Embed Size (px)
Citation preview
Case ReportManagement of Sjogren’s Syndrome Patient: A Case Report ofProsthetic Rehabilitation with 6-Year Follow-Up
Marcos de Mendonça Invernici,1 Amanda Finger Stadler,2
Gastão Vale Nicolau,3 Maria Ângela Naval Machado,3
Antônio Adilson Soares de Lima,3 and Marilia Compagnoni Martins3
1 School of Dentistry, Department of Oral Surgery and Periodontics, Sao Paulo University, Avenida do Cafe, s/n, Monte Alegre,14040-904 Ribeirao Preto, SP, Brazil
2 School of Dentistry, Department of Conservative Dentistry, Federal University of Rio Grande do Sul, Rua Ramiro Barcelos 2492,90035-003 Porto Alegre, RS, Brazil
3 Department of Stomatology, Federal University of Parana, Campus Botanico, Avenida Prefeito Lothario Meissner 632,80210-170 Curitiba, PR, Brazil
Correspondence should be addressed to Marilia Compagnoni Martins; [email protected]
Received 8 August 2014; Accepted 22 October 2014; Published 13 November 2014
Academic Editor: Pia Lopez Jornet
Copyright © 2014 Marcos de Mendonca Invernici et al. This is an open access article distributed under the Creative CommonsAttribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work isproperly cited.
Completely and partially edentulous patients with Sjogren’s syndrome (SS) experience severe hyposalivation, xerostomia, andconsiderable difficulty in using tissue-supported prosthesis. This clinical paper describes the management, treatment, and 6-yearfollow-up of a patient diagnosed with SS type II, who uses corticosteroids and antihyperglycemic drugs. The patient receivedrestorative, periodontal, and surgical treatments followed by implant-supported fixed prosthesis. Radiographic evaluation andprobing depth showed gingival health and no bone loss after 6 years. Treatment with implant-retained dental prosthesis greatlyincreased comfort and function, offering an alternative to patients with SS.
1. Introduction
Dental implants, as treatment in edentulous areas, havebecome a standard of care in the last decade. Although theliterature presents many references as contraindications ofthis type of treatment in patients with systemic diseases, thebenefits of treatment with dental implants in such patientsmight outweigh the risks [1].
Sjogren’s syndrome (SS) is a systemic autoimmune disor-der that affects the exocrine glands, particularly the salivaryand lacrimal glands. The syndrome is characterized by thepresence of an inflammatory infiltrate of lymphocytes inter-fering with the function of the glands confirmed by a biopsyof the labial gland. There are two clinical forms of SS. Theprimary form is characterized by dry eye conjunctiva andhyposalivation and the secondary formoccurs in conjunctionwith other connective tissue diseases such as rheumatoidarthritis and lupus erythematosus [1, 2]. SS affects 0.5–3% of
the population and is more prevalent in women than in men(9 : 1) [3]. It is usually diagnosed during the fifth decade of lifebut can affect all age groups [4, 5].
Oral implications of SS are hyposalivation, xerostomia,inflamed and burning oral mucosa, rampant caries, sclerosisor growth of parotid gland, frequent manifestation of erythe-matous candidosis, angular cheilitis, increased plaque reten-tion, and difficulty in swallowing [6, 7]. Due to xerostomiaand burning of the oral mucosa, patients with SS experi-ence great discomfort and pain when wearing traditionalremovable prostheses.There is no definitive treatment for SS.Alternative therapies, such as use of lubricants and artificialsaliva, increased fluid intake, and salivary stimulation, areused to relieve the symptoms. However, these treatments arepalliative and the use of removable implant-retained dentalprosthesis could help to relieve the discomfort in the patients.
Literature presents six case reports with SS patientstreated with dental implants [8–13]. Moreover, there are few
Hindawi Publishing CorporationCase Reports in DentistryVolume 2014, Article ID 761251, 5 pageshttp://dx.doi.org/10.1155/2014/761251
2 Case Reports in Dentistry
reports in the literature about clinical long-term follow-up ofthis type of treatment [9].The aim of this paper is to describea case report of a patientwith SS type II that required implant-supported fixed prosthesis treatment.
