Embed Size (px)
Citation preview

Journal of The Association of Physicians of India ■ Vol. 64 ■ August 2016 79
C A S E O F T H E M O N T H
Cerebellar Toxoplasmosis in an Immunocompetent Patient with G6PD DeficiencyRishit K Harbada1, Jehangir S Sorabjee2, Nirmal Surya3, Kishor A Jadhav3, Sumeet Mirgh4
1Senior Resident, 2Professor and Head, Department of Medicine, 3Neurologist, Department of Neurology, Bombay Hospital Institute of Medical Sciences, Mumbai, Maharashtra; 4Senior Resident, Department of Clinical Hematology, All India Institute of Medical Sciences, New DelhiReceived: 12.06.2016; Accepted: 22.06.2016
Introduction
To x o p l a s m a g o n d i i , a n u b i q u i t o u s i n t r a c e l l u l a r
parasi te , i s the most common protozoan infections in humans.1
Toxoplasma antibodies are present in near ly 30% of the genera l population with a wide variation ranging from 6 to 90%. Most of the infections are subclinical, but overt and fatal central nervous i n f e c t i o n s o c c u r m a i n l y i n immunocompromised patients with HIV/AIDS and malignancies.G6PD deficient individuals are more predisposed to various bacterial and protozoan infections due to defective neutrophil killing effect.2 We report a case of cerebellar toxoplasmosis masquerading as posterior fossa malignant tumor in a G6PD deficient immunocompetent male. There have been few cases of toxoplasmosis in immunocompetent individuals especially with G6PD deficiency.
Case Report and Discussion
A 23 year-old businessman, residing in a metropolitan city of Oman, was referred to our hospital with a two week history
tendency to fall to the right, and dysgraphia. There were no signs of cranial neuropathy or meningeal irritation. A clinical diagnosis of a right sided cerebellar lesion was made.
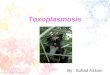
The differential diagnosis of acute to sub acute focal Ipsilateral cerebellar ataxia being 1) Neoplastic- glioma or metastatis, 2) Infectious-A b s c e s s 3 ) D e m y e l i n a t i o n -Multiple sclerosis, AIDS related multifocal leukoencephalopathy 4)Vascular-Infarction, hemorrhage. A l l i n ve s t i g a t i o n s i n c l u d i n g r o u t i n e h a e m o g r a m , b l o o d biochemistry and HIV serology were unremarkable .MRI brain T2 weighted images and FLAIR sequences revealed i l l defined low signal intensit ies in r ight cerebellum and brachium pontis causing mild midline shift and a ring of restricted diffusion and minimal blood on GRE sequence. Post contrast T1 and T2 sequences revealed central enhancement with peripheral ring suggestive of malignant space occupying l e s i o n ( S O L) e t i o l o g y l i k e l y Ependymoma (Figure 1). For the same a neurosurgery reference was given. Patient underwent a sub-occipital craniotomy. During surgery, a f rozen sect ion was reported as necrotic cerebellar t issue. The patient underwent near total excision of the SOL and the tissue removed was sent
of weakness and incoordination of the r ight upper and lower extremities, five day history of generalized throbbing headache with visual blurring, photophobia and vomiting. There was no history of vert igo, a l tered sensorium, seizures, antecedent head trauma, ear discharge or febrile illness. He had no significant past medical history and no history of alcohol intake or smoking.
General examination revealed a pulse rate of 88 beats per minute and a blood pressure of 130/ 80 mmHg. There was no pyrexia , pal lor , jaundice or lymphadenopathy. Examination of cardiovascular, respiratory and abdominal systems was unremarkable. Neurological evaluat ion revealed an intac t sensorium with a scanning slurred speech and right sided nystagmus, dysmetria in both right upper and lower l imbs ( impaired f inger-nose test and heel-knee-shin test), right sided dysdiadochokinesia, broad-based (ataxic) gait with severely impaired tandem walk and
AbstractWe report a case of an immunocompetent patient who presented with a short history of unilateral cerebellar lesion later proven as toxoplasmosis on histopathology. The case highlights that patients with G6PD deficiency are more prone to develop fatal toxoplasma infections than those individuals with normal G6PD activity.

