Embed Size (px)
Citation preview

Critical Care
structures/teams
and outcomes
Michael Power
National Clinical Lead, Critical Care Programme, National Clinical Programmes,
Clinical Strategy and Programmes Division, HSE

Critical Care Service
Joint Faculty of Intensive Care Medicine of Ireland (JFICMI) National
Standards define
Critical Care Service
“appropriate for the care of patients requiring Level 2, 3 and 3(s) critical
care…generally delivered within a High-Dependency Unit (HDU) or Intensive Care
Unit (ICU).”
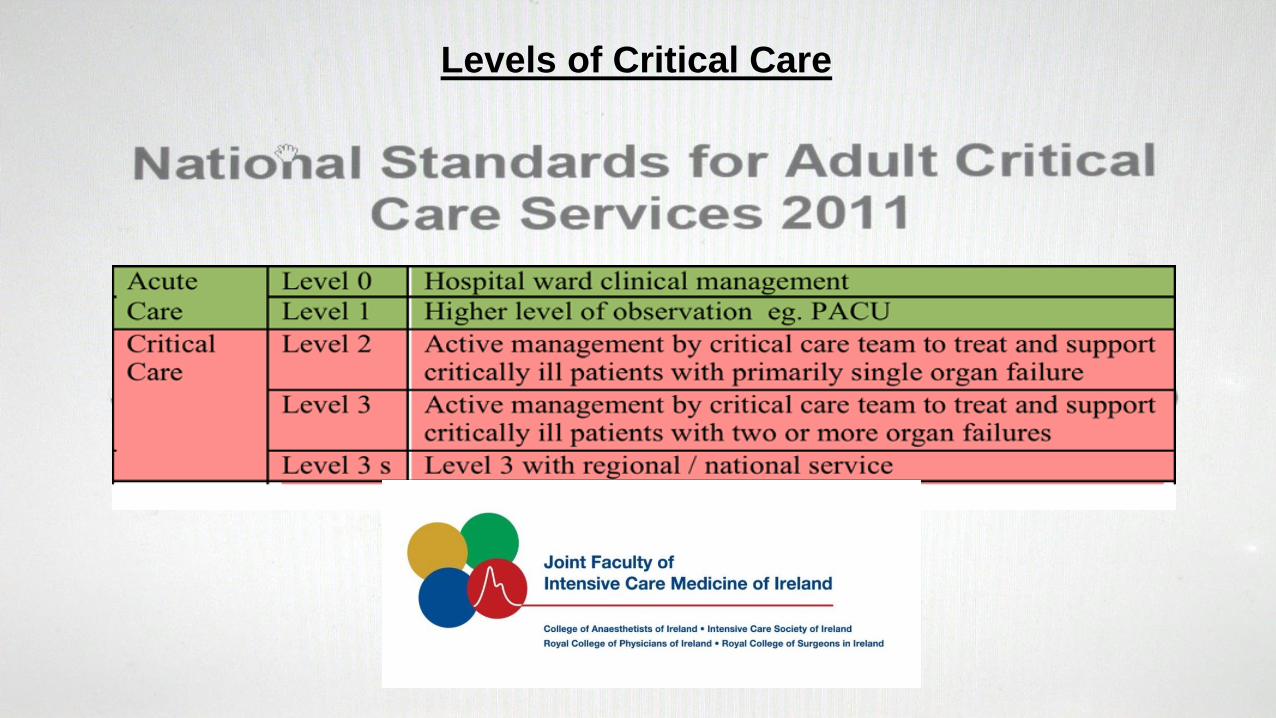
Levels of Critical Care
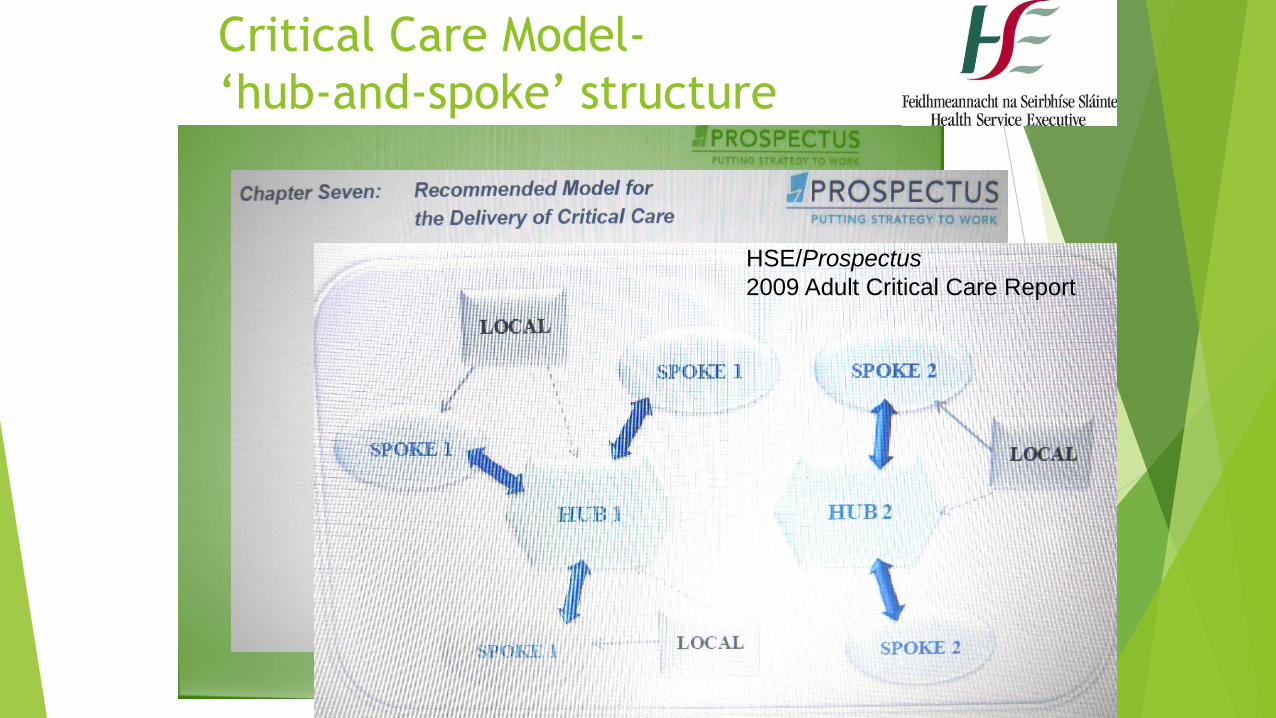
Critical Care Model-
‘hub-and-spoke’ structure
HSE/Prospectus
2009 Adult Critical Care Report

