Embed Size (px)
Citation preview

WEBINAR WELCOME!How hospitalists can lead on quality
Dr. Kevin O’Leary Chief of the Division of
Hospital Medicine Northwestern University
Feinberg School of Medicine
Dr. Vercin Ephrem Chief of Hospital
Medicine LRGHealthcare
Maureen McKinney Editorial Programs
Manager Modern Healthcare
During today’s discussion, feel free to submit questions at any time by using the questions box.
A follow-up e-mail will be sent to all attendees with links to the presentation materials online.
Dr. Robert Wachter Chief of the Division of Hospital Medicine UCSF Medical Center
Panelists:
WEBINAR HOUSEKEEPING

WEBINAR
NOW SPEAKING
How hospitalists can lead on quality
Please use the questions box on your webinar dashboard to submit questions to our moderator
Maureen McKinneyEditorial Programs
Manager Modern Healthcare
WEBINAR
NOW SPEAKING
How hospitalists can lead on quality
Please use the questions box on your webinar dashboard to submit questions to our moderator
Dr. Robert WachterChief of the Division of
Hospital Medicine UCSF Medical Center
Wachter RM, Goldman L. NEJM 1996
An SAT Question
Is to The…
As Is to …
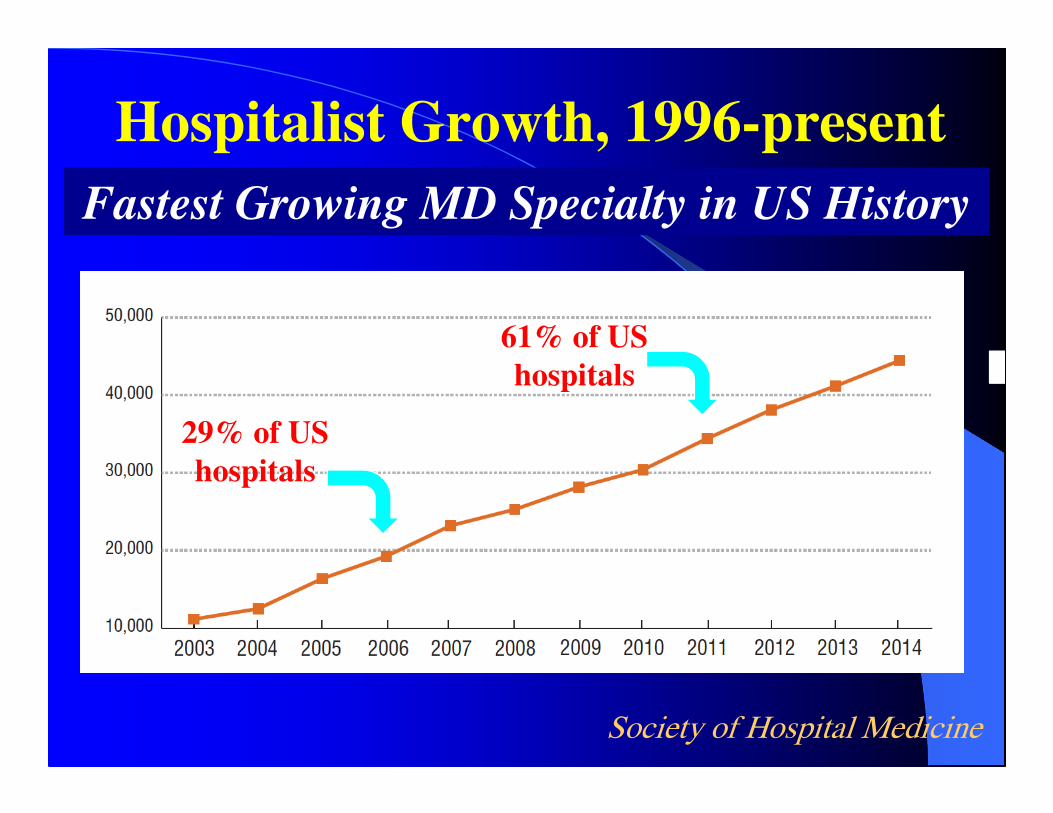
Hospitalist Growth, 1996-present
Society of Hospital Medicine
29% of US
hospitals
61% of US
hospitals
Fastest Growing MD Specialty in US History

Why We’re Being Pressured to Change

“The Challenge That Will
Dominate Your Career…”
Do Data Support Hospitalists’’’’ ““““Value””””?