2. Clinical Report
A 58-year-old female was referred to the PeriodontologyOutpatient Clinic of Federal University of Parana DentalSchool, Brazil, to receive periodontal treatment and to installdental implants in areas equivalent to the superior rightpremolar teeth, in August 2008.
During anamnesis, the patient reported that she had beendiagnosed with SS in 1989, after the appearance of somesymptoms, such as xerostomia and xerophthalmia. Duringthe same year, rheumatoid arthritis was also diagnosed. Shestarted the use of corticosteroids prednisone, 20mg daily,in order to control inflammation and pain. The disease hasbeen controlled ever since. In 2006, the patient was diagnosedwith type II diabetes mellitus and began the use of anoral hypoglycemic drug (sulfonylurea 80mg) andmetforminhydrochloride (500mg) to control blood glucose. Anotherpiece of information recorded in the preliminary case historywas that the patient stopped smoking right after receivingthe SS diagnosis. Besides medication, the patient related theuse of eye drops and water day and night to keep her eyesand mouth moist. The report included dryness of the vaginalmucosa, hands, and feet.
The main complaint of the patient was lack of adaptationin using a partially removable dental prosthesis. Duringthe intraoral examination it was observed that an implantreplaced the central right incisive tooth, and several decayedteeth were noted (first quadrant: canine, first premolar, andthird molar; second quadrant: canine and second molar;third quadrant: first premolar; and fourth quadrant: canineand first premolar) as well as missing teeth (first quadrant:first and second molar; second quadrant: first and secondpremolar and first and third molar; and third and fourthquadrants: from second premolar to third molar). Indicationfor endodontic treatment was observed for the lateral leftupper incisive tooth and first left lower premolar tooth. Thesecond right upper premolar had a ceramic crown witha metal core (Figure 1). The patient was also diagnosedwith generalized chronic periodontitis. An initial panoramicradiograph was taken (Figure 2). Salivary flow rate wasperformed and the result was 0.1mL/minute. The patientagreed to participate in the study by signing an informedconsent form.
After diagnosis, a treatment plan was established torehabilitate the patient with restorative and endodontic pro-cedures, nonsurgical periodontal treatment, osseointegratedimplants, and prosthesis. Due to the patient reporting a lackof adaptation with the removable prosthesis it was decided totry an implant-supported fixed prosthesis.
In October 2008 the patient was submitted to a nonsur-gical periodontal treatment at the periodontology outpatientclinic. One month later, two titanium implants (SysthexSistema de Implantes Osseointegrados Ltda., Curitiba, Brazil)
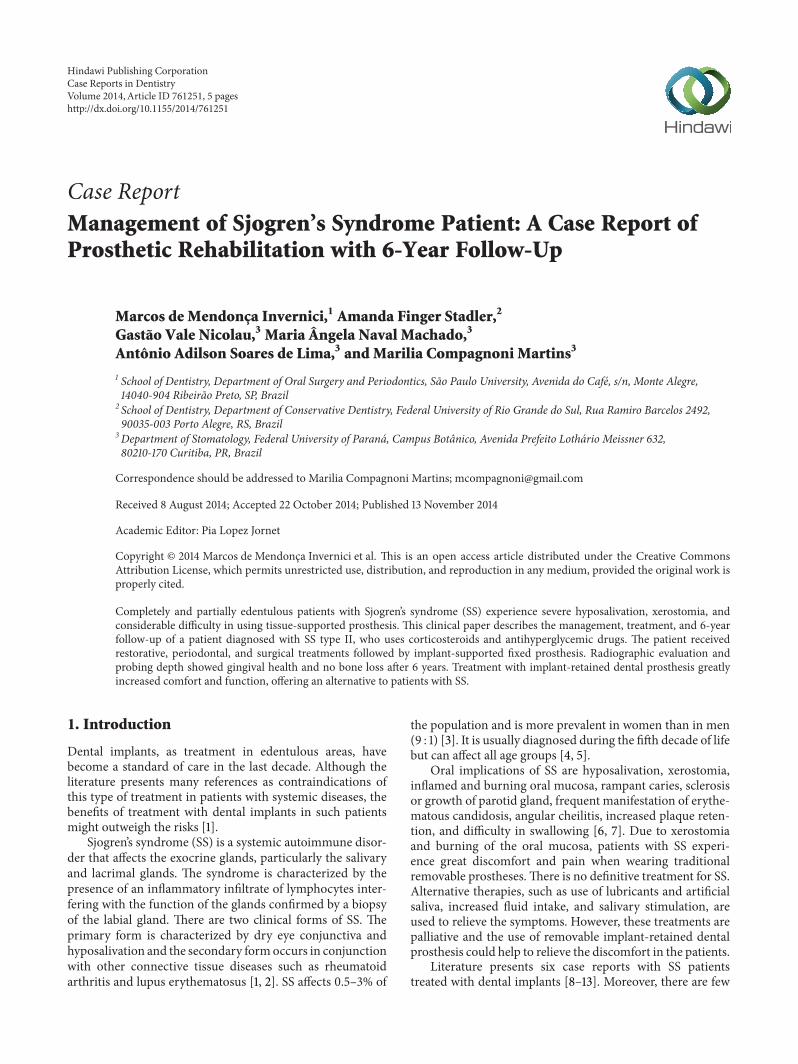
Figure 1: Initial clinical view of the patient with Sjogren’s syndrome(August 2008).
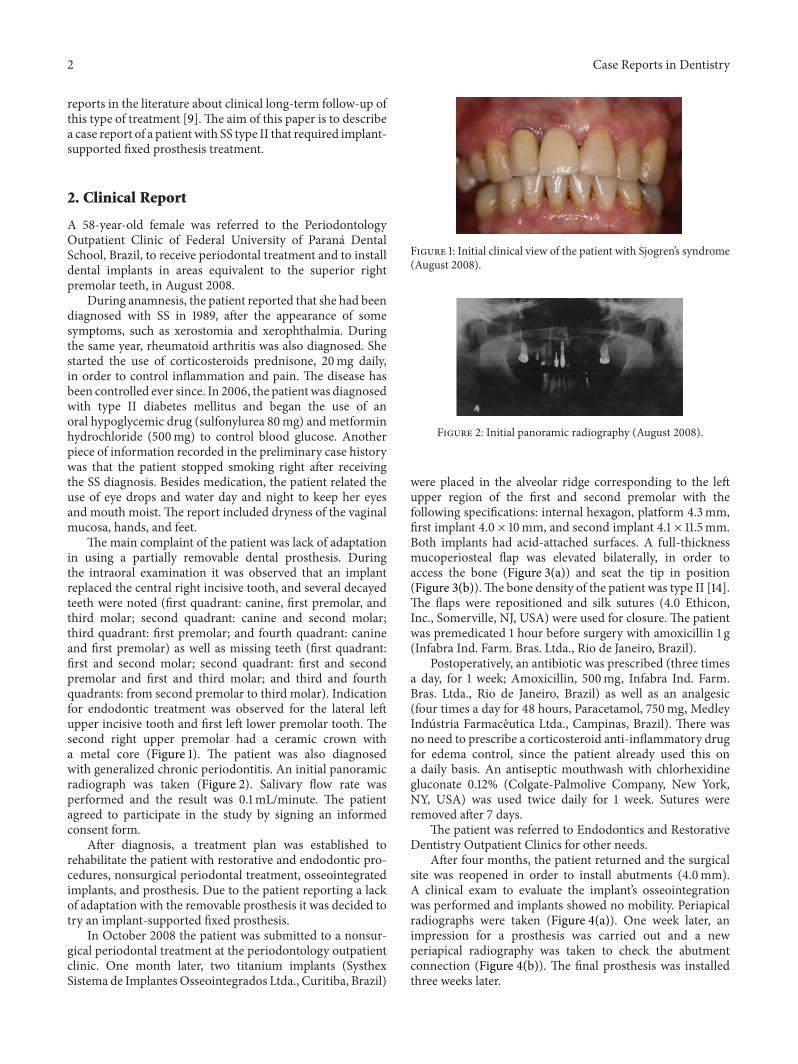
Figure 2: Initial panoramic radiography (August 2008).
