Embed Size (px)
Citation preview

Brain & Development, 15 (1993) 439~145 0387-7604/93/$06.00 © 1993 Elsevier Science Publishers B.V. All rights reserved
BRADEV00101
Autosomal recessive congenital cerebellar atrophy
A clinical and neuropsychological study
F r a n c e s c o G u z z e t t a a, M D , E u g e n i o M e r c u r i a, M D , S t e l l a r i o B o n a n n o a, P s y c h o l o g i s t ,
M a r c e l l o L o n g o b, M D a n d M a r i a S p a n 6 a, M D
aUnit o f ChildNeuropsychiatryand bRadiologicalSciencesDepartment, School ofMedicine, University ofMessina, Messina, Italy
Received 8 February 1993; accepted 23 July 1993
Congenital cerebellar atrophy associated with a non-progressive cerebellar syndrome and mild cognitive retardation is described in seven cases, four of them familial. Their occurrence is consistent with an autosomal recessive inheritance. Clinical and neuroimaging data seem to exclude supratentorial changes. Even though it is not possible to definitely rule out a possible role of the forebrain in determining the mental defect, the neuropsychological study supplies arguments stressing the relationship between cerebellar defect and cognitive development.
Key words: Cerebellar atrophy; Cognitive development; Brain; Congenital pathology
I N T R O D U C T I O N
Congenital cerebellar atrophy, whether isolated or as- sociated with other neurological and systemic disor- ders, is not infrequent [1-8]. Its nosological interpreta- tion is controversial and its pathogenic mechanism het- erogeneous. Isolated diffuse cerebellar atrophy, autoso- mal recessively inherited or sporadically occurring, is described as a separate syndrome [2,9-13] with a non- progressive cerebellar dysfunction and varying degrees of cognitive impairment.
The genetic syndrome has been recognized [14] and there are some clinical features that distinguish the autosomal recessive form from both autosomal [15-17] or sex-linked dominant type [18,19].
Our study concerns 7 new cases, most of them famil- ial, autosomal recessively inherited or sporadic, with congenital non-progressive ataxia and a mild cognitive defect, associated with a diffuse cerebellar atrophy. Neuropsychological tests were carried out in order to assess the possible involvement of the cerebellum in the development of the cognitive competence as was recently suggested [20,21].
Correspondence address: Prof. F. Guzzetta, lstituto di Neuropsi- chiatria Infantile, Policlinico Universitario, Via Consolare Valeria, 98125 Messina, Italy. Fax: (39) (90) 293 0414.
CASE REPORT
Seven children (4 F, 3 M) with cerebellar a t rophy and without any associated supratentorial lesion were stu- died. Clinical findings are summarized in Tables I and II.
No metabolic markers were found and there was no clinical evidence of progression of the disorder.
The age of the subjects ranged from 4 years and 3 months to 8 years and 7 months (medium 6 years and 3 months). A familial history of cerebellar disease was positive for 4 children (two couples of siblings) (Table III). One of the two couples presented with a family history of epilepsy as well.
There was no evidence of complications during preg- nancy, delivery or the perinatal period in any case.
With regard to the onset of symptoms, delayed devel- opment was a common early finding in all the subjects. One of the children (Case l) showed tremors and severe hypotonia as well. Ataxia, language disabilities and co- ordination abnormalities were constantly present. The onset of the ataxic syndrome occurred during the first year of life in all the patients except in Case 3, whose first manifestation of the disorder was at the age of 3 years and 6 months. Muscular tonus was not impaired in 5 subjects.
