Embed Size (px)
Citation preview

Journal of Clinical InvestigationVol. 45, No. 4, 1966
Comparative Morphology, Respiration, and PhagocyticFunction of Leukocytes from Blood and Joint Fluid
in Rheumatoid Arthritis *
PHYLLIS T. BODELt ANDJ. W. HOLLINGSWORTH(From the Department of Internal Medicine, Yale University School of Medicine,
NewHaven, Conn.)
Knowledge of leukocyte function in man is de-rived almost entirely from white cells obtainedfrom blood. In animals, however, most experi-mental work on granulocytes has been carried outwith cells from peritoneal exudates produced bya variety of inflammatory stimuli. Alterations inthe metabolism of leukocytes after migration fromthe blood stream to areas of inflammation havebeen described (1-3). Since polymorphonuclearleukocytes characteristically perform their mostimportant function at extravascular sites, studiesof human leukocytes from an inflammatory exu-date would be of interest.
Synovial effusions from patients with rheuma-toid arthritis provide an excellent source for exu-date leukocytes. In this study, leukocytes fromthe blood and joint fluid of patients with rheuma-toid arthritis were compared in vitro with regardto morphology, viability, respiration, and phago-cytic capacity for Staphylococcus aureus.
Methods
All glassware used was sterilized at 160° C for 2hours to inactivate endotoxin. Krebs-Ringer phosphatebuffer, pH 7.4, modified to contain one-fifth the usualconcentrations of CaCls and MgSO4, was sterilized byautoclaving at 15 pounds pressure for 2 hours.
Patients. Studies were performed on blood and jointfluid from 18 patients with rheumatoid arthritis. Diag-nostic criteria of classical or definite rheumatoid arthritisas defined by the American Rheumatism Associationwere used. All patients were ambulatory or under-going short hospitalizations. Therapy at the time of studywas variable. Nine patients had no medication or were
* Submitted for publication June 11, 1965; accepted De-cember 27, 1965.
Supported in part by a grant for arthritis researchfrom the John A. Hartford Foundation and by a grant(AM-07348) from the U. S. Public Health Service.
t Address requests for reprints to Dr. Phyllis T. Bodel,Yale University School of Medicine, 333 Cedar St., NewHaven, Conn.
on aspirin alone. Four were receiving prednisone, 5 to10 mg per day, and the other five were receiving severalmedications, including gold and hydroxychloroquine. Nopatients were suspected of having intercurrent infections,and none were receiving antibiotics.
Preparation of leukocytes. Sterile siliconized syringescontaining 1 to 2 mg of heparin per 10 ml of fluid wereused to collect blood from the antecubital vein and jointfluid from the knee. Shoulder fluid was used in oneexperiment. Joint fluid was filtered through severallayers of sterile gauze to remove fibrin clumps. Theblood was allowed to settle at room temperature for 1 to1 hour to obtain a plasma layer.
For preparation of "whole fluids," the joint fluid orplasma was centrifuged at 5 to 20° C at 1,500 rpm in anInternational no. 2 centrifuge for 15 to 20 minutes. Itwas found that clumping was markedly reduced whencells were processed at 15 to 200 C, and all later ex-periments were done at these temperatures. Some su-pernatant fluid was removed, and the cells were gentlyresuspended to adjust the concentration of polymorpho-nuclear leukocytes to about 3 X 10' per ml. For prepara-tion of washed cells, portions of joint fluid or plasmawere centrifuged as above, the supernatant was removed,and the cells were resuspended in 40 ml of Krebs-Ringerphosphate buffer containing 2 mg heparin per 10 ml. Aftercentrifugation, the cells were resuspended in a small vol-ume of heparinized buffer to maintain the same concen-tration of polymorphonuclear leukocytes as for the wholefluids. Differential counts were performed on all fluids.In plasma preparations, one to five erythrocytes per leu-kocyte and 250,000 to 750,000 platelets per mm' wereusually present. Joint fluids containing more than 5%monocytes were excluded. All transfers of cells, plasma,and joint fluid in each experiment were autologous.
Bacteria. Staphylococcus aureus, phage type 80-81,was used throughout. The characteristics of this strainhave been previously described (4). The culture waskept on a blood agar plate at 2° C and subcultured every3 to 4 weeks. For each experiment an 18-hour growthof this strain in beef heart infusion broth was centrifuged,washed once with saline, and the bacterial cells resus-pended in a constant volume of buffer containing 0.1%bovine serum albumin. This preparation contained con-sistently 1.2 X 10' bacteria per ml.
Incubation. Incubation was carried out in standardWarburg flasks at a temperature of 37.50 C for 2 hours.
