Embed Size (px)
Citation preview
Atypical pneumonia
1938, H.A.Reimann, atypical pneumonia : not caused by influenza virus, psittacosis different from other pneumonia
Causes of Community-Acquired Atypical PneumoniaMycoplasma M.pneumoniaeRespiratory tract virus Influenza, adenovirus, RSV, parainfluenza virusOther viral agents Varicella-zoster, measles, EBVRickettsia C. burnetii (Q fever)Chlamydia C.psittaci (psittacosis), C.pneumoniaeBacteria Legionella, F.tularensis, Y.pestis, B.anthracisFungi Histoplasma, Blastomyces, Coccidioides
From Fishman’s pulmonary diseases and disorders. 3rd Ed. Morton NS.
Nonzoonotic atypical pneumonia (not spread from animal to human)
Mycoplasma pneumonia (M.pneumoniae)
Legionnaires’ diseases (Legionella species)
Chlamydia pneumonia (Chlamydia pneumoniae)
Zoonotic atypical pneumonia (spread from animal to human)
Psittacosis(Chlamydia psittaci)
Q fever (Coxiella burnetii)
Tularemia (Francisella tularensis)
Atypical pneumonia
Mycoplasma infection
• Smallest free living organism(100-300nm)• Lack of cell wall : no Gram staining, resistant to -lactam• M.pneumoniae M.hominis Ureaplasma urealyticum : urinary calculi
PathogenesisAdhesion to host cell induction of ciliostasisNon-specific stimulation of B lymphocyte trigger autoAb reactive with brain, heart, muscle, erythrocyte I AgIgM autoAb(cold agglutinins) agglutinate human erythrocyte at 4℃
Mycoplasma pneumonia
Epidemiology
• 10-20% of all pneumonia• Common causes of tracheobronchitis, bronchiolitis, pharyngitis• Symptoms persist for weeks or month• Spread by aerosol from person to person• Incubation period 1-3weeks
Common misconception that M.pneumoniae disease is rare among the very young and among older adults has led to a failure of physicians even to consider this conditon in the differential diagnosis.
