Embed Size (px)
Citation preview

Archives of Disease in Childhood 1994; 70: 319-326
Laryngo-onycho-cutaneous syndrome: aninherited epithelial defect
Roderic J Phillips, David J Atherton, Martin L Gibbs, Stephan Strobel, Brian D Lake
Hospital for SickChildren, London,Host Defence GroupRoderic J PhillipsDavid J AthertonStephan Strobel
OphthalmologyDepartmentMartin L Gibbs
HistopathologyDepartmentBrian D Lake
Correspondence to:Dr Rod Phillips, Departmentof Paediatrics, RoyalChildren's Hospital,Parkville, Victoria 3052,Australia.
Accepted 31 August 1993
11
III
IV
V
AbstractThree children with an unusual butclearly defined combination of clinicalfindings that appear to have been in-herited in an autosomal recessive mannerare described. All had developed laryngealabnormalities, chronic skin ulceration,nail dystrophy, and conjunctival diseasein infancy. In every case, dental enamelwas hypoplastic and both skin andmucosal surfaces demonstrated increasedsusceptibility to trauma. Progression ofdisease occurred, to life threatening res-piratory obstruction in two cases and toeffective blindness and fatal respiratoryobstruction in the third child. AUl of thesechildren came from the Pakistani ethnicgroup. No medical treatment has haltedprogression of this disease but lasertherapy has been partially successful inalleviating laryngeal manifestations.
Ultrastructural and immunohistologi-cal examination of unaffected skin wasundertaken in each child. No abnormalitywas found in the child with the mildestclinical disease. Both ofthe other childrenshowed abnormal hemidesmosomes onultrastructural examination. The mostseverely affected child also had abnor-mally weak immunoreactivity withantibodies G71 and GB3 directed againstbasal cell a6P4 integrin and the basementmembrane glycoprotein nicein respect-ively. These abnormal findings are alsoseen in skin from patients with junctionalepidermolysis bullosa.These three children have the laryngo-
onycho-cutaneous syndrome, which maynot be rare in their ethnic group. Theavailable clinical and pathological
Vll V12 V13 V14 V15 V26 V27 V2
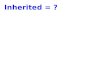
Figure 1 Family pedigree ofpatient 1. The arrow indicates the proband (VlS). Fourrelatives (a sister, Vl l, a brother, V12, and two male cousins, V26 and V27) weresimilarly affected and died in childhood. An affectedfemale relative, V28, is alive. Onebrother, V13, died ofunknown causes at 1 week of age. Open circles represent normalfemales, open squares are normal males, and diamonds do not specify gender.
evidence is consistent with this syndromebeing caused by an inherited defectaffecting the lamina lucida of the skinbasement membrane zone. The laryngo-onycho-cutaneous syndrome may there-fore represent a new and distinctive typeofjunctional epidermolysis bullosa.(Arch Dis Child 1994; 70: 319-326)
Over a period of one year, three childrenpresented with an unusual combination ofclinical problems. Each had developed ahoarse voice in the neonatal period and skin,nail, and conjunctival lesions during infancy.They shared a syndrome only recently recog-nised outside Pakistan and this study wasdesigned to identify the features and theaetiology of the disease.
Case reportsPATIENT 1This boy was the fifth child of consanguineousPakistani parents and was normal at birth. At 1week of age his voice became hoarse, and by 6months several toenails had become thickened.From 8 months ofage he had many episodes ofsoreness and swelling around his eyes. Sites oftrivial skin trauma sometimes healed normallybut occasionally failed to re-epithelialise,developing instead into indolent ulcers. Twofingernails that were lost after minor traumaregrew normally. Transient small blisters wereobserved on a few occasions on his skin andoral mucosa. He had recurrent bleeding fromhis gums.
Five of his relatives in Pakistan had the samesyndrome (fig 1). Of these, two siblings (V11and V12, fig 1) died of progressive respiratoryobstruction, at age 3 years (V11) and 6 years(V12) respectively. No details were availableconcerning the mode of death oftwo cousins atage 3 years (V26) and age 4 years (V27). Thefifth affected relative (V28) was alive at age 16years. One further sibling (V13) died ofunknown causes at 1 week of age withoutshowing any features of the syndrome.When first seen by us at 4 years of age,
patient 1 was a lively boy ofnormal growth anddevelopment who conversed readily, but onlyin a whisper. At the lateral aspect of each eye,mild symblepharon was present with localadhesions between the contiguous bulbar andtarsal conjunctiva and adjacent lid margins (fig2A). A slender frond of pink, moist tissue arosefrom this fused conjunctival tissue. Elsewhere,and in the fornices, the conjunctiva appearednormal. The abnormalities in each eye werevirtually identical. The vision was unimpaired.
