Embed Size (px)
Citation preview

Thorax (1949), 4, 152.
THE RADIOLOGY OF PRIMARY ATYPICAL PNEUMONIABY
P. W. VERCG*From the Institute of Medical and Veterinary Science, Adelaide, and the Department of Experimental Medicine,
University of Adelaide
The pulmonary changes accompanying " primaryatypical pneumonia, aetiology unknown" havebeen of considerable interest to radiologists andphysicians over the past decade. Characteristicvarieties of pulmonary change occurring in thisillness have been the subject of many reports in theliterature, although few studies have been accom-panied by an adequate aetiological investigation.
This condition may be indistinguishable clinicallyfrom many other diseases which occur in bothepidemic and endemic form. Notable among theseare infections with influenza virus A or B (Ziegler,Curnen, and Mirick, 1947), infection with thepsittacosis group of viruses (Treuting and Olson,1944), " Q " fever (Feinstein, Yesner, and Marks,1946), infectious mononucleosis (Wechsler, Rosen-blum, and Sills, 1946) and coccidioidomycosis(Rakofsky and Knickerbocker, 1946). Differentia-tion is made, possibly by isolation of the causativeagent, or by demonstration of a rise of titre in theconvalescent serum of antibody or certain otherproperties of the serum, or by the use of intra-cutaneous sensitivity tests.The investigations of the Commission on Acute
Respiratory Diseases (1944), of Eaton, Meiklejohn,and van Herick (1945), and of the United StatesNavy Research Unit at the Rockefeller InstituteHospital in New York (Curnen and others, 1945)have confirmed, by the correlation of clinical,radiological, and aetiological investigations, thefindings of many previous observers. In thetransmission to human volunteers of the naturallyoccurring illness by inoculation of filtered throatwashings and sputum, the Commission (1946) hasestablished a virus or viruses as the causative agent,and has provided a basis on which the radiologicalstudy of the disease may be founded.
In these reports, the early radiological manifesta-tions in most cases of the naturally occurring diseasewere stated to be an increase in size of one or bothhilar shadows, increasing perihilar infiltration, andextension of the shadow toward the periphery in theshape of a fan. Less commonly the early lesion
* This work was aided by a grant from the National Health andMedical Research Council of Australia.
appeared to lie peripherally in the lung and extensiontook place towards the hilum.However, in the illness transmitted experimen-
tally, pulmonary change became apparent from thesecond to the fifth day after onset, and the earliestsign was a local increase in the density of the lungmarkings without concomitant hilar involvement.This was most commonly seen at the lung bases,best visualized by anterior-oblique films, and theinfiltration appeared either linear as an exaggerationof the basilar truncal markings, or as patches ofsoft irregular density. Frequently the latter werelocated in the most peripheral and dependentportions of the lung, the costo-phrenic sulci, andconnexion with the normal hilar shadow did notappear to be continuous. In the remaining patientsperihilar infiltration with or without parenchymalinvolvement was the earliest manifestation.
Subsequently, in both the naturally occurring andthe experimentally transmitted disease, in somecases the infiltration remained limited to the peri-pheral portions of one or both lower lobes, and thehilar regions were not abnormal at any time, or theearly peribronchial infiltration appeared to spreadcentrally toward the hilum with concomitant radialspread within the lower lobe; in others the perihilarinfiltration became increasingly apparent, and spreadoccurred in the peripheral portion of one or morelobes in a fan shape, with the greatest density at thehilum.
Extraordinary variation in the density of theinfiltration was noted, although usually it appearedsoft and either granular or homogeneous. The lungmarkings were usually visible through the opacity,although their outlines were frequently indistinct.The borders of the areas of infiltration were com-monly ill-defined and irregular, fading into normallung tissue. The infiltration was rarely of sufficientdensity to resemble that of pneumococcal pneu-monia. Distinct but delicate " pencilling " at thesite of the interlobar fissures frequently suggestedpleural involvement. Radiological features suggest-ing an abnormal accumulation of pleural fluid wereuncommon, and " plate-like " atelectasis wasobserved on occasions during convalescence. In
group.bmj.com on August 15, 2017 - Published by http://thorax.bmj.com/Downloaded from

THE RADIOLOGY OF PRIMARY ATYPICAL PNEUMONIA
most patients, the process appeared to be confinedto a local area, most frequently to one of the lowerlobes, and in particular to one of the cardiophrenicangles. Spread of the lesion often occurred withina lobe or in an adjoining lobe, and multiple lobeinvolvement was frequent. In some cases the lesionwas confined to the hilar region.
Occasionally, the lesions lasted only a few days,but usually they progressed, and then underwentslow resolution over a period of one to three weeks.Resolution was observed to occur in several ways.In most instances it proceeded from the peripheryof the lung toward the hilum, but occasionally inthe reverse direction. Also progressive reduction inthe size and diminution in density of the affectedarea was observed until no further evidence ofconsolidation remained. In many instances, duringthe process of resolution, the affected area assumeda diffusely mottled appearance. Frequently, afterall the pulmonary involvement was thought to havedisappeared the broncho-vascular markings remainedprominent. The enlarged hilar shadows oftenpersisted for several weeks.When the infiltration was mottled it occasionally
presented the appearance of small abscess cavities.Infiltrations radiating from the hilum with involve-ment of the upper lobe resembled tuberculosis,whereas other lesions, especially in the lower lobes,simulated bronchiectasis. In several cases of experi-mentally transmitted illness, the pulmonary opacitieswere small, discrete, and nodular in the early stage,later enlarging in size and becoming patchy andconfluent. This type of infiltration might resemblemiliary tuberculosis.
These observers have emphasized that other formsof pneumonia could not be distinguished fromprimary atypical pneumonia on the basis of radio-graphic evidence alone, and that a diagnosis ofprimary atypical pneumonia was not justified unlessmade in conjunction with clinical and laboratoryfindings.Of particular interest is that form of primary
atypical pneumonia in which the pulmonaryopacities resemble miliary tuberculosis. Scadding(1937) described four cases of " disseminated focalpneumonia " and was impressed by the resemblanceof the infiltration to tuberculosis. Radiologicalmanifestations consisted of " areas of diffuse rathercoarse mottling, in foci varying from about 2 to5 mm. in diameter " present in more than one lobein three patients, and resolution was slow in all butone. Scadding cited descriptions of appearancesattributed to bronchopneumonia in " miliary " fociby radiologists in American and German literature;the chief point of discussion in these reports was
the radiological diagnosis distinguishing them frompulmonary tuberculosis. Several of these reports,where the clinical features were presented in sufficientdetail, described in common with his own series asimilar radiological picture, namely a gradual onsetwith predominantly constitutional symptoms, and aprolonged course with eventual complete resolution.Reiman (1938) reported a series of eight cases,which presented a radiological picture and coursestrikingly similar to those of two of Scadding'spatients. All the patients were adults, and a mildinfection of the upper respiratory tract was followedby severe diffuse atypical pneumonia, and in twopatients by encephalitis.
Patients presenting similar radiological features,with severe and prolonged illness, were reported byKneeland and Smetana in 1940. Such cases havesince occurred, usually as a minority in epidemics ofprimary atypical pneumonia. McCarthy (1943)noted that these patients were extremely ill. Lewisand Lusk (1944) reported such cases as a " broncho-alveolar phase," and suggested that the radiographicmanifestations could be explained pathologically bysmall areas of atelectasis and alveolar exudationintermingled with emphysematous areas. Showacre,Wightman, and Moore (1944) recorded theirexperience with probable primary atypical pneu-monia over a decade, and emphasized that theradiographic pattern varied from one season toanother and at times during the same season.
Eaton, Meiklejohn, and van Herick (1942, 1945)reported the isolation of a new virus from cases ofprimary atypical pneumonia; they apparentlytransmitted an infectious agent to cotton rats froma fatal case of a very diffuse " miliary " pneumonia.Jamison (1945) recorded further cases of primaryatypical pneumonia; in two patients the infiltrationwas of a finely nodular or patchy type, scattereduniformly in both lungs. Loffler and Moeschlin(1946) reported a further series of seven such cases,four of which were fatal. In the sera of threepatients ofthe four tested, cold agglutinins developed.Most descriptions of this form of primary
atypical pneumonia, with the exception of that ofScadding (1937), suggest that resolution is early andcomplete. In his patients, resolution tended to beslow and irregularly delayed, and in one was notcomplete for at least 12 weeks from the onset.
PATHOLOGYGolden (1944) has reviewed the pathological
anatomy of necropsy material from cases consideredto be examples of primary atypical pneumonia. Hefound that the pulmonary lesions which all patientshad in common could be summarized as follows.
153
group.bmj.com on August 15, 2017 - Published by http://thorax.bmj.com/Downloaded from

