Embed Size (px)
Citation preview
8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 1/33
} ผูปวยชายไทยคูอายุ 62 ปมีโรคประ ตัวเปน ischemic heartdisease มีปญหา heart failure บอยๆB
} ยาทีกินเปนประ ไดแกB} !Aspirin(80) 1*1 pc
} !Digoxin(0.25) 1*1 pc
} !Furosemide (40) 1*2 pc (เชา-เทียง)} !Isordil (10) 1*3 ac
} !Enalapril(5) 1*1 pc
} !Simvastatin (20) 1*1 hs

8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 2/33
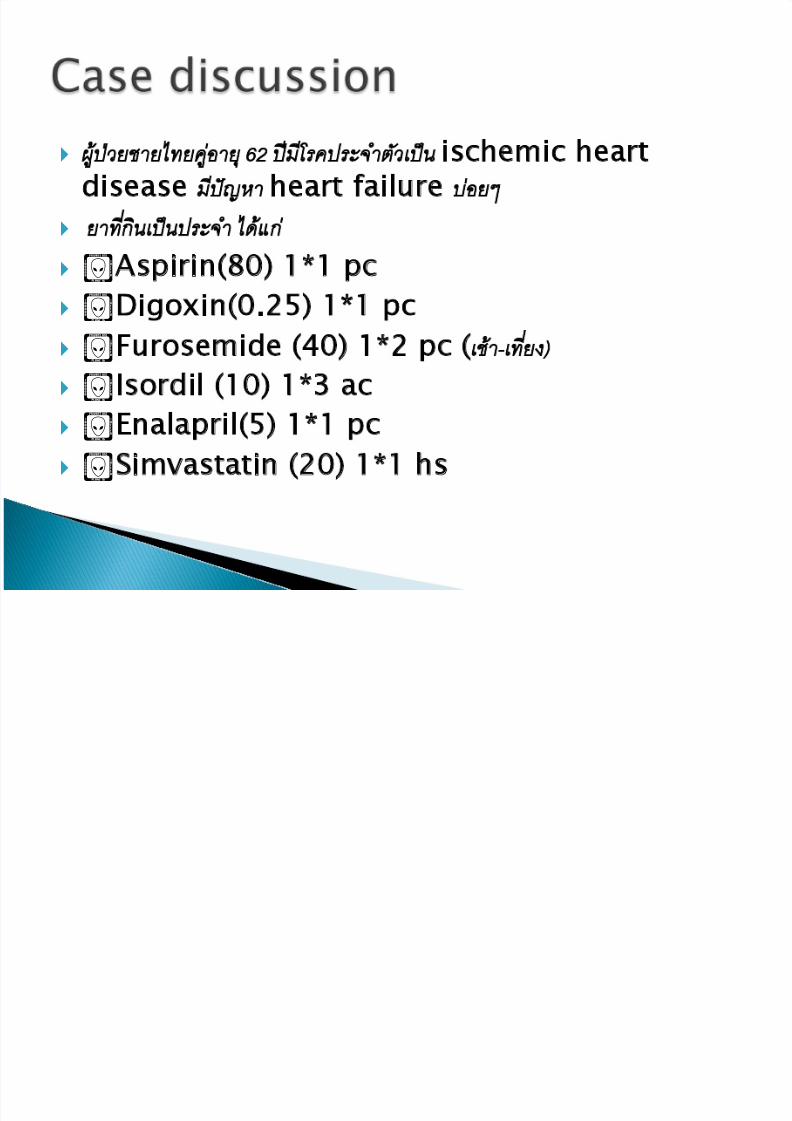
} วันนีมาพบแพทยทีโรงพยาบาลดวยอาการทองเสียถายเหลวB} เปนน้ ประมาณ6-7 ครัง รวมกับอาเจียนอีก 4 ครัง รูสกB} ออนเพลียมากจึงมาพบแพทย} แพทยตรวจรางกายพบ ชีพจรไมสม่ เสมอ34 ครังตอนาที ความดันโลหติB} 100/60 mmHg แพทยเห็นวาชีพจรชามากจึงสัง EKG
8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 3/33
8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 4/33
} Potassium 2.8 mEq/L (diarrhea+vomiting+furosemide)
} Digitalis level 3.5 ng/mL (0.8 - 2 ng/mL)
Impress; Digitalis Intoxication
} (precipitating factor : Hypokalemia)