319
on March 10, 2021 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.70.4.319 on 1 A
pril 1994. Dow
nloaded from

Phillips, Atherton, Gibbs, Strobel, Lake
Figure 2 Patient 1. (A) Right eye. A normal plica semilunaris can be seen at the medialcanthus; (B) toes of right foot.
The nails of the third digits of both hands andthe first and third digits of both feet werethickened and irregular without associatedinflammation (fig 2B), and the fifth toenailshad been lost. There were small ulcers on hishard palate and on his right pinna, and someareas of minor scarring, particularly on bothears. Hair and skin was otherwise normal andno blisters could be induced by rubbing. His
teeth showed hypoplastic enamel covered witha black extrinsic stain, interpreted as due tochromogenic bacteria. There was no evidenceof caries.
Direct laryngoscopy under anaesthesiashowed an extreme degree of obstruction ofthe airway by a laryngeal web and by largesupraglottic and glottic nodules (fig 3); thesewere partially removed by carbon dioxide laser.The polypoid mass in his left eye was surgicallyremoved. Histopathology of laryngeal tissueand of the conjunctival polyp showed acuteand active chronic inflammatory granulationtissue with no specific features. The results ofother investigations are given below.
Over the following year, progressive enlarge-ment of his airway was achieved with repeatedlaser treatment. No regrowth of abnormallaryngeal tissue occurred between treatments.The polyp removed from his left eye recurredwithin two months and further proliferation ofconjunctival tissue occurred in each eye. Whenlast seen, this bound the lateral quarter of bothlid margins and the contiguous bulbarconjunctiva together, giving rise to markedsymblephara. He remained otherwise well.
PATIENT 2This girl was the younger of two children ofconsanguineous Pakistani parents. She wasnormal at birth, but within two weeks haddeveloped a hoarse voice and, on the back ofher right wrist, transient blisters that becamechronic ulcers. By 6 months of age, these hadhealed but several other ulcers had developed,none preceded by blisters. Many of her nailswere abnormal, some with persistentparonychia. She had recurrent eye sorenessand nose bleeding. These problems continueddespite trials of steroid eye drops, antibioticsgiven systemically, topically or as eye drops,and nine months of oral antituberculoustreatment. In other respects she remained well.No other family member has had problemssimilar to those experienced by this patient.When first seen by us at 3 years of age, she
was an active child with normal developmentand a hoarse voice. She was mildly photo-phobic and had large conjunctival massesextending medially from the lateral canthusto the corneoscleral limbus in both eyes.
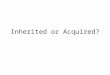
Figure 3 Patient 1. (A) Larynx as seen at laryngoscopy, showing almost total obstruction of the ainvay by a laryngealweb and multiple nodules; (B) key to (A).
320
on March 10, 2021 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.70.4.319 on 1 A
pril 1994. Dow
nloaded from

Laryngo-onycho-cutaneous syndrome: an inherited epithelial defect
Figure 4 Patient 2.(A) Face; (B) first toe, leftfoot.
The abnormal tissue bound the lid marginsand contiguous bulbar conjunctiva together,resulting in extensive symblepharon formation.In addition, a polypoid mass was noted to ariseseparately from the conjunctiva lining themedial aspect of the left upper lid. The remain-
Figure 5, Patient 3, aged 4 months. Fingernails on right hand.
ing conjunctiva appeared normnal. Superficialcorneal scarring was present on the left,consistent with previous corneal epithelialulceration, but vision was unaffected. Onher left cheek, there was a shallow, welldemarcated ulcer with a raised purple edge butno surrounding inflammation (fig 4A). Otherulcers were present on her ears, back, and fore-arms. Skin and hair were otherwise normal.The nails of the first and fifth toes of each footwere irregular, horny masses with surroundinginflammation (fig 4B). Other toenails andfingernails were variably affected. Her teethwere small with hypoplastic enamel.
Direct laryngoscopy under anaesthesiashowed a thin anterior web with overlying softpolypoid mucosa which was partially removedby carbon dioxide laser. Laryngeal biopsy wasunsuccessful. Histopathology of a section ofone conjunctival mass showed granulationtissue with mixed acute and chronic inflam-matory cell infiltration. The results of otherinvestigations are given below.
