previous studies. With respect to pterygium, AS-OCT is not required for its diagnosis,
OCT IN CORNEAL AND CONJUCTIVAL PATHOLOGY
JOURNAL OF EMMETROPIA - VOL 3, OCTOBER-DECEMBER
Figure 20. A. Corneal guttata (x 40). B. Appearance of the guttae on AS-OCT. C. Descemet’s membrane thickness in the same case, 24 µm (the mean in normal eyes is 10 to 16 µm according to age) (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).25
Figure 21. A. Bullous keratopathy in keratoplasty secondary to graft rejection (x 10). B. Bullae on the AS-OCT image with a therapeutic contact lens (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).
A
A
BB
C
For example, if during the course of infectious keratitis, we wish to assess the thinning exactly on the ulcer, in order to decide the time to apply preventive measures such as cyanoacrylate or an amniotic membrane graft in view of a possible perforation, AS-OCT has obvious advantages over ultrasound pachymetry and slit lamp examination, as it enables the measurement to be taken on the exact point at the ulcer, without contact; moreover, it should be remembered that the lower limit of sensitivity for commercially available pachymeters may be above the thickness that we wish to measure. In the pellucid degeneration, we were able to measure the thickness in exactly the area that we wished, and to relate it spatially with the area of the protrusion. In the case of the lipid degeneration, certain equipment like the Orbscan does not allow a reliable
measurement to be taken, due to an alteration in the accuracy when there are opacities, which does not occur with AS-OCT17. � e corneal thickness measurements of di� erent instruments, among them AS-OCT, were compared with those of ultrasound pachymetry, and it was shown that they are not interchangeable17. Finally, it is worth pointing out the capacity of certain AS-OCT instruments for producing pachymetric maps (which is not possible with the HD-Cirrus) and which extends the possible applications of this tecnology18.
- Infectious keratitis.Conventional follow-up of infectious keratitis by slit
lamp is based on measuring the extent of the epithelial defect and the in� ltrate and in taking serial photographs. Using AS-OCT, we can objectively measure certain data that cannot be obtained in the slit lamp examination, such as depth of the in� ltrate, thinning of the stroma in the region of the ulcer, whether in the active phase or in the assessment of the sequelae, and the depth of an endothelial plaque. All this is important for objectively analysing the response to treatment19.
188

OCT IN CORNEAL AND CONJUCTIVAL PATHOLOGY
JOURNAL OF EMMETROPIA - VOL 3, OCTOBER-DECEMBER
Figure 22. A. Conjunctivochalasis, biomicroscopy (x 25).B. AS-OCT image in which the fold of the conjunctiva can be observed. C. � e AS-OCT image enables the cross-sectional area of the conjunctivochalasis to be measured, 487.500 mm2 (Anterior Segment 5 Line Raster. Scan angle: 90º. Spacing: 0.25º Length: 3 mm).24
Figure 23. � e AS-OCT enables the tear meniscus height to be measured, 700 µm in the case of the image, after instillation of arti� cial tears (Anterior Segment 5 Line Raster. Scan angle: 90º. Spacing: 0.25º Length: 3 mm).
A
B
C
- Corneal and conjunctival intraepithelial squamous neoplasia, Salzmann’s degeneration.
� e high resolution of the OCT images enable the epithelial thickness and variations in it to be assessed, as well as its spatial relationship with changes in the stromal thickness. � is has enabled typical patterns to be identi� ed in certain pathologies which help us to di� erentiate them from others. Corneal and conjunctival intraepithelial squamous neoplasia is characterised by thickening of the epithelium which ends abruptly at the limit with the normal epithelium6,
while in pterygium20 and Salzmann’s degeneration21, the epithelium is normal or thins over a stromal nodule, with the origin of the alteration found in the stroma.
- Conjunctival nevus.Shields et al. have recently shown the high sensitivity
of OCT examination in the assessment of conjunctival nevi22. � e presence of cysts is a sign that the lesion is benign and therefore their detection is important. In the case shown in this paper, the cysts were not observed in the slit lamp examination, but were observed in the OCT images.
