Embed Size (px)
Citation preview

The clinical presentation of esophageal cancer in theUnited States and Europe has been changing, butunfortunately, esophageal cancer remains a dreadfuldisease. Patients with esophageal cancer commonlypresent (after a prolonged asymptomatic preclinicalperiod) with advanced inoperable disease and a verypoor prognosis. As described in Chapter 1, themajority of cases of esophageal cancer are of thesquamous cell or adenocarcinoma types. Squamouscell carcinomas typically arise in the proximal tomidesophagus, whereas adenocarcinomas are mostcommonly found in the distal esophagus.
Whereas historically, esophageal squamous cellcarcinoma was the most common histologic type ofesophageal cancer, more recent reports have shownthat over the past few decades, there has been amarked increase in the incidence of adenocarcinomasof the distal esophagus, esophagogastric junction, andgastric cardia.1,2 This has had an important impact onthe development of new approaches to screening,diagnosis, and prevention for this disease. As the pre-dominant cell type of esophageal cancer is changing,so is the location of the tumor, from the upper andmidesophagus more distally toward the esophagogas-tric junction. This may also play an important role inpatterns of growth and spread and in the choice of themost appropriate and accurate staging modalities.
Patients with esophageal cancer most often pre-sent with symptoms of dysphagia, weight loss, andchest pain with or without swallowing. The diagnos-tic assessment usually begins with an upper-gastroin-testinal barium radiographic study (barium swallow)
or endoscopy. Once a diagnosis of esophageal cancerhas been made, the patient should then undergo acomplete staging assessment to evaluate the initialstage and extent of disease. Reliable and precise pre-treatment clinical staging information is crucial toproviding the patient with an accurate prediction ofsurvival and to determining appropriate managementoptions. Determination of extent of disease at initialpresentation can identify those unfortunate patientswho present with advanced unresectable stage IVdisease and thus spare them potential additional mor-bidity and the cost of unnecessary surgery.
Given the recent significant increase in the inci-dence of adenocarcinomas of the esophagogastricjunction, precise localization of tumors detected inor around this area may be helpful in better charac-terizing this entity and may be useful in developingbetter approaches to managing these tumors. Theselesions may be more accurately defined as distalesophageal tumors, “true” esophagogastric-junctiontumors, or proximal gastric tumors.
Precise pretreatment staging of esophageal can-cer is very important in the initial evaluation andassessment of these patients. Since prognosis andmanagement options are highly dependent on accu-rate staging, optimal pretreatment assessment andstratification by stage will allow these patients to beoffered the most appropriate stage-specific treat-ment options. In addition, precise determination ofextent of disease is essential for those patients whoare being considered for an investigational treat-ment protocol.
23
2
Diagnosis and Preoperative Staging of Esophageal Cancer ARNOLD J. MARKOWITZ, MDHANS GERDES, MD

24 CANCER OF THE UPPER GASTROINTESTINAL TRACT
This chapter will discuss approaches to the diag-nosis and staging of esophageal cancer as practicedin the United States and specifically at a compre-hensive cancer center. The various staging modali-ties that have been evaluated will be discussed, andwe will present what we feel represents the state-of-the-art approach to the pretreatment staging ofesophageal cancer. Both diagnosis and staging willbe addressed together under each modality heading.Some of the methods presented have been shown tobe highly sensitive and specific but are not yetwidely available and thus cannot be considered thestandard of care.
STAGING
Over the past century, esophageal cancer staging hasevolved with the development of the internationalclassification system of cancer staging. This systempermits the accurate description of tumors to facili-tate communication between clinicians caring forpatients, to guide therapy, to predict prognosis, andto help standardize subject enrollment and evaluateresults in investigative research.
The Tumor-Node-Metastasis System
The American Joint Committee on Cancer (AJCC)Staging and End Result Reporting was originallyorganized in 1959 with the support of medical, sur-gical, radiologic, and pathologic societies, the Amer-ican Cancer Society, and the National Cancer Insti-tute. Through the creation of task forces appointedto consider malignant neoplasms at different loca-tions, the AJCC published the first comprehensivemanual on cancer staging in 1977. Based on pub-lished data, the manual’s emphasis was on simplic-ity, practicality, and credibility.
These guidelines were originally created in par-allel to those published by the International UnionAgainst Cancer (Union Internationale Contre leCancer [UICC]), which is a consortium of multiplenational committees on tumor-node-metastasis(TNM) staging, including American, British, Cana-dian, French, German, Italian, and Japanese groups.The AJCC manual and the UICC guidelines havesince been revised several times and have together
become an internationally recognized system ofcancer staging. The most recent edition of the AJCCcancer staging manual was published in 1997.3
According to the AJCC, esophageal cancer isclassified according to the extent of the primarytumor (T) and the presence and extent of lymphnode metastases (N) and distant organ metastases(M) (Table 2–1).
The primary tumor (T) stage is based on thedepth of tumor invasion into and through the wall ofthe esophagus. Histologically, the esophageal wallconsists of four distinct layers including themucosa, submucosa, muscularis propria, andadventitia. In contrast to other segments of theluminal digestive tract, the esophagus does not havea serosal layer. The earliest pathologic (p) T stage ofan esophageal cancer is classified as either pTis (ie,carcinoma in situ, for a squamous cell carcinoma)or high-grade dysplasia (for an adenocarcinoma). ApTis or high-grade dysplasia lesion is limited to the
Table 2–1. TUMOR-NODE-METASTASIS STAGING SYSTEM
FOR ESOPHAGEAL CANCER*
Primary tumor (T)TX Primary tumor cannot be assessedT0 No evidence of primary tumorTis Carcinoma in situT1 Tumor invades lamina propria or submucosaT2 Tumor invades muscularis propriaT3 Tumor invades adventitiaT4 Tumor invades adjacent structures
Regional lymph nodes (N)NX Regional lymph nodes cannot be assessedN0 No regional lymph node metastasisN1 Regional lymph node metastasis
Distant metastasis (M)MX Distant metastasis cannot be assessedM0 No distant metastasisM1 Distant metastasis
Tumors of the lower thoracic esophagusM1a Metastasis in celiac lymph nodesM1b Other distant metastasis
Tumors of the midthoracic esophagusM1a Not applicableM1b Nonregional lymph nodes and/or other distant
metastasis
Tumors of the upper thoracic esophagusM1a Metastasis in cervical lymph nodesM1b Other distant metastasis
*American Joint Committee on Cancer (AJCC) classification.Reprinted with permission from Fleming ID, Cooper JS, Henson DE, et al.editors. AJCC cancer staging manual. 5th ed. Philadelphia: Lippincott-Raven;1997.

Diagnosis and Preoperative Staging of Esophageal Cancer 25
epithelial layer of the mucosa and represents nonin-vasive disease. A pT1 tumor represents the earlieststage of invasive disease and is a tumor that pene-trates into the lamina propria (as can be seen inglandular epithelium associated with adenocarci-noma) or submucosa. A pT2 tumor invades deeperinto the muscularis propria layer. A pT3 tumor pen-etrates through all esophageal wall layers and outinto the adventitia. A locally advanced pT4 tumorinvades adjacent mediastinal structures, such as thetracheobronchial tree, the pericardium, or the aorta.Nodal staging for esophageal cancer is based on thepresence or absence of lymph node metastases. Doc-umentation of metastatic disease is based on spreadto distant metastatic foci and (in certain cases) maybe dependent on the primary tumor location withinthe esophagus.
The AJCC divides the esophagus into fourregions to assist localization and staging. Localiza-tion affects tumor classification, lymphatic drainage,and appropriate management options. The very supe-rior portion of the esophagus, the cervical esophagus,extends from the lower edge of the cricoid cartilageto the thoracic inlet, located approximately 18 cmfrom the incisor teeth. The remainder of the esopha-gus is divided into upper, middle, and lower thoracicportions. The upper thoracic esophagus extends fromthe thoracic inlet to the level of the tracheal bifurca-tion, approximately 24 cm from the incisors. Themiddle thoracic esophagus extends from the trachealbifurcation to the level of the distal esophagus,approximately 32 cm from the incisors. The lowerthoracic esophagus is the approximate 8 cm of distalesophagus and includes the intra-abdominal portionand the esophagogastric junction, approximately 40cm from the incisors.
As preoperative staging has evolved over the pasttwo decades, the system has been modified to repre-sent the clinical (cTNM) and pathologic (pTNM)staging of tumors separately because histopatho-logic confirmation of stage may not always be avail-able when treatment decisions are being made.According to the AJCC, the determination of thepathologic nodal staging for an esophageal tumor isgenerally based on the evaluation of six or morelymph nodes removed from the mediastinal lym-phadenectomy specimen. Nearby lymph node
groups are classified by the AJCC as either regionalor distant nodes, depending on their relationship tothe location of the primary esophageal tumor (Table2–2). Lymph node involvement beyond the regionallymph nodes constitutes distant metastases. Forexample, when staging a tumor of the intrathoracicesophagus, involvement of the lymph nodes of thecervical or celiac axis would be considered to bemetastatic (M1) disease.
The determination of M1 disease for anesophageal tumor may be based on the documenta-tion of metastatic spread either to distant lymphnodes or to other solid organs. The most commonsites for metastatic spread of esophageal cancerinclude the liver, lungs, bones, and the peritonealcavity. Clearly, early determination of metastatic dis-ease prior to the initiation of therapy is very impor-tant for determining operability, planning appropri-ate treatment, and determining potential eligibilityfor investigational treatment protocols.
The disease stage is determined according to theactual information for each of these T, N, and M fac-tors (Table 2–3). For example, a tumor limited to theesophageal mucosa or submucosa and withoutlymph node or distant metastases (T1 N0 M0) rep-resents stage I (early) disease whereas a tumor pen-etrating through the esophageal wall, invading anadjacent neighboring organ, and having regional
Table 2–2. CLASSIFICATION OF REGIONAL LYMPH NODES,
BASED ON ESOPHAGEAL TUMOR LOCATION*
Regional lymph nodes
Cervical esophagusScaleneInternal jugularUpper cervicalPeriesophagealSupraclavicularCervical, NOS
Intrathoracic esophagus (upper, middle, and lower)TracheobronchialSuperior mediastinalPeritrachealCarinalHilar (pulmonary roots)PeriesophagealPerigastricParacardialMediastinal, NOS
*American Joint Committee on Cancer (AJCC) classification.Adapted from Fleming ID, Cooper JS, Henson DE, et al., editors. AJCC cancer staging manual. 5th ed. Philadelphia: Lippincott-Raven; 1997.