She was treated with iron and zinc supple-ments, and with steroid eye drops. Duringfollow up over two years, no improvement wasnoted in the lesions affecting her skin or nails,and the conjunctival granulation tissue becamemore extensive.
PATIENT 3This boy was the first child of unrelatedPakistani parents. He was normal at birth, but,within a week, his voice was noted to be soft.At this time, he received a barely noticeablescratch on the right cheek which, instead ofhealing, slowly developed into an indolentulcer. Removal of an adhesive plaster coveringthis first ulcer resulted in a second ulcer onadjacent unaffected skin, and a third developedunder the waistband of his nappy. Oversubsequent months, ulcers occurred in bothaxillae and over the occiput, and his circum-cision scar repeatedly broke down. Over thesame period, all of his nails became abnormal.In each case, proliferating tissue graduallylifted a previously normal nail off the nail bed,commencing distally. Several were shed andparonychia developed in some. He bledfrequently from skin ulcers, nail beds, gums,mouth, and nose. He had sore eyes from theage of 3 months. Treatment with oralflucloxadillin, griseofulvin, and ketoconazoleproduced no change in his condition. There isno family history of similar disease.When first seen by us at 4 months of age he
showed normal growth and development. Hehad oedematous eyelids and was photophobic.Ocular examination revealed thickened, con-gested bulbar conjunctiva at both lateral canthiand directly inferior to the cornea. There wasno proliferation or symblepharon formationand the remaining conjunctiva appearedhealthy. The epithelium over the inferioraspect of both corneas was loose and sloughedreadily. Vision, however, appeared normal.Skin texture was normal, and blisters were notinduced by handling or rubbing. Shallow,crusted ulcers were present on both cheeks, on
321
on March 10, 2021 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.70.4.319 on 1 A
pril 1994. Dow
nloaded from

Phillips, Atherton, Gibbs, Strobel, Lake
Figure 6 Patient 3, aged1 year. (A) Face; (B)teeth; and (C) eyes,attempted opening underanaesthesia.
B
the occiput, in both axillae, on the right elbowand on his flank. All nails had either been liftedup from the nail bed by what appeared to be amass of granulation tissue (fig 5) or had beenlost completely, leaving oozing or crustedgranulation tissue. No other abnormalitieswere noted.
Direct laryngoscopy under anaesthesiashowed normal vocal cords with swollen supra-glottic tissues. The oropharyngeal and nasalmucosa was friable with marked contactbleeding. Biopsies of the supraglottic tissue,abnormal conjunctiva, and the edge of theulcer on his elbow showed no evidence ofbacteria, mycobacteria, or fungi despite the useof special stains and culture. Histopathology ofall these specimens showed ulceration andacutely inflamed granulation tissue withoutgranulomas, giant cells or other specificfeatures. The results of other investigations aregiven below.
Over the subsequent 12 months, moderatelysevere anaemia (haemoglobin concentration62 g/l) responded to iron supplements, butprogression of the disease continued despitetrials of prednisolone (3 mg/kg/day), zinc,sulphapyridine, vitamins, and potent steroideye drops. He failed to thrive (weight 8-6 kg at16 months) and continued to lose blood frompharyngeal, skin (fig 6A), and nail bed lesions.Ulceration at the penile meatus led to strictureformation, chronic urinary obstruction, andthe need to repeatedly open the meatus underlocal anaesthesia. Focal masses, presumed tobe granulation tissue, developed at the gingivalmargin. The enamel of all eight incisors washypoplastic and the upper incisors had pro-gressively worn down to gum level (fig 6B).Proliferation of conjunctival tissue was moremarked than that seen in patients 1 and 2 andled to total occlusion of his left palpebralfissure and almost total occlusion of his right(fig 6C). An oculoplastic procedure wasperformed in which the adhesions between theupper and lower eyelids and between the lidsand the globe were divided bilaterally, excesstissue was excised, and scleral shells wereinserted. However, within weeks the adhesionsreformed and his vision became severelyobstructed again.
In addition to the above problems, he alsodeveloped worsening stridor. Direct laryngo-scopy on two occasions showed increasingepiglottic and supraglottic oedema with ulcera-tion and contact bleeding, swollen and poorlydefined vocal cords, and a normal trachea. Hedied at 18 months of age as a direct resultof upper airway obstruction. Permission forpostmortem was declined.