‘System-of-Care’
Ennis Mallow Tallaght Galway Portlaoise

Hospital Groups and Smaller Hospital Framework 2013
‘Higgins Report’ ‘Smaller Hospital Framework’

SSWHG
ULHG
SaoltaHGRCSIHG
IEHG
IEHG
DMLHG
Hospital Groups
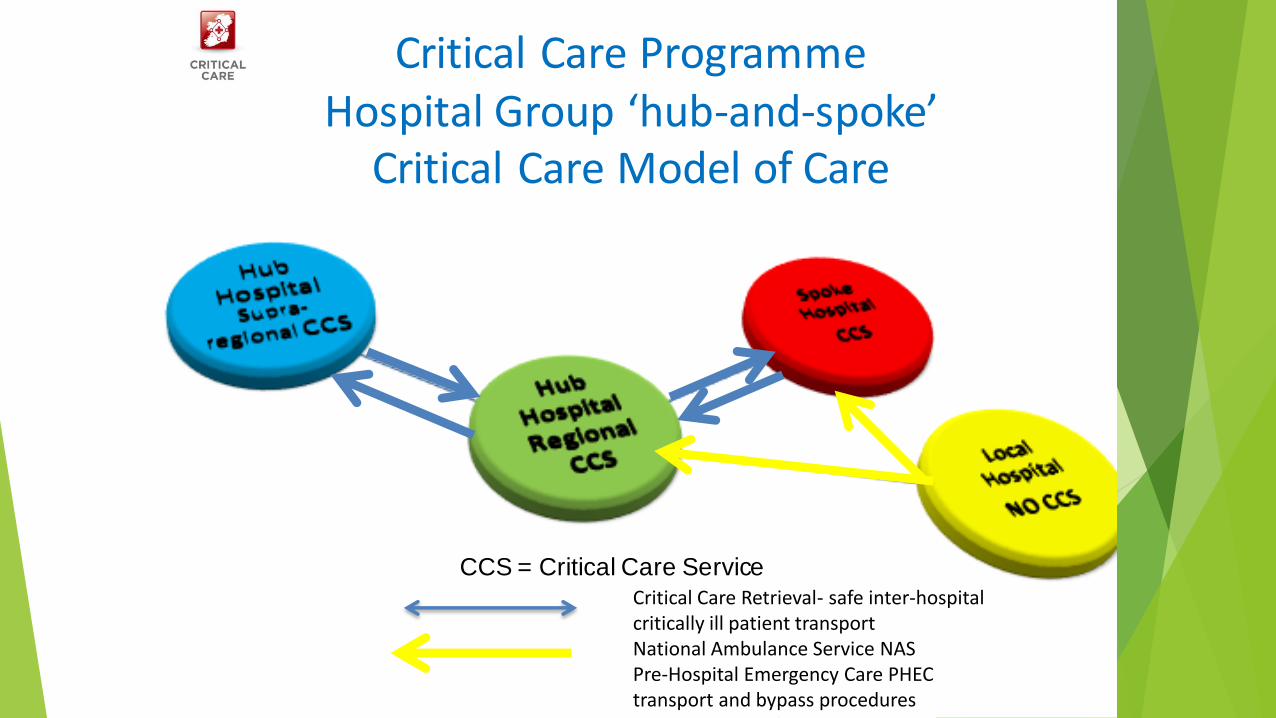
Critical Care Programme Hospital Group ‘hub-and-spoke’
Critical Care Model of Care
CCS = Critical Care ServiceCritical Care Retrieval- safe inter-hospital critically ill patient transportNational Ambulance Service NAS Pre-Hospital Emergency Care PHEC transport and bypass procedures