26 CANCER OF THE UPPER GASTROINTESTINAL TRACT
lymph node involvement and distant metastases (T4N1 M1) reflects stage IV (advanced) disease.
Staging of Cancer of the Esophagogastric Junction
The recent increase in the incidence of esophagealcancer has been associated with a rapid increase inthe rate of adenocarcinomas of the distal esophagusand esophagogastric junction. However, physiciansat different institutions (and even at the same insti-tution) may not classify and approach tumorslocated in this region in the same way. Some physi-cians consider and treat these lesions as esophagealtumors whereas other physicians consider them tobe proximal gastric cancers or even separate and dis-tinct entities. To help to clarify this confusion, arecent consensus conference of the InternationalGastric Cancer Association (IGCA) and the Interna-tional Society for Diseases of the Esophagus (ISDE)agreed that these tumors should be more clearlydefined and classified so as to develop a more con-sistent approach to managing them.4 These groupshave defined adenocarcinomas of the esophagogas-tric junction as tumors that “have their center within5 centimeters proximal and distal of the anatomicalcardia.”4,5 Furthermore, they have developed a clas-sification system for three distinct types of tumorsof the esophagogastric junction, based on thetumor’s apparent point of origin (Table 2–4).
The classification of adenocarcinomas locatedwithin the region of the esophagogastric junction
into more distinct tumor types may significantlyhelp in the ongoing study and understanding of thispotentially heterogenous group of tumors. Whereastype I adenocarcinomas are believed to arise pre-dominantly from specialized intestinal Barrett’sepithelium in the distal esophagus, there appears tobe a low prevalence of intestinal metaplasia at orbelow the level of the gastric cardia in type II and IIItumors (32% and 9%, respectively).4 In addition, thedevelopment of dysplastic changes in segments ofintestinal metaplasia at or below the gastric cardiaappears to be much less frequent an occurrence ascompared to such changes seen in distal esophagealintestinal metaplasia.6 Furthermore, the differingbehaviors of tumors of the esophagogastric junctionmay also be somewhat accounted for by differentpatterns of lymphatic spread. For tumors of the dis-tal esophagus, main lymphatic pathways extend bothcephalically into the mediastinum and caudallytoward the region of the celiac axis, whereas tumorsat or below the gastric cardia spread predominantlytoward the regions of the celiac axis, the splenichilum, and the para-aortic lymph nodes.7,8
The more precise classification and staging ofdistal esophageal tumors at or close to the esopha-gogastric junction may help physicians gain a betterunderstanding of these tumors’ natural history, pat-terns of spread, and expected response to therapy.This knowledge will be invaluable for the design offuture clinical research protocols and treatmentplans for managing patients with these tumors.
Table 2–3. CLASSIFICATION OF STAGE GROUPINGS FOR
ESOPHAGEAL CANCER*
Stage TNM Classifications
0 Tis N0 M0I T1 N0 M0IIA T2 N0 M0
T3 N0 M0IIB T1 N1 M0
T2 N1 M0III T3 N1 M0
T4 Any N M0IV Any T Any N M1IVA Any T Any N M1aIVB Any T Any N M1b
TNM = tumor-node-metastasis.*American Joint Committee on Cancer (AJCC) classification.Adapted from Fleming ID, Cooper JS, Henson DE, et al., editors. AJCC can-cer staging manual. 5th ed. Philadelphia: Lippincott-Raven; 1997.
Table 2–4. CLASSIFICATION* OF CANCERS ARISING IN THE
REGION OF THE ESOPHAGOGASTRIC JUNCTION
Type I tumorAdenocarcinoma of the distal esophagus, which usuallyarises from an area with specialized intestinal metaplasia ofthe esophagus (ie, Barrett’s esophagus); may infiltrate the esophagogastric junction from above
Type II tumorTrue carcinoma of the cardia; arises from the cardiac epithelium or short segments with intestinal metaplasia atthe esophagogastric junction; often referred to as a “junc-tional carcinoma”
Type III tumorSubcardial gastric carcinoma that infiltrates the esophagogastric junction and distal esophagus from below
*International Gastric Cancer Association and the International Society forDiseases of the Esophagus classification.Adapted from Siewert JR, Stein HJ. Classification of adenocarcinoma of theoesophagogastric junction. Br J Surg 1998;85:1457–9.

Diagnosis and Preoperative Staging of Esophageal Cancer 27
METHODS FOR STAGING ESOPHAGEAL CANCER
Barium Radiography and Upper-Gastrointestinal Endoscopy
In a patient presenting with signs and symptoms sug-gestive of a possible esophageal malignancy, the diag-nostic evaluation typically begins with either a single-or double-contrast barium swallow or an upper-gas-
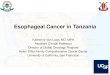
trointestinal (UGI) endoscopy. Both modalities pro-vide a good structural assessment of the esophageallumen and the overlying mucosa. On barium study,abnormal radiographic findings that suggest possi-ble esophageal malignancy include an intraluminalmass–like filling defect, asymmetric stricturing, andmucosal irregularities (Figure 2–1). On occasion,however, an esophageal cancer may even presentradiographically as an apparent smooth circumfer-ential stricture.
Figure 2–1. A, Barium swallow demonstrates an “apple core” filling defect with associated luminal narrowing(arrow) resulting from a proximal esophageal cancer. B, Barium swallow demonstrates a distal esophageal tumorabove a hiatal hernia (arrows). C, Barium swallow demonstrates circumferential narrowing (arrow) due to a dis-tal esophageal tumor extending to the level of the esophagogastric junction. D, Barium swallow demonstratesdistal esophageal wall infiltration (arrow) with minimal proximal dilatation caused by an esophageal carcinoma.
A B
C D

28 CANCER OF THE UPPER GASTROINTESTINAL TRACT
In one study of barium radiography inesophageal disease, four radiologists, blinded to theclinical history, reviewed the barium esophagramsfrom 35 patients (6 normal, 16 with benignesophageal disease, and 13 with small malignanttumors < 3.5 cm in diameter) and accurately diag-nosed the small cancers in 73 percent of tumorcases.9 Of the false-negative evaluations, 21 percentwere interpreted as cases of benign esophageal dis-ease and 6 percent as normal. Thus, although bariumradiography may be a relatively good initial study in
the assessment of symptomatic patients, smallmalignancies may be missed. In addition, allpatients with abnormal barium studies need furtherinvestigation by UGI endoscopy (with biopsies andcytologic brushings) to rule out a potential malig-nancy (Figure 2–2).
In the United States, UGI endoscopy is currentlythe procedure of choice for the initial diagnosticevaluation of symptomatic patients. When combinedwith endoscopic biopsy, UGI endoscopy serves asthe primary screening tool for patients with the pre-
A B
C D
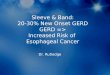
Figure 2–2. Upper gastrointestinal endoscopy, showing masses and tumors at various sites. A, Small esophageal cancer at the squamo-columnar junction. B, Bulky polypoid mass in the distal esophagus. C, Ulcerated mass in the distal esophagus. D, Infiltrative mass in the distalesophagus. E, Gastric cardia component of an infiltrative mass of the esophagogastric junction (same patient as in Figure 2–2D), seen duringretroflexion in the proximal stomach (arrow indicates tumor). F, Submucosal infiltration of the gastric cardia, seen during retroflexion in the proxi-mal stomach. G, Esophageal tumor undergoing biopsy. H, Esophageal tumor undergoing cytologic brushing.

Diagnosis and Preoperative Staging of Esophageal Cancer 29
E F
G H
Figure 2–2. Continued
malignant condition of Barrett’s esophagus. Endo-scopy not only permits the careful inspection andprecise localization of any esophageal lesion but(most important) also allows targeted biopsies ofabnormal areas, for a prompt and definitive histo-logic diagnosis.
Although barium radiography is a very good tech-nique for diagnosing esophageal strictures in patientswith dysphagia and although UGI endoscopy withbiopsy and cytologic brushing is highly accurate inproviding both a gross morphologic description and
a histologic confirmation of malignancy, neither ofthese modalities alone is adequate to provide a com-plete preoperative staging assessment for esophagealmalignancies. Although both techniques do providean excellent structural examination of the esophageallumen, neither modality can assess extraluminal dis-ease. Thus, additional staging procedures are neces-sary (1) to provide accurate information regardingthe depth of tumor invasion and the status of locore-gional lymph nodes and (2) to assess for potentialdistant metastases.