Yes (generally)
Wachter, JAMA 2002 & many others
Key organizational question: do the advantages of
focused practice and on-site presence outweigh the
disadvantages of ““““purposeful discontinuity””””
Vast majority of published studies show ~15% fall
in costs and LOS; many now show better quality
The Fundamental Economic
Truths of the Hospitalist Field
�Non-procedural E&M hospital codes are a tough way to make a living
�90% of hospitalist groups receive support– > $20B (40K hospitalists x $150K/MD x 90%) in
new hospital -> MD dollars since field began
�This isn’t charity: there must be a ROI – Initially, this was cost and LOS reduction
– Now increasingly quality, safety, pt experience, IT
�A positive side-effect: unique hospital-MD alignment/synergy; perhaps a model for others
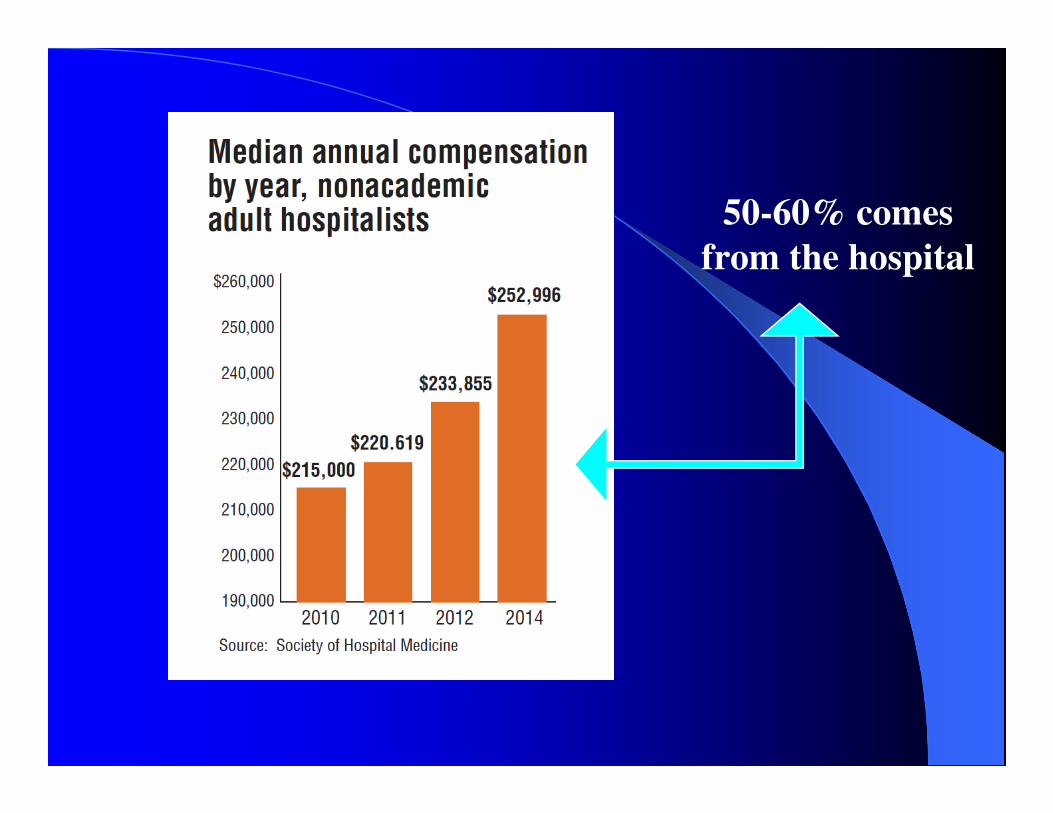
50-60% comes
from the hospital
My Decision as SHM Prez in 1999
�Risk that hospitalists were being branded as
being all about efficiency, LOS
�No physician wants to be “about”
getting grandma out of the
building a day earlier
�To Err is Human published:
opportunity for hospital
medicine to “own” safety, quality
�The “two sick patients” mantra
Business Case for Quality and
Safety has Grown
�Percent of hospital dollars at risk based on
performance in 2000: zero
�Percent at risk in 2008: zero (but stricter
accreditation requirements, public reporting)
�Percent at risk in 2014: 3-4%
�Percent at risk in 2017: 7-8%
�Percent at risk in 2020: who knows, but more
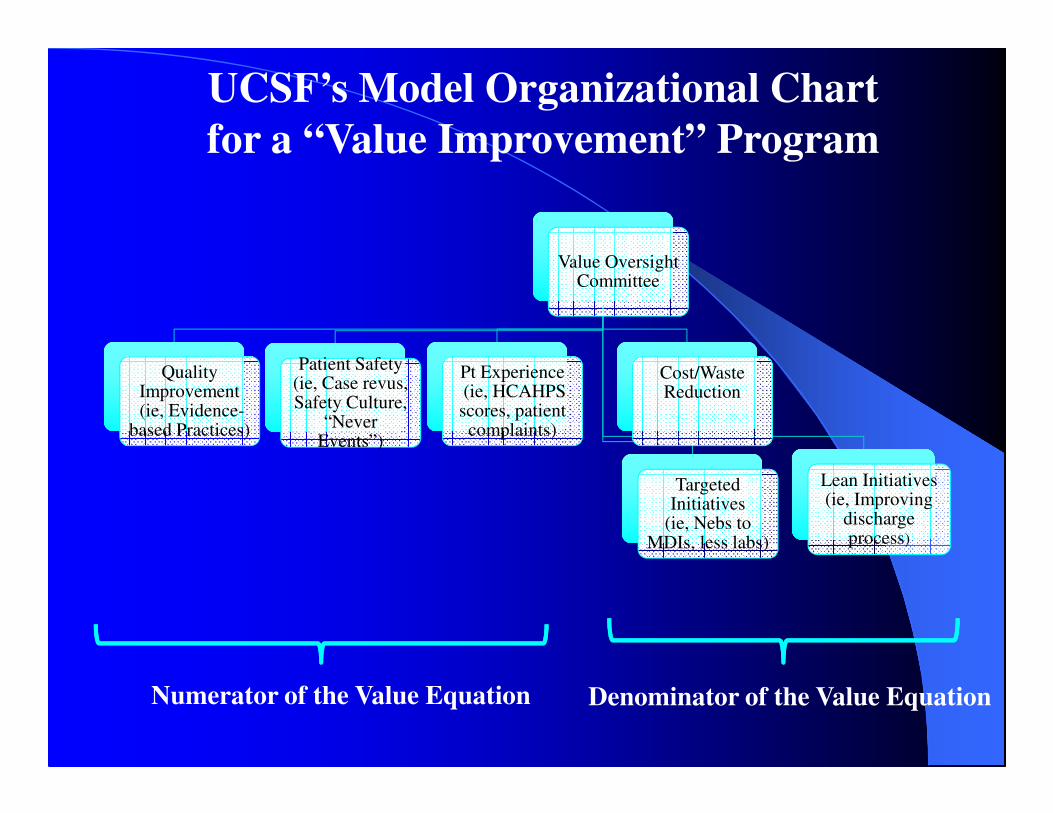
Value Oversight Committee
Quality Improvement(ie, Evidence-
based Practices)
Pt Experience(ie, HCAHPS scores, patient complaints)
Patient Safety(ie, Case revus, Safety Culture,
“Never Events”)
Cost/Waste Reduction
Targeted Initiatives
(ie, Nebs to MDIs, less labs)
Lean Initiatives (ie, Improving
discharge process)
Numerator of the Value Equation Denominator of the Value Equation
UCSF’s Model Organizational Chart
for a “Value Improvement” Program

Hospitalists as System Leaders
The Bottom Line and a Few Predictions
� Hospitalists are now the major U.S. providers of hospital
care
� Studies will continue to show improved value
� The Swiss-army-knife-nature of the field will make it a
perpetually exciting (and challenging) place to be
– Uniquely context dependent
� Often an island of MD-hospital integration in a non-ACO
world (and doesn’t take 50 yrs to build)
� The U.S. healthcare marketplace will
not tolerate failure to innovate in the
name of tradition
Could this be worse?
