-
Continuous TherapyFor Management of RRMM
(continuous versus fixed duration)
Pr Jean Luc HarousseauInstitut de Cancérologie de l’Ouest
France
-
Initially
This should have been a debate between
Paul Richardson (Continuous
therapy) and me (Fixed duration)
-
Initially
This should have been a debate between
Paul Richardson (Continuous
therapy) and me (Fixed duration)
« what can I say ? »
-
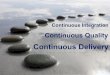
Multiple Myeloma: Patient Outcomes in Real‐World PracticeTreatment Duration and Treatment‐Free Interval by Line of Therapy*
*Data from 4997 patient charts in Belgium, France, Germany, Italy, Spain, Switzerland, and the UK. The proportion of patients who had received each line are from the cross‐sectional review; data on durations of treatment and treatment‐free intervals are from the retrospective review.1L‐5L = first line‐fifth line treatment; CI = confidence interval; m = month.Yong K, et al. Br J Haematol. 2016;175:252‐264.
End5L
Proportion of patients reachingthis line of therapy (%)
3 m 5 m
1 m 4 m
Treatment‐free interval
Median duration in months shown100%
Diagnosis
95%1L
Mean (95% CI): diagnosis, 2 m (1.60, 2.40); 1L, 8 m (7.74, 8.26); 1L maintenance, 9 m (7.78, 10.22)
1 m 6 m6 m
End 1Linduction
Start1L
End 1Lmaintenance
61%2L
Mean (95% CI): interval, 1L‐2L, 16 m (15.0, 17.0); 2L, 9 m (8.64, 9.36)
10 m 7 m
End2L
Start2L
38%3L
Mean (95% CI): interval, 2L‐3L, 11 m (10.22, 11.78); 3L, 8 m (7.63, 8.37)
5 m 6 m
End3L
Start3L
15%4L
Mean (95% CI): interval, 3L‐4L, 7 m (5.9, 8.1); 4L, 6 m (5.5, 6.5)
End4L
Start4L
1%5L
Mean (95% CI): interval, 4L‐5L, 3 m (1.8, 4.2); 5L, 4 m (3.15, 4.85)Start5L
Active treatmentMaintenance treatment
-
Continuous vs Fixed Duration therapyin RRMM
The question is not relevant in laterelapses (>3prior lines
of treatments)
Median PFS are usually
-
Continuous vs fixed durationtherapy in RRMM
Earlier relapses (1 to 3 previous lines of treatment)
-
Double combinations
Median PFS or TTP was short
APEX (VD): 6.2m MM09‐MM10 (LD): 13.4 m
MM03 and Stratus : 4m and 4.6 m (heavilypretreated
patients)
Richardson NEJM 2005;16:2487 Dimopoulos Leukemia 2009;23:2147
San Miguel Lancet Oncol 2013;14:1055 Dimopoulos Blood
2016;128:497
-
Continuous vs Fixed durationThe question is
usually irrelevant with BTZ‐based combinations
Since the maximum number of B cycles is
8
Treatment Plannedduration
Maitenance Effective duration
Median TTFor PFS
APEX VD vs D 8 cycles NO 8
cycles in only 29% pts
7m
ENDEAVOR K56D vs VD Untilprogression or SAE
NO Median 39.9w vs 16.8 w
18.7 m vs 9.4 m
PANORAMA 1 Pan VD vs Plac VD
8cycles 4 cycles in both groups
Median 6m vs 6.6 m
