-
8/18/2019 dr.andrianto sympo-1.pdf
1/32
THE NEW GUIDELINES FOR MANAGEMENT OF STEMI :
Primary PCI, Lytics & Adjuvant Therapy
Andrianto
Devie Caroline
Dept. of Cardiology & Vascular Medicine
Airlangga University - Dr. Soetomo Teaching Hospital
Surabaya
-
8/18/2019 dr.andrianto sympo-1.pdf
2/32
TIME IS MUSCLE
EARLY DIAGNOSIS
EMERGENCY CARE
REPERFUSION
MYOCARDIAL
SALVAGE
Iniitial aim management of STEMI :
to restore blood flow to the infarct zone
-
8/18/2019 dr.andrianto sympo-1.pdf
3/32
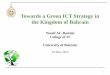
Comparing outcomes
PPCI vs Thrombolysis vs No Reperfusion
P < 0.001s
S. Dharma., D.A Juzar I. Firdaus et al. Neth Heart J (3012) 20:
354-259
% o
f m o r t a
l i t y
In-hospital mortality of STEMI patients
6.2
13.3
5.3
PPCI Fibrinolytic No Reperfusion
-
8/18/2019 dr.andrianto sympo-1.pdf
4/32
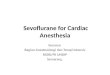
TIME & MORTALITY :
Primary PCI vs Thrombolysis
8
6
4
2
0
0 1 2 3 4 5 6
Onset of pain to treatment (hours)
3 0 - d a y m o
r t a l i t y ( %
)
7 8
12
10
Thrombolysis
Primary PCICommon
total ischaemia time
Huber K et al. Eur Heart J 2005;26:2063 –2074. Huber et al.
Eur Heart J 2005; 26: 1063-1074
-
8/18/2019 dr.andrianto sympo-1.pdf
5/32
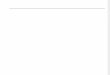
FMC= first medical contact; PCI= percutaneus coronary
intervention
A summary of important delays & treatmentgoals in the
management of acute STEMI
-
8/18/2019 dr.andrianto sympo-1.pdf
6/32
REPERFUSION
-
8/18/2019 dr.andrianto sympo-1.pdf
7/32
What The New Guideline Says ?
2013 ACCF/AHA Guideline for
The Management of STEMI
-
8/18/2019 dr.andrianto sympo-1.pdf
8/32
Fibrinolytic Therapy When
There Is an Anticipated Delay
to Performing Primary PCI
Within 120 Minutes of FMC
Reperfusion at a Non – PCI-CapableHospital
-
8/18/2019 dr.andrianto sympo-1.pdf
9/32
Indications for Transfer for Angiography
After Fibrinolytic Therapy
*Although individual circumstances will vary, clinical stability
is defined by the absence of low
output, hypotension, persistent tachycardia, apparent shock,
high-grade ventricular or symptomatic
supraventricular tachyarrhythmias, and spontaneous recurrent
ischemia.
-
8/18/2019 dr.andrianto sympo-1.pdf
10/32
Adjunctive Antithrombotic Therapy to Support
Reperfusion With Fibrinolytic Therapy
-
8/18/2019 dr.andrianto sympo-1.pdf
11/32
Adjunctive Antithrombotic Therapy to Support
Reperfusion With Fibrinolytic Therapy (cont.)
-
8/18/2019 dr.andrianto sympo-1.pdf
12/32
Transfer of Patients With
STEMI to a PCI Capable
Hospital for Coronary
Angiography After Fibrinolytic
Therapy
Reperfusion at a Non – PCI-CapableHospital
-
8/18/2019 dr.andrianto sympo-1.pdf
13/32
Indications for Transfer for Angiography
After Fibrinolytic Therapy
* Although individual circumstances will vary, clinical
stability is defined by the
absence of low output, hypotension, persistent tachycardia,
apparent shock,
high-grade ventricular or symptomatic supraventricular
tachyarrhythmias,
and spontaneous recurrent ischemia.
-
8/18/2019 dr.andrianto sympo-1.pdf
14/32
PCI of an Infarct Artery in
Patients Who Initially Were
Managed With Fibrinolysis or
Who Did Not Receive
Reperfusion Therapy
Delayed Invasive Management
-
8/18/2019 dr.andrianto sympo-1.pdf
15/32
Indications for PCI of an Infarct Artery in Patients
Who Were Managed With Fibrinolytic Therapy or
Who Did Not Receive Reperfusion Therapy
* Although individual circumstances will vary, clinical
stability is defined by the absence of low output,
hypotension, persistent tachycardia, apparent shock, high-grade
ventricular or symptomatic
supraventricular tachyarrhythmias, and spontaneous recurrent
ischemia.
-
8/18/2019 dr.andrianto sympo-1.pdf
16/32
PCI of a Noninfarct Artery Before Hospital
Discharge
PCI is indicated in a noninfarct artery at a time
separate from primary PCI in patients who have
spontaneous symptoms of myocardial ischemia.
PCI is reasonable in a noninfarct artery at a time
separate from primary PCI in patients with intermediate-
or high-risk findings on noninvasive testing.