were placed in the alveolar ridge corresponding to the leftupper region of the first and second premolar with thefollowing specifications: internal hexagon, platform 4.3mm,first implant 4.0 × 10mm, and second implant 4.1 × 11.5mm.Both implants had acid-attached surfaces. A full-thicknessmucoperiosteal flap was elevated bilaterally, in order toaccess the bone (Figure 3(a)) and seat the tip in position(Figure 3(b)).The bone density of the patient was type II [14].The flaps were repositioned and silk sutures (4.0 Ethicon,Inc., Somerville, NJ, USA) were used for closure. The patientwas premedicated 1 hour before surgery with amoxicillin 1 g(Infabra Ind. Farm. Bras. Ltda., Rio de Janeiro, Brazil).
Postoperatively, an antibiotic was prescribed (three timesa day, for 1 week; Amoxicillin, 500mg, Infabra Ind. Farm.Bras. Ltda., Rio de Janeiro, Brazil) as well as an analgesic(four times a day for 48 hours, Paracetamol, 750mg, MedleyIndustria Farmaceutica Ltda., Campinas, Brazil). There wasno need to prescribe a corticosteroid anti-inflammatory drugfor edema control, since the patient already used this ona daily basis. An antiseptic mouthwash with chlorhexidinegluconate 0.12% (Colgate-Palmolive Company, New York,NY, USA) was used twice daily for 1 week. Sutures wereremoved after 7 days.
The patient was referred to Endodontics and RestorativeDentistry Outpatient Clinics for other needs.
After four months, the patient returned and the surgicalsite was reopened in order to install abutments (4.0mm).A clinical exam to evaluate the implant’s osseointegrationwas performed and implants showed no mobility. Periapicalradiographs were taken (Figure 4(a)). One week later, animpression for a prosthesis was carried out and a newperiapical radiography was taken to check the abutmentconnection (Figure 4(b)). The final prosthesis was installedthree weeks later.
Case Reports in Dentistry 3
(a) (b)
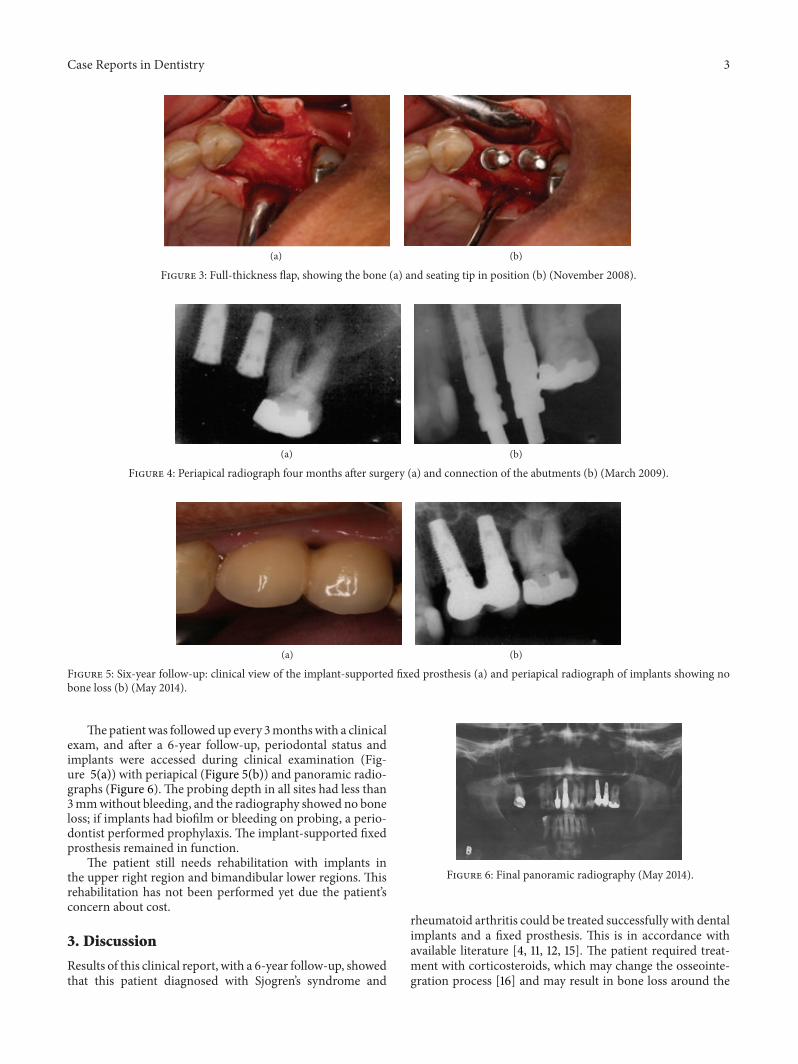
Figure 3: Full-thickness flap, showing the bone (a) and seating tip in position (b) (November 2008).
(a) (b)
Figure 4: Periapical radiograph four months after surgery (a) and connection of the abutments (b) (March 2009).
(a) (b)