MethodsShave skin biopsies of clinically unaffectedskin were taken and prepared for ultrastruc-tural and immunohistological examination aspreviously described.' Immunohistologicalmapping of the basement membrane zonewas performed using three antibodies. Two ofthese, LH7-2 directed against epitopes on
-:- collagen type VII as found in anchoring fibrils
322
on March 10, 2021 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.70.4.319 on 1 A
pril 1994. Dow
nloaded from

Laryngo-onycho-cutaneous syndrome: an inherited epithelial defect
'g
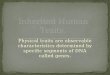
Figure 7 Electron micrographs of the dermoepidermal junctton in skin from (A) patient 1 and (B) patient 3. In (A)normal hemidesmosomes can be seen (arrows). In (B) hemidesmosomal attachment plaques and subbasal dense plates arepoorly defined. Scale mark= 1 micron.
and GB3 directed against the basementmembrane glycoprotein nicein in the laminalucida, were used as previously described.'The third antibody, G7 1, a gift from Dr John
Aplin, is directed against the ,B4 subunit ofthe integrin x6P4 complex,23 which is a
component of hemidesmosomes.4 It was
used at a dilution of 1:400 on cryostatsections.
A
It.,
B
* .i *
'""(A.
C
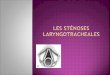
Figure 8 Antibody G71 immunoperoxidase binding at thebasement membrane zone (arrowed) in (A) patient 2,showing normal immunoreactivity; (B) patient 3, showingweak and patchy immunoreactivity; and (C) a child withjunctional epidermolysis bullosa, showing absentimmunoreactivity (X 110).
ResultsLight microscopic examination of shavebiopsies of unaffected skin was normal in allthree patients. Results of ultrastructural (fig 7)and immunohistochemical (fig 8) examinationare given in table 1. Other tests which gave an
abnormal result in any patient are listed intable 2. The results of the following investiga-tions were normal.
Haematology: white cell count and differen-tial, reticulocyte count, haemoglobin electro-phoresis, C reactive protein, coagulationstudies, bleeding time, and sickle cell trait.
Biochemistry: concentrations of glucose,urea, sodium, potassium, calcium, mag-nesium, phosphate, creatinine, bilirubin,copper, zinc, selenium, folate, vitamin B12,vitamin A, retinol binding protein, aminoacids, and organic acids and activities of alka-line phosphatase and aspartate transaminase,and chromosomes.
Immunology: IgG, IgA, IgM, IgE, radio-allergosorbent test (milk, egg, wheat, housedust mite), isohaemagglutinins, nitrobluetetrazolium test for neutrophil oxidativefunction, T cell subsets (CD2, CD3, CD4,CD8, CD14, CD16, CDl9, CD56), lympho-cyte phytohaemagglutinin stimulation, leuco-cyte adhesion molecules (CD1 1A, CD1 1B,CD 18), staphylococcal killing, autoantibodiesto antinuclear antibody, extractable nuclearantibody, reticulin, mitochondria, antineutro-phil cytoplasmic antibody, gastric parietal cell(weakly positive patient 1) and smooth muscle(weakly positive patients 1 and 3), antibodiesto common respiratory pathogens (present),antibodies to diphtheria and tetanus (present),fungal precipitins (absent), and the VenerealDisease Research Laboratory test.
Urine: excretion of organic acids, aminoacids, and protein.
Radiology: radiography of chest, sinuses,lateral skull, neck and knee, echocardiography,cranial ultrasound, and abdominal ultra-sound.
eI
r t
''i; 4J
'.
323
*; .0i
- i,
on March 10, 2021 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.70.4.319 on 1 A
pril 1994. Dow
nloaded from

Phillips, Atherton, Gibbs, Strobel, Lake
Table 1 Histologicalfindings in clinically unaffected skinfrom patients with thelaryngo-onycho-cutaneous syndrome (see figs 7 and 8)
Patient I Patient 2 Patient 3
UltrastructureHemidesmosomes Nonnal Poorly defined Poorly definedAnchoring fibrils Normal Normal Normal
ImmunohistochemistryGB3 Normal Normal DecreasedG7 1 Normal Normal Decreased, patchyLH7-2 Normal Normal Normal
Microbiology: no fungi could be seen on
direct microscopy of nail scrapings or grown inculture. Staphylococcus aureus was culturedfrom infected nail beds in patients 2 and 3. Noother positive result was obtained from cultureof blood, urine, or faeces.