P. W. VERCO
1. There was acute bronchiolitis, focally distri-buted, in which desquamation of the mucosalsurfaces occurred early.
2. The lumens of such bronchioles containedfrank pus, mucoid fluid, and desquamated epithelialclusters or single cells, sometimes in an advancedstage of disintegration.
3. Bacteria in small numbers, and not of uniformtype, could be demonstrated in the bronchiolar pusin some cases; in most instances none could befound.
4. The bronchioles were dilated, sometimesgreatly, even in patients who had died early in thedisease.
5. The walls of such bronchioles were infiltratedchiefly with mononuclear cells, which extendedradially into the regional interstitial tissues of thelung around the bronchioles, in the alveolar walls,and in the pulmonary septums.
6. The alveoli either contained air or werecollapsed, and differed from those involved inbronchopneumonia and lobar pneumonia in beingrelatively free of polymorphonuclear leucocyticexudate.
7. Such areas failed to reveal microorganismson tissue section.
8. With the advent of secondary bacterialinvasion the gross and microscopic pictures werealtered: in some patients there were areas of acuteinterstitial pneumonia adjacent to zones of typicalbronchopneumonia or pulmonary abscess. In fact,unless there was such a partition of the lesions, itwas impossible to state from the pathologicalexamination that there were really two co-existingtypes of lesion in a given case.
Meiklejohn (1947) has suggested that Golden'saccount of the pathological features of primaryatypical pneumonia be accepted with caution, as theaetiological investigations in some cases wereinsufficient.
Parker, Jolliffe, and Finland (1947) reported thenecropsy findings in eight patients, all of whom hadillness characteristic of the severe and extensive typeof primary atypical pneumonia. In every caseradiography showed a soft miliary type of densitywhich eventually spread to involve most of the lungfields. Two of these patients, in one of whom a
significant complement fixation titre for psittacosiswas found, had a diffuse, bullous type of erythemamultiforme. Attempts to isolate a virus from fivepatients were not successful. The duration of theillness varied from 13 to 31 days. Histologically,the characteristic changes in the lungs were a
mononuclear type of alveolar exudate with swelling
and proliferation of the alveolar lining cells. Inter-stitial infiltration, for the most part by plasma cells,was constant and conspicuous in the walls of thebronchioles and around the blood vessels, andfrequently extended into the walls of the alveoli.Oedema of the septums was prominent, thrombi inthe smaller arteries and veins were frequent, andhyaline membranes were found in the alveoli inapproximately half the patients. In contrast to theobservations of Golden, the bronchioles, with rareexceptions, showed no evidence of injury andcontained no exudate in areas free from secondarybacterial infection. Where there was secondarybacterial infection, the lumens of the bronchiolescontained many polymorphonuclear leucocytes,cocci, and often some mucus. Secondary bacterialinvasion seemed to be the rule. In some, but notall such cases, the alveoli contained polymor-phonuclear leucocytes and sometimes fibrin. Organi-zation of the alveolar and bronchiolar exudates wasfound in most patients but was not extensive.
Parker and others (1947) agree with Golden thatthe pulmonary lesions, whilst resembling thosefound in psittacosis, are not identical. In psitta-cosis the alveolar exudate contains considerablymore fibrin and red blood cells, and interstitialinfiltration is not so conspicuous a feature as inprimary atypical pneumonia.Golden considered that descriptions of essentially
the same lesions that occur in primary atypicalpneumonia are to be found among reports ofinfluenzal pneumonia during the 1918-19 pandemic,particularly when death occurred within the firstfive days of illness. When the clinical duration ofthe illness was greater than five to seven days in thepandemic, secondary infection was the rule. Parker,Jolliffe, and Finland (1947) found in influenza thatsecondary staphylococcal invasion caused- a severedisease, fatal either in a few days or after two weeksor more. In the rapidly fatal cases the mostprominent features were oedema and haemorrhage;extensive necrotizing tracheobronchitis and multiplepulmonary abscesses were also seen. In cases oflonger duration the lungs showed extensive fibrosisand cavity formation. No lesions of such extentoccurred in their examples of primary atypicalpneumonia.
Measles may cause a similar acute interstitialpneumonia (Milles, 1945). McCordock and Mucken-fuss (1933) have called attention to the tendency ofviral pulmonary infections, particularly influenzaand measles, to produce this type of pulmonarylesion. Other virus diseases may present compar-able pulmonary lesions, e.g., chickenpox (Waringand others, 1942; Claudy, 1947), infectious mono-
154
group.bmj.com on August 15, 2017 - Published by http://thorax.bmj.com/Downloaded from