580

BLOODANDJOINT FLUID LEUKOCYTESIN RHEUMATOIDARTHRITIS
Manometer joints were wiped with alcohol just beforeuse, and sterile cotton balls were inserted lightly into thejoint. Flasks contained 0.2 ml 15% potassium hydroxidein the center well with a filter paper fan. In the maincompartment was placed 1 ml of the leukocyte suspen-sion containing approximately 3 X 107 leukocytes, eitheras whole fluid or washed cells in buffer, and either 1.6 mlof buffer (when whole fluid was used) or 0.6 ml bufferwith 1 ml of cell-free joint fluid or plasma (when washedcells were used). The cell-free joint fluid and plasmawere prepared by centrifugation at 3,000 rpm at 20 C for20 minutes. The flask sidearm contained 0.2 ml of thesuspension of 80-81 staphylococci (containing about 2 X108 bacteria). After equilibration for 20 minutes, manom-eter readings were taken at 15-minute intervals. Afterabout 1 hour, the contents of the sidearms were added tothe main flask, and incubation with bacteria was carriedout for 1 hour. Control flasks in each experiment includeda thermobarometer and flasks containing cell-free jointfluid or plasma with buffer and staphylococci. To pre-vent clotting of plasma during the 2-hour incubation, atotal of 0.35 mg heparin per ml was found to be neededand was included in all flasks.
Quantitation of phagocytosis. The method of Cohn andMorse (5) was used to enumerate total, supernatant, andcell-associated live bacteria in the flasks at the end ofthe experiment. Samples were centrifuged at 2° C andkept in ice if not plated at once. All samples were ho-mogenized, 100-fold dilutions in saline were made, andpour plates prepared. Staphylococcal colonies on thepour plates were counted after overnight incubation. Ineach experiment, the staphylococcal inoculum, the ther-mobarometer, and the control flasks containing staphylo-cocci with plasma or joint fluid supernatant were counted.Usually the values for supernatant plus cell-associatedstaphylococci equaled 70 to 95% of the value obtainedfrom the sample representing total live staphylococci perflask.
Data. Duplicate flasks were used in as many instancesas possible (half of reported values). Experiments inwhich technical difficulties prevented adequate evaluationof data were excluded. These included incubations inwhich the plasma or joint fluid showed evidence of clot-ting, experiments where results from duplicate flaskswere inconsistent, and experiments where the numbers ofpolymorphonuclear leukocytes in the flask were less than2 X 10 or more than 4.5 X 107. In an occasional ex-periment (3 of the first 20), bactericidal activity of bothplasma and joint fluid was apparent, in that 60 to 95% ofthe bacteria added to the cell-free fluids were killed at theend of the incubation period. These experiments werealso omitted.
Eosin counts. Eosin counts were performed on wholeand washed leukocytes by the method of Hanks and Wal-lace (6). Two hundred white cells were counted in eachdetermination.
Thin preparations for morphology. A sterile slide wasplaced on moist filter paper in a petri dish. A drop ofjoint fluid or plasma was covered with a sterile cover-slip and incubated for 20 minutes at 37°. The coverslip
was gently removed from the slide, quickly dried withcompressed air, and stained with Wright's stain, as de-scribed by Hirsch and Cohn (7).
Antibody assay. Blood and joint fluid antibody titersagainst antigens in 80-81 staphylococcal broth culturefiltrate were determined by a method previously described(8). Washed sheep red cells were incubated with 80-81broth filtrate for 2 hours and then washed and sus-pended in saline. Portions were added to serial twofolddilutions of plasma, serum, or joint fluid that had beenpreviously absorbed with normal sheep cells. Hemag-glutinin titers were read at 24 hours. Plasma or serumand joint fluid supernatants of nine patients were studied.Some fluids had been stored at - 200 C for severalmonths.
Results
Viability and morphology of leukocytes. Leu-kocytes from joint fluid were often more easilydamaged by the isolation procedures than wereplasma leukocytes. Although plasma white cellscould be repeatedly washed in buffer, joint fluidleukocytes frequently disintegrated after severalwashes. In these experiments, therefore, onlyone wash with buffer was carried out routinely.
Examination of Wright's stain preparations in-dicated that among joint fluid leukocytes therewere usually a few cells with pycnotic or highlysubdivided nuclei. These were rarely seen inpreparations of plasma.
Exclusion of eosin dye has been used as a sensi-tive measure of cell viability (6). Eosin countsof leukocytes from blood and joint fluid indicatedno difference in the numbers of viable cells ineach preparation. When the fluids from six pa-tients were examined, there were 1o% eosin-posi-tive cells in joint fluid of three, and less than 17oin the joint fluid from the other three; all plasmaleukocytes were less than 17o positive. After asingle wash, eosin-positive cells in both plasmaand joint fluid preparations varied from 0 to 6%o.
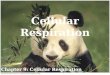
When thin preparations were made, joint fluidpolymorphonuclear leukocytes from many patientswere seen to be strikingly vacuolated and degranu-lated (see Figure 1, B, C, and D). Paired slidesof leukocytes from joint fluid and plasma of rheu-matoid arthritis patients were examined by one ofus with labels obscured. Vacuolization and de-granulation of 50 to 100 consecutive, well-pre-served granulocytes were estimated at 0 to 4 +.An average score was then calculated for eachleukocyte preparation. No plasma preparations
581

PHYLLIS T. BODELAND J. W. HOLLINGSWORTH
had ratings over 1 + (see Figure 1, A), whereas13 of 21 joint fluid preparations showed 2 to 4 +changes. A correlation was noted between thepresence of a positive serum latex or sheep celltiter and morphologic abnormalities of leukocytesfrom joint fluid (see Table I). Six patients inthe series were seronegative, including two withjuvenile rheumatoid arthritis; none had leukocytechanges greater than 2 +. In contrast, 11 of 15seropositive patients showed 3 or 4 + changes.The titer of serum rheumatoid factor also appearedrelated to the degree of cell alteration. All fourseropositive patients showing minimal cell changeshad sheep cell and latex titers less than 160. Incontrast, 9 of 11 seropositive patients with 3 to 4 +changes had one or both of these titers equal to orgreater than 160.