Health Service Reform Programme, 2003, Minister Martin, DOHC
‘main element’ – ‘major rationalisation of existing health service agencies to
reduce fragmentation’
Health Act, 2004 (HSE)
Health Act, 1970 repealed
Health Act, 2007 (HIQA)

www.decentralisation.gov.ie

Roscommon
emergency services
Countervailing local political forces

Acute healthcare sector delivery- system
or local?
“All politics is local”
Senator Thomas P “Tip” O’Neill, Speaker, US House of Representatives, 1977-86

‘Rationalisation’
These are my principles.
If you don’t like them…
Well… I have others.
Groucho Marx

Ferlie Shortell, Milbank Quarterly 2001
Healthcare system “nested”
organisational model

Critical Care Complexity- Daily Care Plan

Critical care reliability-
Plsek’s complexity model
TEAMWORK-Daily Care Plan

EVIDENCE DRIVER:
Antimicrobial delay decreases survival in
sepsis patients with hypotension
Administration of an antimicrobial effective for sepsis within the first hour of
documented hypotension was associated with a survival rate of 79.9%.
Each hour of delay in antimicrobial administration over the ensuing 6 hrs was
associated with an average decrease in survival of 7.6%.
Kumar et al; Critical Care Medicine (journal) 2006 34(6):1589-96.

EVIDENCE DRIVER:
ARDS management and survival
For ARDS patients, an increased tidal volume was associated with a 20%
increase in the risk of ICU mortality.
Thus, within the setting of routine clinical practice, timely adherence to the
use of low tidal volumes for patients with ARDS is associated with improved
survival.
Needham et al; Am J Respir Crit Care Med. 2015 191(2): 177–185.

ICU Daily Care Plan (extract)
Daily 24hr Intensive Care Medicine Plan record
Date: __/__/__ Length of stay: ____(days)
Diagnoses/Problems: Acute Chronic diagnoses
1.
2.
3.
4.
5.
6.
Plan Bundles implementation Yes/No
1.
CRBSI prevention bundle VAP prevention
bundle
2.
1. Hand hygiene 1. Elevation head-of-bed
3.
2. Barrier precautions insertion 2. Daily oral care
4. 3. Chlorhexidine 3. Daily sedation
interruption
as appropriate
5.
4. Appropriate site selection 4. PUD prophylaxis
6. 5. Daily review re removal
Date of insertion:
5. VTE prophylaxis
Discharge Planning
Family Communication Planning
Signed: _______________ICU Registrar, Signed: _____________ICU Consultant
Beaumont Hospital ICU Medicine Patient identifier
ARDS
Ventilation 6mL/kg