THE RADIOLOGY OF PRIMARY ATYPICAL PNEUMONIA
nucleosis (Allen and Kellner, 1947), lymphocyticchorio-meningitis (Smadel and others, 1942), andthe primary virus pneumonia with cytoplasmicinclusion bodies reported by Adams (1941). Per-tussis, a bacterial infection, is capable of producingan acute interstitial pneumonia, in which Haemo-philus pertussis can be demonstrated in the sections.Diverse chemical and physical agents may producesimilar lesions; for instance, the irritant war gases(Winternitz and others, 1920), x-radiation (McIntoshand Spitz, 1939), and hot and irritating vapour(Finland and others, 1946).
It is generally agreed that secondary infection bypathogenic bacteria may obscure the histologicalpicture of pneumonia of virus origin at necropsy.Large doses of sulphonamides or penicillin arelikely to have been given in fatal cases, and maywell affect the important lesions due to secondaryinfection.
MATERIALIn the course of an investigation into primary
atypical pneumonia, aetiology unknown, conductedover a period of 14 months at the Royal AdelaideHospital, 34 cases closely resembling this conditionwere admitted to the hospital. Investigations wereofa satisfactory standard in only 14 of these patients,and the clinical and laboratory features of thesehave been reported in detail elsewhere (Verco,1949). Of these 14 patients, 10 were female and 4were male: their ages varied from 16 to 53 years.Most of them became ill during the period August,1946, to January, 1947, when there was a smallepidemic of similar cases in Adelaide. The patients,with the exception of cases 103 and 128, who livedin the same hostel and came from the same districtas cases 102, 105, 109, and 120, were from widelyseparated areas, and all had been exposed to severalpossible sources of infection. No instance ofprimary atypical pneumonia occurred among thestaff directly responsible for the care of thesepatients.These cases presented remarkably similar clinical
pictures. In several cases the illness began withmild upper respiratory symptoms, but in most theonset was insidious, with constitutional symptomsincreasing in severity, to be followed shortly by anirritating cough, at first unproductive. Headache,often frontal, and irritating cough, at timesparoxysmal, were conspicuous. Severe pleural paindid not occur. Many patients were severely ill, butthe severity of the illness was suggested rather by thefever, the rapid pulse, and frequent respiration thanby the general appearance and mental clarity. Asthe illness progressed, particularly when severe, theleucocyte count tended to rise, due mainly to an
increase in the polymorphonuclear leucocytes.Subsidence of fever by lysis, and slowing of pulseand respiration were usually preceded by a noticeableimprovement in the patient's condition. The illnesswas little influenced by the administration ofsulphonamides and penicillin. It was not possibleto predict accurately either the duration or theseverity of the illness in any given case. All patientsbegan to show clinical improvement, and resolutionof pulmonary opacities began within a month of theonset. Convalescence was often protracted withasthenia and a mild cough.Two patients died; case 108 from extensive
involvement of both lungs by the pneumonia,case 120 from an extensive haemorrhagic leucoen-cephalitis and pneumonia (Fowler and French, 1949).In both patients, the pulmonary lesions had manyfeatures in common with the pathological anatomydescribed by Golden (1944).Case 105 presented, in addition to pulmonary
involvement, an acute haemolytic anaemia withleukaemoid features of the myeloid cells, meningealsymptoms, and an increased cellular content of thecerebrospinal fluid.
Sputa of nine patients were examined. Smearsand cultures revealed the usual pharyngeal organ-isms, including both pneumococci and Gram-negative bacilli in cases 107 and 108, haemolyticstreptococci in cases 110 and 124, and a coagulase-positive haemolytic staphylococcus in case 109.In case 120, the lungs were bacteriologically sterileat necropsy ; no bacteriological studies weremade post-mortem in case 108. The sputum wasnot examined in cases 103 and 105. In cases 102and 104 the cough did not become productive untilconvalescence was established.
Sera were obtained from all patients except case120. Ten patients developed cold agglutinins to atitre of 1: 32 or greater. Sera from 12 patientswere titrated for " T " agglutinins (Lind andMcArthur, 1947), and eight showed titres of 1: 600or greater. In no case was the psittacosis comple-ment fixation titre considered indicative of infectionwith the psittacosis group of viruses, nor didagglutination against Rickettsia burneti develop.Paired acute and convalescent phase sera fromcases 105, 106, 110, and 124, and from 16 othercases of acute pulmonary infection admitted to thehospital during the period of this study, weretitrated for content of antibody against influenzaviruses A and B. No evidence suggesting infectionwith the influenza viruses was obtained.
Intracutaneous tests with histoplasmin and cocci-dioidin (extracts of Histoplasma capsulatum andCoccidioides immitis) were performed in all except
155
group.bmj.com on August 15, 2017 - Published by http://thorax.bmj.com/Downloaded from

P. W. VERCO
the two fatal cases, and were negative. The Mantouxreaction was negative in six and positive in fourpatients. The other two patients presented a changeof Mantoux reaction from negative to positive. Incase 124 this occurred at least four and a halfmonths after the onset of the pneumonia, andindicated recent primary infection. In patient 121the Mantoux test was negative in convalescence, butpositive five months later; this was attributed eitherto recent infection, or to recovery from a period ofanergy occasioned by a severe illness.
Follow-up examination of all patients yielded noevidence of active pulmonary or other forms oftuberculosis.
RADIOLOGICAL FEATURESThe illness was, with few exceptions, well estab-
lished by the time patients were admitted to hospital,and the opportunity to detect early pulmonarylesions did not arise. The severe course of theillness and rapid respirations frequently resulted ininferior films, which had to be taken with aportable apparatus. The character of the estab-lished pulmonary lesions divided the 14 patientsinto two groups.
Group L-In the first group of six patients (Nos.101, 102, 103, 106, 109, and 124), the opacitiestended to be compact and localized, as described inthe majority of cases ofprimary atypical pneumonia.In serial films the appearance of the opacitiesdiffered in no way from those described previouslyin density, form, or distribution. The density variedfrom the degree associated with lobar pneumoniato a haze through which lung markings couldbe clearly seen. In form, variations from appar-ent lobar involvement to smaller, dense, fluffyopacities suggesting lobular pneumonia, or coarseshort streaks of moderate density forming a networkand scattered nodules 2-5 mm. in diameter mostdense at the centre, were seen. Accentuation of thenormal lung markings and unduly prominent vas-cular markings were often present. The lesionswere most frequently situated in the lower lobes.Frequently several forms of opacity were diffuselydistributed in the same film.
In addition to the pulmonary opacities, enlarge-ment of one hilar shadow, confirmed by return tonormal in subsequent films, was present in threepatients. In patients 101 and 124, there wereopacities in the lower part of the left lung, and theleft diaphragm was elevated. In patient 109, denseopacity of the lower half of the right lung, and alittle infiltration at the base of the left lung in thepostero-anterior (P.A.) film, were associated withelevation of the right diaphragm and shift of the
heart to the right. A lateral film showed involve-ment of the middle lobe, of a large segment at theapex of the lower lobe, and there was scatteredinfiltration in the remainder of the lower lobe andin the lower portion of the upper lobe of the rightlung.
In patients 102 and 103 the lower portions of bothlungs were affected, more on the right, and accom-panied by elevation ofa portion of the left diaphragmin patient 102. In patient 106 there was infiltrationof the posterior part of the left upper lobe, andcollapse of the lingula.
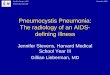
Resolution was rapid after subsidence of the acuteillness, usually within a month of onset. Theopacities diminished in density and extent, to bereplaced by small nodules and a network of coarsestriae, with prominent vascular markings. Thisappearance was very similar to that of certain formsof pulmonary tuberculosis, and may be mimickedby other forms of pneumonia in resolution. Inpatient 101, atelectatic plates were also present atthis stage. The clearing of the infiltration, parti-cularly if it had been fairly dense above an elevatedhemi-diaphragm, as in patient 101, now unexpectedlydisclosed tenting ofthe diaphragm (Figs. 1, 2, and 3).This was usually situated about the middle part ofthe diaphragm, and was present in patients 102,103, and 106 also. In patient 101, in addition tothe tenting of the left diaphragm in this region, thefirst lateral view taken five months after onset
FIG. 1-.Case. 101, P.A. view, August 24, 1945. Leftdiaphragm normal.
156
group.bmj.com on August 15, 2017 - Published by http://thorax.bmj.com/Downloaded from