Clinical Features
• Tracheobronchitis is the most frequent.• Primary cause of “walking” or “atypical” pneumonia(3-10%).• Sore throat, headache, chills, coryza, general malaise(rigors very rare)• Sometimes myringitis(5%), otitis• Lung abscesses, pneumatoceles, extensive lobar consolidation, respirat
ory distress and pleural effusion(20%) may develop.
<P/E>• No findings on chest auscultation even if pneumonia is present• Rales, wheeze present later• Sinus tenderness, pharyngeal erythema, erythema or bulla of tympanic m
embrane, nonprominent cervical adenopathy
Mycoplasma pneumonia
Extrapulmonary Complication
⑴ Hemolytic anemia antibodies to I Ag on erythrocyte membrane cold agglutinin response(60%) positive Coombs’ test, reticulocytosis ⑵ Mucocutaneous lesions(25%) erythematous maculopapular and vesicular exanthems ulcerative stomatitis, conjunctivitis⑶ Gastrointestinal symptoms(25%) nausea, vomiting(common), pancreatitis(rare)⑷ CNS(0.1%) meningoencephalitis, aseptic meningitis, encephalitis, ascending paralysis, transverse myelitis slow recovery, permanent neurologic deficit sometimes ⑸ Rheumatologic symptoms arthralgia(common), actual arthritis(rare)⑹ Cardiac involvement(rare) myopericarditis, hemopericardium, CHF, complete heart block
Mycoplasma pneumonia
Laboratory Abnormalities
① Routine lab is usually normal. Thrombocytosis Leukocytosis(1/4) ESR(1/3)② Subclinical hemolytic anemia positive Coombs’ test , reticulocytosis
Chest X-ray
① Peribronchial pneumonia : most common thickened bronchial shadow streaks of interstitial infiltration atelectasis② Pleural effusion(20%)③ Nodular infiltration④ Hilar adenopathy