8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 5/33
Paramat thimachai,MD
Resident2 toxicology unit

8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 6/33
} Digoxin เปนยาที่สกัดมาจาก ใบของพืชตระกูล
foxglove “ถุงมือจิ ้งจอก” เดมิจัดอยู ในวงศมณเฑียรทอง ( Scrophulariaceae) แตหลังจากการพจิารณาทางphylogenetic ก็ไดรับการจัด
ใหอยู ในตระกูลที่ใหญกวาในวงศเทียนเกล็ดหอย ( Plantaginaceae)
} Other names Digitalis, Lanoxin
} Inotropic and AV node blockingagent.
} Used in the treatment of congestive heart failure, atrialfibrillation, atrial flutter, andtachyarhythmias.
8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 7/33
} 60-85% absorbed after oral administration of tablets
} 75-80% absorbed after administration of elixir} 90-100% absorbed from liquid filled capsules} 80% absorbed from intramuscular injection (not
recommended)} 100% absorbed from intravenous dose
} 40% degraded by intestinal bacteria–1 in 10
8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 8/33
} Initial loading dose required.} 25% protein bound.
} 6-8 hour tissue distribution phase} Widely distributed Vd 5.6 L/kg } Correlates well with lean body
tissue .Early high levels of serumconcentration do not reflect actionat desired site
} Increase Vd in hypothyroid} Heart/blood level = 70/1} Hypokalemia increase
distritbution to heart and muscle.} Receptor binding is the rate
limiting step.} Crosses the placenta and enters
breast milk – Pregnancy category C
8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 9/33
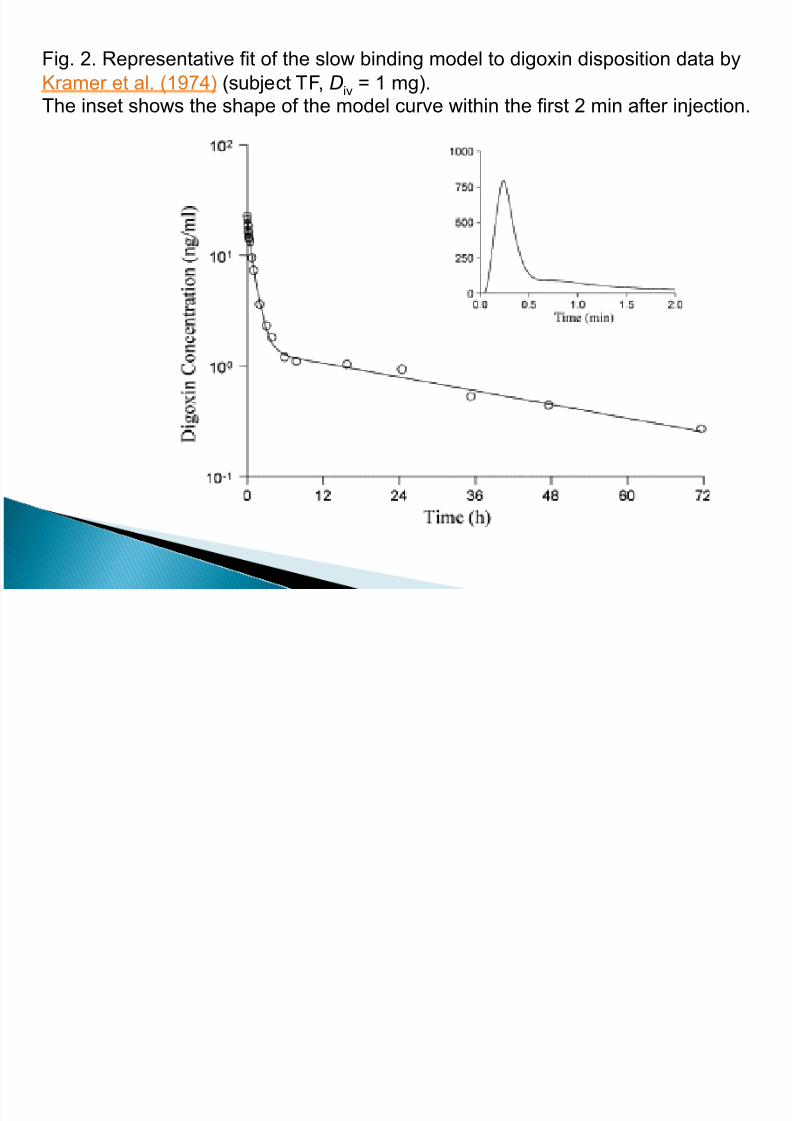
Fig. 2. Representative fit of the slow binding model to digoxin disposition data by
Kramer et al. (1974) (subject TF, Div = 1 mg).The inset shows the shape of the model curve within the first 2 min after injection.
8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 10/33
� Time to peak effect:
1-4 hours (IV) and 2-6 hours (PO)} Half life elimination ;
Parent drug 38 hrsMetabolite -digoxigenin 4 hrs
-monodigitoxoside 3-12 hrs� Therapeutic serum digoxin levels :
0.5-2ng/mL (6 hours after dose)Now is narrow 0.5-0.9 ng/mL
� Inhibits Na-K ATPase� Increases myocardial contraction
◦ Increased cardiac output◦ Improved circulation◦ Improved tissue perfusion
� Decreases conduction through AV node◦ Decreased heart rate