THE RADIOLOGY OF PRIMARY ATYPICAL PNEUMONIA
left diaphragm.
showed considerable thickening of the pleura
against the lower part of the anterior chest wall.
In the P.A. films this had been obscured by the
cardiac shadow. Seventeen months after onset it
FIG. 3.-Case 101, P.A. view, March 10, 1948, 499 daysafter onset. Diaphragmatic adhesions less apparent.
L
had diminished considerably in extent and thetenting of the left diaphragm was less noticeable.In some of these patients, but not all, there wasevidence of previous tuberculous infection; theMantoux test was positive in patient 103, and inpatient 102 there were a few small pulmonary fociof doubtful calcification, with a negative 1: 1,000Mantoux test.As resolution progressed further, the reticulation
and nodules faded slowly, leaving accentuated lungand vascular markings in the affected areas, whichgradually returned to normal on subsequentexamination. In patient 109, considerable resolu-tion had occurred within 60 days of onset, but anarea of scattered opacities persisted in the rightmiddle lobe, associated with a cough productive ofa small amount of mucoid sputum. This area ofopacity, visible in both P.A. and lateral films, slowlyfaded unt 1 it had completely resolved 20 monthsafter onset.
Group II.-The second group comprised theremaining eight patients, 104, 105, 107, 108, 120,121, and 128. The course of the illness was generallymore severe than in the first group, although it rana moderate course in patients 104 and 105; twopatients, 108 and 120, died. The quality of thefilms obtained in this group frequently reflected theseverity of the illness, but the pulmonary lesionspresented remarkable similarities in appearance andbehaviour.The opacities seen in this group resembled those
described in similar cases by others. Drew, Samuel,and Ball (1943), in a series of 54 cases of primaryatypical pneumonia found nine with multiple areasof patchy consolidation as described by Scadding(1937), and 18 with coarse reticulation and anoverlay of haze. In the second group of the presentseries, " nodules " were scattered throughout theaffected lung; they consisted of small roundshadows, 2 to 5 mm. in diameter, of moderatedensity at the centre, and without a clearly definededge. They varied in size and density, were distri-buted unevenly, and remained discrete, althoughtoward the latter part of the illness they appearedto have increased a little in size. In some cases thenodules formed aggregations, rarely larger than1 cm. in diameter, of regular or irregular outline,usually granular but sometimes homogeneous.Forming a background to these nodules was anetwork of streaks, denser t'..an the normal lungmarkings. Besides these nodules and network, thetranslucency of the affected lung was diminished,as though a light haze were cast over it.
In the majority of patients in this group theappearance of miliary nodules predominated,
157
mbm..
group.bmj.com on August 15, 2017 - Published by http://thorax.bmj.com/Downloaded from

!:0:f;;E: ::, .t ; ; 0 ¢ > r rt~~~~~~~~~~~~~~~~~~~~~~~~~~~-NI,A
CO3
00
C's)
4)
ON
CO
#'i
. , . ^>- ?- i ? . l}.;- _ .l_tS............:?.~~~~~~~~~4B 4t i.~~ Fi,? : :. . ? ? _ ,:_,w...................-... g l | :: . ?, ; 1-. , g_g&.>~~~~~~~~~~~~~~~~~~~~~4
. ;e.l1 eeie 2 <, - 3 . . es.2:.e$?.._0|. i L . miS.^s . ; -. . s $
l$?,:r,.:.>t2,.';_ '-2''ie i' gi ?,0
*.,-,., ~~~~~ .:s:<Rf. .. _ ,T,,i:s':':,'t~~~~~~~~~~~4
: . ¢ , : t . . . .i' .j 2' .. .::I.
group.bmj.com on August 15, 2017 - Published by http://thorax.bmj.com/Downloaded from

J >X>-k1r, - F xo
.~~~~~~~~~~~~~~~~~~~~~~~~~~I4 a
I-cu
c-o
>
rZ
ed
s.~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~t,,0;j0 0 0.32
Till
_tS,ms:e ~~~~~~~~~~~~~~~~~~~~~~~0+3_~~~~~~~~~~~~~~~~~~~~~~~~:...Wh sIFf
* 2 ^ 4 ~~~~~~~~~~~~~~~~~~3c a
00q > C
> .s
Ail Oi" ' z e! <; ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~-6,
4v ^i! 'rz !;';, n" 1-'S =^~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~C
. ¢,, , _ _ L~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~dC
group.bmj.com on August 15, 2017 - Published by http://thorax.bmj.com/Downloaded from

P. W. VERCO
FIG. 6.-Case 108, P.A. view, November 13, 1946. Opacright lung 10 days after onset.
although the proportion of" network " and nodulesvaried in different areas of the same lung. Inpatients 104 (Fig. 4), 110 (Fig. 5), 108 (Fig. 7), 121(Fig. 8) and 128 the nodules were so widespreadand numerous as to suggest miliary tuberculosis.In patients 107 and 120, the infiltration was lessextensive. In patient 105 the reticular pattern wasthe more pronounced. Whichever form of opacity,nodules or reticulation, was the more prominent,the bases of the lungs were most frequently affected.The infiltration was remarkably widespread. In
two patients, 108 and 121, the lesions were scatteredthroughout both lungs: in patients 104, 110, and128 the whole of one lung and a considerableportion of the other lung were involved. In theremaining patients 105, 107, and 120, large areas ofboth lungs were affected.
Spread of the pneumonic process was observedin several cases. In the initial film of patient 108
ity in uppe
the right upper zone presentedmany nodules aggregated intoa large dense granular opacity,with individual nodulesapparent toward the periphery(Fig. 6). Improvement in thepatient's general conditionwas followed on the nineteenthday of illness, eight days afterthe initial radiograph, by asudden exacerbation ofsymptoms and considerableextension of physical signs.Radiography 25 days afteronset revealed apparent resolution of the opacity in theright upper zone, and nodulesthroughout both lungs, withlessened translucency. Enlarge*ment of the heart, notedclinically for several days, wasalso evident in this film (Fig. 7).The patient died on thetwenty-seventh day of illness,and the miliary appearancewas attributed to extensiveendobronchiolitis and interstitial pneumonia rather than tovenous congestion. Patients107, 110, and 121 showedextension of a predominantlynodular lesion in serial films.Accompanying these pul-
ar half of monary lesions, one hilarshadow was enlarged inpatients 105 and 128. In
patients 107 and 121, the heart was displaced to theleft, and the left diaphragm was elevated. Inpatient 107 there was also a dense opacity, triangularin shape, with defined edges, suggesting segmentalcollapse at the base of the left lung. When thediaphragm and heart returned to their normalpositions in subsequent films, this opacity wasreplaced by several " atelectatic plates," and stillother areas of atelectasis appeared at the left base.Patient 121 (Fig. 8) showed considerable displace-ment of the heart to the left with elevation of theleft diaphragm. The lower third of the left lungwas obscured by a hazy opacity, of moderatedensity in its upper part, but very dense in its lowerportion. Serial films showed the gradual return ofheart and diaphragm to their normal positions, thebasal opacity decreased in extent and density, Frdthe vascular and lung markings reappeated twomonths after onset. The next examination, four
160
TP
:;,.!M,NP R.7:.-'l, -!.-z...... ..:U ,o
group.bmj.com on August 15, 2017 - Published by http://thorax.bmj.com/Downloaded from

