Embed Size (px)
Citation preview

ORIGINAL CONTRIBUTION spine, immobilization, pediatric
Cervical Spine Stabilization in Pediatric Patients: Evaluation of Current Techniques
We evaluated the performance of commercially available infant and pedi- attic cervical collars, both alone and in combination with commonly used supplemental devices (eg, Kendrick Extrication Device ®, half-spine board). One infant and I1 pediatric-sized collars were tested on mannequins repre- senting an infant and a 5-year old child. Maximum forces generated by co- operative children were measured, then applied to the mannequins to re- produce head and neck flexion, extension, rotation, and lateral motion. Limitation of motion was measured in each direction for each collar and combination method. In general, collars of rigid plastic construction per- formed better than did foam types. However, when used alone none of the collars provided acceptable immobilization, with even the best allowing 17 ° flexion, 19 ° extension, 4 ° rotation, and 6 ° lateral motion. When combined with supplemental devices, immobilization to 3 ° or less in any direction could be achieved. Findings were verified using cooperative children and selected collars. Overall, combination methods were more effective than cer- vical collars alone (P < .00I) or supplemental devices alone (P < .05). The modified half-spine board used with a rigid collar and tape was the most effective combination method. We conclude that prehospital cervical spine stabilization in pediatric patients is best accomplished using a rigid-type cervical collar in combination with supplemental devices as described. /Huerta C, Griffith R, foyce SM: Cervical spine stabilization in pediatric patients: Evaluation of current techniques. Ann Emerg Med October 1987; 16:1121-1126.]
INTRODUCTION Techniques for field stabilization of the cervical spine in pediatric patients
have not as yet been critically examined. Several recent studies have shown the effectiveness of rigid cervical collars combined with supplemental meth- ods in stabilizing the adult cervical spine.], 2 However, this information may not be applicable to pediatric patients due to significant differences in anato- my, size, and equipment design. A review of our experience with pediatric trauma victims over the past two years showed that prophylactic cervical spine stabilization was often performed inadequately, both in the field and in the emergency department.3 There is little or no information available to guide EMS and ED personnel in the proper selection and application of cer- vical spine immobilization devices for use on children.
For these reasons, we performed a study to evaluate the efficacy of com- mercially available cervical spine stabilization devices designed for pediatric patients. Each device was evaluated separately and those found most effec- tive then were evaluated in combination with commonly used supplemental stabilization techniques. Cost-effectiveness and ease of use also were ad- dressed.
MATERIALS AND METHODS A search of several current emergency medical supply catalogues yielded
one "infant" and 11 "pediatric" or "small" cervical collars designed specifical- ly for use on children. The products varied in construction from soft, dloth- covered foam to dense foam with rigid plastic support (Table 1). Commonly used types of extrication boards, head brace devices, bean bags, and an infant car seat were used in combination with selected cervical collars (Table 2). It
Carlos Huerta, MD* Cleveland, Ohio Robert Griffith, MD ~- Long Beach, California Steven M Joyce, MD, FACEP:~ Salt Lake City, Utah
From the Department of Emergency Medical Services, Mount Sinai Medical Center, Cleveland, Ohio;* the Department of Internal Medicine, Saint Mary's Medical Center, Long Beach, California;l and the Section of Emergency Medicine, University of Utah Medical Center, Salt Lake City, Utah.:~
Supported in part by the EMS Coordinating Council of Southeastern Arizona.
Presented at the Scientific Assembly of the American College of Emergency Physicians in Atlanta, September 1986.
Address for reprints: Steven M Joyce, MD, FACEP, Department of Emergency Medical Services, University of Utah Hospital, 50 North Medical Drive, Salt Lake City, Utah 84132.
16:10 October 1987 Annals of Emergency Medicine 1121/55

CERVICAL SPINE STABILIZATION Huerta, Griffith & Joyce
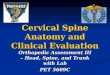
FIGURE. A)Measurement of pressures exerted by live subjects. Each child pushed with m a x i m u m voluntary effort against a stationary blood pres- sure cuff inflated to 20 m m Hg base- line pressure. Pressure exerted was measured in flexion, extension, rota- tion (cuff applied to mandible and cheek), and laterally. B) Application of pressure and measurement of motion in mannequins. Averaged pressures exerted by nine children were applied to the mannequin to push the head in the appropriate direction. When mo- tion ceased, a goniometer measured degrees of motion from the neutral position (coronal plane for flexion and extension, sagittal plane for rotation and lateral).
was thought that a full gamut of cur- rently available cervical spine immo- bilization methods was represented.
