Embed Size (px)
Citation preview

Turk J Med Sci2007; 37 (3): 157-165© TÜB‹TAKE-mail: [email protected]
157
ORIGINAL ARTICLE
Clinical Features, EEG Findings and Outcome inPatients with Bilateral Periventricular Nodular
Heterotopia and Epilepsy
Aim: To review the clinical, electrophysiological and neuroimaging data of eight adult patients (4F/4M) withepilepsy and bilateral periventricular nodular heterotopia (PNH) after a long duration of follow-up.
Materials and Methods: The clinical charts were reviewed for demographic and clinical features, seizuretypes and frequency, treatment and prognosis of all eight patients who were under follow-up by one of theauthors (SS). The recordings of video-EEG monitoring with scalp electrodes in five patients and routine EEGsin all patients were reviewed.
Results: The clinical semiology was in accord with seizures originating from temporal lobe region in fourpatients, while an extratemporal onset was assumed in the others (in one with additional temporal seizures).Interictal EEGs were normal in one patient, who was diagnosed as having psychogenic nonepileptic seizure.Abnormalities seen in interictal EEGs were bilateral independent temporal focus in three, unilateralepileptiform abnormalities in two, and generalized 3 cyc/sec discharges mimicking idiopathic generalizedepilepsies in two patients. Only two patients’ MRI revealed bilaterally contiguous heterotopic nodules(symmetric and asymmetric type) and, interestingly, these two patients did not have intractable seizures whilethe other six patients with bilateral, asymmetric and noncontiguous heterotopic nodules suffered fromintractable seizures.
Conclusions: Patients with bilateral PNH have different clinical features, EEG findings and extension of theheterotopic nodules. These patients may be misdiagnosed as having idiopathic generalized epilepsy, temporallobe epilepsy or even psychogenic nonepileptic seizures without high quality MRI because of the misleadingseizure semiology and interictal-ictal EEG findings. Seizures are usually drug-resistant but the patients whohave diffuse symmetric or asymmetric contiguous heterotopic nodules may have good prognosis.
Key Words: Nodular heterotopia, periventricular heterotopia, subependymal heterotopia, epilepsy, EEG,MRI, prognosis
Bilateral Periventriküler Noduler Heterotopi ve Epilepsi - Klinik, ElektrografikÖzellikler ve Prognoz
Amaç: Epilepsi tan›s› alan ve bilateral periventriküler nodüler heterotopi (PNH) saptanan sekiz eriflkin hastan›n(4F/4M) klinik, elektrofizyolojik, nörogörüntüleme ve prognostik özelliklerini uzun süreli takip sonras›ndade¤erlendirmek.
Yöntem ve Gereç: Olgular›n demografik ve klinik özellikleri, nöbet semiyolojileri, tedavi protokolleri ve klinikizlem özellikleri hastane takip dosyalar› incelenerek elde edildi. Rutin EEG incelemesi tüm olgularda yap›lm›fl,ayr›ca befl olgu video-EEG monitorizasyon incelemesi ile de¤erlendirilmifltir.
Bulgular: Klinik semiyoloji dört hastada temporal lob, dört hastada ise ekstratemporal özellikli nöbetler (birolguda efllik eden temporal nöbetler de vard›) ile uyumlu bulundu. ‹nteriktal EEG de üç hastada bilateralba¤›ms›z temporal odak, iki olguda unilateral epileptiform bozukluk, ve iki olguda idyopatik jeneralizeepilepsiye benzer jeneralize 3 Hz desarjlar› gözlendi. Baflvuru öncesinde psikojenik nonepileptik nöbet tan›s›alm›fl bir olguda normal olarak de¤erlendirildi. ‹ki hastada MRG de bilateral devaml›l›k gösteren heterotopiknodüller (simetrik ve asimetrik tipte) gözlendi, bu olgularda nöbetler ilaca dirençli de¤ildi. Di¤er hastalardabilateral asimetrik ve devaml›l›k göstermeyen nodüller gözlendi, bu olgularda nöbetler ilaca dirençliydi.
Sonuç: Bilateral PNH olgular›nda klinik bulgular, EEG bulgular› ve heterotopik nodüllerin yay›l›m› farkl›l›kgösterir. Bu hastalar idiyopatik jeneralize epilepsi, temporal lob epilepsisi ya da psikojenik non-epileptik nöbettan›lar›n›, ayr›nt›l› MRG incelemeleri yap›lmad›¤›nda alabilirler. Nöbetler genellikle ilaca dirençlidir, ancak diffuzsimetrik ya da asimetrik devaml›l›k gösteren olgularda prognoz iyi olabilir.