“We think that the anxiety, demoralization, and sense of loss of control that afflict all too many healthcare
professionals today comes not from finding themselves to be participants in systems of care, but rather from
finding themselves lacking the skills and knowledge to thrive as effective, proud, and well-oriented agents of
change in those systems…. A physician equipped to help improve healthcare will be not demoralized, but
optimistic; not helpless in the face of complexity, but empowered; not frightened by measurement, but made curious and more interested; not forced by culture to
wear the mask of the lonely hero, but armed with confidence to make a better contribution to the whole.”
Berwick & Finkelstein, Acad Med 2010

WEBINAR
NOW SPEAKING
How hospitalists can lead on quality
Please use the questions box on your webinar dashboard to submit questions to our moderator
Dr. Vercin EphremChief of Hospital Medicine
LRGHealthcare
LRGHealthcare
• Lakes Region General Hospital-137 Bed Rural Community Hospital
• Franklin Regional Hospital-25 Bed Critical Access Hospital
• Two Ambulatory Surgery Centers
• 100+ Provider Practices including 2 Rural Health Clinics
• 13 Hospitalists & 6 APRNs for 2 hospitals & 4 Nursing Homes
• 32,597 ED Visits/Year, 16 % ED Admits

Hospitalists in Community Hospital
Leading Quality