The clinical suspicion was confirmed by CT scan and in four cases also by MRI. Diffuse atrophy was always
Brain & Development, Vol 15. No 6, 1993 439
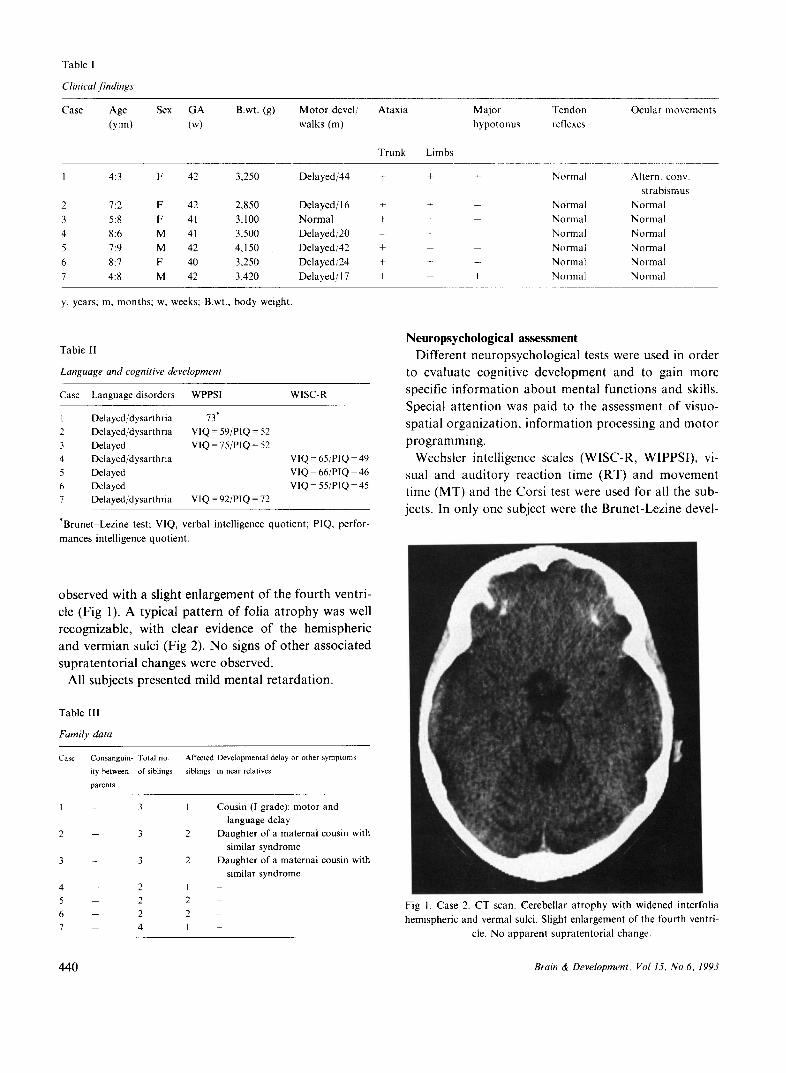
Table I
Clinical findings
Case Age Sex G A B.wt. (g) M o t o r devel/ A tax ia
(y:m) (w) walks (m)
Trunk Limbs
Major Tendon
hypo tonus rel]exes
Ocula r movements
I 4:3 F 42 3,250 Delayed/44 + +
2 7:2 F 42 2,850 Delayed/16 + +
3 5:8 F 41 3,100 N o r m a l + +
4 8:6 M 41 3,500 Delayed/20 - +
5 7:9 M 42 4,150 Delayed/42 +
6 8:7 F 40 3,250 Delayed/24 + +
7 4:8 M 42 3,420 Delayed/17 + -
y, years; m, months ; w, weeks; B.wt., body weight.
Normal Altern. cony.
s t rabismus
- Norma l N o r m a l
- Normal Norma l
Normal Norma l
- Norma l Normal
- Norma l Norma l
+ Norma l Normal
Table II
Language and cognitive development
Case Language disorders WPPSI WISC-R
1 Delayed/dysarthria 73 °
2 Delayed/dysarthria VIQ - 59/P1Q = 52
3 Delayed V1Q = 75/PIQ - 52
4 Delayed/dysarthria
5 Delayed
6 Delayed 7 Delayed/dysarthria VIQ = 92/PIQ = 72
V I Q = 6 5 / P I Q = 4 9
V I Q = 6 6 / P I Q = 4 6
V I Q = 5 5 / P I Q = 4 5
*Brunet-Lezine test; VIQ, verbal intell igence quot ient ; PIQ, perfor-
mances intell igence quot ient .
Neuropsyehologieai assessment Different neuropsychological tests were used in order
to evaluate cognitive development and to gain more specific information about mental functions and skills. Special attention was paid to the assessment of visuo- spatial organization, information processing and motor programming.
Wechsler intelligence scales (WISC-R, WIPPSI), vi- sual and auditory reaction time (RT) and movement time (MT) and the Corsi test were used for all the sub- jects. In only one subject were the Brunet-Lezine devel-
observed with a slight enlargement of the fourth ventri- cle (Fig 1). A typical pattern of folia atrophy was well recognizable, with clear evidence of the hemispheric and vermian sulci (Fig 2). No signs of other associated supratentorial changes were observed.