uncommon
Mycoplasma pneumonia
Diagnosis
There are no distinguishing clinical or radiologic manifestations that allow a secure diagnosis of mycoplasma pneumonia versus other causes of atypical pneumonia such as chlamydia or legionella.
⑴ Serologic test (IgM and IgG antibody to M.pneumoniae by ELISA or CF test) ① A fourfold or greater increase in titer in paired sera ② A single titer of greater than or equal to 1:32 * Antibody titers rise 7-10 days after infection and peak at 3-4 weeks⑵ Cold agglutinin test : neither sensitive nor specific for M.pneumoniae⑶ Antigen capture-enzyme immunoassay (Ag-EIA)⑷ Direct PCR⑸ Isolation of M.pneumoniae
Mycoplasma pneumonia
Treatment of Mycoplasma Pneumonia
No rapid way to make the diagnosis of mycoplasm pneumonia. Empiric therapy for atypical pneumonia for 14-21 day course
① erythromycin : drug of choice
② tetracyclin, doxycycline : suitable alternatives
③ new drug : clarithromycin, azithromycin
Mycoplasma pneumonia
Chlamydial infection
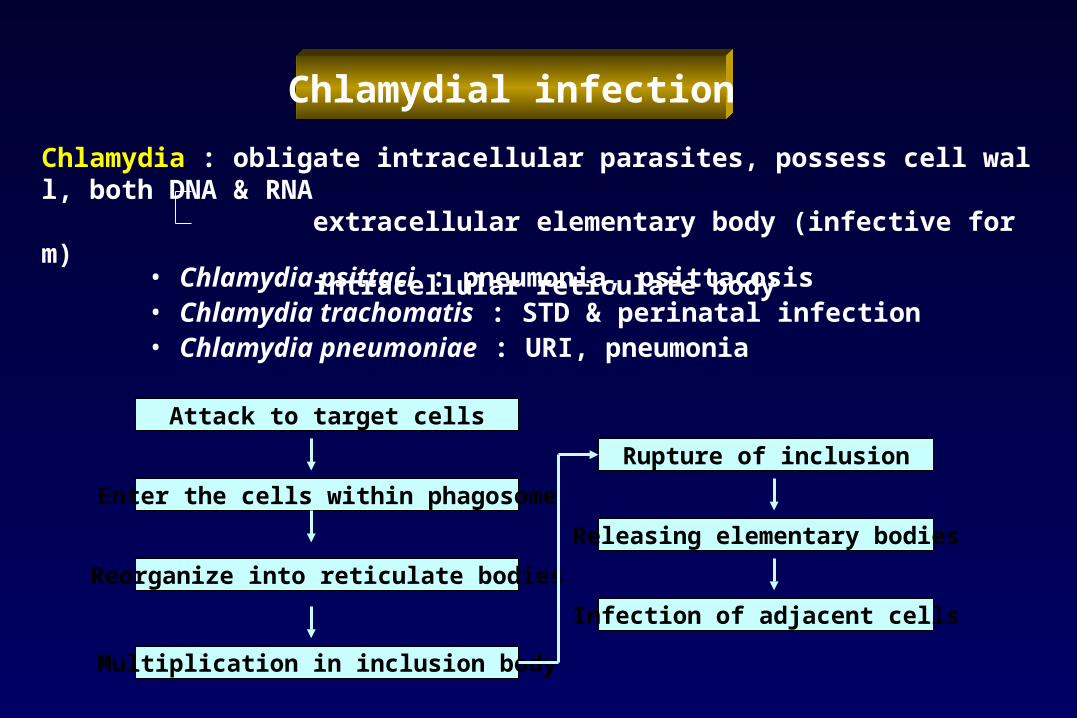
• Chlamydia psittaci : pneumonia, psittacosis• Chlamydia trachomatis : STD & perinatal infection• Chlamydia pneumoniae : URI, pneumonia
Attack to target cells
Enter the cells within phagosome
Reorganize into reticulate bodies
Multiplication in inclusion body
Rupture of inclusion
Releasing elementary bodies
Infection of adjacent cells
Chlamydia : obligate intracellular parasites, possess cell wall, both DNA & RNA extracellular elementary body (infective form) intracellular reticulate body
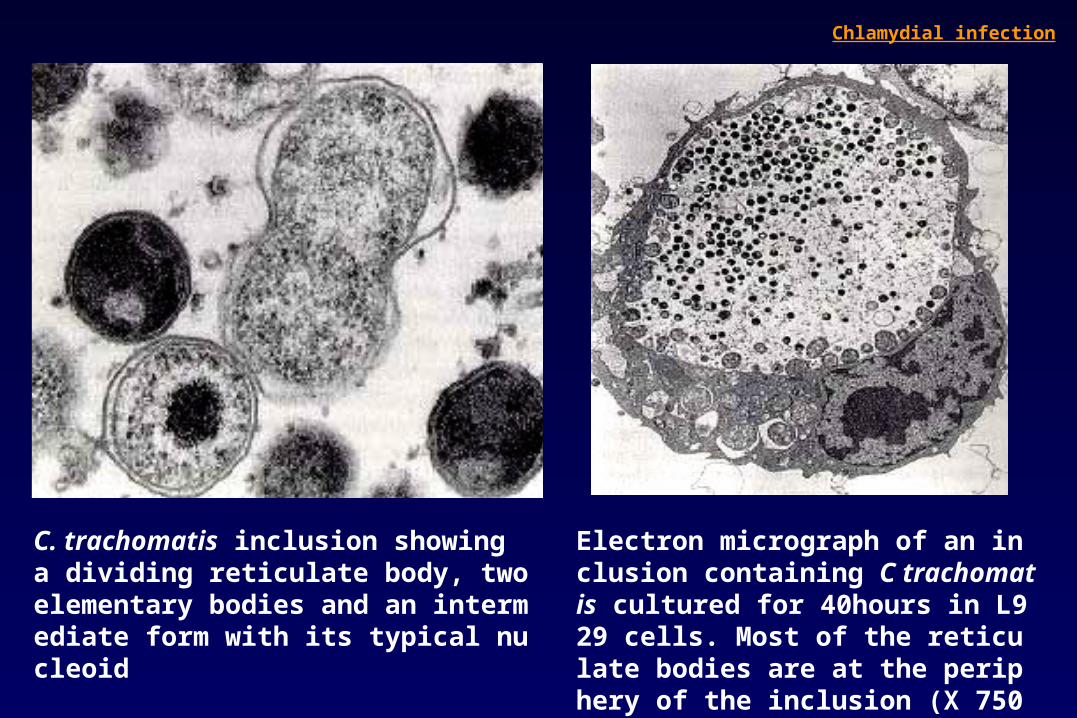
C. trachomatis inclusion showing a dividing reticulate body, two elementary bodies and an intermediate form with its typical nucleoid
Chlamydial infection
