Embed Size (px)
Citation preview
THE RELATIONSHIP BETWEEN HOSPITALISTS
AND PRIMARY CARE PHYSICIANS
by
JAMES R. BURKHART
S. ROBERT HERNANDEZ, COMMITTEE CHAIR
D. ROB HALEY
LARRY R. HEARLD
JEFF M. SZYCHOWSKI
A DISSERTATION
Submitted to the graduate faculty of The University of Alabama at Birmingham
in partial fulfillment of the requirements for the degree of
Executive Doctor of Science in Administration – Health Services
Birmingham, Alabama
2012

Copyright by
James R. Burkhart
2012
iii
THE RELATIONSHIP BETWEEN HOSPITALISTS
AND PRIMARY CARE PHYSICIANS
JAMES R. BURKHART
EXECUTIVE DOCTOR OF SCIENCE IN ADMINISTRATION-HEALTH SERVICES
ABSTRACT
A study of the relationship between primary care physicians (PCPs) and
hospitalists was conducted by surveying the Florida Academy of Family Physicians
(FAFP) membership to determine whether they had an established relationship with a
hospitalist or hospitalist group. The survey responses were then matched with Blue Cross
and Blue Shield of Florida (BCBSF) administrative claims data to provide two groupings
of study respondents with data regarding patients’ average length-of-stay, average 30 day
readmission rate, and average hospital claims payment. The survey also gathered
demographic data, including physicians’ graduation decade, practice locale, type of
practice setting, and employment status. Key questions determined the level of
communication effectiveness between hospitalists and PCPs, the time it takes to receive
notification of patients’ hospitalization, and the time it takes to receive patient
information post-discharge. Although the results of the study did not demonstrate
statistical significance between the two study groups, based on the three outcomes
measures, the relationship between hospitalists and PCPs clearly indicates the need for
additional research in this area.
Keywords: physician relationship, patient outcomes, hospitalists, family physician,
communication
iv
DEDICATION
I dedicate this dissertation to my wife of 35 years, Tina, who has supported me in
all of my career endeavors regardless of the time and resources required to accomplish
my professional goals. Your love and understanding cannot be measured, and your
patience and support, especially when I was not as available to the family as either one of
us would have liked, is remarkable.
To my parents and children, for always believing that I could do anything I set out
to do, and for supporting me with my educational pursuits over the years.
To the University of Florida Academic Health Center (UF&Shands) leadership
team, hospital staff, and medical staff, thanks for your support and encouragement during
my doctoral studies.
To the educators at the University of Alabama, Birmingham (UAB), for having
the foresight to start the doctoral program in Executive Healthcare Management, and for
driving me to achieve my educational goals at both the Master’s and Doctorate level.
v
ACKNOWLEDGEMENTS
I want to personally acknowledge the leadership of UF&Shands, specifically the
Chairman of the Board, Dr. David Guzick, for his phenomenal support and
encouragement during the pursuit of my doctoral degree. I could not have achieved this
milestone in my professional career without the constant support of the management and
staff of my organization. I will always be indebted to each of you.
I also want to thank my dissertation committee, including Dr. S. Robert
Hernandez, Dr. Larry Hearld, Dr. Jeff Szychowski, and Dr. Rob Haley. Your support,
guidance, and motivation gave me the resolve to make it through this dissertation project.
Much gratitude to Steve Blumberg, Kathy Poppell, Jean Marie Hubler and Kelly
Miles of UF&Shands, Jay Milson and Jennifer Young of the Florida Academy of Family
Physicians (FAFP), and Joyce Kramzer, Dr. Jonathan Gavras and Dr. Michael Ryan of
BCBSF for helping me with the data and reviewing my work along the way.
Special acknowledgement goes to Carmen Smotherman of the University of
Florida – Jacksonville, and Jim Willis of BCBSF. Without your time and efforts on my
behalf this project could not have been completed.
Finally, to my classmates and UAB faculty – the friendships and professional
acquaintances I have made during my professional journey will last a lifetime and I will
always be thankful that you were part of my life.
vi
TABLE OF CONTENTS
Page
ABSTRACT ...................................................................................................................... iii
LIST OF TABLES ............................................................................................................. ix
LIST OF FIGURES .............................................................................................................x
LIST OF ABBREVIATIONS ............................................................................................ xi
CHAPTER
1 INTRODUCTION ..........................................................................................................1
Significance of the Study ........................................................................................6
Research Question ..................................................................................................7
Plan of Work ...........................................................................................................8
2 LITERATURE REVIEW ..............................................................................................9
Provider Descriptive ...............................................................................................9
Satisfaction Levels ................................................................................................14
Communication Effectiveness ..............................................................................17
Productivity and Efficiency ..................................................................................22
Patient Outcomes and Clinical Quality .................................................................24
Exchange Theory ..................................................................................................25
Literature Summary ..............................................................................................30
3 RESEARCH METHODOLOGY AND THEORETICAL FRAMEWORK ...............32
Purpose of This Study ...........................................................................................32
Research Question ................................................................................................32
vii
Hypotheses ............................................................................................................33
Data Collection .....................................................................................................34
Statistical Analysis ................................................................................................39
4 RESULTS AND FINDINGS .......................................................................................42
Data Description ....................................................................................................43
Survey Respondents ......................................................................................43
Study Participant Demographics ..................................................................45
Relationship between FP and Hospitalists ....................................................46
Communication between FP and Hospitalists ..............................................48
Respondent Data Analysis ...........................................................................51
Year of Graduation and FP / Hospitalist Relationship..................................51
Practice Locale and FP / Hospitalist Relationship ........................................51
Employment Status and FP / Hospitalist Relationship ................................52
Type of Practice and FP / Hospitalist Relationship .....................................52
Summary of Hypothesis Testing ...........................................................................53
Cost of Care ..................................................................................................53
Length of Stay ..............................................................................................54
Readmission Rate .........................................................................................55
Additional Analysis .....................................................................................56
5 SUMMARY AND CONCLUSIONS ..........................................................................60
Conclusions and Implications ...............................................................................60
Ratings of Communication between FPs and Hospitalists ...........................61
Survey Comments about Communications between FPs and Hospitalists ...62
viii
Limitations of the Study ...............................................................................65
Recommendations for Future Study ............................................................67
Summary ...............................................................................................................69
LIST OF REFERENCES ..................................................................................................70
APPENDICES ..................................................................................................................75
A Letter to FAFP Members ......................................................................................75
B Survey Instrument .................................................................................................77
C UAB IRB Approval Form .....................................................................................81
D UF IRB Approval Letter .......................................................................................82
ix
LIST OF TABLES
Table Page
1 Descriptive Statistics for Total Survey Respondents+ .................................................44
2 Descriptive Statistics for Partial and Completed Survey Respondents+ ......................46
3 Descriptive Statistics for Study Group (BCBSF data available)+
................................47
4 Descriptive Statistics for Established Relationship and Communication
Questions+ ....................................................................................................................50
5 Type of Practice New Categories ................................................................................53
6 Outcome Variable – Cost of Care .................................................................................54
7 Outcome Variable – Length of Stay .............................................................................55
8 Outcome Variable – Readmission Rate .......................................................................55
9 Analysis of Variance – Outcome: Length of Stay ......................................................56
10 Analysis of Variance – Outcome: Readmission Rate ..................................................57
11 Analysis of Variance – Outcome: Charges ...................................................................57
12 Additional Analysis on Communication ......................................................................58
13 Additional Analysis on Locale......................................................................................59
x
LIST OF FIGURES
Figure Page
1 Inclusion / Exclusion Criteria ......................................................................................45
xi
LIST OF ABBREVIATIONS
AAFP American Academy of Family Physicians
AAP American Academy of Pediatrics
ACP American College of Physicians
ANCOVA analysis of covariance
AOA American Osteopathic Association
BCBSF Blue Cross Blue Shield of Florida
CMS Center for Medicare and Medicaid Services
DRG diagnostic related groups
ED emergency department
EKG electrocardiogram
FAFP Florida Academy of Family Physicians
FP family physician
HCAHPS Hospital Consumer Awareness of Healthcare Providers and Systems
HHS United States Department of Health and Human Services
HIV human immunodeficiency virus
LOS length-of-stay
NPI National Provider Identifier
PCMH patient-centered medical homes
PCP primary care physician
SHM Society of Hospital Medicine
1
CHAPTER 1
INTRODUCTION
Before the mid-1980s, medical school graduates who chose to go into primary
care assumed that they would have both an office practice and follow their patients when
they were admitted to the hospital. Academic programs of that time were designed to
teach residents about taking care of patients in outpatient settings, but the majority of
their training took place in the hospital. Most individuals choosing general or family
medicine as a career felt that they would have a wide variety of patient care exposure
from routine health check-ups, but also thought that they would be taking care of their
patients during acute and chronic illness. They expected to establish relationships with
their patients that allowed them to remain the ‘physician-of-record’ across all care
settings. This had been the model of care for many years and no one foresaw the
significant change that came about due to dramatic modifications in government
reimbursement schemes in 1983.
Suddenly, hospital reimbursement by Medicare was placed under a system based
on the episode of care and the primary diagnosis that led to hospital admission (Hamel,
Drazen, & Epstein, 2009). A major concern during post-discharge transition was the
possible failure of physicians to communicate effectively with each other regarding
patient care. This lack of communication has been shown to have an adverse effect on
post-discharge transitions and can lead to safety and quality deficiencies in patient care
(Snow et al., 2009).
2
By the early 90s, hospitalized patients also had more significant illness, requiring
more physician time to expedite discharges. Tests had to be performed quickly, and then
followed-up with the necessary orders to move patients as rapidly as possible. Many
primary care physicians (PCPs), who had to see greater numbers of patients in their office
to survive economically, found that maintaining a hospital-based practice was not cost-
effective, and that they could increase their income by focusing on their office practice.
As a result, a new field of medicine emerged, called hospital medicine, along with a new
brand of physician, the hospitalist.
A recent summary of the literature by a Society of Hospital Medicine / Society of
General Internal Medicine Task Force found that direct communication between hospital
physicians (hospitalists) and PCPs occurred infrequently (in 3%-20% of cases studied).
The availability of a discharge summary at the first post-discharge visit was also low at
(12%-34%) and this availability did not improve greatly even after four weeks (51%-
77%). This lack of availability affected the quality of care in approximately 25% of
follow-up visits. It revealed that communication between PCPs and hospitalists creates a
loop of continuous care and helps diminish morbidity and mortality at the critical
transition point. It further concluded that, although this transition period can be risky, it
can also benefit care if a new physician notices something overlooked by the other
physician (Snow et al., 2009).
The development of the hospitalist specialty has been strongly influenced by
changes in reimbursement methods for inpatient hospital services. Diagnostic-related
groups (DRGs) were implemented in 1983. Hospitals were then under intense pressure to
shorten length-of-stay (LOS) and lower costs under the new fixed-payment system.
3
Hospital administrators were incented to facilitate shorter LOS, which was in direct
conflict with physicians, who were being paid for each day of service. This led to hurried
patient discharges and higher thresholds for hospitalizations. PCPs, which formerly had
8-12 hospitalized patients per day, were seeing their count drop to 1-3 hospitalized
patients per day. Many patients, who in the past would have been hospitalized, were now
being seen on an outpatient basis in their PCP’s office (Wachter, 2009).
Early on, hospitalists focused on the care that was once provided by the PCP.
However, as reimbursement models have continued to change, even specialists have
sought out hospitalists to manage the routine care of their patients while they are
hospitalized. Specialists tend to ‘consult’ patients and allow the hospitalist to provide
other care. Surgeons realize that much of the pre and post-surgical care is more medical
in nature than surgical. Patients requiring wound care, management of diabetes or blood
pressure, those with infections, and those with pulmonary problems are examples of
patients who are better managed by a physician who practices hospital medicine and does
not maintain an office practice. Finally, in academic medical centers, the new limitations
on residency work hours has caused many internal medicine, pediatric, and other
specialties to cap the number of patients their residents can follow in the hospital.
Hospitalists then found a new source of demand for their services (Geehr, & Nelson,
2002).
A study at six U.S. academic medical centers surveyed 1,772 PCPs caring for
2,336 patients and received responses from 908 PCPs representing 1,078 patients. The
results revealed that 77% of the PCPs knew that their patients were in the hospital, but
only had direct communication with the hospitalist 23% of the time. The PCPs received
4
discharge summaries within two weeks 42% of the time and within 30 days of discharge
22% of the patients studied had either revisited the emergency department (ED), been
readmitted, or had died. Results demonstrated the critical need for improvements in the
communication between PCPs and inpatient medical teams, but the study was not able to
demonstrate a significant relationship between several aspects of communication and the
associated adverse clinical outcomes in this patient sample (Bell et al., 2009).
Training in the hospitalist field focuses on many areas that lack quality instruction
in medical schools. Hospitalists are required to work effectively with other health
providers such as pharmacists and nurses. To do this, they must have good overall
communication skills, know how to improve systems of care, have patient quality and
safety skills, and know how to co-manage patients with other specialties. They are able
to round on their assigned patients throughout the day providing a level of care that
cannot be replicated by the patient’s PCP (Wachter, 2009). Because of cost pressures on
the healthcare delivery system, managed care organizations reward professionals who can
provide efficient care to a large panel of patients and be available in the office to see
them promptly as required.
In the hospital setting, parallel pressures for efficiency exist because of the
intensive use of resources, the need to respond quickly to the changes in a patient’s
condition, and the requirement to use resources judiciously. Wachter and Goldman
(1996) suggest that hospitalists should excel in this type of environment and that the
forces promoting the use of the hospitalist model is sufficiently compelling that this
model will continue to be adopted in both teaching and nonteaching settings. As with
any major transition, the medical community must continually reevaluate the new
5
approach to ensure that any possible discontinuity in care is outweighed by improved
clinical outcomes, lower costs, better education for physicians, and greater patient
satisfaction.
The U.S. healthcare system is composed of physician practices, hospitals, and
other providers that are poorly integrated, leading to fragmentation across care sites,
providers, and in the clinical decisions made in caring for patients. The current systems
of payment rewards greater volume and leads to care that is too often provided in silos
and results in poor quality outcomes. At the same time, U.S. medical schools are not
producing enough PCPs to care for adults or children. This is because the current
payment system does not adequately incentivize graduating medical students to choose
primary care as a profession. Over the past quarter of a century, more medical school
graduates have chosen to specialize in areas of medicine outside of primary care. The
existing payment structure also makes it economically unattractive for primary care
providers to follow patients during hospitalization.
These dramatic changes have led to a decline in the inpatient activity of primary
physicians and the advent of the hospitalist as the new model for the provision of care to
hospitalized patients. The issue is whether this new system of care that has developed
over the last fifteen years is having a positive effect on the cost of care to patients and
whether the communication between PCPs and their hospital-based counterparts has had
a positive effect on the quality of patient outcomes.
6
Significance of the Study
This study, which focused on the effect on patient outcomes of family physicians
(FPs) that have an established hospitalist relationship versus FPs who have no such
relationship, adds to the body of research on this subject and should contribute to the
management of patients while hospitalized. The study provides information about the
current level of communication that FPs have with hospitalists. In today’s economic
environment, hospitals will continue to rely on physicians who specialize in the practice
of hospital medicine because hospitalists have a core competency for managing patients
during their hospital stay and work to enhance the performance of hospitals and
healthcare delivery systems. Although there is some empirical research on this topic, it is
limited because most studies are single-site, observational studies. The results of the few
available randomized trials have been mixed. It is clear from the literature review that
little is known about the effect that the relationship between hospitalists and PCPs have
on patient outcomes. This study will provide some of the missing information regarding
hospitalists and their effect on patient outcomes.
The reality of ineffective communication and incomplete handoffs may result in
poor information exchange impacting the care of the patient. By involving a hospitalist
in this process, the coordination of patient care should become seamless and the chance
for medical error should decrease. Wachter (2009) stressed that the key to the future of
the hospitalist model is relationship management. FPs no longer have time to follow
patients admitted to the hospital. The benefit of the hospitalist model should help
mitigate the discontinuity of care to the patient that may be introduced by the increased
demands on PCPs time. Hospitalists should also improve efficiencies in the hospital
7
episode of care, and allow for the more effective use of limited primary care resources.
This study will discuss the concept of exchange theory and evaluate whether FPs who
have developed an established relationship with a hospitalist or hospitalist group have
significantly different patient outcomes than FPs who have no such relationship.
Hospitalists must become more involved in providing continuity to the delivery of
healthcare services and effective communication processes can help resolve the
disconnect that exists as a patient moves across the continuum of care.
Research Question
Because hospital medicine now plays a critical role in the care of hospitalized
patients in the U.S., it is important to evaluate the relationship between hospitalists and
FPs and understand the effectiveness of the communication between these two vital
components of the patient care continuum. This study will address the following research
question: Do FPs who have an established relationship with a hospitalist (six months or
greater) have significantly different patient outcomes for their hospitalized patients than
FPs who have no established relationship with a hospitalist?
In addition to the primary research question, the survey tool asked participants
who have an ongoing relationship with a hospitalist or hospitalist group to rate several
aspects of the communication that takes place. The responses to these questions were
used to address the secondary research aim, which was to assess the quality, timeliness,
and effectiveness of the hospitalist relationship and to generate hypotheses for future
study.
8
Plan of Work
Chapter two reviews the literature on the relationships between hospitalists and
FPs. The existing literature regarding communication, patient outcomes, and resource
efficiencies related to hospital medicine will be presented. Chapter three presents the
hypotheses derived from the literature review and describes the sample and research
methods used to test these hypotheses. Chapter four presents the results of the study
related to length-of stay, hospital costs, and readmission rates. This chapter discusses the
characteristics of the hospitalist / FP relationship. Finally, chapter five provides a
summary of the research results, explanation for these results, practical implications for
healthcare providers, study limitations and future research opportunities.
9
CHAPTER 2
LITERATURE REVIEW
There have been a number of studies regarding hospitalists, their emergence in the
healthcare delivery model in the U.S., and the relationship between hospitalists and PCPs.
The goal of this chapter is to provide the reader with a solid understanding of the
literature on this topic and to help identify gaps in the current literature in regards to the
effect that the relationship between hospitalists and PCPs have on patient outcomes. This
review will provide the reader with a description of family practice and hospitalists along
with some facts and figures regarding each of these fields of medicine. Satisfaction level
studies related to the PCP-hospitalist relationship will be discussed from both the
physician and patient perspective. A primary objective of this study will be to provide a
thorough review of the literature that is focused on the communication effectiveness of
the PCP-hospitalist relationship. The review will also provide insight into information
available about the productivity and effectiveness of the hospitalist model of care and any
findings concerning patient outcomes or ‘clinical quality of care’ found in the literature.
Provider Descriptive
The Society of Hospital Medicine (SHM) defines a hospitalist as a physician
specializing in the practice of hospital medicine and dedicated to the delivery of
comprehensive medical care to hospitalized patients (Society of Hospital Medicine
[SHM], 2011). Since Dr. Wachter and Dr. Lee Goldman described the term ‘hospitalist’
in 1996, this model of care has grown quickly and evidence has suggested that
10
hospitalists markedly improved hospital efficiency and might improve quality. The
hospital medicine field is a relatively new specialty that has grown from a few hundred
physicians in the mid-1990s to more than 20,000 in 2009. Most hospitalists are trained in
internal medicine (80%), family medicine (5%), or pediatrics (10%). Some physicians
also have subspecialty training in areas such as pulmonary medicine, critical care, and
infectious disease (Wachter, 2009). Other studies assert that the hospitalist model is here
to stay and that projections of growth in this field of medicine are vastly understated
(Kuo & Goodwin, 2011; Hamel, Drazen, & Epstein, 2009).
The use of hospitalists continues to spread rapidly, as evidenced by a national
survey of internists in 1999, which found that sixty-five percent of respondents reported
that hospitalist services were available to them in the community (Auerbach et al., 2000).
There are more than 6,000 hospitalists practicing in the U.S. and Canada, which admit
more than 3 million patients annually. By the year 2006, hospitalists are expected to
admit more than 14 million patients nationwide. Hospitalists have been well received by
PCPs, provided their services are offered on a voluntary basis (Geehr & Nelson, 2002).