Due to inabi l i ty of infants and young children to cooperate with cer- vical collar testing, the test subjects consisted of resuscitation mannequins representing an infant (Resusci Baby ®, Laerdal Medical Corp, Armonk, New York) and a 5-year-old child (Resusci Junior ®, Laerdal). Measurements of head and neck circumferences as well as shoulder width agreed to within 20.1% and 11.3% of anthropometric values for infants and 5-year-olds, re- spectively. 4 Ranges of head and neck motion in flexion, extension, rotation, and laterally for both mannequins are shown (Table 3). The authors believe that, while human subjects may have greater ranges of motion in all but ro- tation, the mannequins ' ranges are well in excess of those required to demonstrate acceptable immobiliza- tion.
The m i n i m u m degree of mot ion sufficient to cause spinal cord damage when an unstable cervical spine injury exists has not been defined or sug- gested in the literature. The authors, therefore, defined "ideal" immobiliza- tion as that most closely approaching 0 ° in any direction.
In order to determine how much force could be exerted by normal chil- dren, the following method was de- vised. Nine cooperative children rang- ing in age from 5 to 9 years were selected. Written permission was ob- tained from the parents of each child. The children were healthy and had no history of cervical spine disease or in- jury. Each was instructed to exert
maximum pressure with his or her head against a stationary, hand-held blood pressure cuff, inflated to a base- line pressure of 20 mm Hg. Pressures were recorded in each of four direc- tions: flexion, extension, rotation, and laterally (Figure). Average pressures were determined for each direction and these pressures subsequently re- produced on the mannequins as de- scribed below.
With the mannequin in the supine position, each cervical collar was placed while manual axial traction and immobilization were maintained. Observations on ease of application for a single operator were noted (Table 1). Efficacy of each cervical collar and device was determined by the follow- ing method: the blood pressure cuff was used to push the mannequin's head in the desired direction until the previously determined average live subject pressure was reached and maintained. When motion ceased, a goniometer was used to measure de- grees of motion from the neutral posi- tion (coronal plane for flexion and ex- tension, sagittal plane for rotation and lateral) (Figure). Using simple summa- tion of degrees of motion allowed in each direction (because relative impor- tance of any given type of motion in producing injury is unknown), a scor- ing system was devised to compare performance (Table 4).
Those cervical collars found most effective then were used in combina- tion with other immobilization de-
vices and methods (Table 2). When de- vices such as KED and Extriboard ®, which partially enclose the head, re- stricted lateral and rotational pressure application, manual pressure thought to exceed that produced by live sub- jects was applied. This manual pres- sure method was used only with com- binations of cervical collars and other devices, and only when the blood pressure cuff ~ould not be applied. De- grees of motion allowed were mea- sured as described above, and a score was derived for each combination. In addition, the percentage of normal range of motion allowed was calcu- lated for each device in each direction, and summed percentage scores were derived for each collar, device, and combination.
Differences between groups were analyzed using both summed degree of mot ion scores and summed per- centage scores. Statistical analysis was performed using the Student t test.
In an effort to verify limitation of motion in live subjects, selected cer- vical collars were applied to six coop- erative children aged 4 to 9 years, and range of motion allowed in each direc- tion measured as described for the mannequin model. Summed scores of average motion allowed were derived for each cervical collar.