A
Attempts to correlate abnormalities of leukocyteappearance with rates of respiration were not suc-cessful in a small series. Joint fluid leukocyteswith minimal morphologic changes, obtained fromthree patients, had an average respiration of 9 fulper hour, compared to an average of 12 pl perhour for cells that had 2 to 4 + changes, obtainedfrom six patients. Numbers of leukocytes weresimilar in both experimental groups.
On four occasions, washed plasma leukocyteswere added to cell-free joint fluid, incubated for 2to 3 hours, and then examined morphologically.Patients whose joint fluid leukocytes were ex-tensively vacuolated and degranulated were se-lected. In no experiment were significant mor-phologic changes observed in the plasma poly-morphonuclear leukocytes after incubation. Oc-
o. .6.;.
.9 ::: ..< ........ ...
|...... . s N F i.*... !. !||13t
.:
., _
SF.. ..0s.
Be .:.: : ... ......... .. .....:: !:: z n.; " .: luff, . . . . ...... .. . . . , ,: . t :
..: ... .. .. '......:: . ::* : . .'
: . .. ..* . ... .: . : : A. :', .S.. ., . . . ... ..... X a' . ' ' U.: ;:: :.: :. :: ::. :.:;* .: .:. .: : . :.
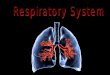
FIG. 1. POLYMORPHONUCLEARLEUKOCYTESFROMPATIENTS WITH RHEUMATOIDARTHRITIS. A)Normal granulocytes from blood. B, C, D) Joint fluid cells showing extensive degranulation(B), partial degranulation with vacuolization (C), and extensive vacuolization with minimaldegranulation (D).
582
W..:t. 11.1

BLOODANDJOINT FLUID LEUKOCYTESIN RHEUMATOIDARTHRITIS
TABLE I
Vacuolization and degranulation of leukocytes from joint fluid
Titer of Degree of morphologic changetNo. of rheumatoid
patients factor* 0 1 + 2 + 3 + 4 +
6 Negative 1 3 26 <160 1 3 29 >1601 4 5
* Sheep cell agglutination and latex fixation titers.t Average of values for 50 to 100 leukocytes per patient (see text).I Titers of one or both tests equaled or exceeded 160.
casionally a granulocyte contained one or two largevacuoles; this occurred after incubation in bothplasma and joint fluid. No increase in respirationof leukocytes from plasma was ever observed dur-ing incubation in joint fluid.
Respiration. Respiration of leukocyte prepara-tions from joint fluid was strikingly lower thanthat of plasma leukocyte preparations from thesame patient, as shown in Table II. Data fromsix consecutive patients are presented. Althoughnumbers of polymorphonuclear leukocytes wereapproximately equal in both media, the respirationof cells in whole joint fluid was less than halfthat of cells in whole plasma. Results obtainedby others indicate that platelets (9) and red cells(10), which were also present in plasma prepara-tions, are not responsible for this difference. Twoexperiments in which 5 x 108 to 1 X 109 plateletswere incubated in our system corroborated this;the respiration was too low to measure.
This difference in respiration of leukocytes fromjoint fluid and plasma was also observed when the
TABLE II
Respiration of leukocyte preparations from plasma andjoint fluid
Joint fluid Plasma
Patient PMN* 02 uptaket PMN* 02 uptaket
gJ/hour/ A4/hour/flask flask
Q 4.5 10 3.0 27B 3.5 4 3.5 20K 3.8 13 4.0 26R 3.0 7 3.0 200 5.0 11 3.0 29S 3.0 18 3.2 30
Mean 3.8 10.5 :2.01 3.3 25.3-+1.8p <0.01
* Total polymorphonuclear leukocytes per flask X 107.t Average of duplicate or triplicate flasks. Flasks contained in the
main compartment 1.0 ml plasma or joint fluid and 1.6 ml Krebs-Ringer phosphate buffer.
t Standard error of mean.
TABLE III
Respiration of washed leukocytes
Leukocyte No. of Suspendingsource patients medium PMN* 02 uptaket
id/hour/flask
Joint fluid (7) 6 Plasma 2.8 10.941.8§Plasma (7) 7 Joint fluid 2.0 23.742.4
p <0.01
* Average polymorphonuclear leukocytes per flask X 107.tAverage of duplicate flasks. Flasks contained in the main com-
partment 1.6 ml Krebs-Ringer phosphate buffer, washed leukocytes,and 1.0 ml plasma or joint fluid supernatant.,
t Figures in parentheses indicate number of experiments.Standard error of mean.
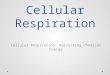
cells were washed and suspended in the oppositefluid from the same patient (see Table III). Av-erage values for respiration of joint fluid leuko-cytes incubated in plasma are less than half thosefor plasma leukocytes incubated in joint fluid.Also, in nearly all experiments, the respiration ofleukocytes from the same source was nearly identi-cal regardless of the suspending medium, as illus-trated in the first part of the curve in Figure 2.