DiscussionThese three children and the other affectedrelatives of patient 1 share an unusual, welldefined set of clinical features that appear tohave been inherited in an autosomal recessivemanner (table 3). This is the laryngo-onycho-cutaneous syndrome, described by Shabbiret al in Pakistan in 1986.5 Subsequent to ourrecognition of the diagnosis in these children,we have searched for other individuals with thefeatures listed in table 3 and we are aware ofanother five, previously undiagnosed childrenwith the syndrome in the United Kingdom.6Hence it may not be rare within the ethnicgroup originating in the north west of theIndian subcontinent. A description of two ofthose five children has appeared elsewhere.7 8The extent of organ involvement varies con-
siderably in this syndrome but the prognosis isgenerally poor. Of the reported cases, mostdied in childhood,57 presumably from causesrelated to respiratory obstruction and/orsecondary infection. Before this paper, deathshave not been recorded in the UnitedKingdom. However, three children haverequired permanent tracheostomies. Thisprocedure itself raises concerns that an
indwelling tracheostomy tube in these patientsmay induce granulation formation andobstruction distally in the trachea. The alter-native of surgical relief of respiratory obstruc-tion has proved satisfactory so far in our
patients (1 and 2), but less so in another child
where recurrence and extension of obstructionwas observed despite three conventionalexcisions. It remains to be seen whether laserexcision provides better long term results thanother surgical methods.
Visual impairment is another major cause ofmorbidity. No mention of eye involvement wasmade in the original report of the syndrome,5but eye abnormalities do appear to be presentin the accompanying photographs and aredescribed in a subsequent report of the samechildren.7 All patients in the United Kingdomhave external eye involvement. Eye problemsrange from episodic eye pain and/or slowlyprogressive conjunctival scarring (for examplepatients 1 and 2) to complete blindness in twochildren. Surgery temporarily restored somevision in patient 3 but within weeks his visionwas again compromised. No treatment has yetbeen shown to have long term benefit for theeyes in this syndrome.The third major cause of morbidity is the
chronic ulceration of skin and nails. This variesin severity from being almost asymptomatic, asin patient 1, to the extensive ulceration withparonychia, blood loss and anaemia seen inpatient 3. One child with mild skin diseaseshowed resolution of skin manifestations by 5years of age.7 In more severe cases, meticulousattention to dressings and protection fromrubbing leads to healing of ulcers and nail bedlesions but may take months and is extremelylabour intensive for the parents.
Although most children with the laryngo-onycho-cutaneous syndrome have progressivemorbidity from infancy and death duringchildhood, this is not always the case. In onechild reported from Pakistan, problemscommenced after infancy, remained relatively
Table 3 Features seen in the laryngo-onycho-cutaneoussyndrome
Muslim Pakistani/Indian ethnic originAutosomal recessive inheritanceNormal appearance at birthHoarse voice, usually within weeks of birthMucosal and laryngeal granulationChronic skin ulcers, usually from infancyChronic nail dystrophy, usually from infancyConjunctival lesions, usually from infancyHypoplastic dental enamelNormal intellectual development in most casesDeath during childhood in most cases
Table 2 Results of investigations that were abnormal in any patient
Investigation(units) (normal range)* Patient 1 Patient 2 Patient 3
Haemoglobin (g/l) 106 102 92Mean corpuscular volume (fl) (70-86) 68 69 73Platelets (150-400X109A1) 293 631 1090Erythrocyte sedimentation rate(<10 mm/hour) 10 20 70
Albumin (g/l) (35-55) 38 37 31Ferritin (,ug/l) (7-150) 5 4 8Iron (,umolA) (14-25) 8 2 7IgG1 (g/l) 8-0 (3-3-7-3) 6-4 (3-3-7-3) 2-8 (1 1-6-0)IgG2 (g/l) 2-0 (0 4-1-9) 1-3 (0 4-1 9) 0-4 (0-4-0-9)IgG3 (g/l) 0-05 (0-15-0-37) 0-20 (0-15-0-37) 0-80 (0-05-0-36)IgG4 (g/l) 0-06 (0 05-0 32) 0-24 (0-05-0-32) 0-09 (0-05-0-18)C3 (g/l) (1-3-5-7) 7-0 >24 12C4 (g/l) (02-07) 0-8 >2-5 >2-5Immune complexes Absent Present Present
*If normal range is not constant for all patients it is given in parentheses after the individual test result.
