Embed Size (px)
Citation preview

CONGRESS REPORT: INVITED LECTURE
Esophagus (2004) 1:169–176 © Japan Esophageal Society and Springer-Verlag 2004DOI 10.1007/s10388-004-0027-z
Simon Law · John Wong
Current status of esophageal cancer treatment in Asia
Received: August 4, 2004
S. Law · J. Wong (*)Division of Esophageal Surgery, Department of Surgery, Universityof Hong Kong Medical Centre, Queen Mary Hospital, 102 PokfulamRoad, Hong KongTel. �852-2855-4610; Fax �852-2816-2094e-mail: [email protected]
This lecture was presented during the international session at the 58thAnnual Meeting of the Japan Esophageal Society.
Abstract Esophageal cancer is becoming a different diseasein Asian and Western countries. The rapidly rising inci-dence of adenocarcinoma of the lower esophagus and car-dia has replaced squamous cell cancers as the predominantcell type in the west. The different cell type and tumorlocation to some extent influence how the disease is treated;other factors are cultural and the way health care isfinanced. The goals of treatment, however, are the same; toprovide long-term cure with minimal morbidity and mortal-ity and to preserve patients’ quality of life. Surgical resec-tion has remained the mainstay treatment in Asia.Improvement in surgical outcome has taken place in manycenters throughout Asia in the past two decades. Emphasishas been centered on epidemiology of the disease, reducingmorbidity and mortality of esophagectomy, and identifyingeffective surgical or nonsurgical methods of treatments.Randomized controlled trials are also increasingly em-ployed to test many unresolved problems. The Asian contri-butions are elaborated with specific examples from Japan,Hong Kong, and China.
Key words Esophageal cancer · Esophagectomy · Resec-tion · Multimodal treatment
Asia versus the West
Asian and Western countries are increasingly encounteringa different form of esophageal cancer (Table 1). The moststriking finding on esophageal cancer in the past three de-cades was the dramatic rise, in the West, in the incidence of
adenocarcinomas of the lower esophagus and around thegastroesophageal junction, which has surpassed squamouscell cancers as the predominant cell type [1]. In Asia, how-ever, esophageal cancers when diagnosed are predomi-nantly squamous cell in type and are mostly located in themiddle third of the esophagus. There has not been anynoticeable rise in the incidence of adenocarcinoma of theesophagus and gastric cardia in published Asian data.
The rise in adenocarcinoma around the gastroesoph-ageal junction in the West is widely believed to be relatedto gastroesophageal reflux disease, obesity, and Barrett’sesophagus [2–4], which are uncommon in Asian populations[5]. The higher prevalence of Helicobacter pylori infectionin Asia is also postulated to be “protective” against gastroe-sophageal reflux disease and its consequent Barrett’s cancer[6]. This association, however, remains hypothetical.
Regardless of the reasons for the difference in epidemi-ology, this trend has practical implications in research andmanagement strategies. In the West, research in recentyears has focused toward studying the etiology of Barrett’sesophagus, surveillance policies, molecular indicators ofdysplastic and carcinomatous transformation from Barrett’sesophagus, and treatment of dysplastic and early adenocar-cinomas. The Barrett’s esophagus – dysplasia – cancer se-quence, for instance, may allow surveillance programs to beinstituted in Western countries, with the possibility of diag-nosing the disease at a readily treatable stage [7,8]. High-grade dysplasia is amenable to surgical resection or otherforms of ablative therapies, such as endoscopic mucosalresection or photodynamic therapy. There is evidence thatpatients with Barrett’s esophagus who are recruited intosurveillance programs have a better prognosis [8]. The opti-mal surveillance interval, its cost-effectiveness, the relativemerits of the various treatment approaches, and impact onthe population at large are still debated [9].
In Asia, early squamous cell cancers are primarily stud-ied in endemic areas such as China, with most early cancersdiagnosed by population screening, or in Japan, where pan-endoscopy practice is widespread to screen for gastric can-cer. There is no good marker for the precancerous stage andearly cancer, so most patients still present with symptom-

170
atic, advanced stage of disease. In both Asia and the West,techniques of resection and multimodal treatments are in-tensely studied, but the differences in cell type and tumorlocations dictate preferences in surgical approaches. Also,because of difference in cultural attitude and health carefinancing, the application of multimodal therapies followsdifferent emphasis. Thus, one has to be mindful of theseimportant differences between Asia and the West whentreatment results are compared.
Results of surgical resection
Surgical resection remains the mainstay treatment forpatients with localized esophageal cancer. Whether in Asiaor in Western countries, surgical results have improved indedicated centers, where mortality after esophagectomyhas been reduced to less than 5% [10–17]. It is, however,also true that the overall mortality rate still approximates10% when population data are studied [18–20]. In HongKong, an audit by the local Hospital Authority showed thatthe overall mortality rate after esophagectomy for intratho-racic cancer was 11% for the whole city, although the bestresult of 1% in one hospital was also observed [20]. InJapan, low mortality rates are commonly reported in thesurgical literature, but a Comprehensive Registry of Esoph-ageal Cancer revealed a postoperative death rate of 12%[21]. This difference between specialized high-volume cen-ters and national figures also applies to Western data [22].