• Ideal Position, Since Hospitalist is Knowledgeable about the Entire
Patient Care Continuum
• Working with Same Team on a Daily Basis to Ensure Best Practices
Are Followed
• Easier to Implement Quality Improvements projects & Ensure that
they are Being Followed
• Ability to Involve Other Community Partners in Quality Projects
Challenges to Hospitalists in Community
Hospital Leading Quality
• Financial Support
• Staff Support
• Few Resources
• Launched in 2010, BOOST Implementation Team included
other Health Care Related Agencies including Home Health,
Mental Health, Long Term Care
•Common Goals
•Developed Systems to Communicate & Coordinate in
Caring for Patients
•Used all the BOOST Tools such Risk Identification, Teach-
Back, etc.
Implementation of BOOST-Better Outcomes By
Optimizing Safe Transitions
• Patient Flow Meetings:
• Co-Chairs Hospitalist/ ER
• Bed “Czar” Concept
• “Bed Ahead” Process
• Bridge Orders to Facilitate Admission
• Hall Beds
Process Improvements in Transitioning Patients from
ED to Bed
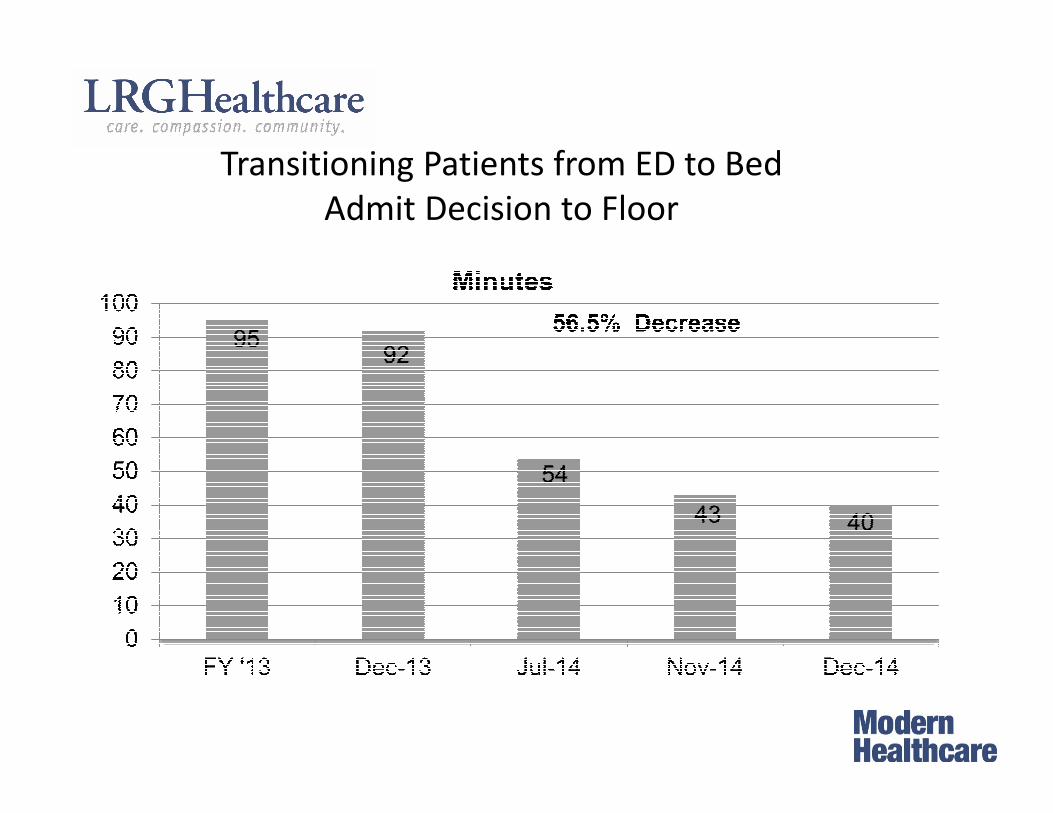
Transitioning Patients from ED to Bed
Admit Decision to Floor
•Daily Rounding with Hospitalist and the Entire
Multidisciplinary Team
•Medication Reconciliation with Hospitalist and Clinical
Pharmacist Day Prior to Discharged
•Weekly Meeting to Discuss “Challenging Discharges” &
Review of Readmissions for Learning by Team