RESULTS Cervical collar construction, prices,
and ease of use are shown (Table 1). High-cut collars (designed to provide
56/1122 Annals of Emergency Medicine 16:10 October 1987

TABLE 1. Pediatric cervical collars tested
Product Name Manufacturer
Infant: Prosplints ® cervical collar Med Spec
Child ("Pediatric . . . . Child" or "Small")§
Foam extrication collar Life Assist
Disposable foam Health Care Group, extrication collar Inc
Ferno-Fit ® extrication collar Ferno Washington
Standard extrication collar Dyna Med
Hare ® extrication collar Dyna Med
Thomas ® extrica- tion collar Life Assist
Flex-Support ® 4-way Frank Stubbs extrication 3" collar Co, Inc
Flex-Support ¢ 4-way Frank Stubbs extrication 2" collar Co, Inc
Vertebrace ® extrication collar Jobst
Stif-Neck ® extrication California collar Medical Products
Philadelphia ® extrication collar Armstrong Industries
Construction*
Soft foam
High or Unit Ease Low Cutt Price Of Use$
Low $ 6.35 +
Soft foam
Soft foam
Firm foam
Firm foam
Firm foam
Foam + rigid plastic (2-piece)
Foam + rigid plastic
Foam ÷ rigid plastic
Foam + ngid plastic
Foam + rigid plastic
Foam + rigid plastic (2-piece)
Low $ 4.60 +
Low $ 4.60 +
Low $14.50 +
Low $ 8.85 +
High $ 9.60 +
High $26.00 -
High $11.90 +
High $11.90 +
High $20.75 ÷
High $19.40 +
High $19.25 -
*Construction types - - Soft foam: no other structural support; firm foam: more rigid than soft foam but no other structural support; foam and rigid plastic: usually firm foam surrounded or reinforced by rigid plastic, circumferentially or shanks.
tHigh cut: supporting the mandible and extending to the mastoid processes or occiput; low cut: lying below the mandible, mastoids, and occiput when applied.
~Ease of use in supine position by one person: ÷, easily and quickly applied; - , more difficult to apply and/or requiring longer application time.
§When "small" had been designated by the manufacturer for use in children.
points of support at the chin, angle of jaw, and mastoid processes, and/or oc- ciput) of rigid plastic construct ion were the most expensive, with the exception of the Flex-Support ® 4-way extrication collar (Frank Stubbs, Burbank, California), which com- pared favorably in price to firm foam collars. Both two-piece collars tested (Thomas ® [Temco Medical Health Care, Passaic, New Jersey] and Phila- delphia ® [ A r m s t r o n g Indus t r i e s , Northbrook, Illinoisl) were difficult to apply in the supine model, requiring some movement of the head or shoul- ders. Application of these two collars would be expected to be easier in a sit- ting model.
Degrees of motion allowed by each cervical collar when used alone, as well as summed scores of degrees of
mot ion and percentage of normal ranges of motion for each, are shown (Table 4).
Cervical collars of soft foam con- struction allowed the most motion, up to 100% of control values for some collars. Although the infant collar of soft foam performed better than its pe- diatric counterparts, it still allowed up to 20 ° of motion in the lateral direc- tion.
The best performance was delivered by collars of rigid plastic construction, closely followed by those of firm foam. However, none of the pediatric collars, when used alone, was able to restrict motion to less than 17 ° of flex- ion, 15 ° of extension, 4 ° of rotation, and 3 ° of lateral motion. The values for flexion and extension are consider- ably higher than those that the au-
thors would consider acceptable. Hence, none of the collars were con- sidered effective when used alone, and none of the intergroup differences were analyzed statistically.
Degrees of motion allowed by each combina t ion of devices wi th and without cervical collars, and summed degree and percent scores for each, are shown (Table 2).
For the infant model, standard spine immobil izat ion devices (half-spine board, KED ®) performed better than the infant car seat, and were markedly enhanced by the addition of the infant cervical collar.
For the pediatric mannequin, rigid spine immobilization devices (KED ®, Extr iboard ®, full- and half-spine boards) performed better than head immobilization devices designed to be
16:10 October 1987 Annals of Emergency Medicine 1123/57

CERVICAL SPINE STABILIZATION Huerta, Griff i th & Joyce
TABLE 2. Efficacy of other devices and methods
Collar
Infant Infant car seat, padd ing ,
tape with foam col lar
Head Brace ® With foam col lar
Hal f -sp ine board , tape With foam co l lar
Kendr ick 's Ext r icat ion Dev ice ®
With f oam co l lar
Child (Control) Head Immob i l i ze r ®
( foam cush ions a t t ached to sp ine board )
With Ve r teb race ®
Head Brace ® With F lex -Suppor t ®
Kendr ick 's Ext r icat ion Dev ice ®
With F lex -Suppor t ®
Ex t r iboard D i sposab le ® Extr icat ion dev i ce
With Ve r teb race ®
Hal f -sp ine boa rd + t ape With F lex -Suppor t ® + t ape
Ful l -spine boa rd + tape + Tape + b e a n b a g
+ F lex -Suppor t ® Tape, b e a n b a g
Degrees of Motion Allowed From Neutral Position In Mannequin Models
Flexion Extension Rotation Lateral Summed Score* (%)t
8 12 2 ° 3 ° 25 (64)
35 38 4 ° 1 o 78 (205) 11 19 2 ° 2 ° 34 (87)
1 1 4 ° 6 ° 12 (23) 1 1 2 ° 4 ° 8 (17)
12 10 19 ° 9 ° 50 (92) 1 1 4 ° 1 ° 7 (11)
11 18 26 ° 3 ° 58 (122) 10 14 1 ° 1 ° 26 (66)
16 12 2 ° 1 ° 31 (82) 7 9 5 ° 2 ° 23 (58)
6 8 4 ° 2 ° 20 (53) 4 3 1 ° 2 ° 10 (31)
9 7 5 ° 4 ° 24 (73) 3 2 2 ° 1 ° 8 (20)
10 1 40 7 ° 22 (79) 2 3 1 ° 2 ° 8 (26)
4 12 5 ° 3 ° 24 (63)
10 9 3 ° 2 ° 24 (66) 5 5 0 ° 1 ° 11 (31)
*Summed score, arithmetic sum of degrees of motion in each direction. (degrees of motion allowed X ) tSummed % score, arithmetic sum of percentage of control motion control 100 in each direction.