When staphylococci were added from the side-arm, both joint fluid and plasma leukocytes showedan increase in oxygen consumption with phago-cytosis (see Figure 2). This increase appearedsimilar in most experiments. However, the ex-
70?
60.
d 50
k 40
4 30I.-
of 200
10l
0
PL CELLS (in JF )
PL CELLS (in PL)
JF CELLS (in PL)JF CELLS (in JF)
*STAPHYLOCOCCI
I /li a/^ rSTAPHYLOCOCCI
.-,
-40 -20 0 20 40 60
TIME (minutes)
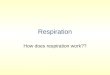
FIG. 2. RESPIRATION OF CELLS FROMJOINT FLUID (JF)AND PLASMA (PL) OF A PATIENT WITH RHEUMATOID
ARTHRITIS. Flasks contained 3.0 to 4.5 X 107 polymorpho-nuclear leukocytes suspended in 1.0 ml plasma or jointfluid cell-free supernatant, plus 1.6 ml Krebs-Ringer phos-phate buffer in the main chamber and 0.2 ml- 15% KOHin the center well. Live staphylococci (2.0 X 10k) were
tipped into the main chamber at zero time. In twoflasks, the staphylococci were added to 1.6 ml buffer and1.0 ml cell-free plasma or joint fluid. The lines repre-
sent averages of duplicate flasks.
583
F

PHYLLIS T. BODELAND J. W. HOLLINGSWORTH
act increment in oxygen consumption of the leuko-cytes alone could not usually be determined, since
the oxygen uptake of staphylococci in cell-freeplasma or joint fluid was frequently about 20 IMIper hour. In three similar experiments, however,in which the respiration of the bacteria was neg-
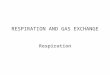
ligible (less than 7 A4 of oxygen per hour), theaverage increase in oxygen consumption of jointfluid was 27 1.l per hour, compared to an increaseof 34 pl for preparations of blood leukocytes.Furthermore, in one experiment (Figure 3),heat-killed staphylococci were added to flaskscontaining whole plasma or whole joint fluid in a
ratio of about 10 bacteria per leukocyte. In-creased respiration occurred in all flasks contain-ing cells after bacteria were added, although theresponse in the joint fluid flasks was delayed.After 20 minutes, the respiration of both leuko-cyte preparations was similar for the remainder ofthe experiment (29 Al for joint fluid compared to36. pl for plasma).
Phagocytosis. When 80-81 staphylococci were
added to whole joint fluid or whole plasma con-
taining similar numbers of granulocytes, less phag-ocytosis appeared to take place in joint fluid (seeTable IV). More live staphylococci were presentin the supernatants of the joint fluid flasks, as wellas more total live bacteria per flask. These val-ues appear to reflect diminished phagocytosis ofbacteria by the leukocytes in whole joint fluidcompared with the leukocytes in whole plasma.'
1 There was frequently some bactericidal activity insamples of cell-free plasma and joint fluid. Althoughthis activity was on the average greater in plasma, it didnot appear to explain the consistently greater loss of
60
50
;403z30
20
PLASMA
,xo JOINT F LUID
STAPHYLOCOCCI P C- {(AHEAT-KILLED}/IoED
-60-40-20020400STAPHYLOCOCCf-(HEAT-KILL ED)
-60 -40 -20 0 20 40 6o so IOU Izo
TIME (minutes)
FIG. 3. RESPIRATION OF JOINT FLUID AND PLASMA
PREPARATIONSFROMA PATIENT WITH RHEUMATOIDARTH-
RITIS. Flasks contained plasma or joint fluid with 3.2 to3.5 X 107 polymorphonuclear leukocytes, 1.6 ml Krebs-Ringer phosphate buffer, and 0.2 ml 15% KOH in thecenter well. About 3 X 108 heat-killed staphylococciwere tipped into the main flask at zero time. In twoflasks, heat-killed bacteria were added to 1.6 ml bufferand 1.0 ml cell-free joint fluid or plasma. Values forrespiration represent averages of triplicate flasks of cellpreparations and duplicate flasks of bacteria.
There was no significant difference in the num-
bers of cell-associated live bacteria. This findingsuggests that the intracellular destruction of in-gested bacteria proceeded similarly in both typesof leukocytes.
It was clearly of interest to determine whetherthe diminished phagocytosis in joint fluid was dueto differences in the leukocytes or the cell-freefluid or both. To investigate the role of the in-cubation medium, we washed leukocytes from
bacteria from the supernatants of flasks containing plasmawith white cells. Thus, in four experiments from TableIV in which cell-free joint fluid had equal or greater bac-tericidal activity than plasma, measurements of phago-cytosis in plasma all exceeded those in joint fluid.
TABLE IV
Phagocytosis of staphylococci by leukocytes from joint fluid and plasma
No. of Live staph after phagocytosistNo. of staph Live staph in
Leukocyte source patients PMN* addedt Total Supernatant Cell-associated control flaskt
Whole joint fluid (9)§ 8 3.3 20.3 9.5 4.2 3.9 22.742.011 ±1.3 40.73 4±0.26
Whole plasma (8) 6 2.8 20.0 4.3 0.70 3.1 17.0±0.81 ±0.09 ±t0.78 ±0.06
p <0.05 p <0.05 p <0.2
* Average polymorphonuclear leukocytes per flask X 107.t Average per flask X 107.t Control flask contains buffered cell-free fluid and staphylococci.