Figure 5: Six-year follow-up: clinical view of the implant-supported fixed prosthesis (a) and periapical radiograph of implants showing nobone loss (b) (May 2014).
Thepatientwas followed up every 3monthswith a clinicalexam, and after a 6-year follow-up, periodontal status andimplants were accessed during clinical examination (Fig-ure 5(a)) with periapical (Figure 5(b)) and panoramic radio-graphs (Figure 6).The probing depth in all sites had less than3mmwithout bleeding, and the radiography showed no boneloss; if implants had biofilm or bleeding on probing, a perio-dontist performed prophylaxis. The implant-supported fixedprosthesis remained in function.
The patient still needs rehabilitation with implants inthe upper right region and bimandibular lower regions. Thisrehabilitation has not been performed yet due the patient’sconcern about cost.
3. Discussion
Results of this clinical report, with a 6-year follow-up, showedthat this patient diagnosed with Sjogren’s syndrome and
Figure 6: Final panoramic radiography (May 2014).
rheumatoid arthritis could be treated successfully with dentalimplants and a fixed prosthesis. This is in accordance withavailable literature [4, 11, 12, 15]. The patient required treat-ment with corticosteroids, which may change the osseointe-gration process [16] and may result in bone loss around the

4 Case Reports in Dentistry
implants [11]. However, during follow-up, no complicationswere diagnosed in the repair process, and the level of crestalbone around implants remained unchanged. This situationdiffers from that reported by Payne et al. [11], in which apatient with SS treated with cortisone therapy showed boneloss around the implants.
The patient also had a diagnosis of diabetes mellitus, andthe literature shows that there is a significant correlationbetween oral dryness and type II diabetes mellitus [17].A recent systematic review found a difference in statisticsbetween diabetic and nondiabetic patients, with regard tomarginal bone loss, with less bone loss for the nondiabeticpatients [18]. Nevertheless, this patient showed no bone lossduring the 6-year follow-up, despite the diagnosis of Sjogren’ssyndrome, rheumatoid arthritis, and diabetes mellitus.