Anahtar Sözcükler: Nodüler heterotopi, perivetriküler heterotopi, subepandimal heterotopi, epilepsi, EEG,MRG, prognoz
Aysun ÜNAL
Serap SAYGI
Department of Neurology,Faculty of Medicine,Hacettepe University,06100 S›hhiye, Ankara - TURKEY
Received: November 06, 2006Accepted: May 11, 2007
Correspondence
Serap SAYGIDepartment of Neurology,
Faculty of Medicine,Hacettepe University,
06100 S›hhiye, Ankara - TURKEY

Introduction
Heterotopias are malformations of corticaldevelopment characterized by the presence of apparentlynormal brain cells in abnormal position. Neurons thatpopulate the adult cortex first occur in the germinal layerof the ventricular zone, and to get to their proper adultlocation, most cerebral cortical neurons migrate alongtracks of radially oriented glial cells. In periventricularnodular heterotopia (PNH), there is a total failure ofmigration of some neurons. These neurons remain in theventricular zone as clumps or nodules of differentiatedneurons, while the remainder of the neurons migratenormally and completely to form the proper six-layeredcortex (1-4).
An X-linked dominant inheritance has been establishedfor familial bilateral PNH in females, a condition alsocharacterized by a high incidence of spontaneousmiscarriages particularly in male fetuses. Linkage analysismapped this disorder to Xq28, and filamin 1 gene wasidentified as the related gene (5-7). Sporadic cases ofbilateral PNH both in females and males have also beendescribed (8,9). Nodular heterotopias are also observedin other conditions with multiple causative genes, andenvironmental etiologies are suggested (10).
Magnetic resonance imaging (MRI) is the best imagingmodality to disclose PNH and describe the morphology,extension, and boundaries of the malformation, and itmay display associated cortical dysplasias or other brainmalformations. High resolution MRI has revolutionizedthe study of cortical dysplasia by showing how importantthese conditions are as a cause of epilepsy (11-14). MRIfeatures of PNH are sufficient to identify it as a distinctneuronal migration disorder. However, while manyrecent papers have described the advances ofneuroradiological aspects of cortical malformations, fewstudies have investigated the clinical, prognostic and long-term follow-up of patients with these malformations(10,14-16).
In this study, we investigated the clinical,neurophysiological, and neuroimaging features of eightepilepsy patients with bilateral PNH, focusing on thecourse and prognosis of epilepsy in this group of corticalmalformations.
Materials and Methods
Six of the eight patients included in the study werereferred to the epilepsy center of our hospital because ofdrug-resistant seizures. The presence of PNH wasassessed by means of MRI in all cases (Figure 1). Thepatients were characterized by bilateral multiple nodulesof heterotopic gray matter in the subependymal region ofventricles.
The clinical histories of the patients were analyzedwith particular attention paid to a family history ofepilepsy, spontaneous miscarriages, early infant or childdeaths and other cardiac, renal or neurological diseases.The presence of risk factors for brain damage duringprenatal or perinatal life; their motor, mental and speechdevelopment; their neurological status; and their mentallevel were all questioned in detail. The epileptic histories,the age and modality of seizure onset, and the semiologyof the seizures were carefully reviewed. Theelectroclinical features and clinical course of the epilepsyas well as the response to different antiepileptic drugtherapies were recorded.
The routine EEG was recorded after the 10-20international systems of electrode positioning with 8-channel Grass EEG machine. Long-term video EEGmonitoring, with 32 channels, and added T1-T2 and ECGelectrodes, could be performed in five patients(Telefactor Beehive or Millennium). Videotapes and ictal-interictal EEGs were also reviewed in detail. The MRIscans were made at a field strength of 1.5 or 3.0 Tesla(including T1-weighted sagittal and transverse, T2-weighted and FLAIR transverse and coronal, 3B T1-weighted gradient echo coronal examinations) with1.5mm slices.
Results
The studied group consisted of eight patients (4males, 4 females; age range: 20 to 59 years).Consanguineous marriage was present in five patients.Miscarriage or early child death was reported in threefamilies. Family history of epilepsy was not reported inany patient. Perinatal risk factors were reported in onepatient with a threatened abortion at the third month ofpregnancy, and she was delivered via caesarian section(Case 1). All patients except one (Case 5) had normalacquisition of early developmental milestones. Only Case5 also had neurological deficit, dysmorphism and severe
158
ÜNAL, A et al. Periventricular Nodular Heterotopia and Epilepsy Turk J Med Sci

mental retardation with chromosomal abnormality. Threepatients had a junior high school diploma, three had asenior high school diploma and one had a universitydegree.