Electron micrograph of an inclusion containing C trachomatis cultured for 40hours in L929 cells. Most of the reticulate bodies are at the periphery of the inclusion (X 7500).
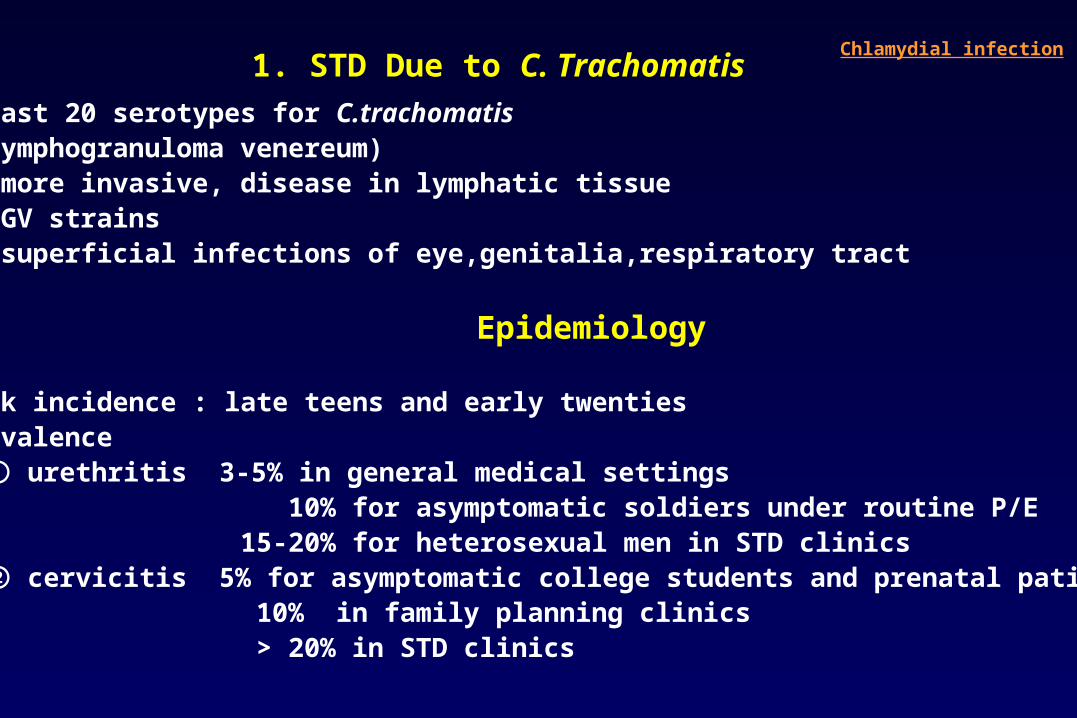
At least 20 serotypes for C.trachomatisLGV(lymphogranuloma venereum) : more invasive, disease in lymphatic tissueNon-LGV strains : superficial infections of eye,genitalia,respiratory tract
Epidemiology
• Peak incidence : late teens and early twenties• Prevalence ① urethritis 3-5% in general medical settings 10% for asymptomatic soldiers under routine P/E 15-20% for heterosexual men in STD clinics ② cervicitis 5% for asymptomatic college students and prenatal patients 10% in family planning clinics > 20% in STD clinics
1. STD Due to C. Trachomatis Chlamydial infection
Clinical Features of STD
⑴ Nongonococcal and postgonococcal urethritis
⑵ Epididymitis
⑶ Reiter’s syndrome
⑷ Proctitis
⑸ Mucopurulent cervicitis
⑹ Pelvic inflammatory disease(PID)
Chlamydial infection
ㅊ
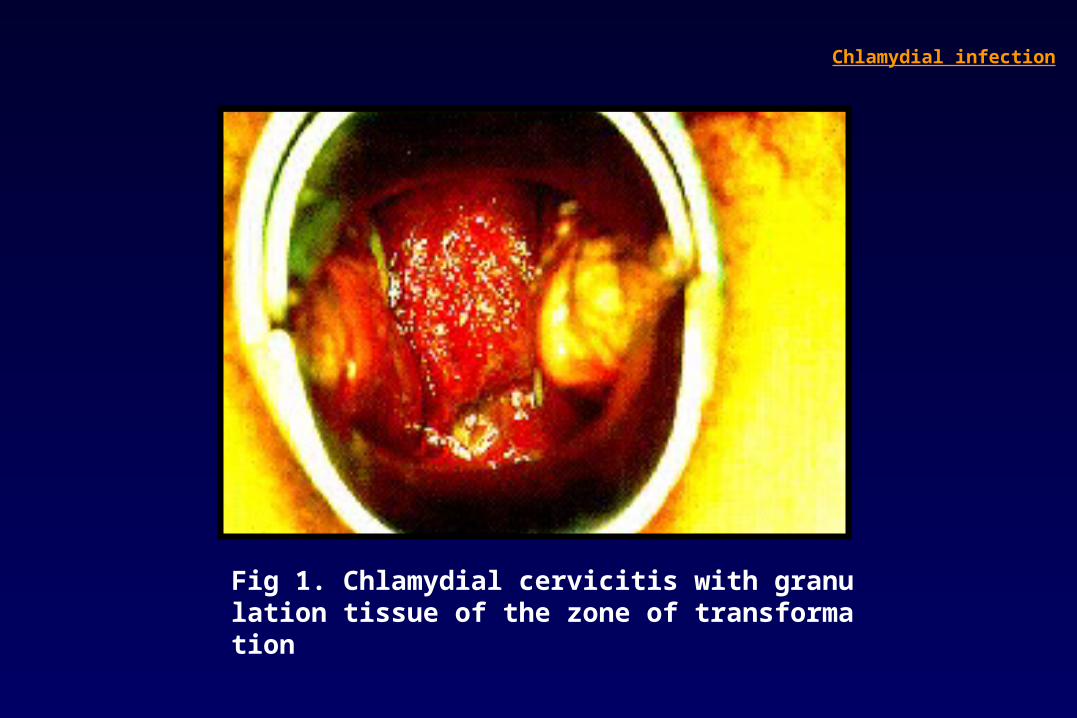
Fig 1. Chlamydial cervicitis with granulation tissue of the zone of transformation
Chlamydial infection
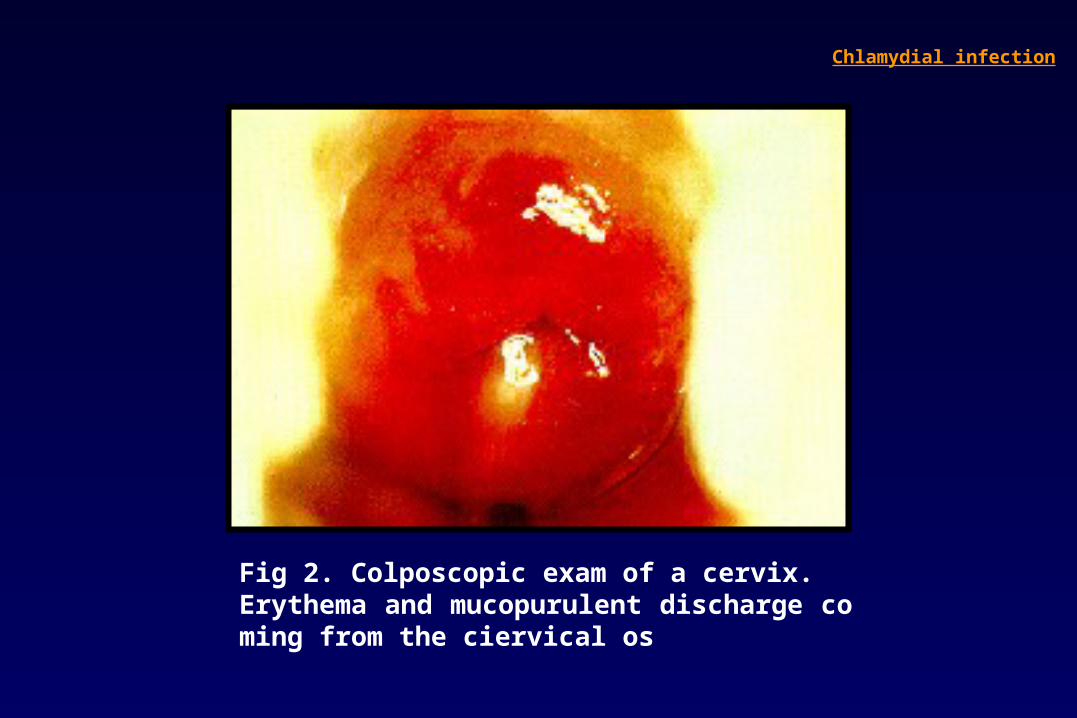
Fig 2. Colposcopic exam of a cervix.Erythema and mucopurulent discharge coming from the ciervical os
Chlamydial infection

Fig 3. Unilateral chronic follicular conjunctivitis
Chlamydial infection
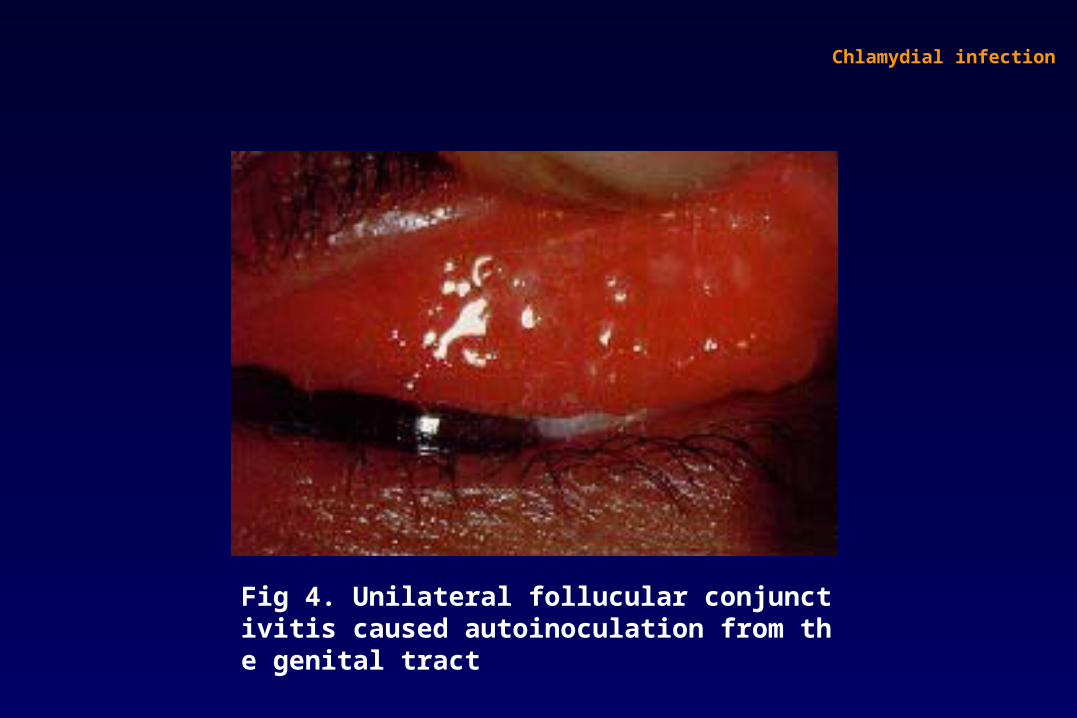
Fig 4. Unilateral follucular conjunctivitis caused autoinoculation from the genital tract
Chlamydial infection
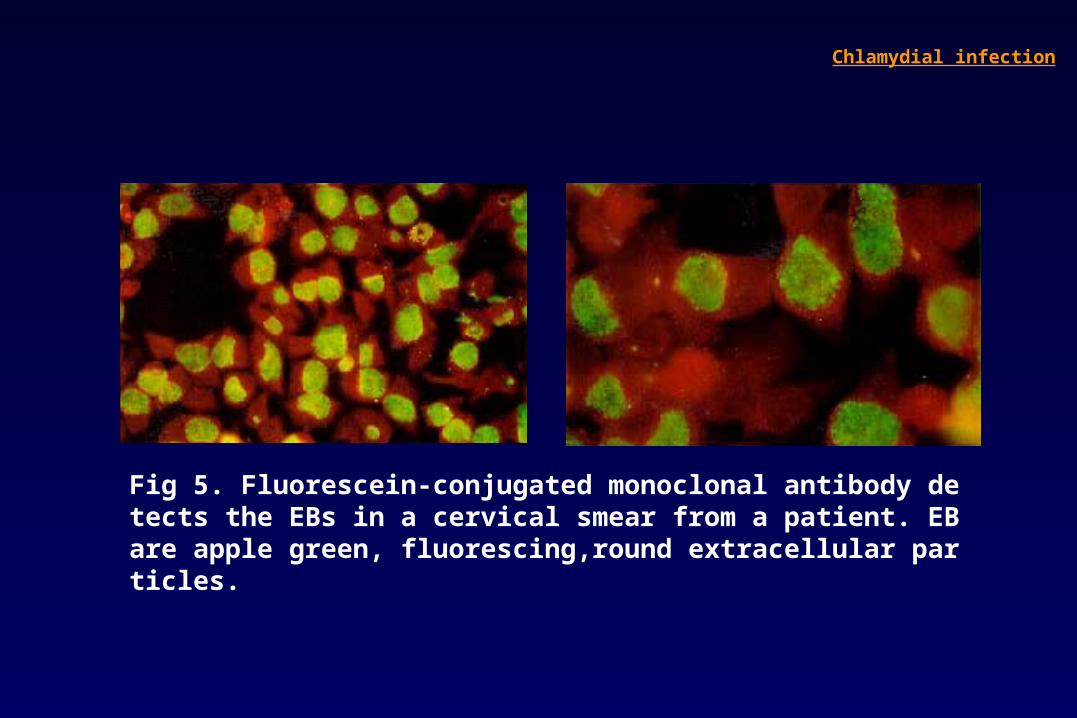
Fig 5. Fluorescein-conjugated monoclonal antibody detects the EBs in a cervical smear from a patient. EB are apple green, fluorescing,round extracellular particles.