It is also interesting to observe that mortality rates inAsia, notably in China and Japan, are in general lower thanin most Western countries. The reasons for this are notimmediately apparent. Patient selection and different pa-tient risk profiles may in part contribute. Surgical experi-ence, especially in endemic areas, can be extensive and isimportant in achieving good outcome. It is remarkable thata 30-day mortality rate of 4.6% could be achieved during1952–1976 in China [23]. It has been consistently shown thatgood results from complex surgery such as esophagectomyare much more likely in dedicated high-volume centers withhigh-volume surgeons, where a mortality rate from surgeryof 2%–3% can be achieved [10–14,24,25].
Treatment strategies in Japan
Japan has played a leading role in many aspects of pioneer-ing treatment of esophageal cancer, and results haveimproved over the years [12,26]. The most notable contribu-tion in surgical technique is in the role of three-fieldlymphadenectomy for esophageal cancer, which has beenstudied since the 1980s [27]. The rationale for extensivelymphadenectomy for esophageal cancer is that lymphaticinvolvement spreads early and widely. Between 8% and30% of patients with tumors reaching the muscularis muco-sae, and 30% to 58% for tumors involving the submucosa,have pathological lymph nodes [27]. The overall rate ofcervical lymph node metastases has been documented andis approximately 30%. In relation to the level of primarytumor, cervical lymph nodes are involved in 60%, 20%, and12.5% of upper, middle, and lower third tumors, respec-tively [27]. In Japan, lymph node dissection is extended tothe superior mediastinum and the neck, most importantlyalong the recurrent laryngeal nerves, in addition to the stan-dard two-field lymph node dissection that is more widelypracticed. For Barrett’s adenocarcinomas of the loweresophagus in the West, presumably with less chance of su-perior mediastinal and cervical lymph node spread, thismeans that this surgical approach is less commonly em-ployed. Only in very selected centers in the United Statesand Europe has this procedure been tested, which interest-ingly also yielded similar incidences of positive cervicallymph nodes [13,28]. A recent review of three-field lym-phadenectomy showed an overall hospital mortality rate of4% and morbidity rate of 44.8%. Septic complications werethe most common at 26.8%, followed by pulmonary com-plications at 21.3%. Recurrent laryngeal nerve injury canoccur in more than 50% of patients [29], which predisposesto pulmonary complications and impairs long-term qualityof life [30].
Although a very low mortality rate and reasonable mor-bidity rate can be achieved, all these reports come fromexperienced and specialized institutions, and such extensivesurgery is expected to carry with it more unfavorable out-come if more widely and unselectively applied. The othermajor criticisms of three-field dissection are that the prog-
Table 1. Comparisons of esophageal cancer between Asia and Western countries
Factor Asia West
Cell type Squamous cell cancer AdenocarcinomaLocation Mid- and lower esophagus Lower esophagus/cardiaMain risk factors Smoking and alcohol Gastroesophageal reflux
History of other upper aerodigestive tract cancers ObesitySocioeconomic status Blue collar White collarComorbid diseases Pulmonary disease Ischemic heart disease
CirrhosisIdentifiable premalignant lesions ? Dysplasia Barrett’s esophagus and dysplasiaScreening/surveillance Only in endemic areas, e.g., China Endoscopic surveillance for
Barrett’s esophagusSurgical approaches Predominantly transthoracic, three-field Transthoracic/transhiatal two-field
lymphadenectomy or minimal lymphadenectomyPrognosis Worse? Better?

171
nostic superiority over conventional resection is a result ofstage migration. Although statistical methods such as theCox regression model can be applied to provide evidencefor the benefits of three-field dissection [31], the more ro-bust evidence of a well-performed randomized controlledtrial has never been acquired. Only two small trials havebeen published. The first showed a higher postoperativemortality rate for two-field and a survival advantage forthree-field dissection; in the second, 5-year survival rateswere not statistically different for three-field dissection(66.2%) and two-field dissection (48%). In both studies,patient groups appeared highly selected, not well matched,and adjuvant therapies were not controlled [32,33]. Perhapsrealizing such an extensive operation carries with it substan-tial morbidity, and that not all patients could benefit, therecent focus of research in this area is to further refine theindication of extended lymphadenectomy, such as confiningthe mediastinal dissection in the thoracic cavity [34], usingintraoperative polymerase chain reaction to examine recur-rent laryngeal nerve lymph node to predict the need forcervical dissection [35], and even taking a two-stage ap-proach to select patients suitable for cervical lymphadenec-tomy [36]. Preliminary data from sentinel lymph nodemetastases show that the concept is feasible, and it is hopedthat in the future it can be applied to individualized treat-ment of esophageal cancer, just as in melanoma and breastcancer [37].
Japanese surgeons are also among the first to grasp theimpact of new technology. One example is endoscopicultrasound (EUS), which has been widely used andresearched in Japan. In one study, combination of percuta-neous ultrasound and EUS was used to assess the numberof lymph node metastases. It showed that the number oflymph nodes involved can be predicted accurately. Theaccuracy rates associated with zero, one to three, four toseven, and eight or more lymph nodes were 83.3%, 59.7%,43.3%, and 96%, respectively, with corresponding 5-yearsurvival of 53.3%, 33.8%, 17%, and 0%. The differencesamong groups were statistically significant [38]. The accu-racy by ultrasound examination for patients without me-tastases and for those with eight or more lymph nodesinvolved was high, but both over- and underestimation oc-curred for patients with an intermediate number of lymphnodes involved. The number of involved lymph nodes hasbeen repeatedly shown to be valuable as a prognostic factorand has already been incorporated into the latest Guide-lines for Clinical Studies on the Esophagus by the JapaneseSociety for Esophageal Diseases in staging [39]. The TNMclassification of the International Union Against Cancer hasadopted lymph node number for use in gastric, colonic,rectal, pancreatic, and breast cancer but has been slow inapplying it to the esophagus [40]. This kind of study givesmore impetus to the concept of lymph node load as a prog-nostic factor, especially if technological advances in EUScan give us accurate information preoperatively.