12 m vs 8.2 m
CASTOR DaraVD vs VD
8 cycles Dara
onlyUntilprogression or SAE
57% received
8 cycles VD vs 79% DVD
NR vs 7.2
-
Continuous therapyLenalidomide‐based combinationsTreatment
Planned
duration Maintenance Effective
duration Median PFS (m)
ASPIRE K27d vs Rd 18 cycles Rd in botharms
Median 88 w vs 57 w
26.3 vs 17.6
TOURMALINE1 IRd vs Rd Untilprogression or SAE
Mediannumber of cycles 17 vs 15 (48%vs 43%> 18 cycles
20.6 vs 14.7
ELOQUENT 2
EloRd vs Rd Untilprogression,SAE or consent withdrawal
17m vs 12m 14.9 vs 19.4
POLLUX DaraRd vs Rd Untilprogression, SAE or consent
withdrawal
24 m vs 16m
NR (68% at 24 m) vs 17
-
Lenalidomide‐Dex1 vs ≥vs 2 prior
therapies
Stadtmauer E Eur J Haematol 2009;82:426
-
Treatment
of First RelapseLong PFS are achieved with
current triplets
Aspire KRd
vs Rd KRD Med PFS 29.6m
Tourmaline-MM1 Ird vs Rd HR 0.88(0.6 if no prior Tx)
Pollux DaraRd
vs Rd HR 0.44 p
-
34%
26%
13%10%
6% 3%0
10
20
30
40 DRd (n = 286)
POLLUX: MRD‐Negative Rates and Time to MRD Negativity
•
In the total evaluable population, MRD negative rates were more than 3‐fold higher with DRd
versus Rd at all sensitivity thresholds•
MRD negative patients (identified at the 10–5
sensitivity threshold) accumulated more rapidly with DRd
versus Rd
MRD = minimal residual disease.Dimopoulos
MA, et al. Presented at European Hematology Association Annual Meeting. June 22‐25, 2017. Madrid, Spain. Abstract P334.
MRD
Negative Ra
te (%
)
P
-
PFS Based on MRD Negativity in the ITT POLLUX & CASTOR
PFS was prolonged in patients who achieved MRD negativity
Courtesy Avet Loiseau H
-
OS Based on MRD Negativity in the ITT POLLUX & CASTOR
OS was prolonged in patients who achieved MRD negativity
-
PFS Based on Sustained MRD Negativity (10-5; > 12 Months)
PFS was prolonged in patients with sustained MRD negativity 12
months, regardless of treatment arm
-
OS Based on Sustained MRD Negativity (10-5; 6 Months)
OS was prolonged in patients with sustained MRD negativity 6
months, regardless of treatment arm
-
IN FIRST RELAPSE
With modern combinations The objective of treatment should now
be
to achieve the best possible PFS And to achieve and prolong
-
It is the same old story
…. AS for Frontline therapy
-
CONTINUOUS THERAPY
Until progression or SAE One of the causes of the major
improvement in MM outcome observedover the last 20 years
With the objectives of- deepening the response- delaying
progression
-
What would be the interestof fixed (reduced) duration
Decrease the incidence of adverse eventsand improve quality of
life
Decrease costs Save effective drugs for later treatments
Decrease the risk of resistance ?