There were more than 14,000 hospitalists practicing in the United States in 2007, and the
number was anticipated to reach 25,000 by 2010 (Kripalani et al., 2007).
Family medicine is the medical specialty that provides continuing and
comprehensive healthcare for individuals and families. FP’s are considered primary care
physicians (PCPs), as the doctors that diagnose and treat 90% of all patient problems.
They describe the cornerstone of their profession as the ongoing, personal patient-
physician relationship focused on integrated care. Because they have long-term
relationships with their patients, FPs know their detailed medical history and are better
11
able to recommend necessary treatment while providing high quality care resulting in
high patient satisfaction (Florida Academy of Family Physicians, 2011). Blue Cross and
Blue Shield of Florida (BCBSF) developed a physician excellence program to reward
physicians committed to the delivery of high-quality care and services to their patients.
Physicians eligible to participate in the program include those working in family practice,
general practice, internal medicine, pediatrics, geriatrics, and obstetrics and gynecology
(Blue Cross and Blue Shield of Florida [BCBSF], 2008).
Often, FPs cannot afford to be the attending physician while their patients are
hospitalized. Currently, reimbursement is based on the quantity of services provided
instead of the quality or outcomes of the care delivered to the patient. This means that
FPs have stopped going to the hospital and have increased the number of patients they
see in their offices. Increased patient demands have contributed to long wait times and
inadequate quality of care to the patient. Many patients say they cannot schedule timely
appointments with their FP so they, along with those who do not have an FP, have
resorted to the use of the hospital EDs for primary care (Bodenheimer, 2006).
The economics of the new healthcare environment necessitates that FPs either
lose contact with their patients when they are hospitalized or develop relationships with
hospitalists. Hospitalists return the patient to their FP for follow-up after discharge
(Florida Academy of Family Physicians [FAFP], 2011). The median income of
specialists in 2009 was almost twice as much as that of PCPs and the income gap
continues to widen. It is not surprising that fewer U.S. medical students are choosing
careers in primary care (Bodenheimer, 2006). The rapid growth in hospitalists can be
attributed to economic, efficiency, and quality pressures, as well as managed care models
12
which require PCPs to see more patients in the outpatient setting. Additional pressures
exist to discharge patients as quickly and efficiently as possible. All of these factors have
helped promote the hospitalist model of care (Leykum & Mortensen, 2010).
From 1980 to 2005, hospital utilization by traditional PCPs declined. This change
began before the emergence of hospitalists and appears related to the declining LOS and
an overall increase in the number of generalist physicians (Chung, 2010). Both of these
factors are consistent with the conclusion that the reduced number of patients a generalist
physician would likely follow in the hospital has weakened their incentives to provide
hospital care (Wachter, 2010). In 2007, hospitalists on average provided 2,011 inpatient
care hours per year. Over 60% averaged 1,342 hours per year of on-call responsibility,
and 73% indicated an average of 299 hours of non-patient work each year. Average
annual gross charges for a hospitalist were $343,512. Each had 2,560 encounters
annually, with 827 new patients (admits and consults), and their relative value units
(RVUs) averaged 3,406. Hospitalists averaged $163,515 in annual compensation, with
63% of the hospitalist groups reporting that they offered bonuses. For the physicians
receiving a bonus, the average annual base salary was $142,698, with an average bonus
of $23,759 (Geehr & Nelson, 2002).
In 2002, 38% of hospitalists were employed by hospitals, as compared to 23% in
1997 (excluding universities), while the number of medical groups that employed
hospitalists declined from 35% to 17% over the same five year period. Hospitalist-only
groups grew significantly over these five years (1997-2002), leading to predictions that
this field of medicine may evolve in the same way as emergency medicine did in the
1970s and 1980s. In 2000, hospitalists were mostly internal medicine physicians (83%)
13
as compared to internal medicine subspecialists (17%). By 2002, the number of internal
medicine subspecialists had dropped to 5%, which may reflect the decline in the number
of pulmonologists who initially provided hospitalist services. Demographics reveal that
the mean age of the hospitalists was 40, most were male (73%), and came from U.S.
medical schools (87%). Hospitalists were satisfied with their work, with 92% being
somewhat or very satisfied, 84% planning to stay in the hospitalist field for 2-3 years, and
64% expecting to continue in the field for more than 7 years (Geehr & Nelson, 2002).
The rapidly changing healthcare environment will continue to put a premium on
the time and availability of PCPs. Many new healthcare reform initiatives are built
around the concept of patient-centered medical “homes,” a concept which strives to
provide a primary care “home” for every American. Major medical associations including
the American Academy of Family Physicians (AAFP), the American Academy of
Pediatrics (AAP), the American College of Physicians (ACP), and the American
Osteopathic Association (AOA), have developed a set of joint principles for patient-
centered medical homes (PCMH). The PCMH model is an approach to insure the
provision of primary care for children, youth, and adults by providing a healthcare setting
that facilitates the physician-patient relationship.
These medical associations have developed a set of joint principles which
includes a personal physician/provider for each patient and physician-directed medical
practice team concept. In addition, there is an orientation on the whole person to include
all stages of life such as acute care, chronic care, preventive care, and end-of-life care.
The PCMH model calls for an integrated care strategy where care is coordinated across
all components of the healthcare delivery system. It includes a system for enhanced
14
access to care by providing for open scheduling, extended hours, and new ways for
patients and physicians to communicate effectively, as well as a system that recognizes
the added value of the medical home model and rewards practitioners in this model with
better payment and incentive based upon savings for the healthcare delivery system.
The overall goal of the PCMH model is to provide better access to healthcare
while increasing patient satisfaction and the overall health of the community served. The
model is designed to provide a single point of coordination for all needed healthcare
services including specialty, hospital, and post-acute services. This model is also
expected to lower overall healthcare costs by eliminating redundancies and unnecessary
care through reductions in unneeded tests, hospital stays and unnecessary visits to
specialists. Hospitalists will play a key role in the PCMH model by becoming part of the
‘team concept’ of care for patients while they are in the hospital which also allows PCPs
to stay in the outpatient and office setting where they offer the most benefit under this
model. (Center for Studying Health System Change, 2008; Rosenthal, 2008; Bailit and
Hughes, 2008).
Satisfaction Levels
The ACP warns that primary care, which is the backbone of the nation’s
healthcare system, is at grave risk of collapse. The basis for this statement is that PCPs
are frustrated with their current working environment due to the uneven quality of care,
inadequate reimbursement, and the fact that fewer U.S. medical students are choosing to
enter the field. PCPs are still expected to treat patients routinely for uncomplicated
upper respiratory, urinary tract infections, diabetes, coronary heart disease, arthritis, and
15
depression. However, these same PCPs are hurried, overworked, and underpaid when
compared to their peers (Bodenheimer, 2006).
The hospitalist model is generally accepted by other physicians, has achieved
many of the attributes of traditional medical specialties, and seems destined to continue to
grow (Wachter & Goldman, 2002). However, critics argue that limiting PCPs to an
outpatient practice threatens their professional identity, thereby further reducing
professional satisfaction (Brown, 1998; Schroeder and Schapiro, 1999; Sox, 1999).
There is also general disagreement among physicians regarding the merits of
hospitalists. Advocates would point out the increases in efficiency and quality that have
occurred, and note that patients admitted to the hospital are sicker now than ever before.
This increase in inpatient acuity requires quick response to changes in a patient’s
condition that can only be met by an in-house physician (Schroeder & Schapiro, 1999;
Sox, 1999). Hospital leaders and government-based payers demand that in-house
physicians are available to quickly deal with patient issues in order to meet quality
metrics, improve patient safety, and satisfy patients. Another positive is that PCPs can
improve office productivity because they no longer have to leave work to follow patients
who are hospitalized (Wachter & Goldman, 1996).
Fundamental changes in the reimbursement system must be coupled with use of
electronic solutions. There must be team-based care models that cohesively and
efficiently care for patients as PCPs lack the time to provide all evidenced-based
preventive and chronic care services to their patients. The current primary care
workforce is grossly insufficient to care for the entire population (Bodenheimer, 2006).
Critics feel that patient care is compromised during patient handoffs and that the lack of

16
communication between hospitalists and PCPs leads to information loss compromising
the continuity of care to the patient (Schroeder & Schapiro, 1999; Flanders & Wachter,
2003). The thesis is that patients should be followed by hospitalists during their inpatient
stays so that the PCP can focus on providing the best possible care for their patients in the
ambulatory setting (Bodenheimer, 2006).
A study of hospitalized patients’ knowledge, preferences, and satisfaction level
with their PCP’s involvement in their inpatient care found that 87% of those studied had
a PCP and 33% had some contact with their PCP during their hospitalization. Most
patients (61%) knew that communication between the hospitalist and PCP had occurred,
and 50% believe that when a serious diagnosis or medical care choices were to be
discussed, they should be between the patient and the PCP (Hruby, Pantilat, & Lo, 2001).
At the same time, even though patients still prefer to seek initial care from a PCP rather
than a specialist, their unhappiness with their primary care experience is growing
(Bodenheimer, 2006).
Patients had favorable views of a system of inpatient care that included
considerable contact among inpatients, their PCPs, and hospitalists. They agreed with the
basic premises of the hospitalist system that hospitalists are more available to inpatients
and are more experienced in managing inpatient conditions than their PCPs. However,
patients also felt that PCPs and hospitalists needed to communicate with each other for
optimal care to be delivered. Some patients do not feel comfortable having their hospital
care managed by a physician with whom they do not have a prior relationship (Sox,
1999). Patients have a higher trust level with the doctor that they have known the longest
17
(their PCP) and definitely want their PCP involved when serious, complicated medical
decisions are discussed (Hruby, Pantilat, & Lo, 2001).
Organizations who develop hospitalist programs should take steps to mitigate
potential adverse effects of discontinuity of care that occurs between patients and their
PCPs. Even though the division of labor between PCPs and hospitalists is more efficient,
discontinuities between inpatient and outpatient care are likely to increase, and healthcare
organizations and physicians need to anticipate how this discontinuity influences the
patient-provider relationship. They can then ensure that steps are taken to maintain
appropriate continuity of care. To maintain patient and physician satisfaction levels,
organizations need to anticipate when it is desirable to involve the PCP in inpatient care
and construct systems to ensure such involvement (Hruby, Pantilat, & Lo, 2001).
Communication Effectiveness
Patients admitted to general medicine inpatient services are increasingly cared for
by hospitalists rather than their PCPs (Bell et al., 2009). A study addressing the issue of
attitudes regarding the communication that takes place between hospitalists and PCPs,
focusing on deficits in communication and information transfer between the two
physician groups, found that there are clear implications for patient safety and continuity
of care based on delayed or inaccurate communication between hospitalists and PCPs at
the time of hospital discharge which may adversely affect patient care. PCPs prefer to
communicate with hospitalist by phone at admission time (73%) or discharge time (78%),
and only 33% of PCPs reported that discharge summaries always or usually arrive before
the patient is seen in follow-up visits (Pantilat et al., 2001).
18
Communication between hospitalists and PCPs often occurs through the use of
discharge summaries. Discharge summaries may not provide important information
regarding primary diagnosis, abnormal results of tests, detail of the hospitalization,
follow-up instructions to the patient / family, or indications when test results are still
pending. There is also the issue of delays in receiving discharge summaries prior to the
patients’ next visit with their PCP. One study found this time delay occurs in about 75%
of the cases and restricts the PCPs ability to provide adequate follow-up care in 24% of
post-hospital visits. Another study found that PCPs are unaware of pending test results
that came in after the patient was discharged in 62% of the cases and of those 32% were
results that required further action on the part of the PCP (Kripalani et al., 2007). This is
the same type of information that many studies have found to be missing from the
communication between PCPs and hospitalists.
Deficits in communication and information transfer at hospital discharge are
common and may adversely affect patient care. PCPs generally rated main diagnosis,
pertinent physical findings, results of procedures and laboratory tests, discharge
medications with reasons for any changes to the previous medication regimen, details of
follow-up arrangements made, information given to the patient and family, test results
pending at discharge, and specific follow-up needs as most important for providing
adequate follow-up care (Kripalani et al., 2007). A study conducted to determine if
hospital discharge summaries sent to follow-up physicians after hospitalization helped
reduce the risk of hospital readmission revealed that only 12.2% of those patients in the
study group had discharge summaries available (568 of 4,639), and 27% (240) patients
were urgently readmitted to the hospital. There was also a trend toward a decreased risk
19
of readmission for patients who were seen in follow-up by a physician who had received
a discharge summary and concluded that the risk of re-hospitalization may decrease when
patients are assessed following discharge by physicians who have received the discharge
summary; however, further research is required to determine if better continuity of
patient information improves patient outcomes (Walraven et al., 2002).
Urgent improvements are needed in the processes and formats used for
transferring information to PCPs at hospital discharge. Interventions such as computer-
generated summaries and standardized formats may facilitate more timely transfer of
pertinent patient information to PCPs and make discharge summaries more consistently
available during follow-up care (Kripalani et al., 2007). Another methodology to
overcome problems with communication is the ‘continuity visit’ by PCPs. The intent is to
help overcome the discontinuity in care created between the outpatient and inpatient
setting. Major concerns related to a drop-off of information as patients move from the
office to the hospital, then back again, and about patient dissatisfaction when being cared
for by a separate inpatient provider from their usual PCP exist. There is a clear need for
hospitalists to initiate communication with patients’ PCPs (Hinami et al., 2009; Arora et
al., 2009; Calkins et al., 1997) and to encourage, even embrace, the PCPs who are willing
to make a continuity visit on their patients who are being followed in the hospital by the
hospitalist (Wachter & Pantilat, 2002).
Continuity visits would include a brief discussion with the patient regarding their
care, a focused physical exam and a review of the hospital course of care being provided
by the hospitalist, and ideally a brief face-to-face discussion with the hospitalist. The
entire visit should only take 30 minutes and would help alleviate the patient’s feeling of
20
abandonment, facilitate exchange of clinical and non-clinical insights between
physicians, facilitate the patients’ transition after their hospital stay, and allow the PCP to
better maintain a collegial relationship with their hospital counterparts. This would
require establishment of reimbursement for a single low-complexity hospital visit for
PCPs to visits their patients approximately once every three days of hospitalization.
Short of that, a telephone call process, or better yet, a video communication between the
primary physician, the patient, and then the hospitalist could be developed with current
technology. The establishment of continuity visits could help reduce the potential
liabilities of the current hospitalist model and enhance the outcomes for patients and the
overall healthcare delivery system (Wachter & Pantilat, 2002).
A study on communication between hospital-based physicians and PCPs looked at
patients admitted to six U.S. academic centers over a two year period with 77% of PCPs
responding that they were aware that their patient was admitted to the hospital and that
discharge summaries were available within two weeks of discharge 42% of the time. The
study revealed that 22% of patients had died, were readmitted to the hospital, or visited
an ED within 30 days of discharge. Direct communication between the hospitalist and
PCP only occurred 23% of the time, leading to the conclusion that communication
between PCPs and hospitalists left much room for improvement (Bell et al., 2009).
Computer-generated discharge summaries, standardized report formats, and
patients serving as couriers has helped facilitate more timely transfer of information back
to the PCP, making discharge summaries more consistently available for follow-up care
(Pantilat et al., 2001). PCPs prefer telephone communication, at admission and
discharge, containing specific information regarding their patients’ hospitalization. Only
21
half of PCPs studied were satisfied with their communication with hospitalists. Few
visited their hospitalized patients, and even fewer telephoned their hospitalized patients.
Increased PCP-patient contact and improved PCP-hospitalist communication may
mitigate the potential harm of discontinuity of care (Pantilat et al., 2001).
There is considerable evidence regarding the importance of communication when
patients leave the hospital. Results of surveys conducted on patients and their attending
physicians who had recently been discharged from the hospital after having pneumonia or
acute myocardial infarction show that the quality of discharge planning is an important
determinant of patient outcomes following hospital discharge and that many times
patients do not have a clear understanding of the major elements of the post-discharge
treatment plan, including medications and daily activities. Eighty-nine percent of
physicians believed that their patients understood the post-discharge instructions
regarding medication side effects, while only 57% of patients responded that they
understood those instructions. Ninety-five percent of physicians believed that their
patients understood when they could resume normal daily activities, while only 58% of
patients responded that they understood those instructions (Calkins et al., 1997).
Studies demonstrate the critical nature of the communication process at discharge
and researchers conclude that steps should be taken to improve communication about
post-discharge treatment. Incomplete handoffs during service changes are associated
with potential harm to patients. Systems are not fully developed around these handoffs,
and physicians overestimate patients’ understanding of the post-discharge treatment plan
(Arora et al., 2009; Bell et al., 2009; Calkins et al., 1997; Hinami et al., 2009).
22
In order to expand on the current hospitalist model and make it more clinically
diverse and dynamic, all stakeholders must develop an economic model that accounts for
the value that the hospitalist brings. The more quantifiable these programs become, the
easier it will be to prove their value and implement them in capital-strapped facilities.
The hospitalist model must address relationship management to include communication
between hospitalists, medical staffs, and management, as well as educating the
community as to the benefits of hospitalists in the overall delivery of patient care (Bernd,
2009).
It would appear that the hospitalist model of care is here to stay based on the
growing evidence of its benefits to patients, hospitals, and physicians (Wachter &
Pantilat, 2002). Further research is needed to assess the impact of communication on
patient satisfaction and outcomes (Pantilat et al., 2001). The transition from hospital to
home is a vulnerable period of discontinuity and potential adverse events. Hospitalists
and other inpatient providers should not view discharge as an end to their obligation to
the patients but rather should attempt to promote a safe and efficient transition of care.
Hospitalists can play an important role in bridging the gap between inpatient and
outpatient care through appropriate discharge planning and effective communication with
patients, their family members, and their PCPs (Kripalani et al., 2007).
Productivity and Efficiency
The question that remains is how effective the field of hospital medicine has been
in addressing the cost and quality of care for hospitalized patients. It seems certain that
the hospitalist movement has achieved some of its promise. Care by hospitalists is
23
associated with shorter LOS and reduced costs. However, there is not clear evidence as
to whether hospitalist-based care results in either adverse or favorable effects on
mortality or readmission rates. There are also several potentially negative aspects of
hospitalist care, such as disruption of continuity of care provided by the PCP, the
lessening of career satisfaction and professional collegiality among PCPs, and an overall
reduction in the number of medical students choosing to go into primary care medicine
today. A possible solution is deployment of proactive strategies to enhance
communication between hospitalists and PCPs and to efficiently transmit discharge
summaries and updated medication lists to promote better patient care (Hamel, Drazen, &
Epstein, 2009).
The most vulnerable period of time for patients is the transition between the care
of the hospitalist and the PCP. Approximately half of adults experience a medical error
after hospital discharge, and 19%-23% suffer an adverse event, most commonly an
adverse drug event. Patient discharges require a transition from the hospital to the home
and a transfer of responsibility from the hospitalist back to the primary physician. This
highlights the inpatient-outpatient physician discontinuity that has developed with the
advent of the hospitalist model in this country (Kripalani et al., 2007).
Cost shifts between providers and settings occur when hospitalists care for older
inpatients. Amongst the Medicare population, hospital LOS decreases 0.64 days and
charges are $282 lower for patients cared for by hospitalists. Medicare costs 30 days
after discharge are $332 higher for patients cared for by hospitalists. Patients are also less
likely to be discharged to home by hospitalists and more likely to have ED visits or
readmissions after discharge than those cared for in the hospital by their PCP. Patients
24
cared for by hospitalists have fewer visits with their PCP and more nursing home visits
than those cared for in the hospital by their PCP, leading to the conclusion that decreased
LOS and hospital costs associated with hospitalist care are offset by higher medical
utilization and costs after discharge (Kuo & Goodwin, 2011).