Chlamydial infection
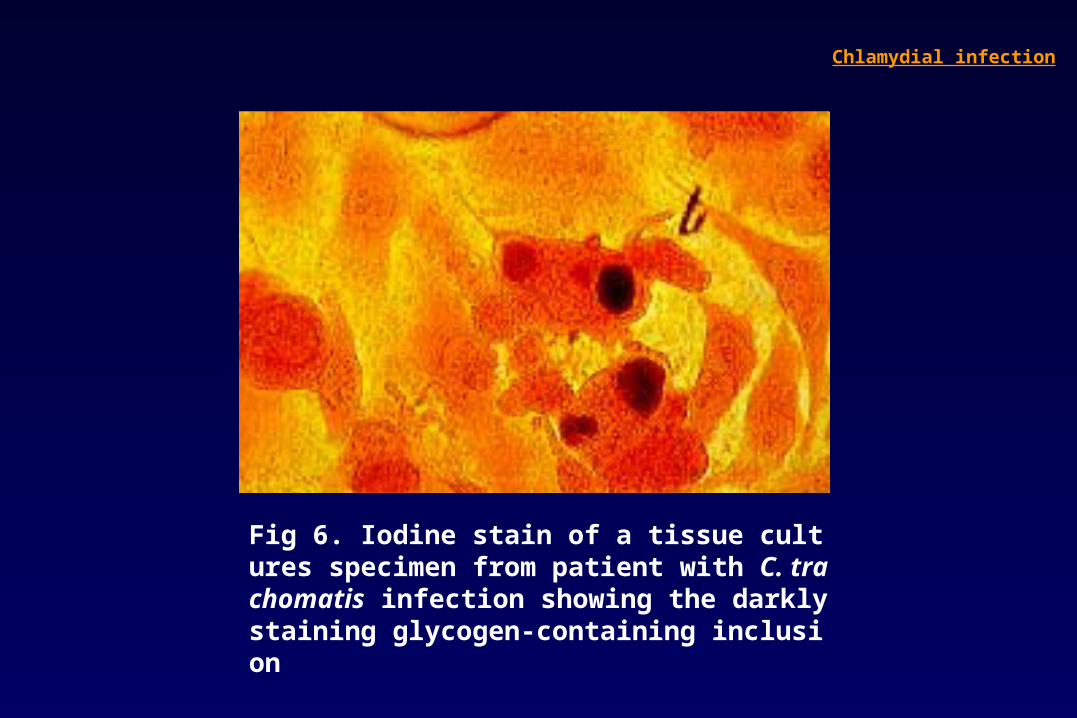
Fig 6. Iodine stain of a tissue cultures specimen from patient with C. trachomatis infection showing the darkly staining glycogen-containing inclusion
Chlamydial infection
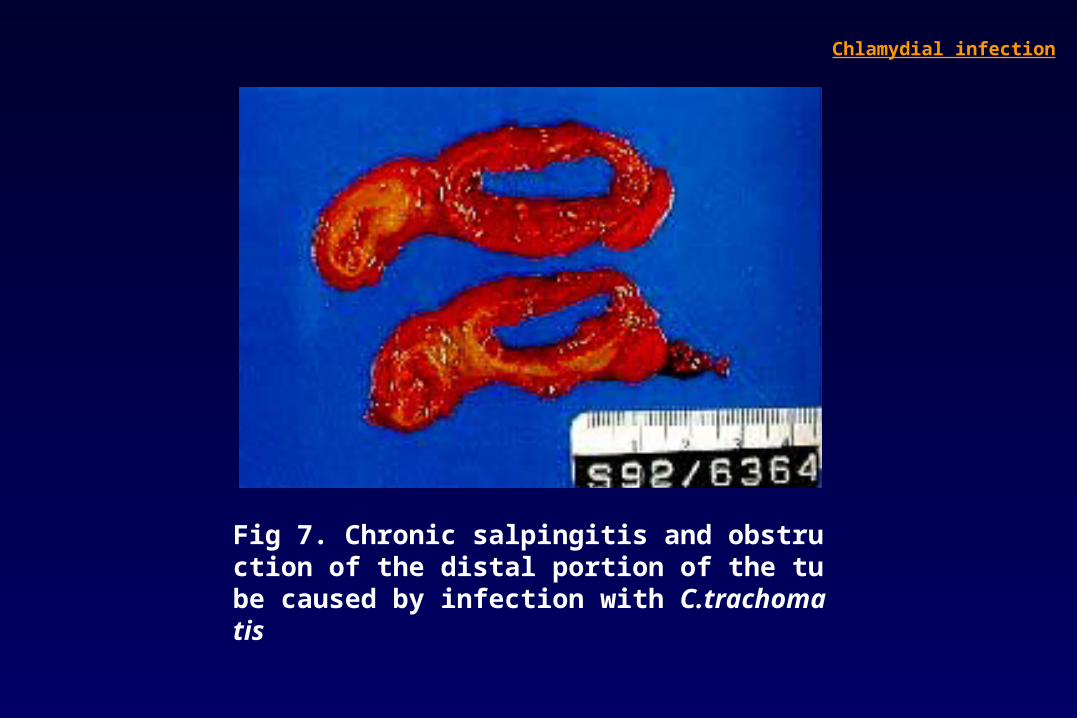
Fig 7. Chronic salpingitis and obstruction of the distal portion of the tube caused by infection with C.trachomatis
Chlamydial infection
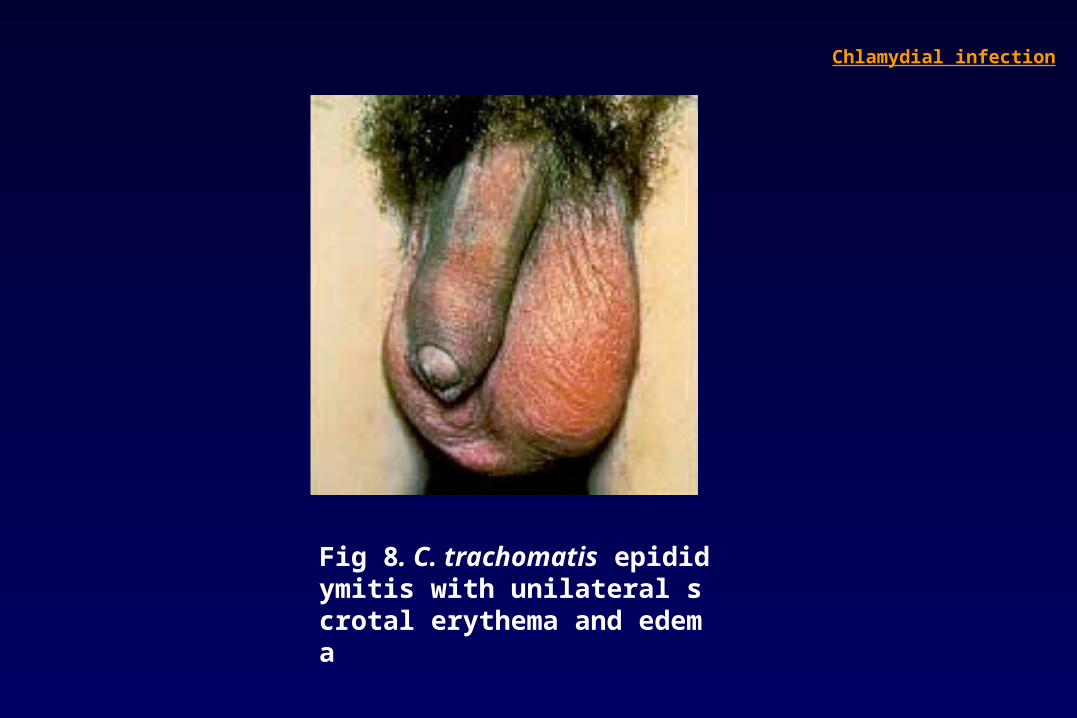
Fig 8. C. trachomatis epididymitis with unilateral scrotal erythema and edema
Chlamydial infection
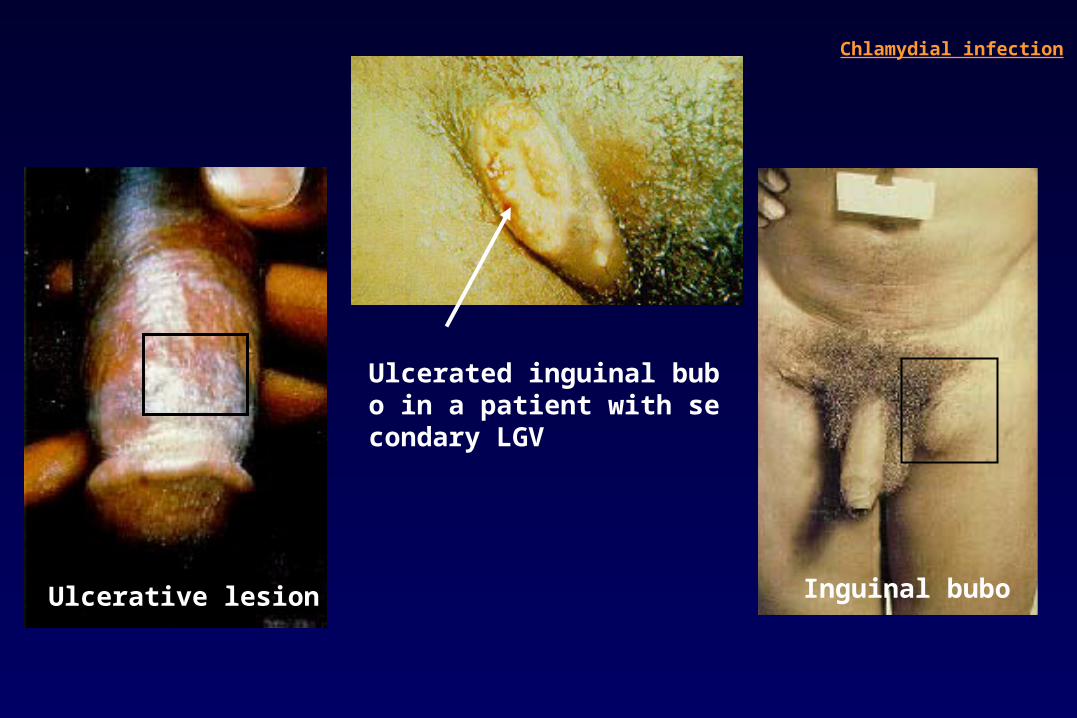
Ulcerated inguinal bubo in a patient with secondary LGV
Chlamydial infection
Ulcerative lesion Inguinal bubo
2. C. Pneumniae Infections
• C.pneumoniae : more difficult to culture than other chlamydiae • Peak incidence : young adults Secondary episode : older adults• Transmission : from person to person, primarily in schools and family units• Clinical spectrum : acute pharyngitis, sinusitis, bronchitis, pneumonitis• Clinical features ① resembles that of M.pneumoniae pneumonia (leukocytosis(-), antecedent URI