Relating to the use of EUS, Japanese investigators havealso studied in detail the application of endoscopic mucosalresection (EMR) in early cancer [41]. The ability to distin-guish different depths of penetration by the tumor using
EUS (from m1,2,3 to sm1,2,3) allows selective use of thetechnique, because penetration to m3 and sm levels predictsa high probability of lymph node spread, for which EMRmay not be suitable. Increasingly, early cancers are diag-nosed in Japan owing to widespread pan-endoscopic exami-nations. Similar EMR strategies have been applied in theWest for ablative therapy for Barrett’s esophagus [42].
The use of neoadjuvant or adjuvant treatments in Japanseems less compared to Western countries, especially theUnited States. Primary chemoradiation therapy has almostbecome the “standard of care” of treatment in NorthAmerica, despite the lack of clear evidence [43,44]. InJapan, these treatments are becoming more widely used,especially in patients with advanced disease [31,38,45], butthe standard treatment of resectable cancers is still primarysurgical resection, with or without postoperative chemo-therapy or radiotherapy. The Japan Clinical OncologyGroup has conducted randomized controlled trials in theuse of postoperative chemotherapy. The first trial comparedpostoperative cisplatin and vindesine chemotherapy with50Gy of radiotherapy [46]. In the second, a surgery-alonegroup with the same chemotherapy was compared [47].Neither showed an advantage for adjuvant chemotherapy.A more recent report on 242 patients compared surgicalresection with the addition of postoperative cisplatin and 5-fluorouracil (5-FU) [48]. The 5-year disease-free survivalrate was significantly different at 45% with surgery aloneand 55% with surgery plus chemotherapy. The overall 5-year overall survival rates, however, were not significantlydifferent at 52% and 61%, respectively. The effect wasmore remarkable in the subgroup with lymph node metasta-sis. It is most encouraging that randomized controlled trialsare increasingly conducted in Japan, a country traditionallyresistant to these kinds of studies. Randomized trials arealso conducted for various surgical techniques [49]. Further-more, the quality of these studies can be expected to be ofthe highest order, knowing the meticulousness of Japanesesurgeons.
The meticulous manner of the Japanese surgeons’ ap-proach to study means that data captured could form thebase for much research. The detailed examination of lymphnode spread and their classifications, for instance, whetherin esophageal or gastric cancer, have been exemplary. TheComprehensive Registry in Esophageal Cancer is a usefulnational database for comparisons of data [21]. Other suchstudies allow prognostic stratification of disease [50].
Physiological and basic scientific research is also active inJapan, such as studies on pulmonary functions and immuneresponses in the perioperative period [51–53]. Interven-tional randomized trials are also conducted based on thesefindings; one example is the use of perioperative corticos-teroid. The results suggest that prophylactic administrationof corticosteroids is associated with a decrease in postopera-tive morbidity. The laboratory data suggest that corticoster-oids may attenuate surgical stress-induced inflammatoryresponses, both directly by suppressing the release of pro-inflammatory cytokines and via inducing IL-10 synthesis[54]. Molecular studies are most useful as prognosticmarkers [55].

172
Treatment strategies in Hong Kong
In Hong Kong, much effort in recent years has been appliedin reducing morbidity and mortality from esophagectomy,and many technical aspects of esophagectomy have beentested in randomized controlled trials. The most commonsurgical complication after esophagectomy has been anasto-motic leak. A randomized trial was conducted comparing ahandsewn one-layer continuous method in esophagogastricintrathoracic anastomosis with stapled anastomosis. Al-though leak rates were low in both methods, stricture ratewith a stapled anastomosis was four times as frequent [56].An appraisal of the effects of intrathoracic leaks demon-strated a leak rate of 3.5% in 475 patients, an associatedmortality rate of 35%, and an overall leak-related mortalityrate of 1%. More importantly, it was shown that for mostleaks a technical error could be identified even in retrospec-tive review, indicating that these leaks were potentially pre-ventable [57]. A recent study of the type of gastric conduitfashioned also showed that use of the distal stomach(resecting of the gastric fundus) with incorporation of thegastric stapled line in the esophagogastric anastomosis andan anastomosis in the neck were independent factors forstricture formation [58].
The need for a pyloric drainage procedure using thegastric conduit after esophagectomy was shown in anotherrandomized trial. In 13% of patients without a pyloroplasty,significant gastric outlet obstruction occurred [59]. A one-layer technique is comparable to a two-layer method [60],and a pyloromyotomy was shown to be as effective as apyloroplasty [61].
Other technical aspects of an esophagectomy have beensystemically studied, such as using a small, vacuum systemthat is ambulatory for the patient [62], the need of neckdrain after cervical anastomosis [63], comparing the differ-ent routes of placement of the esophageal replacement con-duit [64], and the use of gastric or colonic conduits [65]. Allthese are important variables in an esophagectomy. Fromthe analgesic point of view, one of the most important anes-thetic advances in the last decade was the use of postopera-tive epidural analgesia; the use of this method of pain reliefwas significantly associated with reduction in postoperativemortality [66].