Group 2� e information provided by OCT in the cases
classi� ed into group 2 was not relevant for either the diagnosis or treatment (34.9% of the cases studied). When it comes to assessing the usefulness of the technique, we must take into account that in the classi� cation that we used in this paper, we have adhered to information which is relevant for the diagnosis or treatment. Nevertheless, in some of the cases classi� ed into group 2, the high resolution of the images obtained enables measurements to be taken that cannot be obtained by biomicroscopy; although not relevant in clinical practice, these could be important for research. For example, the technique enables the tear meniscus height23, magnitude of conjunctivochalasis24, and Descemet’s membrane thickness25 to be measured, as has been observed in previous studies. With respect to pterygium, AS-OCT is not required for its diagnosis,
OCT IN CORNEAL AND CONJUCTIVAL PATHOLOGY
JOURNAL OF EMMETROPIA - VOL 3, OCTOBER-DECEMBER
Figure 20. A. Corneal guttata (x 40). B. Appearance of the guttae on AS-OCT. C. Descemet’s membrane thickness in the same case, 24 µm (the mean in normal eyes is 10 to 16 µm according to age) (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).25
Figure 21. A. Bullous keratopathy in keratoplasty secondary to graft rejection (x 10). B. Bullae on the AS-OCT image with a therapeutic contact lens (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).
A
A
BB
C
For example, if during the course of infectious keratitis, we wish to assess the thinning exactly on the ulcer, in order to decide the time to apply preventive measures such as cyanoacrylate or an amniotic membrane graft in view of a possible perforation, AS-OCT has obvious advantages over ultrasound pachymetry and slit lamp examination, as it enables the measurement to be taken on the exact point at the ulcer, without contact; moreover, it should be remembered that the lower limit of sensitivity for commercially available pachymeters may be above the thickness that we wish to measure. In the pellucid degeneration, we were able to measure the thickness in exactly the area that we wished, and to relate it spatially with the area of the protrusion. In the case of the lipid degeneration, certain equipment like the Orbscan does not allow a reliable
measurement to be taken, due to an alteration in the accuracy when there are opacities, which does not occur with AS-OCT17. � e corneal thickness measurements of di� erent instruments, among them AS-OCT, were compared with those of ultrasound pachymetry, and it was shown that they are not interchangeable17. Finally, it is worth pointing out the capacity of certain AS-OCT instruments for producing pachymetric maps (which is not possible with the HD-Cirrus) and which extends the possible applications of this tecnology18.
- Infectious keratitis.Conventional follow-up of infectious keratitis by slit
lamp is based on measuring the extent of the epithelial defect and the in� ltrate and in taking serial photographs. Using AS-OCT, we can objectively measure certain data that cannot be obtained in the slit lamp examination, such as depth of the in� ltrate, thinning of the stroma in the region of the ulcer, whether in the active phase or in the assessment of the sequelae, and the depth of an endothelial plaque. All this is important for objectively analysing the response to treatment19.
189

OCT IN CORNEAL AND CONJUCTIVAL PATHOLOGY
JOURNAL OF EMMETROPIA - VOL 3, OCTOBER-DECEMBER
not included in our study3. Among the limitations, those of the instrument with which the examinations were carried out should also be mentioned. � e HD-Cirrus allows high resolution images of the cornea and conjunctiva to be obtained, but not anterior segment limbus-to-limbus cross-sections like those provided by the Visante7. � ese sections enable biometric measures of the anterior segment to be obtained, which are useful for programming certain surgeries, such as graft dimensions in keratoplasty, angle-angle measurements for phakic lens implants and angle measurements in glaucoma, the usefulness of which has been demonstrated in other studies and which are not shown in this study either3.