Median age at onset of recurrent seizures was 15years (range: 6 months – 24 years). Complex partialseizures were reported by seven patients, but secondarygeneralized seizures in five patients. Falling attacks werealso reported in four patients. The clinical semiology wasin accord with seizures originating from temporal regionin four, from extratemporal regions (frontal and parietal)in three, and extratemporal onset together with temporalonset was assumed in one patient (Table 1). The meanfollow-up was 13.4 years, with a minimum of two and amaximum of 35 years from the onset of epilepsy.Although the frequency of seizures decreased with drugs,all patients except two continued to have disablingfrequent seizures. Vagal nerve stimulation was used inone patient (Case 1). At least one drug was used in
therapy. On the 35th year of follow-up, Case 4 stillreported complex partial seizures with three antiepilepticdrug combinations.
Routine interictal EEG recordings showed a normalbackground activity in five patients. Slow backgroundactivity was recorded in three patients. Focalabnormalities, nonspecific (theta activity) or epileptiform,were present in seven recordings. In one patient, allroutine EEG examinations (6 recordings) were regardedas normal (Case 8). No patient showed photic driving orother EEG changes during photic stimulation. Isolatedspike activity was recorded in two patients. 3-3.5cyc/secgeneralized spike–wave activity mimicking primarygeneralized epilepsy was detected in two cases (Figure 2).Video-EEG monitorization with scalp electrodes wasperformed in five patients. Ictal rhythmic activity wasrecorded in four patients. Twenty-six seizures wererecorded during 1-3 days (mean: 6.5 seizures perpatient). Ictal EEGs of four patients showed rhythmic
159
Vol: 37 No: 3 Periventricular Nodular Heterotopia and Epilepsy June 2007
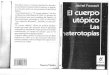
Figure 1. MRI. All cases have simple bilateral PNH. (a) Case 1, coronal T2 weighted image displays periventricular nodulesin the left peritrigonal region and bilateral frontal horns (arrow). The signal from the nodules is homogeneousand consistent with grey matter. (b) Case 2, bilateral nodules are present along the posterior cavity boundary.(c) Coronal TSE IR T1 weighted image from Case 3, with bilateral PNH. (d) Coronal T2 weighted image fromCase 4, shows nodules localized at the level of posterior trigones, larger in number in the right side (arrows).(e,f) Cases 5 and 6, axial T2 weighted images show multiple subependymal heterotopic nodules in occipital hornsof ventricles.
a b c
d e f

160
ÜNAL, A et al. Periventricular Nodular Heterotopia and Epilepsy Turk J Med Sci
Tabl
e 1.
Clin
ical
, dem
ogra
phic
, his
tory
, neu
roim
agin
g an
d fo
llow
-up
resu
lts o
f th
e pa
tient
s w
ith b
ilate
ral P
NH
(BP
NH
).
Age/
Pare
ntal
Seiz
ure
Fam
ily h
isto
rySe
izur
e ty
pes
in h
isto
ry a
ndN
odul
eAn
tiepi
lept
icD
rug
resp
onse
sex
cons
angu
inity
onse
t (a
ge)
follo
w-u
plo
catio
nth
erap
y
Case
122
/FFi
rst-
degr
ee15
Unr
emar
kabl
e1.
CPS
: at
age
15, 7
-8/d
ayVN
S2.
FS
w/w
o G
TCS:
at
age
16,
BPN
H+
once
in 2
-3 m
onth
s(O
+T+F
)LT
G 2
00 m
g/d
CPS:
4-6
t/d
3. F
allin
g se
izur
es, l
ook-
like
(Fig
1a)
PB 2
00 m
g/d
FS: s
topp
edat
onic
sei
zure
s: in
last
CBZ
800
mg
Falli
ngs:
2 t
/m18
mon
ths,
5-6
t/m
LTC
1000
mg/
d
Case
222
/FSe
cond
-deg
ree
13U
nrem
arka
ble
1. G
TCS:
at
age
13, o
nce
inBP
NH
CBZ
400
mg/
d2-
3 m
(O+T
) CL
Z 2x
0.5
mg/
dG
TCS:
sto
pped
2. C
PS: 2
-3 t
/m(F
ig 1
b)PB
125
mg/
dCP
S: 4
-12
t/d
Case
320
/M(-
)18
Mot
her
had
two
1. C
PS: 1
0-12
t/w
eek
OxC
BZ 1
500
mg/
dCP
S: 2
-3 t
/dm
isca
rria
ges
in t
he2.
GTC
S: o
nly
once
BPN
HLT
C 10
00 m
g/d
FS: s
topp
edfir
st t
rim
este
r3.
FS:
onc
e in
2-3
mon
ths
(O+T
) G
TCS:
sto
pped
Has
2 h
ealth
y si
ster
s (F
ig 1
c)
Case
459
/MSe
cond
-deg
ree
24A
sist
er d
ied
in t
he f
irst
1. C
PS: 1
0-12
t/m
BPN
HLT
C 20
00 m
g/d
CPS
with
pur
eye
ar; h
as a
hea
lthy
son
2. G
TCS:
1-2
t/y
ear
(O+T
+F)
CBZ
1200
mg/
dam
nesi
a: 2
-3 t
/man
d a
heal
thy
daug
hter
;3.