symptoms, fever, nonproductive cough,minimal findings on chest auscultaton small segmental infiltrates on chest x-ray) ② severe especially in elderly patients• Diagnosis acute and convalescent-phase sera for chlamydial CF antibody ( but not distinguish C.pneumoniae from C.trachomatis or C.psittaci)• Treatment erythromycin or tetracycline 2g/day for 10-14days
Chlamydial infection
3. Psittacosis
Clinical Features incubation period : 7-14 days more gradual onset with fever, headache, nonproductive cough untreated cases -> sustained or remittent fever for 10days to 3weeks -> gradually abateDiagnosis acute and convalescent-phase sera for chlamydial CF antibodyDifferential diagnosis Mycoplasma pneumonia, C.pneumoniae pneumonia, legionellosis viral pneumonia, Q feverTreatment tetracycline 2g/day for 7-14days
Infectious disease of birds caused by C.psittaciTransmissin from birds to humans -> febrile illnessAlmost always transmitted to humans by the respiratory route (rarely bite of a pet bird) upper respiratory tract ->bloodstream -> pulmonary alveoli, RES -> lymphocytic inflammation in alveolar walls and interstitium
Chlamydial infection
Legionella Infection
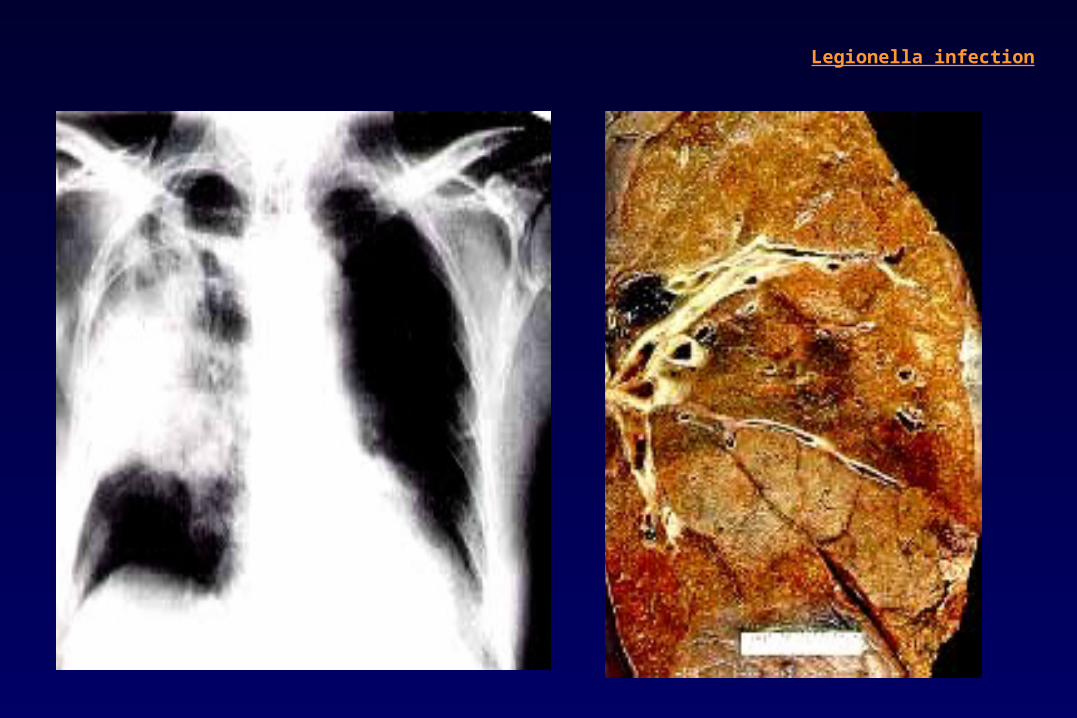
Legionellosis : two clinical syndromes by genus Legionella Pontiac fever : acute,febrile,self-limited illness by Legionella species Legionnaires’ disease : pneumonia by Legionella speciesLegionnaires’ disease 1976 outbreak of pneumonia at a hotel in Philadelphia during American Legion Convention aerobic G(-) bacterium named Legionella pneumophila in lung specimens EtiologyFamily Legionellaceae : 41 species with 63 serogroupsL.pneumophila aerobic G(-) bacilli 80-90% of human infections at least 14 serogroups (most common serogroups 1,4, 6)17 species other than L.pneumophila associated with human infections L. micdadei, L. bozemanii, L. dumoffii, L. longbeachae
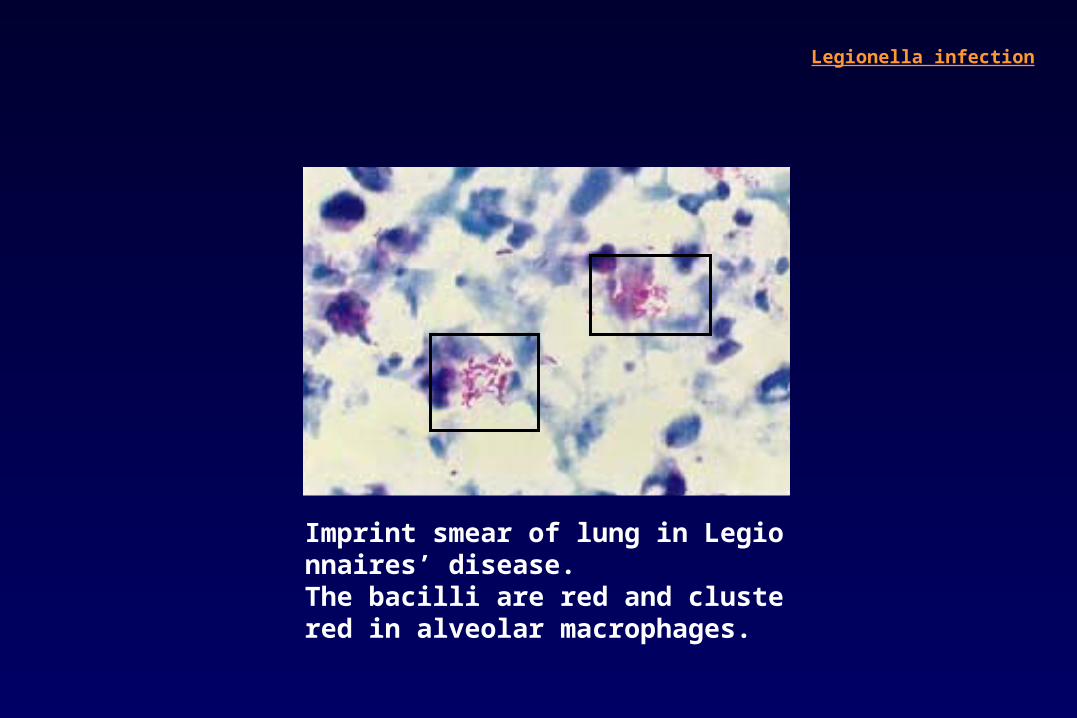
Imprint smear of lung in Legionnaires’ disease.The bacilli are red and clustered in alveolar macrophages.
Legionella infection
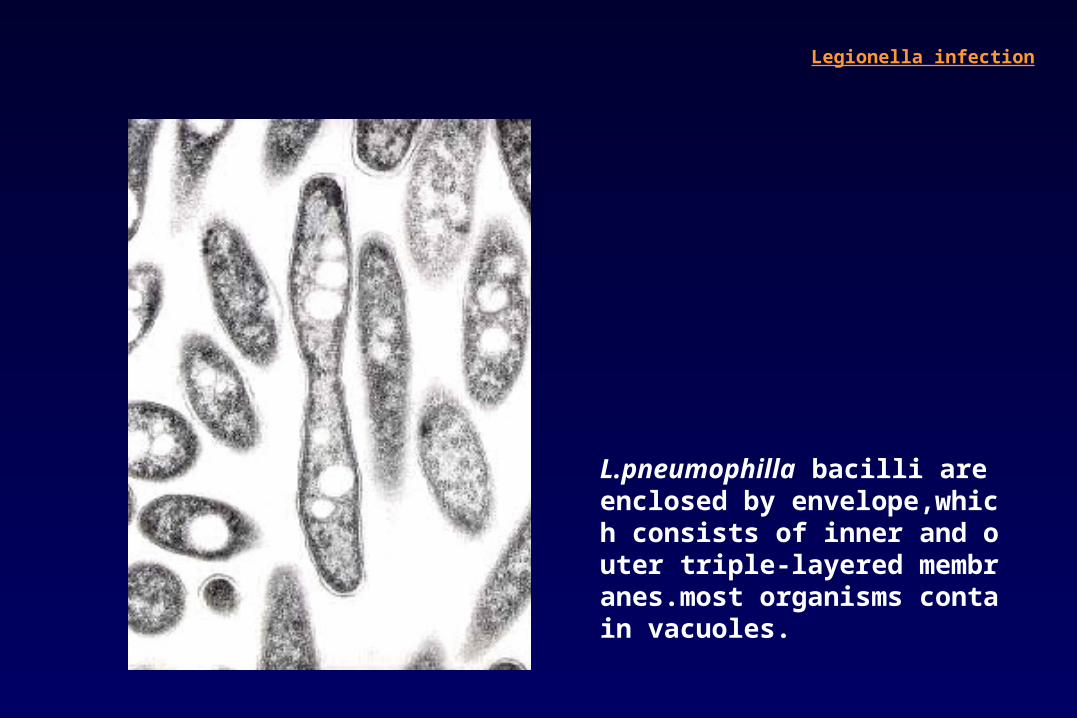
L.pneumophilla bacilli are enclosed by envelope,which consists of inner and outer triple-layered membranes.most organisms contain vacuoles.
