Embed Size (px)
Citation preview

MOUNT SINAI JOURNAL OF MEDICINE 75:472–477, 2008 472
EVIDENCE-BASED MEDICINE
Clinical Prediction Rules forHospitalists
Ramiro Jervis, MD, and Thomas McGinn, MD
Mount Sinai School of Medicine, New York, NY
Hospitalists struggle like all physicians to incorporatethe best evidence into daily practice. The busy workflow of the hospital, however, with an emphasison both throughput and quality, produces uniquepressures to diagnose and treat patients as efficientlyas possible. These pressures highlight a need to bringthe practice of evidence-based medicine (EBM) to thebedside of patient care in the most efficient mannerpossible.
Clinical prediction rules (CPRs) form a uniquesubset of the practice of EBM and strive to addressthis challenge of using EBM at the bedside. A CPRis a clinical tool that quantifies the individualcontributions that various components of the history,physical examination, and basic laboratory resultsmake toward the diagnosis, prognosis, or likelyresponse to treatment of a patient. Clinical decisionrules attempt to formally test, simplify, and increasethe accuracy of clinicians’ diagnostic and prognosticassessments.1
CPRs are most likely to be useful in situationsin which decision making is complex, the clinicalstakes are high, or there are opportunities toachieve cost savings without patient care beingcompromised.1 Many examples of CPRs exist, andthis article provides a sampling of clinical scenariosthat highlight the utility of these tools for hospitalists,followed by a discussion on assessing the validity ofCPRs before they are incorporated into daily practice.
Address Correspondence to:
Ramiro Jervis, MDMount Sinai School of Medicine
New York, NYEmail: ramiro.jervis@
mountsinai.org
CLINICAL PREDICTION RULES:CASE EXAMPLES
Using Clinical Prediction Rules ToAssess Pretest Probability forPulmonary EmbolismPulmonary embolism (PE) remains a major publichealth problem and by some estimates accountsfor 10% of all hospital deaths.2 The importance ofaccurate and efficient diagnoses of thromboembolicdisease makes this disease an ideal starting pointfor CPRs. Pretest probability, defined as the prob-ability of disease before the test result is known,is often a challenging variable to less experiencedclinicians and plays a key role in the diagnoses ofmany disease, including PE. CPRs can simplify andstandardize the assessment of a patient’s pretest prob-ability of disease. Consider this typical case admittedby a hospitalist.
A 50-year-old woman with a history of orthopedicsurgery 3 weeks prior and no past medical historypresents with acute onset of pleuritic chest painand shortness of breath while lifting a heavy object.Her pain lasted only seconds, but her shortness ofbreath persists. She has no leg swelling or pain. Sheadmits to symptoms of anxiety and stress. Her physicalexamination demonstrates a blood pressure of 100/70,a pulse of 80, and an O2 saturation of 97% on roomair. Her chest X-ray is clear, her electrocardiogram isnormal, and her laboratory work and arterial bloodgas are unremarkable. The patient is admitted to themedical floor while her workup is pending.
The decision for further action for this patientis highly dependent on the clinician’s perception ofrisk for PE, and the interpretation of further resultsis dictated by the pretest probability. If, for example,the patient in question is low-risk by clinical intuition,a low-probability ventilation perfusion (VQ) scanmay be sufficient for a clinician to safely dischargethe patient. Similarly, if the patient is perceived as
Published online in Wiley InterScience (www.interscience.wiley.com).DOI:10.1002/msj.20066
2008 Mount Sinai School of Medicine

MOUNT SINAI JOURNAL OF MEDICINE 473
medium- or high-risk, a low-probability VQ scan maynot be sufficient, and further testing with D-dimer,lower extremity Dopplers, computed tomography(CT) angiography, or pulmonary angiography maybe required.
This dependence on pretest probability is notrestricted to testing with a VQ scan. CT pulmonaryangiography, for example, has a negative likelihoodratio of only 0.2. (Likelihood ratios incorporate thesensitivity and specificity of a test and provide insightinto how much the pretest probability goes up ordown with a given test result. A further and morein-depth discussion of likelihood ratios can be foundin Grimes and Schulz.3) A high pretest probability of67%, for example, would be reduced only to a 12%probability of disease with a negative CT angiogram,which is unacceptable for many clinicians, giventhe morbidity and mortality associated with PE.4
Although exact numbers like this can be helpful,most clinicians will intuitively understand that a highclinical suspicion requires a more robust burdenof proof to counter a diagnosis, whereas a lowclinical suspicion of disease needs fewer confirmatorynegative tests. The diagnosis of PE and many otherdiseases for that matter is then highly dependenton an accurate pretest probability, regardless of thediagnostic modality.