•“Almost Home” to Teach Patients/Families to Care for
Themselves at Home
•As of Feb, 2015, Bedside Medication Delivery Prior to
Discharge
Process Improvements in Transitioning Patients from
Bed to Discharge
• Home Care, Embedded Care Coordinator, Long Term
Care Staff at Discharge Planning Meeting Helping to
Facilitate Communication About Patient
• Hospitalist contacting PCP Prior to Discharge
• Follow up Appointment with PCP within 3 to 7 Days
• Embedded Care Coordinators making follow up
phone calls to patients within 48 hours of Discharge
• Hospitalists caring for patients in the Nursing Homes
Transitioning Patients from Discharge to
Nursing Home or Home
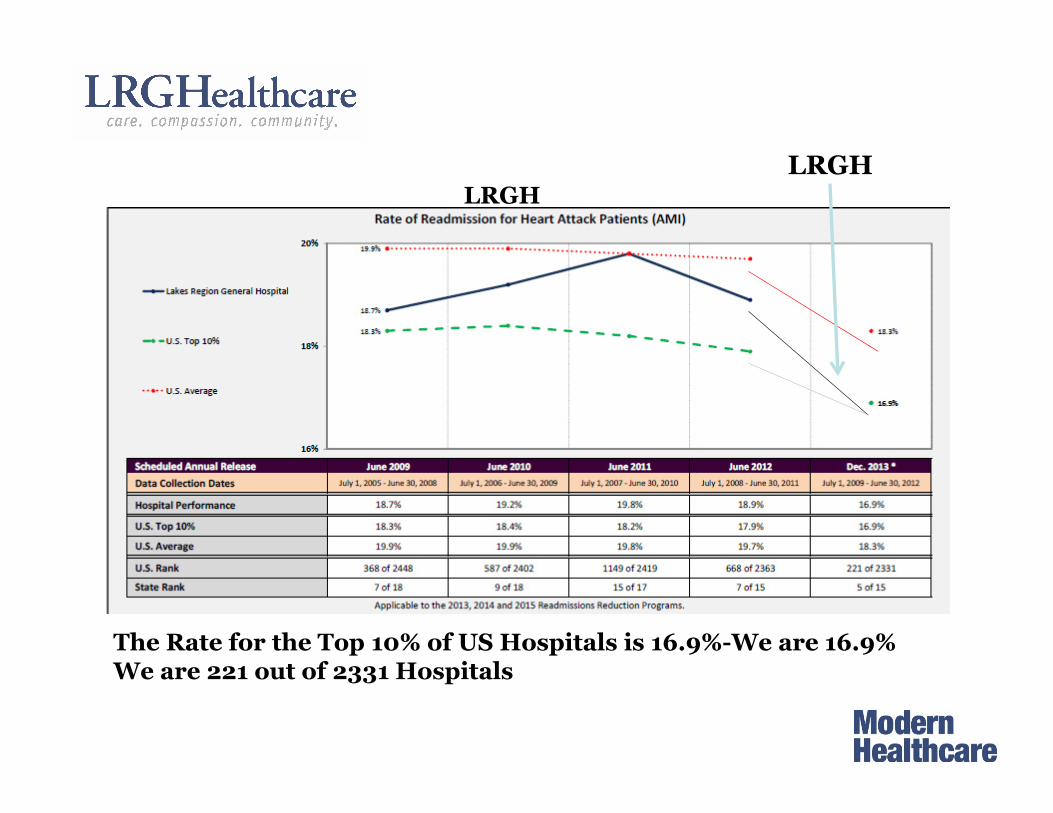
The Rate for the Top 10% of US Hospitals is 16.9%-We are 16.9%We are 221 out of 2331 Hospitals
LRGH
LRGH
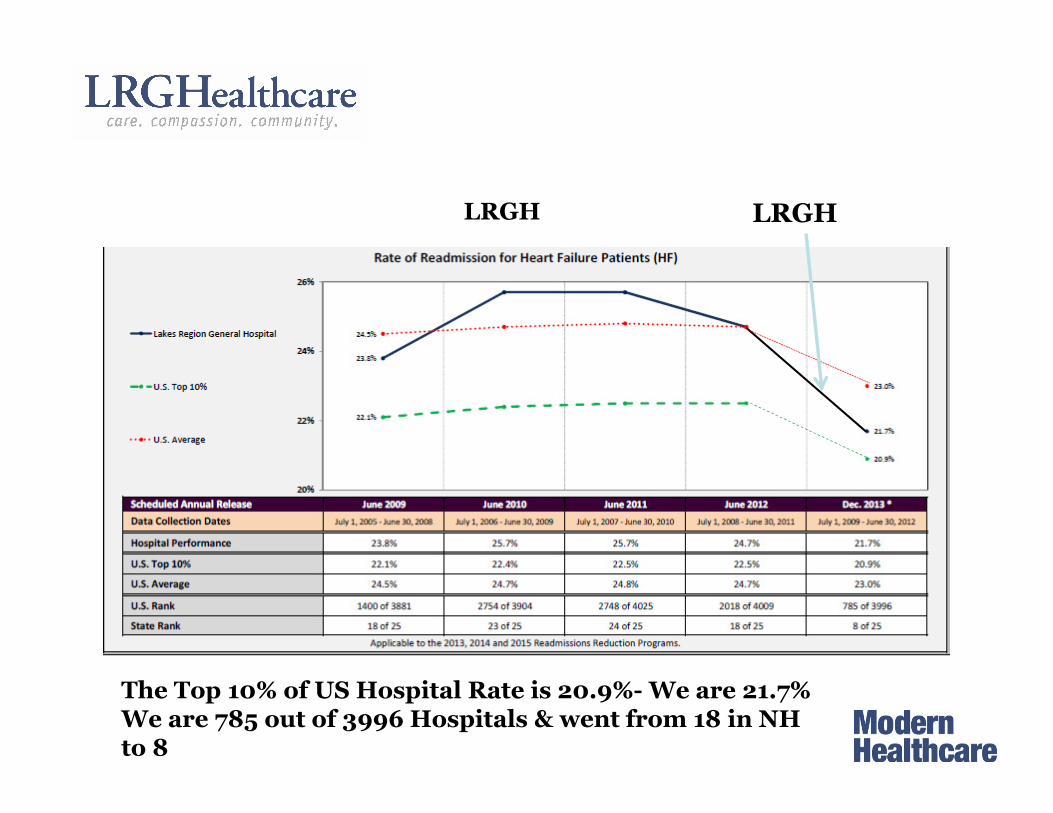
The Top 10% of US Hospital Rate is 20.9%- We are 21.7% We are 785 out of 3996 Hospitals & went from 18 in NH to 8
LRGH LRGH
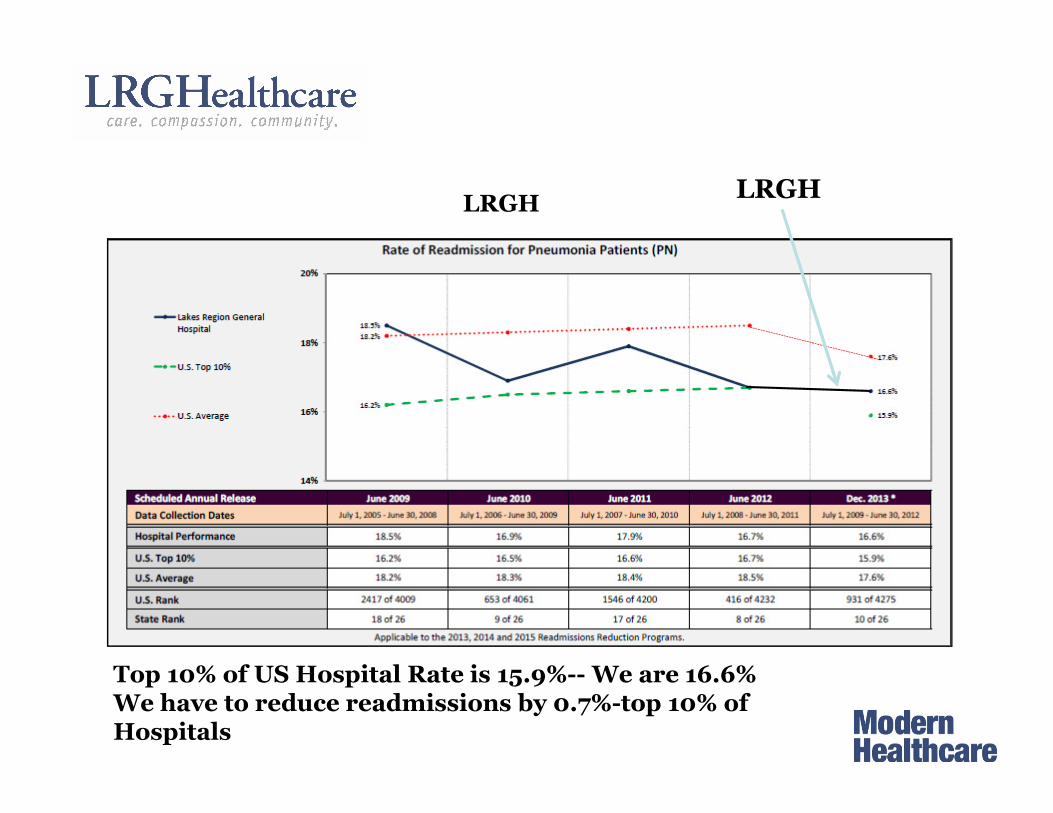
Top 10% of US Hospital Rate is 15.9%-- We are 16.6%We have to reduce readmissions by 0.7%-top 10% of Hospitals
LRGHLRGH
LRGHealthcare
WEBINAR
NOW SPEAKING
How hospitalists can lead on quality
Please use the questions box on your webinar dashboard to submit questions to our moderator
Dr. Kevin O’LearyChief of the Division of