Legionella infection
Epidemiology
Transmission natural habits for L.pneumophila : aquatic bodies(lakes, streams) enter aquatic reservoirs(cooling towers or water-distribution systems) grow and proliferate ( enhance colonization in warm temperature 25-42℃) aerolization, aspiration, direct instillation into the lung
Epidemiology3-15% of community-acquired pneumonia10-50% of nosocomial pneumonias when a hospital’s water system is colonized with the organismsMost common risk factors cigarette smoking, chronic lung disease, old age, immunosuppressionMost often develops in elderly. Surgery is a prominent predisposing factor in nosocomial infection
Legionella infection
Pathogenesis
Enter the lungs via aspiration or direct inhalationAdherence to respiratory tract epithelial cells
1. Conditions that impair mucociliary clearance smoking, lung disease, alcoholism2. Cell-mediated immunity is the primary mechanism. transplant recipients, HIV patients, patients receiving glucocorticoid hairy cell leukemia(monocyte deficiency and dysfunction)3. Role of neutrophil : minimal4. Humoral immune system IgM, IgG witin weeks ofinfection promote killing of legionellae by neutrophils,monocytes,alveolar M neither enhance lysis by complememt nor intracellular multiplication
Legionella infection
Pontiac Fever
Acute, self-limiting, flulike illness with a 24-48h incubation period
Pneumonia does not develop.
Fever, headache, malaise, fatigue, myalgias : the most frequent symptoms
Complete recovery within only a few days without antibiotic therapy
Diagnosis by antibody seroconversion
Legionella infection
Legionnaires’ disease(pneumonia)
Clinical Clues suggestive of Legionnaires’ Disease
DiarrheaHigh fever ( > 40℃ )Numerous neutrophils but no organisms revealed by Gram’s staining of respiratory secretionsHyponatremia (serum sodium level of < 131 meq/L)Failure to respond to -lactam drugs and aminoglycoside antibioticsOccurrence of illness in an environment in which the potable water supply is known by be contaminated with LegionellaOnset of symptoms within 10 days after discharge from the hospital
Legionella infection
Legionella infection
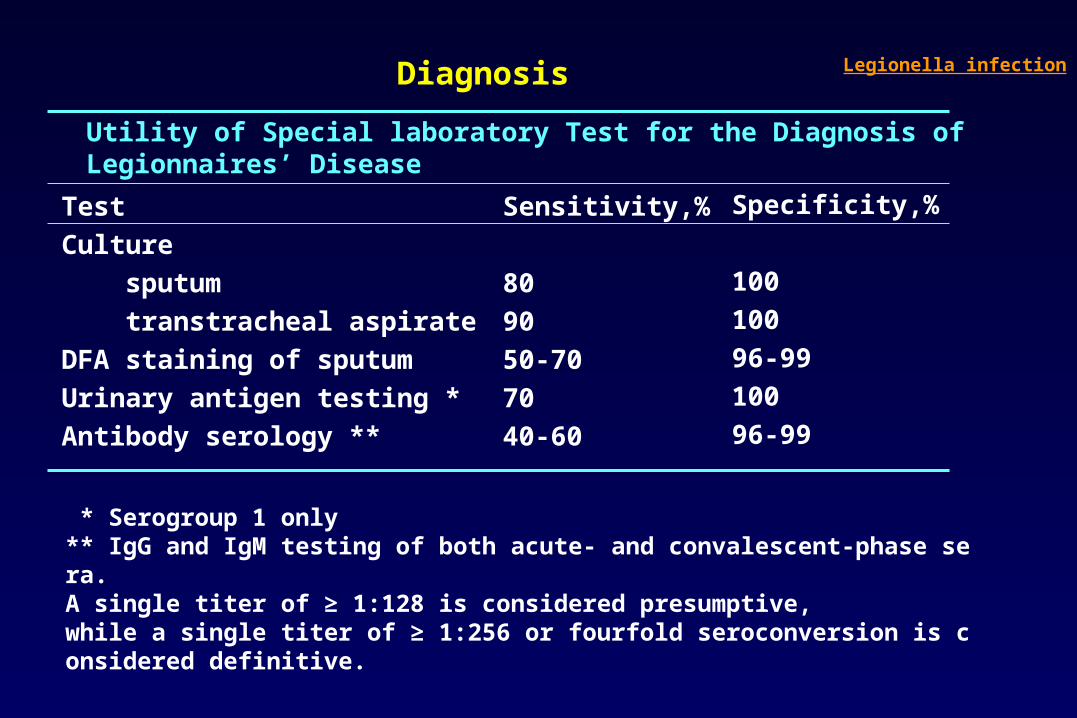
Utility of Special laboratory Test for the Diagnosis ofLegionnaires’ Disease
TestCulture sputum transtracheal aspirateDFA staining of sputumUrinary antigen testing *Antibody serology **
Sensitivity,%
809050-707040-60
Specificity,%
10010096-9910096-99
* Serogroup 1 only** IgG and IgM testing of both acute- and convalescent-phase sera.A single titer of ≥ 1:128 is considered presumptive,while a single titer of ≥ 1:256 or fourfold seroconversion is considered definitive.
Diagnosis Legionella infection
Extrapulmonary Legionellosis
Usually result from bloodborne dissemination from the lungSinusitis, peritonitis, pyelonephritis, cellulitis, pancreatitis : predominantly in immunosuppressed patientsThe most common extrapulmonary site Heart : myocarditis, pericarditis, postcardiotomy syndrome, prosthetic-valve endocarditis Most cases hospital-acquired
Legionella infection

Direct immunofluorescence of L. pneumophila of lung. Numerous bacilli in alveolar macrophages
Legionella infection
Treatment
Antibiotics for 10-14 days * longer period(3 weeks) for immunosuppressed① Erythromycin② New macrolides(azithromycin, clarithromycin, roxithromycin, josamycin)③ Ciprofloxacin : transplanted patient④ Rifampin + macrolides or quinolone
Pontiac fever requires only symptom-based treatment, not antibiotics Prevention
Disinfection of the water supply is the ultimate preventive measure.① Superheat and flush method heating of the water( 70-80℃ ) flushing with hot water for at least 30 min.② copper and silver ionization method③ hyperchlorination is no longer recommended
Legionella infection





![l & E x perimenta l i n ic lp Journal of Clinical ... · the so-called atypical pneumonia, which is a type of pneumonia with an overall prevalence of 22.7% [1]. It is also a causative](https://img.pdfslide.net/doc/110x75/6082e1604c6d78134f366804/l-e-x-perimenta-l-i-n-ic-lp-journal-of-clinical-the-so-called-atypical.jpg)