Resource allocation
and deploy-ment
Daily Plan clinical
evaluation clinical decision making
Actual Critical
Care Delivery
Measured critical care
organ support
activities
Patient outcomes
Health system Impact
Clinical Microsystems
Critical Care Process for the Critically Ill Patient
Critical care clinicians operational groups- ‘on the floor’ ‘huddles’ during ‘surges’

A profile of adult critical care activity in
Ireland
80%20%

ICU-BIS (Bed Information System, Bed Bureau)
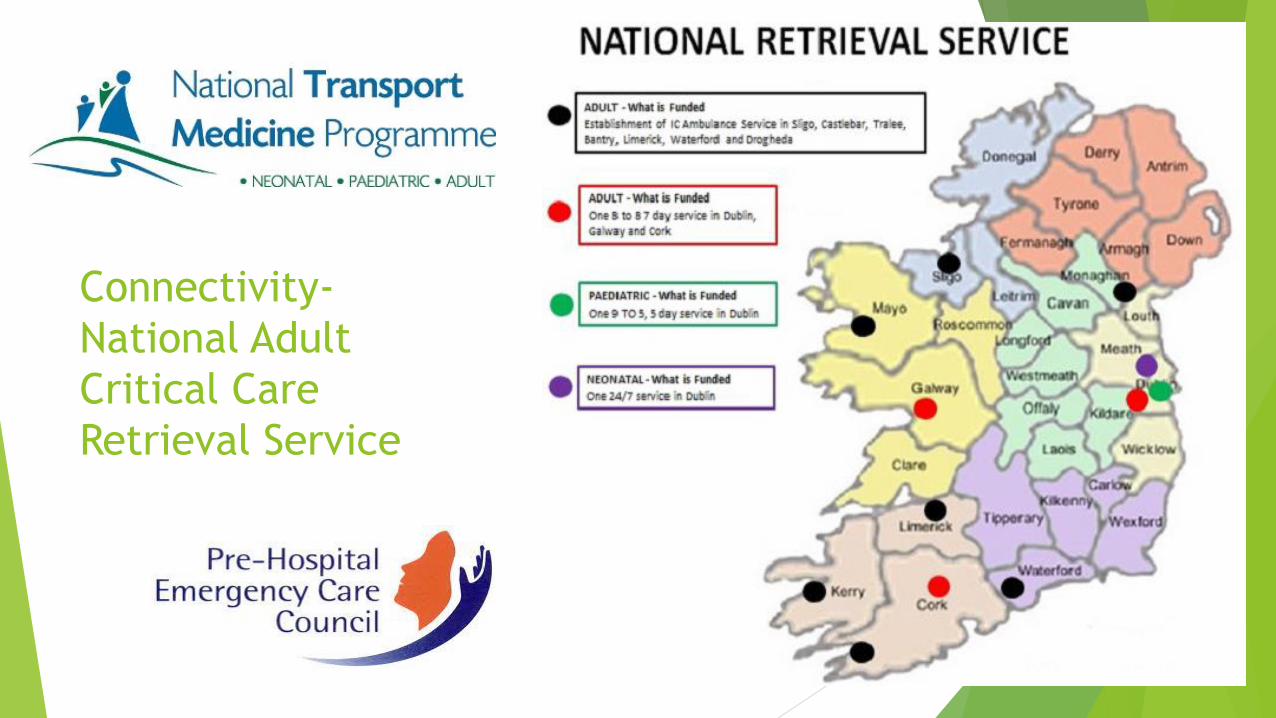
Connectivity-
National Adult
Critical Care
Retrieval Service
“Chain-of-Survival”

Critical Care Programme Hospital Group ‘hub-and-spoke’
Critical Care Model of Care
CCS = Critical Care ServiceCritical Care Retrieval- safe inter-hospital critically ill patient transportNational Ambulance Service NAS Pre-Hospital Emergency Care PHEC transport and bypass procedures

ILCOR Advisory Statement
(Circulation 2015, in press)
Temperature Management After Cardiac Arrest- An Advisory Statement by the Advanced Life Support Task Force of the International Liaison Committee on Resuscitation and the American Heart Association Emergency Cardiovascular Care Committee and the Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation
“The Task Force recommends targeted temperature management for adults with out-of-hospital cardiac arrest with an initial shockable rhythm at a constant temperature between 32°C and 36°C for at least 24 hours.”