Considering all of the above, it may be that in a context where refractive surgery is performed, and with additional AS-OCT equipment, the usefulness of the examination could be even greater than can be inferred from our study. Finally, another limitation is related precisely with the retrospective design of the study; the selection of the cases for AS-OCT examination is biased by the usefulness that this tool has for each of the ophthalmologists in the cornea and ocular surface unit, which depends on their own criteria, knowledge of the technique and cases in which previous publications have demonstrated its usefulness.
In conclusion, our study shows that AS-OCT examination is a useful tool for diagnosis and treatment planning in corneal-conjunctival disease, which makes its inclusion recommended among the equipment of an ocular surface and corneal unit of a tertiary hospital.
BIBLIOGRAPHY1. Izatt JA, Hee MR, Swanson EA, et al.
Micrometer-scale resolution imaging of the anterior eye in vivo with optical coherence tomography. Arch Ophthalmol.1994; 112: 1584-1589.
2. Radhakrishnan S, Rollins AM, Roth JE, et al. Real-time optical coherence tomography for the anterior segment at 1310 nm. Arch Ophthalmol. 2001; 119: 1179-1185.
3. Doors M, Brendschot TJM, Brabander J, Webers CAB, Nuijts R. Value of optical coherence tomography for anterior segment surgery. J Cataract Refract Surg. 2010; 36: 1231-1229.
4. Lorente R, de Rojas V, Orbegozo J, Méndez J, Mendicute J, Lorente B. Aplicaciones OCT-SA en cristalino y cirugía de catarata. In: Muñoz FJ, Rebolleda G, Díaz M, editors. Tomografía de coherencia óptica. LXXXVII Ponencia O� cial de la Sociedad Española de Oftalmología, Madrid,2011: 167-186.
5. Lorente R, Méndez J, de Rojas V, et al. Tomografía de coherencia óptica de segmento anterior en cirugía combinada. In: Lorente R, editors. Catarata & Glaucoma. Monografía Sociedad Española de Cirugía Ocular Implanto Refractiva, Madrid, 2012: 79-91.
6. Shousha MA, Karp CL, Pérez VL et al. Diagnosis and management of conjunctival and corneal intraepithelial neoplasia using ultra high-resolution optical coherence tomography. Ophthalmology 2011; 118: 1531-1537.
7. Lara J, Ispa C, González del Valle F, Muñoz FJ, Rebolleda G. OCT de segmento anterior: dispositivos, correlación anatómica y principales aplicaciones. In: Muñoz FJ, Rebolleda G, Díaz M, editors. Tomografía de coherencia óptica. LXXXVII Ponencia O� cial de la Sociedad Española de Oftalmología, Madrid, 2011: 114-124.
8. Winn BJ, Lin SC, Hee MR, Chiu C. Repair of Descemet membrane detachments with the assistance of anterior segment optical coherence tomography. Arch Ophthalmol.2008; 126: 730-732.
9. Wylegala E, Nowinska A. Usefulness of anterior segment optical coherence tomography in Descemet membrane detachment. Eur J Ophthalmol. 2009; 19: 723-728.
10. Jhanji V, Constantinu M, Beltz J, Vajpajee R. Evaluation of posterior wound pro� le after penetrating keratoplasty using anterior segment optical coherence tomography.Cornea 2011; 30: 277-280.
11. Reinhart WJ, Musch DC, Jacobs DS, Lee WB, Kaufman SC, Shtein RM. Deep anterior lamellar keratoplasty as an alternative to penetrating keratoplasty. A report by the American Academy of Ophthalmology. Ophthalmology 2011; 118: 209-218.
12. Terry MA, Straiko MD, Goshe JM, Li JY, Davis-Boozer D. Descemet’s stripping automated endothelial keratoplasty: the tenuous relationship between donor thickness and postoperative vision. Ophthalmology 2012; 119: 1988-1996.