Figures in parentheses indicate number of experiments.Standard error of mean.
584
,,,,lxy
so
0

BLOODANDJOINT FLUID LEUKOCYTESIN RHEUMATOIDARTHRITIS
TABLE V
Efect of incubation medium on phagocytosis by leukocytes from joint fluid and plasma
No. of Live staph in supernatant after phagocytosistNo. of staph
Leukocyte source patients PMN* addedt Joint fluid medium Plasma medium
Joint fluid (10)t 8 3.2 20.4 3.01 41 0.47§ 0.84 i 0.19 p < 0.01Plasma (9) 6 2.3 20.8 2.38 i 0.56 0.73 i 0.15 p < 0.02
Medium 20.6 23.4 4 0.17 17.8 t 0.12 p < 0.05alone (13) (14)
* Average polymorphonuclear leukocytes per flask X 107.t Average per flask X 107.I Figures in parentheses indicate number of experiments.§ Standard error of mean.
either joint fluid or plasma once, resuspendedthem in buffer, and incubated them in autologouscell-free plasma and joint fluid. Since sufficientnumbers of leukocytes from both sources were notalways available in each patient, two groups ofexperiments are presented in Table V. The upper
half of the Table shows the effect of the incubationmedium on phagocytosis of staphylococci by leuko-cytes from joint fluid of eight patients; the lowerhalf is a comparable experiment with plasma leu-kocytes from a different group of six patients.Plasma medium permitted more phagocytosis byboth joint fluid and plasma leukocytes than did thejoint fluid medium, as determined by the numbersof live bacteria remaining in the flask supernatantfluid after incubation. The bactericidal activityof cell-free plasma in these experiments is similarto that which has been described previously (seefootnote 1). It appears, then, that leukocytes fromeither joint fluid or plasma are capable of greaterphagocytosis in plasma than in joint fluid.
The decrease in phagocytic capacity of wholejoint fluid compared to whole plasma (shown inTable IV) appears, then, to be largely explained
by differences between joint fluid and plasma me-
dia (shown in Table V). However, there was
considerable variation in phagocytic activity ofcells from the different patients included in theexperiments in Table V. Because of this varia-tion, it was possible that a subtle difference inphagocytic ability of cells from joint fluid andblood of any single patient might have been over-
looked. To investigate this possibility, we obtainedcells from both plasma and joint fluid from thesame patient, washed them once, and incubatedsamples of cells from each source with either cell-free joint fluid or plasma from that patient.These experiments are presented in Table VI.When incubated in joint fluid, plasma leukocytesshowed a somewhat greater phagocytic capacity(p = < 0.05) than did joint fluid cells from thesame patient (see upper half of Table VI). Leu-kocyte preparations from both sources, however,when incubated in plasma showed similar phago-cytic ability (see lower half of Table. VI). Inthese experiments, then, little evidence was ob-tained for a difference in phagocytic capacity ofcells from blood and joint fluid.
TABLE VI
Effect of leukocyte source on phagocytosis in joint fluid and plasma
Live staph in supernatant*No. of Staph
Medium patients added* Medium alone Plasma leukocytes Joint fluid leukocytes
Joint fluid (8)t 8 21.8 24.7 :+ 0.06 2.15 d 0.73t 5.15 ± 1.30 p < 0.05(2.6)§ (2.8)§
Plasma (6) 5 19.8 17.8 d 0.06 0.49 1 0.01 0.54 + 0.01(2.4)§ (2.6)§
* Average per flask X 107.t Figures in parentheses indicate number of experiments.t Standard error of mean.§ Average polymorphonuclear leukocytes per flask -X 107.
585

PHYLLIS T. BODELAND J. W. HOLLINGSWORTH
broth filtrate antigens
Plasma orPatient Joint fluid serum
O's 64 128K 128 128H 4 8R 8 16T 16 320 16 32D 8 8S 32 64B 64 64
* Reciprocal of highest dilution with 1 + hemagglutinin.
Antibody studies. Since phagocytosis of somestrains of Staphylococcus aureus is enhanced bythe presence of strain-specific antibody (5), a de-termination was made of antibody titers in cell-free plasma and joint fluid to antigens present in80-81 staphylococcal broth culture filtrate. Theparticular antigens that normal sheep cells adsorband to which antibody titers were determined havenot been clearly defined, but they probably in-clude an antigen common to several gram-positiveorganisms (11), as well as an antigen specific tothe staphylococcus (12). Plasma and joint fluidsupernatants of nine patients were studied. Anti-body titers are given in Table VII. Although inmost cases joint fluid antibody levels were slightlylower than those in plasma, antibody against anti-gens present in 80-81 staphylococcal filtrate wasdemonstrated in both fluids. Several reports haveindicated that the protein content of rheumatoid ar-thritis joint fluid is similar to that of serum, withan equal or slightly lower gamma globulin con-tent (13, 14). These observations make it un-likely that differences in antibody levels of serumand joint fluid are responsible for the observeddifferences in phagocytosis.