CPRs may be especially useful for less experi-enced clinicians,5 and one of the most widely usedCPRs for predicting thromboembolism is the Sim-plified Wells Scoring System.6 This scoring system(Table 1) looks at different aspects of the history andphysical examination and weighs them to calculate ascore for risk. The Wells scoring system (also knownas the Wells criteria) has compared favorably withexperienced clinical intuition, with disease probabil-ities for PE in 10 prospective studies ranging from3% to 28%, from 16% to 46%, and from 38% to 98%in the low, moderate, and high pretest probabilitygroups, respectively.5 Defining the lower risk groupsis helpful to the less experienced clinician, as fewer
additional tests (such as D-dimer or lower extremityultrasound) will be necessary for this group to reducethe disease probability to a more comfortable rangeprior to discharge.
Case ResolutionThe patient has no signs or symptoms suggestive ofDVT. An alternative diagnosis of musculoskeletal painand anxiety is at least as likely as a diagnosis of PE.There is no tachycardia as defined under the Wellscriteria, and there is no history of thromboembolism,cancer, or hemoptysis. Only a history of recentsurgery gives the patient a total of 1.5 points onthe Wells score; this is defined as low-risk becausethe score is less than 2. The doctor decides that thepatient does not need a VQ scan or CT angiogram andthat the patient can be safely discharged if a D-dimeris negative. Recent studies, in fact, validate thisapproach.7 The patient is subsequently dischargedwith outpatient follow-up.
Predicting Risk for PneumoniaPneumonia is a common ailment treated by hospital-ists and may be associated with high mortality in cer-tain populations. Low-risk patients, however, can betreated in the community if they can be reliably iden-tified. Such risk assessment then is crucial to the mis-sion of hospitalists in reducing unnecessary resourceutilization. Consider the following typical case.
A healthy 62-year-old patient is admitted to aservice with a diagnosis of pneumonia. She has ahistory of controlled hypertension and diabetes andhad presented to the Emergency Department withproductive cough and fever at home. A left lower lobeinfiltrate is present on chest X-ray. Her laboratorywork is unremarkable except for a white count of18,000. The patient is alert and oriented, has atemperature of 38.5 ◦C, a blood pressure of 110/70,and an oxygen saturation of 95% on room air, and
Table 1. Wells Clinical Prediction Rule for PE (Simplified Criteria).
Points If the Total PEScore Is Probability Is
• Clinical symptoms of PE: chest pain, shortness of breath, and oxygensaturation <90% (3.0 points)
<2.0 points Low
• No alternative diagnosis (3.0 points) 2.0–6.0 points Moderate• Heart rate >100 (1.5 points) <6.0 points High• Immobilization or surgery in the previous 4 weeks (1.5 points)• Previous DVT/PE (1.5 points)• Hemoptysis (1 point)• Malignancy (1 point)
Abbreviations: DVT, deep vein thrombosis; PE, pulmonary embolism.
DOI:10.1002/MSJ

474 R. JERVIS AND T. MCGINN: EVIDENCE-BASED MEDICINE–CLINICAL PREDICTION RULES FOR HOSPITALISTS
is breathing at a rate of 20. The patient wants to gohome but ‘‘only if the physicians think it is safe.’’