Patient Outcomes and Clinical Quality
Hospitalists improve patient efficiency without harmful effects on quality or
patient satisfaction. Hospitalist programs are associated with significant reductions in
resource use, usually measured as hospital costs (average decrease, 13.4%) or average
LOS (average decrease, 16.6) (Wachter & Goldman, 1996). On a severity and age /
gender adjusted scale, mean charges of $5,680 by the PCPs are significantly lower than
that of the critical care hospitalists at $10,231, and for that of the family physician
hospitalists at $7,699. Mean LOS for critical care hospitalist patients was 3.8 days,
compared to 3.9 days for family physician hospitalist patients, and 2.6 days for PCP
patients. Critical care hospitalists are more likely to request additional chest x-rays and
their patients are more likely to have lengthy stays in the intensive care unit.
Better and less costly care by hospitalists requires further investigation. Some
argue that the use of hospitalists should not be mandated, and that the use of FPs as
hospitalists should be considered a good alternative to the use of subspecialists. These
conclusions are drawn from a single, private, urban community hospital. Patients with
nosocomial infections, human immunodeficiency virus (HIV), and acquired
immunodeficiency syndrome were excluded from the study (Smith, Westfall, &
25
Nicholas, 2002). Other studies also failed to find a relationship between aspects of
communication and adverse clinical outcomes (Bell et al., 2009).
Exchange Theory
Social exchange theory developed from the convergence of economics,
psychology, and sociology. Homans (1958) is credited with being the father of social
exchange theory and believed that individuals create and maintain social structures,
taking into account the given conditions that influence individual behavior: their stimuli,
rewards, and punishments. Homans explained social behavior as the interaction between
individuals and their actions to reward or punish the other party. He believed that in an
exchange relationship, an individual expects to receive as much reward as they give to
the other party.
Homans’ work had a profound influence on the thinking of major sociologists
such as Peter Blau, John Thibaut, and Harold Kelly. It expands on the social exchange
theory, moving beyond the micro-level to the institutional level as institutionalized
systems of exchange. Blau’s theory on the social nature of exchange differs from
Homans’ work in several important ways. His framework is not based on behavior
psychology but on the micro-economic reasoning of social exchange, which theorizes
that social activity gives rise to different forms of association and therefore takes on
different organizational forms. His interest lies in how the structure of the organization is
sustained by those engaging in exchanges between peer (equality) and still allows for
differentiation of status (hierarchy) based on whether the benefits received during an
exchange are reciprocated or not. Blau believes that human behavior attempts to
26
exchange both symbolic and non-symbolic rewards and that individuals will continue to
participate in the exchange as long as they perceive they derive equal benefit from their
participation (Blau, 1964).
Thibaut and Kelly (1959) focus their work around the communication theory for
social exchange. They write that people strive to minimize cost and maximize rewards
and base the likelihood of developing a relationship with someone on the perceived
outcomes of the exchange. The greater the outcome, the more an individual will disclose
to the other party and the closer the relationship will be with that person. Thibaut and
Kelly also suggest that there are two standards by which we evaluate the outcome we
receive from an exchange. First is the level of satisfaction we receive – how happy or sad
the interpersonal outcome makes a participant feel. The second is how the outcome pays
off in comparison to any other alternatives available. They developed a system to
quantify and calculate the advantages and disadvantages of the social exchange
concluding that individuals will choose to leave a relationship and enter into a new one if
the perceived rewards of the current relationship are less than the perceived rewards of
the new relationship.
Why would a PCP establish a relationship with a hospitalist or hospitalist group?
One could speculate that the PCP wants to assure that their patients receive excellent care
while they are hospitalized and that because they can no longer afford to follow these
patients while in the hospital, they develop strong ties with a physician that they trust to
assume this important role. Once this relationship is developed, repeated interactions
between the hospitalist and the PCP foster a comfort level leading to more patient
referrals.
27
The physician’s decision-making role in the allocation of medical resources is
well recognized. An important part of this role is one physician’s decision to refer a
patient to another physician for care. The central thesis behind exchange theory is that an
individual is motivated to interact with another in an activity if they expect associating
with them will result in a positive outcome. The more rewarding the behavior of the
interaction between the parties is, the more likely they are to participate actively to
cultivate the relationship. If the outcome exceeds the individuals’ relevant comparison
levels, the relationship will be highly valued and similar behavior may be expected from
each in the future. Rewards are positive reinforcements that meet either the intrinsic or
extrinsic needs of the participating parties. Costs refer to any negative reinforcement
including unfulfilled expectations, fatigue or anxiety from engaging in the behavior, and
the value of rewards foregone by engaging in a particular activity rather than others (the
opportunity cost).
From a theoretical framework perspective, this study will focus on the work
conducted by Shortell’s (1974) exchange theory approach to physician relationships. In
this model, the exchange occurs to maximize benefits and minimize costs between the
parties involved in the interaction. The theory holds that people will weigh the benefits
and risk of relationships and when the risks outweigh the rewards, the relationship will be
terminated or abandoned by the parties. Shortell describes comparison levels as the
degree to which the outcome of a particular interaction satisfies the individual in relation
to his / her expectations, the outcomes received by others similar to him/her, and the
alternative choices available. There are clearly rewards and costs for both the referring
and consulting physicians which determine the outcomes they receive from engaging in
28
referral activity. With physician to physician interactions, the referral process is viewed
in terms of the physician’s perceptions of the variables that affect his / her decisions, the
consequences in terms of their position within the professional medical community, and
the benefits they will gain from the referral. These could include emotional comfort
related to the care of their patients, development of referrals to their practice, satisfied
patients, and cost benefits based on avoiding the loss of time, money, and lost referrals.
In the case of the PCP’s interaction with the hospitalist, the PCP would be looking
for his / her referral to the hospitalist for inpatient care to result in improved patient
outcomes. Rewards could include higher quality care for the PCP’s patients, prompt and
clear communication from the hospitalist back to the PCP, and the possibility that the
hospitalist relationship could generate new referrals back to the PCP’s practice. The PCP
who refers their inpatients to the hospitalist would also have the ability to see more
patients in their office, spend more time with their patients, and increase their practice
revenues through efficient use of their time. For the consultant, the hospitalist in this
case, the primary reward is receiving referrals. Negatives could include the costs of
improper work-up of patients, poor communication back to the PCP about the patient’s
condition or status, patient dissatisfaction with being referred to another physician, and
poor follow-up care for the patient. The PCP’s decision whether to treat the patient,
refer the patient to another physician, refer the patient to a health agency, or admit the
patient to the hospital has system, as well as individual, implications in terms of the cost,
quality, and utilization of medical services (Shortell, 1974; Blau, 1964; Homans, 1958;
Homans, 1961; Thibaut and Kelly, 1959).
29
Another key factor in the PCP-hospitalist relationship is the status of the PCP.
Studies have shown that board certified internists receive fewer referrals than non-
certified internists, suggesting that this may be due to differences in the fee structure.
Also general internists in solo practice refer fewer patients to other physicians than
internists in group practice settings suggesting that solo practitioners are concerned that
they may lose patients that are referred out or that they have more difficulty with the
referral process itself. Due to the continuing specialization of medical practice and the
increasing economic pressures on PCPs and hospitals, referral relationships are likely to
continue to increase in the new healthcare environment. These referral relationships must
provide outcomes and rewards that exceed the individuals’ relevant comparison levels of
any alternative choices the PCP could make (Shortell, 1974).
Further study is clearly needed regarding physician referral behavior, particularly
as it relates to PCP to hospitalist handoffs that will likely increase in the proposed
healthcare delivery models currently under consideration. Shortell (1974) did not look at
the hospitalist model of care because it did not exist to any extent until the 1990s.
Research should also be conducted to determine support for an exchange theory
explanation for the number of referrals PCPs make to hospitalists. Healthcare leaders
need clear evidence about the delivery of medical care that results from the PCP-
hospitalist relationship. This study attempts to show that patient outcomes are
significantly enhanced when FPs have established a relationship with a hospitalist or
hospitalist group and refer patients needing inpatient care based on this relationship. It
also attempts to provide the reader with insight into the effectiveness of the
communication that takes place between FPs and hospitalists and whether FPs feel that
30
the information provided to them regarding their patients’ hospitalization is sufficient for
them to provide high quality follow-up care.
Literature Summary
It is clear from the literature that hospital medicine has become an integral part of
healthcare delivery in the U.S. Hospitalists are still the fastest growing field in medicine
and current discussions around healthcare reform should only strengthen the need for
physicians who only focus on the patient during hospitalization. PCPs will also be in
great demand as the medical “home” model of care gains popularity and healthcare
coverage for all Americans becomes a reality. The level of satisfaction related to the
hospitalist model of care is somewhat mixed. Given a choice, PCPs and their patients
would prefer that the hospitalist not be injected into the middle of the long-standing
relationship between physician and patients. The economic structure of healthcare today
dictates that the PCP focuses their attention on their office practice and allows the
hospitalist to care for the hospitalized patient. As hospitalists become more prevalent and
patients become comfortable with the PCP-hospitalist relationship, the satisfaction levels
of all stakeholders should continue to improve.
The foremost area of concern regarding the PCP-hospitalist relationship is
focused on communication. The literature clearly demonstrates that communication
between PCPs and hospitalists leaves much room for improvement, that improved PCP-
hospitalist communication could mitigate the potential harm of discontinuity of care, and
that the critical nature of the communication process at discharge calls for improved
communication about post-discharge treatment. Growth in the number of hospitalists is

31
attributed to economic, efficiency, and quality pressures. There are several potentially
negative aspects of hospitalist care such as disruption of continuity of care provided by
the PCP and the added pressure to discharge patients as quickly and efficiently as
possible. Many feel that the use of hospitalists should not be mandated, that the use of
FPs as hospitalists should be considered a good alternative, and that patient outcomes and
clinical quality have not been empirically demonstrated to date. Further investigation is
required to demonstrate that better and less costly care is delivered through the hospitalist
model of care.
32
CHAPTER 3
RESEARCH METHODOLOGY AND THEORETICAL FRAMEWORK
Purpose of This Study
The purpose of this study was to determine the impact on patient outcomes (LOS,
hospital costs, and readmission rates) for FPs who had an established relationship with a
hospitalist or hospitalist group versus FPs who did not have such a relationship. The
study also attempted to assess the level of communication that FPs felt they had with
hospitalists. FPs represent a significant number of the PCPs practicing in the United
States. For this reason, FPs were chosen as the best group to reflect the outcomes and
communications that occur between hospitalists and PCPs. Based on the survey tool
utilized in this study, the quality of communication between the hospitalists and FPs are
addressed only from the qualitative perspective because respondents who have no
relationship with a hospitalist were not required to answer the questions related to
communication resulting in a sample size too small for statistical analysis.
Research Question
Do FPs who have an ongoing relationship with a hospitalist or hospitalist group
(six months or greater) have significantly different patient outcomes than FPs who have
no established relationship with a hospitalist?
33
Hypotheses
Because hospitalists have become an integral part of the care delivery system, it is
important to measure their overall effect on the quality of care delivered during the
patient’s hospital stay. It is logical to assume that a physician who only takes care of
patients during their hospitalization provides continuity of care that may result in better
patient outcomes. Measures such as LOS and the cost of care should be lower than when
a patient is cared for by the FP or through the emergency room. Due to the pressure
placed on cost and LOS by insurance companies and hospitals, one could easily presume
that patients who are provided care by hospital-based physicians would have lower
overall costs and LOS. At the same time, readmission rates may be higher because
hospitalists want the patient discharged quickly and are not worried about readmissions,
which are monitored for the FP and not the hospitalist.
It is obvious that communication between hospitalists and FPs is critical to the
delivery of high quality, cost-effective patient care. The question is whether an FP’s
established relationship with a hospitalist has any significant effect on key patient
outcome metrics. The current literature provides little evidence regarding the effect on
overall quality of care to the patient. It is difficult to look at measures such as patient
satisfaction, mortality rates, and infection rates because there is currently no standardized
method of measurement for these indicators. Insurance companies do have information
regarding readmission rates, cost, and LOS. Based on these measures, the impact of
having an established relationship with a hospitalist or hospitalist group on FP’s patient
outcomes was assessed by testing the following hypotheses.
34
H1. The mean cost of care for patients of FPs who have an established relationship
with a hospitalist will be lower than the mean cost of care for patients of FPs with
no hospitalist relationship.
H2. The mean LOS for patients of FPs who have an established relationship with a
hospitalist will be lower than the mean LOS for patients of FPs with no hospitalist
relationship.
H3. The readmission rate for patients of FPs who have an established relationship with
a hospitalist will be higher than the readmission rate for patients of FPs with no
hospitalist relationship.
Data Collection
The data collection was performed in two stages. First, demographic information
such as the physician’s year of graduation, practice locale, and group make-up (solo or
number of physicians in the practice), was collected and recorded through Survey
Monkey. Survey Monkey is an internet-based service that allows surveys to be created,
distributed, and completed from a personal computer without involving paper-based
forms and mail service. The survey instrument was sent to members of the FAFP, which
is comprised of approximately 3,000 FPs from across the state of Florida. The FAFP is a
component society of the American Academy of Family Practice (AAFP) and its goals
are to promote and maintain high quality standards amongst their members, provide
advocacy, representation, continuing education, and leadership to family practice
physicians, to promote respect, skill, and teamwork within the field of family medicine,
and to preserve and promote quality, cost-effective healthcare for all Floridians. In
35
addition, the FAFP is the voice for family practice medicine in the medical community,
with healthcare insurers, legislators and regulators, and to the public at-large. The survey
asked respondents to provide their national provider identifier (NPI), but only for
purposes of matching the provider to the BCBSF patient database that was used to
analyze the differences in patient outcomes between the two groupings.
FAFP staff sent out the survey instrument to their membership electronically
through the use of Survey Monkey. The survey instrument was open for response for
approximately 10 weeks to allow for maximum participation. FAFP sent three
compressed folders that contained the FAFP survey results to BCBSF staff. Survey data
was captured and recorded through online survey techniques and the aggregate report
contained no individual identifiers.
The final report creation process removed ten columns; each containing a variable
collected by the survey, and then added back seven columns. Columns representing
collector id, start date, end date, IP address, email address, first name, last name, custom
data, NPI, and BCBSF number were removed by BCBSF staff to protect the
confidentiality of the participants. Columns representing readmission percentage,
inpatient LOS, inpatient average charge, all-claims LOS, all claims average charge,
outpatient LOS, and outpatient average charge were then added. The BCBSF claims
information was inserted at the end of the survey results and the respondent identity
columns were deleted from the final report sent to the researcher for analysis. The survey
results were recorded in Excel and the final report had 34 variables stored in separate
columns and 224 rows, each corresponding to a separate survey responder.
36
The process kept the identity of the respondents confidential and protected the
survey information from any form of adulteration, compression or deletion. The
respondent’s NPI or BCBSF provider number was used by BCBSF staff to capture each
respondent’s BCBSF claim history. Some rows were missing NPIs and some rows were
missing BCBSF numbers. If a row in the results had insufficient provider identification,
the row did not have claims information in the final report. If a survey respondent had
valid provider identification, but did not have any BCBSF claims, the final report did not
have any claims information for that survey respondent. BCBSF staff used a ten step
process to clean and protect the data.
Step 1 – To preserve the survey results integrity, the columns ‘respondentID,’ ‘NPI,’ and
‘BCBSF number’ were copied into a new tab and a “rownum” column was added that
numerically represented each row in the survey results. The ‘respondentID’ and
‘rownum’ columns guaranteed that the claims information was added to the correct row
in the survey results. The ‘rownum’ column was not seen in the final report.
Step 2 – The ‘NPI’ and ‘BCBSF number’ values from the new tab were then compared to
a BCBSF table that contained the NPI and BCBSF number for all providers known to
BCBSF. The first reading of the survey ID numbers by BCBSF staff revealed that
several numbers had missing values, added values, transposed numbers or added
characters. BCBSF staff reviewed each of the unmatched survey result identification
numbers and corrected the discrepancies in the new tab until they were 100% confident
that they had the valid identification numbers for that survey result row. Survey result
37
rows that did not have identification numbers did not have claims information in the final
report.
Step 3 – Based on the NPI values, eight of the survey respondents answered the survey
twice. It is possible for providers to share NPIs yet have different BCBSF numbers. If a
survey result ID number was duplicated, and the BCBSF provider number was the same
or could not be determined, then the final report added the claims information to the last
response of the provider. There were 164 rows in the survey results with NPI values and
59 rows without. Survey result rows without an NPI (i.e. those that are the first NPI in a
duplicate response or are valid NPIs without claims in the BCBSF claims system) had no
values in the claims analysis columns of the final report.
Step 4 – BCBSF staff then gathered all inpatient, outpatient, and professional service
claims submitted by the Step 2 and Step 3 NPIs from January 1, 2011 up to and including
the date of the execution of the program. These claims were used to create the ‘all’
column values. Some individual providers share NPIs with an institution and only bill
BCBSF through their parent institution.
Step 5 – Inpatient services are submitted to BCBSF from facilities on UB-04(CMS-1450)
claim forms. The survey respondents were providers who submit claims on different
forms (ex: CMS 1500). To measure readmissions and LOS, BCBSF gathered inpatient
claims for the members associated to the providers’ claims found in Step 4. Readmission,
charge and LOS values were the inpatient readmission and inpatient LOS values of the
38
members identified on the claims found in Step 4.
Step 6 – The readmission (within 28 days of discharge), charge and LOS values were for
claims for the Step 2 and Step 3 provider ID numbers.
Step 7 – The survey results were best defined by NPI. The BCBSF claims are best
defined by BCBSF number. To protect the survey results from any change, BCBSF staff
associated each survey NPI to a BCBSF number in the claim calculation information and
then associated the claims calculations information to the appropriate survey result NPI,
respondentID and rownum.
Step 8 – BCBSF staff inserted the claims information into new columns at the end of the
rows of the tab created in Step 1. Staff then insured that 100% of the claims information
lined up by row then wrote the claims information into new columns at the end of the
FAFP survey results used to build the Step 1 information.
Step 9 – BCBSF staff then removed the collector ID, start date, end date, IP address,
email address, first name, last name, custom data, NPI, and BCBSF number columns.
They formatted the column headers into easy to read cell sizes by changing the word
wrapping and cell width for the first row.
Step 10 – BCBSF staff then copied the tab from Step 9 into the definitions and layout
spreadsheet created by the researcher, renamed the Step 9 tab as ‘final report’ and
39
emailed the spreadsheet back to the researcher to conduct data analysis based on the
research questions and hypotheses.
The primary question in the study was “do you currently have an established
relationship with a hospitalist or hospitalist group?” The secondary question was “how
long have you had this established relationship?” Additional questions were related to
physicians’ year of graduation, practice location, and group make-up. The definition of
an established relationship was clearly defined for the respondent in order to remove any
ambiguity to the extent possible. The physicians who responded ‘yes’ to the established
relationship question were placed in the first study group (group 1) and compared with
the physicians who responded ‘no’ (group 2). A response rate of up to 10% was sought,
which would have provided approximately 300 physicians from across the state for use in
the study. Once collected, the data was exported to Microsoft Excel 2010 for use by
BCBSF personnel.
Next, the BCBSF managed care database was used to match the physician’s
provider number to his / her patient outcomes tracked by BCBSF. The outcomes of
interest were: average LOS during hospitalization, average claims payments associated
with the hospitalization and average hospital readmission rates (28 day readmission to
hospital).
Statistical Analysis
Descriptive statistics of demographic data are presented to characterize the
physicians and their family practice. The physicians were categorized based on the year
of graduation. The family practices were described based on their location (urban,
suburban or rural) and group make-up (solo or the number of physicians in the practice).
40
The demographic characteristics of survey responders were presented by multiple
groupings including those who had established hospitalist relationships vs. those without
vs. those who did not answer the question, as well as complete survey responders vs.
incomplete survey responders. Categorical variables were presented as counts and
percentages. Characteristics of those who had established relationships were compared to
those without established relationships using the chi-square test of association. Fisher’s
exact test was alternatively performed if the expected number of counts was less than 5,
as the chi-square test was invalid in this case.
Primary outcome information regarding hospital claims payments for FP’s
admitted patients, LOS, and readmission rate data was collected as continuous variables.