Journal of The Association of Physicians of India ■ Vol. 64 ■ August 201680
with a choking sensation in the throat. He had a weak gag reflex and a right sided sixth and seventh nerve palsy.
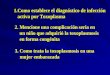
M e a n w h i l e , t h e f i n a l h i s t o p a t h o l o g y r e p o r t w a s suggestive of areas of cerebellum interspersed with necrosis and hemorrhage. Perivascular infiltrate of lymphocytes, glitter cells and pseudo-cysts of Toxoplasma gondii with evidence of cerebritis and encephalitis (Figure 2).
O u r p a t i e n t ’ s T o x o p l a s m a IgM was negative while IgG was positive. In view of histopathologic evidence of Toxoplasmosis, repeat HIV ELISA and HIV RNA PCR, to rule out immunocompromised status were negative. In acute infect ion, IgG and IgM levels rise during the first two weeks of infection. Elevation of Toxoplasma-specific IgG antibodies indicates infection, but does not discriminate between recent and past infection. A negative IgM with a positive IgG usually indicates infection of at least six months duration.3
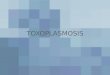
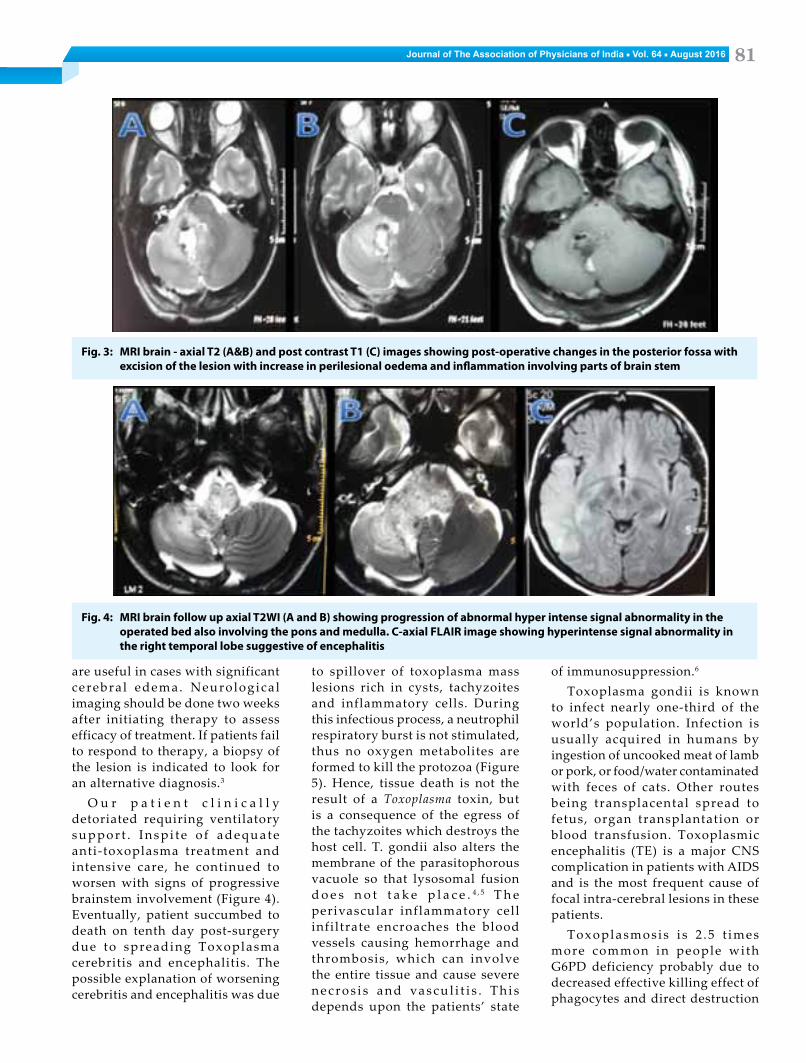
Before starting treatment, he was found to be G6PD deficient, hence he was started on Clindamycin 300 mg intravenous six hourly and Azithromycin 500 mg intravenous once da i ly . Repea t MRI scan done in view of his deteriorating neurological status revealed an increase in the perilesional edema and inflammation involving parts of the brain stem (Figure 3). In view of worsening MRI findings and clinical picture, steroid doses were increased.