30 CANCER OF THE UPPER GASTROINTESTINAL TRACT
Computed Tomography
Over recent years, computed tomography (CT) hasbecome the method most used in the initial stagingof newly diagnosed esophageal malignancies. Oncean esophageal cancer has been confirmed by UGIendoscopy and biopsy, the patient’s extent of diseaseevaluation often begins with a CT of the chest andabdomen. Current high-resolution helical CT ishelpful in identifying metastatic disease to such sitesas the liver, lungs, mediastinal and retroperitoneallymph node areas, and intraperitoneal areas.
Imaging with CT can usually identify medium tolarge esophageal masses by the evident thickeningof the esophageal wall and by the proximal luminaldilation caused by the obstruction (Figure 2–3, A toD). However, CT cannot accurately determine thedepth of tumor invasion within the esophageal wallbecause of its inability to define individual layers ofwall tissue and often cannot even identify the pres-ence of small T1 and T2 masses. The resolution ofcurrent CT can only help to confirm the presence ofan esophageal mass and the suspicion of invasion ofadjacent mediastinal organs (T4), but it does not per-mit the accurate classification of T stage.
Lymph node metastases are identified on CTscans by the finding of enlarged and rounded hypo-dense structures in the mediastinum, adjacent to thestomach, and in the retroperitoneum or porta hepatis(see Figure 2–3, E to G). Mediastinal lymph nodes> 1.0 cm in maximum short-axis diameter in thetransverse plane are considered to represent nodalmetastases10 and can sometimes be seen by CT.
On a CT scan, distant metastatic disease to theliver or lung usually appears as one or more hypo-dense round areas within the liver or lungparenchyma that enhance after the administration ofintravenous contrast material (see Figure 2–3, H andI). Peritoneal disease can be strongly suggested bythe finding of a thickening of the omentum or peri-toneal surfaces, irregular contours on the bowel sur-face, or the presence of ascites.
When reviewing the many studies in the litera-ture that report on the sensitivity, specificity, andaccuracy of CT in the preoperative staging ofesophageal cancer, one must take into account thatmany of these studies were not prospective, used
early-generation CT technology, were limited bysmall sample sizes, and may have used varying def-initions of metastatic disease (ie, celiac lymph nodeinvolvement) in their assessments.
One study from Duke University evaluated CT inthe staging of 76 esophageal cancer and esopha-gogastric cancer patients.11 The study compared thefindings in these patients with the findings in 26control patients without esophageal cancer and whohad a normal mediastinum at surgery. A group offour radiologists were blinded to the patients’ under-lying diagnoses; they identified the CT scans of all26 controls as normal. In the 61 cancer patients whowere explored, there was an 88 percent accuracy ratefor the detection of both local mediastinal invasion(depth of tumor penetration) and distant abdominalmetastases. In a separate cohort of 12 patients, CTwas less accurate in staging tumors of the esopha-gogastric junction and yielded accuracy rates of 50percent for the prediction of both mediastinal inva-sion and distant metastases. In this study, CT cor-rectly staged 94 percent of patients with esophagealcancer and 42 percent of those with cancers of theesophagogastric junction. Some of the difficultywith CT in assessing the T stage of distal tumors inthe region of the esophagogastric junction may berelated to poor gastric distention and/or the presenceof a hiatal hernia in this region.
In a study from Vanderbilt University, CT find-ings in 18 esophageal cancer patients were com-pared with their operative findings and surgicalpathology.12 The accuracy of CT for localized tumorinvolvement was 77 percent whereas its accuracywas 94 percent for detecting direct aortic invasionand 88 percent for detecting tracheobronchial inva-sion. Computed tomography demonstrated a 72 per-cent accuracy for local lymph node involvement inmediastinal nodes; however, it was inaccurate forassessing distant lymph node metastases to intra-abdominal nodes in 11 of 18 patients. In 9 of these11 cases (6 middle-thoracic and 3 lower-thoraciccases), positive celiac or left gastric nodes werefound that were not detected by CT (false-nega-tives). In the other 2 cases, CT predicted abdominallymph node involvement due to radiographicallyenlarged nodes (these were confirmed as beingincreased in size at surgery, but pathology failed to

Diagnosis and Preoperative Staging of Esophageal Cancer 31
Figure 2–3. Computed tomography of esophageal massesand metastatic spread. A, An early-stage cancer of the esopha-gogastric junction (same patient as in Figure 2–2A) (arrow indi-cates tumor). B, A small distal esophageal tumor (arrow). C, Anobstructing tumor (arrow) of the distal esophagus. D, A polypoidmass (arrow) filling the esophageal lumen. E, Metastatic spreadof esophageal cancer to a subcarinal lymph node (arrow). Thiswas confirmed by endoscopic ultrasonography (EUS)–guidedfine-needle aspiration (FNA). F, Metastatic spread of esophagealcancer to perigastric and celiac lymph nodes (arrow indicateslymph node).This was confirmed by EUS-guided FNA. G, A sus-picious-appearing necrotic celiac lymph node (n) in a patient withan esophagogastric-junction cancer (T). H, A distal esophagealtumor (t) and two hypodense liver metastases (arrows) I, Twosmall peripheral left lung metastases (arrows) in a patient with anesophageal cancer (confirmed by thoracoscopy).
A B
C D
E F
G
I
H

32 CANCER OF THE UPPER GASTROINTESTINAL TRACT
demonstrate metastatic disease [false-positives]).Finally, accuracy for distant metastatic disease (notincluding the celiac or left gastric nodes) was 94percent. Overall, surgical findings altered the TNMstaging in 8 (73%) of 11 patients.
Another study of CT from Washington University(St. Louis, MO) reviewed CT findings in 30esophageal cancer patients and correlated those find-ings with surgical findings, in 28 of 30 of thepatients, or autopsy findings.13 They reported find-ings similar to that of the Vanderbilt study, in that CTwas demonstrated to be accurate for assessing tumorsize, local invasion of the tracheobronchial tree, andmetastatic disease to distant intra-abdominal lymphnodes (celiac and left gastric nodes) and solid organs(liver and adrenals), but to be inaccurate for assess-ing spread to regional periesophageal lymph nodes.Interestingly, most of the periesophageal nodes thatwere positive for metastatic tumor were not enlargedwhereas the positive distant intra-abdominal nodes(M1 disease) were enlarged.
An important limitation of CT in stagingesophageal tumors is its lack of sensitivity for accu-rately determining lymph node metastases (N stage).Also, an important factor, illustrated by both theVanderbilt and Washington University studies, isthat even normal-sized lymph nodes might containmicroscopic foci of metastatic disease that is beyondthe level of detection offered by CT.
In another retrospective study that assessed theaccuracy of preoperative staging by CT in 33 patientswith esophageal cancer, a comparison was made withsurgical and pathologic findings.14 Of note, thiscohort of patients was preselected for having no evi-dence of liver metastases, based on preoperativestaging assessment. This study used the AJCC TNMclassification for tumor staging. Enlarged lymphnodes seen by CT were defined as being > 1 cm indiameter. The study reported excellent rates for sen-sitivity (100%), specificity (97%), and accuracy(97%) for the detection of tracheobronchial invasionbut found that CT was not as accurate for determin-ing aortic involvement (with rates of 100% for sensi-tivity, 52% for specificity, and 55% for accuracy).Once again, CT fared poorly in determining regionallymph node metastases (celiac nodes were defined asregional nodes for distal esophageal tumors whereas
they were defined as distant nodes for proximal andmidesophageal tumors), demonstrating rates of only61 percent for sensitivity, 60 percent for specificity,and 61 percent for accuracy. The authors perceivedthis to be related to the difficulty of CT in distin-guishing periesophageal nodes from adjacent tumor.Computed tomography did somewhat better with dis-tant lymph node involvement, showing sensitivity,specificity, and accuracy rates of 67 percent, 87 per-cent, and 85 percent, respectively. The sensitivity ofCT for the detection of distant liver metastases couldnot be assessed in this study because the patientswere preselected for not having liver metastases, butexcellent specificity and accuracy rates (100% forboth) were demonstrated for this modality. Overall,however, CT was able to correctly stage only 39 per-cent (13) of the 33 patients. The authors attributedthe understaging by CT to its inability to accuratelydefine depth of tumor invasion and to determinedirect periesophageal mediastinal invasion.
An additional study that compared preoperativeCT with surgical and pathologic findings in a cohortof 50 patients with esophageal cancer (University ofBern, Bern, Switzerland) found a very high accu-racy rate for the detection of direct tumor invasioninto the tracheobronchial tree (100%) for proximalthoracic tumors and for aortic involvement (95 to100%) for proximal, middle, and distal tumors.15
However, CT assessment of intra-abdominal lymphnode metastases demonstrated sensitivity, speci-ficity, and accuracy rates of 57 percent, 100 percent,and 80 percent, respectively. The low sensitivity forthe detection of distal intra-abdominal nodes thuslimited the overall accuracy rates for CT staging toonly 80 percent, 68 percent, and 65 percent forupper, middle, and lower thoracic esophagealtumors, respectively.
Despite the limitations of CT for assessing Tstage and N stage, our institution continues to relyon chest and abdominal spiral CT with oral andintravenous contrast early in the evaluation to detectthose patients with apparent metastatic disease. Theidentification of metastatic disease at presentationpermits immediate triage of these patients to sys-temic therapy or investigational treatment protocols,with the avoidance of surgery. Patients in whom ini-tial CT does not reveal metastatic disease then