All approximately normally distributed variables (p>.05 in Shapiro-Wilk’s test) were
described using mean and standard deviation, and then compared between those with
established hospitalist relationships and those without using two Sample Independent T-
tests. If the continuous variables were not normally distributed, they were described
using medians (minimum, maximum) and compared using the non-parametric Wilcoxon
Rank Sum tests. Evaluations of these outcomes were performed as two-sided tests at the
0.05 level of significance. Two-sided tests of significance were performed to allow for
the possibility of significant differences of study outcomes in directions opposite of those
hypothesized.
Analysis of covariance (ANCOVA) models were developed to determine the
relationship between each of the outcomes, LOS, readmission rate and charges, and
hospitalist relationship, while accounting for year of graduation, practice locale, type of
practice and employment status. The Tukey adjustment was used for multiple

41
comparisons. Estimates of the means for each study outcome from the ANCOVA models
are presented. All data management and statistical analysis was done using SPSS 20.0®
(Chicago, IL).
42
CHAPTER 4
RESULTS AND FINDINGS
This chapter explains the results of the survey analysis and addresses the key
research questions and hypotheses outlined for this study in chapter three. The first
section provides the descriptive statistics of the study participants, including demographic
information outlined in narrative and graphic formats. The responses received from FPs
belonging to the FAFP are described and the process of determining the final study group
is discussed. The responding physicians are categorized based on the year of graduation,
the location of their practice (urban, suburban, or rural) and the type of setting in which
they practice (group, solo, multispecialty, other). The demographic data is then analyzed
using descriptive statistics to characterize the practice of each FP. Information regarding
hospital costs for FPs admitted patients, their LOS, and their 28 day readmission rate data
is analyzed to investigate whether having an established relationship with a hospitalist or
hospitalist group has any effect on these measures.
Respondents were placed into two groups based on answering ‘yes’ or ‘no’ to the
question “do you have an established relationship with a hospitalist or hospitalist group
that has been in place for at least six months?” The question also specified that the
established relationship meant that the FP routinely referred patients to a particular
hospitalist for hospitalization.
43
Data Description
Survey Respondents
The data collection for this study was collected in two stages. First, a survey
instrument was sent electronically using ‘Survey Monkey’ to all members of the FAFP.
The survey was sent out by the FAFP office to maintain respondent confidentiality.
Members had six weeks to complete the survey instrument with all responses going to
FAFP administrative staff. The total number of physician responses was 223. The
majority of respondents (61%) graduated between 1980 and 1999; 77 (34.5%) graduated
between 1980 and 1989; 59 (26.5%) graduated between 1990 and 1999; and 9 (4.0%)
graduated before 1970. Most had their practice in a suburban (52.5%) or urban (35.0%)
location. Full-time practice (89.2%) was the most prevalent. One hundred and six
(47.5%) were part of a group practice, 60 (26.9%) were solo practice and 22 (9.9%) were
part of a multi-specialty group. One hundred and forty-two (63.7%) had an established
relationship with a hospitalist and 70 (31.4%) did not. A detailed summary of their
demographics is presented in Table 1.
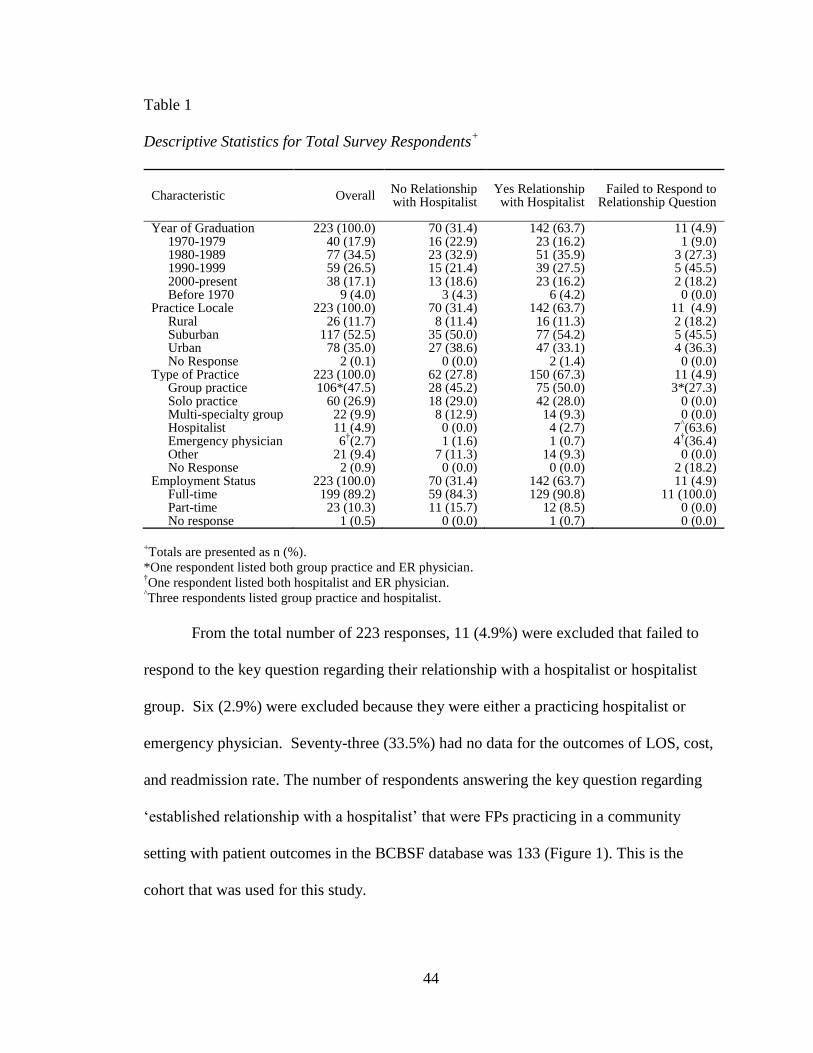
44
Table 1
Descriptive Statistics for Total Survey Respondents+
Characteristic Overall No Relationship with Hospitalist
Yes Relationship with Hospitalist
Failed to Respond to Relationship Question
Year of Graduation 223 (100.0) 70 (31.4) 142 (63.7) 11 (4.9) 1970-1979 40 (17.9) 16 (22.9) 23 (16.2) 1 (9.0) 1980-1989 77 (34.5) 23 (32.9) 51 (35.9) 3 (27.3) 1990-1999 59 (26.5) 15 (21.4) 39 (27.5) 5 (45.5) 2000-present Before 1970
38 (17.1) 9 (4.0)
13 (18.6) 3 (4.3)
23 (16.2) 6 (4.2)
2 (18.2) 0 (0.0)
Practice Locale 223 (100.0) 70 (31.4) 142 (63.7) 11 (4.9) Rural 26 (11.7) 8 (11.4) 16 (11.3) 2 (18.2) Suburban Urban No Response
117 (52.5) 78 (35.0)
2 (0.1)
35 (50.0) 27 (38.6)
0 (0.0)
77 (54.2) 47 (33.1)
2 (1.4)
5 (45.5) 4 (36.3) 0 (0.0)
Type of Practice 223 (100.0) 62 (27.8) 150 (67.3) 11 (4.9) Group practice 106*(47.5) 28 (45.2) 75 (50.0) 3*(27.3) Solo practice Multi-specialty group Hospitalist Emergency physician Other No Response
60 (26.9) 22 (9.9) 11 (4.9) 6
†(2.7)
21 (9.4) 2 (0.9)
18 (29.0) 8 (12.9)
0 (0.0) 1 (1.6)
7 (11.3) 0 (0.0)
42 (28.0) 14 (9.3) 4 (2.7) 1 (0.7) 14 (9.3) 0 (0.0)
0 (0.0) 0 (0.0)
7^(63.6)
4†(36.4)
0 (0.0) 2 (18.2)
Employment Status Full-time Part-time No response
223 (100.0) 199 (89.2) 23 (10.3) 1 (0.5)
70 (31.4) 59 (84.3) 11 (15.7)
0 (0.0)
142 (63.7) 129 (90.8)
12 (8.5) 1 (0.7)
11 (4.9) 11 (100.0)
0 (0.0) 0 (0.0)
+Totals are presented as n (%).
*One respondent listed both group practice and ER physician. †One respondent listed both hospitalist and ER physician.
^Three respondents listed group practice and hospitalist.
From the total number of 223 responses, 11 (4.9%) were excluded that failed to
respond to the key question regarding their relationship with a hospitalist or hospitalist
group. Six (2.9%) were excluded because they were either a practicing hospitalist or
emergency physician. Seventy-three (33.5%) had no data for the outcomes of LOS, cost,
and readmission rate. The number of respondents answering the key question regarding
‘established relationship with a hospitalist’ that were FPs practicing in a community
setting with patient outcomes in the BCBSF database was 133 (Figure 1). This is the
cohort that was used for this study.
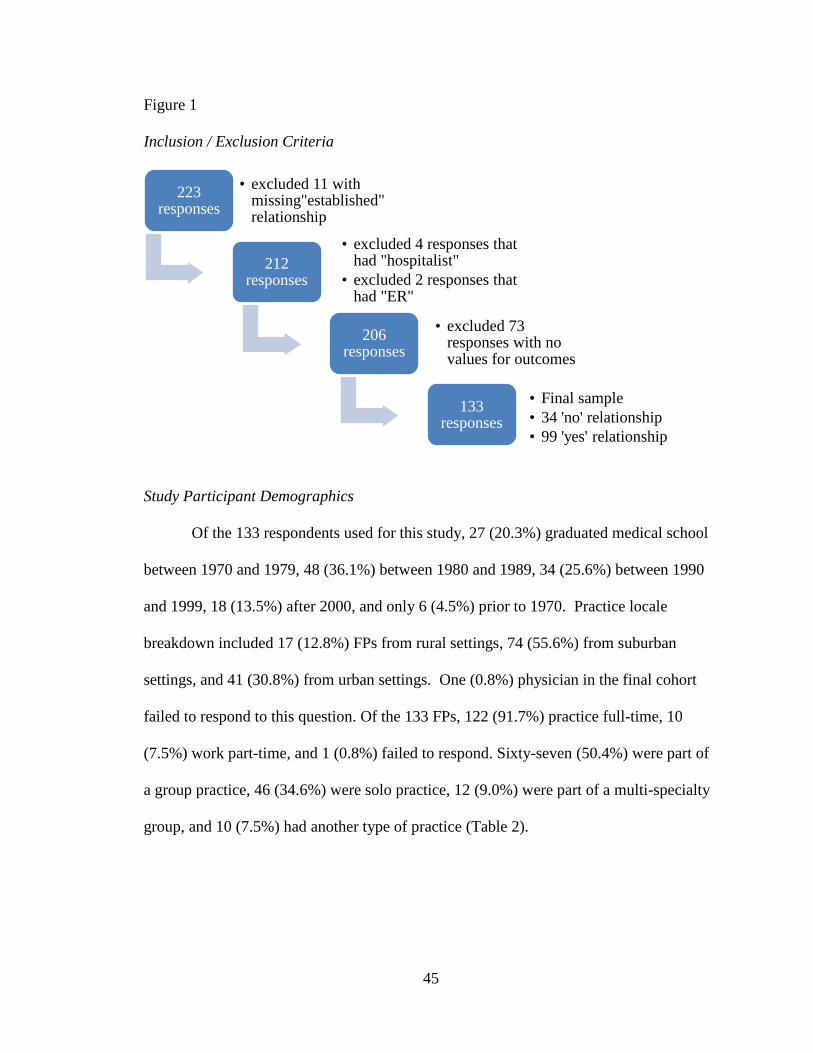
45
Figure 1
Inclusion / Exclusion Criteria
Study Participant Demographics
Of the 133 respondents used for this study, 27 (20.3%) graduated medical school
between 1970 and 1979, 48 (36.1%) between 1980 and 1989, 34 (25.6%) between 1990
and 1999, 18 (13.5%) after 2000, and only 6 (4.5%) prior to 1970. Practice locale
breakdown included 17 (12.8%) FPs from rural settings, 74 (55.6%) from suburban
settings, and 41 (30.8%) from urban settings. One (0.8%) physician in the final cohort
failed to respond to this question. Of the 133 FPs, 122 (91.7%) practice full-time, 10
(7.5%) work part-time, and 1 (0.8%) failed to respond. Sixty-seven (50.4%) were part of
a group practice, 46 (34.6%) were solo practice, 12 (9.0%) were part of a multi-specialty
group, and 10 (7.5%) had another type of practice (Table 2).
223 responses
• excluded 11 with missing"established" relationship
212 responses
• excluded 4 responses that had "hospitalist"
• excluded 2 responses that had "ER"
206 responses
• excluded 73 responses with no values for outcomes
133 responses
• Final sample
• 34 'no' relationship
• 99 'yes' relationship
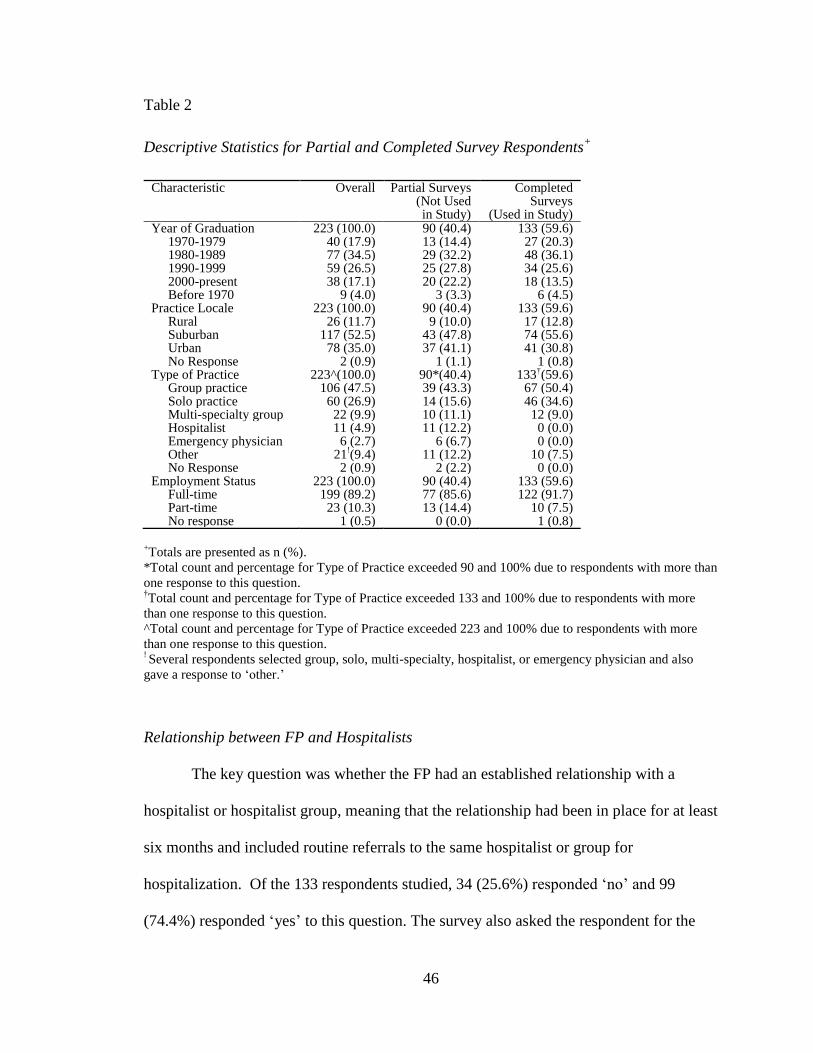
46
Table 2
Descriptive Statistics for Partial and Completed Survey Respondents+
Characteristic Overall Partial Surveys (Not Used in Study)
Completed Surveys
(Used in Study) Year of Graduation 223 (100.0) 90 (40.4) 133 (59.6) 1970-1979 40 (17.9) 13 (14.4) 27 (20.3) 1980-1989 77 (34.5) 29 (32.2) 48 (36.1) 1990-1999 59 (26.5) 25 (27.8) 34 (25.6) 2000-present Before 1970
38 (17.1) 9 (4.0)
20 (22.2) 3 (3.3)
18 (13.5) 6 (4.5)
Practice Locale 223 (100.0) 90 (40.4) 133 (59.6) Rural 26 (11.7) 9 (10.0) 17 (12.8) Suburban Urban No Response
117 (52.5) 78 (35.0)
2 (0.9)
43 (47.8) 37 (41.1) 1 (1.1)
74 (55.6) 41 (30.8)
1 (0.8) Type of Practice 223^(100.0) 90*(40.4) 133
†(59.6)
Group practice 106 (47.5) 39 (43.3) 67 (50.4) Solo practice Multi-specialty group Hospitalist Emergency physician Other No Response
60 (26.9) 22 (9.9) 11 (4.9) 6 (2.7) 21
!(9.4)
2 (0.9)
14 (15.6) 10 (11.1) 11 (12.2)
6 (6.7) 11 (12.2) 2 (2.2)
46 (34.6) 12 (9.0) 0 (0.0)
0 (0.0) 10 (7.5)
0 (0.0) Employment Status Full-time Part-time No response
223 (100.0) 199 (89.2) 23 (10.3) 1 (0.5)
90 (40.4) 77 (85.6) 13 (14.4) 0 (0.0)
133 (59.6) 122 (91.7) 10 (7.5)
1 (0.8)
+Totals are presented as n (%).
*Total count and percentage for Type of Practice exceeded 90 and 100% due to respondents with more than
one response to this question. †Total count and percentage for Type of Practice exceeded 133 and 100% due to respondents with more
than one response to this question.
^Total count and percentage for Type of Practice exceeded 223 and 100% due to respondents with more
than one response to this question. ! Several respondents selected group, solo, multi-specialty, hospitalist, or emergency physician and also
gave a response to ‘other.’
Relationship between FP and Hospitalists
The key question was whether the FP had an established relationship with a
hospitalist or hospitalist group, meaning that the relationship had been in place for at least
six months and included routine referrals to the same hospitalist or group for
hospitalization. Of the 133 respondents studied, 34 (25.6%) responded ‘no’ and 99
(74.4%) responded ‘yes’ to this question. The survey also asked the respondent for the
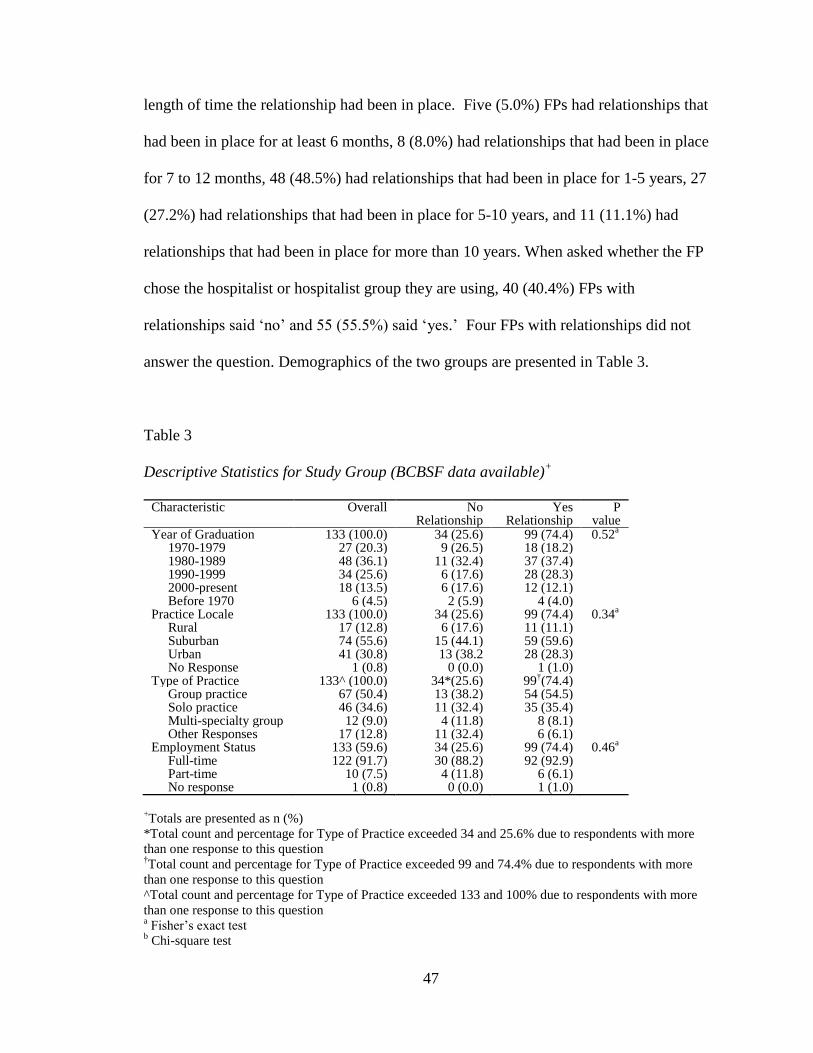
47
length of time the relationship had been in place. Five (5.0%) FPs had relationships that
had been in place for at least 6 months, 8 (8.0%) had relationships that had been in place
for 7 to 12 months, 48 (48.5%) had relationships that had been in place for 1-5 years, 27
(27.2%) had relationships that had been in place for 5-10 years, and 11 (11.1%) had
relationships that had been in place for more than 10 years. When asked whether the FP
chose the hospitalist or hospitalist group they are using, 40 (40.4%) FPs with
relationships said ‘no’ and 55 (55.5%) said ‘yes.’ Four FPs with relationships did not
answer the question. Demographics of the two groups are presented in Table 3.