Discussion
The morphological differences between the jointfluid and plasma polymorphonuclear leukocytesobserved in these studies included, in many pa-tients, large numbers of joint fluid leukocytes thatwere vacuolated and extensively degranulated.These cells were viable as measured by the abilityof their membranes to exclude a vital dye. In al-most all instances, joint fluid cells respired at alower rate than did similar preparations of plasma
leukocytes. The suspending medium clearly didnot influence the respiration, and the presence ofother blood elements in the plasma preparationsdoes not explain the difference. Platelets sus-pended in heparinized plasma have been found tohave no measurable oxygen consumption (9).The red cells in our preparations (1 to 20 X 107)are insufficient for measurable respiration (10).
The extent of morphologic changes in joint fluidcells in these few studies did not correlate withthe absolute values of oxygen consumption. Thisfinding suggests that low respiration may be acharacteristic of exudate granulocytes in thesepatients. Differences in lactate production be-tween guinea pig circulating and exudate leuko-cytes have been described (1, 3); respiration wasnot measured. It has been suggested (15) that adecrease in oxidative metabolism is the earliestdefect observed in aging or damaged polymorpho-nuclear leukocytes. Since more than 90% of thenormal leukocyte's energy is derived from gly-colysis (16), a defect in oxidative metabolism maybe relatively unimportant to cell function. In ourexperiments, most joint fluid cells appeared tohave a normal increase in respiration after phago-cytosis. In other granulocytes this increase oc-curs primarily by way of the hexose monophos-phate pathway (17), and is not dependent on thecytochrome system.
Phagocytosis is generally considered a usefulindicator of granulocyte function. However, vari-ous factors in the suspending medium influence therate at which cells phagocytize particles (18). Thephagocytic capacity of both joint fluid and bloodleukocytes for staphylococci was less when thesecells were suspended in joint fluid than when theywere suspended in plasma. Several factors mightbe implicated to explain this finding. Levels ofcomplement in most joint fluids are lower thanthose in serum (19). In rheumatoid arthritis,elevated serum levels and depressed joint fluidlevels, compared to normal, have been reported(19, 20). Since complement probably enhancesphagocytosis of staphylococci (5, 21), this differ-ence in complement activity may be an importantfactor. Staphylococcal antibody titers were notsubstantially different in the two media. Altera-tions of the surface properties of leukocytes andbacteria influence phagocytosis (22). Joint fluidcomponents such as hyaluronic acid might impede
Titer* of antibody to
TABLE VII
staphylococcal
586

BLOODANDJOINT FLUID LEUKOCYTESIN RHEUMATOIDARTHRITIS
phagocytosis by interfering with cell-particle as-
sociation. However, in one experiment, treat-ment of joint fluid with hyaluronidase did notchange the phagocytic capacity of the fluid. Fur-thermore, since phagocytosis does not requireexogenous glucose (17), the low levels of glucosepresent in rheumatoid arthritis effusion (13) donot appear to play a role.
The half-life for granulocytes in effusions ofrheumatoid arthritis has been calculated to be lessthan 6 hours (23). New cells are, therefore, con-
tinually entering the joint fluid, either directlyfrom the blood stream or from tissue spaces.
However, the observations that joint cells hadoccasional pycnotic nuclei and low respiration sug-
gest that these cells, though viable and metaboli-cally active, may be an older population than cellsobtained from blood. Since the mature polymor-phonuclear leukocyte is present in the blood foronly a few hours (24), these alterations must de-velop while the cell resides in extravascular sites.
Ingested aggregates of 19 S and 7 S gamma
globulin in joint fluid granulocytes, probably rep-
resenting antigen-antibody complexes, have beenreported by Hollander, McCarty, Astorga, andCastro-Murillo and confirmed by Astorga andBollet (25, 26). This phenomenon appears to oc-
cur in most rheumatoid arthritis patients, even
if rheumatoid factor cannot be demonstrated inthe blood. In our series, good correlation was ob-served between the presence of vacuolization anddegranulation and the presence of serum rheuma-toid factor as measured by sheep cell and latexagglutination titers. However, when suspendedin plasma, these markedly abnormal granulocytesseemed to have a normal phagocytic capacity forstaphylococci. Only when suspended in the lesseffective joint fluid media was a slight deficiencydetectable in phagocytic activity of granulocytesfrom joint fluid, as compared with those fromblood. Since materials from the original suspend-ing medium probably remain fixed to the cellsafter a single washing, this small difference may
not represent a true alteration in cell function.The ingestion of antigen-antibody complexes
in vitro by human blood leukocytes is accompaniedby increased oxygen consumption (27). Whenblood leukocytes from patients with rheumatoidarthritis were washed and suspended in joint fluid,however, the respiration of these cells was not al-
tered. Furthermore, joint fluid cells with morpho-logic changes presumably related to phagocytosisof globulin aggregates did not have a greater res-piration than did cells without such changes.Finally, incubation of plasma leukocytes for 2 or3 hours in joint fluid from patients with sero-positive arthritis and markedly altered joint fluidcells failed to produce morphologic or respiratorychanges in the blood cells.