324
on March 10, 2021 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.70.4.319 on 1 A
pril 1994. Dow
nloaded from

Laryngo-onycho-cutaneous syndrome: an inherited epithelial defect
Hemidesmosome,Attachment plaque, SBDP
-Anchoring fibrils
Figure 9 Structure of the dermoepidermal junction in normal skin (SBDP=sub-basaldense plate).
mild, and substantially resolved during teenageyears.7Of the pharmacological treatments tried to
date, only iron supplementation has shown a
clear, albeit limited benefit, namely partialresolution of anaemia. Oral prednisolone atdoses up to 3 mg/kg/day may have initiallyaccelerated skin healing in patient 3, but anybenefit was not sustained. Flucloxacillin hadlittle effect on the paronychia and there was no
response to antituberculous, antifungal, or
sulpha drugs.The distinctive clinical picture limits the
differential diagnosis in these children. It isnot consistent with any of the acquired bullousdisorders of childhood, nor any of theectodermal dysplasias. A vasculitic disorder isunlikely, both on clinical grounds and becauseof the absence of supporting evidence frominvestigations. No evidence to suggest an
immunodeficiency was found: none of our
patients showed a predisposition to common
infections other than paronychia, and testing ofthe humoral, T cell, and phagocytic branchesof the immune system did not reveal an
immune defect. A primary infective cause isalso unlikely on account of the ethnic speci-ficity, the evidence of autosomal recessiveinheritance, the early onset, and our inabilityto find a causative infective agent.We suggest that the disease in these children
is related to junctional epidermolysis bullosa.This disease is one of a group of inheritedstructural defects of the skin that result inskin fragility and are collectively labelled as
epidermolysis bullosa. Junctional epidermoly-sis bullosa is characterised by defects at thelevel of the lamina lucida of the skin basementmembrane (fig 9). Superficially, an associationbetween the laryngo-onycho-cutaneous syn-drome and junctional epidermolysis bullosaseems unlikely, as children with the latterdisease typically have extreme skin fragility andextensive skin blistering within days of birth.This was not seen in our patients. Even themost severely affected child, patient 3, couldbe handled without any precautions by his
parents without showing any mechanical skinfragility. However, there are some strikingsimilarities between the two conditions.Children with junctional epidermolysis bullosacan show involvement of:* Larynx: hoarseness within weeks of birth
is common and fatal laryngeal disease has beenreported.9
* Teeth: enamel hypoplasia is usuallypresent and can be severe. Microscopiccleavage at the dental basal lamina duringdevelopment has been demonstrated.1012
* Eyes: the progressive, extensive symble-pharon formation and growth of inflammatorytissue that has been seen in the laryngo-onycho-cutaneous syndrome has not beenreported in junctional epidermolysis bullosa.However, small, localised symblepharabetween cornea and lid margin are well docu-mented in junctional epidermolysis bullosa, asare conjunctival and corneal erosions andscarring.12 13
* Nails: virtually all patients with junctionalepidermolysis bullosa show nail changes.These may be mild or may be severe withcomplete onycholysis, nail bed ulceration, andflorid granulation tissue.