Diagnosis and Preoperative Staging of Esophageal Cancer 33
undergo more advanced staging evaluations and aremore appropriately offered curative surgical treat-ment or multimodality treatment protocols withcurative intent.
Endoscopic Ultrasonography
Endoscopic ultrasonography (EUS) is a new andpowerful imaging modality that has been developedover the past 15 years. It provides detailed imagingof the esophageal wall, nearby lymph nodes, andother adjacent structures. This modality makes useof the ability to introduce an ultrasound transducerdirectly into the gastrointestinal tract, thus bringingit into close proximity to the tumor. This eliminatesthe artifacts, created by intraluminal air and food,found in standard transcutaneous ultrasonographyand CT.
Coupled with the development of new high-fre-quency ultrasound transducers, EUS permits thedetailed evaluation of most areas of the gastrointesti-nal tract that are within the reach of standard endo-scopes (Figure 2–4). While it does require sedationfor most evaluations of the upper-gastrointestinaltract, EUS examinations are performed with the easeand comfort of most routine upper-gastrointestinalendoscopies. There is minimal risk, and EUS hasproved to be well tolerated by most patients.
Many studies have shown that the resolutionpower of currently available EUS instruments pro-vides superior assessment of almost all neoplasms ofthe esophagus, in addition to those involving thestomach, pancreas, and rectum. The 5-, 7.5-, and 12-MHz probes fitted on these scopes permit the assess-ment of microscopic tissue planes in the gastroin-
testinal tract, including the distinction of the normalmultilayered histologic architecture of the mucosa,submucosa, muscularis propria, and serosa.16–18 Thefirst wall layer is bright and corresponds to a borderecho and the superficial mucosa; the second is darkand corresponds to the deep mucosa (including themuscularis mucosae); the third is bright and corre-sponds to the submucosa and the acoustical interfacebetween the submucosa and muscularis propria; thefourth is dark and corresponds to the muscularis pro-pria; and the fifth is bright and corresponds to theadventitial interface (Figure 2–5). In contrast to CT,the ability of EUS to distinguish wall layers allows itto provide a more accurate determination of depth ofinvasion by tumors; EUS thus has the potential toidentify early-stage intramural disease.
On EUS, normal esophageal wall thickness isabout 0.3 cm.19 On EUS, an esophageal malignancyappears as a hypoechoic abnormality within thewall, disrupting the normal wall echolayers. Thelower-frequency transducers permit the evaluationof extramural disease (including local and regionallymphadenopathy and disease in adjacent organssuch as the liver, spleen, and pancreas), in additionto the identification of ascites. Thus, EUS providesaccurate assessment of depth of tumor invasion intoand through the wall of the esophagus (Figure 2–6,A to C), detection of direct invasion into adjacentstructures (see Figure 2–6, D and E), and identifica-tion of local lymph node metastases (see Figure 2–6,F and G), making it an ideal modality for determin-ing clinical tumor stage according to the TNMmethod of cancer staging.
Computed tomography characterizes lymph nodesthat are abnormally large (> 1 cm in diameter) as sus-
Figure 2–4. Olympus mechanical radial (left) and Pentax linear (right) array endoscopic ultrasoundscopes.

34 CANCER OF THE UPPER GASTROINTESTINAL TRACT
picious for tumor involvement. In addition to size,EUS also uses additional criteria (such as roundedshape, homogeneous hypoechoic pattern, and sharplydemarcated borders) to assess for metastatic lymphnodes.20,21 Nodes that appear to be benign on EUSmay be > 1 cm in diameter but are typically elongatedin shape, demonstrate a hyperechoic pattern with dis-tinct cortical and medullary areas, and have lesssharply demarcated borders.22
In locoregional staging for esophageal cancer,EUS is superior to CT.23 This is due to its more pre-cise imaging of distinct esophageal wall layers andits better ability to assess malignant nodal disease.
In numerous studies of preoperative endosono-graphic assessment of esophageal cancer by EUS ascompared with surgical pathology in resected speci-mens, the accuracy of EUS for determining depth oftumor invasion (T stage) has been reported to rangefrom 75 to 90 percent.24–34 In studies comparingEUS to CT for preoperative T staging, the accuracyof EUS ranges from 76 to 89 percent, and that of CTranges from 49 to 59 percent.21,26,27 At our institu-tion, a prospective comparative study of preopera-tive EUS versus dynamic CT for esophageal cancerin 50 patients demonstrated an accuracy of 92 per-cent for T staging with EUS and 60 percent for Tstaging with CT (p < .0003).19 A reasonable estima-tion of the overall accuracy of EUS for T staging,
based on the now extensive published literature, isapproximately 85 percent.23
Although EUS is highly accurate for determiningT stage, it may have some difficulty distinguishingbetween T1 (mucosal invasion) and T2 (submucosalinvasion) tumors.35 Since T2 tumors are associatedwith a high risk (30 to 70%) of lymph node metas-tases, this differentiation between early-stage T1 andT2 disease is extremely important if one is to con-sider the option of minimally invasive endoscopicresection to treat T1 lesions.23 The accuracy of EUSfor T staging superficial esophageal tumors has beenreported to be 72 percent.34 The use of smallcatheters (which can be passed through the instru-ment channel of a standard endoscope) containinghigher-frequency 20-MHz transducers that offerhigher resolution of esophageal wall layers may helpovercome this issue in the future36 (Figure 2–7).
For staging regional lymph node metastases(N stage), EUS has also been found to be more accu-rate than CT. The distinction between benign andmalignant nodes is still a problem. Unlike CT, how-ever, EUS not only can assess lymph node size butcan also evaluate for additional criteria, such aswell-circumscribed, rounded, and hypoechoic nodalcharacteristics, to predict metastatic nodal involve-ment. With CT, normal-sized lymph nodes contain-ing occult microscopic metastases lead to understag-
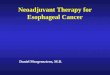
Figure 2–5. Endoscopic ultrasonography imageof the normal echoarchitecture of the esophagealwall. The central concentric rings are artifacts cre-ated by the ultrasound scope. (M = mucosa; SM =submucosa; MP = muscularis propria; A = adventi-tia; B = water-filled balloon filling the esophageallumen.)

Diagnosis and Preoperative Staging of Esophageal Cancer 35
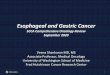
Figure 2–6. Endoscopic ultrasonography (EUS) of esophagealtumors and lymph node metastases. A, A T1 esophageal tumor (T)extending into the submucosa. (at arrow) in the same patient shownin Figure 2–2A. B, A T2 esophageal tumor extending into the mus-cularis propria (at arrow) (T = tumor, Ao = aorta.) C, A T3esophageal tumor infiltrating through all wall layers and out into theadventitia (at arrows) (T = tumor, Ao = aorta.) D, A T4 esophagealtumor (T) invading the aorta (Ao) arrow indicates point of invasion.E, A T4 esophageal tumor (T) invading the trachea (Tr). Arrow indi-cates point of invasion. (Ao = aorta.) F, Locoregional lymph nodemetastases in a patient with an esophageal tumor. (n =periesophageal lymph node; Ao = aorta; LA = left atrium.) G, Lymphnode metastases involving the perigastric (In) and celiac-axis (LN)lymph nodes in a patient with an esophageal tumor (confirmed byEUS-guided fine-needle aspiration).
A B
C D
E F
G

36 CANCER OF THE UPPER GASTROINTESTINAL TRACT
ing whereas benign enlarged inflammatory nodeslead to overstaging.
In a study from the Cleveland Clinic, EUS fea-tures of lymph node metastases were assessed in 100patients with esophageal cancer.37 When stringentcriteria regarding lymph node size (> 1 cm), shape(round), border demarcation (sharp), and centralecho pattern (homogeneous and hypoechoic) wereapplied, the sensitivity and specificity of EUS indetecting lymph node metastases were 89.1 percentand 91.7 percent, respectively; when all four fea-tures were present, accuracy of predicting lymphnode metastases was 100 percent.
Multiple reports of preoperative EUS assessmentof regional lymph node metastases in esophagealcancer since 1992 demonstrate accuracy rates rang-ing from 70 to 90 percent.24,25,27–31,34,38 In comparingpreoperative EUS to CT for N staging, the accuracyrates for EUS range from 72 to 80 percent whereasaccuracy rates for CT range from 46 to 58 per-cent.21,27,30 In the study from our institution thatdirectly compared EUS and CT in this setting, wereported accuracy rates of 88 percent with EUS and74 percent with CT.19 Overall, the extensive pub-lished data suggest an EUS accuracy rate of approx-imately 75 percent for regional N staging.23 As withCT, the reduced accuracy of EUS for N staging isrelated to the issue of distinguishing benign frommalignant lymph nodes.
For the detection of advanced (T4) disease, EUShas been demonstrated to be more accurate than CTin determining vascular invasion of the aorta orpericardium.39 In another series (a recent multicen-ter retrospective cohort study of 79 patients withstage T4 esophageal cancer as determined by pre-operative EUS staging), EUS was more accuratethan CT in determining T4 tumor invasion, withrates of 87.5 percent and 43.8 percent, respectively(p = .0002).40 The accurate preoperative determina-tion of locally advanced T4 disease would clearlyhave an impact on the treatment options offered tothe patients as the patients would no longer be ini-tial surgical candidates but would perhaps (in somecenters) be eligible for investigational protocolsevaluating the usefulness of preoperative neoadju-vant chemoradiotherapy.
In esophageal cancer patients, EUS is not asaccurate as CT in the detection of distant metastaticdisease to such common sites as the liver, lungs, andperitoneal cavity. In the series from our institution,CT demonstrated an accuracy of 90 percent in thestaging of distant metastases, as compared to the 70percent accuracy of EUS (p < .02).19 One potentialadvantage of EUS, as compared to CT, may be in themore accurate detection of M1 disease related toceliac node involvement.
Another limitation of EUS in the preoperativeassessment of esophageal cancer is its inability tocompletely evaluate severely strictured esophagealtumors. As it is common for patients to present withadvanced disease, there have been reports of high-grade malignant strictures in 20 to 44 percent ofpatients at initial presentation.41 These stricturesmay prevent passage of the echoendoscope and thusnot allow a complete EUS staging examination.
An increased risk of perforation has beenreported in patients with high-grade malignant stric-tures who undergo esophageal dilatation followed byEUS staging. In a study of 79 patients withesophageal cancer from the Cleveland Clinic, 26.6percent presented with a high-grade malignant stric-ture; of these 21 patients, 24 percent developed anesophageal perforation as a result of the wire-guideddilatation or as a direct result of the EUS procedure.42
However, some other ultrasonographers havereported that such high-grade malignant strictures
Figure 2–7. Size comparison of four different endoscopic ultra-sonography (EUS) instruments. (a = Olympus EUS colonoscope;b = Olympus EUS gastroscope; c = Olympus prototype miniprobe;d = Boston Scientific EUS miniprobe.)