Fal
ling
seiz
ures
: 1-2
t/m
(Fig
1d)
PB 2
50 m
g/d
Falli
ngs:
stop
ped
His
dau
ghte
r ha
s on
eG
TCS:
sto
pped
mis
carr
iage
Case
526
/MSe
cond
-deg
ree
6 m
onth
sM
othe
r re
port
ed 3
ear
ly1.
FS
with
SG
TCS:
1 t
/mBP
NH
LTG
100
mg/
din
fant
dea
ths
2. F
allin
g se
izur
es: 1
-2 t
/m(O
+T+F
) CL
Z 1x
2 m
g/d
FS w
sG
TCS:
1-2
tM
ater
nal a
unt
expe
rien
ced
(Fig
1e)
DPH
: 400
mg/
din
6 m
onth
s3
earl
y ch
ild d
eath
sFa
lling
s: 1
-2 t
/m
Case
620
/MFi
rst-
degr
ee
14U
nrem
arka
ble
1. C
PS: 2
5-30
t/m
BPN
H(O
+T)
LTC
2000
mg/
dCP
S:15
-20
t/m
(Fig
1f)
TPM
100
mg/
dCB
Z 60
0 m
g/d
Case
727
/F(-
)16
Unr
emar
kabl
e1.
CPS
: onc
eBP
NH
2. G
TCS:
2 t
imes
in t
he f
irst
(con
tiguo
us n
odul
es)
CBZ
900
mg/
dSe
izur
e-fr
eeye
ar o
f fo
llow
-up
(Fig
3a)
Case
826
/F(-
)14
Unr
emar
kabl
e1.
SPS
and
CPS
: 1-2
t/w
BPN
HCB
Z 20
0-60
0 m
g/d
SPS
with
aut
onom
ic(C
ontig
uous
nod
ules
,sy
mpt
oms:
1-2
t/w
pred
omin
antly
on
the
righ
t si
de)
(Fig
3b)
CPS:
Com
plex
par
tial s
eizu
re. F
S: F
ocal
mot
or s
eizu
re. G
TCS:
Gen
eral
ized
ton
ic-c
loni
c se
izur
e. F
SwsG
TCS:
Foc
al m
otor
sei
zure
with
sec
onda
ry g
ener
aliz
atio
n. t
: Tim
es. m
: Mon
th. O
: Occ
ipita
l. T:
Tem
pora
l. F:
Fro
ntal
.VN
S: V
agal
ner
ve s
timul
atio
n. L
TG: L
amot
rigi
ne. P
B: P
heno
barb
ital.
CBZ:
Car
bam
azep
ine.
LTC
: Lev
etir
acet
am. C
LZ: C
lona
zepa
m. O
xCBZ
: Oxc
arba
maz
epin
e. D
PH: D
iphe
nylh
ydan
toin
. TPM
: Top
iram
ate.

161
Vol: 37 No: 3 Periventricular Nodular Heterotopia and Epilepsy June 2007
Tabl
e 2.
Ict
al a
nd in
teri
ctal
ele
ctro
grap
hic
and
clin
ical
fin
ding
s of
the
pat
ient
s.