Table 3
Descriptive Statistics for Study Group (BCBSF data available)+
Characteristic Overall No Relationship
Yes Relationship
P value
Year of Graduation 133 (100.0) 34 (25.6) 99 (74.4) 0.52a
1970-1979 27 (20.3) 9 (26.5) 18 (18.2) 1980-1989 48 (36.1) 11 (32.4) 37 (37.4) 1990-1999 34 (25.6) 6 (17.6) 28 (28.3) 2000-present Before 1970
18 (13.5) 6 (4.5)
6 (17.6) 2 (5.9)
12 (12.1) 4 (4.0)
Practice Locale 133 (100.0) 34 (25.6) 99 (74.4) 0.34a
Rural 17 (12.8) 6 (17.6) 11 (11.1) Suburban Urban No Response
74 (55.6) 41 (30.8) 1 (0.8)
15 (44.1) 13 (38.2 0 (0.0)
59 (59.6) 28 (28.3)
1 (1.0)
Type of Practice 133^ (100.0) 34*(25.6) 99†(74.4)
Group practice 67 (50.4) 13 (38.2) 54 (54.5)
Solo practice Multi-specialty group Other Responses
46 (34.6) 12 (9.0)
17 (12.8)
11 (32.4) 4 (11.8) 11 (32.4)
35 (35.4) 8 (8.1) 6 (6.1)
Employment Status Full-time Part-time No response
133 (59.6) 122 (91.7) 10 (7.5) 1 (0.8)
34 (25.6) 30 (88.2) 4 (11.8)
0 (0.0)
99 (74.4) 92 (92.9)
6 (6.1) 1 (1.0)
0.46a
+Totals are presented as n (%)
*Total count and percentage for Type of Practice exceeded 34 and 25.6% due to respondents with more
than one response to this question †Total count and percentage for Type of Practice exceeded 99 and 74.4% due to respondents with more
than one response to this question
^Total count and percentage for Type of Practice exceeded 133 and 100% due to respondents with more
than one response to this question a Fisher’s exact test
b Chi-square test
48
Communication between FP and Hospitalists
Communication between physicians is critical to the overall quality of patient
care. The survey included several questions regarding communication between the FP
and the hospitalist, one being “how would you rate the communication that takes place
between you and the hospitalist?” Twenty-eight (82.4%) of the FPs with ‘no relationship’
did not respond to this question, 2 (5.9%) rated communication as ‘good’ and 4 (11.8%)
rated it as ‘poor.’ Nine (9.1%) of the FPs with established relationships rated
communication as ‘excellent.’ Eighteen (18.2%) rated communication as ‘very good.’
Twenty-nine (29.3%) rated communication as ‘good.’ Twenty-eight (28.3%) rated
communication as ‘fair.’ Fourteen (14.1%) rated communication as ‘poor.’ There was
one (1.0%) FP with an established relationship who did not respond to this question.
Respondents were asked how quickly they are notified that a patient has been
admitted. Here, most FPs with no hospitalist relationship did not respond to the question
(82.4%), though one FP (2.9%) responded that they were usually notified by the next day
and five FPs (14.7%) responded that they were routinely not notified. For those FPs with
hospitalist relationships, four (4.0%) responded that they were notified immediately, 19
(19.2%) responded that they were notified the same day, 34 (34.3%) responded that they
were notified by the next day, 16 (16.2%) responded that they were notified before
discharge, and 26 (26.3%) responded that they were routinely not notified.
Respondents were also asked “after discharge, how long is it before you receive
information such as the discharge summary, test results, pending test results, medication
summary information, post-discharge treatment plans, etc.?” Once again, 28 (82.4%) FPs
with no hospitalist relationship failed to answer this question, one (2.9%) responded that
49
they received post-discharge information in 4-7 days, one (2.9%) responded that they
received post-discharge information after more than seven days, and four (11.8%)
responded that they routinely did not receive any post-discharge information. For the FPs
with established hospitalist relationships, 11 (11.1%) responded that they received post-
discharge information on the same day, 46 (46.5%) responded that they received post-
discharge information in 1-3 days, 10 (10.1%) responded that they received post-
discharge information in 4-7 days, 14 (14.1%) responded that they received post-
discharge information after more than 7 days, and 18 (18.2%) responded that they
routinely did not receive any post-discharge information. Finally, when asked whether
improving communication between hospitalists and FPs would improve the quality of
patient care, 20 (58.8%) FPs with no hospitalist relationship and 95 (96.0%) FPs with
established hospitalist relationships answered ‘yes.’ The distribution of responses for
those with an established relationship with a hospitalist is presented in Table 4.

50
Table 4
Descriptive Statistics for Established Relationship and Communication Questions+
Characteristic Overall Responses
Rating of Communication Overall Excellent Very Good Good Fair Poor No Response Notification of Patient’s Hospitalization Immediately Same Day Next Day Before Discharge Routinely Not Notified Rating of Information Received During Hospitalization Excellent Very Good Good Fair Poor No Response Timeframe for Communication During Hospitalization Immediately Same Day Next Day Before Discharge Routinely Not Notified No Response Timeframe for Post-Discharge Information Same Day 1-3 Days 4-7 Days Over 1 Week Routinely Don’t Receive Types of Communication Received (Multiple Responses) Discharge Summary Test Results Pending Test Results Medication Summary Post-Discharge Plans Major Changes in Patient Status
99 9 (9.1)
18 (18.2) 29 (29.3) 28 (28.3) 14 (14.1)
1 (1.0) 99
4 (4.0) 19 (19.2) 34 (34.3) 16 (16.2) 26 (26.3)
99 9 (9.1)
19 (19.2) 17 (17.2) 35 (35.4) 17 (17.2)
2 (2.0) 99
5 (5.1) 16 (16.2) 24 (24.2) 21 (21.2) 31 (31.3) 2 ( 2.0)
99 11 (11.1) 46 (46.5) 10 (10.1) 14 (14.1) 18 (18.2)
99 83 (83.8) 28 (28.3) 17 (17.2) 40 (40.4) 40 (40.4) 29 (29.3)
+Total are presented as n (%)
51
Respondent Data Analysis
The two groups, ‘no relationship’ and ‘with relationship,’ were compared with
respect to the following demographic attributes: year of graduation, practice locale,
employment status, length of relationship, choice of hospitalist, and communication
ratings.
Year of Graduation and FP / Hospitalist Relationship
Of the 99 respondents with established hospitalist relationships, 18 (18.2%)
graduated medical school between 1970 and 1979, 37 (37.4%) graduated between 1980
and 1989, 28 (28.3%) graduated between 1990 and 1999, 12 (12.1%) graduated after
2000, and only 4 (4.0%) graduated prior to 1970. Of the 34 respondents with no
hospitalist relationship, 9 (26.5%) graduated medical school between 1970 and 1979, 11
(32.4%) graduated between 1980 and 1989, 6 (17.6%) graduated between 1990 and 1999,
6 (17.6%) graduated after 2000, and 2 (5.9%) graduated prior to 1970. There was no
difference in the distribution of the respondents’ year of graduation between FPs with no
hospitalist relationship compared to those with FPs with established hospitalist
relationships (Fisher’s p=3.2, p=0.52) (Table 3).
Practice Locale and FP / Hospitalist Relationship
Of the 99 respondents with established hospitalist relationships, 11 (11.1%) FPs
practiced in rural settings, 59 (59.6%) practiced in suburban settings, and 28 (28.3%)
practiced in urban settings. One (1.0%) physician failed to respond to this question. Of
the 34 respondents with no hospitalist relationship, 6 (17.6%) FPs practiced in rural
52
settings, 15 (44.1%) practiced in suburban settings, and 13 (38.2%) practiced in urban
settings. There was no difference in the distribution of practice locale between FPs with
no hospitalist relationship compared to those with FPs with established hospitalist
relationships (Fisher’s p=3.3, p=0.34) (Table 3).
Employment Status and FP / Hospitalist Relationship
Of the 99 respondents with established hospitalist relationships, 92 (92.9%)
worked full-time, 6 (6.1%) worked part-time, and 1 (1.0%) failed to respond. Of the 34
respondents with no hospitalist relationship, 30 (88.2%) worked full-time and 4 (11.8%)
worked part-time. There was no difference in the distribution of practice locale between
FPs with no hospitalist relationship compared to those with FPs with established
hospitalist relationships (Fisher’s p=1.7, p=0.46) (Table 3).
Type of Practice and FP / Hospitalist Relationship
Of the 99 respondents with established hospitalist relationships, 54 (54.5%) were
part of a group practice, 35 (35.4%) were solo practice, 8 (8.1%) were part of a multi-
specialty group, and 6 (6.1%) had another type of practice. Of the 34 respondents with no
hospitalist relationship, 13 (38.2%) were part of a group practice, 11 (32.4%) were solo
practice, 4 (11.8%) were part of a multi-specialty group, and 11 (32.4%) had another type
of practice (Table 3). For analysis, the respondents who answered ‘solo practice’ and
‘other practice’ were placed in the solo practice category. One respondent chose both
‘group practice’ and ‘multi-specialty practice.’ This response was placed in the group
practice category. Another respondent chose both ‘solo practice’ and ‘other practice.’
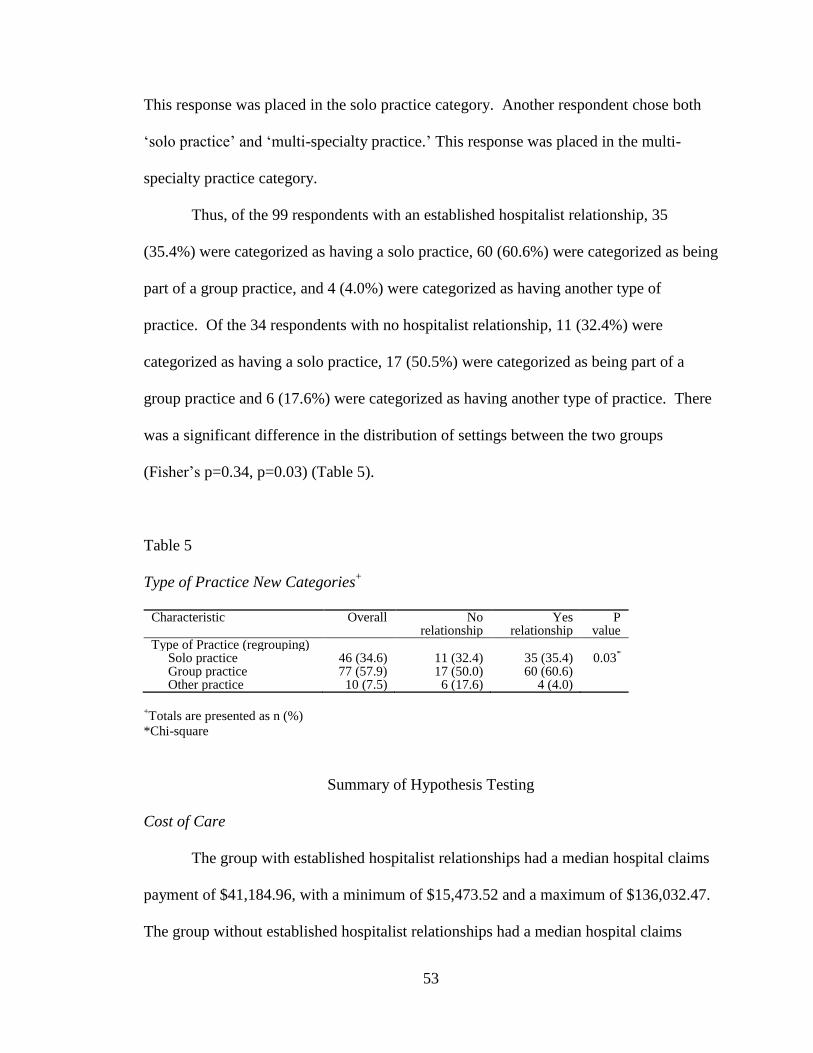
53
This response was placed in the solo practice category. Another respondent chose both
‘solo practice’ and ‘multi-specialty practice.’ This response was placed in the multi-
specialty practice category.
Thus, of the 99 respondents with an established hospitalist relationship, 35
(35.4%) were categorized as having a solo practice, 60 (60.6%) were categorized as being
part of a group practice, and 4 (4.0%) were categorized as having another type of
practice. Of the 34 respondents with no hospitalist relationship, 11 (32.4%) were
categorized as having a solo practice, 17 (50.5%) were categorized as being part of a
group practice and 6 (17.6%) were categorized as having another type of practice. There
was a significant difference in the distribution of settings between the two groups
(Fisher’s p=0.34, p=0.03) (Table 5).
Table 5
Type of Practice New Categories+
Characteristic Overall No relationship
Yes relationship
P value
Type of Practice (regrouping) Solo practice 46 (34.6) 11 (32.4) 35 (35.4) 0.03
*
Group practice 77 (57.9) 17 (50.0) 60 (60.6) Other practice 10 (7.5) 6 (17.6) 4 (4.0)
+Totals are presented as n (%)
*Chi-square
Summary of Hypothesis Testing
Cost of Care
The group with established hospitalist relationships had a median hospital claims
payment of $41,184.96, with a minimum of $15,473.52 and a maximum of $136,032.47.
The group without established hospitalist relationships had a median hospital claims
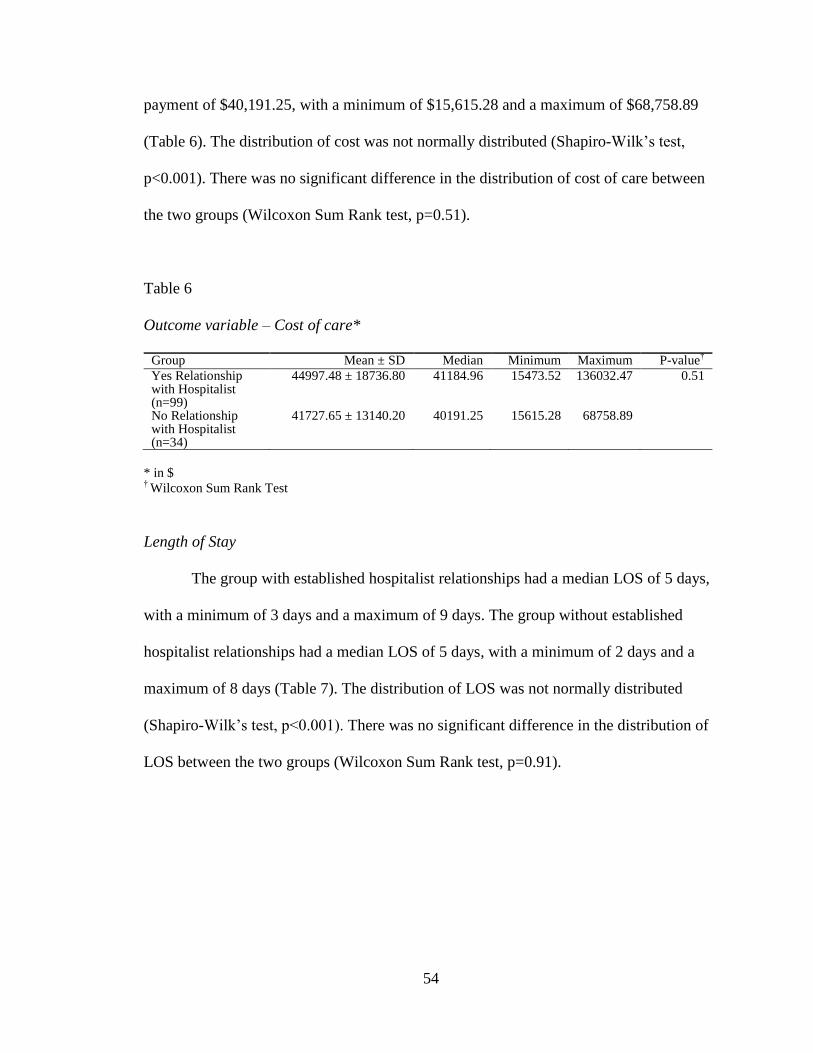
54
payment of $40,191.25, with a minimum of $15,615.28 and a maximum of $68,758.89
(Table 6). The distribution of cost was not normally distributed (Shapiro-Wilk’s test,
p<0.001). There was no significant difference in the distribution of cost of care between
the two groups (Wilcoxon Sum Rank test, p=0.51).
Table 6
Outcome variable – Cost of care*
Group Mean ± SD Median Minimum Maximum P-value
†
Yes Relationship with Hospitalist (n=99)
44997.48 ± 18736.80 41184.96 15473.52 136032.47 0.51
No Relationship with Hospitalist (n=34)
41727.65 ± 13140.20 40191.25 15615.28 68758.89
* in $ † Wilcoxon Sum Rank Test
Length of Stay
The group with established hospitalist relationships had a median LOS of 5 days,
with a minimum of 3 days and a maximum of 9 days. The group without established
hospitalist relationships had a median LOS of 5 days, with a minimum of 2 days and a
maximum of 8 days (Table 7). The distribution of LOS was not normally distributed
(Shapiro-Wilk’s test, p<0.001). There was no significant difference in the distribution of
LOS between the two groups (Wilcoxon Sum Rank test, p=0.91).