attached to backboards (ie, Head Im- m o b i l i z e r ® , [Fe rno W a s h i n g t o n , W i l m i n g t o n , Ohio) , Head Brace ® [Medix Choice, E1 Cajon, California]). The latter two devices were notably poor in limiting flexion extension un- less supplemented with a cervical col- lar.
Overall for the pediatric manne- quin, the combination of the various devices tested with a rigid plastic cer- vical collar was superior in immo- bilization to either the devices used alone (P < .05) or cervical collars used alone (P < .001). Similar observations can be made for the infant manne- quin, a l though differences were no t statistically significant due to small sample size (one collar, three devices).
TABLE 3. Range of neck motion in mannequins
Pediatric control Infant control
Flexion Extension Rotation Lateral 35 ° 45 ° 80 ° 16 °
35 ° 38 ° > 9 0 ° 40 °
When cervical collars were applied to six live subjects, limitation of mo- tion to less than l0 ° in any direction could not be achieved by any collar. Because of anxiety, short a t ten t ion span, and discomfort, none of the chil- dren successfully tested all of the cer- vical col lars , nor w o u l d any ade- quately test combination devices.
DISCUSSION Prior to age 8, the age after which
the cervical spine assumes adult con~ figuration, significant structural dif- ferences predisposing to potential in- jury exist.S, 6 The odontoid ossification front between the dens and the axis is weaker than the interface between the lower cervical bodies and their end-
58/1124 Annals of Emergency Medicine 16:10 October 1987

TABLE 4. Pediatric cervical collar efficacy
Collar
Infant Control (no collar)
Prosplints ® cervical collar
Child Control (no collar)
Foam extrication
Disposable foam
Ferno-Fit ® Standard
Hare ®
Thomas ® Flex-Support ® 3" 4-way
Flex-Support ® 2" 4-way
Vertebrace ®
Stif-Neck ®
Philadelphia ®
Degrees of Motion Allowed From Neutral Position In Mannequin Models
Flexion Extension Rotation Lateral Summed Score* (%)t
35 38 180 40 293 (400)
11 19 12 20 62 (138)
35 45 80 16 176 (400) 35 45 16 11 107 (289)
24 32 7 5 68 (180)
36 31 8 6 81 (217) 21 23 10 3 57 (142)
35 45 12 6 98 (253)
24 21 6 7 58 (168)
17 19 4 6 46 (134)
23 23
20 18
20 18
23 15 *Summed score, arithmetic sum of degrees of motion in each direction. tSummed % score, arithmetic sum of percentage of control motion
7 5 58 (157)
9 7 54 (152)
6 8 52 (155)
5 12 55 (180)
( ~legrees °f m°tion all°wed X ) control 100 in each direction.
