Embed Size (px)
Citation preview
May 1,1984 THE AMERICAN JOURNAL OF CARDIOLOGY Volume 53 1405
Atrial Fibrillation Induced by Adenosine Triphosphate
BERNARD BELHASSEN, MD AMIR PELLEG, PhD
DAVID SHOSHANI, MD SHLOMO LANIADO, MD
Adenosine triphosphate (ATP) has been successfully used for years in Europe for prompt termination of paroxysmal supraventricular tachycardia.’ Drury and Szent-Gyorgyis noted more than 50 years ago that in the presence of adenosine, atria1 flutter and atria1 fibrilla- tion (AF) could be readily induced by atria1 pacing. Similar findings were subsequently observed in exper-
From the Department of Cardiology, Tel Aviv Medical Center, lchilov Hospital, Tel Aviv, Israel, and the Cardiac Electrophysiology Laboratory, Hahnemann University, 230 North Broad Street, Philadelphia, Penn- sylvania 19102. Manuscript received December 23, 1983; revised manuscript received March 2, 1984, accepted March 5, 1984.
imental studies with ATP.:+ In the patient reported herein, AF developed after the administration of ATP during both atria1 and ventricular pacing. This is the first report of the fibrillatory effects of ATP in the human atrium.
The patient, a 51-year-old man, was referred for electro- physiologic evaluation of recurrent AF associated with Wolff-Parkinson- White syndrome. In the last year before his admission, he had 2 episodes of AF with rapid ventricular rates. The first episode converted spontaneously to sinus rhythm upon arrival to hospital; the second episode, which lasted several hours, was terminated by intravenous lido- Caine. In both instances, the shortest RR interval during preexcited beats was 240 ms. Physical examination and noninvasive studies revealed no evidence of organic heart disease. The electrocardiogram showed normal sinus rhythm and left posteroseptal preexcitation. During exercise testing (maximal rate 170 beatslmin), the degree of preexcitation diminished and no arrhythmia was induced. Antiarrhythmic therapy was discontinued for 72 hours before the electro- physiologic study. Quadripolar electrode catheters were placed in the high right atrium, His bundle area and right
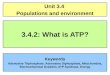
FIGURE 1. Induction of atrial fibrillation during atrial pacing after administration of adenosine triphosphate. Leads I, II, Ill, VI and intracardiac electrograms from the His bundle (HBE) and high right atrium (HRA) are shown. Twenty sec- onds after the bolus administration during atrial pacing, atrial fibrillation is induced.
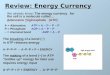
FfGURE 2. Induction of atrial fibrillation during ventricular pacing after admin- istration of adenosine triphosphate. The figure is arranged as Figure 1 except for ECG leads I, II and Ill, which are omitted. Transient high-degree ventriculoatrial block develops 18 seconds after ad- ministration of adenosine triphosphate. A few seconds later, after resumption of 1:l retrograde conduction, atrial fi- brillation occurs.

1406 BRIEF REPORTS
ventricular apex. Both atria1 and ventricular stimulation were performed with stimulus intensity at twice diastolic threshold. The anterograde effective refractory period of the accessory pathway was 260 ms at a basic cycle length (CL) of 600 ms. The minimal atria1 CL that resulted in I:1 con- duction through the accessory pathway was 250 ms. No arrhythmia could be induced by either single or double atria1 extrastimulation or rapid atria1 pacing up to a CL of 240 ms. During right ventricular pacing, progressive prolongation of ventriculoatrial (VA) conduction time was noted during both incremental pacing and extrastimulation. Retrograde atria1 activation had a low-to-high sequence. VA block oc- curred at a CL of 300 ms. No arrhythmia could be induced by either ventricular extrastimulation OF rapid ventricular pacing.
Bolus injections of 20 mg of ATP (Striadyne, Lab Auclair, France) were administered through a femoral vein 10 min- utes apart during atria1 and ventricular pacing at a CL of 400 ms. No arrhythmia occurred during the 3-minute period of control pacing. During atria1 pacing, AF2 minutes in dura- tion occurred 20 seconds after the administration of ATP (Fig. 1). When ATP was given during ventricular pacing, transient (2-second) high-degree VA block occurred after 18 seconds; then, I:1 conduction resumed (Fig. 2). Four seconds later, AF that lasted for 15 minutes occurred. The shortest RR interval during both episodes of AF was 250 ms.
A close relation between the administration of ATP and the occurrence of AF was present in our patient. AF developed 20 to 22 seconds after the administration of ATP during both atria1 and ventricular pacing at a CL of 400 ms. This is in agreement with the pharmacoki- netics of ATP, which reaches its maximal effect 10 to 30 seconds after its administration.‘y2 Induction of AF after ATP contrasted with the noninducibility of AF during atria1 pacing at shorter CLs.