Icta
l EEG
Inte
rict
al E
EGSe
mio
logy
of
seiz
ures
EEG
foc
us
Case
1
Left
tem
pora
l 5-6
cyc
/sec
, rh
ythm
icBa
ckgr
ound
act
ivity
: 7-
8 cy
c/se
c Is
olat
ed
Loss
of
cons
ciou
snes
s, b
linki
ng,
Bila
tera
l tem
pora
l with
left
shar
p w
aves
, th
en g
ener
aliz
ed s
harp
spik
e ac
tivity
ove
r le
ft p
oste
rior
tem
pora
lw
ith a
utom
atis
ms
in h
ands
and
pred
omin
ance
and
slow
wav
e co
mpl
exes
(10
-30
sec)
regi
on a
nd 3
-3.5
cyc
/sec
gen
eral
ized
spi
keur
inar
y in
cont
inen
ce (
15-2
0 se
c)w
ave
activ
ity (
Fig
2)
Case
2
Seve
n se
izur
es r
ecor
ded;
rhy
thm
ic s
harp
Back
grou
nd a
ctiv
ity.:
9-10
cyc
/sec
CPS
with
out
auto
mat
ism
sBi
late
ral i
ndep
ende
nt t
empo
ral
thet
a an
d al
pha
activ
ity in
the
left
tem
pora
lCe
ntra
l, ri
ght
cent
ro-p
arie
tal a
nd(2
0-30
sec
)re
gion
in f
our
and
the
sam
e ac
tivity
in t
hebi
late
ral f
ront
al s
pike
s Pa
roxy
smal
act
ivity
righ
t te
mpo
ral r
egio
n in
thr
ee o
f th
eof
inde
pend
ent
thet
a, d
elta
slo
w a
nd s
harp
seiz
ures
wav
es o
ver
bila
tera
l tem
pora
l reg
ions
Case
3
Dur
ing
5 da
ys m
onito
riza
tion
noBa
ckgr
ound
act
ivity
: 9-
10 c
yc/s
ec(R
ecor
ded
duri
ng f
ollo
w-u
p)Le
ft t
empo
ral r
egio
nse
izur
e w
as d
etec
ted
Back
grou
nd a
ctiv
ity:
9-10
cyc
/sec
Amne
sia
and
conf
usio
n w
ithou
tau
tom
atis
ms
(pur
e am
nest
ic)
Case
4
Back
grou
nd a
ctiv
ity;
9-10
cyc
/sec
Isol
ated
sha
rp w
aves
ove
rU
nfor
ced
devi
atio
n of
hea
d t
o ri
ght
Rig
ht t
empo
ral r
egio
npa
riet
o-oc
cipi
tal a
lpha
and
5-7
cyc
/sec
righ
t t
empo
ral r
egio
nsi
de,
auto
mat
ism
in t
he r
ight
han
d,ce
ntra
l the
ta B
ilate
ral f
ast
activ
ity f
ordy
ston
ia in
the
left
han
d,5
sec,
then
5-7
cyc
/sec
the
ta o
ver
righ
tun
cons
ciou
snes
s (4
0-60
sec
) te
mpo
ral r
egio
n an
d bi
late
ral d
elta
and
thet
a ac
tivity
with
vol
tage
dep
ress
ion
Case
5
Not
per
form
edBa
ckgr
ound
act
ivity
: 7-
8 cy
c/se
c(h
isto
ry)
L pa
riet
o-oc
cipi
tal r
egio
nsl
ow a
nd s
harp
wav
es in
left
par
ieto
-occ
ipita
lCl
onic
mov
emen
ts in
the
rig
htre
gion
arm
spr
eadi
ng t
o ri
ght
leg
then
seco
ndar
y ge
nera
lizat
ion.
Case
63-
4 cy
c/se
c hi
gh a
mpl
itude
del
taBa
ckgr
ound
act
ivity
: 7-
8 cy
c/se
c th
eta
Voca
lizat
ion,
loss
of
cons
ciou
snes
s,R
ight
tem
pora
l reg
ion
activ
ity o
ver
righ
t te
mpo
ral r
egio
n,1-
2cyc
/sec
slo
w-s
harp
wav
e de
lta a
ctiv
ityau
tom
atis
ms
in b
oth
hand
ssp
read
ing
to ip
sila
tera
l hem
isph
ere
over
rig
ht t
empo
ral r
egio
nw
ith a
mpl
itude
asy
mm
etry
hig
her
than
50%
, th
en g
ener
aliz
atio
n
Case
7
Not
per
form
edSl
ow-s
harp
wav
es in
bila
tera
l tem
pora
l(h
isto
ry)
Bila
tera
l tem
pora
l reg
ions
regi
ons
with
left
pre
dom
inan
ceVi
sual
hal
luci
natio
ns,
mov
emen
tsw
ith le
ft p
redo
min
ance
in h
er le
ft a
rm a
nd le
g th
at w
ould
spre
ad t
o in
volv
e th
e fa
ce a
ndsu
bseq
uent
ly h
er e
ntir
e bo
dy
Case
8N
ot p
erfo
rmed
Nor
mal
,(h
isto
ry)
Coul
d no
t be
det
ecte
dBa
ckgr
ound
act
ivity
: 9-
10 c
yc/s
ec
Left
sid
ed f
ocal
mot
or-s
enso
ryse
izur
es
w/w
o se
cond
ary
gene
raliz
atio
n Is
olat
ed s
eizu
res
with
auto
nom
ic s
ympt
oms
(tac
hyca
rdia
,ch
est
pain
and
sw
eatin
g)
CPS:
Com
plex
par
tial s
eizu
re.
w/w
o: W
ith o
r w
ithou
t.

activities over the temporal lobes initially. Ictal andinterictal EEG changes with seizure semiology arepresented in Table 2.