' plates. 5 Secondly, hypermobil i ty and laxity of the cervical ligaments allows for considerable anterior-posterior ex- cursion of C-1 on C-2 (pseudosubluxa- tion). This laxity, combined with the relatively horizontal configuration of the facet joints, permits striking mo- bility of C-2 on C-3 and C-3 on C-4. 6 Finally, weaker ped ia t r i c ce rv ica l musculature is a predisposing factor for torsional or longitudinal injuries. 6
Considering these facts it is fortu- nate, as both Hubbard and Griffi th point out, that cervical spine injuries in children are rare.3, 7 However, when cervical spine injuries do occur in children younger than 8 years, they are more likely to involve the upper cervical spine than in adults.6, 7
They commonly occur in motor ve- hicular accidents either as passenger or as struck pedestrian.S, 8 Unstable injuries following falls have been re- ported from distances as little as sev- eral feet. 7~9 While the majority of pe- diatric cervical spine f rac tures are unstable, only a minori ty will present with a neurological deficit.hg,10 Delay in diagnosis of these fractures is com- m0nS, n and long-term complications of missed odontoid fractures in this
age group have been described.8 Indications for prophylactic cervical
spine stabilization are poorly defined. In a review of 161 children under age 5 presenting to our emergency depart- ment in whom the mechanism of in- jury suggested potential for cervical spine injury, only 46% of the 84 chil- dren who received prehospital care had any form of prophylactic stabiliza- tion. Of those who were stabilized, only six were rigidly stabilized. Fur- thermore, of the 77 children who ar- rived in the ED by private vehicle, only six had cervical spine stabiliza- tion performed in the department. 3
The efficacy of various cervical im- m o b i l i z a t i o n devices has been ad- dressed in several studies. 1~q6 The consensus of these studies appears to be that cervical collars alone are inad- equate for immobilization of the adult cervical spine; the use of a rigid back- board device is mandatory; and high- cut firm or rigid cervical collars are the most effective.
Our findings concur with those of adult studies. Our data demonstrate that none of the commercially avail- able pediatric collars provide adequate stabilization of the cervical spine if
used alone. Many of the supplemental devices
and methods showed superior immo- bilization over cervical collars when used alone. Exceptions were found w i t h the use of the Head I m m o - bilizer ® and Head Brace ®, which al- lowed unacceptable motion in flexion and extension.
The most significant finding is that despite recent improvements in cer- vical collar construct ion and design, combinations work better than collars alone. In all cases when the best cer- v ica l col lars were c o m b i n e d w i t h other devices and methods , mo t ion allowed was equal or decreased in all directions from single immobilization techniques (P < .05).
Our study has several l imitations requiring consideration. Mannequins do not possess the full range of mo- tion of pediatric subjects, nor are they i nc l i ned to s t ruggle w h e n i m m o - bilized. We found, however, that chil- dren of the appropriate ages (5 to 9 years) were unable or unwilling to un- ders tand i n s t ruc t i ons or coopera te fully with the experimental protocol. Our at tempt to confirm our findings in cooperative children tends to sup-
16:10 October 1987 Annals of Emergency Medicine 1125/59

CERVICAL SPINE STABILIZATION Huerta, Griffith & Joyce
port the conc lus ion that cervical col- lars used a lone are inadequa te for im- mobi l iza t ion .
Second, the use of a blood pressure cuff as a t ransducer for pressure mea- s u r e m e n t m a y be subject to s o m e dis- pute. It was the authors ' i n t en t to ar- r ive at a rough e s t ima te of pressures tha t ch i ld ren m i g h t exer t agains t an i m m o b i l i z a t i o n d e v i c e . In o r d e r to avoid bias, we used chi ldren older and p resumably s t ronger than the 5-year- old group tha t t he ped ia t r i c m a n n e - qu in represented. These same average pressures also were applied to the in- fan t m a n n e q u i n . B e c a u s e the s a m e average pressures were applied in the same m a n n e q u i n for each cervical col- lar, we be l ieve tha t the t e c h n i q u e is r e p r o d u c i b l e and s c i e n t i f i c a l l y va l id g iven t h e l i m i t a t i o n s of t he m a n n e - quin model .
Finally, h o w m a y t h e f i nd ings of this s tudy be applied to injured chil- dren in t he field and in the ED? Be- cause our l ive subjects were unab le to cooperate in tes t ing even a few collars and devices, we w o u l d expec t s o m e frightened, t r auma t i zed chi ldren to be s i m i l a r l y u n c o o p e r a t i v e . W h i l e i t is poss ib l e t ha t s t r u g g l i n g aga ins t re- s t ra ining devices m i g h t exacerbate ex- is t ing injuries, such s i tua t ions are no t c o m m o n in our exper ience and should be dealt w i t h at the d iscre t ion of per- sonne l on the scene. In these cases, m a n u a l i m m o b i l i z a t i o n m i g h t prove easier to manage and less f r ightening to p e d i a t r i c p a t i e n t s . U n t i l c l i n i c a l
data are available, the authors bel ieve that the resul ts of this s tudy m a y be appl ied as gu ide l ines for s e l ec t i on of p r o p h y l a c t i c c e r v i c a l s p i n e i m m o - b i l iza t ion m e t h o d s in pediat r ic and in- fant t r a u m a v ic t ims .