Out-of-hospital cardiac arrests-
Care pathway implementation
increases survival
London Ambulance Service LAS- pop. 8m.
Clinical pathways “Chain-of-Survival” and “Heart Attack Hospital”
Bystander CPR, AED deployment
Fast pre-hospital emergency care response and hospital bypass procedure
Extra 222 patients “survived to hospital discharge” in 5 years (VF survival-
12% increased to 32%)
Editorial- “It takes a system to save a victim”
Fothergill, Resuscitation 2013

Trauma Teams and trauma ‘under-triage’
“…the true cost of [trauma] under-triage in population terms is an excess
mortality of almost 25%”
Haas B et al; Survival of the Fittest: the Hidden Cost of
Undertriage of Major Trauma; J Am Coll Surg 2010: 211-
804.

Multiple trauma patients
Damage Control Surgery
Intensive Care role
Traditional approach
Damage control approach

Major Trauma Volume Outcomes
Resuscitation Outcomes Consortium

Increased Trauma Center Volume Is Associated With Improved Survival After Severe Injury: Results of a Resuscitation Outcomes Consortium Study.Minei, Joseph et al Annals of Surgery. 260(3):456-465, September 2014.
Increased trauma survival at
Royal London Hospital
Mortality at RLH decreased from 2000 to 2005 by 48% from 34.2% to 17.9%
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53%
relative decrease in mortality
Davenport, BJS 2010

Neurocritical Care Teams
“There is limited evidence supporting a strategy of secondary transfer of
severe non-surgical traumatic brain injury patients to specialist neuroscience
centres.”
The effectiveness of specialist neuroscience care in severe traumatic brain
injury: a systematic review; Fuller G et al; Br J Neurosurgery 2014

London Stroke StrategyHub-and-spoke stroke care- Hyper-acute
stroke unit (HASU) and stroke units teams
Hyper-acute
stroke unit
HASU

Impact of centralising acute stroke services in
English metropolitan areas on mortality…;
Morris et al; BMJ 2014
4% risk-adjusted decrease in mortality
2008 2012
“This suggests that the type of system redesign and the extent of its implementation can affect patient outcomes and needs to be taken into account by those who are reorganising services.”

Benefit of multidisciplinary
critical care teams
US 112 ICUs, 107,324 patients
“Daily rounds by a multidisciplinary team are associated with lower mortality
among medical ICU patients. ”
“The survival benefit of intensivist physician staffing is in part explained by
the presence of multidisciplinary teams in high-intensity physician-staffed
ICUs.”
Kim et al; Arch Int Med 2010