13. Shih CY, Ritterband DC, Palmiero P-M, Seedor JA, Papachristou G, Harizman N, Liebmann JM, Ritch R. � e use of postoperative slit-lamp optical coherence tomography to predict primary failure in Descemet stripping automated endothelial keratoplasty. Am J Ophthalmol.2009; 147: 796-800.
14. Holz HA, Meyer JJ, Espandar L, Tabin GC, Mi� in MD, Moshirfar M. Corneal pro� le analysis after Descemet stripping endothelial keratoplasty and its relationship to postoperative hyperopic shift. J Cataract Refract Surg. 2008; 34: 211-214.
15. Tarnawska D, Wylegala E. Monitoring cornea and graft morphometric dynamics after Descemet stripping and endothelial keratoplasty with anterior segment optical coherence tomography. Cornea 2010; 29: 272-277.
16. Lai MM, Tang M, Andrade EMM, Li Y, Khurana RN, Song JC, Huang D. Optical coherence tomography to assess intrastromal corneal ring segment depth in keratoconic eyes.J Cataract Refract Surg. 2006; 32: 1860-1865.
17. Li EYM, Mohamed S, Leung ChKS, et al. Agreement among 3 methods to measure corneal thickness: ultrasound pachymetry, Orbscan II, and Visante anterior segment optical coherence tomography. Ophthalmology 2007; 114: 1842-1847.
18. Li Y, Meisler DM, Tang M et al. Keratoconus diagnosis with optical coherence tomography pachymetry mapping. Ophthalmology 2008; 115: 2159-2166.
19. Konstantopoulos A, Kuo J, Anderson D, Hossain P. Assessment of the use of anterior segment optical coherence tomography in microbial keratitis. Am J Ophthalmol. 2008; 146: 534-542.
20. Kieval JZ, Karp CL, Shousha MA et al. Ultra high resolution optical coherence tomography for di� erentiation of ocular squamous neoplasia and pterygia.Ophthalmology 2012; 119: 481-486.
21. Hurmeric V, Yoo SH, Karp CL et al. In vivo morphologic characteristics of Salzmann nodular degeneration with ultrahigh resolution optical coherence tomography. Am J Ophthalmol 2011; 151: 248-256.
22. Shields CL, Belinsky I, Romanelli-Gobbi M et al. Anterior
OCT IN CORNEAL AND CONJUCTIVAL PATHOLOGY
JOURNAL OF EMMETROPIA - VOL 3, OCTOBER-DECEMBER
Figure 24. A. Pterygium, biomicroscopy (x 16). B. OCT image in which it can be observed that the epithelial thickness is normal (arrow) over the area of underlying � brotic tissue, unlike intraepithelial squamous neoplasia in which the epithelium thickens (Figure 14) (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).20
Figure 25. A. Biomicroscopic image of the yellowish conjunctival mass in a patient with non-X histiocytosis (x 6). B. AS-OCT image in which the opacity of the mass causes a posterior shadow, obscuring visualisation of the posterior edge of the lesion (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).
AA
B
B
but the images show how AS-OCT can discriminate between di� erent patterns of epithelial versus stromal thickness, which cannot be done with the slit lamp; this could be useful in cases of pterygium with atypical characteristics in the diagnosis versus intraepithelial neoplasia20.
� e case of detection of endothelial precipitates and Tyndall in uveitis was classi� ed into group 2 because they were observed clearly in the slit lamp. Nevertheless, it may be that if it is not possible to detect them, due to corneal oedema for example, they could be observed on the AS-OCT image26. � e in� ammatory cells are between 10 and 20 µm and therefore, some may be below the limit of resolution of the OCT equipment. However they can be visualised since they tend to form groups, which facilitates their detection.
Group 3In group 3, the lesions in the only case classi� ed here
caused a shadow on the OCT examination due to their opacity, which prevented the posterior part of the lesion from being visualised; in this case the images did not
contribute any additional information to that obtained by biomicroscopy. � us, in the case of large tumours where their opacity does not allow light through or pigmented tumours, it has been observed that ultrasound biomicroscopy is superior to AS-OCT27.