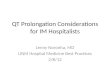
Much effort has gone into developing riskstratification tools to safely triage patients who may ormay not need further inpatient management. The firstof these tools by Fine et al.8 was developed in 1997and comprises 20 clinical variables to triage patientsinto 5 risk categories, with risk of death ranging from0.5% for inpatients stratified to the lowest risk groupto 27% 30-day mortality for the highest risk group.Although handheld programs or online calculatorscan assist in the calculation of these scores, thecomplexity of the Pneumonia Severity Index (PSI)may limit its everyday use. The PSI is calculatedwith the flow diagram in Figure 1. A simpler tool,CURB-65, was developed to predict risk for inpatientmortality with only 5 readily available clinicalcharacteristics: presence of confusion, blood ureanitrogen >20 mg/dL, respiratory rate >30, systolicblood pressure <90 or diastolic blood pressure <60,and age >65. An evenly weighted score of <2 islow-risk, a score of 2 is medium-risk, and a scoreof >2 is high-risk, with 30-day mortality predictedto be as low as 0.6% for no points and as high as47% for the highest risk strata. Each of these decisiontools has its strengths and weaknesses, with the PSIhaving slightly better ability to discriminate betweenrisk groups, but CURB-65 has far greater ease of use.9
The original authors of the PSI suggested thatpatients in risk classes I and II could safely be
treated as outpatients, whereas clinician judgmentmay play a bigger role in class III. Similarly, patientswith CURB-65 scores of 1 to 2 can be treated asoutpatients. Both the Infectious Disease Society andthe American Thoracic Society recommend the use ofeither scoring system in their consensus guidelines.10
Case ResolutionIn the case example, the doctor determines the riskon the basis of both the CURB-65 and the PSI. Thepatient is calculated to belong to PSI risk class II andto have a CURB-65 score of 0. The doctor decidesthat the patient can be safely discharged earlier thaninitially expected. The patient is reassured and senthome with a 7-day course of oral antibiotics and withfollow-up with her primary care provider.
Evaluating Need for Isolation forPulmonary TuberculosisAppropriate isolation of patients with tuberculosisis often delayed, and patients without tuberculosisare often isolated unnecessarily; this aggravates thealready stressed bed capacity and throughput issuesstraining hospitals nationwide. In a low endemicarea, for example, tuberculosis was identified in only1 of 92 patients that were isolated.11 A tool that candiscriminate these patients more appropriately wouldbe useful. With this in mind, consider the next case.
A 67-year-old man with no past medicalhistory presents with a 5-day history of productive
Step 1: Stratify to Risk Class I vs. Risk Classes II-V• Presence of any of following:
– Over 50 years of age– Altered mental status– Pulse ≥125/minute– Respiratory rate >30/minute– Systolic blood pressure <90 mm Hg– Temperature <35°C or ≥40°C– History of:
• Neoplastic disease• Congestive heart failure• Cerebrovascular disease• Renal disease• Liver disease
If none of above factors present then assign to Risk Class I, else go to step 2
Step 2:Demographics Points AssignedIf Male +Age (yr)If Female +Age (yr) –10Nursing home resident +10ComorbidityNeoplastic disease +30Liver disease +20Congestive heart failure +10Cerebrovascular disease +10Renal disease +10Physical Exam FindingsAltered mental status +20Pulse ≥125/minute +20Respiratory rate >30/minute +20Systolic blood pressure<90 mm Hg +15Temperature <35°C or ≥40°C +10Lab and Radiographic FindingsArterial pH <7.35 +30Blood urea nitrogen ≥30 mg/dl(9 mmol/liter) +20Sodium <130 mmol/liter +20Glucose ≥250 mg/dl(14 mmol/liter) +10Hematocrit <30% +10Partial pressure of arterial O2<60mmHg +10Pleural effusion +10
Step 3: Point assignment<=70 Class II
71-90 Class III
91-130 Class IV
>130 Class V
Fig 1. Pneumonia Severity Index algorithm. The original authors8 suggested that patients with class I,class II, and possibly class III pneumonia could be treated as outpatients.
DOI:10.1002/MSJ

MOUNT SINAI JOURNAL OF MEDICINE 475
cough, shortness of breath, fever, chills, and scanthemoptysis. Prior to this illness, he was doing wellwith no report of weight loss or night sweats.Physical examination is unremarkable except forright-sided crackles. An X-ray demonstrates a denseleft upper lobe infiltrate. The emergency departmentphysician suspects tuberculosis on the basis of thechest radiograph, and the patient is admitted to thehospitalist service, but no respiratory isolation bedsare available.
Several decision tools have been devised to helpin the risk stratification of patients with suspectedtuberculosis. One, devised by Wisnivesky et al.,12
calculates a score based on 5 readily availableclinical criteria, including X-ray findings of upperlobe infiltrate, presence of shortness of breath, fever,a history of positive purified protein derivative, andother tuberculosis risk factors (Table 2). A cutoff of0 points indicates a need for respiratory isolation.In a prospective study of over 500 patients, the ruledemonstrated a negative predictive value of 99.7%.The study estimated that about 35% of potentialadmissions may have been avoided had the decisionrule been used in this cohort of patients.