* Skin: indolent ulcers identical in appear-ance to those seen in patients 1-3 are commonin junctional epidermolysis bullosa'4 and canoccur without a history of blistering.Our conviction on clinical grounds of an
association between the laryngo-onycho-cutaneous syndrome and junctional epider-molysis bullosa is further strengthened by (i)the blisters seen in patients 1 and 2; (ii) thedevelopment of an ulcer after removal ofadhesive tape (patient 3); (iii) the developmentof ulcers at sites exposed to repeated rubbingor trivial trauma (all patients); and (iv) the firstand fifth toenails always being the worstaffected. All these observations suggest that aninherent epithelial weakness is present in thelaryngo-onycho-cutaneous syndrome.Some confirmation of a link between
the laryngo-onycho-cutaneous syndrome andjunctional epidermolysis bullosa has beenprovided by the electron microscopic appear-ance of abnormal hemidesmosomes in two ofour patients (fig 7). We have also foundabnormal hemidesmosomes in another patientwith the laryngo-onycho-cutaneous syndrome.4Poorly defined or rudimentary hemidesmo-somes are characteristic of most patients withjunctional epidermolysis bullosa. The othercharacteristic ultrastructural finding in junc-tional epidermolysis bullosa, namely a cleavageplane at the level of the lamina lucida, was notseen in our patients. However, a cleavage planeis occasionally not seen in patients with junc-tional epidermolysis bullosa if their skin is notparticularly fragile. The absence of a split in ourpatients does not preclude them from having aform of junctional epidermolysis bullosa.Of the three antibodies used in this study for
immunohistochemical analysis, LH7 2 andGB3 have been well characterised in epider-molysis bullosa. LH7-2 delineates anchoringfibrils and its immunoreactivity is normal injunctional epidermolysis bullosa and weak or
325
on March 10, 2021 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.70.4.319 on 1 A
pril 1994. Dow
nloaded from

Phillips, Atherton, Gibbs, Strobel, Lake
absent in recessive dystrophic epidermolysisbullosa. 15 GB3 binds to the lamina lucidaglycoprotein nicein (also known as epiligrinor BM600) 16 and its immunoreactivity isweak or absent in most cases of junctionalepidermolysis bullosa. The third antibodyused, G7 1, is directed against the P4 subunit ofo634 integrin, a glycoprotein complex that islocalised to hemidesmosomes and is thought tohave a major role in epithelial adhesion.2 3 TheG7 1 antibody is therefore of considerableinterest in diseases in which epithelial adhesionis deficient. We have recently shown that skinfrom each of nine patients with known junc-tional epidermolysis bullosa whom we testedshowed decreased immunoreactivity with thisantibody, whereas skin from patients withother forms of epidermolysis bullosa showednormal immunoreactivity.'7 Thus G71 can beregarded as a useful marker for the diagnosis ofjunctional epidermolysis bullosa. Of our threepatients, patient 3 showed abnormally weakimmunostaining with both G71 (fig 8) andGB3 (table 1), again suggestive of a linkbetween the laryngo-onycho-cutaneous syn-drome and junctional epidermolysis bullosa.
It is interesting that there is a correlationbetween the histological findings in our patientsand their clinical course. No histologicalabnormalities were seen in skin from patient 1with the mildest disease, ultrastructural but notimmunohistochemical abnormalities were seenin patient 2, and both ultrastructural andimmunohistochemical abnormalities were pre-sent in patient 3 with the most severe andultimately fatal disease. A similar correlation isknown for junctional epidermolysis bullosawhere more striking pathological abnormalitiesgenerally imply severe skin disease.None of the histological findings in our
patients are suitable for prenatal diagnosis atthis time and, as yet, there is no informationabout the location of the genetic defect. Thevariability between patients in our series couldbe explained if several gene mutations affectingone protein are being carried by this popula-tion. Different combinations might give differ-ent clinical effects as has been shown in otherdiseases.On the available clinical and pathological
evidence, we would propose that the laryngo-onycho-cutaneous syndrome is caused by aninherited defect affecting the lamina lucida ofthe skin basement membrane zone and that itmay therefore represent a new and distinctivetype of junctional epidermolysis bullosa. Bycomparison with the common 'Herlitz' form ofjunctional epidermolysis bullosa, the laryngo-onycho-cutaneous syndrome shows littlemechanical skin fragility but a greater predis-position to granulation tissue formation at sitesof mild trauma. This proliferation of granula-tion tissue may be a secondary phenomenonrelated to an inability of the normal epithelial
repair mechanisms to function properly in thepresence of an abnormality of basementmembrane adhesion. We suggest that thename laryngo-onycho-cutaneous syndromeused by Shabbir et al in their seminal work5should at present be retained.We are grateful to the following people for assistance (Hospitalsfor Sick Children unless otherwise specified): Professor GShabbir (Mayo Hospital, Lahore); Mr D Tavlor, Mr M Kerr-Muir (St Thomas's Hospital, London), and Mr J Collin(Moorfields Eve Hospital, London) for eye examinations,biopsies and treatment; .Mr D Albert for larvngoscopic exami-nations, biopsies and treatment; Dr A McCartney (Institute ofOphthalmology, London) and Professor R Eady (St Thomas'sHospital, London) for helpful discussions; Mrs V Smith andMiss A Puri for expert technical assistance in electronmicroscopy and cytochemistry; Dr J Aplin (Universitv ofManchester) for a gift of antibody G7 1; Dr G Roberts, Mr DPlint, and Miss K Harlev for dental examinations; the nationalepidermolysis bullosa association DEBRA for financial supportfor purchase and maintenance of a Diatome ultramicrotomeknife; and Dr M Crock, Dr C Crock, and Mr H Crock(Cromwell Hospital, London) for reviewing the manuscript.