Literature shows that patients with SS have difficultieswith eating, swallowing, and speaking and present a highprevalence of caries. A recent publication also found asignificant correlation between oral dryness and the qualityof sleep, anxiety, and depression [17]. Usually, these patientsreport regular dental visits over a long period of time and anincreased number of decayed teeth between visits, in spiteof good oral hygiene [2]. Tooth decay is accelerated as aresult of a reduction in salivary flow rate and the subsequentloss of saliva antibacterial properties in a dry mouth. In fact,unexplained rampant dental caries may be the first sign ofa dry mouth. The factors related to pathogenesis of dentalcaries in SS may be the loss of the salivary buffering capacityand the increased intake of cariogenic drinks [19]. Even withexcellent levels of oral hygiene, tooth decay and prematureloss are frequent in SS patients. It is not unusual for patientswith a more advanced disease to be edentulous or to havecomplete dentures [6, 8]. They also have a higher DMFT(decayed/missing/filled teeth) score compared to individualsin the control group [19]. In the present case report, thepatient presented at the initial exam showing several missingand decayed teeth. Severe caries activity might be the causeof early tooth loss.
Although the literature presents 6 papers [8–13] concern-ing SS patients treated with dental implants, no systematicinvestigations have yet been done to evaluate the influence ofSS and its effect on bone healing and remodeling after implantplacement [11]. Minimal long-term clinical documentationsalso exist in literature regarding this type of treatment [9].
Often the rehabilitation of patients with SS is neglectedand only symptomatic treatment is performed. As a resultof continuous hyposalivation, patients with SS consequentlyhave various dental treatments that fail.This explains why it isso complex to finish the research subject’s oral rehabilitationand the reason this patient remains in treatment. Manage-ment of SS requires multidisciplinary dental care, mainlyrestorative, endodontic, prosthetic, and implant rehabilita-tion. After care and rehabilitation it is necessary to maintaincontinuous follow-up over a long period of time.
One reason motivating the treatment of patients with SSwith dental implants is that they have difficulty in adaptingto removable partial dentures, due to hyposalivation and,in some cases, the report of the sensation of a burningmouth. There are no published articles about the immediate
prosthetic loading in patients with SS. This was the mainreason why the authors decided to use a 2-stage implanttreatment, with prosthetic loading after 5 months.
4. Conclusion
Within the limitations of this case report, we can suggestthat it is possible to treat partial edentulous patients withSjogren’s syndrome associated with rheumatoid arthritis anddiabetes, using corticosteroids and oral hyperglycemic ther-apy with dental implants and fixed prosthesis. This treatmentimproved the patient’s comfort and showed no bone loss after6 years. Therefore, more studies are needed to validate theeffects of the implant therapy and fixed prosthesis in patientswith Sjogren’s syndrome.
Consent
Thepatient signed an informed consent formagreeing to haveher case reported.
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper.
References
[1] C. Scully and M. Carrozzo, “Oral mucosal disease: lichenplanus,” British Journal of Oral and Maxillofacial Surgery, vol.46, no. 1, pp. 15–21, 2008.
[2] R. Fox and F. Howell, “Oral problems in patients with Sjogren’ssyndrome,” Scandinavian Journal of Rheumatology, vol. 15, no.61, pp. 194–200, 1986.
[3] M. Margaix-Munoz, J. V. Bagan, R. Poveda, Y. Jimenez, and G.Sarrion, “Sjogren’s syndrome of the oral cavity. Review andupdate,” Medicina Oral, Patologia Oral y Cirugia Bucal, vol. 14,no. 7, pp. E325–E330, 2009.
[4] R. K. Akin, A. J. Kreller III, P. J. Walters, and J. S. Trapani, “Sjo-gren’s syndrome,” Journal of Oral Surgery, vol. 33, no. 1, pp. 27–33, 1975.
[5] J. C. Atkinson and P. C. Fox, “Sjogren’s syndrome: oral anddental considerations.,” The Journal of the American DentalAssociation, vol. 124, no. 3, pp. 74–78, 1993.
[6] S. Carsons, “A review and update of Sjogren’s syndrome: man-ifestations, diagnosis, and treatment,” The American Journal ofManaged Care, vol. 7, no. 14, pp. S433–S443, 2001.