Hospital Medicine Northwestern University
Feinberg School of Medicine
How Hospitalists can Lead
Quality
Kevin O’Leary MD, MS
Northwestern Medicine
Recognize trends that affect both
hospitals and hospital medicine
ACA Impact on Hospitals
• Will expand the base of insured patients
• Decrease overall payment rates to hospitals
• Incentives and penalties
– Readmission Reduction Program
– Value Based Purchasing
– HAC Reduction Program
– Bundled payments
– Accountable Care Organizations
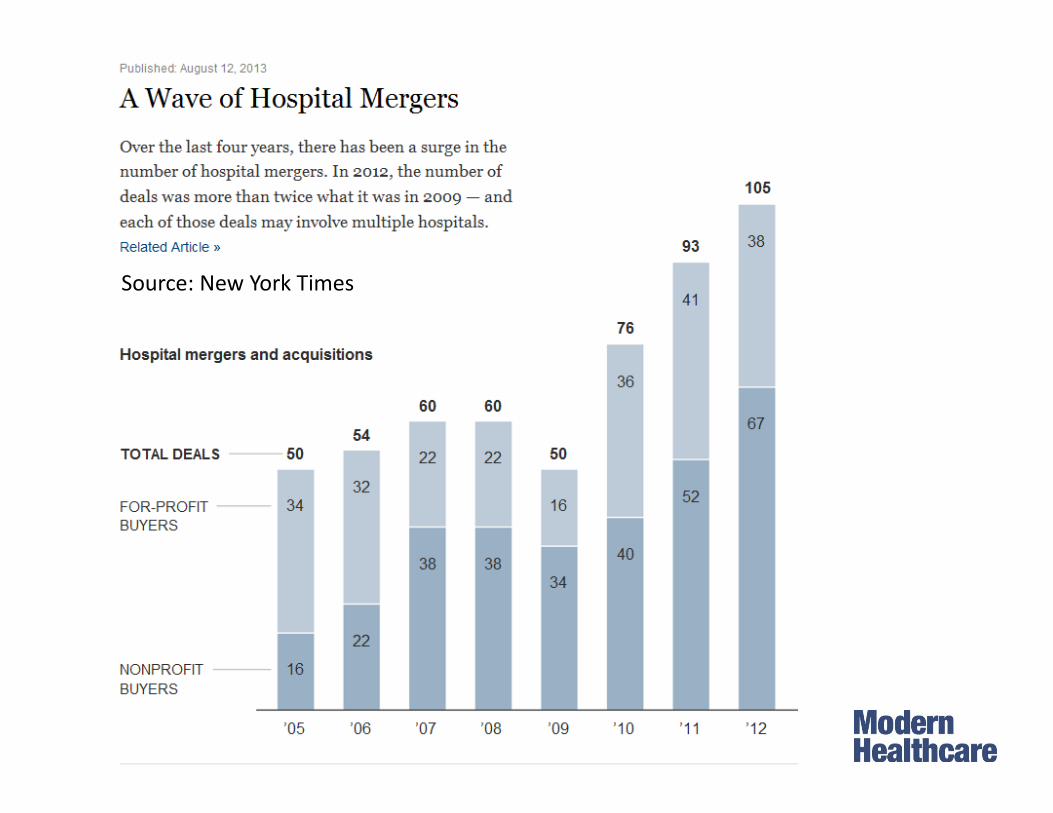
Source: New York Times
What does consolidation mean for
hospitalists?
• Hospitals will prefer single group per hospital
• Lays foundation for true partnership
• Potential for collaboration across sites
– Joint recruitment, credentialing
– Share best practices, innovate on larger scale
• Pressure to address population health (high
utilizers, recidivist patients)

Create innovative partnerships
between hospitalists and hospital
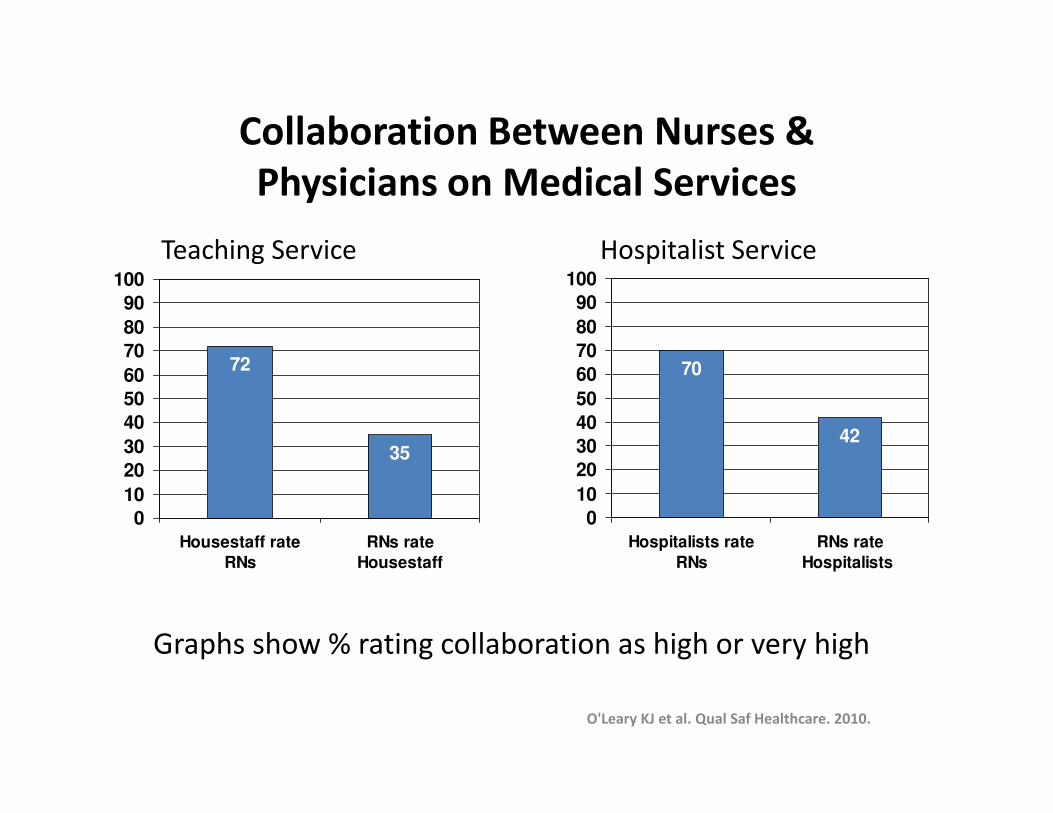
Collaboration Between Nurses &
Physicians on Medical Services
70
42
0
10
20
30
40
50
60
70
80
90
100
Hospitalists rate
RNs
RNs rate
Hospitalists
Graphs show % rating collaboration as high or very high
72
35
0
10
20
30
40
50
60
70
80
90
100
Housestaff rate
RNs
RNs rate
Housestaff
Teaching Service Hospitalist Service
O'Leary KJ et al. Qual Saf Healthcare. 2010.