Proactive diagnosis and treatment of postoperativecomplications are essential in good outcome. We have dem-onstrated, for instance, that postoperative onset of atrialfibrillation, although mostly a benign arrhythmia, more im-portantly signifies the presence of underlying pulmonaryand septic complications, and is associated with a muchworse outcome compared to patients who do not have theabnormal rhythm [67]. Vigilant postoperative managementand early intervention are essential for success. Factors thatare predictive of postoperative complications and death areimportant and were identified by multivariate analysis,which led to modifications in management [68,69]. Ad-vanced age, proximally located tumors, and long operatingtime were associated with postoperative pulmonary com-plications; advanced age and blood loss were found to be
independent predictive factors for postoperative death [69].This finding led us to be very vigilant in caring for elderlypatients, especially those with proximally located tumors,where recurrent laryngeal nerve palsy rate is higher. Moreaggressive use of postoperative bronchoscopic sputum suc-tion, avoidance of fluid overload, tracheostomy, and pulmo-nary care are required in this group of at-risk individuals.Much effort has also been expended in being meticulous atthe time of surgery to avoid blood loss.
Another major area of research has been in the use ofmultimodal therapies in the treatment of esophageal can-cer, which were done mainly in the form of prospectiverandomized trials. One trial on adjuvant radiotherapy dem-onstrated improved local control and reducing the chanceof death from tracheobronchial recurrence, especially inpatients with residual mediastinal tumor after resection, butoverall survival was not affected [70]. Another trial withneoadjuvant chemotherapy again showed no overall im-provement in survival compared to surgical resection alone,but a response rate of 50% and a pathologically completeresponse rate of 7% was achieved. More importantly, thisstudy was one of the first to show that responders to chemo-therapy fared much better than patients who underwentresection alone, but conversely nonresponders did worse,indicating the importance of response prediction [71].
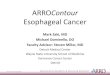
Neoadjuvant chemoradiation is currently studied in arandomized controlled trial for resectable tumors and isalso prospectively evaluated in patients with locally ad-vanced (T4) or metastatic disease (stage IV); preliminarydata showed encouraging results. Patients with advancedcancers can be downstaged, some converted to resectabletumors, and most derived significant palliation. The avail-ability of chemoradiation therapy importantly changed ourmanagement strategies. Resection rate was reduced be-cause patients with advanced and metastatic disease cannow be palliated by nonoperative means. R0 resectionswere increased because of better patient selection and tu-mor downstaging, with consequent better survival. Patientswith nonoperative treatments also derived good palliationfrom chemoradiation, with procedures such as bypass op-erations minimized [11,72]. The other major nonoperativetreatment for esophageal cancer is the use of self-expandingmetallic stents [73]. Current treatment protocol at the Uni-versity of Hong Kong Medical Centre in shown in Fig. 1.
In recent years, much energy has also been put intoresearching the genetic basis of esophageal cancer and intoprediction of response to neoadjuvant therapies [74–78].
Treatment strategies in China
Certain provinces of China have some of the highestincidences of esophageal cancer in the world and as suchcontribute greatly in many aspects of esophageal cancerresearch. Screening, whether by balloon cytology or by en-doscopic methods, results in diagnosis of cancer at the as-ymptomatic stage [79]. A large number of patients withearly cancers can thus be diagnosed. One study reported on

173
long-term results of mass screening since 1972 in the ruralareas of Henan, Hebei, and northern Jiangsu provinces in160000 individuals. Of these individuals, 30000 high-riskpersons were identified. Endoscopy was carried out in24600, and esophageal or cardia cancers were diagnosed in2094 patients, of whom 757 were found to have superficialcancers and 420 received esophagectomy. One-monthoperative mortality occurred in 5 patients only (1.2%).Pathology of the cancer specimens showed that there werecarcinoma in situ in 76 (all without lymphatic metastasis),intramucosal (TIa) carcinoma in 126 [2 (1.6%) with lym-phatic metastasis], and submucosal (TIb) carcinoma in 218[34 (15.6%) with lymphatic metastasis]. The 5-, 10-, 15-,20-, and 25-year survival rates were 86.14%, 75.03%,64.48%, 56.17%, and 49.93%, respectively [80]. This kind oflarge-scale study is only possible in China.
Surgical results have always been excellent in series pub-lished in China. Again, patient selection and experienceprobably contribute to good results. Mortality rates havebeen consistently below 5%, even in the 1950s, and long-term 5-year survival rates of 20%–30%, comparable toWestern series, were reported [16,23]. It is interesting tolearn that patients selected for operation tend to be about10 years younger than in most Western series [16]. Thistrend most likely is a reflection of patient selection, but thepossibility of its being due to the endemic nature of thedisease in these high incidence provinces remains.
Surgical resection is the mainstay treatment of esoph-ageal cancer in China, and the use of adjuvant or
neoadjuvant therapies is less frequent. However, large-scalestudies on radiotherapy, whether pre- or postoperative,have been conducted as randomized trials [81–83]. Unfortu-nately, no clear advantage has been demonstrated. Themost recent trial on postoperative radiotherapy, the largestof its kind, randomized 495 patients with intrathoracic squa-mous cell cancers [83]. Postoperative radiotherapy of 50–60Gy was given to 220 patients to the entire mediastinumand bilateral supraclavicular fossa. The radiotherapy grouphad more male patients and more patients with positivelymph nodes. Per protocol analysis showed no overall dif-ference in 5-year survival at 31.7% for the surgery-alonegroup and 41.3% for the radiotherapy group. A benefit inthe radiotherapy group was observed in stage III patients;5-year survival rates were 13.1% and 35.1% (P � 0.0027).In patients with node-positive disease, difference in survivalwas of borderline significance. The chance of mediastinal,cervical lymph node, and anastomotic recurrences was alsoreduced. Use of chemotherapy has been less common inChina, perhaps because of financial reasons, although re-cent trends have seen it becoming more popular.