Well-defined small nodules of heterotopic grey matterappeared isointense as normal grey matter on all imagingsequences. The nodules were localized along the walls ofthe ventricles bilaterally in all cases. Nodules weremultiple, but not contiguous in six patients. Bilaterallylocated contiguous nodules were present in two patients;one symmetric and one asymmetric (Cases 7 and 8,Figure 3). None had nodules along the third or fourthventricles. Nodules were located in occipital and temporalhorns in four patients, and in occipital, temporal andfrontal horns in two patients (Table 1). No patient wasaffected by PNH associated with other more pronouncedbrain malformations (i.e., schizencephaly andpolymicrogyria) or structural abnormality, but in MRI ofCase 8 hippocampal morphological asymmetry was seen.
Discussion
A wide variety and heterogeneity of clinical pictureshave been reported in patients with PNH. Many reportedseries have included all kinds of heterotopias, orperiventricular heterotopias with other corticaldysgenesis or structural brain abnormalities. Dubeau etal. (17) divided PNH patients according to the type of the
heterotopic grey matter into two groups as simple PNH(patients with PNH without other cortical and/or cerebralmalformations) and PNH-plus (PNH patients with othercortical and/or cerebral malformations). The nodules canalso be anatomically subdivided into two types: unilateralor bilateral in disposition and focal or diffuse inlocalization (10,18,19). Therefore, it will be better toanalyze PNH patients first in two groups as simple andplus, and then as bilateral symmetric, asymmetric, andunilateral. In this study, PNH demonstrated by highresolution MRI was found as an isolated anomaly (simplePNH), and all nodules were bilaterally located in theperiventricular region. One was bilateral diffusesymmetric and the other seven were bilateralasymmetric.
Epilepsy has been reported in the second or thirddecade of life or earlier in PNH patients with nodysmorphic features (10,14). Seizure frequency rangesfrom rare to very frequent, and seizures are oftenresistant to polytherapy (5,14,18). Six of the eightpatients in the presented study came to medical attentionbecause of their intractable seizures. In two patients, withbilateral diffuse PNH, response to medical therapy wasgood (Cases 7 and 8). Resistant seizures and severemental retardation with dysmorphic features werepresent in Case 5. He was followed-up for 25 years withthe diagnosis of cerebral palsy and mental retardation.Case 6 and Case 4 were misdiagnosed and followed-up astemporal lobe epilepsy for years. Case 8 was diagnosed asanxiety and panic attack disorder and none of the routine
162
ÜNAL, A et al. Periventricular Nodular Heterotopia and Epilepsy Turk J Med Sci
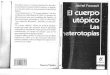
Figure 2. 3.0-3.5 Hz generalized spike-wave activity recorded duringlong-term video EEG monitoring of Case 1.
Figure 3. a) Axial SE T1 weighted image from Case 7, shows bilateralsymmetric heterotopic grey matter localized alongsubependymal region of lateral ventricles. b) T2 weightedimage of Case 8 with bilateral asymmetric located PNH.
a b

EEG examinations revealed any abnormality. Evaluationwith detailed MRI was helpful in the proper diagnosis inall presented cases. Therefore, it is important firstly toknow and call to mind PNH, and then to examine theperiventricular walls, especially with high resolution MRI,in searching the cause of epilepsy.
Incidence of complex partial seizures with severalclinical symptoms suggesting mesial or neocorticaltemporal and parieto-occipital onset was striking. Limbicand visual auras were recorded in two patients. Threepatients presented with focal motor seizures suggestingcentral or frontal origin. Three patients tended to havebilateral independent temporal epileptic abnormalities.Isolated spike activity was recorded in two patients. 3-3.5cyc/sec generalized spike–wave activity mimickingprimary generalized epilepsy was detected in two cases.Raymond et al. (18) first mentioned generalizeddischarges mimicking primary generalized epilepsy in1994 in three of the 13 PNH patients in their series. In1995, Dubeau et al. (17) mentioned the same activity inone patient. We evaluated the characteristics of thesepreviously reported four cases; nodules were locatedbilaterally asymmetric in three of them, as in our cases,and unilateral in the remaining one. However, Battaglia etal. (10) in 1997 reported that EEG abnormalities werealways focal in their cases, unlike previously describedones. In 14 cases of Battaglia’s series, PNH wasassociated with another structural abnormality of thebrain. The remaining three cases were in simple PNHform, but the location and type of PNH was bilateral inonly one of them. In five of the six patients with 3-3.5 Hzgeneralized spike-wave activity (including ours), noduleswere located bilaterally and asymmetric.
Bilateral diffuse symmetrical form of PNH has beenreported more than bilateral asymmetrical and unilateralforms in the literature. The patients with bilateralasymmetrical PNH were thought to share similar featureswith patients with bilateral symmetrical or unilateral PNH(16). Most of the reported patients with bilateralasymmetrical PNH in the literature have associatedstructural abnormalities of the posterior fossa, and apositive family history for epilepsy, as in the case ofbilateral symmetrical PNH, but the localization of nodulesare more pronounced in the paratrigonal regions, as inunilateral PNH. Although clear female predominance andfrequent familial occurrence in bilateral, symmetrical, anddiffuse cases have been reported, unilateral and bilateral
asymmetric cases are not associated with sex prevalence.In accord with the previously reported bilateralasymmetric PNH cases, two of the six presented cases inthis study were female.