[7] T. E.Daniels, “Clinical assessment anddiagnosis of immunolog-ically mediated salivary gland disease in Sjogren’s syndrome,”Journal of Autoimmunity, vol. 2, no. 4, pp. 529–541, 1989.
[8] F. Isidor, K. Brøndum, H. J. Hansen, J. Jensen, and S. Sindet-Pedersen, “Outcome of treatment with implant-retained dentalprostheses in patients with Sjogren syndrome,” The Interna-tional Journal of Oral & Maxillofacial Implants, vol. 14, no. 5,pp. 736–743, 1999.
[9] P. P. Binon, “Thirteen-year follow-up of a mandibular implant-supported fixed complete denture in a patient with Sjogren’ssyndrome: a clinical report,” Journal of Prosthetic Dentistry, vol.94, no. 5, pp. 409–413, 2005.

Case Reports in Dentistry 5
[10] M. M. Bornstein, N. Cionca, and A. Mombelli, “Systemic con-ditions and treatments as risks for implant therapy,” The Inter-national Journal of Oral & Maxillofacial Implants, vol. 24, pp.12–27, 2009.
[11] A. G. T. Payne, J. F. Lownie, andW. J. van der Linden, “Implant-supported prostheses in patients with Sjogren’s syndrome: aclinical report on three patients,” International Journal of Oraland Maxillofacial Implants, vol. 12, no. 5, pp. 679–685, 1997.
[12] S. Spinato, C. M. Soardi, and A. M. Zane, “A mandibularimplant-supported fixed complete dental prosthesis in a patientwith sjogren syndrome: case report,” Implant Dentistry, vol. 19,no. 3, pp. 178–183, 2010.
[13] P. P. Binon and C. N. Fowler, “Implant-supported fixed pros-thesis treatment of a patient with Sjogren’s syndrome: a clin-ical report,” The International Journal of Oral & MaxillofacialImplants, vol. 8, no. 1, pp. 54–58, 1993.
[14] P. Trisi and W. Rao, “Bone classification: clinical—histomor-phometric comparison,”Clinical Oral Implants Research, vol. 10,no. 1, pp. 1–7, 1999.
[15] E. Theander and L. T. H. Jacobsson, “Relationship of Sjogren’ssyndrome to other connective tissue and autoimmune disor-ders,” Rheumatic Disease Clinics of North America, vol. 34, no.4, pp. 935–947, 2008.
[16] J.-H. Fu, J. D. Bashutski, K. Al-Hezaimi, and H.-L. Wang,“Statins, glucocorticoids, and nonsteroidal anti-inflammatorydrugs: their influence on implant healing,” Implant Dentistry,vol. 21, no. 5, pp. 362–367, 2012.
[17] M. Gandıa, E. M. Morales-Espinoza, R. M. Martın-Gonzalezet al., “Factors influencing dry mouth in patients with primarySjogren syndrome: usefulness of the ESSPRI index,”Oral Healthand Dental Management, vol. 13, no. 2, pp. 402–407, 2014.
[18] B. R. Chrcanovic, T.Albrektsson, andA.Wennerberg, “Diabetesand oral implant failure: a systematic review,” Journal of DentalResearch, 2014.
[19] A. J. Carr, W.-F. Ng, F. Figueiredo, R. I. MacLeod, M. Green-wood, and K. Staines, “Sjogren’s syndrome—an update fordental practitioners,” British Dental Journal, vol. 213, no. 7, pp.353–357, 2012.
Submit your manuscripts athttp://www.hindawi.com
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oral OncologyJournal of
DentistryInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
International Journal of
Biomaterials
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Case Reports in Dentistry
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oral ImplantsJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Anesthesiology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Radiology Research and Practice
Environmental and Public Health
Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Dental SurgeryJournal of
Drug DeliveryJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oral DiseasesJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
ScientificaHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PainResearch and TreatmentHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Preventive MedicineAdvances in
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
OrthopedicsAdvances in