These experiments make it unlikely that thesequence of events postulated by Hollander andco-workers-phagocytosis of aggregates, degranu-lation, and release of inflammatory materials-oc-curs in the joint fluid itself. The same sequencemight well occur in the synovial tissue, whererheumatoid factor has been demonstrated by im-munofluorescent methods (28). In one criticalexperiment by Restifo and associates (29), thedata seem best fitted to an immunologic event inthe synovium rather than in the joint cavity.These investigators injected autologous gammaglobulin into the knee joints of patients with rheu-matoid arthritis and observed an immediate inflam-matory response. However, the characteristicgranulocyte inclusions containing 19 S and 7 Sglobulin complexes were not detected in the jointfluid cells until 24 hours later, when the inflam-matory reaction actually was subsiding. It is ofcourse possible that other cells in the synoviumreact to antigen-antibody complexes and take partin the inflammatory response (30). Evidencethat might implicate cells other than those in thejoint fluid is our observation that several patientswith clinically severe arthritis consistently havenormally granulated exudate cells.
Polymorphonuclear leukocytes are important inthe early defense against staphylococcal disease, ashas been shown experimentally in dermal (31),peritoneal (32), and intravenous infections (33).In synovial effusions, particularly in rheumatoidarthritis, the granulocytes are already in the jointfluid and should be capable of rapidly destroyinginvading staphylococci. However, several clini-cal reports suggest that inflamed joints are quitefrequently a site of secondary staphylococcal in-vasion (34-36). The observation that joint fluidfrom patients with rheumatoid arthritis is an un-favorable medium for staphylococcal phagocytosismay in part explain this apparently paradoxicalsituation.
587

PHYLLIS T. BODELAND J. W. HOLLINGSWORTH
SummaryLeukocytes from blood and joint fluid of 18 pa-
tients with rheumatoid arthritis were comparedin vitro with regard to morphology, viability, res-piration, and phagocytic capacity for Staphylococ-cus aureus.
Joint fluid granulocytes were frequently vacuo-lated and degranulated, especially those obtainedfrom patients with demonstrable serum rheumatoidfactor. Respiration of joint fluid leukocytes wasless than half that of plasma leukocytes, regard-less of the medium in which the cells were incu-bated. These changes in respiration were notcorrelated with the degree of morphologic changein the joint fluid granulocytes.
Phagocytosis of staphylococci during 1 hour inwhole joint fluid was less than that in wholeplasma. When 'washed leukocytes from eithersource were incubated in cell-free joint fluid andplasma, less phagocytosis occurred in joint fluidmedium. Moreover, when suspended in jointfluid, washed joint fluid leukocytes appeared to beless active phagocytes than were plasma leuko-cytes. This difference in function was not de-tected, however, when the cells were suspended inplasma.
These observations suggest that differences be-tween the joint fluid and plasma media are pri-marily responsible for decreased phagocytosis ofbacteria by leukocytes in joint fluid. Inefficientphagocytosis of staphylococci in synovial exudatemay be a factor in the reported susceptibility ofdiseased joints to bacterial infection.
AcknowledgmentWewould like to thank Dr. Elisha Atkins for his help-
ful criticisms and Marcia Abdalla for technical assistance.
References1. Hartman, J. D., and M. Reidenberg. Comparison
of the glycolytic activity of blood and exudateleucocytes. J. appl. Physiol. 1958, 12, 477.
2. Berlin, R. D., and W. B. Wood, Jr. Molecularmechanisms involved in the release of pyrogenfrom polymorphonuclear leucocytes. Trans. Ass.Amer. Phycns 1962, 75, 190.
3. Antonioli, J. A. Metabolism of the white blood cellinside and outside the blood stream in BiologicalActivity of the Leucocyte, Ciba Foundation StudyGroup No. 10, G. E. W. Wolstenholme and M.O'Connor, Eds. London, J. & A. Churchill, 1961,p. 92.
4. Atkins, E., and L. R. Freedman. Studies in staphylo-coccal fever. I. Responses to bacterial cells. YaleJ. Biol. Med. 1963, 35, 451.
5. Cohn, Z. A., and S. J. Morse. Interactions betweenrabbit polymorphonuclear leucocytes and staphylo-cocci. J. exp. Med. 1959, 110, 419.
6. Hanks, J. H., and J. H. Wallace. Determination ofcell viability. Proc. Soc. exp. Biol. (N. Y.) 1958,98, 188.
7. Hirsch, J. G., and Z. A. Cohn. Degranulation ofpolymorphonuclear leucocytes following phago-cytosis of microorganisms. J. exp. Med. 1960, 112,1005.
8. Bodel, P. T., and E. Atkins. Studies in staphylococ-cal fever. IV. Hypersensitivity to culture filtrates.Yale J. Biol. Med. 1964, 37, 130.
9. Campbell, E. W., W. J. Small, and W. Dameshek.Metabolic activity of human blood platelets. J.Lab. clin. Med. 1956, 47, 835.
10. Angelone, L., D. H. Watkins, and C. A. Angerer.Oxygen consumption of erythrocytes from patientswith various thyroid conditions related to theirrespective serum protein-bound iodine concentra-tions. Blood 1954, 9, 953.