All subjects presented mild mental retardation.
Table III
Family data
Case Consanguin- Total no. ity between of siblings
parents
Affected Developmental delay or other symptoms
siblings in near relatives
3 1
3 2
3 2
2 1 2 2
2 2
4 1
Cousin (I grade): motor and
language delay Daughter of a maternal cousin with
similar syndrome Daughter of a maternal cousin with
similar syndrome
Fig 1. Case 2. CT scan. Cerebel lar a t r ophy wi th widened interfol ia
hemispher ic and vermal sulci. Slight en la rgement of the fourth ventri-
cle. No apparen t supra ten tor ia l change.
440 Brain & Development, Vol 15, No 6, 1993
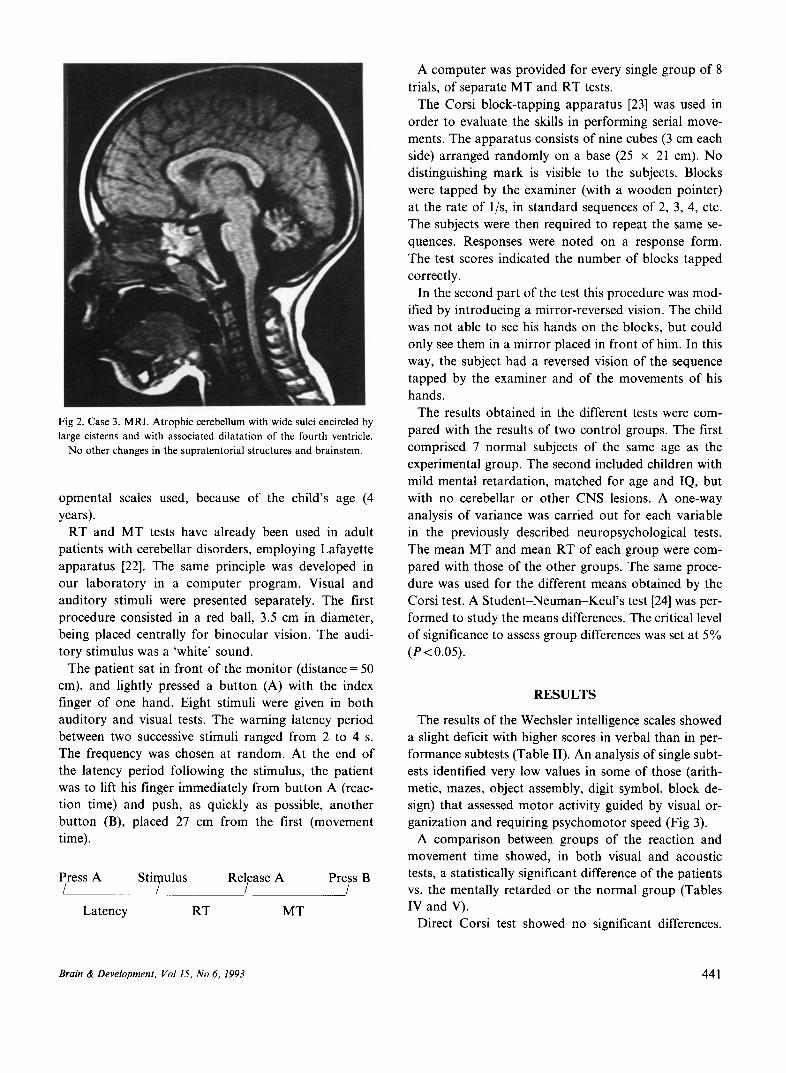
Fig 2. Case 3. MRI. Atrophic cerebellum with wide sulci encircled by large cisterns and with associated dilatation of the fourth ventricle.
No other changes in the supratentorial structures and brainstem.
opmental scales used, because of the child's age (4 years).
RT and MT tests have already been used in adult patients with cerebellar disorders, employing Lafayette apparatus [22]. The same principle was developed in our laboratory in a computer program. Visual and auditory stimuli were presented separately. The first procedure consisted in a red ball, 3.5 cm in diameter, being placed centrally for binocular vision. The audi- tory stimulus was a 'white' sound.