Other clinical decision rules exist to risk-stratifypatients at risk for pulmonary tuberculosis and havebeen reviewed elsewhere.11 Self-reported tuberculinskin testing results and upper lobe infiltrates showedthe highest association with subsequent diagnosis ofinfection. Interestingly, hemoptysis, admission whiteblood cell count, and human immunodeficiency virusstatus failed to show a predictive association in thesestudies.
Case ResolutionThe presence of an upper lobe infiltrate is of concern(6 points), but the absence of both of a suspicioushistory for tuberculosis or a positive tuberculin skintest, and the presence of crackles and shortnessof breath on examination (−3 points each), gives
Table 2. Clinical Prediction Rule for Isolating Patientswith Suspected Tuberculosis.
Variable Points
Tuberculosis risk factors or symptoms +4Positive purified protein derivative tuberculin
test results+5
Shortness of breath −3Fever
<38.5 +038.5–39.0 +3>39.0 +6
Crackles on physical examination −3Upper lobe consolidation on chest radiograph +6
a total of 0 points, reinforcing a decision not toisolate. This finding with the decision tool reassuresthe clinician that the patient’s symptoms are mostconsistent with community-acquired pneumonia. Thepatient is triaged to a regular bed (there are severalavailable), and appropriate treatment for community-acquired pneumonia is provided.
Triage of Patients with Chest PainChest pain accounts for a substantial number ofadmissions through the Emergency Department.About 5% of patients with acute coronary syndrome(ACS) are improperly diagnosed in the EmergencyDepartment and sent home,13 and some of thesepatients go on to experience an adverse cardiac eventor arrhythmia. This occurs despite a multitude ofways to risk-stratify patients with clinical or computeralgorithms, biomarkers, or continuous ST segmenttrend monitoring.14 Consequently, a liberal admissionpolicy for patients with chest pain is commonpractice and contributes to Emergency Departmentovercrowding and poor throughput as patients awaitscarce telemetry beds. Recent studies, however,suggest that a low-risk cohort with suspected ACScan be identified that receives little benefit frominpatient telemetry.14 The following case illustratesa typical case that may benefit from implementationof a CPR to tease out those patients who would notbenefit from a monitored bed.
A 68-year-old man presents to the EmergencyDepartment with severe substernal chest pain radi-ating to his left arm for 1 hour. He has a historyof diabetes but otherwise has an unremarkable pastmedical history. The pain is relieved with nitroglyc-erin in the Emergency Department, and the patientis now pain-free. The electrocardiogram is withoutischemic changes, and his physical examination isunremarkable. The patient is triaged to a monitoredbed with telemetry under the hospitalist service, butthere are no monitored beds available.
In 1996, Goldman et al.15 derived a riskindex that took into account the following riskfactors: presence of ischemic electrocardiographicchanges, systolic blood pressure less than 90 mm Hg,congestive heart failure on examination as evidencedby rales above the bases, and presence of pain similarto or worse than prior ACS in a patient with ahistory of coronary artery disease. The event ratesfor patients with none of these risk factors wereas low as 0.2% in 1 validation study. An impactanalysis was performed at Cook County Hospitalin Chicago in a prospective cohort of over 1000patients. Implementing the use of the rule in thetriage decisions of the clinicians did not lead to any
DOI:10.1002/MSJ

476 R. JERVIS AND T. MCGINN: EVIDENCE-BASED MEDICINE–CLINICAL PREDICTION RULES FOR HOSPITALISTS
adverse cardiac events or arrhythmias in unmonitoredbeds, and more patients with suspected ACS weretriaged to an unmonitored bed. In fact, 21% of ACSadmissions had been triaged to an unmonitored bedprior to implementation of the rule versus 36% ofadmissions after its implementation, and this suggeststhat the use of the Goldman rule may lead to a moreefficient use of telemetry resources.16
Case ResolutionThe patient has no Goldman risk factors present,and this leads the clinician to triage the patientto an unmonitored bed; there are many available.The patient is placed on the schedule for the nextavailable stress test before his discharge is planned.