8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 11/33
� 16% is metabolized by liver� Metabolism ;Substrate of CYP 3A4 [minor]
� 50-70% is excreted almost entirelyunchanged by the kidneys
� Excretion proportional to GFR
� Half life: 36-48 hours,
increased in renal impairment
� Not effectively removed by dialysis
8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 12/33
} Toxicity level: >2.4ng/mL} 1/3 of patients have toxic
symptoms at <2.0ng/mL} First signs of toxicity:
◦ Abdominal pain◦ Anorexia◦ Nausea◦ Vomiting◦ Visual disturbances◦ Bradycardia◦
Arrhythmias◦ Confusion◦ Delirium
} Infants: arrhythmias
8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 13/33
} Serious adverse reaction
} May result in 1st, 2nd or 3rd degree block
} Ventricular dysrhythmias
} Three cardiac altered functions◦ Suppression of AV conduction
◦ Increased automaticity
◦ Decreased refractory period in ventricles
} Dilantin and Lidocaine effective treatment
8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 14/33
} The combination of SVT and AV block, for example, is highlysuggestive of digitalis toxicity .
} Although hypokalemia predisposes to digitalis toxicity,massive overdose can lead to hyperkalemia as inhibition of the Na-K-ATPase pump impairs potassium entry into cells.
} Plasma digoxin levels are markedly elevated in these patients,usually being above 10 ng/mL
} Other signs of toxicity can occur at lower levels of 3 to 5 ng/mL.
} Several factors (importantly hypokalemia) can predispose totoxicity at levels below 2 ng/mL, which is considered theupper limit of normal.
} On the other hand, clearly elevated levels (above 3 ng/mL)can be seen in asymptomatic patients.

8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 15/33
} Drug Interactions ◦ A number of drugs can raise digitalis levels by
interfering with its metabolism or renal excretion
◦ CYP 450 = CYP 3A4
} Colchicine,donedarone,midodrine - increase level.} Antiarrhythmics – increase serum levels of digoxin
} Spironolactone – increases half life of digoxin
} Beta blockers – additive bradycardia
} Thiazide and Loop diuretics – cause hypokalemia} Cortisone – Na retention and K loss} All of these increase the risk of toxicity