Diagnosis and Preoperative Staging of Esophageal Cancer 37
can be safely dilated to allow passage of the echoen-doscope just prior to the EUS staging procedure.33
As a result of the experience of severalesophageal perforations at our institution, we do nottypically dilate high-grade malignant esophagealstrictures during EUS staging. Instead, our approachin these cases is to perform a limited ultrasono-graphic staging examination at the upper extent ofthe tumor or to use the new wire-guided thin-caliberEUS scope (MH 908, Olympus), which easily passeseven obstructing tumors to permit full staging with-out the increased risk.
Endoscopic Ultrasonography–Guided Fine-Needle Aspiration
Although both CT and EUS can detect enlarged andsuspicious-appearing lymph nodes, both techniquesare limited to morphologic characterization. The pres-ence of enlarged and inflammatory lymph nodes inesophageal cancer can reduce the specificity of bothimaging modalities for detecting lymph node metas-tases. An important recent advance in the field ofendoscopic ultrasonography was the use of EUS-guided fine-needle aspiration (FNA) to sample sub-mucosal lesions, nearby lymph nodes, and other adja-cent structures throughout the gastrointestinal tract.
The linear-array ultrasonographic endoscope pro-vides scanning that is oriented parallel to the long axisof the endoscope and is capable of tracking the passageof a biopsy needle (Figure 2–8). Ultrasonography-guided tissue sampling can thus be obtained by thepassage of a cytology needle through the instrumentchannel of the scope and directly into the plane of theultrasonographic image (Figure 2–9), permitting
very precise positioning of the needle in lesions andnodes as small as 1 cm and as far as 5 cm from thewall of the gastrointestinal tract.
In a series from the University of California atIrvine, EUS-guided FNA was used to assess submu-cosal gastrointestinal tract lesions and extraluminallymph nodes and masses in 38 patients.43 Of the 46lesions that were sampled, 34 were extraluminal (8periesophageal nodes, 1 mediastinal mass, 6 celiacnodes, 12 pancreatic masses, 1 perigastric mass, 1liver mass, 1 periduodenal node, 2 pericolonic masses,1 perirectal mass, and 1 perirectal node) and 12 weresubmucosal (8 gastric, 3 duodenal, and 1 esophageal).The overall diagnostic accuracy of FNA was 87 per-cent. In patients with known malignant lesions, thesensitivity and specificity of FNA was 91 percentand 100 percent, respectively. Celiac nodes weresuccessfully sampled and diagnostic in 5 (83%) of6 patients. In this study, EUS-guided FNA providedan initial tissue diagnosis of malignancy in 66 per-cent of cancer patients without a previous diagno-sis, and the preoperative stage was changed for 44percent of cancer patients. No complications werereported in this series.
Another group, from Indiana University, recentlyreported their experience with EUS-guided FNA in288 patients with suspected gastrointestinal or medi-astinal masses.44 They reported an 87 percent over-all diagnostic accuracy, an 89 percent sensitivity,and a 100 percent specificity. Within their cohort,subgroup analysis demonstrated that FNA had anaccuracy of 95 percent for the diagnosis of medi-astinal lymph nodes (n = 43) and an accuracy of 85percent for intra-abdominal lymph nodes (n = 13).Their immediate complication rate was 2 percent, all
Figure 2–8. Pentax linear array endoscopic ultrasound scope with fine-needle aspiration (FNA) biopsyneedle (arrow).

38 CANCER OF THE UPPER GASTROINTESTINAL TRACT
related to FNA of pancreatic lesions (2 with bleed-ing and 2 with pancreatitis).
Endoscopic ultrasonography–guided FNA israpidly becoming an important tool in the staging ofpatients with gastrointestinal cancers and othermalignancies (including primary lung cancer) andhas both diagnostic and therapeutic implications.
Bronchoscopy
Bronchoscopy has been performed by some physi-cians as part of the initial preoperative staging assess-ment in patients presenting with esophageal tumorsinvolving the cervical and upper thoracic esophagusto assess for direct tracheobronchial invasion indica-tive of locally advanced stage T4 disease. Bron-choscopy allows direct visualization and biopsy ofany suspicious areas in the trachea or bronchi. If thebronchoscopic examination is positive for direct inva-sion, the patient is no longer a candidate for surgicalresection and may be offered treatment with com-bined chemotherapy and radiation therapy or may beoffered available investigational treatment protocols.
A recent prospective study from Munich, Ger-many, evaluated the diagnostic usefulness of bron-choscopy in the preoperative assessment of 116patients with esophageal cancer, to determine directairway invasion and resectability.45 The investigators
compared the findings of 150 bronchoscopy exami-nations in this cohort with their intraoperative find-ings and surgical pathology. The overall accuracy ofbronchoscopy (with brush cytology and biopsy) fordetermining direct tracheobronchial invasion inpatients who were otherwise surgical candidates was95.8 percent. In addition, the results of bron-choscopy and CT were discordant in 40 percent ofthe patients, with higher specificity and positive pre-dictive value for bronchoscopy than for CT.
To date, we are not familiar with any comparativestudies between bronchoscopy and EUS. At ourinstitution, bronchoscopy is selectively used to assistin the staging of patients with cervical and upperthoracic esophageal malignancies.
Magnetic Resonance Imaging
The role of magnetic resonance imaging (MRI) inthe preoperative staging of esophageal cancer is cur-rently under investigation; however, results to datedo not appear to demonstrate that MRI adds any-thing to CT imaging in this group of patients.
In a recent prospective study from Osaka, Japan,MRI and CT results were compared with surgical orautopsy findings in 31 patients with esophageal can-cer.46 The accuracy rates of MRI and CT for detect-ing regional lymph nodes were 68 percent and 65percent, respectively; for distant nodes, it was 77percent for both modalities. As with CT, MRI has adecreased accuracy for detecting regional lymphnode metastases because it misses normal-sizelymph nodes with metastases. Overall, the accuracyrates for predicting resectability were similar, being87 percent for MRI and 84 percent for CT.
In a study from Milan, Italy, investigators evalu-ated preoperative MRI in assessing direct locore-gional and mediastinal lymph node spread in 32esophageal cancer patients and compared the resultswith surgical pathology.47 They reported accuracyrates of 84 percent for the detection of mediastinalinvasion, 87 percent for detecting tracheobronchialinvasion, 91 percent for detecting aortic invasion,and 72 percent for detecting mediastinal lymph nodemetastases. Despite such good results, the overallaccuracy rate for predicting resectability was only75 percent for MRI in this study.
Figure 2–9. Endoscopic ultrasonography–guided fine-needleaspiration of a malignant mediastinal lymph node in a patient withesophageal cancer. Arrow indicates biopsy needle. (Ln = lymphnode; Ao = aorta.)

Diagnosis and Preoperative Staging of Esophageal Cancer 39
In an earlier study from the University of Michi-gan of the use of MRI for staging esophageal can-cers, MRI and CT findings in 10 esophageal cancerpatients were compared with their operative findingsand surgical pathology, and with the MRI and CTassessments of 20 control patients with normalesophagi.48 Both MRI and CT had low overall accu-racy in staging (40% and 70%, respectively). Theinvestigators attributed this poor accuracy primarilyto the inability of MRI and CT to detect precisedepth of tumor invasion (T stage).
Minimally Invasive Surgical Staging:Laparoscopy, Laparoscopic
Ultrasonography, and Thoracoscopy
Over the past decade, improvements in anesthe-sia and laparoscopic techniques and instrumentationhave fueled the development of minimally invasivesurgery for the management of benign diseases aswell as the diagnosis, staging, and treatment of manytypes of cancers. Adding to successful experienceswith laparoscopic cholecystectomy, surgeons haveworked to develop minimally invasive surgery forcancer management.
Initial studies of laparoscopy in the staging ofupper-gastrointestinal malignancies indicate thatlaparoscopy is highly sensitive for detecting metasta-tic disease, particularly the identification of smalltumor implants on the peritoneal surfaces and liverthat are not detected by conventional imagingmodalities (Figure 2–10, A to C). Laparoscopy alsopermits the evaluation of lymph nodes for metastaticdisease (see Figure 2–10, D). In a study from ourinstitution, laparoscopic exploration in 110 patientswith gastric cancer accurately staged 94 percent ofpatients for metastatic disease, with a sensitivity of84 percent and a specificity of 100 percent.49 Theprevalence rate of metastatic disease is 37 percent inall patients who had been preselected by an abnor-mal CT scan.
A large study of laparoscopic staging in 280patients with cancer of the esophagus and 89patients with gastric cardia cancer demonstratedmetastatic disease to the liver, peritoneum, omen-tum, stomach, and lymph nodes in 52 patients (14%)and to the gastric wall or regional lymph nodes in 36
patients (9.7%).50 The rate of false-negative findingsby laparoscopy in this series was 4.4 percent (2.8%for liver metastases, 1.2% for peritoneal seeding,and 0.4% for omental implants).
A recent advance in minimally invasive surgicalstaging is the addition of laparoscopic ultrasonography(LUS) in the evaluation of patients with upper-gas-trointestinal malignancies (Figure 2–11). One studyfrom Denmark evaluated EUS, laparoscopy, LUS, CT,and transcutaneous ultrasonography in patients withupper-gastrointestinal malignancies.51 Forty-fourpatients with esophageal, gastric, and pancreatic can-cer were studied preoperatively, and the results ofthese examinations (which were used to determine theresectability and curability of the tumors, based onTNM staging) were compared to findings at laparo-tomy. The reported accuracy for predicting resectabil-ity and curability was 91 percent for EUS, 64 percentfor CT and ultrasonography combined, 68 percent forlaparoscopy alone, 95 percent for LUS alone, and 95percent for EUS and LUS combined.
In a study from the University of Amsterdam, theNetherlands, laparoscopy and LUS was performedin 233 patients with upper-gastrointestinal tumors(tumors of the esophagus, gastric cardia, liver, bileduct, and pancreas) believed to be surgicallyresectable after conventional preoperative staging.52
Of the 64 patients with esophageal or gastric cardiacancers (preoperative evaluation included EUS),findings at laparoscopy prevented laparotomy in 4patients (6%) because of the detection of unsus-pected metastatic disease.
The application of laparoscopic techniques andinstruments in the chest has resulted in advances invideo-assisted thoracoscopy and in the application ofthoracoscopy to the surgical staging of esophagealcancer. Thoracoscopy allows the direct visualizationof the entire thoracic esophagus, the accurate assess-ment of tumor invasion into the adventitia and adja-cent mediastinal structures, and the evaluation andsampling of regional lymph nodes for histology.53 Itcan also detect occult pleural and pulmonary metas-tases. However, to assess for intra-abdominal disease(including liver metastases and peritoneal implants)and to sample perigastric and celiac lymph nodes,thoracoscopy must be combined with diagnosticlaparoscopy. Furthermore, tumors of the esopha-