THE RADIOLOGY OF PRIMARY ATYPICAL PNEUMONIA
months after onset, showed tenting at the anteriorand medial part of the left diaphragm, which wasstill present 16 months later.
In the initial A.P. film of patient 105, obtained12 days after onset, there were two fine, parallel,linear opacities in the lower half of the right lung.These opacities began just lateral to the cardio-phrenic angle, and extended in a slightly curvedfashion, with the concavity toward the hilum, to theregion of the middle of the transverse fissure. AP.A. film taken a fortnight later, when the reticularopacity had almost resolved, showed that the twolines had been replaced by one wider linear opacity,tapering at its upper extremity, in the same site.Subsequent films four, 13, and 19 months afteronset no longer showed this linear opacity, but a
few abnormal markings persisted at the base of theleft lung. Linear opacities of a similar unusualtype were recorded by Finland, Ritvo, Davidson,and Levenson (1946) and were attributed by themto atelectasis.
Resolution soon followed recovery from the acuteillness, and progressed by diminution in number anddensity of the nodules, return of the normal translu-cency, and a slower decrease of the reticulation. Asthe reticulation waned, there remained accentuationof the normal lung markings. These slowly subsidedover further examinations.Adhesions affecting the middle portion of the
diaphragm became apparent in four patients duringresolution. The left side was affected in patient121, and the right side in patients 104, 110, and 128.An initial A.P. filn of patient 110, obtained 18 daysafter onset, showed an aggregation of nodules at thebase of the right lung. Lateral films a week latershowed the right diaphragm to be elevated in itsmid-portion, with infiltration of the lung above, anda crowded leash of broncho-vascular markingsascending to the right hilum. In later films,resolution of this infiltration showed a small" tent " of diaphragm in this area, five weeks afteronset. Examination three and ten months afteronset showed no abnormality except prominenceof the peripheral lung markings in each lowerzone.
The radiological findings are summarized inTable I. The unusually high proportion of patientspresenting a disseminated focal type ofpneumonia, inmost instances associated with a severe illness, was
probably due to the selection of the more ill patientsfor admission to a busy public hospital. The studywas hampered by the absence of chest films takenbefore the onset of the illness, the frequency ofsevere illness and rapid respirations, and shortagesof films from time to time. In most patients it was
not possible to determine precisely which lobes ofthe lung were involved.
Certain features which were prominent in thisstudy have not been emphasized in other reports.These were the frequent evidence of atelectasis, theformation of diaphragmatic adhesions, and theprolonged persistence of exaggerated lung markings.In general, the more severe and prolonged the acuteillness, the slower was resolution, and the moreprotracted was convalescence by persisting cough,asthenia, and shortness of breath on exertion.Resolution usually advanced at a varying pace to astage at which accentuated lung markings, oftenaccompanied by prominent vascular markingsremained. From this stage, it slowly continued, butalthough in many patients the appearance of thelungs became normal, and in some tenting of thediaphragm became less apparent or disappeared,resolution was not complete in four patients at theend of the period of observation.The tendency of the pulmonary lesions of primary
atypical pneumonia to resolve slowly, the persistenceofabnormal pulmonary markings, and the formationof diaphragmatic adhesions are indicative oforganization of the inflammatory products in part.Golden (1944) described the interspersion of mildand severe bronchiolar lesions. In the latter, he wasimpressed by the dilatation of the bronchioles, thedestruction of the elastic fibres, the fragmentationof the muscle bundles and shredding of the reticularnetwork. It was considered that such lesions couldheal only with persistent dilatation and scar forma-tion, although this did not of necessity imply thatsuch lesions would or could be clinically manifestas chronic bronchiectasis. In other areas of thelungs, a not infrequent feature was masses of fibrin,occasionally seen undergoing organization, fillingalveoli and taking their shape.
Parker, Jolliffe, and Finland (1947) consideredthat polymorphonuclear exudate within the bron-chiolar lumen was the result of secondary bacterialinfection, and that injury to the bronchiolar mucosais not a feature of primary atypical pneumonia. Intheir series, organization of the alveolar and bron-chiolar exudates was found in the majority of casesbut was not extensive.
In the lungs of the two fatal cases seen in Adelaide(Verco, 1949; Fowler and French, 1949), thebronchiolar plugs within the same area appeared tovary greatly in age. Some were recent with poly-morphonuclear exudate, whereas in neighbouringbronchioles organization of the plugs was advanced,although death occurred seven days after the onsetof the illness in one patient, and nine days afterextensive spread of the process in the other (Fig. 9).
161
group.bmj.com on August 15, 2017 - Published by http://thorax.bmj.com/Downloaded from

P. W. VERCO
*C-CNOC
0 bNoc
=~
Z ;-4-
--- -C~n
uollnTosaEl ~ W 14- (2;4 -
bnuQccr0uU C bL
0enpl90
C)~~ ~ ~ ~ ~~~C
SUOT}L3UUp-i13xa
U014-Llo C)CO
N NNN N N
Jo uoTI.E1o9-xa
XuaSo)Id t CO 00 csuolsaqpv I
JreuSeIqd0)l( cC CO 10
p_qsq.o__s_AIpuaxeddV C C] 10 -u014nlosaa_lI S~ -
pauouiLuirl oU,)fnlosaj A A V A
ssOulOf --m
JO 01uolXena _>
S?pop3agI JO 0 a NsZlUbeTA3 IoLi1O C) -aoua)PIAH jaqlo
ijtTqIt j'qs-
uLu.iqd!(r I CO.JO UOJlCeAaI o lI
CA
P9ATOAUI* sIuoz
1. 9 -4
I O U) o Q :Hs~~~~~U
f QSan c X
-~~~~~~~~~~~~~~~~~~-
CC-,0~~~
-n..0(tU ":
CZ CZ C
0 4*
CZ~E-4- -4CZ~~~ ~ ~ ~ ~ ~~.CZ CII
0.0 ~~~ ~~~~~~00c
0 0) 0cCCZ C'~~~~~~0~0C) CZ
+
00C9CO
C--C
IN N >N
t.4N
C).
I
_ I.
CO 00 C
I C N
r- or, I CZ r- C.;C) Cl l cl
V V V V V
It in to r-
r- _ICO 10 10
a s
I41 ~ -~ =
- ~
a C- c O
-
l4
00oo o
t
CY.
10, COI.I-^ CO
co cl1
zl-Z N NI_I
_- 0C:11:4 - 04OCl'
- II_
-
A
00N
CIC-I
CO
CO
1(0 CO)
P
I NL")NNN IO-~N 'N
pe ~ - :
0. _ -
NW.° 't, <, - 00I o C O Co
_ -_ - -
NNNNNNNNNNN NNNN
00 to 00 CO
oC 0Z - 00- 0. 0.4
04
c-0
iC'0t 0
0
4)1.
to
C.-
Cr
06
C
-C
Co1.
c- II:>0.4.
162
z0
P..
z
UA
m 0
0
04)L1J4
>4)
>4)
0)
UW4
IdJop~ O C 0 C
4.evlur ,, C), 00 - _
laquinNjiw o Co o
I
juawas.irlu,qJ-eITH
group.bmj.com on August 15, 2017 - Published by http://thorax.bmj.com/Downloaded from

THE RADIOLOGY OF PRIMARY ATYPICAL PNEUMONIA
Further, in the peribronchiolar and other alveoli ofboth patients, organization, although not extensive,was proceeding (Figs. 10 and 11). In other respectsthe histological lesions in the lungs of these twopatients were very similar to those described byGolden.These histological findings suggest that delay in
resolution in primary atypical pneumonia withpersisting symptoms may well be due to localobliterative bronchiolitis, fibrosis in the bronchiolarwall, and organization within the alveoli.
FIG. 9.-Case 108. Photomicrograph of section stainedwith Krajian's reticulum stain showing organizationwithin bronchiole with recently formed collagenfibres. X 210.
FIG. 10.-Case 108. Photomicrograph of section stainedwith Kraiian's reticulum stain showing organizationof alveolar exudate with recently formed collagenfibres within the alveoli. x 175.
FIG. 11.-Case 120. Photomicrograph stainedwith Masson's trichrome stain showingorganization within alveoli, probably of aprotruding bronchiolar plug. X 175.
DIFFERENTIAL DIAGNOSISIn the first group of six patients the course of the
illness was not severe, and the radiological lesionswere of the form which usually accompanies primaryatypical pneumonia. This more compact, localizedform of opacity may mimic many other diseases,not only as it develops, but when at its maximum,and again in resolution. Previous observers haveemphasized that other forms of pneumonia, not theleast among which was pulmonary tuberculosis,could not be distinguished from primary atypicalpneumonia on the basis of radiographic evidencealone, as the shadows were not distinctive of thiscondition exclusively.
In the experience of most observers, the widelydisseminated, focal form of pneumonia observed inthe second group of eight patients has been asso-ciated with a severe and prolonged course. Thedifferential diagnosis of these " disseminated focal"cases will be considered in more detail.The pulmonary lesions of acute miliary tuber-
culosis are small, of uniform size, and evenlydistributed throughout the lungs. Acino-nodularforms of tuberculosis usually complicate pre-existingpulmonary tuberculosis and are seldom seen in pureform for any length of time. Miliary forms ofpneumonia have been described accompanyingmeasles, chickenpox (Waring, Neubuerger, andGeever, 1942), epidemic influenza (Shore, 1918),
163
group.bmj.com on August 15, 2017 - Published by http://thorax.bmj.com/Downloaded from