8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 16/33
} Renal insufficiency ◦ End-stage renal disease, prolongs the half-life of
digoxin and reduces its volume of distribution
◦ There must be reductions both in the loading dose
(by about 40 percent) and in the maintenance dose(by 50 to 75 percent) in this setting.
8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 17/33
} Finally, there are a number of factors thatcan increase the sensitivity to digoxin andpredispose to toxicity at plasma levels atthe upper limits of normal1. Old age
2. Certain cardiac diseases - active ischemia,myocarditis, cardiomyopathy, cardiac amyloidosis,cor pulmonale.
3. Metabolic factors - hypokalemia,hypomagnesemia, hypoxemia, hypernatremia,hypercalcemia, and acid-base disturbances.
8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 18/33
} Monitor pulse prior to administration} Monitor blood pressure throughout therapy
} Monitor ECG throughout IV administration
and periodically during therapy, as newarrhythmias and bradycardia may develop
} Kidney and thyroid dysfunction alters dosagerequired
} Increased age increases risk of toxicity
8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 19/33
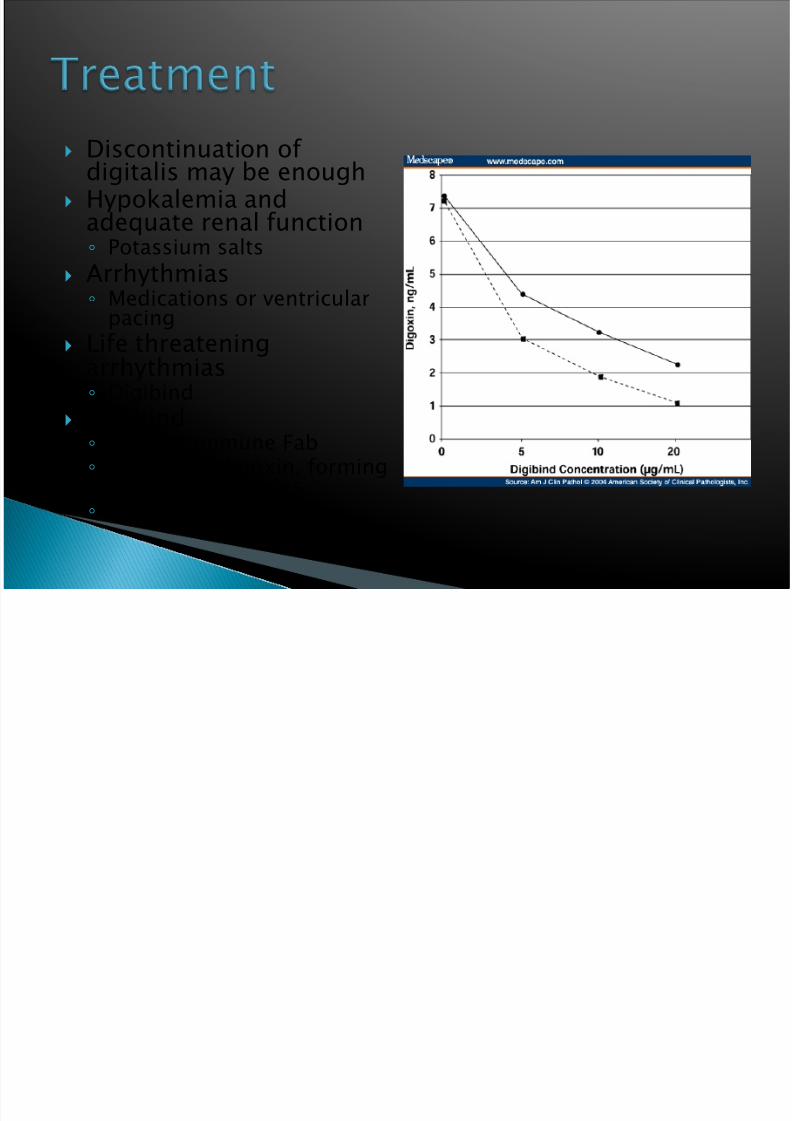
} Discontinuation of digitalis may be enough
} Hypokalemia andadequate renal function◦ Potassium salts
} Arrhythmias◦ Medications or ventricular
pacing
} Life threateningarrhythmias◦ Digibind
} Digibind◦ Digoxin immune Fab◦ Binds with digoxin, forming
complex molecules◦ Excreted in urine
8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 20/33
} Digoxin-specific antibody Fab fragments(Digibind®), purified from sheep IgG, rapidlybind to circulating digoxin and are indicatedin1. Ingestion of more than 10 mg of digoxin in adults
or 4 mg in children.
2. Plasma digoxin concentration above 10 ng/mL .
3. A plasma potassium concentration above 5 meq/L
in the presence of life-threatening arrhythmia –ventricular tachycardia or fibrillation, progressivebradycardia, or high degree AV nodal block.