11. Grov, A., B. Myklestad, and P. Oeding. Immuno-chemical studies on antigen preparations fromStaphylococcus aureus. I. Isolation and chemicalcharacterization of antigen A. Acta path. micro-biol. scand. 1964, 61, 588.
12. Bodel, P. T., and E. Atkins. Studies in staphylo-coccal fever. V. Staphylococcal filtrate pyrogen.Yale J. Biol. Med. 1965, 38, 282.
13. Ropes, M. W., and W. Bauer. Synovial FluidChanges in Joint Disease. Cambridge, HarvardUniversity Press, 1953, pp. 18-77.
14. Wilkinson, M., and B. S. Jones. Serum and synovialfluid proteins in arthritis. Ann. rheum. Dis. 1962,21, 51.
15. Tullis, J. L. The origin, properties, function andpreservation of white blood cells in Blood Cellsand Plasma Proteins, J. L. Tullis, Ed. New York,Academic Press, 1953, p. 276.
16. Beck, W. S., and W. N. Valentine. The aerobiccarbohydrate metabolism of leucocytes in healthand leukemia. I. Glycolysis and respiration. Can-cer Res. 1952, 12, 818.
17. Karnovsky, M. L. Metabolic basis of phagocytic ac-tivity. Physiol. Rev. 1962, 42, 143.
18. Florey, H. W. Chemotaxis, phagocytosis and theformation of abscesses in General Pathology, H.Florey, Ed. Philadelphia, W. B. Saunders, 1962,p. 98.
19. Pekin, T. J., and N. J. Zvaifler. Hemolytic com-plement in synovial fluid. J. clin. Invest. 1964,43, 1372.
20. Fostiropoulos, G., K. F. Austen, and K. J. Bloch.Total hemolytic complement (CH,0) and secondcomponent of complement (C'2hu) activity in se-rum and synovial fluid. Arthr. and Rheum. 1965,8, 219.
588

BLOODANDJOINT FLUID LEUKOCYTESIN RHEUMATOIDARTHRITIS
21. Austen, K. F., and Z. A. Cohn. Contribution of se-rum and cellular factors in host defense reactions.I. Serum factors in host resistance. New Engl. J.Med. 1963, 268, 994.
22. Mudd, S., M. McCutcheon, and B. Lucke. Phago-cytosis. Physiol. Rev. 1934, 14, 210.
23. Bertino, J. R., J. W. Hollingsworth, and A. R.Cashmore. Granulocyte kinetics in rheumatoideffusions studied by a biochemical label. Trans.Ass. Amer. Phycns 1963, 76, 63.
24. Craddock, C. G. The production, utilization, anddestruction of white blood cells in Progress inHematology. New York, Grune & Stratton, 1962,vol. 3, p. 92.
25. Hollander, J. L., D. J. McCarty, Jr., G. Astorga, andE. Castro-Murillo. Studies on the pathogenesis ofrheumatoid joint inflammation. I. The "R.A. cell"and a working hypothesis. Ann. intern. Med. 1965,62, 271.
26. Astorga, G., and A. J. Bollet. Diagnostic specificityand possible pathogenetic significance of inclusionsin synovial leucocytes. Arthr. and Rheum. 1965,8, 511.
27. Strauss, B. S., and C. A. Stetson, Jr. Studies on theeffect of certain macromolecular substances on therespiratory activity of the leukocytes of peripheralblood. J. exp. Med. 1960, 112, 653.
28. Mellors, R. C., R. Heimer, J. Corcos, and L. Korn-gold. Cellular origin of rheumatoid factor. J.exp. Med. 1959, 110, 875.
29. Restifo, R. A., A. J. Lussier, A. J. Rawson, J. H.
Rockey, and J. L. Hollander. Studies on the patho-genesis of rheumatoid joint inflammation. III.The experimental production of arthritis by theintra-articular injection of purified 7S gammaglobulin. Ann. intern. Med. 1965, 62, 285.
30. Waksman, B. H. The toxic effects of the antigen-antibody reaction on the cells of hypersensitive re-actors in Cellular and Humoral Aspects of theHypersensitive States, H. S. Lawrence, Ed. NewYork, Hoeber-Harper, 1959, p. 123.
31. Miles, A. A., and J. S. F. Niven. The enhancementof infection during shock produced by bacterialtoxins and other agents. Brit. J. exp. Path. 1950,31, 73.
32. Cohn, Z. A. Determinants of infection in the peri-toneal cavity. II. Factors influencing the fate ofstaphylococcus aureus in the mouse. Yale J. Biol.Med. 1962, 35, 29.
33. Rogers, D. E. Studies on bacteriemia. I. Mecha-nisms relating to the persistence of bacteriemia inrabbits following the intravenous injection ofstaphylococci. J. exp. Med. 1956, 103, 713.
34. Kellgren, J. H., J. Ball, R. W. Fairbrother, andK. L. Barnes. Suppurative arthritis complicatingrheumatoid arthritis. Brit. med. J. 1958, 1, 1193.
35. Rosin, A. J., and A. Goldberg. Infective complica-tions of rheumatoid arthritis. Scot. med. J. 1962,7, 296.
36. De Andrade, J. R., and C. R. Tribe. Staphylococ-cal septicaemia with pyoarthrosis in rheumatoidarthritis. Brit. med. J. 1962, 1, 1516.
589