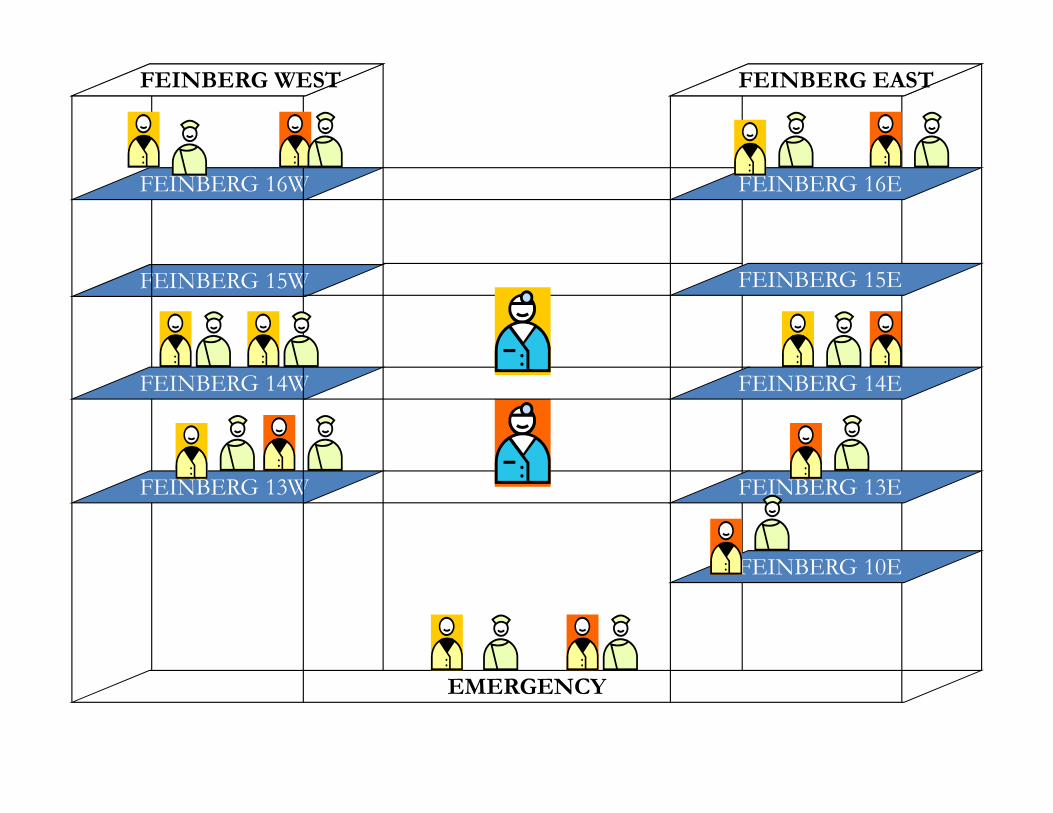
FEINBERG 15W
EMERGENCY
FEINBERG 16W
FEINBERG 14W
FEINBERG 13W
FEINBERG 16E
FEINBERG 14E
FEINBERG 13E
FEINBERG 10E
FEINBERG WEST FEINBERG EAST
FEINBERG 15E
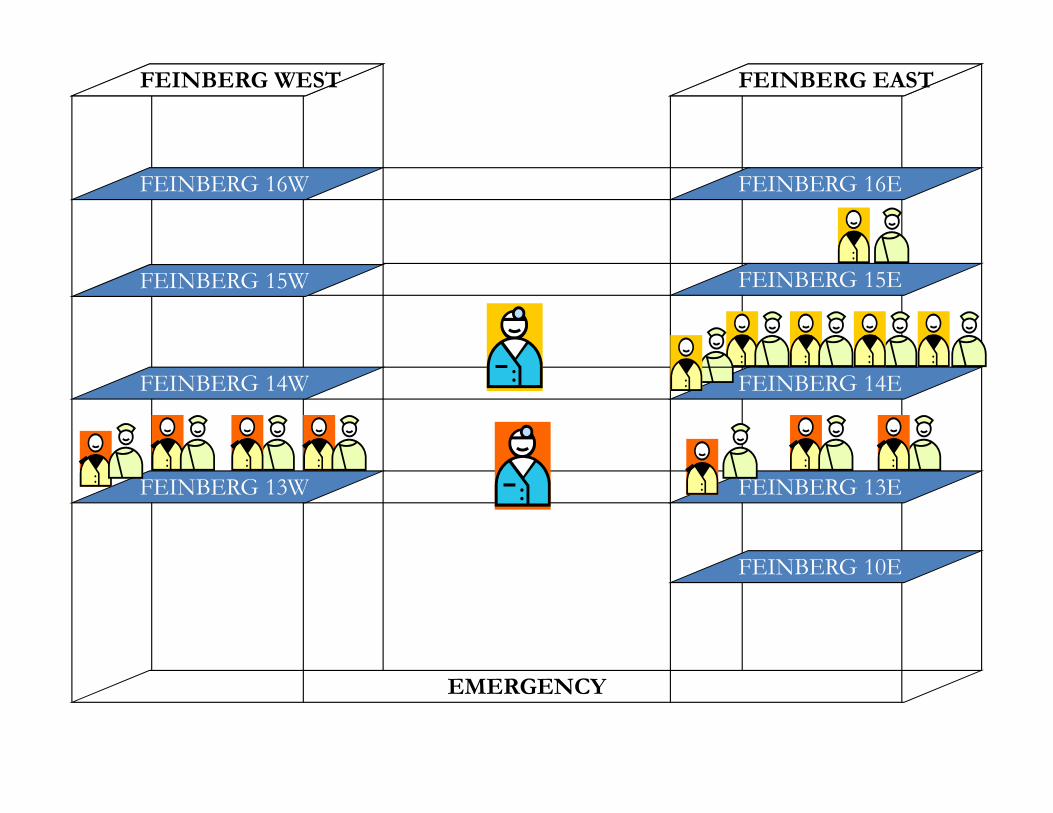
EMERGENCY
FEINBERG 16E
FEINBERG 15E
FEINBERG 14E
FEINBERG 13E
FEINBERG 10E
FEINBERG WEST FEINBERG EAST
FEINBERG 16W
FEINBERG 15W
FEINBERG 14W
FEINBERG 13W
• Unit Based Co-leadership
– Nurse manager and unit medical director
– Co-leadership training
• Structured Inter-Disciplinary Rounds (SIDR)
– Designed by frontline professionals
– Uses a structured communication tool
– Nurse manager & medical director co-facilitate
– All RNs, physicians, pharmacists, social work, and case management attend
INTERACT Intervention:
Unit Based Co-leadership and SIDR
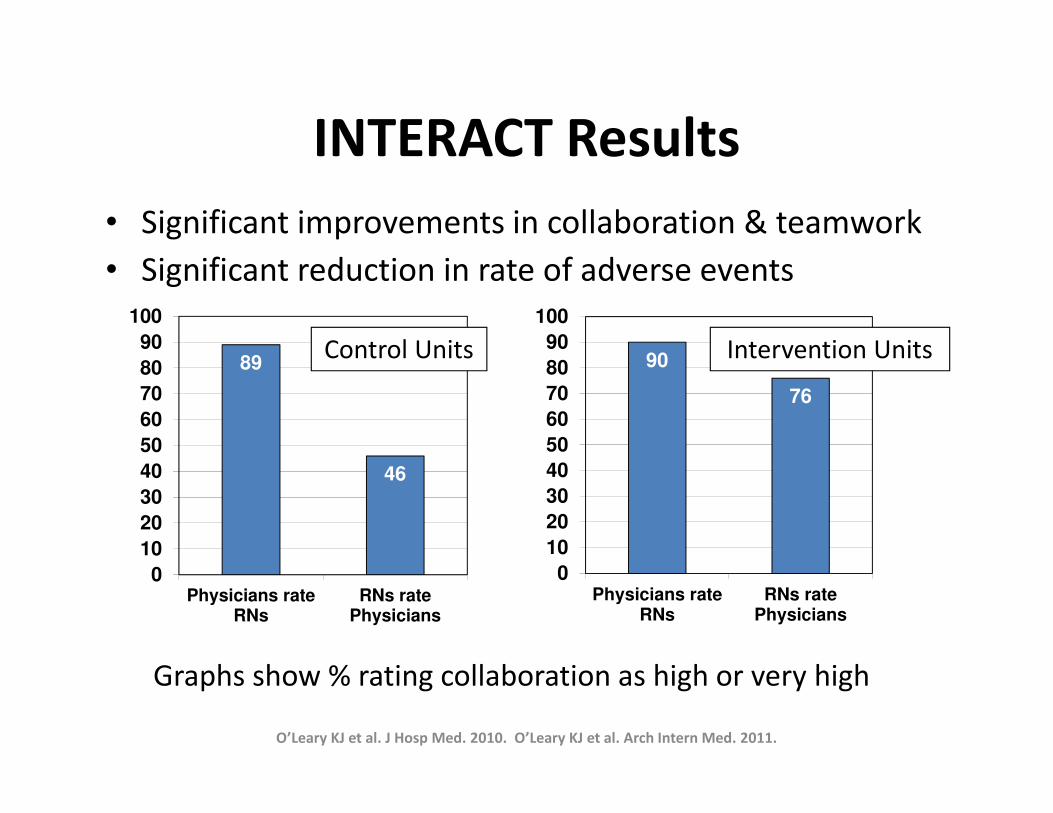
INTERACT Results
• Significant improvements in collaboration & teamwork
• Significant reduction in rate of adverse events
O’Leary KJ et al. J Hosp Med. 2010. O’Leary KJ et al. Arch Intern Med. 2011.
89
46
0
10
20
30
40
50
60
70
80
90
100
Physicians rateRNs
RNs ratePhysicians
90
76
0
10
20
30
40
50
60
70
80
90
100
Physicians rateRNs
RNs ratePhysicians
Control Units Intervention Units
Graphs show % rating collaboration as high or very high

Develop Quality Improvement
Leaders
Professional Development
Opportunities in QI