When it comes to assessing the results of our study, both the context in which it was conducted and certain limitations must be taken into account. With respect to the context, this is the corneal and ocular surface unit of a tertiary hospital in which a wide variety of specialised corneal and conjunctival surgical techniques are performed, and to which patients are referred from a large healthcare area (516,000 inhabitants). � e usefulness of the technique would probably not be the same in the context of general ophthalmology, an area with fewer patients or in which certain surgical techniques such as corneal transplants, intrastromal segment implants, etc. are not performed. � is context also imposes certain limitations, as it is a public centre in which refractive surgery is not carried out. � e usefulness of AS-OCT examination in refractive surgery has been analysed in previous publications which are
190

OCT IN CORNEAL AND CONJUCTIVAL PATHOLOGY
JOURNAL OF EMMETROPIA - VOL 3, OCTOBER-DECEMBER
not included in our study3. Among the limitations, those of the instrument with which the examinations were carried out should also be mentioned. � e HD-Cirrus allows high resolution images of the cornea and conjunctiva to be obtained, but not anterior segment limbus-to-limbus cross-sections like those provided by the Visante7. � ese sections enable biometric measures of the anterior segment to be obtained, which are useful for programming certain surgeries, such as graft dimensions in keratoplasty, angle-angle measurements for phakic lens implants and angle measurements in glaucoma, the usefulness of which has been demonstrated in other studies and which are not shown in this study either3.
Considering all of the above, it may be that in a context where refractive surgery is performed, and with additional AS-OCT equipment, the usefulness of the examination could be even greater than can be inferred from our study. Finally, another limitation is related precisely with the retrospective design of the study; the selection of the cases for AS-OCT examination is biased by the usefulness that this tool has for each of the ophthalmologists in the cornea and ocular surface unit, which depends on their own criteria, knowledge of the technique and cases in which previous publications have demonstrated its usefulness.
In conclusion, our study shows that AS-OCT examination is a useful tool for diagnosis and treatment planning in corneal-conjunctival disease, which makes its inclusion recommended among the equipment of an ocular surface and corneal unit of a tertiary hospital.
BIBLIOGRAPHY1. Izatt JA, Hee MR, Swanson EA, et al.
Micrometer-scale resolution imaging of the anterior eye in vivo with optical coherence tomography. Arch Ophthalmol.1994; 112: 1584-1589.
2. Radhakrishnan S, Rollins AM, Roth JE, et al. Real-time optical coherence tomography for the anterior segment at 1310 nm. Arch Ophthalmol. 2001; 119: 1179-1185.
3. Doors M, Brendschot TJM, Brabander J, Webers CAB, Nuijts R. Value of optical coherence tomography for anterior segment surgery. J Cataract Refract Surg. 2010; 36: 1231-1229.
4. Lorente R, de Rojas V, Orbegozo J, Méndez J, Mendicute J, Lorente B. Aplicaciones OCT-SA en cristalino y cirugía de catarata. In: Muñoz FJ, Rebolleda G, Díaz M, editors. Tomografía de coherencia óptica. LXXXVII Ponencia O� cial de la Sociedad Española de Oftalmología, Madrid,2011: 167-186.
5. Lorente R, Méndez J, de Rojas V, et al. Tomografía de coherencia óptica de segmento anterior en cirugía combinada. In: Lorente R, editors. Catarata & Glaucoma. Monografía Sociedad Española de Cirugía Ocular Implanto Refractiva, Madrid, 2012: 79-91.
6. Shousha MA, Karp CL, Pérez VL et al. Diagnosis and management of conjunctival and corneal intraepithelial neoplasia using ultra high-resolution optical coherence tomography. Ophthalmology 2011; 118: 1531-1537.