8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 21/33
8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 22/33
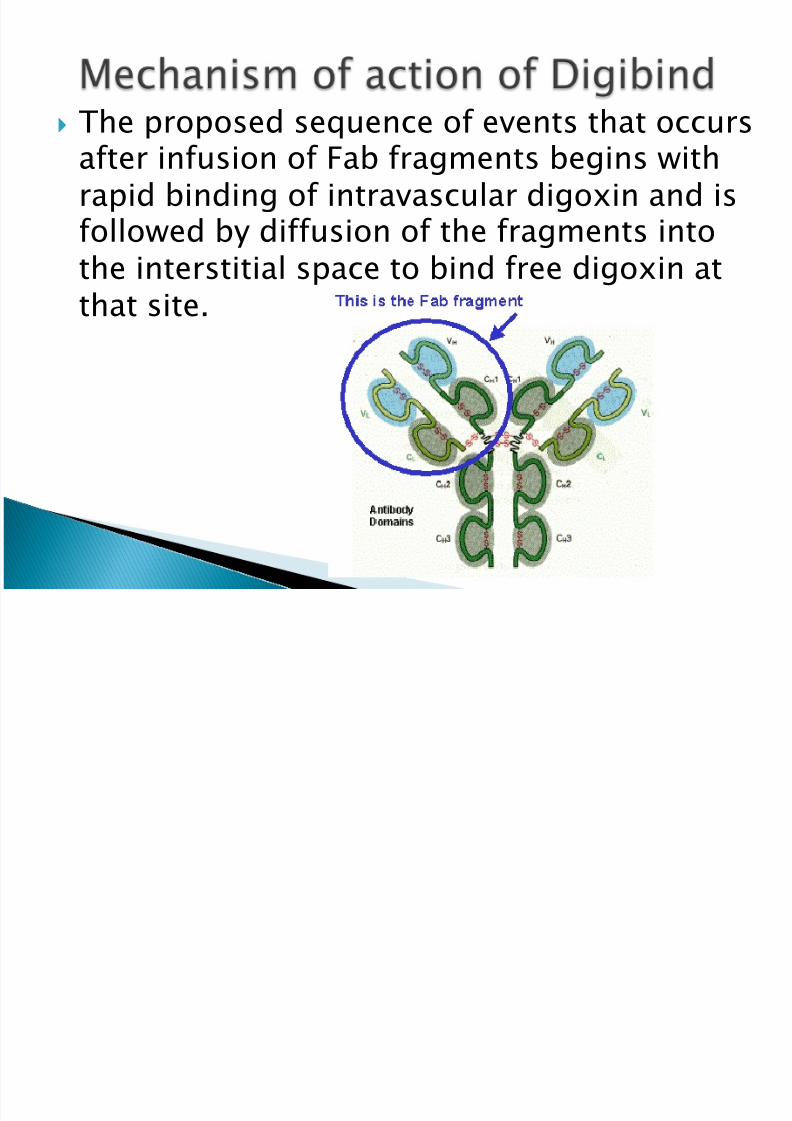
} The proposed sequence of events that occursafter infusion of Fab fragments begins withrapid binding of intravascular digoxin and isfollowed by diffusion of the fragments into
the interstitial space to bind free digoxin atthat site.

8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 23/33
} The affinity of the fragments for digoxin isgreater than the affinity of digoxin for Na-KATPase.
} The Fab fragments are relatively small (molwt 50,000) which allows them and bounddigoxin to be rapidly excreted byglomerular filtration in patients with near-
normal renal function.} The elimination half-life of the fragments is
15 to 20 hours in this setting.
8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 24/33
} Digibind can also be successfully in patientswith renal insufficiency, including those onmaintenance dialysis .
} In the largest study, 18 patients had apretreatment plasma creatinine concentrationof more than 5 mg/dL, including five whowere on dialysis.
} These patients responded to Digibind in amanner similar to patients with normal renalfunction.
8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 25/33
} In the largest series of 150 patients withlife-threatening digitalis toxicity,◦ 80 percent had resolution of all signs and
symptoms,
◦ 10 percent improved, and◦ 10 percent showed no response
} The median time to initial response was 19minutes and the time to complete responsewas 88 minutes
} Of the patients who experienced cardiacarrest, 54 percent survived hospitalization
8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 26/33
1. underlying heart disease that was the true cause of some of the presumed manifestations of digitalistoxicity.
2. too low a dose of Fab .
3. treatment of patients who were already moribund
} A dramatic fall in the plasma potassium concentration canoccur after digibind therapy .
} The decline in the plasma potassium concentration beginswithin one hour and is complete within 4 hrs.
} Thus, monitoring of the plasma potassium concentration
should be performed in all patients receiving this therapy
Several factors which contribute to
partial responses.