Therapy with pyrimethamine a n d s u l f a d i a z i n e i s u s u a l l y effective in CNS toxoplasmosis. In pat ients wi th su l fadiaz ine intolerance either cl indamycin or atovaquone can be used in combination with pyrimethamine, continued for at least six weeks and if immune-suppression is present, s e c o n d a r y p r o p h y l a x i s w i t h trimethoprim/sulfamethoxazole or pyrimethamine/sulfadiazine is continued indefinitely. Steroids
Fig. 1: MRI brain Panel A- Axial T2 weighted image showing an ill-defined hyper intense lesion in right cerebellar hemisphere with perilesional oedema and extending along the right foramen of Luschka. Panel B, C, D- Post contrast T1 axial, coronal and saggital images showing heterogeneous post-contrast enhancement with peripheral enhancing ring
Fig. 2: Histopathological examination - Panel A, B, C, D- areas of cerebellum interspersed with necrosis and hemorrhage. Perivascular infiltrate of lymphocytes, glitter cells and pseudocysts (C) of Toxoplasma gondii with evidence of cerebritis and encephalitis
for detai led histopathological examination. Post operatively, patient was given ceftriaxone and amikacin along with tapering doses
of dexamethasone. He worsened with the taper ing of s tero ids on fourth day post-surgery. He developed difficulty in swallowing
Journal of The Association of Physicians of India ■ Vol. 64 ■ August 2016 81
Fig. 3: MRI brain - axial T2 (A&B) and post contrast T1 (C) images showing post-operative changes in the posterior fossa with excision of the lesion with increase in perilesional oedema and inflammation involving parts of brain stem
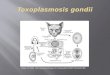
Fig. 4: MRI brain follow up axial T2WI (A and B) showing progression of abnormal hyper intense signal abnormality in the operated bed also involving the pons and medulla. C-axial FLAIR image showing hyperintense signal abnormality in the right temporal lobe suggestive of encephalitis