P. W. VERCO
pertussis (Caffey, 1945; Lapin, 1943), acute bron-chiolitis in children (Paul, 1941), brucellosis (Aus-trian and Brown, 1942), and tularaemia (Archer,Blackford, and Wissler, 1935), and due to haemolyticstreptococci (Ellman, 1946). Pneumonia of thisdistribution is apparently not produced by thepsittacosis group of viruses or by Rickettsia burneti,though it may appear in the later stages of scrubtyphus. Chemical pneumonia may be delayed inonset, or may follow immediately the inhalation or
aspiration of noxious material. In irrespirable gas
intoxication the picture resembles that of acutepulmonary oedema, except that the nodules are
more distinctfiand the cardiac silhouette is unaltered;in the presence of secondary infection the roentgenfindings may alter considerably (Rubin, 1947).Finland and others (1946) encountered similaropacities among victims of the Cocoanut Grove firein Boston. The acute pulmonary disease whichmay follow inhalation of fumes arising from theheat processing of beryllium (van Ordstrand andothers, 1945) and cadmium (Paterson, 1947) may
cause miliary shadows. Aluminium pneumoconiosis(Shaver and Riddell, 1947) is said to arise as a resultof breathing concentrations of powdered aluminiumover periods as short as three months. Lipoidpneumonia, aspiration pneumonia consequent upona disorder of swallowing, or the pulmonary lesionsaccompanying cardiospasm may assume a diffusenodular form (Hawes and Soule, 1945).
In individuals subject to asthma, transientdisseminated foci of opacity may be associated witha high percentage of eosinophils in the circulatingblood. A similar form of pulmonary opacityaccompanies " tropical eosinophilia " (Hodes andWood, 1945), and may be present in periarteritisnodosa (King, 1938), erythema multiforme exuda-tivum (Kneeland and Smetana, 1940), and dis-seminated lupus erythematosus (Austrian andBrown, 1942). Coccidioidomycosis (Rakofsky andKnickerbocker, 1946) and histoplasmosis (Colvin,Gore, and Peters, 1944) may produce miliary lesionsin the lungs. Fawcitt (1938) described an occupa-
tional hazard of agricultural workers associatedwith infections by a number of fungi; a frequentradiological finding was a rather soft, snow-flakemottling, widely distributed throughout both lungs,with a tendency for the mid-lung fields and bases tobe more affected than the apices. Tornell (1946)described miliary disease of the lungs accompanyinginfection with monilia. It is suspected that themiliary mottlings in the lungs of bagasse workers(Lemone and others, 1947) are due to organisms,probably fungi, attached to the fibres of bagasse(Gerstl and others, 1947).
La Due (1941) has reported a case of bronchiolitisfibrosa obliterans, which presented a focal dis-seminated form of opacity. Toxoplasmosis hasbeen reported in Australia (Robertson, 1946); thedescription of the pulmonary lesions by Pinkertonand Henderson (1941) is of interest. Other condi-tions which might conceivably present confusion arepulmonary metastases of malignant disease, irra-diation pneumonitis (Widmann, 1942), the pneu-moconioses, sarcoidosis (Garland, 1947), bron-chiectasis and cystic disease of the lungs, alveolarfilling with iodized oil, endogenous pulmonarysiderosis (Scott and others, 1947), pulmonaryossification accompanying mitral stenosis (Elkelesand Glynn, 1946), the pneumonia accompanyingacute rheumatic fever (Mossberger, 1947), miliarygummata in syphilis, purpura, schistosomiasis(Shanks and others, 1938), miliary leprosy (Deland,1948), polycythaemia vera, and the pulmonarychanges in scleroderma (Rubin, 1947; Lloyd andTonkin, 1948), the xanthomatoses, and ituberosesclerosis (Berg and Nordenskjold, 1946).
DIscussIoNAetiology.-Among the many descriptions of
epidemic and endemic primary atypical pneumonia,few are accompanied by adequate aetiologicalinvestigation (Commission on Acute RespiratoryDisease, 1944 and 1946; Meiklejohn, 1947; Curnenand others, 1945; Eaton and others, 1942).
Scadding (1948) has reviewed the literature onthis subject. He has suggested that in many reportscase histories and radiographs were consistent witha segmental collapse. This might well be that typeof atelectasis described by Ramsay and Scadding(1939), believed to result from infected mucus ofnasal or bronchial origin obstructing bronchi orbronchioles. This phenomenon is of sporadicoccurrence, and associated with acute or chroniccatarrh of the respiratory tract.The Commission on Acute Respiratory Diseases
(1946) were able to transmit "primary atypicalpneumonia" to human volunteers, using filteredthroat washings and sputum. The high associatedincidence of acute upper respiratory tract infectionsin the recipients indicated that probably severalvirus infections were transmitted. More recently,an illness like the common cold, another illnessresembling the acute pharyngitis of recruits, and" primary atypical pneumonia " were transmittedto human volunteers. Subsequent challenge experi-ments have provided some evidence of the indivi-duality of these virus diseases (Commission onAcute Respiratory Diseases, 1947). These experi-ments strongly suggest that primary atypical
164
group.bmj.com on August 15, 2017 - Published by http://thorax.bmj.com/Downloaded from