I IIa IIb III
I IIa IIb III
Adj ti A tith b ti Th t S t PCI
-
8/18/2019 dr.andrianto sympo-1.pdf
17/32
Adjunctive Antithrombotic Therapy to Support PCI
After Fibrinolytic Therapy
-
8/18/2019 dr.andrianto sympo-1.pdf
18/32
Adjunctive Antithrombotic Therapy to Support PCI
After Fibrinolytic Therapy (cont.)
*Balloon angioplasty without stent placement may be used in
selected
patients. It might be reasonable to provide P2Y12 inhibitor
therapy to patients
with STEMI undergoing balloon angioplasty after fibrinolysis
alone
according to the recommendations listed for BMS. (Level of
Evidence: C )
-
8/18/2019 dr.andrianto sympo-1.pdf
19/32
Adjunctive Antithrombotic Therapy to Support
PCI After Fibrinolytic Therapy (cont.)
-
8/18/2019 dr.andrianto sympo-1.pdf
20/32
Primary PCI in STEMI
Reperfusion at a PCI-CapableHospital
-
8/18/2019 dr.andrianto sympo-1.pdf
21/32
Primary PCI in STEMI
-
8/18/2019 dr.andrianto sympo-1.pdf
22/32
Adjunctive Antithrombotic Therapy to
Support Reperfusion With Primary PCI
*The recommended maintenance dose of aspirin to be
used with ticagrelor is 81 mg daily.
-
8/18/2019 dr.andrianto sympo-1.pdf
23/32
Indications for Fibrinolytic Therapy When There Is
a >120-Minute Delay From FMC to Primary PCI
-
8/18/2019 dr.andrianto sympo-1.pdf
24/32
Routine Medical TherapiesGuideline for STEMI
-
8/18/2019 dr.andrianto sympo-1.pdf
25/32
Beta Blockers
Oral beta blockers should be initiated in the first 24 hours
inpatients with STEMI who do not have any of the following:
signs
of HF, evidence of a low output state, increased risk for
cardiogenic shock,* or other contraindications to use of oral
beta
blockers (PR interval >0.24 seconds, second- or
third-degree
heart block, active asthma, or reactive airways disease).
Beta blockers should be continued during and after
hospitalization for all patients with STEMI and with no
contraindications to their use.
Risk factors for cardiogenic shock (the greater the number of
risk factors present, the higher the
risk of developing cardiogenic shock) are age >70 years,
systolic BP 110 bpm or heart rate
-
8/18/2019 dr.andrianto sympo-1.pdf
26/32
Renin-Angiotensin-Aldosterone System Inhibitors
An ACE inhibitor should be administered within
the first 24 hours to all patients with STEMI with
anterior location, HF, or EF ≤ 0.40, unlesscontraindicated.
An ARB should be given to patients with STEMIwho have
indications for but are intolerant of
ACE inhibitors.
I IIa IIb III
I IIa IIb III
-
8/18/2019 dr.andrianto sympo-1.pdf
27/32
Renin-Angiotensin-Aldosterone System Inhibitors
An aldosterone antagonist should be given to
patients with STEMI and no contraindications who
are already receiving an ACE inhibitor and beta
blocker and who have an EF ≤ 0.40 and either
symptomatic HF or diabetes mellitus.
ACE inhibitors are reasonable for all patients with
STEMI and no contraindications to their use.
I IIa IIb III
I IIa IIb III
-
8/18/2019 dr.andrianto sympo-1.pdf
28/32
Lipid Management
High-intensity statin therapy should be
initiated or continued in all patients with
STEMI and no contraindications to its
use.
It is reasonable to obtain a fasting lipid
profile in patients with STEMI, preferably
within 24 hours of presentation.
I IIa IIb III
I IIa IIb III
-
8/18/2019 dr.andrianto sympo-1.pdf
29/32
Summary
•The first therapeutic aim of STEMI is restore blood flow
toinfarct zone in order to myocardial salvage by reperfusion
therapy.
• Primary PCI is preferred reperfusion methodes; when itcannot
be perfomed in due time ( more than 120 minutes),
fibrinolysis followed by coronary angiography in the the
next few hours (3-24 hours) constitutes a valid alternative.
• Beside reperfusion therapy, management of STEMI requires
antithrombotic medications combining dual antiplatelet
therapy and anti coagulant , B-blockers, ACE-I and statin
-
8/18/2019 dr.andrianto sympo-1.pdf
30/32
For Your Attention
-
8/18/2019 dr.andrianto sympo-1.pdf
31/32
-
8/18/2019 dr.andrianto sympo-1.pdf
32/32
Media campaign
Patient education
Methods ofSpeeding
Time to
Reperfusion
Greater use of
9-1-1
Prehospital Rx
MI protocol
Critical pathway
Qualityimprovement
program
Bolus lyticsDedicated
PCI team
5 min < 30 minD-B ≤ 90 min
D-N ≤ 30 min
Goals
Prehospital
ECG
Patient Transport Inhospital Reperfusion
Reperfusion