Validity of Clinical Prediction RulesCPRs suffer the same limitations as other modernmedical interventions: an intervention or rule maywork in the narrow confines of a testing environment,but this does not mean it will work in everydaypractice.
A hierarchy of evidence (Table 3) provides aframework through which clinicians can judge thestrength of evidence in a given CPR.1 The lowestlevel (level IV) of evidence is identified when theCPR is derived or created. CPRs are usually derivedby the construction of a list of potential predictors,which typically includes items from the history,physical examination, and basic laboratory results.A group of patients are then examined to see ifthe clinical predictors are present, along with theoutcome of interest. Statistical analyses may revealwhich predictors are most powerful and which onescan be omitted without the CPR losing its predictiveability.1 As an example, the PSI was derived in this
way by an examination of 250 predictors in over14,000 patients.8 Alternatively, clinical predictors maybe chosen on the basis of expert consensus muchin the way that the Wells criteria were chosen.6
The rule should make clinical sense and be basedon a patient population of sufficient size, withenough outcomes and important predictors presentin the study population. Interested readers can find acomplete discussion of the derivation of CPRs in anarticle by Laupacis et al.17
Even a rigorously derived prediction rule,however, cannot be considered ready for clinical useuntil the CPR has been prospectively validated so thatit can move up the hierarchy to a level II or III rule.The associations found in a level IV rule may be dueto chance or may be related to idiosyncratic featuresof the patient population or the clinicians using therule.1 In either case, such a CPR may perform poorlywhen tested in another patient population or clinicalsetting. For this reason, validation, or testing therule in different patient populations with differentclinicians and settings, plays a crucial role beforeit advances up the hierarchy ladder. For example,clinicians will have a higher degree of confidence inthe Wells criteria, a level II rule, because they havebeen validated in over 10 different clinical settings.
Another problem may be that using the rulein everyday clinical scenarios may prove too cum-bersome or impractical. For example, the PSI hasbeen criticized because it requires multiple clinicalvariables before a score can be computed. Some lab-oratory values may not be available at the time whenthe emergency clinician is making the decision forinpatient management of the patient’s pneumonia.The end result is a CPR that works well in theory butperforms poorly in practice. Alternatively, the CPRmay be easy to use and accurate but not superior to
Table 3. Hierarchy of Evidence for Clinical Prediction Rules.
Level Rule Category Underlying Evidence
I Rules that can be used in a wide variety ofsettings with confidence that they can changeclinician behavior and improve patientoutcomes
At least 1 prospective validation in a differentpopulation and 1 impact analysis havedemonstrated changes in clinician behaviorwith beneficial consequences.
II Rules that can be used in various settings withconfidence in their accuracy
Accuracy has been either demonstrated in 1 largeprospective study involving a broad spectrumof patients and clinicians or validated in severalsmaller settings that differ from one another
III Rules that clinicians may consider using withcaution and only if the patients in the studyare similar to those in their clinical setting
These rules have been validated in only 1 narrowprospective sample.
IV Rules that need further evaluation before theycan be applied clinically
These clinical prediction rules have been derivedbut not validated or have been validated onlyin split samples, in large retrospectivedatabases, or by statistical techniques.
DOI:10.1002/MSJ

MOUNT SINAI JOURNAL OF MEDICINE 477
clinician intuition, or external forces (eg, fear of litiga-tion or patient demand for services) may override anypotential benefit from use of the CPR. For example,fear of litigation for missed myocardial infarction maylead to overdiagnoses of ACS and triage to telemetrydespite a reasonably accurate CPR.
For these reasons, an impact analysis study isessential to attain the highest level of evidence forCPRs. An impact study may randomize several insti-tutions to use of the CPR versus several controlinstitutions and measure cost savings, resource uti-lization, diagnostic accuracy, or safety as outcomes.The complexity of this approach, however, often lim-its impact analyses to much simpler before-and-afterstudies at a single institution. The difficulty of car-rying out an impact analysis may explain why fewCPRs have attained a level I status.
Of the CPRs discussed in the previous examples,only Goldman’s CPR has an associated impact analy-sis that has demonstrated decreased use of telemetrybeds with wide implementation of the rule, and so itis the only level I rule. The tuberculosis isolation ruleby Wisnivesky et al.12 should be used cautiously asit is a level III rule; it has been validated only in thesame institution in which it was derived. The otherrules are level II and can be used more confidently.