THE RADIOLOGY OF PRIMARY ATYPICAL PNEUMONIA
pneumonia is caused by a virus or viruses. Thedifficulties of this sort of work are great: attemptsto procure experimental transmission to man ofvirus influenza and the common cold have beenremarkable for failures and difficulty in obtaining"'takes," and the resulting illness has usually beenmild. Eaton, Meiklejohn, and van Herick (1945)transmitted a virus from cases of primary atypicalpneumonia to chick embryos by inoculation withsuspensions of bacteriologically sterile lung tissue orfiltered sputum. Strains of this virus have beenadapted by passage to infect cotton rats or hamstersby intranasal inoculation, causing pulmonary lesions.Considerable difficulty was experienced because ofcontamination with latent respiratory viruses alreadypresent in the animals. The agent propagated inthe chick embryos was specifically neutralizable bythe sera of patients convalescent from primaryatypical pneumonia, but not by acute phase sera.This virus seems fairly well established as a cause ofdisease in man, and Eaton has estimated that itaccounts for a considerable portion of cases ofprimary atypical pneumonia (1945). Breslow (1945)studied clinically an outbreak of acute respiratorydisease associated with atypical pneumonia in whichthere was serological evidence of infection by thisvirus. The illness was generally mild, and only asmall proportion of cases showed clinical evidenceof pneumonia. He concluded that the disease wasprobably not primarily a pneumonia: the designa-tion " atypical pneumonia " seemed to exaggeratewhat was probably only an incident in the disease.
Evidence obtained by transmission experimentsand in aetiological studies strongly supports a virusor viruses as the cause of this condition. It is notimprobable that the same agent should be respon-sible for the two forms of pulmonary opacity,which are associated with very similar clinical andlaboratory findings. The radiological lesions, whilefalling into two groups, have certain likenesses,gradations between the two groups occur, and thecompact localized form of opacity has been followedby disseminated focal spread in the same patient(Figs. 6 and 7). Cases of the disseminated focalform of pneumonia have occurred as a minority inepidemics of primary atypical pneumonia, andsimilar pulmonary lesions were present in severalcases of experimentally transmitted disease (Com-mission on Acute Respiratory Diseases, 1946).Pulmonary Changes in Long Incubation Period
Virus Diseases.-Both forms of opacity accompanylong incubation period virus diseases, notablymeasles, and occur at a period when superimposedsecondary infection is unlikely. Though thefrequent involvement of the lower portions of the
lungs in primary atypical pneumonia has beenaccepted as evidence of infection and spread by theair passages, a rather similar distribution of thelobes involved occurs in measles pneumonia.Kohn and Koiransky (1929) have drawn attention
to the early and frequent pulmonary involvementpresent in the eruptive and pre-eruptive stages ofmeasles in children. On radiography this wasmanifest in nearly all the cases of one study (Kohnand Koiransky, 1933) as enlargement of the lymphnodes about the tracheal bifurcation, and was mostreadily detected in lateral films. Pulmonaryinfiltration occurred in some 60 per cent of cases,and was either widely disseminated or more localized.Pleural involvement was frequently shown byvisibility of the fissures between the lobes: in somecases substantial opacities were seen in thesesituations and against the anterior chest wall. Apost-mortem radiograph of the lungs from a childdying with the widely disseminated focal form ofmeasles pneumonia revealed innumerable smalldense opacities of varying size scattered throughoutboth lungs, without much tendency to coalesce orform large confluent areas. Histologically, thelesions were comparable with those of primaryatypical pneumonia described by Golden (1944).Compared with a radiograph of the lungs of a childwho died of miliary tuberculosis, the nodules inmeasles are larger, of less uniform size, and not soevenly distributed throughout the lungs.
Milles (1945) recorded the deaths of two adultsfrom measles, and noted the radiographic resem-blance of the disseminated bronchiolitis, peribron-chiolitis, and bronchopneumonia of measles tomiliary tuberculosis and to some cases of primaryatypical pneumonia.
Waring, Neubuerger, and Geever (1942) recordedtwo cases of pneumonia accompanying severechickenpox in adults, with one fatality. Thepneumonia in the fatal case was of virus type, andin both cases radiography five and six days after theonset revealed " widespread mottling" or innumer-able small shadows throughout both lungs, similarto certain cases of pneumonia accompanyingmeasles. Both cases were thought to be examplesof primary pneumonia due to the virus of chicken-pox, although the non-fatal case was complicatedby secondary infection with a haemolytic strepto-coccus.
Evidence has been presented by the Commissionon Acute Respiratory Diseases (1946), that theincubation period of primary atypical pneumonia isfrom seven to fourteen days when transmitted tohuman volunteers. This minimal incubation periodof seven days is much longer than one would expect
165
group.bmj.com on August 15, 2017 - Published by http://thorax.bmj.com/Downloaded from

P. W. VERCO
in a purely local respiratory disease such as influenza,in which the incubation period is about two days.
In primary atypical pneumonia the widespreadpulmonary lesions, often symmetrical, are verysimilar to those seen in the primary pneumonias ofthe long incubation period virus diseases, measlesand chickenpox, and may resemble in distributionthose of miliary tuberculosis. This suggests ana-logous dissemination of the causative organism bythe blood stream, although " thresher's lung," anacute miliary pneumonia caused by monilia, appar-ently results from extensive airborne infection frommouldy grain while threshing (Tornell, 1946). Inprimary atypical pneumonia enlargement of thespleen sometimes occurs, and in an acute febrileillness this of itself suggests haematogenous spread.The occurrence of leucoencephalitis, as in patient120, and of a haemolytic anaemia with myeloidprimitive cells in patient 105, together with symptomsof meningeal involvement with an increased cellularcontent of the cerebrospinal fluid, are suggestive ofa general systemic disease. The occurrence of coldagglutinins and of " T" agglutinins, like heterophilagglutinins in mononucleosis, indicates the presenceof some widespread interference with the globulin-producing mechanism.
These features suggest that primary atypicalpneumonia may be a general systemic disorderwhich almost invariably localizes in the lungs. Itmay be that there is a primary localized focus ofinfection in the respiratory tract, which may eitherspread directly along the mucous membranes toproduce a rather extensive local consolidation, ormay be followed by invasion of the blood streamvia the regional lymph nodes. Most frequently,perhaps, both modes of spread would occur. Thewidely disseminated lung lesions may follow theperiod of viraemia directly; or probably there is, asFenner (1948) has postulated for the acute exanthe-mata, a period of multiplication of virus in the cellsof the reticulo-endothelial system in the spleen andelsewhere before sufficient virus is freed into theblood stream to cause the widely scattered foci inthe lungs. There is no doubt that other factors suchas the amount of the infecting agent, its invasivenessand virulence, the general and local resistance of theinfected host, and the presence of hypersensitivity orallergy to the infecting agent determines the distri-bution and extent of the resulting lesion.
Incomplete Resolution.-In this series of cases,patients in the first group were only moderately ill.A severe and prolonged course was frequent in thesecond group, and there were two fatalities. Resolu-tion followed subsidence of the acute symptoms inboth groups, but in many cases accentuated lung
markings persisted in the affected areas. In severalpatients tenting of the central portion of onediaphragm was disclosed, although there was nosensitivity to the Mantoux test. Subsequently, theabnormal lung markings and diaphragmatic adhe-sions disappeared in some patients, but in othersremained throughout the period of observation.The two fatal cases had been treated with peni-
cillin intramuscularly. The lungs of patient 120were bacteriologically sterile at necropsy, andbacteria were not seen in the sections, but areas ofpolymorph exudate which were not within thebronchioles and suggesting secondary bacterialinfection, were present in the lungs. Such areaswere few and of small extent in patient 108. Despitethe short duration of the illness in one patient, andrecent spread of the process in the other, somebronchiolar plugs were in a state of advancedorganization, and fibroblasts with newly formedfibres of collagen were present amid the exudate ofmononuclear cells in some peribronchiolar andother alveoli.Though the organization was not extensive in
these cases, it has been observed in similar cases byGolden (1944) and Parker, Jolliffe, and Finland(1947). In this series the early organization isconsidered to be responsible for the delay in resolu-tion with persisting accentuated lung markings, forthe appearance of diaphragmatic adhesions, and tofavour the conception that, like measles andinfluenza, primary atypical pneumonia may lead toresidual pulmonary fibrosis.
SUMMARYThe radiological features of a series of 14 cases
of primary atypical pneumonia were studied. Themajority of these cases occurred during an epidemic.Aetiological studies were carried out. The clinical,radiological, and laboratory features closelyresembled those described in this condition by otherobservers, as did the histology of the lungs in thetwo fatal cases.
In six patients the opacities in the radiographs ofthe lungs were localized. In the remaining eight,the radiographs indicated lesions in widely dis-seminated foci; these patients were more ill, andtwo of them died. In five patients of this group,the radiological features suggested acute miliarytuberculosis.During resolution which followed subsidence of
the acute symptoms, tenting of the central portionsof either half of the diaphragm was disclosed incertain patients. As resolution advanced, abnor-mally increased lung markings persisted for varyingperiods, and in four patients were still present at
166
group.bmj.com on August 15, 2017 - Published by http://thorax.bmj.com/Downloaded from