7. Lara J, Ispa C, González del Valle F, Muñoz FJ, Rebolleda G. OCT de segmento anterior: dispositivos, correlación anatómica y principales aplicaciones. In: Muñoz FJ, Rebolleda G, Díaz M, editors. Tomografía de coherencia óptica. LXXXVII Ponencia O� cial de la Sociedad Española de Oftalmología, Madrid, 2011: 114-124.
8. Winn BJ, Lin SC, Hee MR, Chiu C. Repair of Descemet membrane detachments with the assistance of anterior segment optical coherence tomography. Arch Ophthalmol.2008; 126: 730-732.
9. Wylegala E, Nowinska A. Usefulness of anterior segment optical coherence tomography in Descemet membrane detachment. Eur J Ophthalmol. 2009; 19: 723-728.
10. Jhanji V, Constantinu M, Beltz J, Vajpajee R. Evaluation of posterior wound pro� le after penetrating keratoplasty using anterior segment optical coherence tomography.Cornea 2011; 30: 277-280.
11. Reinhart WJ, Musch DC, Jacobs DS, Lee WB, Kaufman SC, Shtein RM. Deep anterior lamellar keratoplasty as an alternative to penetrating keratoplasty. A report by the American Academy of Ophthalmology. Ophthalmology 2011; 118: 209-218.
12. Terry MA, Straiko MD, Goshe JM, Li JY, Davis-Boozer D. Descemet’s stripping automated endothelial keratoplasty: the tenuous relationship between donor thickness and postoperative vision. Ophthalmology 2012; 119: 1988-1996.
13. Shih CY, Ritterband DC, Palmiero P-M, Seedor JA, Papachristou G, Harizman N, Liebmann JM, Ritch R. � e use of postoperative slit-lamp optical coherence tomography to predict primary failure in Descemet stripping automated endothelial keratoplasty. Am J Ophthalmol.2009; 147: 796-800.
14. Holz HA, Meyer JJ, Espandar L, Tabin GC, Mi� in MD, Moshirfar M. Corneal pro� le analysis after Descemet stripping endothelial keratoplasty and its relationship to postoperative hyperopic shift. J Cataract Refract Surg. 2008; 34: 211-214.
15. Tarnawska D, Wylegala E. Monitoring cornea and graft morphometric dynamics after Descemet stripping and endothelial keratoplasty with anterior segment optical coherence tomography. Cornea 2010; 29: 272-277.
16. Lai MM, Tang M, Andrade EMM, Li Y, Khurana RN, Song JC, Huang D. Optical coherence tomography to assess intrastromal corneal ring segment depth in keratoconic eyes.J Cataract Refract Surg. 2006; 32: 1860-1865.
17. Li EYM, Mohamed S, Leung ChKS, et al. Agreement among 3 methods to measure corneal thickness: ultrasound pachymetry, Orbscan II, and Visante anterior segment optical coherence tomography. Ophthalmology 2007; 114: 1842-1847.
18. Li Y, Meisler DM, Tang M et al. Keratoconus diagnosis with optical coherence tomography pachymetry mapping. Ophthalmology 2008; 115: 2159-2166.
19. Konstantopoulos A, Kuo J, Anderson D, Hossain P. Assessment of the use of anterior segment optical coherence tomography in microbial keratitis. Am J Ophthalmol. 2008; 146: 534-542.
20. Kieval JZ, Karp CL, Shousha MA et al. Ultra high resolution optical coherence tomography for di� erentiation of ocular squamous neoplasia and pterygia.Ophthalmology 2012; 119: 481-486.
21. Hurmeric V, Yoo SH, Karp CL et al. In vivo morphologic characteristics of Salzmann nodular degeneration with ultrahigh resolution optical coherence tomography. Am J Ophthalmol 2011; 151: 248-256.