It is interesting to compare different treatment strategiesfrom different countries within Asia. One such report com-pared surgical results from one prestigious center each inChina and Japan. It was found that endoscopic ultrasoundand Lugol’s iodine staining were routinely used in Japan butnot in China. Consequently, more early lesions were identi-fied (pathological T1 disease was found in 32% in Japanbut only in 6.3% in China). During esophagectomy, more
Fig. 1. Management protocol at the University of Hong Kong Medical Centre

174
lymph node stations were taken in Japan, with more exten-sive lymphadenectomy. Operation time was prolonged andmore postoperative complications were encountered inJapan, but in-hospital mortality was not increased. Therewas a tendency for better survival when patients with T1–T3stages were compared (approximately 15% difference),although this did not reach statistical significance [84].
Future directions of development
Asia has made substantial contribution to studies in esoph-ageal cancer. Although in this article the authors have con-centrated on taking examples from Japan, Hong Kong, andChina, this selection is obviously not exhaustive, and manyvaluable contributions from other Asian countries havebeen omitted. Compared with the West, squamous cell can-cers still remain the predominant cell type. Improvement insurgical outcome has taken place in many centers through-out Asia in the past two decades. The emphasis has beencentered on epidemiology of the disease, reducing mor-bidity and mortality of esophagectomy, and identifyingeffective surgical or nonsurgical treatment methods.Randomized controlled trials are also increasingly em-ployed to test many unresolved problems. In recent years,more basic scientific research has been conducted in mo-lecular and genetic studies.
In Asia, financial support in medical research tends to beless compared with developed Western countries. Healthexpenditure as percentage of gross domestic product(GDP) is only 5% in Hong Kong, 5.6% in China, and 7.1%in Japan, but it is 11.1% in Germany and 13.9% in theUnited States. Despite this shortcoming, Asia has madeimportant contributions in esophageal cancer research. It isanticipated that research efforts from Asia will continue toprovide the world with much needed evidence-based datato fight the battle against this deadly disease.
References
1. Devesa SS, Blot WJ, Fraumeni-JF J. Changing patterns in theincidence of esophageal and gastric carcinoma in the United States.Cancer (Phila) 1998;83(10):2049–53.
2. Peters JH, Hagen JA, DeMeester SR. Barrett’s esophagus. JGastrointest Surg 2004;8(1):1–17.
3. Lagergren J, Bergstrom R, Lindgren A, Nyren O. Symptomaticgastroesophageal reflux as a risk factor for esophageal adenocarci-noma. N Engl J Med 1999;340(11):825–31.
4. Lagergren J, Bergstrom R, Nyren O. Association between bodymass and adenocarcinoma of the esophagus and gastric cardia.Ann Intern Med 1999;130(11):883–90.
5. Goh KL, Chang CS, Fock KM, Ke M, Park HJ, Lam SK. Gastro-oesophageal reflux disease in Asia. J Gastroenterol Hepatol2000;15(3):230–8.
6. Graham DY. The changing epidemiology of GERD: geographyand Helicobacter pylori. Am J Gastroenterol 2003;98(7):1462–70.
7. Provenzale D, Kemp JA, Arora S, Wong JB. A guide for surveil-lance of patients with Barrett’s esophagus. Am J Gastroenterol1994;89:670–80.
8. Peters JH, Clark GW, Ireland AP, Chandrasoma P, Smyrk TC,DeMeester TR. Outcome of adenocarcinoma arising in Barrett’s
esophagus in endoscopically surveyed and nonsurveyed patients.J Thorac Cardiovasc Surg 1994;108(5):813–21; discussion 821–2.
9. Spechler SJ, Barr H. Review article: screening and surveillance ofBarrett’s oesophagus: what is a cost-effective framework? AlimentPharmacol Ther 2004;19(suppl 1):49–53.
10. Hagen JA, DeMeester SR, Peters JH, Chandrasoma P, DeMeesterTR. Curative resection for esophageal adenocarcinoma: analysisof 100 en bloc esophagectomies. Ann Surg 2001;234(4):520–30.
11. Law S, Kwong DL, Kwok KF, Wong KH, Chu KM, Sham JS,et al. Improvement in treatment results and long-term survival ofpatients with esophageal cancer: impact of chemoradiation andchange in treatment strategy. Ann Surg 2003;238(3):339–48.
12. Ando N, Ozawa S, Kitagawa Y, Shinozawa Y, Kitajima M.Improvement in the results of surgical treatment of advancedsquamous esophageal carcinoma during 15 consecutive years. AnnSurg 2000;232(2):225–32.
13. Altorki N, Kent M, Ferrara C, Port J. Three-field lymph nodedissection for squamous cell and adenocarcinoma of the esopha-gus. Ann Surg 2002;236(2):177–83.
14. Siewert JR, Stein HJ, Feith M, Bruecher BL, Bartels H, Fink U.Histologic tumor type is an independent prognostic parameter inesophageal cancer: lessons from more than 1,000 consecutiveresections at a single center in the Western world. Ann Surg2001;234(3):360–7.
15. Shao L, Gao Z, Wei GQ. Surgical treatment of carcinoma of theesophagus and gastric cardia: 34-year investigation. Chin J Surg2001;39(1):44–6.