CONCLUSION
CPRs provide a valuable tool for busy hospitaliststo use to incorporate the best evidence intothe daily care of their patients. CPRs can helpdiagnose patients more efficiently, triage them moresafely, and help allocate valuable hospital resourcessafely and rationally. With an understanding ofthe levels of evidence of CPRs, an informedhospitalist can incorporate other rules into his orher practice as these emerge in the literature. OtherCPRs that hospitalists may find useful, along withtheir associated level of evidence, can be foundonline at http://www.mssm.edu/medicine/general-medicine/ebm/.
DISCLOSURES
Potential conflict of interest: Nothing to report.
REFERENCES
1. McGinn TG, Guyatt GH, Wyer PC, et al. Users’ guidesto the medical literature: XXII: How to use articles
about clinical decision rules. Evidence-Based MedicineWorking Group. JAMA 2000; 284: 79–84.
2. Demonaco NA, Dang Q, Kapoor WN, Ragni MV.Pulmonary embolism incidence is increasing with useof spiral computed tomography. Am J Med 2008; 121:611–617.
3. Grimes DA, Schulz KF. Refining clinical diagnosis withlikelihood ratios. Lancet 2005; 365: 1500–1505.
4. Stein PD, Fowler SE, Goodman LR, et al. Multidetectorcomputed tomography for acute pulmonary embolism.N Engl J Med 2006; 354: 2317–2327.
5. Chunilal SD, Eikelboom JW, Attia J, et al. Does thispatient have pulmonary embolism? JAMA 2003; 290:2849–2858.
6. Wells PS, Ginsberg JS, Anderson DR, et al. Use of aclinical model for safe management of patients withsuspected pulmonary embolism. Ann Intern Med 1998;129: 997–1005.
7. Wells PS, Anderson DR, Rodger M, et al. Excludingpulmonary embolism at the bedside without diagnosticimaging: management of patients with suspectedpulmonary embolism presenting to the emergencydepartment by using a simple clinical model andD-dimer. Ann Intern Med 2001; 135: 98–107.
8. Fine MJ, Auble TE, Yealy DM, et al. A prediction ruleto identify low-risk patients with community-acquiredpneumonia. N Engl J Med 1997; 336: 243–250.
9. Aujesky D, Auble TE, Yealy DM, et al. Prospectivecomparison of three validated prediction rules forprognosis in community-acquired pneumonia. Am JMed 2005; 118: 384–392.
10. Mandell LA, Wunderink RG, Anzueto A, et al.Infectious Diseases Society of America/AmericanThoracic Society consensus guidelines on themanagement of community-acquired pneumonia inadults. Clin Infect Dis 2007; 44(suppl 2): S27–S72.
11. Wisnivesky JP, Serebrisky D, Moore C, et al. Validityof clinical prediction rules for isolating inpatients withsuspected tuberculosis. A systematic review. J GenIntern Med 2005; 20: 947–952.
12. Wisnivesky JP, Henschke C, Balentine J, et al.Prospective validation of a prediction modelfor isolating inpatients with suspected pulmonarytuberculosis. Arch Intern Med 2005; 165: 453–457.
13. Pope JH, Aufderheide TP, Ruthazer R, et al. Misseddiagnoses of acute cardiac ischemia in the emergencydepartment. N Engl J Med 2000; 342: 1163–1170.
14. Hollander JE, Sites FD, Pollack CV Jr, Shofer FS. Lackof utility of telemetry monitoring for identificationof cardiac death and life-threatening ventriculardysrhythmias in low-risk patients with chest pain. AnnEmerg Med 2004; 43: 71–76.
15. Goldman L, Cook EF, Johnson PA, et al. Prediction ofthe need for intensive care in patients who come tothe emergency departments with acute chest pain. NEngl J Med 1996; 334: 1498–1504.
16. Reilly BM, Evans AT, Schaider JJ, et al. Impact of aclinical decision rule on hospital triage of patients withsuspected acute cardiac ischemia in the emergencydepartment. JAMA 2002; 288: 342–350.
17. Laupacis A, Sekar N, Stiell IG. Clinical predictionrules. A review and suggested modificationsof methodological standards. JAMA 1997; 277:488–494.
DOI:10.1002/MSJ