are useful in cases with significant cerebra l edema. Neurologica l imaging should be done two weeks after initiating therapy to assess efficacy of treatment. If patients fail to respond to therapy, a biopsy of the lesion is indicated to look for an alternative diagnosis.3
O u r p a t i e n t c l i n i c a l l y detoriated requiring ventilatory s u p p o r t . I n s p i t e o f a d e q u a t e anti-toxoplasma treatment and intensive care, he continued to worsen with signs of progressive brainstem involvement (Figure 4). Eventually, patient succumbed to death on tenth day post-surgery due to spreading Toxoplasma cerebritis and encephalitis. The possible explanation of worsening cerebritis and encephalitis was due
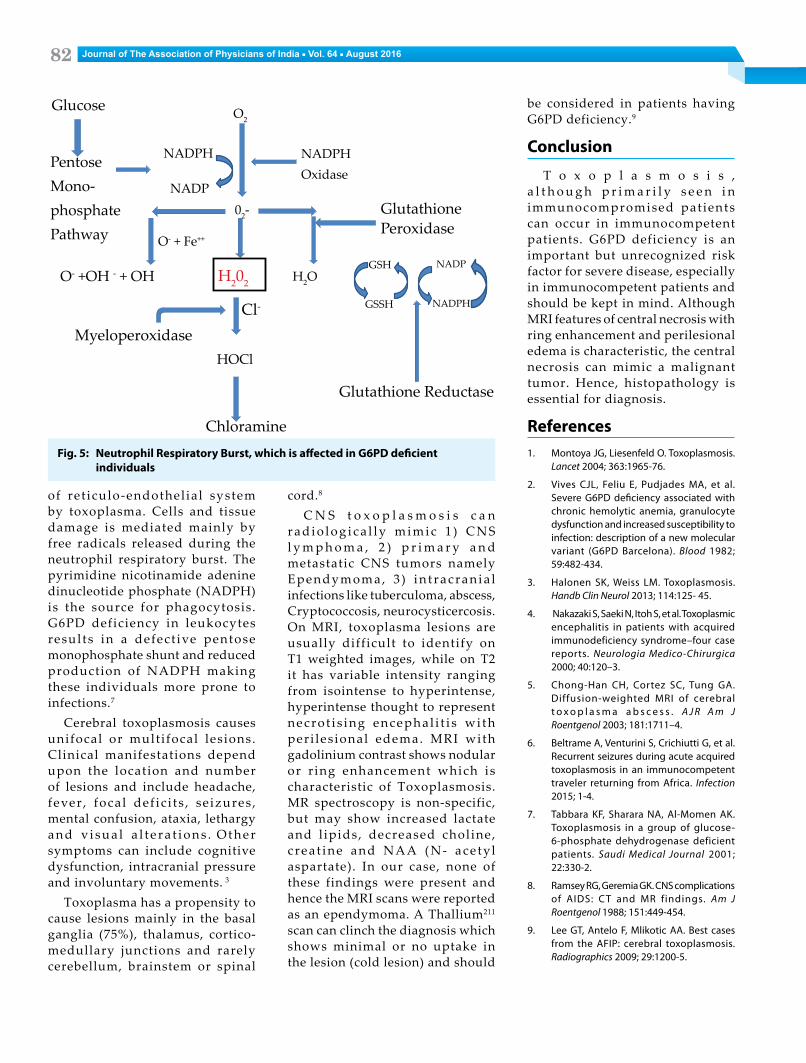
to spillover of toxoplasma mass lesions rich in cysts, tachyzoites and inflammatory cells. During this infectious process, a neutrophil respiratory burst is not stimulated, thus no oxygen metabolites are formed to kill the protozoa (Figure 5). Hence, tissue death is not the result of a Toxoplasma toxin, but is a consequence of the egress of the tachyzoites which destroys the host cell. T. gondii also alters the membrane of the parasitophorous vacuole so that lysosomal fusion d o e s n o t t a k e p l a c e . 4 , 5 T h e perivascular inflammatory cell infiltrate encroaches the blood vessels causing hemorrhage and thrombosis, which can involve the entire tissue and cause severe n e c r o s i s a n d va s c u l i t i s . T h i s depends upon the patients’ state
of immunosuppression.6
Toxoplasma gondii is known to infect nearly one-third of the world’s population. Infection is usually acquired in humans by ingestion of uncooked meat of lamb or pork, or food/water contaminated with feces of cats. Other routes being transplacental spread to fetus, organ transplantation or blood transfusion. Toxoplasmic encephalitis (TE) is a major CNS complication in patients with AIDS and is the most frequent cause of focal intra-cerebral lesions in these patients.