The patient sat in front of the monitor (distance = 50 cm), and lightly pressed a button (A) with the index finger of one hand. Eight stimuli were given in both auditory and visual tests. The warning latency period between two successive stimuli ranged from 2 to 4 s. The frequency was chosen at random. At the end of the latency period following the stimulus, the patient was to lift his finger immediately from button A (reac- tion time) and push, as quickly as possible, another button (B), placed 27 cm from the first (movement time).
l~ress A Stimulus/ Re~ease A Pre~ss B
Latency RT MT
A computer was provided for every single group of 8 trials, of separate MT and RT tests.
The Corsi block-tapping apparatus [23] was used in order to evaluate the skills in performing serial move- ments. The apparatus consists of nine cubes (3 cm each side) arranged randomly on a base (25 x 21 cm). No distinguishing mark is visible to the subjects. Blocks were tapped by the examiner (with a wooden pointer) at the rate of l/s, in standard sequences of 2, 3, 4, etc. The subjects were then required to repeat the same se- quences. Responses were noted on a response form. The test scores indicated the number of blocks tapped correctly.
In the second part of the test this procedure was mod- ified by introducing a mirror-reversed vision. The child was not able to see his hands on the blocks, but could only see them in a mirror placed in front of him. In this way, the subject had a reversed vision of the sequence tapped by the examiner and of the movements of his hands.
The results obtained in the different tests were com- pared with the results of two control groups. The first comprised 7 normal subjects of the same age as the experimental group. The second included children with mild mental retardation, matched for age and IQ, but with no cerebellar or other CNS lesions. A one-way analysis of variance was carried out for each variable in the previously described neuropsychological tests. The mean MT and mean RT of each group were com- pared with those of the other groups. The same proce- dure was used for the different means obtained by the Corsi test. A Student-Neuman-Keul 's test [24] was per- formed to study the means differences. The critical level of significance to assess group differences was set at 5% (t '<0.05).
RESULTS
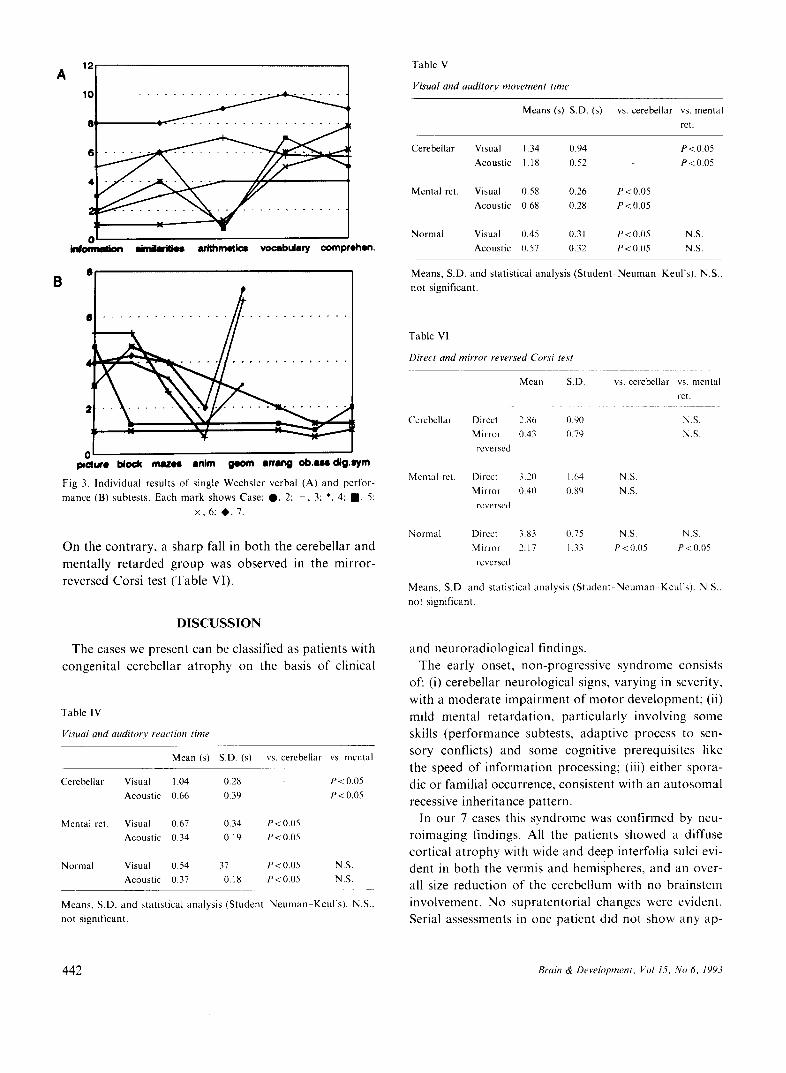
The results of the Wechsler intelligence scales showed a slight deficit with higher scores in verbal than in per- formance subtests (Table II). An analysis of single subt- ests identified very low values in some of those (arith- metic, mazes, object assembly, digit symbol, block de- sign) that assessed motor activity guided by visual or- ganization and requiring psychomotor speed (Fig 3).