40 CANCER OF THE UPPER GASTROINTESTINAL TRACT
gogastric junction also require a combined laparo-scopic approach to completely evaluate the inferioraspect of the primary tumor and to assess for intra-abdominal disease.
A study from the University of Pittsburgh com-pared the accuracy of EUS with thoracoscopic andlaparoscopic staging in evaluating lymph nodemetastases in 26 patients with surgically resectableesophageal cancer (24 patients with adenocarcinomaof the esophagogastric junction and 2 with squamouscell carcinoma of the midthoracic esophagus).54 In 5patients (19%), complete assessment by EUS was
not possible due to high-grade malignant stricturethat did not allow passage of the scope; in 3 of these5 patients, laparoscopy and thoracoscopy revealedN1 disease. Endoscopic ultrasonography detected N1disease in 13 patients, and laparoscopy and thora-coscopy confirmed N1 disease in 12 (92%) of these13 patients. The sensitivity and specificity of EUSfor nodal evaluation were 65 percent and 66 percent,respectively. The sensitivity of EUS decreased to 44percent when EUS was used for detecting occultmetastatic disease in lymph nodes less than 1 cm indiameter. No disease staged as T3 by EUS was up-
Figure 2–10. A, Solitary liver metastasis, shown at laparoscopy. (M = liver metastasis; L = liver; G = grasper [instrument diameter = 0.3 cm];D = diaphragm, TL = triangular ligament.) (×15 original magnification.) (Courtesy of Dr. Tracey Weigel.) B, Multiple small metastases involvingthe right lobe of the liver, shown at laparoscopy. Arrow indicates falciform ligament. (M = liver metastasis; L = liver.) (×15 original magnifica-tion.) (Courtesy of Dr. Tracey Weigel.) C, Multiple small (< 0.1cm in diameter) metastatic nodules studding the peritoneal surface in the regionof the gastrohepatic ligament, shown at laparoscopy. Arrows indicate instrument port (port diameter = 0.5 cm). (M = metastatic peritoneal nod-ule; S = stomach; D = diaphragm.) (×15 original magnification.) (Courtesy of Dr. Tracey Weigel.) D, Metastatic disease to a left gastric arterylymph node, shown at laparoscopy. Black arrows indicate lymph node, white arrows indicate left gastric artery. (RP = retroperitoneum; RC =right crus of diaphragm; D = diaphragm.) (×15 original magnification.) (Courtesy of Dr. Tracey Weigel.)
A B
C D

Diagnosis and Preoperative Staging of Esophageal Cancer 41
staged to T4 by laparoscopy or thoracoscopy. How-ever, whereas EUS did not detect distant metastasesin any patient, laparoscopy identified M1 disease dueto liver metastases in 4 (15%) of 26 patients.
In a more recent study from the Pittsburgh group,staging with laparoscopy and thoracoscopy wascompared to conventional staging with CT and EUSin 53 patients with esophageal cancer.55 In thiscohort, after CT and EUS staging (1 case as carci-noma in situ, 1 case as stage I, 23 as stage II, 20 asstage III, and 8 as stage IV disease), laparoscopy andthoracoscopy changed the stage in 17 patients(32%), down-staging disease in 10 patients and up-staging disease in 7 patients.
In a study from the University of Rotterdam‘Dijkigt’ in the Netherlands, conventional preopera-tive imaging (including EUS) was compared withlaparoscopy and LUS in staging 40 patients withesophageal cancer and 20 patients with gastric cardiacancer.56 In 1 (2.5%) of 40 patients with esophagealcancer, laparoscopy detected M1 disease due to aliver metastasis. Of the 20 patients with gastric car-dia cancer, laparoscopy detected 4 (20%) with M1disease (peritoneal seeding in 3 and omental metas-tases in 1) whereas LUS detected an additional 4(20%) (liver metastasis in 2 and celiac lymph nodemetastasis in 2), demonstrating the detection of oth-erwise unsuspected M1 disease in 8 (40%) of the 20patients by laparoscopy and LUS combined.
Minimally invasive surgical staging with thora-coscopy and laparoscopy for patients with cancers ofthe esophagus and the esophagogastric junctionoffers the ability to detect a small but significantnumber of patients with distant M1 disease thatwould not be detected by conventional preoperativeimaging studies. In addition, direct tissue samplingof lymph node and peritoneal lesions increases thespecificity for finding such abnormalities. Theimproved accuracy of preoperative staging offeredby these procedures may improve the selection ofpatients for surgery and increase the curative resec-tion rates at some hospitals while reducing the num-ber of unnecessary laparotomies.
There are, however, limitations and risks relatedto thoracoscopy and laparoscopy staging proce-dures. Both procedures are invasive and are per-formed in an operating room under general anesthe-
sia, which is associated with its own related costsand potential complications. In a small number ofpatients, laparoscopy may not be successful due toadhesions from prior abdominal surgery. There is apotential risk, albeit small, of tumor spillage andport site metastases related to these procedures. Inaddition, following thoracoscopy, a chest tube mustbe inserted, which requires the inconvenience andcost of a limited hospital stay for management andpatient recovery.
The University of Pittsburgh group reported itsprocedure-related morbidities associated with thora-coscopic and laparoscopic staging.54 In this study, 8(30.8%) of the 26 patients developed “minor com-plications” (2 patients with prolonged ileus, 2 withatelectasis, 2 with urinary retention, and 2 with portsite infections). One patient (3.8%) experienced a“major complication” (a small-bowel obstructionfollowing laparoscopy). Thus, in this study, the over-all rate of complications associated with thora-coscopy and laparoscopy for staging was 34.6 per-cent (9 of 26). Furthermore, the Pittsburgh group
Figure 2–11. Laparoscopic ultrasonography (LUS) of a livermetastasis in a patient with an esophagogastric-junction tumor (M =metastasis; L = liver.) (Courtesy of Dr. Tracey Weigel.)

42 CANCER OF THE UPPER GASTROINTESTINAL TRACT
also reported its operating-room times and thelength of hospital stays. The average operating-roomtime was 4.2 hours (a range of 1 to 6 hours), and theaverage length of hospital stay was 3.4 days (a rangeof 1 to 11 days). The authors did note, however, thatboth of these times decreased during the course oftheir study; for the last 10 patients, the average oper-ating-room time was 3.6 hours and the average hos-pital stay was 1.8 days.
A potential role for minimally invasive preopera-tive staging is to complement the use of EUS or CTfor properly stratifying (on the basis of optimal stag-ing) those patients who are candidates for therapy inthe context of a clinical trial.
Positron Emission Tomography
Positron emission tomography (PET) is a relativelynew imaging modality that makes use of the abilityto visualize tumors by virtue of differences in meta-bolic activity between tumor and normal tissue.Tumor tissues are generally more metabolicallyactive than normal non-neoplastic tissues and haveincreased glycolytic activity. The administration of[18F]-fluoro-2-deoxy-D-glucose (FDG) to an individ-ual with cancer therefore results in a greater uptakeof FDG by the tumor tissue than by most normal tis-sues. Once FDG enters cancer cells, it is phosphory-lated and trapped within the cells, thereby renderingthe cells radioactive. This enables cancerous tumorsto be detected by the radioactivity emitted from thetrapped radiolabeled FDG. Tumors of sufficient sizeand with a sufficient uptake of FDG are thereforereadily detected by using a gamma camera. Throughthe technique of tomographic imaging, whole-bodyPET can provide detailed images that can be super-imposed on conventional CT scans, correlating theareas of increased radioisotope activity with anatomicsites of disease (Figure 2–12).
Imaging by PET is currently under investigationto determine its potential role in preoperative stag-ing for esophageal cancer. In a study from the Uni-versity of Pittsburgh, PET was performed in 35patients with esophageal cancer, and results werecompared with surgical findings and pathology.57
For the detection of locoregional lymph node metas-tases, PET demonstrated a sensitivity of 45 percent,
a specificity of 100 percent, and an overall accuracyof 48 percent. There were 11 false-negative PETstudy results for small (mean diameter of 0.52 cm),intracapsular locoregional nodal metastases. Fordetecting distant metastases, PET showed a sensitiv-ity of 88 percent, a specificity of 93 percent, and anaccuracy of 91 percent. It detected nine sites of dis-tant metastases not identified by conventional scan-ning. One false-negative PET study result occurredin a patient with a small (0.2 cm) liver lesion. Theinvestigators concluded that current PET technologywas not accurate enough to detect small locore-gional nodes. Its potential benefit in staging patientswith esophageal cancer may be its ability to identifyunsuspected distant metastases, which it accom-plished in up to 20 percent of study patients whowere found to be falsely negative for M1 disease byconventional preoperative staging modalities.
In a prospective study from Amsterdam, PETwas evaluated in 26 patients with esophageal andesophagogastric cancers and was compared with CTand surgical findings, primarily to determine itsability to stage metastatic disease.58 The rate of visu-alization of the primary tumor was 81 percent withCT and 96 percent with PET. Neither CT nor PETwas good at determining the depth of wall penetra-tion (T stage). For N staging, the sensitivity of CTwas 38 percent, its specificity was 100 percent, andits overall accuracy was 62 percent whereas PETshowed a sensitivity of 92 percent, a specificity of88 percent, and an accuracy of 90 percent. In regardto determining M stage, CT detected distant metas-tases in 5 patients, with one false-positive liverhemangioma, and PET detected distant metastasesin 8 patients, with one false-positive in the supra-clavicular area (that was not confirmed on subse-quent cytology assessment). The overall diagnosticaccuracy for determining resectability was 65 per-cent for CT and 88 percent for PET.
In a more recent report, the investigators at theUniversity of Pittsburgh updated their data todescribe their prospective experience with 100 PETscans in 91 patients with esophageal cancer.59 Theycompared PET with CT, bone scan, and surgicalfindings. In this study, a total of 70 distant metas-tases were confirmed in 39 patients by minimallyinvasive surgical staging or clinical correlation.