22. Shields CL, Belinsky I, Romanelli-Gobbi M et al. Anterior
OCT IN CORNEAL AND CONJUCTIVAL PATHOLOGY
JOURNAL OF EMMETROPIA - VOL 3, OCTOBER-DECEMBER
Figure 24. A. Pterygium, biomicroscopy (x 16). B. OCT image in which it can be observed that the epithelial thickness is normal (arrow) over the area of underlying � brotic tissue, unlike intraepithelial squamous neoplasia in which the epithelium thickens (Figure 14) (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).20
Figure 25. A. Biomicroscopic image of the yellowish conjunctival mass in a patient with non-X histiocytosis (x 6). B. AS-OCT image in which the opacity of the mass causes a posterior shadow, obscuring visualisation of the posterior edge of the lesion (Anterior Segment 5 Line Raster. Scan angle: 0º. Spacing: 0.25º Length: 3 mm).
AA
B
B
but the images show how AS-OCT can discriminate between di� erent patterns of epithelial versus stromal thickness, which cannot be done with the slit lamp; this could be useful in cases of pterygium with atypical characteristics in the diagnosis versus intraepithelial neoplasia20.
� e case of detection of endothelial precipitates and Tyndall in uveitis was classi� ed into group 2 because they were observed clearly in the slit lamp. Nevertheless, it may be that if it is not possible to detect them, due to corneal oedema for example, they could be observed on the AS-OCT image26. � e in� ammatory cells are between 10 and 20 µm and therefore, some may be below the limit of resolution of the OCT equipment. However they can be visualised since they tend to form groups, which facilitates their detection.
Group 3In group 3, the lesions in the only case classi� ed here
caused a shadow on the OCT examination due to their opacity, which prevented the posterior part of the lesion from being visualised; in this case the images did not
contribute any additional information to that obtained by biomicroscopy. � us, in the case of large tumours where their opacity does not allow light through or pigmented tumours, it has been observed that ultrasound biomicroscopy is superior to AS-OCT27.
When it comes to assessing the results of our study, both the context in which it was conducted and certain limitations must be taken into account. With respect to the context, this is the corneal and ocular surface unit of a tertiary hospital in which a wide variety of specialised corneal and conjunctival surgical techniques are performed, and to which patients are referred from a large healthcare area (516,000 inhabitants). � e usefulness of the technique would probably not be the same in the context of general ophthalmology, an area with fewer patients or in which certain surgical techniques such as corneal transplants, intrastromal segment implants, etc. are not performed. � is context also imposes certain limitations, as it is a public centre in which refractive surgery is not carried out. � e usefulness of AS-OCT examination in refractive surgery has been analysed in previous publications which are
191

ISSN: 2171-4703© 2010 SECOIRSociedad Española de Cirugía Ocular Implanto-Refractiva
ARTICLE
Intrastromal Corneal Ring Segment and intraocular lens implantation in patients with keratoconus and cataract
Jose F. Alfonso, MD, PhD1,2; Luis Fernández-Vega Cueto, MD1;David Madrid-Costa, OD, PhD3; Robert Montés-Micó, OD, PhD3
PURPOSE: To evaluate the e� cacy, safety and predictability of sequential KeraRing Intrastromal corneal ring segment (ICRS) and intraocular lens (IOL) implantation with opposite clear corneal incisions in patients with keratoconus and cataract.
SETTING: Fernandez-Vega Ophthalmological Institute (Oviedo, Spain).
METHODS: � is study comprised patients with keratoconus and cataract who had ICRS implantation , followed 6 months later by IOL implantation with corneal relaxing incisions. � e uncorrected (UDVA) and corrected (CDVA) distance visual acuities and residual refractive errors, analyzed using vector analysis, were recorded preoperatively, 6 months after ICRS implantation, and 6 months after IOL implantation.