A comparison between groups of the reaction and movement time showed, in both visual and acoustic tests, a statistically significant difference of the patients vs. the mentally retarded or the normal group (Tables IV and V).
Direct Corsi test showed no significant differences.
Brain & Development, Vol 15, No 6, 1993 441
'21 10 . . . . . .
8
A
4
2
0 ' '
ink)rnmlk~ d n d l m ~ s arithmetics vocabulary comprehen.
8
e "
4
B
~ e I ~ o ~ m a z ~ anita geom a m m g o b . u e d t g . ~ m
Fig 3. Ind iv idua l results of single Wechsler verbal (A) and perfor-
mance (B) subtests. Each mark shows Case: O , 2; + , 3: *, 4: l l , 5:
x , 6 ; @.7 .
On the contrary, a sharp fall in both the cerebellar and mentally retarded group was observed in the mirror- reversed Corsi test (Table VI).
DISCUSSION
The cases we present can be classified as patients with congenital cerebellar atrophy on the basis of clinical
Table IV
Visual and auditory reaction time
Mean (s) S.D. (s) vs. cerebellar vs. mental
Cerebellar Visual 1.04 0.28 P < 0.05
Acoustic 0.66 0.39 P < 0.05
Mental ret. Visual 0.67 0.34 P<0 .05
Acoustic 0.34 0.19 P<0 .05
Normal Visual 0.54 37 P<0 .05 N.S.
Acoustic 0.37 0.18 P<0 .05 N.S.
Means, S.D. and stat ist ical analysis (Student N e u m a n Keul's). N.S..
not significant.
Table V
Visual and auditor), movement time
Means (s) S.D. (s) vs. cerebellar vs. mental ret.
Cerebellar Visual 1.34 0.94 P<0.05
Acoustic 1.18 0.52 P<0.05
Mental ret. Visual 0.58 0.26 P<0 .05
Acoustic 0.68 0.28 P<0 .05
Normal Visual 0.45 0.31 P<0.05 N.S. Acoustic 0.57 0.32 P < 0.05 N.S.
Means, S.D. and stat is t ical analys is (Student N e u m a n . Keul 's). N.S..
not significant.
Table V1
Direct and mirror reversed Corsi test
Mean S.D. vs. cerebellar vs. mental
ret.
Cerebellar Direct 2.86 0.90 N.S.
Mirror 0.43 0.79 N.S.
reversed
Mental ret. Direct 3.20 1.64 N.S.
Mirror 0.40 0.89 N.S.
reversed
Normal Direct 3.83 0.75 N.S. N.S.
Mirror 2.17 1.33 P<0 .05 P<0.05
reversed
Means. S.D. and stat is t ical analysis (Student Neuman Keul's). N.S.,
not significant.
and neuroradiological findings. The early onset, non-progressive syndrome consists
of: (i) cerebellar neurological signs, varying in severity, with a moderate impairment of motor development; (ii) mild mental retardation, particularly involving some skills (performance subtests, adaptive process to sen- sory conflicts) and some cognitive prerequisites like the speed of information processing; (iii) either spora- dic or familial occurrence, consistent with an autosomal recessive inheritance pattern.
In our 7 cases this syndrome was confirmed by neu- roimaging findings• All the patients showed a diffuse cortical atrophy with wide and deep interfolia sulci evi- dent in both the vermis and hemispheres, and an over- all size reduction of the cerebellum with no brainstem involvement. No supratentorial changes were evident. Serial assessments in one patient did not show any ap-
442 Brain & Development, Vol 15, No 6, 1993
parent progression of the imaging changes. A pathological definition of these findings is not easy
and is only speculative. Cortical dysplasia due to an early degeneration and/or necrosis of migrating gran- ule cells, like that shown by the patients of Norman [9] and Jervis [10] can be proposed. A primary defect of the Bergman glia guiding the inward migration of granule cells with their consequent death was suggested, as de- monstrated in the Weaver mutant mouse, an excellent example of cerebellar dysplasia with predominant changes of the granule cells [25]. Following the hypoth- esis that there is diffuse neuronal death at the base of the disease, we prefer to use the denomination of cere- bellar atrophy rather than hypoplasia.