Recent human and experimental studies have shownneuronal connections between heterotopic nodules andbetween nodules and cortex (6). These studies havesuggested that intranodular neurons have alteredexcitatory or inhibitory transmission. Hannan et al. (20)showed, in surgical specimens obtained from epilepticchildren with nodular heterotopia, that the heterotopia,either subcortical or subependymal, had sparseconnections with each other and with other parts of thehemisphere, including the cortex (21). Aghakhani et al.(22) analyzed the respective roles of heterotopia,temporal and extra-temporal neocortex and mesialtemporal lobe structures in the generation of epilepticactivity in a relatively large series of patients with PNHand focal epilepsy. They confirmed that nodules ofheterotopic grey matter can generate both normal andabnormal electrical activity (23). Bilateral multiple orcontiguous PNH were often associated with widespreadepileptogenesis, where classical surgical approaches(temporal resection) are unlikely to be effective (24).Aghakhani et al. (22) used amygdalo-hippocampectomyin two patients (outcome: Engel class Id and III),amygdalo-hippocampectomy plus removal of an adjacentheterotopion in two patients (class Ia), resection of twocontiguous nodules plus a small rim of overlying occipitalcortex in one patient (class Id) and hippocampectomy plusremoval of three adjacent heterotopia in one patient(class IV) as the surgical approaches. In unilateral nodules,they suggested that investigation by stereo-EEG mayindicate a focal resection, and a good outcome may beexpected (Engel class I). In this study, there were twopatients with bilateral noncontiguous asymmetric nodulesand they were the most intractable ones of the operatedcases (Engel class III and IV).
In 2003, d’Orsi et al. (14) compared clinical andelectrophysiological findings of eight simple PNH patientswith eight PNH-plus patients. PNH cases with unilateralor bilateral asymmetric localization were evaluated. Theyfound that neurological deficits were more common andseizure frequency was higher in the PNH-plus group anddrop attacks were experienced only in these patients. Werecorded three patients with falling attacks similar toatonic seizures. Although the number of reported cases
163
Vol: 37 No: 3 Periventricular Nodular Heterotopia and Epilepsy June 2007

with falling attacks is so small, this finding suggests thatfalling attack is another seizure type that can be seen inbilateral asymmetric PNH cases. It was exciting for us tosee that the clinical symptoms of one of the cases inD’Orsi’s series were similar with those of Case 5: facialdysmorphisms, small penis and undescended testes,hypoplastic distal and middle phalanges, obesity, mentalretardation and epilepsy.
Generalized tonic-clonic seizures occurred duringthe early phases of epilepsy in five patients in our study,and were completely controlled by treatment in all exceptone. However, complex partial seizures were mainlyresistant to therapy. The oldest patient of published casesis presented here, at 59 years of age; he is quite welldespite the intractable focal seizures. Surprisingly, twopatients became seizure-free.
In conclusion, patients with bilateral PNHs havevariable clinical features, EEG findings and extension ofthe heterotopic nodules. These patients may bemisdiagnosed as having idiopathic generalized epilepsy,temporal lobe epilepsy or even psychogenic nonepilepticseizures without high quality MRI because of themisleading seizure semiology and interictal-ictal EEGfindings. Seizures are usually drug-resistant but thepatients who have diffuse symmetric or asymmetriccontiguous heterotopic nodules may have goodprognosis. Studies taking into account the type,multiplicity and localization of the nodules will be morehelpful in explaining the clinical characteristics and follow-up strategies in patients with PNH.
164
ÜNAL, A et al. Periventricular Nodular Heterotopia and Epilepsy Turk J Med Sci
References1. Pearlman AL, Faust PL, Hatten ME, Brunstrom JE. New directions
for neuronal migration. Curr Opin Neurobiol 1998; 8(1): 845-854.
2. Fox JW, Walsh CA. Periventricular heterotopia and the genetics ofneuronal migration in the cerebral cortex. Am J Hum Genet1999; 65: 19-24.
3. Pilz D, Stoodley N, Golden JA. Neuronal migration, cerebralcortical development, and cerebral cortical anomalies. JNeuropathol Exp Neurol 2002; 61(1): 1-11.