-
Safety in RCT
ASPIRE TOURMALINE 1 ELOQUENT2 POLLUX CASTOR
Treatmentdiscontinuation due to SAE
15.3% 17% 13.5% 6.7% 7.4%
-
In the past Continuous or maintenance therapyhas always
prolonged PFS
in responding patients Chemotherapy
Interferon
Thalidomide
-
But the key question is OS BENEFIT Adverse events and extra-cost
of continuous
therapy are justified only if there is an OS benefit
Chemotherapy: no OS benefit 1 Interferon: 4 to 8 m benefit 2,3
Thalidomide : OS benefit not in all trials
(6 RCT 4 , one meta-analysis 5 )New agents were not always
available
EARLY versus LATE Thalidomide
23
1 Belch Br J Cancer 1988;57:94 2 Ludwig H Acto Oncol 2000;39:815
Myeloma trialists Br J Haematol 2001;113:10204 Ludwig H Blood
2012;119:3003 5 Wang Y J Natl Cancer Instit 2016;108;dlv 342
-
Lenalidomide post ASCTFour randomized trials show a dramatic
PFSimprovement
HR 0.57 p
-
Results are less clear for OS
Significant OS benefit CALGB
MRC XI
No significant OS benefit GIMEMA
IFM
-
The OS benefit may be delayed due to better salvage
treatments
Meta-analysis of the 3 trials (1208 pts, 79.5 mo median f-up)
The benefit of a longer duration of first response translates into
a longer OS only
after 5 years
Mc Carthy P (JCO 2017 online)
-
Survival after 1st progression was shorter in the IFM 05-02 with
lenalidomide
Patients in the lenalidomide arm responded less wellto HD
Len-Dex at relapse
P
-
Maintenance or continuoustherapy in elderly patients
28
-
MM‐015: MP 9 cycles vs MPR 9 cycles +/‐
R PFS and OS (459 pts)
• Trend for extended OS with MPR-R vs MP (estimated 3-yr OS: 73%
vs 65%; p=0.254)
PFS OS
Palumbo et al. NEJM 2012;366:1759-69
4-year OSMPR-R 69%MPR 61%MP 58%
-
FIRST trial (1623 pts)MPT 12 cycles vs Rd 12 cycles vs Rd continuous
PFS OS
Benboubker L NEJM 2014;371:906 T Facon Blood 2018;131:301
Rd>MPT (PFS and OS)Rd continuous not >Rd 18m for OS
-
MRC XI TRIAL Lenalidomide
maintenance in the TNE Pathway
PFS med 26 m vs 11 m
3‐yr OS 67% vs 70%
Jackson GH Lancet Oncol 2019;20:57-73
-
Duration of treatment in First Relapse
Until now no randomized study addressed this question
Continuous treatment may be associated with more CR
(KRd parients in the ASPIRE study)
Cumulative ≥ CR rates PFS according
to CR
Dimopoulos M J Haemtol Oncol 2018;11:49
-
Duration of treatment in First Relapse
Until now no randomized study addressed this question
Continuous treatment may be associated with more CR Continuous
treatment may be associated with more
-
Duration of treatment in First Relapse
Until now no randomized study addressed this question
Continuous treatment may be associated with more CR Continuous
treatment may be associated with more
-
PFS in LEN‐refractory patients
CASTOR
ENDEAVOR
OPTIMISMM
Chanan-Khan A ASH 2016 Moreau P Leukemia 2017;31:115 Richardson
P Lancet 2019
-
Double refractory MM
RR to first treatment 12% if Bort or Len
35 % if Pom or Car Med PFS 5m Med OS 15m
80
60
40
20
0Pa
tient
s, %
Overall survival
0 12 24 36 48 60
Duration From Time Zero, months
9Event-free survival 5 (
Kumar S Leukemia 2017
-
Duration of treatment in First Relapse
Until now no randomized study addressed this question
Continuous treatment may be associated with more CR Continuous
treatment may be associated with more
-
Is it possible to design a trial addressing the question
of treatment duration in First Relapse ? Pharma companies are
more interested in trials
testing new drugs or new startegies Should be academic ( ex :
IFM trial comparing
DaraRd continuous versus 2y in first relapse) Primary objective
?
- OS too long and non-inferiority design- PS probably in favor
of continuous
Based on MRD
-
Conclusion
In the majority of patients with RRMM treatment should be
continued
But in First relapse where a high incidence of long PFS is hoped
with new combinations
The question of longer PFS (continued therapy) vs
toxicity/quality of life and extra-costs (fixed or result-adapted
duration) should addressed


















![COMY slide.pptx [Sola lettura] - Siematologia · COMY slide.pptx [Sola lettura] Author: Francesca Created Date: 1/11/2016 9:15:21 AM](https://img.pdfslide.net/doc/110x75/60ad29456126f07bb23e5dde/comy-slidepptx-sola-lettura-siematologia-comy-slidepptx-sola-lettura-author.jpg)