RESULTS: � e study enrolled 32 eyes (21 patients). � e mean UDVA (Snellen decimal) was 0.02 ± 0.02 preoperatively, 0.06 ± 0.05 six months after ICRS implantation (P = 0.004), and 0.53 ± 0.22 six months after IOL implantation (P < 0.0001). � e CDVA changed from 0.46 ± 0.22 before surgery to 0.54 ± 0.21 six months after KeraRing ICRS implantation(P = 0.0002) and to 0.71 ± 0.19 six months after IOL implantation (P < 0.0001). Six months after IOL implantation, the e� cacy index was 1.15 and the safety index, 1.54. At 6 months, 70.97% of eyes were within ± 1.00 diopter (D) of the desired refraction and 45.16% were within ± 0.50 D. � e mean spherical equivalent after IOL implantation was –0.53 ± 1.13 D.
CONCLUSION: Sequential KeraRing ICRS and IOL implantation plus corneal relaxing incisions provides good visual and refractive outcomes, indicating that it is a predictable procedure for patients with keratoconus and cataracts.
J Emmetropia 2012; 3: 193-200
Keratoconus is a progressive, non-in� ammatory disorder of the cornea in which the cornea assumes a conical shape. � e corneal thinning induces irregular astigmatism, myopia and protrusion, leading to a mild
to severe decrease in the visual quality1,2. � e onset is usually at puberty, and progression mainly occurs until the third or fourth decade of life2. Recent studies have shown that intrastromal corneal ring segment (ICRS) implantation with femtosecond laser is an e� ective method for improving the corneal shape, reducing astigmatism and corneal higher order aberrations (HOAs) in patients with clear corneas and contact lens intolerance3-9. Indeed, a recently published study10
found that sequential ICRS and an implantable collamer phakic intraocular lens (IOL) with relaxing incision provided good visual and refractive outcomes, indicating that this is a predictable procedure for refractive correction of keratoconus. In this previous study, all patients were young and had clear lens. Logically, patients with cataract and keratoconuswill not obtain the same visual results as thosewith clear lens.
Submitted: 10/24/2012 Accepted: 11/6/20121 Fernández-Vega Ophthalmological Institute, Oviedo, Spain.2 Surgery Department, School of Medicine, University of Oviedo, Spain.3 Optics Department, Faculty of Physics, University of Valencia, Spain.
Financial Disclosure: � e authors have no proprietary interest in any of the materials mentioned in this article.
Corresponding Author: José F. Alfonso, MD, PhDInstituto Oftalmológico Fernández-Vega Avda. Dres. Fernández-Vega 34, 33012 (Oviedo), SpainTelf: +34 985 245533 Fax: +34 985 233288E-mail: [email protected]
OCT IN CORNEAL AND CONJUCTIVAL PATHOLOGY
JOURNAL OF EMMETROPIA - VOL 3, OCTOBER-DECEMBER
First author:
Victoria De Rojas MD, PhD
Complexo Hospitalario Universitario,A Coruña, Spain
segment optical coherence tomography of conjunctival nevus. Ophthalmology 2011; 118: 915-919.
23. Shen M, Li J, Wang J et al. Upper and lower tear meniscus in the diagnosis of dry eye. Invest Ophthalmol.Vis Sci. 2009; 50: 2722-2726.
24. Gumus K, Crockett CH, P� ugfelder SC. Anterior segment optical coherence tomography: a diagnostic instrument for conjunctivochalasis. Am J Ophthalmol. 2010; 150: 798-806.
25. Shousha MA, Pérez VL, Wang J et al. Use of ultra high resolution optical coherence tomography to detect in vivo characteristics of Descemet´s membrane in Fuchs` dystrophy. Ophthalmology 2010; 117: 1220-1227.
26. Agarwal A, Ashokkumar D, Jacob S, Agarwal A, Saravanan Y. High-speed optical coherence tomography for imaging anterior
chamber in� ammatory reaction in uveitis: clinical correlation and grading. Am J Ophthalmol. 2009; 147:413-416.
27. Bianciotto C, Shields CL, Guzman JM, et al. Assessment of anterior segment tumors with ultrasound biomicroscopy versus anterior segment optical coherence tomography in 200 cases. Ophthalmology 2011; 118: 1297-1302.
192





