8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 27/33
} Despite the improvement induced by digibind,potentially important side effects can occur
1. Exacerbation of congestive heart failure,
2. Increased ventricular response in patientswith A-fib.
3. Hypokalemia .
} Idiosyncratic allergic manifestations are veryrare, occurring in less than one percent of cases.
} Plasma digoxin measurements are unreliable forone to two weeks after fragment therapy.
8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 28/33
} Total body load of digitalis (TBL, in mg)= SDC (serum digitalis concentration) x
volume of distribution x weight (kg)
} The serum digitalis concentration ismeasured in ng/mL and for digoxin, thevolume of distribution is 5.6 L/kg, therefore ◦ TBL = (SDC x 5.6 x weight) ÷ 1000
} One vial of digibind contains 40 mg, whichneutralizes approximately 0.6 mg of digoxin

8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 29/33
} Number of vials = TBL ÷ 0.6
Or
} Number of vials = (SDC x weight)
100
8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 30/33
} If the amount ingested is known, then the TBLcan be calculated directly:
} TBL = Dose ingested (mg) x 0.8 fordigoxin which has 80 percent bioavailability
} If the SDC and the amount ingested are not
known, then digibind is given empiricallyaccording to the following regimen
} For an acute overdose in adults:◦ Give 10 vials; repeat with another 10 vials if indicated
} With chronic toxicity:◦ Give 6 vials to an adult, one vial to a child
8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 31/33
} Hemodialysis or hemoperfusion can helpcontrol hyperkalemia or volume overloadin patients with concurrent renal failure
} They are, however, of limited utility inremoval of digoxin because of itsextensive tissue binding and very largevolume of distribution (5.6 L/kg)

8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 32/33
} Deglin, J.H. & Vallerand, A. H.. (2001). Daviss Drug Guide for Nurses (7th Ed.). E.A. Davis
Company:Philadelphia.
} Deska-Pagana, K. & Pagana, T.J.. (2002). Mosbys Manual of Diagnostic and Laboratory Tests(2nd Ed.). Mosby: St Louis.
} GlaxoKlineSmith. (2006). Lanoxin. [Online]. Available at http://us.gsk.com/products/assets/us_lanoxin_tablets.pdf.
} LeFever-Kee, J. & Hayes, E.R.. (2000). Pharmacology: A Nursing Process Approach. W.B.
Saunders: Philadelphia.} Muira, T., Kojima, R., Suguira, Y., Mizutani, M., Takatsu, F., & Suzuki, Y.. (2000). Effect of
aging on the incidence of digoxin toxicity. The Annals of Pharmacotherapy 34(4), 427-432.
} Weiss, M. (2007). Mechanistic modeling of digoxin distribution kinetics incorporating slowtissue binding. European Journal of Pharmaceutical Sciences 30(3-4), 256-263.
} Wikipedia. (2008). Digoxin. [Online]. Available at http://en.wikipedia.org/wiki/Digoxin.
} Wikipedia. (2008). Na-K-ATPase. [Online]. Available at http://en.wikipedia.org/wiki/Na%2B,K%2B-ATPase.
} Williamson, K., Thrasher, K., Fulton, K., Lapointe, N., Dunham, G., Cooper, A., Barrett, P., &Patterson, J.. (1998). Digoxin toxicity. Archives of Internal Medicine 158(22), 2444-2449.
8/4/2019 dig intox 23554
http://slidepdf.com/reader/full/dig-intox-23554 33/33