Whatever the pathological interpretation, neuroima- ging seems to distinguish our cases from those with dominant inheritance [15 17,19,26]. In the latter only the involvement of the vermis is reported, and above all that of the anterior part of cerebellar vermis [15- 17,26].
The only cases we know of dominant inheritance, showing neuroimaging findings similar to ours, are those reported by Kornberg and Shields [27] and by Ruggeri et al. [28]. Nevertheless, in all these cases with dominant inheritance, there was no evidence of cogni- tive impairment.
On the contrary, our cases presenting an autosomal recessive inheritance, like the few others with similar findings described in the literature [2,9-12], show mild developmental delay and mild mental retardation. These findings allow them to be distinguished from cases with other likewise inherited syndromes reported in the literature. Hagberg et al. [4] showed a form of fixed cerebellar congenital syndrome, named disequili- brium syndrome, and proposed a possible genetic ori- gin with an autosomal recessive inheritance. Peculiar findings in their cases were a severe motor impairment with a marked delay in acquisition of the first motor milestones, and a generally severe mental retardation. A superior-anterior vermis atrophy seems characteris- tic of this syndrome [29].
A marked developmental delay was also generally found in the Joubert syndrome, another characteristic genetic cerebellar malformation with dysgenesis of the vermis, frequently associated with hypoplasia of the brainstem. Clinical findings include sporadic respira- tory disturbances, abnormal eye movements and atax- ia. The inheritance of this syndrome is autosomal and recessive [1,30]. Another more complex autosomal re- cessive syndrome was described where cerebellar, namely vermal hypoplasia, is associated with several
systemic clinical findings (short stature, endosteal sclerosis, microcephaly and hip dislocation) [31,32]. Fi- nally, generally more severe and heterogeneous clinical and neuroimaging findings were reported by Young et al. [33] in their familial cases of congenital ataxia with sex-linked recessive inheritance.
The impairment of the cognitive development in our patients with congenital cerebellar syndromes and no apparent supratentorial changes raises the problem of the relationship between the cerebellum and mental skills.
Some authors [13], in an attempt to explain the asso- ciation of cerebellar atrophy, language disorders and mental retardation, suggest the possibility that a single event could be responsible for the involvement of dif- ferent regions. The various degrees of impairment could be due to the different chronological rates of development of the cerebellar and brain cortex, the mi- gration and development of the granular layer cells of the cerebellum occurring later than those of cortical cells. Thus, a late injury could be responsible for the morphological and functional changes in the develop- ing cerebellar structures. The same event would not cause any major morphological changes in brain corti- cal cells, detectable with neuroradiological investiga- tions, but only minor disorders which, however, could still cause functional abnormalities.
On the other hand, there is growing evidence that the cerebellum participates in some cognitive processes, like motor learning [22], speed of information processing [34], associative learning of motor and non-motor tasks [35-40], time interval perception [41,42], cogni- tive planning [43].
The low degree of cognitive impairment found in our patients, allowed us to perform some neuropsychologi- cal tests in order to detect specific deficits in mental skills. The area of perceptual and motor organization for any concrete task seems particularly involved, as shown by the results of the Wechsler test (PIQ defi- nitely lower than VIQ), with the lowest scores in some items (arithmetic, mazes, object symbol, black design). The speed of information processing was always very low, even in comparison with the mentally retarded control group, matched for age and IQ, thus confirm- ing the results of a study on a sample of patients with pure CBS atrophy [34].
Short-term memory for sequential movements does not seem to be involved, but the adaptive process fol- lowing the mirror-reversed test was impaired, as it was in the mentally retarded group, suggesting a dysfunc- tion in re-making up the cognitive plan as a representa-
Brain & Development, Vol 15, No 6, 1993 443
tion of a series of temporal integrated movements in a unitary sequence [44].
The function of cerebellum in the cerebellar-frontal axis in order to perform the cognitive planning is un- clear [45], however, these results provide some points in favour of the role of the cerebellum in the cognitive development of infants and young children. The deficit of the adaptive processes in motor learning could im- pair the mechanisms of the motor scheme integration, which is at the basis of the beginning of mental devel- opment, according to Piaget's theory. Obviously, more pathological studies are required to support this specu- lation. The occurrence of minor supratentorial changes, not visible with the usual neuroimaging techniques, should be excluded.