The occurrence of AF was probably not related to vagal stimulation induced by ATP or its principal me- tabolite, adenosine, since studies in humans have shown that the actions of both compounds are independent of
the vagus.4,5 However, the occurrence of AF was prob- ably caused by the shortening of atria1 action potential duration after ATP or adenosine.6 This alteration in the action potential duration apparently overcomes the hyperpolarization of atria1 cells by adenosines (and probably ATP), which would tend to reduce the sus- ceptibility to AF. A critical short atria1 CL was also an important factor in initiation of AF. Indeed, AF devel- oped during ventricular pacing only after resumption of 1:l VA conduction and not during transient VA block.
Despite a wide clinical use of ATP in the acute man- agement of paroxysmal supraventricular tachycardia, there has been no reported case of induction of AF after administration of ATP during tachycardia. This suggests a very low probability of occurrence of AF in a clinical setting. The occurrence of AF after ATP ad- ministration in our patient was probably facilitated by administration of the drug during cardiac pacing. Fur- ther studies are required to determine whether ad- ministration of ATP during cardiac pacing could be used as a diagnostic tool to identify patients susceptible to development of AF.
1.
2.
3.
4.
5.
6.
References
Belhassen B, Pelleg A, Shoshanl II, Geva B, Laniado S. Electrophysiologic effects of adenosine 5’-triphosphate (ATP) on atrioventricular reentrant tachvcardia. Circulation 1983:88:827-833. Drub AN, Szent-Gy(irgyi A. The physiologic activity of a&nine compounds with especial reference to their actions upon the mammalian heart. J Physiol ILond1 1929:68:213-236. irelIes A, Belhassen B, Terdfman R, Shargorodsky B, Laniado S. Electro- physiologic effects of adenosine triphosphate and adenosine on the canine heart (abstr). Fed Proc 1983;42:731. Lechat P, Tonet JL, Cohen A, Frank R, Fontaine G, Grosgogeat Y. Mech- anism of atrioventricular conduction blockade by adenosine triphosphate (abstr). Circulation 1982;86:suppl ll:ll-380. DlMarco JP! Sellers TD, Berne RM, West GA, Belardinetll L. Adenosine: electrophyslologic effects and therapeutic use for terminating paroxysmal supraventricular tachycardia. Circulation 1983;68:1254-1263. Belardtneltl L, tsenberg 0. Isolated atrial myocytes: adenosine and acetyl- choline increase potassium conductance. Am J Physiol 1983;244:H734- H737.
Orthostatic Atrial Tachycardia: Autonomic Influence on
Atrial Pacemakers
BRUCE B. LERMAN, MD ERIC J. TOPOL, MD
EDWARD V. PLATIA, MD KENNETH L. BAUGHMAN, MD
Orthostatic atria1 tachycardia (AT) is a rare rhythm disturbance characterized by persistent tachycardia and an exaggerated rate increase related to orthostasis.1-3 First described as a separate entity in 1940,l only 2 cases have since been reported.2*3 No study has characterized the mechanism of the rhvthm or included electro-
From the Clinical Electrophysiology Laboratory, The Johns Hopkins Hospital, Division of Cardiology, Department of Medicine, The Johns Hopkins School of Medicine, Baltimore, Maryland 21205. Manuscript received September 22, 1983, revised manuscript received March 2, 1984, accepted March 3, 1984.
physiologic evaluation. We present electrophysiologic data from a patient with orthostatic AT that reveal the automatic properties of the rhythm and its unique au- tonomic dependence.
A 34-year-old woman was referred for evaluation of re- fractory AT. She had episodic palpitations for 20 years, often associated with dizziness and weakness. Symptomatic epi- sodes were usually precipitated by a change in position from supine to sitting OF standing. They occurred as many as 20 times per day, and lasted for as long as 30 minutes. In the last 2 years she received propranolol, verapamil, quinidine and disopyramide, which were ineffective singly and in combi- nation. Blood pressure was 130/80 mm Hg and supine pulse was 110 beatslmin. M-mode and 2-dimensional echocardi- ograms, chest roentgenogram, thyroid function tests, blood chemistries and urine collection for catecholamines and metabolites were normal. Supine electrocardiogram showed a regular rate of 110 beatslmin and an inverted P wave in lead aVL. The P-wave axis was 90’. When the patient as- sumed the upright position, the heart rate abruptly in- creased to 150 beatslmin, while the P-wave morphologic features and axis did not change. Carotid sinus pressure did not alter the atria1 rate or produce atrioventricular block.








![Increased Rate of Adenosine Triphosphate …...(CANCER RESEARCH 55, 4352-4360, October 1, 1995] Increased Rate of Adenosine Triphosphate-dependent Etoposide (VP-16) Efflux in a Murine](https://img.pdfslide.net/doc/110x75/5e7e8d68c5d0407f2447f2a9/increased-rate-of-adenosine-triphosphate-cancer-research-55-4352-4360-october.jpg)