Diagnosis and Preoperative Staging of Esophageal Cancer 43
Positron emission tomography identified 51 metas-tases in 27 of the 39 cases, demonstrating a sensitiv-ity of 69 percent, a specificity of 93.4 percent, andan accuracy of 84 percent, whereas CT detected only26 metastases in 18 of the 39 cases, indicating a sen-sitivity of 46.1 percent, a specificity of 73.8 percent,and an accuracy of 63 percent (p < .01).
Another recent prospective comparison of PETwith conventional staging modalities for preoperativeassessment of esophageal cancer was reported fromLeuven, Belgium.60 The authors evaluated 43patients with esophageal cancer and 31 with esopha-gogastric cancer and compared their findings withCT and EUS findings. Positron emission tomogra-phy detected the primary tumors in 70 (95%) of 74patients and gave false-negative results in 4 patientswith early-stage T1 lesions. In the 34 patients (46%)with advanced (stage IV) disease, PET demonstrateda higher accuracy rate (82%) for diagnosing stage IVdisease than did the combination of both CT andEUS, which had an accuracy of 64 percent (p = .004).Positron emission tomography also demonstratedadditional benefit in 16 patients (22%) by up-staging11 patients (15%) and by down-staging 5 patients
(7%). In the 39 patients (53%) who underwent a 2- or3-field lymphadenectomy, lymph node metastaseswere detected in 21 local and 35 regional or distantnodes. For the detection of local lymph node metas-tases, PET demonstrated a lower sensitivity (33% ascompared to EUS at 81% [p = .027]) but a higher,although not statistically significant, specificity(89%, compared to 67% for EUS). For the detectionof regional and distant nodal metastases, PETdemonstrated a sensitivity of 46 percent, similar tothat of the combination of CT and EUS (43%) (p =not significant); however, its specificity was 98 per-cent, compared to 90 percent for the combination ofCT and EUS (p = .025).
Positron emission tomography for staging thesecancers remains investigational, but further studymay prove it to be a useful adjunct as a preoperativestaging tool.
Computed Tomography of the Head andRadionucleotide Bone Scan
Some clinicians routinely perform CT of the headand radionucleotide bone scan imaging in patients
Figure 2–12. Positron emission tomography scans A, A tumor (t) of the gastroesophageal junction and fundus, withmetastatic spread to celiac lymph nodes (confirmed by endoscopic ultrasonography–guided fine-needle aspiration) insame patient shown in Figure 2–6G) (arrow indicates celiac lymph node). B, A proximal esophageal tumor (long arrow)with metastatic spread to a right paraesophageal lymph node (short arrow).
A B

44 CANCER OF THE UPPER GASTROINTESTINAL TRACT
with newly diagnosed esophageal carcinoma, on therationale that it is crucial to rule out distant metas-tases (M1 disease) in these patients.
In a study from the University of Michigan, therecords of 838 patients with esophageal cancer wereretrospectively reviewed to assess the frequency andlocation of metastatic disease at initial presentation.61
In this cohort, 147 patients (18%) had M1 disease. In110 (75%) of these 147 patients, distant metastaticdisease was detected preoperatively by conventionalimaging or clinical examination; in 102 (69%) of the147 patients, this was detected by CT of the chest orabdomen. The most common site of detected distantmetastases was in the intra-abdominal lymph nodes(45%), followed by the liver (35%), lungs (20%),cervical/supraclavicular nodes (18%), bone (9%),adrenals (5%), peritoneum (2%), and brain (2%), andby the stomach, pancreas, pleura, skin/body wall,pericardium, and spleen (each 1%). In this study, nei-ther bone scan nor CT of the head detected unsus-pected metastatic disease in any case staged as M0by chest and abdominal CT.
In a prospective study that compared several dif-ferent imaging modalities for the preoperative stag-ing assessment of 33 patients with esophageal can-cer,62 radionucleotide bone scan detected a metastaticlesion in one case that was missed by CT. Thus, thisstudy recommended the use of bone scan, along withCT and bronchoscopy, in the standard preoperativeevaluation of these patients.
SUMMARY
To provide a reproducible and practical means of cat-egorizing the extent of disease, the staging of malig-nancies has become internationally standardized.Accurate preoperative staging of a newly diagnosedesophageal cancer is very important in the planningof treatment but becomes most important in centerswhere treatment may vary according to stage. In thepast, staging was performed surgically, but recenttechnologic advances in radiographic and minimallyinvasive imaging now permit accurate nonsurgicalstaging in most patients with esophageal cancer.
Following a tissue confirmation of malignantdisease (most commonly performed by UGIendoscopy with biopsy), we recommend that the ini-
tial staging evaluation be performed by CT of thechest and abdomen, primarily to rule out distantmetastatic disease. In the absence of radiographicevidence of metastatic disease found by CT, EUSshould be performed to determine the depth oftumor invasion into the esophageal wall and to iden-tify any locoregional lymph node metastases.Although still investigational, PET seems to addimportant information about distant metastatic dis-ease undetected by CT and EUS, and this modalitymay someday replace CT in the staging of gross dis-tant metastases. Bronchoscopy remains important inthe evaluation of upper and midthoracic esophagealtumors, to rule out locally advanced stage T4 diseasedue to direct tracheobronchial invasion, but thiscould be obviated by the use of EUS. The role oflaparoscopy in staging tumors of the esophagogas-tric junction is currently being investigated, but itsrole in the assessment of cervical, upper thoracic,and middle thoracic esophageal cancer is minimal.Currently, there does not seem to be a role for bonescan, CT of the head, or MRI.
At this time, we feel that EUS provides accuratelocoregional T and N staging in esophageal andesophagogastric-junction tumors, plays a vital rolein the triage of patients to surgery or neoadjuvantchemotherapy protocols, but remains complemen-tary to the use of CT. The recent addition of EUS-guided FNA offers a significant improvement in theability of EUS to accurately determine metastaticlymph node involvement. Further improvements inPET are likely to result in greater reliance on thismodality for preoperative staging.
The approach to the staging of esophageal cancerat different institutions varies because of the limitedavailability of different imaging modalities such asEUS and PET. However, as more individuals aretrained in EUS, and as the approach to treatingesophageal cancer becomes more tailored to stage,EUS and PET are likely to become the standards inthe staging of patients with esophageal cancer.
REFERENCES
1. Pera M, Cameron AJ, Trastek VF, et al. Increasing incidenceof adenocarcinoma of the esophagus and esophagogastricjunction. Gastroenterology 1993;104:510–3.
2. Blot WJ, Devesa SS, Kneller RW, Fraumeni JF. Rising inci-