THE RADIOLOGY OF PRPMARY ATYPICAL PNEUMONIA
the termination of the study. The persisting lungmarkings and the formation of diaphragmaticadhesions were taken as evidence ofresidual fibrosis,and histological confirmation was obtained from bothfatal cases.
My thanks are due to the honorary and technicalstaff of the Radiological Section of the Royal AdelaideHospital for help and criticism in carrying out thisinvestigation, and to Mr. L. N. Jones for reproducingthe radiographs.
REFERENCESAdams, J. M. (1941). J. Amer. med. Ass., 116,925.Allen, F. H., and Kellner, A. (1947). Amer. J. Path., 23,
463.Archer, V. W., Blackford, S. D., and Wissler, J. E.
(1935). J. Amer. med. Ass., 104, 895.Austrian, C. R., and Brown, W. H. (1942). Amer. Rev.
Tuberc., 45, 751.Berg, G., and Nordenskjbld, A. (1946). Acta med.
scand., 125, 428.Breslow, L. (1945). J. clin. Invest., 24, 775.Caffey, J. (1945). Pediatric X-Ray Diagnosis, The Year
Book Publishers, Chicago, 264.Claudy, W. D. (1947). Arch. intern. Med., 80, 185.Colvin, S. H., Gore, I., and Peters, M. (1944). Amer. J.
med. Sci., 207, 378.Commission on Acute Respiratory Diseases (1944).
Amer. J. Hyg., 39, 67, 197, 298.(1946). Bull. Johns Hopk. Hosp., 79, 97.(1947). J. clin. Invest., 26, 957.
Curnen, E. C., Mirick, G. S., Ziegler, J. E., Thomas, L.,and Horsfall, F. L. (1945). J. clin. Invest., 24, 209.
Deland, C. M. Personal communication.Drew, W. R. M., Samuel, E., and Ball, M. (1943).
Lancet, 1, 761.Eaton, M. D., (1945). Calif. Med., 26, 957.
Meiklejohn, G., and van Herick, W. (1945). J. clin.Invest., 24, 241.
and Talbot, J. C. (1942). Science, 96, 518.Elkeles, A., and Glynn, L. E. (1946). J. Path. Bact., 58,
517.Ellman, P. (1946). Brit. med. J., 1, 127.Fawcitt, R. (1938). Brit. J. Radiol., n.s., 11, 378.Feinstein, M., Yesner, R., and Marks, J. L. (1946).
Amer. J. Hyg., 44, 72.Fenner, F. (1948). Lancet, 2, 915.Finland, M., Ritvo, M., Davidson, C. S., and Levenson,
S. M. (1946). Amer. J. Roentgenol., 55, 1.Fowler, M., and French, E. L. (1949). Med. J. Australia,
1,267.Garland, L. H. (1947). Radio.ogy, 48, 333.Gerstl, B., Tager, M., and Marinaro, N. A. (1947).
Arch. Path., 44, 343.Golden, Alfred (1944). Arch. Path., 38, 187.Hawes, L. E., and Soule, A. B. (1945). Amer. J. Roent-
genol., 53, 124.Hodes, P. J., and Wood, F. C. (1945). Amer. J. med.
Sci., 210, 288.Jamison, H. W. (1945). Radiology, 45, 15.King, D. S. (1938). New International Clinics, 1, 115.Kneeland, Y., and Smetana, H. F. (1940). Bull. Johns
Hopk. Hosp., 67, 229.Kohn, J. L., and Koiransky, H. (1929). Amer. J. Dis.
Child., 38, 258.(1933). Ibid., 46,40.
La Due, J. S. (1941). Arch. intern. Med., 68, 663.Lapin, J. H. (1943). Whooping Cough. Charles C.
Thomas, Springfield, Illinois.Lemone, D. V., Scott, W. G., Moore, S., and Link
Koven, A. (1947). Radiology, 49, 556.Lewis, E. K., and Lusk, F. B. (1944). Radiology, 42,423.Lind, P. E., and McArthur, N. R. (1947). Aust. J. exp.
Biol. med. Sci., 25, 247.Lloyd, W. E., and Tonkin, R. (1948). Thorax, 3,241.Loffler, W., and Moeschlin, S. (1946). Schweiz. med.
Wschr., 76, 815.McCarthy, Paul V. (1943). Radiology, 40, 344.McCordock, H. A., and Muckenfuss, R. S. (1933).
Amer. J. Path., 9, 221.McIntosh, H. C., and Spitz, S. (1939). Amer. J.
Roentgenol., 41, 605.Meiklejohn, G. (1947). Med. Clin. N. Amer., 31, 1442.Milles, G. (1945). Amer. J. clin. Pzth., 15, 334.Mossberger, J. I. (1947). J. Pediat., 30, 113.Parker, F., Jolliffe, L. S., and Finland, M. (1947). Arch.
Path., 44, 581.Paterson, J. C. (1947). J. industr. Hyg., 29, 294.Paul, L. W. (1941). Amer. J. Roentgenol., 45, 41.Pinkerton, H., and Henderson, R. G. (1941). J. Amer.
med. Ass., 116, 807.Rakofsky, M., and Knickerbocker, T. W. (1946). Amer.
J. Roentgenol., 56, 141. .Ramsay, H., and Scadding, J. G. (1939). Qiart. J.
Med., n.s., 8, 79.Reimann, H. A. (1938). J. Amer. med. Ass., 111, 2377.Robertson, E. G. (1946). Med. J. Australia, 2, 449.Rubin, E. H. (1947). Diseases of the Chest, W. B.
Saunders Co., Philadelphia.Scadding, J. G. (1937). Brit. med. J., 2, 956.- (1948). Lancet, 1, 89.
Scott, L. W. D., Scott Park, S. D., and Lendrum, A. C.(1947). Brit. J. Radiol., n.s., 20, 100.
Shanks, S. C., Kerley, P., and Twining, E. W. (1938).Text-book of X-ray Diagnosis by British A!thors, 1,London.
Shaver, C. G., and Riddell, A. D. (1947). J. industr.Hyg., 29, 145.
Shore, T. H. G. (1918). Special Report Series, No. 36,96. London.
Showacre, E. C., Wightman, H. B., and Moore, N. S.(1944). N.Y. St. J. Med., 44, 872.
Smadel, J. E., Green, R. H., Paltauf, R. M., and Gon-zales, T. A. (1942). Proc. Soc. exp. Biol., N.Y.,49, 683.
Tornell, E. (1946). Acta med. scand., 125, 191.Treuting, W. L., and Olson, B. J. (1944). Publ. Hlth
Rep., 59, 1331.van Ordstrand, H. S., Hughes, R., de Nardi, J. M., and
Carmody, M. G. (1945). J. Amer. med. Ass., 129,1084.
Verco, P. W. (1949). Med. J. Australia, 1, 254.Waring, J. J., Neubuerger, K., and Geever, E. F. (1942).
Arch. intern. Med., 69, 384.Wechsler, H. F., Rosenblum, A. H., and Sills, C. T.
(1946). Ann. intern. Med., 25, 113.Widmann, B. P. (1942). Amer. J. Roentgenol., 47, 24.Winternitz, M. C., Wason, I. M., and McNamara, F. P.
(1920). Pathology of Influenza, Yale UniversityPress, New Haven, Connecticut.
Ziegler, J. E., Curnen, E. C., Mirick, G. S., and Horsfall,F. L. (1947). Amer. J. med. Sci., 213,268.
167
group.bmj.com on August 15, 2017 - Published by http://thorax.bmj.com/Downloaded from

Atypical PneumoniaThe Radiology of Primary
P. W. Verco
doi: 10.1136/thx.4.3.1521949 4: 152-167 Thorax
http://thorax.bmj.com/content/4/3/152.citationUpdated information and services can be found at:
These include:
serviceEmail alerting
the online article. article. Sign up in the box at the top right corner of Receive free email alerts when new articles cite this
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on August 15, 2017 - Published by http://thorax.bmj.com/Downloaded from








![l & E x perimenta l i n ic lp Journal of Clinical ... · the so-called atypical pneumonia, which is a type of pneumonia with an overall prevalence of 22.7% [1]. It is also a causative](https://img.pdfslide.net/doc/110x75/6082e1604c6d78134f366804/l-e-x-perimenta-l-i-n-ic-lp-journal-of-clinical-the-so-called-atypical.jpg)