1 Phillips RJ, Harper JI, Lake BD. Intraepidermal collagentype VII in dystrophic epidermolysis bullosa: report of fivenew cases. BrjDenrmatol 1992; 126: 222-30.
2 Aplin JD, Sief MW. Basallv located epithelial cell surfacecomponent identified by a novel monoclonal antibodytechnique. Exp Cell Res 1985; 160: 550-5.
3 Aplin JD, Satter A, Mould AP. Variant choriocarcinoma(BeWo) cells with differing adhesion and migrationto fibronectin display conserved pattems of integrinadhesion. ] Cell Sci 1992; 103: 435-44.
4 Sonnenberg A, Calafat J, Janssen H, et al. Integrin a634complex is located in hemidesmosomes, suggesting amajor role in epidermal cell-basement membraneadhesion. JCell Biol 1991; 113: 907-17.
5 Shabbir G, Hassan M, Kazmi A. Larvngo-onycho-cutaneous syndrome. Biomedica 1986; 2: 15-25.
6 Phillips RJ, Strobel S, Gibbs M, Atherton DJ. Laryngo-onvcho-cutaneous svndrome: a new form of junctionalepidermolysis bullosa? Proceedings of the British PacdiatricAssociation Anniiual Meeting. Warwick, April 1992: 69.
7 Ainsworth JR, Shabbir G, Spencer AF, Cockbum F.Multisvstem disorder of Punjabi children exhibitingspontaneous dermal and submucosal granulation tissueformation: logic syndrome. Clinical DvsniorphologD 1992;1: 3-14.
8 Ainsworth JR, Spencer AF, Dudgeon J, Geddes NK, LeeWR. Laryngeal and ocular granulation tissue formation intwo Punjabi children: logic syndrome. Eve 1991; 5:717-22.
9 Davies H, Atherton DJ. Acute larvngeal obstruction injunctional epidermolysis bullosa. Pediatr Derinatol 1987;4: 98-101.
10 Winter GB. Dental problems in epidermolysis bullosa. In:Priestlev GC, Tidman MJ, Weiss JB, Eady RAJ, eds.EpidennolNsis bullosa: a conprehensive reziew of classifi-catioon, tianagement and laboratory sti4dies. Crowthorne,Berkshire: Dystrophic Epidermolvsis Bullosa ResearchAssociation, 1990: 21-7.
11 Brain EB, Wigglesworth JS. Developing teeth in epider-molysis bullosa hereditaria letalis. Br Dent J 1968; 124:255-60.
12 Holbrook KA. Extracutaneous epithelial involvement ininherited epidermolysis bullosa. Arch Dennatol 1988; 124:726-31.
13 McDonnell PJ, Schofield OMV, Spalton DJ, Eadv RAJ. EL einvolvement in junctional epidermolysis bullosa. ArchOphthalniol 1989; 107: 1635-7.
14 Lin AN, Carter DM, Caldwell-Brown D. Wound healingand cultured epidermal autografts in epidermolvsisbullosa. In: Priestley GC, Tidman MJ, Weiss JB, EadvRAJ, eds. Epidennolvsis buillosa: a co?nprehensive revi.ew ofclassificationl, managemient anid laboratory, studies. Crow-thorne, Berkshire: Dystrophic Epidermolysis BullosaResearch Association, 1990: 152-5.
15 Leigh IM, Eady RAJ, Heagerty AHM, et al. Type VIIcollagen is a normal component of epidermal basementmembrane which shows altered expression in recessivedystrophic epidermolysis bullosa. J Inivest Dermiatol 1988;90: 639-42.
16 Domloge-Hultsch N, Gammon WR, Briggaman RA, GilSG, Carter WG, Yancey KB. Epiligrin, the major humankeratinocyte integrin ligand, is a target in both an acquiredautoimmune and an inherited subepidermal blisteringskin disease. Clirn Invest 1992; 90: 1628-33.
17 Phillips RJ, Aplin JD, Lake BD. Antigenic expression ofintegrin cs6fl4 in junctional epidermolvsis bullosa.Histopathology 1994 (in press).
326
on March 10, 2021 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.70.4.319 on 1 A
pril 1994. Dow
nloaded from