ACKNOWLEDGEMENTS
This research was supported by an Italien CNR grant (no.
91.00267.04).
REFERENCES
I. Joubert M, Eisenring J, Robb JP, Andermann F. Familial agen- esis of the cerebellar vermis. Neurology (Minneapolis) 1969; 19:
813-25. 2. Lesny 1. Symmetrical hypogenesis of the cerebellum. Aeta Neurol
Scand 1970; 46:642 7.
3. Weiner MD, Konigsmark BW. Hereditary diseases of the cerebel- lar parenchyma. Birth De['ects: Original Article Series 1971: 7:
192 6. 4. Hagberg B, Sanner G, Steen M. The disequilibrium syndrome in
cerebral palsy. Acta Paediatr Seand 1972; 61 (Suppl 226).
5. Friede RL. Uncommon syndromes of cerebellar vermis aplasia. 1I. Tecto-cerebellar dysraphia with occipital encephalocele. Dev Med Child Neurol 1978; 20:764 72.
6. Sarnat HBH, Alcala H. Human cerebellar hypoplasia: a syn-
drome of diverse cause. Arch Neurol 1980; 37: 300-5. 7. Clement MC, Briard ML, Ponsot G, Arthuis M. Ataxies cerebel-
leuse cong~nitale non-progressive. Arch Fr P~diatr 1984; 41:695
700. 8. Miller G, Cala LA. Ataxic cerebral palsy: clinico-radiologic cor-
relations. Neuropediatrics 1989; 20: 84~9. 9. Norman RM. Primary degeneration of granular layer of cerebel-
lum, an unusual form of familial cerebellar atrophy occurring in
early life. Brain 1940; 63:365 70. 10. Jervis GA. Early familial cerebellar degeneration. J Nerv Ment
Dis 1950: 111: 398~407. 11. Wichman A, Frank LM, Kelly TE. Autosomal recessive congeni-
tal cerebellar hypoplasia. Clin Genet 1985; 27:373 82. 12. Mathews KD, Afifi AK. Hanson JW. Autosomal recessive cere-
bellar hypoplasia. J Child Neurol 1989: 4:189 94. 13. Lyon G, Gadisseux GF. Structural abnormalities of the brain in
developmental disorders. In: Rutter M, Casaer P, eds. Biological risk factors .['or psychosocial disorders. Cambridge: Cambridge University Press, 1991:1 19.
14. McKusick VA. Mendelian inheritance in man, 8th ed. Baltimore: Johns Hopkins Press, 1988: 54.
15. Furman JM, Baloh RW, Chugani H, Waluch V, Bradley WG.
Infantile cerebellar atrophy. Ann Neurol 1985; 17: 399402.
16. Tomiwa K, Baraitser M, Wilson J. Dominantly inherited conge- nital cerebellar ataxia with atrophy of the vermis. Pediatr Neurol
1987; 3: 36(~2.
17. Rivier F, Echenne B. Dominantly inherited hypoplasia of the vermis. Neuropediatrics 1992: 23: 2068 .
18. Malamud N, Cohen P. Unusual form of cerebellar ataxia with sex linked inheritance. Neurology (Minneapolis) 1958; 8:261 6.
19. Fenichel GM, Phillips JA. Familial aplasia of the cerebellar ver- mis. Arch Neurol 1989; 46:582 3.
20. Bracke-Tolkmitt R, Linden A, Canavan AGM, et al. The cere-
bellum contributes to mental skills. Behav Neurosci 1989; 103: 442 6.
21. Leiner HC, Leiner AL, Dow RS. Reappraising the cerebellum:
what does the hindbrain contribute to the forebrain? Behav Neu-
rosci 1989~ 103:998 1008. 22. Sanes JN, Dimitrov B, Hallett M. Motor learning in patients
with cerebellar dysfunction. Brain 1990; 113:103 20. 23. Milner B. Interhemispheric differences in the localisation of psy-
chological process in man. Br Med Bull 1971: 27:272 7.
24. Glanz AS. II caso speciale di due gruppi:il test t. In: Glantz SA, ed. Statistica per discipline biomediche. Milano: McGraw Hill
Italia, 1987:82 6. 25. Rakic P, Sidman R. Sequence of developmental abnormalities
leading to granular cell deficit in the cerebellar cortex of weaver mutant mice. J Comp Neurol 1973: 152:103 32.