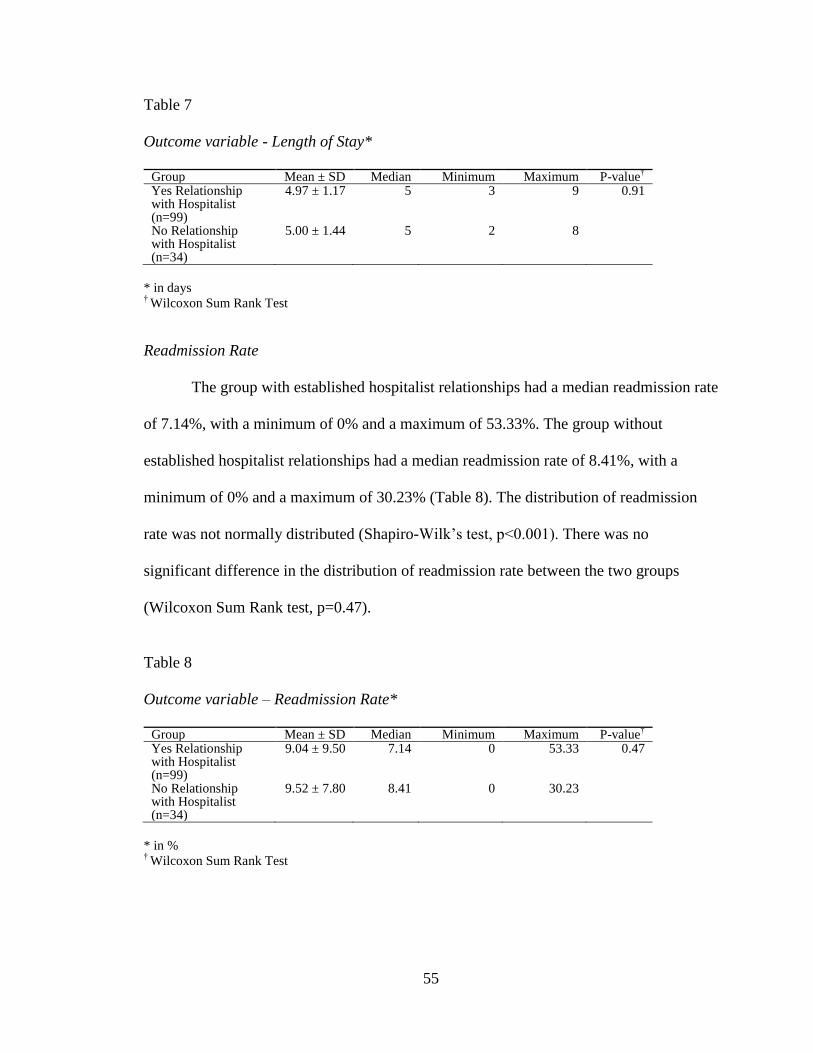
55
Table 7
Outcome variable - Length of Stay*
Group Mean ± SD Median Minimum Maximum P-value
†
Yes Relationship with Hospitalist (n=99)
4.97 ± 1.17 5 3 9 0.91
No Relationship with Hospitalist (n=34)
5.00 ± 1.44 5 2 8
* in days † Wilcoxon Sum Rank Test
Readmission Rate
The group with established hospitalist relationships had a median readmission rate
of 7.14%, with a minimum of 0% and a maximum of 53.33%. The group without
established hospitalist relationships had a median readmission rate of 8.41%, with a
minimum of 0% and a maximum of 30.23% (Table 8). The distribution of readmission
rate was not normally distributed (Shapiro-Wilk’s test, p<0.001). There was no
significant difference in the distribution of readmission rate between the two groups
(Wilcoxon Sum Rank test, p=0.47).
Table 8
Outcome variable – Readmission Rate*
Group Mean ± SD Median Minimum Maximum P-value
†
Yes Relationship with Hospitalist (n=99)
9.04 ± 9.50 7.14 0 53.33 0.47
No Relationship with Hospitalist (n=34)
9.52 ± 7.80 8.41 0 30.23
* in % † Wilcoxon Sum Rank Test
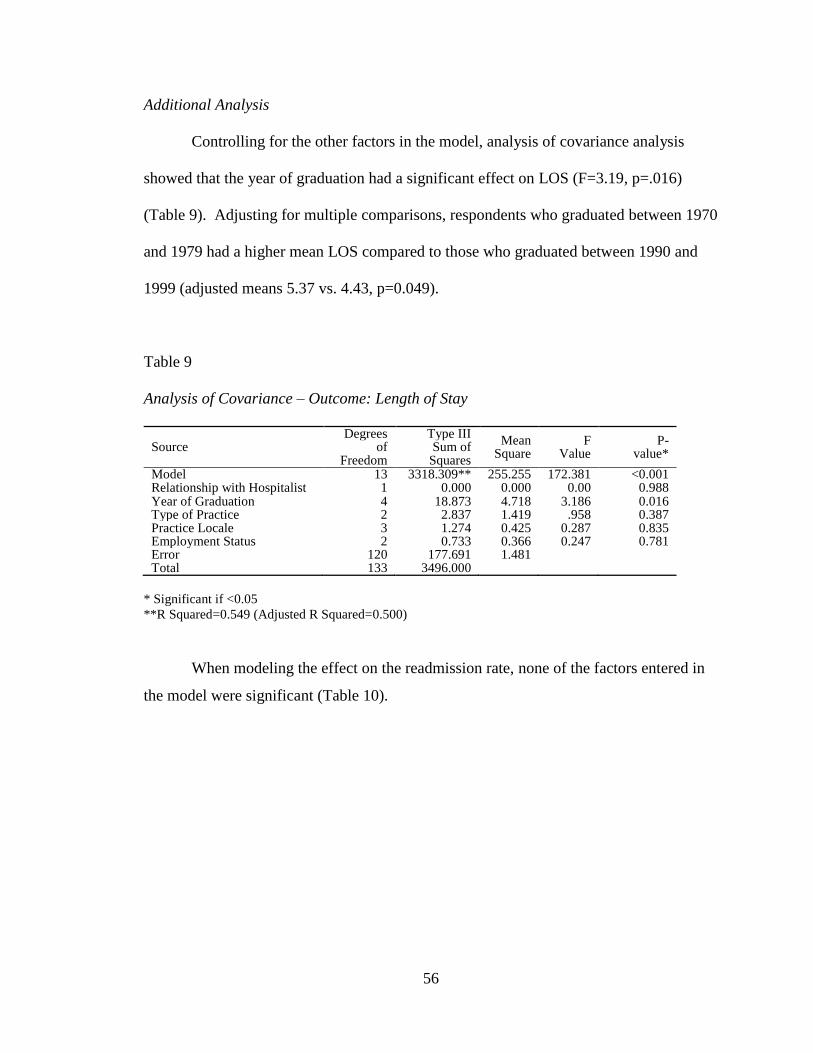
56
Additional Analysis
Controlling for the other factors in the model, analysis of covariance analysis
showed that the year of graduation had a significant effect on LOS (F=3.19, p=.016)
(Table 9). Adjusting for multiple comparisons, respondents who graduated between 1970
and 1979 had a higher mean LOS compared to those who graduated between 1990 and
1999 (adjusted means 5.37 vs. 4.43, p=0.049).
Table 9
Analysis of Covariance – Outcome: Length of Stay
Source Degrees
of Freedom
Type III Sum of
Squares
Mean Square
F Value
P- value*
Model 13 3318.309** 255.255 172.381 <0.001 Relationship with Hospitalist 1 0.000 0.000 0.00 0.988 Year of Graduation 4 18.873 4.718 3.186 0.016 Type of Practice 2 2.837 1.419 .958 0.387 Practice Locale 3 1.274 0.425 0.287 0.835 Employment Status 2 0.733 0.366 0.247 0.781 Error 120 177.691 1.481 Total 133 3496.000
* Significant if <0.05
**R Squared=0.549 (Adjusted R Squared=0.500)
When modeling the effect on the readmission rate, none of the factors entered in
the model were significant (Table 10).
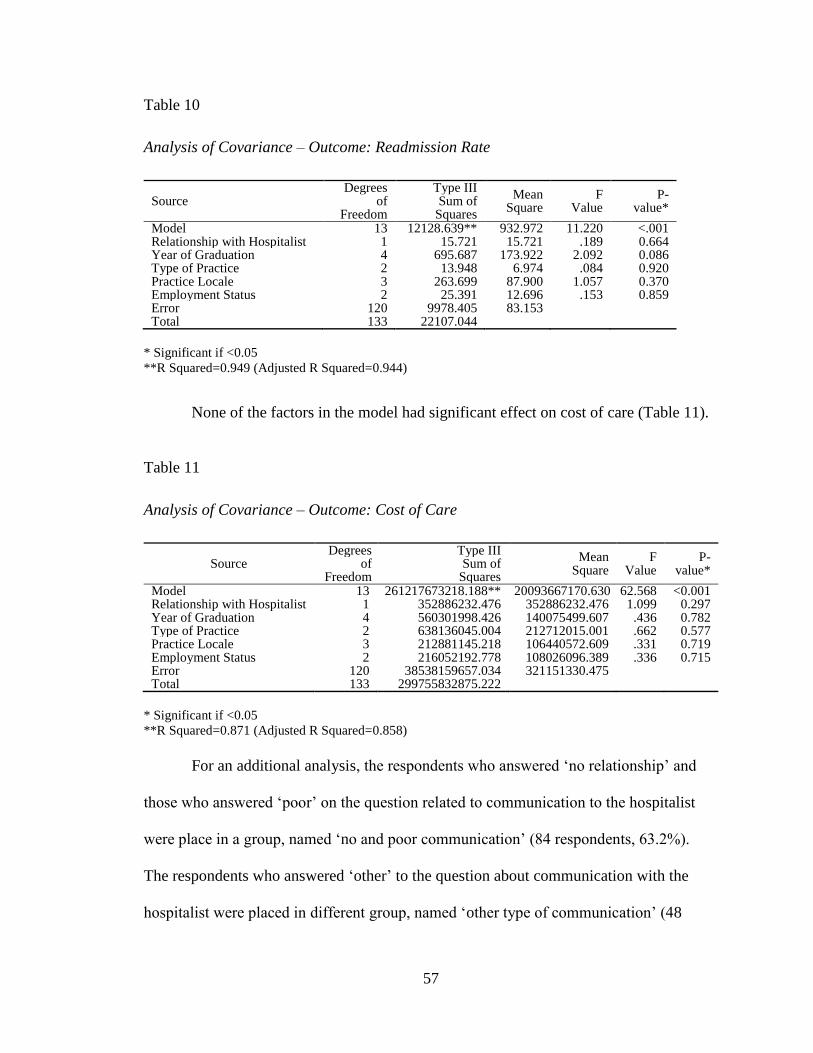
57
Table 10
Analysis of Covariance – Outcome: Readmission Rate
Source Degrees
of Freedom
Type III Sum of
Squares
Mean Square
F Value
P- value*
Model 13 12128.639** 932.972 11.220 <.001 Relationship with Hospitalist 1 15.721 15.721 .189 0.664 Year of Graduation 4 695.687 173.922 2.092 0.086 Type of Practice 2 13.948 6.974 .084 0.920 Practice Locale 3 263.699 87.900 1.057 0.370 Employment Status 2 25.391 12.696 .153 0.859 Error 120 9978.405 83.153 Total 133 22107.044
* Significant if <0.05
**R Squared=0.949 (Adjusted R Squared=0.944)
None of the factors in the model had significant effect on cost of care (Table 11).
Table 11
Analysis of Covariance – Outcome: Cost of Care
Source Degrees
of Freedom
Type III Sum of Squares
Mean Square
F Value
P- value*
Model 13 261217673218.188** 20093667170.630 62.568 <0.001 Relationship with Hospitalist 1 352886232.476 352886232.476 1.099 0.297 Year of Graduation 4 560301998.426 140075499.607 .436 0.782 Type of Practice 2 638136045.004 212712015.001 .662 0.577 Practice Locale 3 212881145.218 106440572.609 .331 0.719 Employment Status 2 216052192.778 108026096.389 .336 0.715 Error 120 38538159657.034 321151330.475 Total 133 299755832875.222
* Significant if <0.05
**R Squared=0.871 (Adjusted R Squared=0.858)
For an additional analysis, the respondents who answered ‘no relationship’ and
those who answered ‘poor’ on the question related to communication to the hospitalist
were place in a group, named ‘no and poor communication’ (84 respondents, 63.2%).
The respondents who answered ‘other’ to the question about communication with the
hospitalist were placed in different group, named ‘other type of communication’ (48
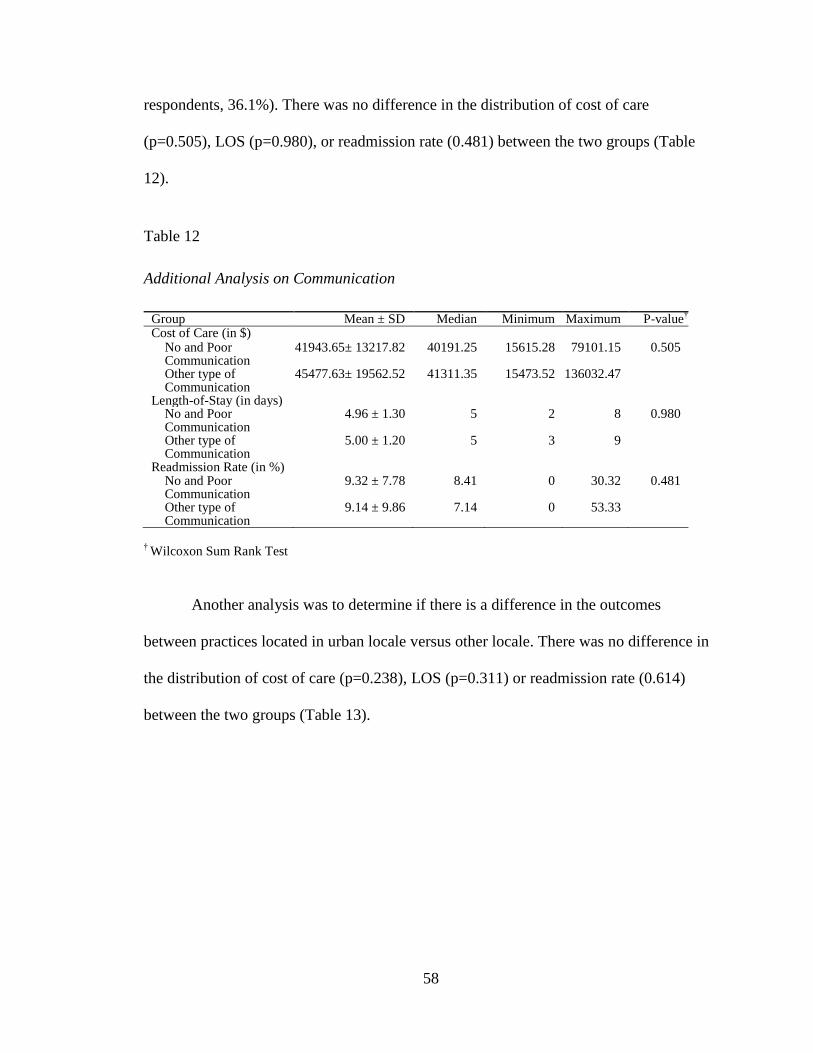
58
respondents, 36.1%). There was no difference in the distribution of cost of care
(p=0.505), LOS (p=0.980), or readmission rate (0.481) between the two groups (Table
12).
Table 12
Additional Analysis on Communication
Group Mean ± SD Median Minimum Maximum P-value†
Cost of Care (in $) No and Poor Communication
41943.65± 13217.82 40191.25 15615.28 79101.15 0.505
Other type of Communication
45477.63± 19562.52 41311.35 15473.52 136032.47
Length-of-Stay (in days) No and Poor Communication
4.96 ± 1.30 5 2 8 0.980
Other type of Communication
5.00 ± 1.20 5 3 9
Readmission Rate (in %) No and Poor Communication
9.32 ± 7.78 8.41 0 30.32 0.481
Other type of Communication
9.14 ± 9.86 7.14 0 53.33
† Wilcoxon Sum Rank Test
Another analysis was to determine if there is a difference in the outcomes
between practices located in urban locale versus other locale. There was no difference in
the distribution of cost of care (p=0.238), LOS (p=0.311) or readmission rate (0.614)
between the two groups (Table 13).
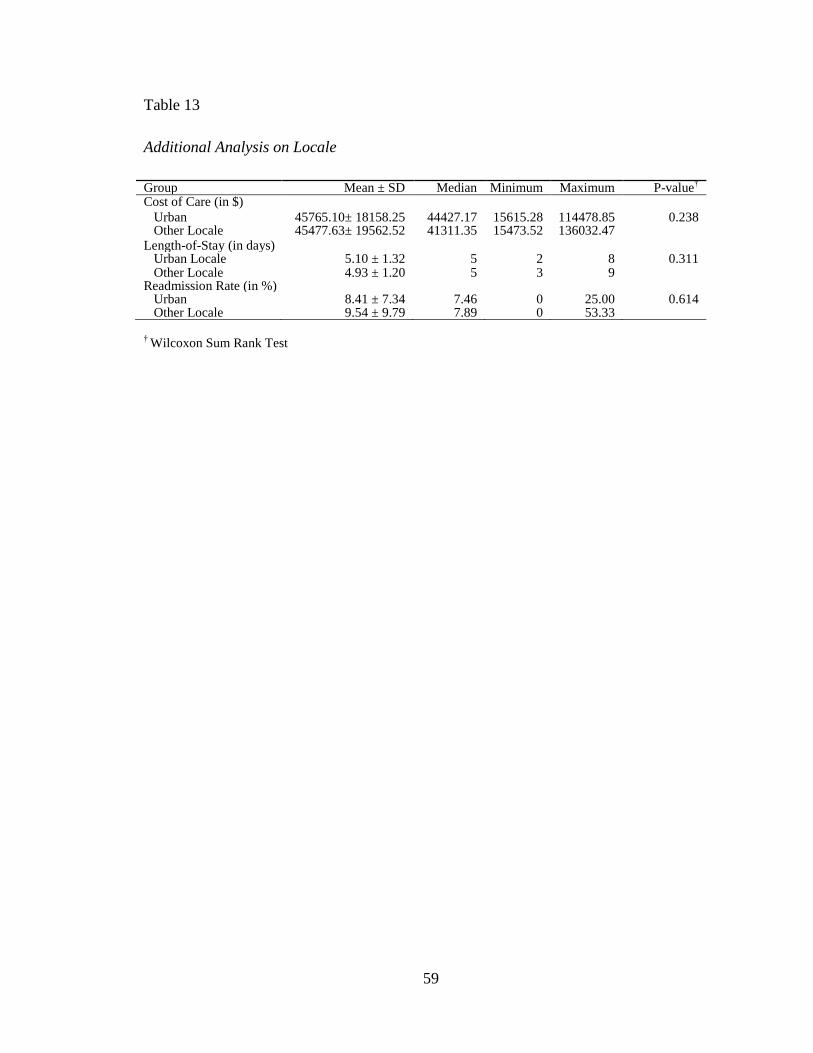
59
Table 13
Additional Analysis on Locale
Group Mean ± SD Median Minimum Maximum P-value†
Cost of Care (in $)
Urban 45765.10± 18158.25 44427.17 15615.28 114478.85 0.238 Other Locale 45477.63± 19562.52 41311.35 15473.52 136032.47 Length-of-Stay (in days) Urban Locale 5.10 ± 1.32 5 2 8 0.311 Other Locale 4.93 ± 1.20 5 3 9 Readmission Rate (in %) Urban 8.41 ± 7.34 7.46 0 25.00 0.614 Other Locale 9.54 ± 9.79 7.89 0 53.33
† Wilcoxon Sum Rank Test
60
CHAPTER V
SUMMARY AND CONCLUSIONS
The purpose of this study was to determine the effect on patient outcomes of FPs
with an established relationship with a hospitalist or hospitalist group versus FPs who do
not have such a relationship. This study is also meant to provide the reader with insight
about the level of communication FPs feel they have with hospitalists today. By
analyzing the relationships between FPs and hospitalists, then determining the effect on
patients’ LOS, readmissions rate, and payments for hospitalization, practitioners and
researchers can have a better understanding of how an established relationship relates to
these patient outcomes. Other considerations such as year of graduation, practice locale,
type of office arrangement, employment status, and length of the relationship also play a
role in these outcomes. Most of the empirical research on this topic has been limited to
single site, observational studies, and the results of the few randomized trials have been
mixed. This study provides additional information regarding hospitalists and their effect
on these three patient outcome measures.
Conclusions and Implications
The three hypotheses for this study set out to answer two questions. First, do FPs
who have an ongoing relationship with a hospitalist or hospitalist group (six months or
greater) have significantly different patient outcomes for their hospitalized patients than
FPs who have no established relationship with a hospitalist? Second, how do FPs with an
61
established relationship with a hospitalist or hospitalist group rate the communication that
takes place between themselves and the hospital-based physician?
Each of the three hypotheses was tested based on responses to the study survey
and matched to the BCBSF database to determine patients’ mean cost of care, LOS, and
risk of readmission. The hypotheses were focused on the effect on patient outcomes for
these three measures for FPs having an established relationship with a hospitalist versus
those that did not have such a relationship. For each measure, the hypothesis was that
having or not having an established relationship would cause a significant difference in
outcomes between the two groups.