16. Li H, Yao SC. Surgical treatment for carcinoma of the oesophagusin Chinese language publications. Br J Surg 1997;84(6):855–7.
17. Hofstetter W, Swisher SG, Correa AM, Hess K, Putnam JB Jr,Ajani JA, et al. Treatment outcomes of resected esophagealcancer. Ann Surg 2002;236(3):376–84.
18. Medical Research Council Oesophageal Cancer Working Party.Surgical resection with or without preoperative chemotherapyin oesophageal cancer: a randomised controlled trial. Lancet2002;359(9319):1727–33.
19. Bailey SH, Bull DA, Harpole DH, Rentz JJ, Neumayer LA,Pappas TN, et al. Outcomes after esophagectomy: a ten-year pro-spective cohort. Ann Thorac Surg 2003;75(1):217–22.
20. Hospital Authority Hong Kong. Clinical audit on esophagectomyand hepatectomy in Hong Kong. 2002.
21. Comprehensive registry of esophageal cancer in Japan (1998, 1999)& long-term results of esophagectomy in Japan (1988–1997). In:Ide H, editor. http://jsed.umin.ac.jp. 2002.
22. Patti MG, Costantini M, Godwin DH, Way LW. A hospital’sannual rate of esophagectomy influences the operative mortalityrates. J Gastrointest Surg 1998;2(2):186–92.
23. Liu JF, Wang QZ, Hou J. Surgical treatment for cancer of theoesophagus and gastric cardia in Hebei, China. Br J Surg2004;91(1):90–8.
24. Birkmeyer JD, Siewers AE, Finlayson EV, Stukel TA, Lucas FL,Batista I, et al. Hospital volume and surgical mortality in theUnited States. N Engl J Med 2002;346(15):1128–37.
25. Birkmeyer JD, Stukel TA, Siewers AE, Goodney PP, WennbergDE, Lucas FL. Surgeon volume and operative mortality in theUnited States. N Engl J Med 2003;349(22):2117–27.
26. Ohga T, Kimura Y, Futatsugi M, Miyazaki M, Saeki H, Nozoe T.Surgical and oncological advances in the treatment of esophagealcancer. Surgery (St. Louis) 2002;131(1 suppl):S28–34.
27. Akiyama H, Tsurumaru M, Udagawa H, Kajiyama Y. Radicallymph node dissection for cancer of the thoracic esophagus. AnnSurg 1994;220(3):364–72.
28. Lerut T, Coosemans W, De Leyn P, Deneffe G, Topal B, Van deVen C, et al. Reflections on three field lymphadenectomy incarcinoma of the esophagus and gastroesophageal junction.Hepatogastroenterology 1999;46(26):717–25.
29. Tachibana M, Kinugasa S, Yoshimura H, Dhar DK, Nagasue N.Extended esophagectomy with 3-field lymph node dissection foresophageal cancer. Arch Surg 2003;138(12):1383–9.
30. Baba M, Aikou T, Natsugoe S, Kusano C, Shimada M, Nakano S,et al. Quality of life following esophagectomy with three-field lym-phadenectomy for carcinoma, focusing on its relationship to vocalcord palsy. Dis Esophagus 1998;11(1):28–34.

175
31. Udagawa H, Akiyama H. Surgical treatment of esophageal cancer:Tokyo experience of the three-field technique. Dis Esophagus2001;14(2):110–14.
32. Kato H, Watanabe H, Tachmimori Y, Iizuka T. Evaluation of necklymph node dissection for thoracic esophageal carcinoma. AnnThorac Surg 1991;51:931–5.
33. Nishihira T, Hirayama K, Mori S. A prospective randomized trialof extended cervical and superior mediastinal lymphadenectomyfor carcinoma of the thoracic esophagus. Am J Surg1998;175(1):47–51.
34. Watanabe H, Kato H, Tachimori Y. Significance of extended sys-temic lymph node dissection for thoracic esophageal carcinoma inJapan. Recent Results Cancer Res 2000;155:123–33.
35. Yoshioka S, Fujiwara Y, Sugita Y, Okada Y, Yano M, Tamura S,et al. Real-time rapid reverse transcriptase-polymerase chain reac-tion for intraoperative diagnosis of lymph node micrometastasis:clinical application for cervical lymph node dissection in esoph-ageal cancers. Surgery (St. Louis) 2002;132(1):34–40.
36. Noguchi T, Wada S, Takeno S, Hashimoto T, Moriyama H, UchidaY. Two-step three-field lymph node dissection is beneficial forthoracic esophageal carcinoma. Dis Esophagus 2004;17(1):27–31.
37. Kitagawa Y, Fujii H, Mukai M, Ando N, Kubota T, Ikeda T, et al.The validity of the sentinel node concept in gastrointestinal can-cers. Nippon Geka Gakkai Zasshi 2000;101(3):315–19.
38. Natsugoe S, Yoshinaka H, Shimada M, Sakamoto F, Morinaga T,Nakano S, et al. Number of lymph node metastases determined bypresurgical ultrasound and endoscopic ultrasound is related toprognosis in patients with esophageal carcinoma. Ann Surg2001;234(5):613–18.
39. Japanese Society for Esophageal Diseases. Guidelines for clinicaland pathologic studies on carcinoma of the esophagus. 9th ed.Tokyo: Kanehara; 2001.