Diagnosis and Preoperative Staging of Esophageal Cancer 45
dence of adenocarcinoma of the esophagus and gastriccardia. JAMA 1991;265:1287–9.
3. Fleming ID, Cooper JS, Henson DE, et al., editors. AJCCcancer staging manual. 5th ed. American Joint Committeeon Cancer. Philadelphia: Lippincott-Raven; 1997.
4. Siewert JR, Stein HJ. Classification of adenocarcinoma of theoesophagogastric junction. Br J Surg 1998;85:1457–9.
5. Siewert JR, Stein HJ. Adenocarcinoma of the gastroe-sophageal junction. Classification, pathology and extentof resection. Dis Esophagus 1996;9:173–82.
6. Weston AP, Krmpotich PT, Cherian R, et al. Prospective eval-uation of intestinal metaplasia and dysplasia within thecardia of patients with Barrett’s esophagus. Dig Dis Sci1997;42:597–602.
7. Aikou T, Shimazu H. Difference in main lymphatic pathwaysfrom the lower esophagus and gastric cardia. Jpn J Surg1989;19:290–5.
8. Tachimori Y, Kato H, Watanabe H, et al. Difference betweencarcinoma of the lower esophagus and the cardia. World JSurg 1996;20:507–10.
9. Moss AA, Koehler RE, Margulis AR. Initial accuracy ofesophagograms in detection of small esophageal carci-noma. AJR Am J Roentgenol 1976;127:909–13.
10. Glazer GM, Gross BH, Quint LE, et al. Normal mediastinallymph nodes: number and size according to AmericanThoracic Society mapping. AJR Am J Roentgenol1985;144:261–5.
11. Thompson WM, Halvorsen RA, Foster WL Jr, et al. Com-puted tomography for staging esophageal and gastroe-sophageal cancer: reevaluation. AJR Am J Roentgenol1983;141:951–8.
12. Lea JW 4th, Prager RL, Bender HW Jr. The questionable roleof computed tomography in preoperative staging ofesophageal cancer. Ann Thorac Surg 1984;38:479–81.
13. Picus D, Balfe DM, Koehler RE, et al. Computed tomogra-phy in the staging of esophageal carcinoma. Radiology1983;146:433–8.
14. Quint LE, Glazer GM, Orringer MB, Gross BH. Esophagealcarcinoma: CT findings. Radiology 1985;155:171–5.
15. Becker CD, Barbier P, Porcellini B. CT evaluation of patientsundergoing transhiatal esophagectomy for cancer. J Com-put Tomogr 1986;10:607–11.
16. Aibe T, Fuji T, Okita K, Takemoto T. A fundamental study ofnormal layer structure of the gastrointestinal wall visual-ized by endoscopic ultrasonography. Scand J Gastroen-terol 1986;21 Suppl 123:6–15.
17. Tio TL, Tytgat GNJ. Endoscopic ultrasonography of normaland pathologic upper gastrointestinal wall structure: com-parison of studies in vivo and in vitro with histology.Scand J Gastroenterol 1986;21 Suppl 123:27–33.
18. Kimmey MB, Martin RW, Haggitt RC, et al. Histologic cor-relates of gastrointestinal ultrasound images. Gastroen-terology 1989;96:433–41.
19. Botet JF, Lightdale CJ, Zauber AF, et al. Preoperative stagingof esophageal cancer: comparison of endoscopic US anddynamic CT. Radiology 1991;181:419–25.
20. Aibe T, Ito T, Yoshida T. Endoscopic ultrasonography oflymph nodes surrounding the upper GI tract. Scand J Gas-troenterol 1986;21 Suppl 123:164–9.
21. Tio TL, Cohen P, Coene PP, et al. Endosonography and com-puted tomography of esophageal carcinoma: preoperativeclassification compared to the new (1987) TNM system.Gastroenterology 1989;96:1478–86.
22. Lightdale CJ. Practice guidelines: esophageal cancer. Am JGastroenterol 1999;94:20–9.
23. Rösch T. Endosonographic staging of esophageal cancer: areview of literature results. Gastrointest Endosc Clin NAm 1995;5:537–47.
24. Dittler HJ, Siewert JR. Role of endoscopic ultrasonographyin esophageal carcinoma. Endoscopy 1993;25:156–61.
25. Grimm H, Binmoeller K, Hamper K, et al. Endosonographyfor preoperative locoregional staging of esophageal andgastric cancer. Endoscopy 1993;25:224–30.
26. Hordijk ML, Zander H, van Blankenstein M, Tilanus HW.Influence of tumor stenosis on the accuracy ofendosonography in preoperative T staging of esophagealcancer. Endoscopy 1993;25:171–5.
27. Kalantzis N, Kallimanis G, Laoudi F, et al. Endoscopic ultra-sonography and computed tomography in preoperative(TNM) classification of oesophageal carcinoma[abstract]. Endoscopy 1992;24:653.
28. Nobre-Leito C, Santos AA, Mides Correia J, Costra Mira F.Esophageal carcinoma: preoperative staging with endo-sonography [abstract]. Endoscopy 1992;24 Suppl 1:379.
29. Rösch T, Lorenz R, Zenker K, et al. Local staging and assess-ment of resectability in carcinoma of esophagus, stomachand duodenum by endoscopic ultrasonography. Gastroin-test Endosc 1992;38:460–7.
30. Souquet JC, Napoléon B, Pujol B, et al. Endosonography-guided treatment of eosphageal carcinoma. Endoscopy1992;24 Suppl 1:324–8.
31. Grimm H. Binmoeller KF, Hamper K, Soehendra N. Accuracyof endoscopic ultrasound (EUS) in preoperative staging ofesophageal carcinoma [abstract]. Endoscopy 1992;24:652.
32. Fok M, Cheng SWK, Wong J. Endosonography in patientselection for surgical treatment of esophageal carcinoma.World J Surg 1992;16:1098–103.
33. Kallimanis GE, Gupta PK, Al-Kawas FH, et al. Endoscopicultrasound for staging cancer, with or without dilation, isclinically important and sage. Gastrointest Endosc 1995;41:540–6.
34. Yoshikane H, Tsukamoto Y, Niwa Y, et al. Superficialesophageal carcinoma: evaluation by endoscopic ultra-sonography. Am J Gastroenterol 1994;89:702–7.
35. Souquet JC, Napoléon B, Pujol B, et al. Endoscopic ultra-sonography in the preoperative staging of esophageal can-cer. Endoscopy 1994;26:764–6.
36. McLoughlin RF, Cooperberg PL, Mathieson JR, et al. Highresolution endoluminal ultrasonography in the staging ofesophageal carcinoma. J Ultrasound Med 1995;14:725–30.
37. Catalano MF, Sivak MV Jr, Rice T, et al. Endosonographicfeatures predictive of lymph node metastasis. GastrointestEndosc 1994;409:442–6.
38. Dittler HJ, Fink U, Siewert JR. Response to chemotherapy inesophageal cancer. Endoscopy 1994;26:769–71.
39. Ginsberg GG, Al-Kawas FH, Nguyen CC, et al. Endoscopicultrasound evaluation of vascular involvement inesophageal cancer: a comparison with computed tomog-raphy [abstract]. Gastrointest Endosc 1993;39:276.

46 CANCER OF THE UPPER GASTROINTESTINAL TRACT
40. Chak A, Canto M, Gerdes H, et al. Prognosis of esophagealcancers preoperatively staged to be locally invasive (T4)by endoscopic ultrasound (EUS): a multicenter retrospec-tive cohort study. Gastrointest Endosc 1995;42:501–6.
41. Van Dam J. Endoscopic evaluation of the patient withesophageal carcinoma. In: Wanebo HJ, editor. Surgery forgastrointestinal cancer: a multidisciplinary approach.Philadelphia: Lippincott-Raven Publishers; 1997.
42. Van Dam J, Rice TW, Catalano MF, et al. High-grade mal-ignant stricture is predictive of esophageal tumor stage:risks of endosonographic evaluation. Cancer 1993;71:2910–7.
43. Chang KJ, Datz KD, Durbin TE, et al. Endoscopic ultra-sound-guided fine-needle aspiration. Gastrointest Endosc1994;40:694–9.
44. Gress FG, Hawes RH, Savides TJ, et al. Endoscopic ultra-sound-guided fine-needle aspiration biopsy using lineararray and radial scanning endosonography. GastrointestEndosc 1997;45:243–50.
45. Riedel M, Hauck RW, Stein HJ, et al. Preoperative broncho-scopic assessment of airway invasion by esophageal can-cer: a prospective study. Chest 1998;113:687–95.
46. Takashima S, Takeuchi N, Shiozaki H, et al. Carcinoma ofthe esophagus: CT vs. MR imaging in determiningresectability. AJR Am J Roentgenol 1991;156:297–302.
47. Petrillo R, Balzarini L, Bidoli P, et al. Esophageal squamouscell carcinoma: MRI evaluation of mediastinum. Gas-trointest Radiol 1990;15:275–8.
48. Quint LE, Glazer GM, Orringer MB. Esophageal imaging byMR and CT: study of normal anatomy and neoplasms.Radiology 1985;156:727–31.
49. Burke EC, Karpeh MS, Conlon KC, Brennan MF.Laparoscopy in the management of gastric adenocarci-noma. Ann Surg 1997;225:262–7.
50. Dagnini G, Caldironi MW, Marin G, et al. Laparoscopy inabdominal staging of esophageal carcinoma: report of369 cases. Gastrointest Endosc 1986;32:400–2.
51. Mortensen MB, Scheel-Hincke JD, Madsen MR, et al. Com-bined endoscopic ultrasonography and laparoscopic ultra-sonography in the pretherapeutic assessment of resectabil-
ity in patients with upper gastrointestinal malignancies.Scand J Gastroenterol 1996;31:1115–9.
52. van Dijkum EJMN, de Wit LT, van Delden OM, et al. Theefficacy of laparoscopic staging in patients with uppergastrointestinal tumors. Cancer 1997;79:1315–9.
53. Sugarbaker DJ, Jaklitsch MT, Liptay MJ. Thoracoscopic stag-ing and surgical therapy for esophageal cancer. Chest1995;107:218S–23S.
54. Luketich JD, Schauer P, Landreneau R, et al. Minimally inva-sive surgical staging is superior to endoscopic ultrasoundin detecting lymph node metastases in esophageal cancer.J Thorac Cardiovasc Surg 1997;114:817–23.
55. Luketich JD, Meehan M, Nguyen NT, et al. Minimally inva-sive surgical staging for esophageal cancer. Surg Endosc2000;14:700–2.
56. Romijn MG, van Overhagen H, Spillenaar Bilgen EJ, et al.Laparoscopy and laparoscopic ultrasonography in stagingof oesophageal and cardial carcinoma. Br J Surg 1998;85:1010–2.
57. Luketich JD, Schauer PR, Meltzer CC, et al. Role of positronemission tomography in staging esophageal cancer. AnnThorac Surg 1997;64:765–9.
58. Kole AC, Plukker JT, Nieweg OE, Vaalburg W. Positron emis-sion tomography for staging of oesophageal and gastroe-sophageal malignancy. Br J Cancer 1998;78:521–7.
59. Luketich JD, Friedman DM, Weigel TL, et al. Evaluation ofdistant metastases in esophageal cancer: 100 consecutivepositron emission tomography scans. Ann Thorac Surg1999;68:1133–6.
60. Flamen P, Lerut A, Van Cutsem E, et al. Utility of positronemission tomography for the staging of patients withpotentially operable esophageal carcinoma. J Clin Oncol2000;18:3202–10.
61. Quint LE, Hepburn LM, Francis IR, et al. Incidence and dis-tribution of distant metastases from newly diagnosedesophageal carcinoma. Cancer 1995;76:1120–5.
62. Inculet RI, Keller SM, Dwyer A, Roth JA. Evaluation of non-invasive tests for the preoperative staging of carcinoma ofthe esophagus: a prospective study. Ann Thorac Surg1985;40:561–5.












![[Ghiduri][Cancer]Esophageal Cancer](https://img.pdfslide.net/doc/110x75/577cc7761a28aba711a10585/ghiduricanceresophageal-cancer.jpg)