Toxoplasmosis i s 2 .5 t imes more common in people with G6PD deficiency probably due to decreased effective killing effect of phagocytes and direct destruction
Journal of The Association of Physicians of India ■ Vol. 64 ■ August 201682
of ret iculo-endothel ial system by toxoplasma. Cells and tissue damage is mediated mainly by free radicals released during the neutrophil respiratory burst. The pyrimidine nicotinamide adenine dinucleotide phosphate (NADPH) is the source for phagocytosis. G6PD deficiency in leukocytes results in a defect ive pentose monophosphate shunt and reduced production of NADPH making these individuals more prone to infections.7
Cerebral toxoplasmosis causes unifocal or multifocal lesions. Clinical manifestations depend upon the location and number of lesions and include headache, fever , focal def ic i ts , se izures , mental confusion, ataxia, lethargy a n d v i s u a l a l t e r a t i o n s . O t h e r symptoms can include cognitive dysfunction, intracranial pressure and involuntary movements. 3
Toxoplasma has a propensity to cause lesions mainly in the basal ganglia (75%), thalamus, cortico-medullary junctions and rarely cerebellum, brainstem or spinal
cord.8
C N S t o x o p l a s m o s i s c a n r a d i o l o g i c a l l y m i m i c 1 ) C N S l y m p h o m a , 2 ) p r i m a r y a n d metastatic CNS tumors namely Ependymoma, 3 ) in t racran ia l infections like tuberculoma, abscess, Cryptococcosis, neurocysticercosis. On MRI, toxoplasma lesions are usually difficult to identify on T1 weighted images, while on T2 it has variable intensity ranging from isointense to hyperintense, hyperintense thought to represent necrot i s ing encephal i t i s wi th peri les ional edema. MRI with gadolinium contrast shows nodular or r ing enhancement which is characteristic of Toxoplasmosis. MR spectroscopy is non-specific, but may show increased lactate and l ipids, decreased choline, c rea t ine and NAA (N- ace tyl aspartate). In our case, none of these findings were present and hence the MRI scans were reported as an ependymoma. A Thallium211 scan can clinch the diagnosis which shows minimal or no uptake in the lesion (cold lesion) and should
be considered in patients having G6PD deficiency.9
Conclusion
T o x o p l a s m o s i s , a l t h o u g h p r i m a r i l y s e e n i n immunocompromised patients can occur in immunocompetent patients. G6PD deficiency is an important but unrecognized risk factor for severe disease, especially in immunocompetent patients and should be kept in mind. Although MRI features of central necrosis with ring enhancement and perilesional edema is characteristic, the central necrosis can mimic a malignant tumor. Hence, histopathology is essential for diagnosis.
References1. Montoya JG, Liesenfeld O. Toxoplasmosis.
Lancet 2004; 363:1965-76.
2. Vives CJL, Feliu E, Pudjades MA, et al. Severe G6PD deficiency associated with chronic hemolytic anemia, granulocyte dysfunction and increased susceptibility to infection: description of a new molecular variant (G6PD Barcelona). Blood 1982; 59:482-434.
3. Halonen SK, Weiss LM. Toxoplasmosis. Handb Clin Neurol 2013; 114:125- 45.
4. Nakazaki S, Saeki N, Itoh S, et al. Toxoplasmic encephalitis in patients with acquired immunodeficiency syndrome–four case reports. Neurologia Medico-Chirurgica 2000; 40:120–3.
5. Chong-Han CH, Cortez SC, Tung GA. Diffusion-weighted MRI of cerebral t o x o p l a s m a a b s c e s s . A J R A m J Roentgenol 2003; 181:1711–4.
6. Beltrame A, Venturini S, Crichiutti G, et al. Recurrent seizures during acute acquired toxoplasmosis in an immunocompetent traveler returning from Africa. Infection 2015; 1-4.
7. Tabbara KF, Sharara NA, Al-Momen AK. Toxoplasmosis in a group of glucose-6-phosphate dehydrogenase deficient patients. Saudi Medical Journal 2001; 22:330-2.
8. Ramsey RG, Geremia GK. CNS complications of AIDS: CT and MR findings. Am J Roentgenol 1988; 151:449-454.
9. Lee GT, Antelo F, Mlikotic AA. Best cases from the AFIP: cerebral toxoplasmosis. Radiographics 2009; 29:1200-5.
Fig. 5: Neutrophil Respiratory Burst, which is affected in G6PD deficient individuals
Glucose
PentoseMono-phosphatePathway
NADPH
NADP
NADPHOxidase
GlutathionePeroxidase
GSH
GSSH
NADP
NADPH
Glutathione Reductase
Chloramine
MyeloperoxidaseHOCl
O2
H202 H2O
02-
Cl-
O- +OH - + OH
O- + Fe++
v
v
v
v
v