26. Kattah JC, Kolsky MP, Guy J. Primary position vertical nystag-
mus and cerebellar ataxia. Arch Neurol 1983; 40: 31(~ 4.
27. Kornberg A J, Shields LK. An extended phenotype of an early- onset inherited non-progressive cerebellar ataxia syndrome. J Child Neurol 1991; 6:20 5.
28. Ruggeri V. Ataxie c6r+belleuse congenitale autosomique domi-
nante, avec hypoplasie du cervelet et quotient intellectuel nor- mal. Proc. 20~me R~'union Soci~t~; Europ~enne de Neurologie Pgdiatrique, Bruxelles, 4 7 Dec 1991.
29. Sanner G. The disequilibrium syndrome. Neuropaediatrie 1973; 4: 403 13.
30. Kendall B, Kingsley D, Lambert SR, Taylor D, Finn P. Joubert
syndrome: a clinico-radiological study. Neuroradiology 1990; 31: 502 6.
31. Stoll C, Talon P, Alembik J, Levy JM. Hypoplasie c6r~belleuse congenitale avec lesions osseuses. Ann Pediatr 1986; 33:417 21.
32. Charrow J, Poznanski AK, Unger FM, Robinow M. Autosomal recessive cerebellar hypoplasia and endosteal sclerosis: a newly recognized syndrome. Am J Med Genet 1991: 41 :464 8.
33. Young ID, Moore JRT, Tripp JH. Sex-linked recessive congeni- tal ataxia. J Neurol Neurosurg Psychiatry 1987: 50:1230 2.
34. Botez MI. Botez T, Elie R, Attig E. Role of the cerebellum in
complex human behavior, ltal J Neurol Sci 1989; 10:291 300. 35. Lye RH, O'Boyle D J, Ramdsen RT, Schady W. Effects of a
unilateral cerebellar lesion on the acquisition of eye-blink condi- tioning in man. J Physiol 1988: 403: 58.
36. Moore JW, Berthier NE. Purkinje cell activity and the condi- tioned nictitating membrane response. In: Glickstein M, Yeo C, Stein .I., eds. Cerebellum and neuronal plasticity. New York: Ple- num Press, 1987:339 52.
37. Yeo C. Cerebellum and classical conditioning. In: Glickstein M, Yeo C, Stein J, eds. Cerebellum and neuronal plasticiO,. New York: Plenum Press, 1987:321 38.
38. Thompson RF. The neural basis of basic associative learning of discrete behavioural responses. Trends Neurosci 1988:11 : 152 5.
444 Brain & Development, Vol 15, No 6. 1993

39. Watson PJ. Nonmotor functions of the cerebellum. Psychol Bull 1978; 85: 944~7.
40. Leiner HC, Leiner AL, Dow RS. Does the cerebellum contribute to mental skills? Behav Neurosci 1986; 100: 443-54.
41. Leiner HC, Leiner AL, Dow RS. Cerebro-cerebellar learning loops in apes and humans, ltal J Neurol Sci 1987; 8: 425-36.
42. Ivry RB, Keele SW, Diener HC. Dissociation of the lateral and medial cerebellum in movement timing and movement execution. Exp Brain Res 1988; 73: 167-80.
43. Grafman J, Litvan I, Massaquoi M, et al. Cognitive planning deficit in patients with cerebellar atrophy. Neurology 1992; 42: 1493-6.
44. Ito M. A new physiological concept on cerebellum. Rdv Neurol (Paris) 1990; 146: 564-9.
45. Decety J, Sjoholm H, Ryding E, Stenberg G, Ingvar DH. The cerebellum participates in mental activity: tomographic measure- ments of regional cerebral blood flow. Brain Res 1990; 535: 313- 7.
Brain & Development, Vol 15, No 6, 1993 445











![Ataxia telangiectasia: a reviewataxia, oculocutaneous telangiectasia and frequent pul-monary infection [1]. Definition A-T is an autosomal recessive cerebellar ataxia [2]. It has also](https://img.pdfslide.net/doc/110x75/60c0274fdc425b48211dfd10/ataxia-telangiectasia-a-review-ataxia-oculocutaneous-telangiectasia-and-frequent.jpg)

