• Internal programs
• Certificate programs
– Intermountain Healthcare ATP, IHI, NAHQ
• Masters programs
– Northwestern, Thomas Jefferson University
Hospitals should invest in professional development
Hospitalists and Hospital QI: You
complete me
You had me at hello!

WEBINAR
TODAY’S PANELISTS
How hospitalists can lead on quality
During today’s discussion, feel free to submit questions at any time by using the questions box
Dr. Kevin O’Leary Chief of the Division of
Hospital Medicine Northwestern University
Feinberg School of Medicine
Dr. Vercin Ephrem Chief of Hospital
Medicine LRGHealthcare
Maureen McKinney Editorial Programs
Manager Modern Healthcare
Dr. Robert Wachter Chief of the Division of Hospital Medicine UCSF Medical Center
Expect a follow-up email within two weeks with links to presentation materials and information about how to offer feedback.
For more information about upcoming webinars, please visit ModernHealthcare.com/webinars
WEBINAR THANK YOU FOR ATTENDINGHow hospitalists can lead on qualityThanks also to our panelists:
Dr. Kevin O’Leary Chief of the Division of Hospital Medicine Northwestern University Feinberg School of Medicine
Dr. Vercin Ephrem Chief of Hospital Medicine LRGHealthcare
Maureen McKinney Editorial Programs Manager Modern Healthcare
Dr. Robert Wachter Chief of the Division of Hospital Medicine UCSF Medical Center