40. Hermanek P, Sobin LH. UICC TNM classification of malignanttumors. Berlin: Springer; 1987.
41. Inoue H, Fukami N, Yoshida T, Kudo SE. Endoscopic mucosalresection for esophageal and gastric cancers. J GastroenterolHepatol 2002;17(4):382–8.
42. Pacifico RJ, Wang KK, Wongkeesong LM, Buttar NS, Lutzke LS.Combined endoscopic mucosal resection and photodynamictherapy versus esophagectomy for management of early adenocar-cinoma in Barrett’s esophagus. Clin Gastroenterol Hepatol2003;1(4):252–7.
43. Daly JM, Fry WA, Little AG, Winchester DP, McKee RF, StewartAK, et al. Esophageal cancer: results of an American College ofSurgeons Patient Care Evaluation Study. J Am Coll Surg2000;190(5):562–72.
44. Suntharalingam M, Moughan J, Coia LR, Krasna MJ, Kachnic L,Haller DG, et al. The national practice for patients receivingradiation therapy for carcinoma of the esophagus: results of the1996–1999 Patterns of Care Study. Int J Radiat Oncol Biol Phys2003;56(4):981–7.
45. Gomi K, Oguchi M, Hirokawa Y, Kenjo M, Ogata T, Takahashi Y,et al. Process and preliminary outcome of a patterns-of-care studyof esophageal cancer in Japan: patients treated with surgery andradiotherapy. Int J Radiat Oncol Biol Phys 2003;56(3):813–22.
46. Japanese Esophageal Oncology Group. A comparison of chemo-therapy and radiotherapy as adjuvant treatment to surgery foresophageal carcinoma. Chest 1993;104(1):203–7.
47. Ando N, Iizuka T, Kakegawa T, Isono K, Watanabe H, Ide H, et al.A randomized trial of surgery with and without chemotherapyfor localized squamous carcinoma of the thoracic esophagus: theJapan Clinical Oncology Group Study. J Thorac CardiovascSurg 1997;114(2):205–9.
48. Ando N, Iizuka T, Ide H, Ishida K, Shinoda M, Nishimaki T, et al.Surgery plus chemotherapy compared with surgery alone forlocalized squamous cell carcinoma of the thoracic esophagus: aJapan Clinical Oncology Group Study–JCOG9204. J Clin Oncol2003;21(24):4592–6.
49. Tabira Y, Sakaguchi T, Kuhara H, Teshima K, Tanaka M,Kawasuji M. The width of a gastric tube has no impact on outcomeafter esophagectomy. Am J Surg 2004;187(3):417–21.
50. Nozoe T, Sugimachi K. Simple staging criteria for esophagealcarcinoma: classification with a strict prognostic stratification. AmJ Clin Oncol 2003;26(3):307–11.
51. Nagamatsu Y, Shima I, Yamana H, Fujita H, Shirouzu K, IshitakeT. Preoperative evaluation of cardiopulmonary reserve with the
use of expired gas analysis during exercise testing in patients withsquamous cell carcinoma of the thoracic esophagus. J ThoracCardiovasc Surg 2001;121(6):1064–8.
52. Watanabe I, Fujihara H, Sato K, Honda T, Ohashi S, Endoh H,et al. Beneficial effect of a prone position for patients with hypo-xemia after transthoracic esophagectomy. Crit Care Med2002;30(8):1799–802.
53. Tashiro T, Yamamori H, Takagi K, Hayashi N, Furukawa K, NittaH, et al. Changes in immune function following surgery for esoph-ageal carcinoma. Nutrition 1999;15(10):760–6.
54. Sato N, Koeda K, Ikeda K, Kimura Y, Aoki K, Iwaya T, et al.Randomized study of the benefits of preoperative corticosteroidadministration on the postoperative morbidity and cytokine re-sponse in patients undergoing surgery for esophageal cancer. AnnSurg 2002;236(2):184–90.
55. Shimada Y, Imamura M. Prognostic factors for esophageal cancer– from the viewpoint of molecular biology. Gan To Kagaku Ryoho1996;23(8):972–81.
56. Law S, Fok M, Chu KM, Wong J. Comparison of hand-sewn andstapled esophagogastric anastomosis after esophageal resectionfor cancer: a prospective randomized controlled trial. Ann Surg1997;226(2):169–73.
57. Whooley BP, Law S, Alexandrou A, Murthy SC, Wong J. Criticalappraisal of the significance of intrathoracic anastomotic leakageafter esophagectomy for cancer. Am J Surg 2001;181(3):198–203.
58. Law S, Suen D, Wong K, Kwok K, Wong J. A single layer, continu-ous hand-sewn technique in esophageal anastomosis: prospectiveevaulation in 218 patients. Arch Surg (in press).
59. Fok M, Cheng SW, Wong J. Pyloroplasty versus no drainage ingastric replacement of the esophagus. Am J Surg 1991;162(5):447–52.
60. Lee YM, Law S, Chu KM, Wong J. Pyloroplasty in gastric replace-ment of the esophagus after esophagectomy: one-layer or two-layer technique? Dis Esophagus 2000;13(3):203–6.
61. Law S, Cheung MC, Fok M, Chu KM, Wong J. Pyloroplasty andpyloromyotomy in gastric replacement of the esophagus afteresophagectomy: a randomized controlled trial. J Am Coll Surg1997;184(6):630–6.
62. Law S, Boey JP, Kwok KF, Wong KH, Chu KM, Wong J. Pleuraldrainage after transthoracic esophagectomy: experience with avacuum system. Dis Esophagus 2004;17(1):81–6.