C O N C L U S I O N M a n y types of cervical collars and
var ious spinal i m m o b i l i z a t i o n devices are cur ren t ly m a r k e t e d for use in field s tabi l iza t ion of chi ldren w h e n cervical sp ine i n j u r y is s u s p e c t e d . O b j e c t i v e cl inical s tudies of thei r efficacy in pe- d i a t r i c p a t i e n t s a re n o t a v a i l a b l e . U s i n g m a n n e q u i n m o d e l s , w e f i n d that in the pediatr ic age range cervical col lars w h e n used a lone do no t pro- v i d e a d e q u a t e i m m o b i l i z a t i o n . We c o n c l u d e t h a t p r e h o s p i t a l c e r v i c a l s p i n e s t a b i l i z a t i o n is b e s t a c c o m - p l i shed by us ing a rigid type cervical collar in c o m b i n a t i o n w i t h a rigid spi- nal i m m o b i l i z a t i o n device. Field stud- i e s c o n f i r m i n g t h e s e f i n d i n g s a re needed . U n t i l l i m i t s for a c c e p t a b l e cerv ica l sp ine m o t i o n f o l l o w i n g im- m o b i l i z a t i o n are es tabl ished, we be- l ieve tha t u t m o s t c a u t i o n s h o u l d be exercised by us ing those m e t h o d s al- lowing least mot ion .
R E F E R E N C E S 1. Podolsky S, Baraff L, Simon RR, et al: Efficacy of cervical spine immobilization meth- ods. J Trauma 1983;6:461-464. 2. Cline JR, Scheidel E, Bigsby E: A comparison of methods of cervical immobilization used in patient extrication and transport. J Trauma 1985;7:649k653.
3. Griffith R, Joyce SM: Prophylactic cervical
stabilization in pediatric trauma victims: Cur- rent practices (unpublished).
4. Snyder RG, Spencer ML, Owings CL, et al: Anthropometry of U.S. Infants and Children Detroit, SAE Automotive Engineering Congress and Exposition, 1975.
5. Sherk HH: Musculoskeletal injuries, in Fleisher G, Ludwig S (eds): Textbook of Pedi- atric Emergency Medicine. Baltimore, Williams and Wilkins, I984.
6. Sherk HH, Schit L, Lane JM: Fractures and dislocations of the cervical spine in children Orthop Clin North Am 1976;7:593-604.
7. Hubbard DD: Injuries of the spine in chil= dren and adolescents. Clin Orthop and Rel Res 1974;100:56-65.
8. Fielding JW, Griffin PP: Os odontoideun: An acquired lesion. J Bone Joint Surg 1974;56- A{1): 187-190.
9. Gaufin LM, Goodman SJ: Cervical spine in- juries in infants: Problems in management. J Neurosurg i975;42:179-184.
10. Weiss MH, Kaufman B: Hangmans fracture in an infant. Am J Dis Child 1973;126:268-269.
ll. Griffiths SC: Fracture of odontoid process in children. J Ped Surg 1972;7:680-683.
12. Dick T, Land R: Spinal immobilization de- vices part 1: Cervical extrication collars. JEM5 1982;Dec:26-32.
13. Dick T, Land R: Spinal immobilization de- vices part 2: Cervical extrication devices. JEMS 1983;Jan:23-30.
14. Dick T, Land R: Spinal immobilization de- vices part 3: Full spinal immobilizers. JEMS 1983;Feb:34-43.
15. Aprahamian C, Thompson B, Finger WA, et al: Experimental cervical spine injury model: Evaluation of airway management and splinting techniques. Ann Emerg Med 1984;8:584-587.
16. McCabe JB, Nolan D: Comparison of the ef- fectiveness of different cervical immobilization collars. Ann Emerg Med 1986;1:50-53.
60/1126 Annals of Emergency Medicine 16:10 October 1987