4. Guerrini R. Genetic malformations of the cerebral cortex andepilepsy. Epilepsia 2005; 46 (suppl 1): 32-37.
5. Huttenlocher PR, Taravath S, Mojtahedi S. Periventricularheterotopia and epilepsy. Neurology 1994; 44(1): 51-55.
6. Eksioglu YZ, Scheffer IE, Cardenas P, Knoll, J, DiMario F, RamsbyG et al. Periventricular heterotopia: an X linked dominant epilepsylocus causing aberrant cerebral cortical development. Neuron1996; 16: 77-87.
7. Fink JM, Dobyns WB, Guerrini R, Hirsch BA. Identification ofXq28 associated with bilateral periventricular nodularheterotopia. Am J Hum Genet 1997; 61: 379-387.
8. Sisodiya SM, Free SL, Thom M, Everitt AE, Fish DR, Shorvon SD.Evidence for nodular epileptogenicity and gender differences inperiventricular nodular heterotopia. Neurology 1999; 52: 336-341.
9. Sheen VL, Topcu M, Berkovic S, Yalnizoglu D, Blatt I, Bodell A etal. Autosomal recessive form of periventricular heterotopia.Neurology 2003; 60(7): 1108-1112.
10. Battaglia G, Granata T, Farina L, D'Incerti L, Franceschetti S,Avanzini G. Periventricular nodular heterotopia: epileptogenicfindings. Epilepsia 1997; 38(11): 1173-1182.
11. Barkovich AJ. Magnetic resonance imaging: role in theunderstanding of cerebral malformations. Brain Dev 2002; 24:2–12.
12. Barkovich AJ, Kuzniecky RI, Jackson GD, Gueprini R, Dobyns WB.Classification system for malformations of cortical development.Neurology 2001; 57: 2168–2178.
13. Barkovich AJ, Kjos BO. Gray matter heterotopias: MRcharacteristics and correlation with developmental and neurologicmanifestations. Radiology 1992; 182: 493-499.
14. D’Orsi G, Tinuper P, Bisulli F, Zaniboni A, Bernardi B, Rubboli Get al. Clinical features and long term outcome of epilepsy inperiventricular nodular heterotopia. Simple compared with plusforms. J Neurol Neurosurg Psychiatry 2004; 75: 873-878.
15. Chang BS, Ly J, Appignani B, Bodell A, Apse KA, Ravenscroft RSet al. Reading impairment in the neuronal migration disorder ofperiventricular nodular heterotopia. Neurology 2005; 64(5):799-803.
16. Battaglia G, Chiapparini L, Franceschetti S, Freri E, Tassi L,Bassanini S et al. Periventricular nodular heterotopia:classification, epileptic history, and genesis of epileptic discharges.Epilepsia 2006; 47(1): 86-97.
17. Dubeau F, Tampieri D, Lee N, Andermann E, Carpenter S, LeblancR et al. Periventricular and subcortical nodular heterotopia. Astudy of 33 patients. Brain 1995; 118: 1273-1287.

165
Vol: 37 No: 3 Periventricular Nodular Heterotopia and Epilepsy June 2007
18. Raymond AA, Fish DR, Stevens JM, Sisodiya SM, Alsanjari N,Shorvon SD. Subependymal heterotopia: a distinct neuronalmigration disorder associated with epilepsy. J Neurol NeurosurgPsychiatry 1994; 57: 1195-1202.
19. Kothare SV, VanLandingham K, Armon C, Luther JS, Friedman A,Radtke RA. Seizure onset from periventricular nodularheterotopias: depth-electrode study. Neurology 1998; 51(6):1723-1727.
20. Hannan AJ, Servotte S, Katsnelson A, Sisodiya S, Blakemore C,Squier M et al. Characterization of nodular heterotopia inchildren. Brain 1999; 22: 219-238.
21. Tassi L, Colombo N, Cossu M, Mai R, Francione S, Russo GL et al.Electroclinical, MRI and neuropathological study of 10 patientswith nodular heterotopia, with surgical outcomes. Brain 2005;128: 321-337.
22. Aghakhani Y, Kinay D, Gotman J, Soualmi L, Andermann F, OliverA et al. The role of periventricular nodular heterotopia inepileptogenesis. Brain 2005; 128: 641-651.
23. Jakobs KM, Kharazia VN, Prince DA. Mechanisms underlyingepileptogenesis in cortical malformations. Epilepsy Res 1999;36(2-3): 165-188.
24. Li LM, Dubeau F, Andermann F, Fish DR, Watson C, Cascino GDet al. Periventricular nodular heterotopia and intractable temporallobe epilepsy: poor outcome after temporal lobe resection. AnnNeurol 1997; 41: 662-668.
















![[Foucault, Michel] o Corpo Utópico, As Heterotopias](https://img.pdfslide.net/doc/110x75/563dbad9550346aa9aa8955f/foucault-michel-o-corpo-utopico-as-heterotopias.jpg)