Volume-outcome effect
US, 169 ICUs, 24,726 patients
Ventilation in a hospital >300 ventilated patients p.a. confers mortality ARR
3.4%
Volume <100 100-199 200-299 300-599 >600
Mortality 40.1 39.1 37.0 32.4 32.4P=0.04
Kahn et al; Health Services Research 2009
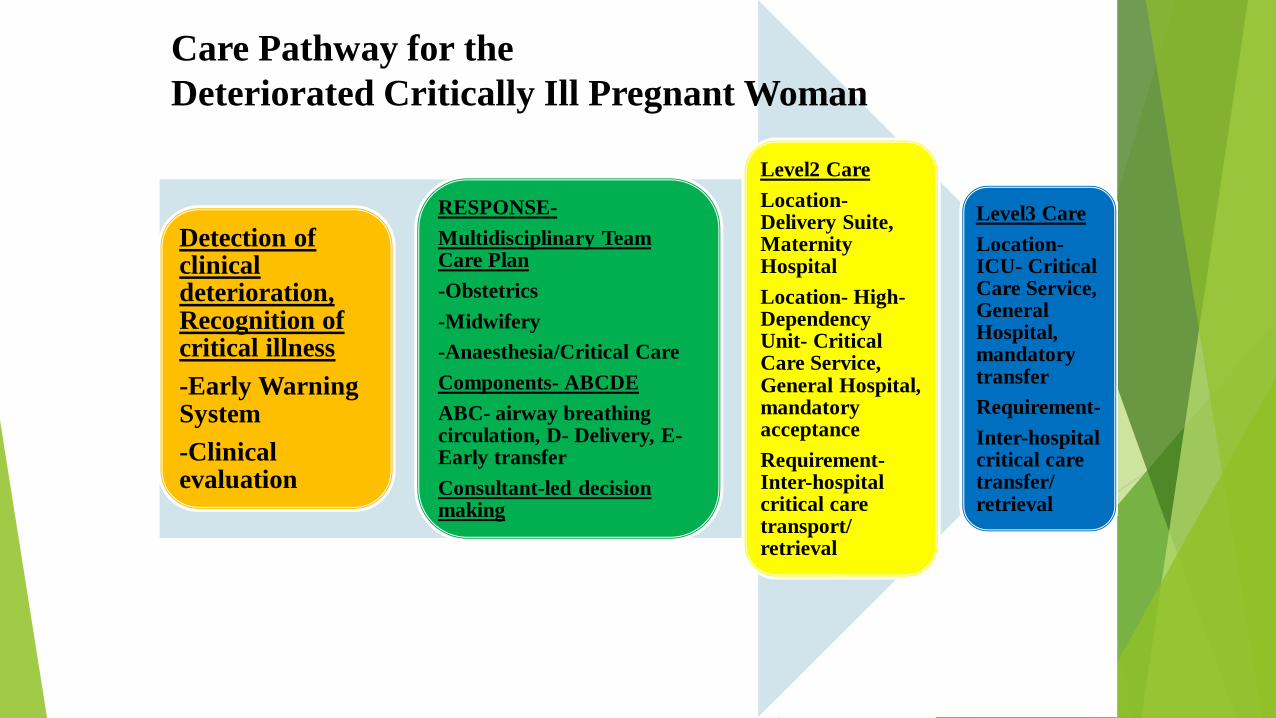
Detection of clinical deterioration, Recognition of critical illness
-Early Warning System
-Clinical evaluation
RESPONSE-
Multidisciplinary Team Care Plan
-Obstetrics
-Midwifery
-Anaesthesia/Critical Care
Components- ABCDE
ABC- airway breathing circulation, D- Delivery, E-Early transfer
Consultant-led decision making
Level2 Care
Location-Delivery Suite, Maternity Hospital
Location- High-Dependency Unit- Critical Care Service, General Hospital, mandatory acceptance
Requirement-Inter-hospital critical care transport/ retrieval
Level3 Care
Location-ICU- Critical Care Service, General Hospital, mandatory transfer
Requirement-
Inter-hospital critical care transfer/ retrieval
Care Pathway for the
Deteriorated Critically Ill Pregnant Woman

Critical Care Programme Hospital Group ‘hub-and-spoke’
Critical Care Model of Care
CCS = Critical Care ServiceCritical Care Retrieval- safe inter-hospital critically ill patient transportNational Ambulance Service NAS Pre-Hospital Emergency Care PHEC transport and bypass procedures

Critical care reliability-
Plsek’s complexity model
TEAMWORK-Daily Care Plan

ICU Daily Care Plan (extract)
Daily 24hr Intensive Care Medicine Plan record
Date: __/__/__ Length of stay: ____(days)
Diagnoses/Problems: Acute Chronic diagnoses
1.
2.
3.
4.
5.
6.
Plan Bundles implementation Yes/No
1.
CRBSI prevention bundle VAP prevention
bundle
2.
1. Hand hygiene 1. Elevation head-of-bed
3.
2. Barrier precautions insertion 2. Daily oral care
4. 3. Chlorhexidine 3. Daily sedation
interruption
as appropriate
5.
4. Appropriate site selection 4. PUD prophylaxis
6. 5. Daily review re removal
Date of insertion:
5. VTE prophylaxis
Discharge Planning
Family Communication Planning
Signed: _______________ICU Registrar, Signed: _____________ICU Consultant
Beaumont Hospital ICU Medicine Patient identifier
ARDS
Ventilation 6mL/kg

Advocates
Dr B Marsh
Dr M Donnelly
Dr G Fitzpatrick
Dr A Fahy
Dr A Westbrook
Dr M Scully
Dr J Bates
Dr J Smith
Dr F Colreavy
Dr P Seigne
Dr R Plant
Dr I Hayes
Dr J Moriarty
Dr B McCloskey
Dr K Carson
Dr F O’Donovan
Dr B O’Hare
Ms M Hanlon, IACCN
Ms Y Dunne, IACCN
Dr J Laffey
Dr R Dwyer
Dr D Phelan
Dr J O’Dea
Dr C Motherway
Dr J McAdoo
Dr D Doherty
Dr V Hamilton
Dr J Whyte
Dr B Warde
Acknowledgements Ms U Quill Mr D Cribbin CCP
Dr A GirbesDr G LaveryProf M MythenProf K Rowan

Thank you





