The study focused on the fact that many feel that LOS and hospital costs are
significantly less when FPs use hospitalists for patients’ hospitalizations. It is also
commonly felt that readmissions are higher when hospitalists are involved because their
goal is to get the patient out of the hospital as quickly and inexpensively as possible
because of pressure from both the hospital and insurance companies. Although there were
detected differences between those having and not having an established relationship,
there was no significance in these findings. In fact, the numbers for this study
demonstrated that the group with established relationships had higher overall costs,
longer LOS, and lower readmission rates.
Ratings of Communication between FPs and Hospitalists
Based on Homan’s exchange theory approach regarding physician relations,
physicians seek to collaborate with other physicians when providing care to their patients
in an exchange that maximizes benefits and minimizes costs between the parties involved
62
in the interaction (Shortell, 1974). The theory holds that when the benefits outweigh the
risk of the exchange, the interaction will occur, but it will be terminated or abandoned if
the risks become too great. Another aspect of this study was to determine if the length of
the established relationship had a significant effect on patient outcomes. It is reasonable
to think that FPs with an established relationship with a hospitalist for more than five
years are reasonably satisfied with the relationship. Although not statistically significant,
most physicians with an established relationship of more than five years rated their
communication with the hospitalist as good, very good, or excellent.
Survey Comments about Communications between FPs and Hospitalists
During the survey, respondents were asked “do you believe that improving
communication between hospitalists and FPs would improve the quality of patient care?”
They were then asked to elaborate on how to improve the communication, if they
answered ‘yes,’ or to comment on why improving communication would not improve
care, if they responded ‘no.’ Over 86% of the respondents used for the final analysis
stated that improving communication quality would have a positive effect on patient care.
Many FPs felt that timely feedback from specialists and hospitalists would improve care
and prevent redundant testing. They complained about the current lack of information
that they receive from hospitalists and felt that this can only harm patients in the long run.
One respondent wrote that “I have complained and tried to have a system where I am
notified and receive records from hospitalized patients. It is not being done.” Others
stated that communication is better when the relationship between the FP and hospitalist
is established, but one FP wrote that “hospitalists who admit my patients to a hospital I
63
don't go to tell me nothing...ever!!” In academic settings, faculty physicians stated that
they were trying to teach residents how to best communicate with FPs during a patient’s
hospitalization.
Respondents also felt that when they are not notified of a hospitalization, the
hospital team frequently is unaware of important information which might benefit the
patient's care (recent labs, current meds, and other information). This wastes resources
by repeating tests that have already been done. Hospitalists rarely have the context of the
longitudinal care of the patient which can only be gleaned from the FP through records or
direct communication.
In order to provide comprehensive health care management and oversight, it is
imperative for the FP to receive accurate and up-to-date information. FPs responding to
the survey commented that patient care would definitely improve if there was direct
communication with the hospitalist, particularly regarding medication changes and
patient disposition, which is critical to coordinate post-hospitalization care. Respondents
stated that discharge summaries are not often transcribed in a timely manner and that
patients often return bottles of unknown medicines. Many FPs stated that it is rare to
receive a call from a hospitalist to elicit information about patients. One FP stated that
they have given their patients cards with their contact information and asked the patient
to show the card to any other providers caring for them. Several FPs stated that, if they
are aware of a hospitalization of one of their patients, they try to make a social visit
during the hospitalization in order to work with the hospital team and to facilitate the
transition to outpatient care. Almost all respondents commented that there is a need for
enhancements in communication and records transfers.
64
Improvements in communication would help ensure that patients’ wishes are
respected, eliminate unnecessary testing, and allow FPs to be more aggressive in
scheduling follow-up office visits. Interoperability between hospitals’ records systems
and FPs’ records systems would also better facilitate the transition of patient care.
Medication reconciliation, pending tests, specialist follow-up, PCP follow-up, and other
information is critical to preventing patients from falling through the cracks and
potentially suffering setbacks or hospital readmission. It would also minimize errors in
prescriptions, diagnostic tests and referrals. Immediate notification on day of admission
and day of discharge would better facilitate post-discharge follow-up and care.
Many respondents stated that hospitalists are usually assigned by insurance
companies or the hospital. They felt that they have no personal relationship with these
assigned physicians and that these hospitalists do not seem to be interested in the
continuity of care. One respondent wrote “it depends upon whether you use a private
hospitalist, or a hospital-contracted hospitalist. I went the latter route and hated it. Since
going the former route, the care for patients and communication has markedly improved.”
A common theme from survey respondents centered on the need for seamless and
automatic electronic communication regarding notification of admission, discharge, test
results, and follow-up. When electronic communication doesn’t occur, FPs (or their
staff) must look up this information when the patient comes to the office. To demonstrate
this, one respondent wrote that they currently receive a brief email that a patient was
discharged on a certain date for a particular diagnosis. Once in a while the email will
include suggested follow-up. However, more often than not, the email only refers the
provider to the discharge summary that will arrive in 1-3 days. Unfortunately, the
65
discharge summary does not always include lab or imaging results. This means that the
FP must log onto the hospital’s electronic medical record system, which is slow and
makes retrieval of information cumbersome at best. When there is not communication
from the hospitalist, FPs designate staff to call for the information, which also delays
follow-up care in the office setting.
Several respondents stated that many times the patient just assumes they know
what is happening, but this is only true if the FP has consistent communication with the
hospitalist or has access to the electronic health record. Most FPs stated that they would
be glad to share patients’ charts (with diagnoses, past procedures and medication list) and
even recent lab, x-ray or EKG, at the time of hospitalization. Only rarely are they ever
asked for this information. Many FPs feel that the hospitalist tries to do the bare
minimum to get the patient out of the hospital, leaving the FP hardly knowing why the
patient went to the hospital in the first place.
Limitations of the Study
There are several limitations to this study, with the primary issue relating to the
sample size that was available for the final analysis. The request to participate resulted in
232 responses to the survey sent to the members of the FAFP. Initially, this appeared to
be a sufficient number of study responses to test the three hypotheses and address the
research questions regarding the differences the existent or nonexistent relationships
between FPs and hospitalists might have on patient outcomes. After excluding responses
that did not address the established relationship question, removing FPs who function as
66
hospitalists or emergency room physicians, and eliminating those respondents who had
no BCBSF data, the final sample size was 133.
These 133 respondents represented slightly more than 4% of the FAFP members
surveyed, but the distribution of responses between the ‘established relationship’ group
versus the ‘no relationship’ group was 74% to 26% respectively. Examination of the
power for this study shows that, given the achieved sample size and observed variability,
there was only 57% power to detect a 0.50 day difference in LOS. In order to achieve a
desired 80% power to detect this effect size, at least 76 responses would have been
needed in each of the two groupings. The achieved power estimates for cost (47% for a
$5,000 difference) and for readmission rate (24% for a 2% difference were also low. A
significantly larger sample would be required to achieve 80% power for either of these
two outcomes.
A secondary limitation was that the study methodology did not provide the
researcher with the patient counts for each respondent. This limitation made it difficult to
exclude outliers that may have had an adverse effect on the three outcome measures.
Further, the study was limited to the membership of the FAFP, which only represents FPs
from the State of Florida. Also, the distribution of the survey responses from across the
state was not controlled because addresses and/or zip codes were not captured by the
survey instrument to protect the anonymity of the respondents.
Another key issue was that the survey was not limited to physicians who were
known to have patients in the BCBSF database. This caused many responses (73) to be
excluded from the final analysis. The survey was conducted by the FAFP in an effort to
67
elicit greater physician participation. However, all members of this association are not
participants in the BCBSF network and this factor greatly affected the final sample size.
Finally, when physicians were asked to provide their NPI, many chose not to
respond even when assured of the confidentiality of their responses. It is felt that the
survey methodology limited the number of responses despite the fact that the actual
responses were confidential and a number of incentives were given for participation.
Recommendations for Future Study
This study provides a solid baseline for additional research into how the
relationship between hospitalists and FPs affects patient outcomes. Although there are
some studies in the literature regarding hospitalists and patient outcomes, it is important
that more research be conducted to determine the significance of the hospitalist’s role in
the delivery of quality, cost-effective healthcare. Most health systems spend considerable
resources to insure that hospitalists are available to take unassigned patients and the
patients of physicians who no longer practice in the inpatient setting.
Future research should be conducted by healthcare organizations in cooperation
with key insurers such as BCBSF to help validate the effect that hospitalists have on
improving patient outcomes, improving patient and physician satisfaction, and bending
the cost curve. A study looking at patient outcomes of only physicians who participate in
BCBSF plans should be conducted to improve the sample size and provide the power to
determine if significant differences exist in key patient metrics such as LOS, readmission
rates, expected mortality rates, and other outcomes that measure the effectiveness of
efforts to improve the quality of the healthcare delivery system. Future studies should
68
also look at the effect that payor mix and case mix have on selected outcomes.
Additional investigation regarding the communication taking place between physicians
and how it affects patient outcomes is also warranted.
Research should be conducted on the effect that specific types of communication
between hospitalists and PCPs have on the quality of care provided to patients.
Respondents in this study shared perceptions they have about the type and quality of
interaction they had with hospitalists. They perceived that improvements in these
interactions will result in better outcomes for their patients. More research should
examine specific types of communication and the effect, if any, they have on outcomes.
Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS)
is a national, standardized, survey of patients’ perspectives about the care they receive
during hospitalization. This information was first publically reported on the U.S.
Department of Health and Human Services (HHS) Hospital Compare website beginning
in 2008. Participation by hospitals was initially voluntary but is now required for
participation in Medicaid and Medicare. Now that this comparative database is fully
implemented, the core measures could be used to compare patient data where the
hospitalists were involved in the inpatient stay versus the outcomes for patients with no
hospitalist involvement. The HCAHPS metrics are available for almost all hospitals and,
because they are publically reported, they are readily available for use by researchers.
The Center for Medicare and Medicaid Services (CMS) HCAHPS database has over
3,700 hospitals that report their data and CMS will begin imposing financial penalties for
excess admissions in 2013. National benchmarks on patient quality outcomes such as
69
falls, infection rates, pressure ulcer rates, etc. will be easily accessed and available for
research purposes.
Summary
The field of hospital medicine is here to stay. It is vitally important that hospitals,
physicians, payors, and employers know whether hospitalists have a positive effect on
patient outcomes. This study attempted to address this overarching research question and
prove or disprove three hypotheses related to patient outcomes. It examined whether FPs
who have developed an established relationship with a hospitalist or hospitalist group
have significantly better patient outcomes than FPs who have no such relationship.
Hospitals continue to rely on physicians who specialize in the practice of hospital
medicine (hospitalists). The SHM states that hospitalists have a core competency for
managing patients during their hospital stay and work to enhance the performance of
hospitals and healthcare delivery system. It is clear that hospitalists should help resolve
the issues of ineffective communication and incomplete handoffs, which results in poor
information exchange and negatively impacts patient care. By enhancing communication
between hospitalists and FPs, care to the patient should become seamless and number of
medical errors should decrease. The future of the hospitalist model centers on the
relationship between the PCP and the hospitalist. PCPs are no longer able to follow
patients admitted to the hospital. The benefit of the hospitalist model is improved
continuity of care for the patient, which should definitely lead to better patient outcomes.
The question that still remains is whether this can be proven.
70
REFERENCES
Arora, V.M., Manjarrez, E., Dressler, D.D., Basaviah, P., Halasyamani, L., & Kripalani,
S. (2009). Hospitalist Handoffs: A Systematic Review and Task Force
Recommendations. Journal of Hospital Medicine, 4 (7), 433-440.
Auerbach, A.D., Aronson, M.D., Davis, R.B., & Phillips, R.S. (2003). How Physicians
Perceive Hospitalist Services After Implementation; Anticipation vs. Reality.
Archives of Internal Medicine, 163 (19), 2330-2336.
Auerbach, A.D., Nelson, E.A., Lindenauer, P.K., Pantilat, S.Z., Katz, P.P., & Wachter,
R.M. (2000). Physician Attitudes Toward and Prevalence of the Hospitalist Model
of Care: Results of a National Survey. American Journal of Medicine, 109 (8)
648-653.
Auerbach, A.D., Wachter, R.M., Katz, P., Showstack, J., Baron, R.B., & Goldman, L.
(2002). Implementation of a Voluntary Hospitalist Service at a Community
Teaching Hospital: Improved Clinical Efficiency and Patient Outcomes. Annals of
Internal Medicine, 137 (11) 859-865.
Bailit, M., & Hughes, C. (2008). The Patient-Centered Medical Home: A Purchaser
Guide. Patient-Centered Primary Care Collaborative. Retrieved from
http://www.pcpcc.net/content/purchasers-guide-0
Bell, C.M., Schnipper, J.L., Auerbach, A.D., Kaboli, P.J., Wetterneck, T.B., Gonzales,
D.V., Arora, V.M., Zhang, J.X., & Meltzer, D.O. (2009). Association of
Communication Between Hospital-based Physicians and Primary Care Providers
with Patient Outcomes. Journal of General Internal Medicine, 24 (3) 381-386.
Bernd, D.L. (2009). The Future Role of Hospitalists. The Hospitalist, Retrieved from
www.the-hospitalist.org/details/article/279375
Blau, P. (1964). Exchange and Power in Social Life. New York, NY: John Wiley and
Sons.
Blue Cross & Blue Shield of Florida (2008). Recognizing Physician Excellence Program.
Retrieved from http://www.bcbsfl.org/DocumentLibrary/Providers/Content/
RPEPhysicianToolsManual.pdf
Bodenheimer, T. (2006). Primary Care – Will It Survive. New England Journal of
Medicine, 355, 861-864.
71
Brown, R.G. (1998). Hospitalist Concept: Another Dangerous Trend. American Family
Physician, 58 (2), 339-42.
Calkins, D.R., Davis, R.B., Phillips, R.S., Pineo, K.L., Delbanco, T.L., & Lezzoni, L.I.
(1997). Patient-physician Communication at Hospital Discharge and Patients’
Understanding of the Post-discharge Treatment Plan. Archives of Internal
Medicine, 157 (9), 1026-1030.
Coffman, J., & Rundall, T.G. (2005). The Impact of Hospitalists on the Cost and Quality
of Inpatient Care in the United States: A Research Synthesis. Medical Care
Research and Review, 62 (4), 379-406.
Committee on Healthcare in America, Institute of Medicine (2001). Crossing the Quality
Chasm: A New Health System for the 21st Century. Washington, DC: National
Academies Press.
Conway, P.H. (2009). Value-Driven Health Care: Implications for Hospitals and
Hospitalists. Journal of Hospital Medicine, 4 (8), 507-511.
Flanders, S.A., & Wachter, R.M. (2003). Hospitalists: The New Model of Inpatient
Medical Care in the United States. European Journal of Internal Medicine, 14
(1), 65-70.
Geehr, E.D., & Nelson, J.R. (2002). Hospitalists: Who They Are and What They Do.
Physician Executive Journal, 28 (6), 26-31.
Gregory, D.W., Baigelman, W., & Wilson, I.B. (2003). Hospital Economics of the
Hospitalist. Health Services Research Journal, 38 (3), 905-918.
Hamel, M.B., Drazen, J.M., & Epstein, A.M. (2009). The Growth of Hospitalists and the
Changing Face of Primary Care. New England Journal of Medicine, 360 (11),
1141-1143.
Harlan, G., Srivastava, R., Harrison, L., McBride, G., & Maloney, C. (2009). Pediatric
Hospitalists and Primary Care Providers: A Communication Needs Assessment.
Journal of Hospital Medicine, 4 (3), 187-193.
Hauer, K.E., Wachter, R.M., McCulloch, C.E., Woo, G.A., & Auerbach, A.D. (2004).
Effects of Hospitalist Attending Physicians on Trainee Satisfaction with Teaching
and with Internal Medicine Rotations. Archives of Internal Medicine,164 (17),
1866-1871.
Henry, L.A. (1998). What the Hospitalist Movement Means to Family Physicians. Family
Practice Management Journal, 5 (10), 54-62.
72
Hinami, K., Farnan, J.M., Meltzer, D.O., & Arora, V.M. (2009). Understanding
Communication During Hospitalist Service Changes: A Mixed Methods Study.
Journal of Hospital Medicine, 4 (9), 535-540.
Homans, G.C. (1958). Social Behavior as Exchange. American Journal of Sociology, 63
(6), 597-606.
Homans, G.C. (1961). Social Behavior: Its Elementary Forms. New York, NY:
Harcourt, Brace, and World Inc.
Hruby, M., Pantilat, S.Z., & Lo, B. (2001). How Do Patients View the Role of the
Primary Care Physician in Inpatient Care?. American Journal of Medicine, 111
(9B), 21S-25S.
Kim, C.S., Hart, A.L., Paretti, R.F., Kuhn, L., Dowling, A.E., Benkeser, J.L., &
Spahlinger, D.A. (2011). Excess Hospitalization Days in an Academic Medical
Center: Perceptions of Hospitalists and Discharge Planners. American Journal of
Managed Care, 17 (2), e34-e42.
Kohn, L.T., Corrigan, J.M., & Donaldson, M.S., Eds. (2000). To Err is Human: Building
a Safer Health System. Washington, DC: National Academy Press.
Kripalani, S., LeFevre, F., Phillips, C.O., Williams, M.V., Basaviah, P., & Baker, D.W.
(2007). Deficits in Communication and Information Transfer between Hospital-
Based and Primary Care Physicians: Implications for Patient Safety and
Continuity of Care. Journal of the American Medical Association, 297 (8), 831-
841.
Kripalani, S., Jackson, A.T., Schnipper, J.L., & Coleman, E.A. (2007). Promoting
Effective Transitions of Care at Hospital Discharge: A Review of Key Issues for
Hospitalists. Society of Hospital Medicine, 2 (5), 314-323.
Kuo, Y.F., & Goodwin, J.S. (2011). Association of Hospitalist Care with Medical
Utilization after Discharge: Evidence of Cost Shift from a Cohort Study.
American College of Physicians, Annals of Internal Medicine, 155 (3), 152-159.
Leykum, L., & Mortensen, E. (2010). Exploring the Potential Causes of the Emergence
of Hospitalists: Chicken vs. Egg. Journal of General Internal Medicine, 25 (5),
378-379.
Meltzer, D.O., & Chung, J.W. (2010). U.S. Trends in Hospitalization and Generalist
Physician Workforce & the Emergence of Hospitalists. Journal of General
Internal Medicine, 25 (5), 453-459.
73
Meltzer, D., Manning, W.G., Morrison, J., Shah, M.N., Jin, L., Guth, T., & Levinson, W.
(2002). Effects of Physician Experience on Costs and Outcomes on an Academic
General Medicine Service; Results of a Trial of Hospitalists. Annals of Internal
Medicine, 137 (11), 866-874.
Pantilat, S.Z., Lindenauer, P.K., Katz, P.P., & Wachter, R.M. (2001). Primary Care
Physician Attitudes Regarding Communication with Hospitalists. American
Journal of Medicine, 111 (9B) 15S-20S.
Ranji, S.R., Rosenman, D.J., Amin, A.N., & Kripalani, S. (2006). Hospital Medicine
Fellowships: Works in Progress. American Journal of Medicine, 119 (1), 1-7.
Rosenthal, T. (2008). The Medical Home: Growing Evidence to Support a New
Approach to Primary Care. Journal of the American Board of Family Medicine,
21 (5), 427-440.
Roytman, M.M., Thomas, S.M., & Jiang, C.S. (2008). Comparison of Practice Patterns of
Hospitalists and Community Physicians in the Care of Patients with Congestive
Heart Failure. Journal of Hospital Medicine, 3 (1), 34-41.
Schroeder, S.A., & Schapiro, R. (1999). The Hospitalist: New Boon for Internal
Medicine or Retreat from Primary Care?. Annals of Internal Medicine, 130 (4),
382-387.
Sehgal, N.L., & Wachter, R.M. (2006). The Expanding Role of Hospitalists in the United
States. Swiss Medical Weekly, 136 (37), 591-596.
Shortell, S. M. (1974). Determinants of Physician Referral Rates: An Exchange Theory
Approach. Medical Care, 12 (1), 13-31.