63. Choi HK, Law S, Chu KM, Wong J. The value of neck drainin esophageal surgery: a randomized trial. Dis Esophagus1998;11(1):40–2.
64. Wong AC, Law S, Wong J. Influence of the route of reconstructionon morbidity, mortality and local recurrence after esophagectomyfor cancer. Dig Surg 2003;20(3):209–14.
65. Davis PA, Law S, Wong J. Colonic interposition afteresophagectomy for cancer. Arch Surg 2003;138(3):303–8.
66. Tsui SL, Law S, Fok M, Lo JR, Ho E, Yang J, et al. Postoperativeanalgesia reduces mortality and morbidity after esophagectomy.Am J Surg 1997;173(6):472–8.
67. Murthy SC, Law S, Whooley BP, Alexandrou A, Chu KM, WongJ. Atrial fibrillation after esophagectomy is a marker for postopera-tive morbidity and mortality. J Thorac Cardiovasc Surg 2003;126(4):1162–7.
68. Whooley BP, Law S, Murthy SC, Alexandrou A, Wong J. Analysisof reduced death and complication rates after esophageal resec-tion. Ann Surg 2001;233(3):338–44.
69. Law S, Wong K, Kwok K, Chu K, Wong J. Predictive factorsfor postoperative pulmonary complications and mortality afteresophagectomy for cancer. Ann Surg (in press).
70. Fok M, Sham JS, Choy D, Cheng SW, Wong J. Postoperativeradiotherapy for carcinoma of the esophagus: a prospective, ran-domized controlled study. Surgery (St. Louis) 1993;113(2):138–47.
71. Law S, Fok M, Chow S, Chu KM, Wong J. Preoperative chemo-therapy versus surgical therapy alone for squamous cell carcinomaof the esophagus: a prospective randomized trial. J ThoracCardiovasc Surg 1997;114(2):210–17.
72. Whooley BP, Law S, Murthy SC, Alexandrou A, Chu KM, WongJ. The Kirschner operation in unresectable esophageal cancer: cur-rent application. Arch Surg 2002;137(11):1228–32.
73. Law S, Tung PH, Chu KM, Wong J. Self-expanding metallic stentsfor palliation of recurrent malignant esophageal obstructionafter subtotal esophagectomy for cancer. Gastrointest Endosc1999;50(3):427–36.

176
74. Tang JC, Lam KY, Law S, Wong J, Srivastava G. Detection ofgenetic alterations in esophageal squamous cell carcinomas andadjacent normal epithelia by comparative DNA fingerprintingusing inter-simple sequence repeat pcr. Clin Cancer Res 2001;7(6):1539–45.
75. Tang JC, Wan TS, Wong N, Pang E, Lam KY, Law SY, et al.Establishment and characterization of a new xenograft-derivedhuman esophageal squamous cell carcinoma cell line SLMT-1 ofChinese origin. Cancer Genet Cytogenet 2001;124(1):36–41.
76. Jin Y, Jin C, Law S, Chu KM, Zhang H, Strombeck B, et al.Cytogenetic and fluorescence in situ hybridization characterizationof clonal chromosomal aberrations and CCND1 amplification inesophageal carcinomas. Cancer Genet Cytogenet 2004;148(1):21–8.
77. Kwong D, Lam A, Guan X, Law S, Tai A, Wong J, et al. Chromo-somal aberrations in esophageal squamous cell carcinoma amongChinese: Gain of 12p predicts poor prognosis after surgery. HumPathol 2004;35(3):309–16.
78. Lam KY, Law S, Ma LT, Ong SK, Wong J. Pre-operative chemo-therapy for squamous cell carcinoma of the oesophagus: dohistological assessment and p53 overexpression predict chemo-responsiveness? Eur J Cancer 1997;33(8):1221–5.
79. Dawsey SM, Shen Q, Nieberg RK, Liu SF, English SA, Cao J, et al.Studies of esophageal balloon cytology in Linxian, China. CancerEpidemiol Biomarkers Prev 1997;6(2):121–30.
80. Wang GQ, Jiao GG, Chang FB, Fang WH, Song JX, Lu N, et al.Long-term results of operation for 420 patients with early squa-mous cell esophageal carcinoma discovered by screening. AnnThorac Surg 2004;77(5):1740–4.
81. Huang GJ, Gu XZ, Wang LJ, Wang M, Zhang DW, Yin WB, et al.Combined preoperative irradiation and surgery versus surgeryalone for squamous cell carcinoma of the midthoracic esophagus: aprospective randomized study in 360 patients. In: Ferguson MK,Little AG, Skinner DB, editors. Diseases of the esophagus. Malig-nant diseases. New York: Futura; 1990. p. 275–81.
82. Wang M, Gu XZ, Yin WB, Huang GJ, Wang LJ, Zhang DW.Randomized clinical trial on the combination of preoperative irra-diation and surgery in the treatment of esophageal carcinoma:report on 206 patients. Int J Radiat Oncol Biol Phys 1989;16(2):325–7.
83. Xiao ZF, Yang ZY, Liang J, Miao YJ, Wang M, Yin WB, et al.Value of radiotherapy after radical surgery for esophageal carci-noma: a report of 495 patients. Ann Thorac Surg 2003;75(2):331–6.
84. Fang W, Kato H, Chen W, Tachimori Y, Igaki H, Sato H. Compari-son of surgical management of thoracic esophageal carcinoma be-tween two referral centers in Japan and China. Jpn J Clin Oncol2001;31(5):203–8.