Smith, P.C., Westfall, J.M., & Nichols, R.A. (2002). Primary Care Family Physicians and
2 Hospitalist Models: Comparison of Outcomes, Processes, and Costs. Journal of
Family Practice, 51 (12), 1021-1027.
Snow, V., Beck, D., Budnitz, T., Miller, D.C., Potter, J., Wears, R.L., Weiss, K.B., &
Williams, M.V.; American College of Physicians; Society of General Internal
Medicine; Society of Hospital Medicine; American Geriatrics Society; American
College of Emergency Physicians; Society of Academic Emergency Medicine.
(2009). Transitions of Care Consensus Policy Statement American College of
Physicians-Society of General Internal Medicine-Society of Hospital Medicine-
American Geriatrics Society-American College of Emergency Physicians-Society
of Academic Emergency Medicine. Journal of General Internal Medicine, 24 (8):
971-976.
74
Society of Hospital Medicine, University of Texas Medical Branch Researchers (2011).
Hospitalists May Not Produce Higher Medicare Savings, Study Finds. Annals of
Internal Medicine, 1-2.
Society of Hospital Medicine (2011). Hospitalists. Transforming Healthcare.
Revolutionizing Patient Care. Retrieved from www.hospitalmedicine.org
Sox, H.C. (1999). The Hospitalist Model: Perspectives of the Patient, the Internist, and
Internal Medicine. Annals of Internal Medicine, 130 (4), 368-72.
Thibaut, J.W., & Kelley, H.H. (1959). The Social Psychology of Groups. New York, NY:
John Wiley and Sons.
Vasilevskis, E.E., Knebel, R.J., Dudley, R.A., Wachter, R.M., Auerbach, A.D. (2010).
Cross-Sectional Analysis of Hospitalist Prevalence and Quality of Care in
California. Journal of Hospital Medicine, 5 (4), 200-2007.
Wachter, R.M., & Goldman, L. (1996). The Emerging Role of Hospitalists in the
American Health Care System. New England Journal of Medicine, 335 (7), 514-
517.
Wachter, R.M., & Goldman, L. (2002). The Hospitalist Movement 5 Years Later. Journal
of the American Medical Association, 287 (4), 487-494.
Wachter, R.M. (2009). Growth in Care Provided by Hospitalists. New England Journal of
Medicine, 360 (26), 2789-2790.
Wachter, R.M. (2004). Hospitalists in the United States-Mission Accomplished or Work
in Progress?. New England Journal of Medicine, 350 (19), 1935-1936.
Wachter, R.M., & Pantilat, S.Z. (2002). The Continuity Visit and the Hospitalist Model
of Care. Disease-a-Month, 48 (4), 267-272.
Wachter, R.M. (2009). The Hospitalist Model of Care: the Fastest Growing Specialty in
Medical History.
Wachter, R.M. (2006). Reflections: the Hospitalist Movement a Decade Later. Journal
of Hospital Medicine, 1 (4), 248-252.
Wachter, R.M. (2010). The Relationship between Hospitalists and Primary Care
Physicians. Annals of Internal Medicine, 152 (7), 474.
Walraven, C.V., Seth, R., Austin, P., & Laupacis, A. (2002) Effect of Discharge
Summary Availability During Post-discharge Visits on Hospital Readmission.
Journal of General Internal Medicine, 17 (13), 186-192.
75
APPENDIX A
LETTER TO FAFP MEMBERS
Dear FAFP Member:
You are invited to participate in a study entitled “The Relationship between Hospitalists
and Primary Care Physicians" Protocol Number X120115011. This study will investigate
the relationship between family medicine physicians and hospitalists, and is part of the
requirements to complete a Doctor of Science in Administration-Health Services at the
University of Alabama at Birmingham (UAB). You are invited to participate in this study
because you are a physician member of the Florida Academy of Family Physicians
(FAFP). The goal of this study is to provide physicians and healthcare professionals with
additional information on how the evolving connection between hospital-based
physicians and their community-based colleagues has progressed since "Hospital
Medicine" was introduced in the 1990s.
Respondents to this survey will be eligible for a drawing to win one of four prizes given
to completed survey participants. Prizes include two (2) iPad 2s, a one-week stay in a
Tennessee cabin (Laurel Valley in Townsend),or a certificate for a one-week stay at a
Mexico timeshare location at Playa Grande in Cabo San Lucas. Both of the one-week
stays include accommodations so the winner would only have to cover travel and meals.
FAFP will be conducting the drawing for prizes to protect the identity of physician
participants. However, for the two accommodation prizes (Tennessee cabin and Cabo
timeshare) the name of the individual will need to be known for scheduling purposes. The
physician provider number of the individuals winning these four prizes does not need to
be known by the researcher, only their name and contact information so that prizes can be
delivered to them. In addition, all participants in the survey will receive an electronic
copy of the completed study including the aggregate results of the survey questionnaire.
If you agree to voluntarily participate, you will be asked to complete an on-line survey
where you will be asked to respond to 15 questions regarding the demographics of your
practice and the relationship that exists between you and hospitalists in your area. The
survey will also ask you to provide your physician's 'provider number,' but only for
purposes of matching the provider to the patient database (BCBSF) that will be used in
determining patient outcomes. Your response will be sent electronically through the
"survey monkey" tool directly to FAFP. Information gathered in this survey will be
utilized only as grouped or summary information and is being collected by FAFP through
its website on behalf of the doctoral student conducting this study. The survey should
take no longer than 15-20 minutes to complete, and you are free to withdraw from this
study at any time by exiting the survey. There is no compensation or direct benefit for
participation in this study. The number of expected participants in this study is estimated
to be 600.
76
There is a minimal risk of loss of confidentiality associated with this study. However, no
individual data or reports will be formulated or released and your answers will be kept
confidential. The researcher will not have access to specific physician-patient information
and will only be evaluating aggregate data based on two groupings, those with
established hospitalist relationships and those who respond that no such relationship
exists. Your responses are confidential to the extent provided by law; your identity will
not be given out or known.
If you have any questions, concerns, or complaints about the research, please contact me
at:
Jim Burkhart
UAB Doctoral Student
655 West 8th Street
Jacksonville, Fl 32209
Phone number: 904-244-3002
Email address: [email protected] or [email protected]
If you have questions about your rights as a research participant, or concerns or
complaints about the researcher, you may call the Office of Institutional Review Board
(OIRB) at (205) 934-3789 or 1-800-822-8816. If calling the 800 number, press the option
for "all other calls" or for an operator or to speak with an attendant ask for extension 4
3789. Regular hours for the OIRB are 8:00- 5:00 CT Monday through Friday. You may
call this number in the event the researcher cannot be reached or you wish to talk to
someone else.
Thank you for your valuable time and input, it is greatly appreciated.
Sincerely,
James R. Burkhart, BA, MSHHA
Doctoral Student - DSc in Administration-Health Services
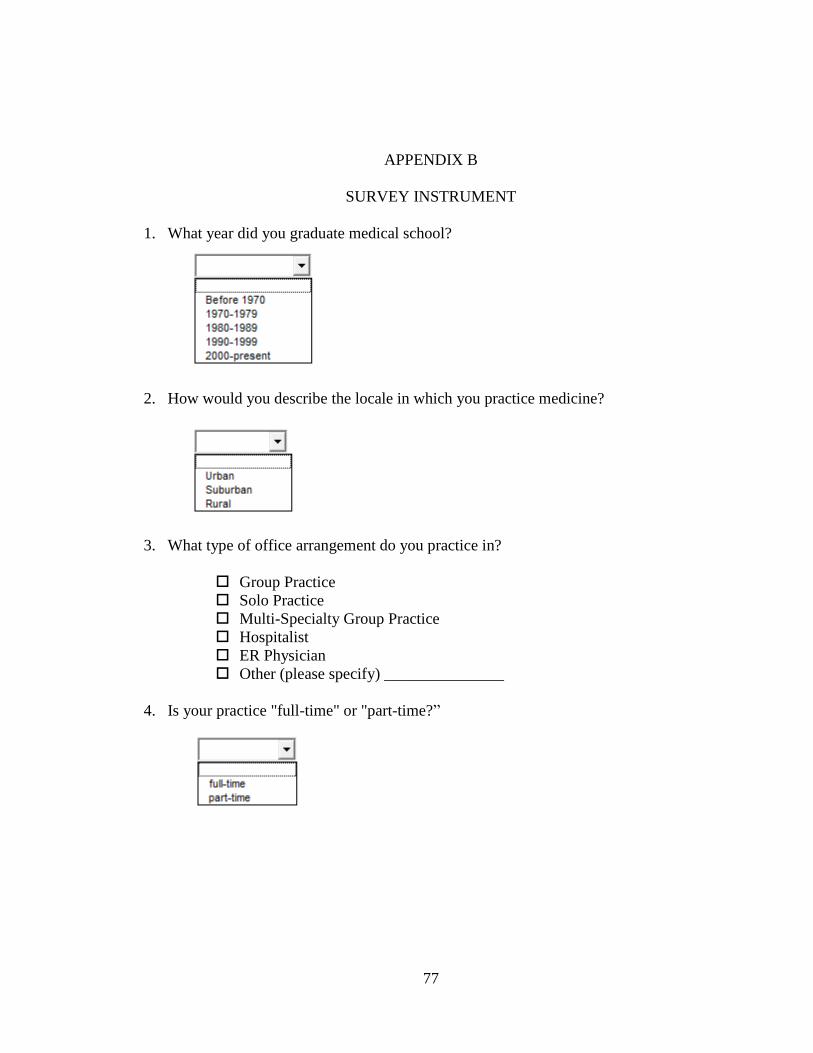
77
APPENDIX B
SURVEY INSTRUMENT
1. What year did you graduate medical school?
2. How would you describe the locale in which you practice medicine?
3. What type of office arrangement do you practice in?
Group Practice
Solo Practice
Multi-Specialty Group Practice
Hospitalist
ER Physician
Other (please specify) _______________
4. Is your practice "full-time" or "part-time?”
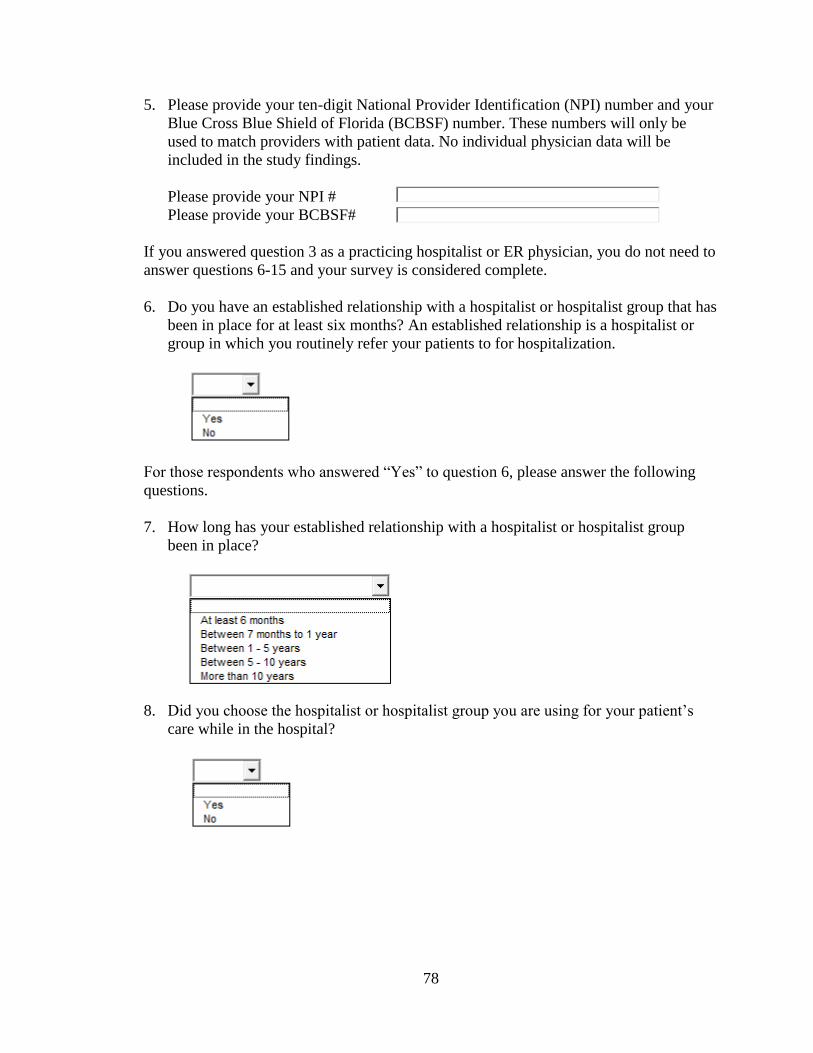
78
5. Please provide your ten-digit National Provider Identification (NPI) number and your
Blue Cross Blue Shield of Florida (BCBSF) number. These numbers will only be
used to match providers with patient data. No individual physician data will be
included in the study findings.
Please provide your NPI #
Please provide your BCBSF#
If you answered question 3 as a practicing hospitalist or ER physician, you do not need to
answer questions 6-15 and your survey is considered complete.
6. Do you have an established relationship with a hospitalist or hospitalist group that has
been in place for at least six months? An established relationship is a hospitalist or
group in which you routinely refer your patients to for hospitalization.
For those respondents who answered “Yes” to question 6, please answer the following
questions.
7. How long has your established relationship with a hospitalist or hospitalist group
been in place?
8. Did you choose the hospitalist or hospitalist group you are using for your patient’s
care while in the hospital?
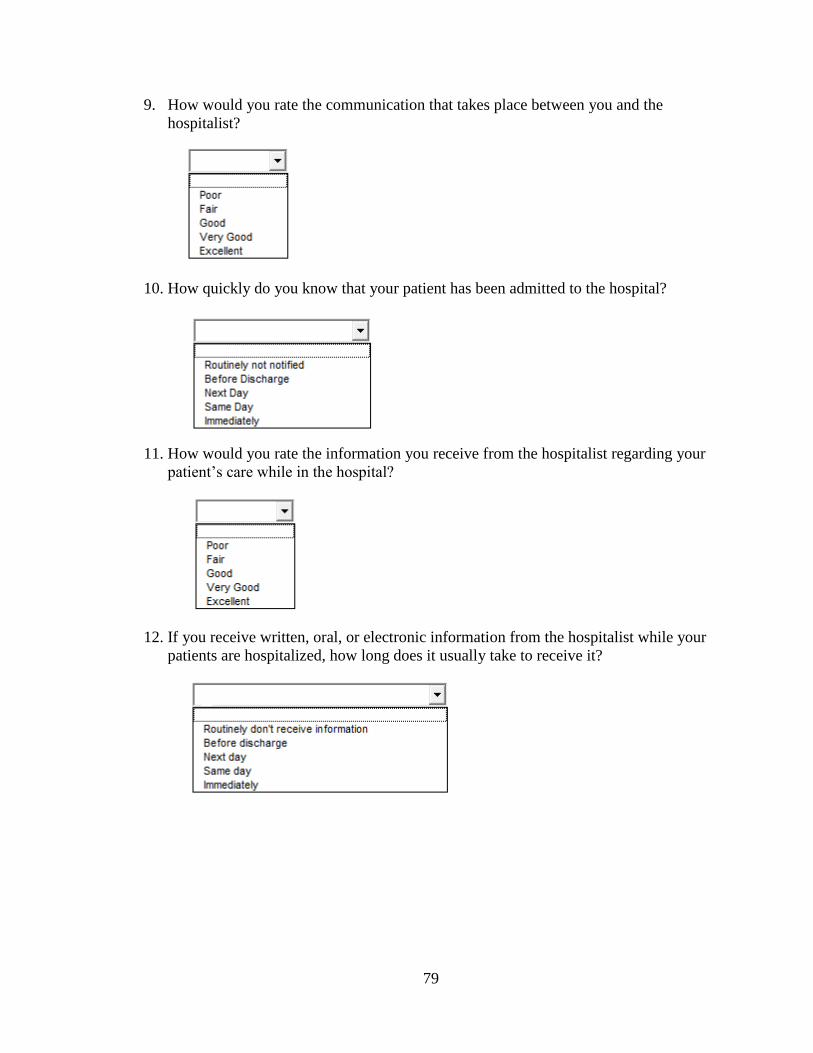
79
9. How would you rate the communication that takes place between you and the
hospitalist?
10. How quickly do you know that your patient has been admitted to the hospital?
11. How would you rate the information you receive from the hospitalist regarding your
patient’s care while in the hospital?
12. If you receive written, oral, or electronic information from the hospitalist while your
patients are hospitalized, how long does it usually take to receive it?
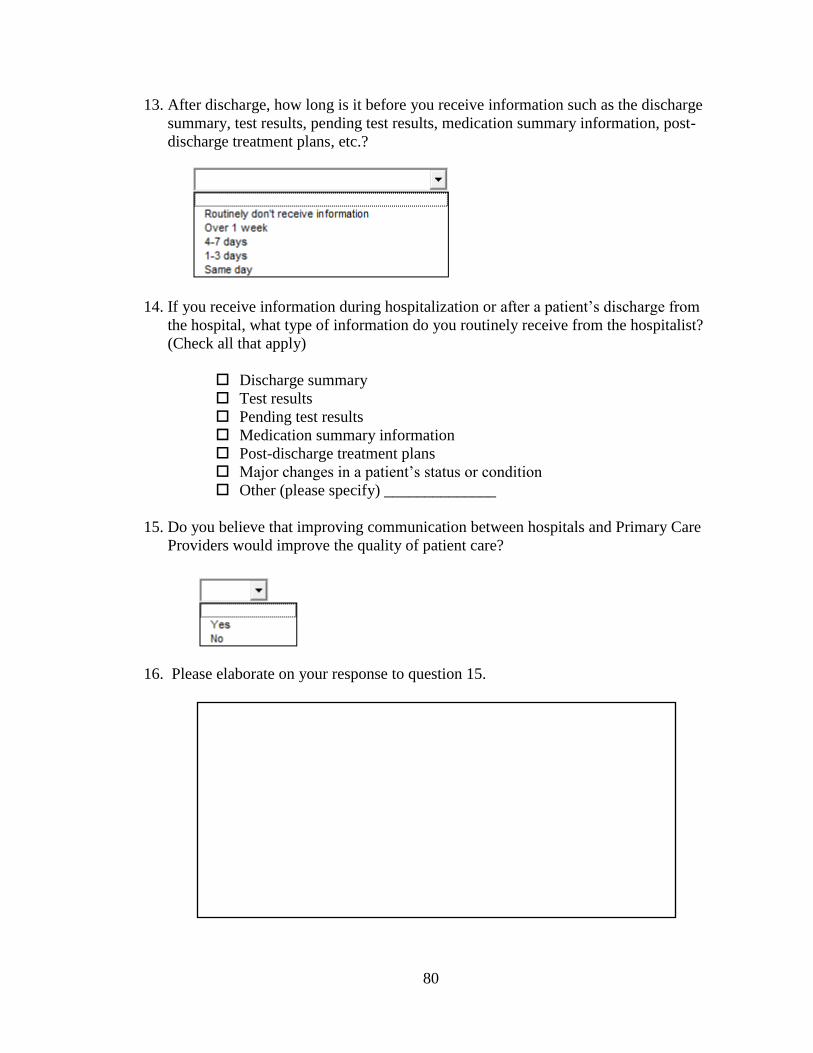
80
13. After discharge, how long is it before you receive information such as the discharge
summary, test results, pending test results, medication summary information, post-
discharge treatment plans, etc.?
14. If you receive information during hospitalization or after a patient’s discharge from
the hospital, what type of information do you routinely receive from the hospitalist?
(Check all that apply)
Discharge summary
Test results
Pending test results
Medication summary information
Post-discharge treatment plans
Major changes in a patient’s status or condition
Other (please specify) ______________
15. Do you believe that improving communication between hospitals and Primary Care
Providers would improve the quality of patient care?
16. Please elaborate on your response to question 15.
81
APPENDIX C
IRB APPROVAL FORM
82
APPENDIX D
IRB APPROVAL LETTER